

Abstract
Purpose
To identify the relationship of race and gender with 3 aspects of life satisfaction and depressive symptoms after spinal cord injury (SCI), evaluating the extent to which socioeconomic factors mediate any observed relationships.
Methods
Adults with traumatic SCI of at least 1-year duration (N = 1,549) were identified through a Southeastern United States SCI Model System of care, and cross-sectional survey data were collected at a Southeastern United States medical university. Three aspects of life satisfaction (home life satisfaction, vocational satisfaction, global satisfaction) were measured using 20 satisfaction items from the Life Situation Questionnaire-Revised. The Older Adult Health and Mood Questionnaire measured depressive symptoms. MANCOVA assessed mediation of socioeconomic status between race and life satisfaction and depression.
Results
Home life satisfaction and vocational satisfaction were significantly related to race, with White participants scoring higher than Black participants during the first stage of the regression. However, socioeconomic factors mediated the relationships such that race was no longer significant after considering economic factors. Race was significantly associated with global satisfaction after adjusting for socioeconomic factors. Depression was not significantly related to race. Gender was unrelated to all study outcomes. Of the socioeconomic mediators, family income was a significant predictor of each outcome, whereas education was only predictive of vocational satisfaction.
Conclusion
Socioeconomic factors are important mediators of the relationship between race and certain aspects of life satisfaction among persons with SCI. Family income and, to a lesser extent, education should be considered when evaluating race differences in life satisfaction after SCI.
Keywords: depression, health status disparities, socioeconomic factors, spinal cord injury
Aside from physical effects, spinal cord injury (SCI) may lead to serious consequences including an elevated risk of depressive disorders and decreased satisfaction with life (SWL).1–4 Racial disparities in SWL and depression among subpopulations of persons with SCI have been noted in numerous studies, showing higher risk of depression and lower levels of SWL among Blacks than among Whites.2,5–9 In addition, some studies showed the disparity in risk of depression to be even greater among Black women with SCI.7,10 However, with regard to gender disparities in SWL, mixed findings have been observed with most trends likely to not be significant.11 Although racial disparities have been seen in SWL and depression after SCI, it is unlikely that race itself is the cause of the differences. In the general US population, there are disparities in income between Whites and Blacks, with Whites having a higher median household income.12 Therefore, differences in socioeconomic status (SES) could be contributing to the disparities. Many of the existing studies looking at disparities have not controlled for SES, although this has been shown to mediate disparities with regard to other outcomes among persons with SCI. One previous study found SES did not fully mediate the relationship between race and clinically significant depressive symptomatology among persons with SCI, as Black women were still at elevated risk of depression.2
Mediational models have proven to be useful tools for observing interrelationship predictor variables and outcomes.2,10,13–15 Prior studies have used mediational models relating independent variables (ie, gender, race, or age) with various outcomes (ie, subjective well-being, SWL, and depression) to examine whether education and income will mediate and account for the existing trends among persons with SCI.2,10
For the mediational model to be valid, relationships must be established between all variables tested (Figure 1). The mediational model assumes:
Figure 1.
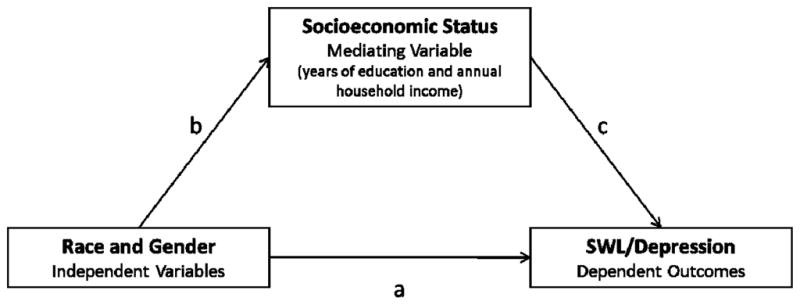
Mediational Model
A direct correlation between the independent variables and dependent outcomes.
A direct correlation between the mediating variable and independent variables.
A direct correlation between the mediating variable and dependent outcomes.
Once the first 3 conditions are met, one can examine whether the original correlation between the independent and dependent variables remains unchanged after controlling for the mediating variable.
Using a mediational model, literature has shown that disparities in levels of depression are reduced but not eliminated when controlling for years of education and household income. For instance, years of education and household income were found to mediate the relationships between race and a depressive diagnosis for men but not for women.2 The odds of a depressive diagnosis were no longer statistically significant for Black men after introduction of SES mediators. However, the odds of a depressive diagnosis decreased, but were not eliminated, for Black women after introducing these mediators.2 Research has determined that Black persons with SCI report lower satisfaction in some areas compared with White persons.6 Significant disparities have been noted in career satisfaction, opportunities for skill development, and finances among racial groups, with Black participants scoring lower than White participants on these factors.16,17 This finding further suggests that the differences in Blacks and Whites in access to economic resources may account for disparities in health outcomes.13,18 However, race differences appeared to be restricted to vocational and economic areas and did not generalize to other aspects of SWL.
The purpose of this study was to use a mediational model to analyze the relationship between race and gender with SWL and depression among persons with SCI, using socioeconomic variables as mediators. The independent variables tested were gender and race. Scores from 3 satisfaction factors and a measure of depressive symptoms were used as outcomes. Years of education and annual household income were then tested as the mediating variables within this mediational model.
Two hypotheses were tested:
Race is related to SWL and depressive symptomatology, but the relationship is mediated by SES as measured by income and education.
Gender is related to SWL and depressive symptomatology, but the relationship is mediated by SES as measured by income and education.
METHODS
Participants
After institutional review board approval, participants were selected from 3 different sources of records at a large specialty hospital in the Southeastern United States that is part of the SCI Model Systems: (1) SCI Model Systems patient database, (2) Model Systems registry, and (3) outpatient directory. Although participants were identified through one of the SCI Model Systems, our data were specifically collected for this study, and we did not utilize any of the data routinely collected by the SCI Model Systems. Potential participants met 3 inclusion criteria: traumatic SCI, 18 years old or older at the time of study, and minimum of 1 year post injury. The response rate for the survey was 62.5%, with 1,549 of 2,480 potential participants meeting the criteria and returning their survey. Participants differed from nonparticipants on gender (males were less likely to respond) and race (Whites were more likely to respond than Blacks). Only participants who self-identified as either “White, non-Hispanic” or “Black, non-Hispanic” were included in the analysis as there were too few persons who identified as Hispanic for meaningful analysis. This eliminated less than 6% of the total participants, leaving 1,466 for analysis.
Procedures
Preliminary letters describing the research and method by which potential participants would receive materials were sent 5 weeks prior to the initial survey packet. The initial packet included a letter about the study that served as implied consent, as well as the survey to be completed and returned by mail. A second mailing was set in place for all who did not return their first packet. If there was no response to the second mailing, a phone call was made to engage in active conversation with the potential participant. A third mailing was used only for those who consented by phone to receive another packet due to either misplacing or accidently discarding the original survey. Remuneration of $50 was given to all participants who completed the survey.
Measures
The Life Situation Questionnaire-Revised (LSQ-R) was used to measure SWL.19 It includes 20 satisfaction items. Each was measured using a 5-point Likert scale where 1 = very dissatisfied and 5 = very satisfied. Three factor scales were identified in earlier research, including home life satisfaction (HLS), vocational satisfaction (VOC), and global satisfaction (GS).20 Alpha coefficients ranged from .78 to .93, with an average coefficient of .86.
The Older Adult Health and Mood Questionnaire (OAHMQ) is a 22-item set of true or false questions that measures depressive symptoms.21 It was designed to minimize the number of somatic symptoms that may compromise its validity with older adults and with those who have medical complications. In terms of validity when screening for any depressive disorder, the sensitivity was found to be .93 and the specificity was .87.21–23
The OAHMQ and 3 validated categorical satisfaction factors developed from the LSQ-R (HLS, VOC, and GS) were used in this study as dependent variables. The independent variables measured in this study consisted of participants grouped into either gender (men vs women) or race (White vs Black) categories. Socioeconomic indicators, years of education, and annual household income were used as mediating variables. Education was measured as the number of years of education completed at survey. Household income was measured by 8 response categories for income: <$10,000, $10,000–14,999, $15,000–19,999, $20,000–24,999, $25,000–34,999, $35,000–49,999, $50,000–74,999, $75,000+. Additionally, injury level (cervical vs noncervical), ambulatory status (yes vs no), etiology (violent vs nonviolent), age, and years post injury were used as statistical controls in each model.
Analyses
Descriptive statistics of the gender and race categories, injury -elated variables, the 3 satisfaction factors of the LSQ-R, and the overall OAHMQ score were generated.
Multivariate analysis of covariance (MANCOVA) was used to identify the main effects for gender and race and the interaction effects between gender and race across the SWL outcomes (HLS, VOC, GS), since the 3 outcomes are part of the same measurement tool. Analysis of covariance (ANCOVA) was used to identify the main effects for gender and race for the OAHMQ.
MANCOVA was further used to assess whether the mediating variables accounted for the observed significant relationships between independent and dependent variables. Stage 1 of the MANCOVA controlled for injury-related variables such as chronologic age, cause of injury, number of years post injury, ambulation, and neurologic level of injury. Stage 2 included the independent variables (gender and race). Stage 3 added the socioeconomic indicators (years of education and annual household income). If mediation is indeed observed, any significant effects seen between race and gender with depression and SWL scores should become nonsignificant at Stage 3. Using the same stages, ANCOVA was used to assess the relationships between independent variables and the OAHMQ. We tested for collinearity between education and income for each outcome using tolerance and the variance inflation factor.
RESULTS
The majority of participants were men (73%) and White (77%). The average age of participants at the time of study was 45.1 years (SD = 13.5; range, 18–85), and the average number of years post injury was 12.6 years (SD = 8.8; range, 1–59). Level of injury among participants was classified as cervical (52%) and noncervical (48%). Violent etiology accounted for 8% of injuries. The average number of years of education was 13.7 years (range, 5–20). Twenty-two percent of participants reported an annual household income of $75,000 or more. Twenty-one percent of participants reported probable major depression as defined by an OAHMQ score of 11 or more, and the average OAHMQ score was 6.3 (SD = 5.0). The average score for HLS was 15.6 (SD = 3.9), for VOC was 8.6 (SD = 3.8), and for GS was 42.3 (SD = 10.9).
MANCOVA statistics revealed significant main effects for race but not for gender (Table 1). The interaction effects with gender and race were also not significant for any of the outcomes. Race was significantly related to HLS and VOC but not GS or the OAHMQ.
Table 1.
The effects of race and gender on satisfaction with life and depression outcomes
| Gender | Race | Gender F statistic | Race F statistic | |||
|---|---|---|---|---|---|---|
|
| ||||||
| Male | Female | Black | White | |||
|
| ||||||
| Mean (SD) | ||||||
| Home life satisfaction | 15.52 (3.87) | 15.78 (4.03) | 15.11 (3.98) | 15.43 (3.88) | 0.99 | 5.08* |
| Vocational satisfaction | 8.45 (3.80) | 8.82 (3.72) | 7.35 (3.48) | 8.91 (3.79) | 3.36 | 36.42** |
| Global satisfaction | 42.43 (10.79) | 42.00 (11.24) | 42.19 (11.29) | 42.35 (10.81) | 1.23 | 0.07 |
| Overall satisfactiona | 5.37* | 19.67** | ||||
| OAHMQ | 6.22 (5.05) | 6.44 (4.89) | 6.64 (4.50) | 6.18 (5.15) | 0.51 | 2.12 |
Note: OAHMQ = Older Adult Health and Mood Questionnaire.
P < .05.
P < .0001.
Wilks lamda test of overall effect.
Results from the MANCOVA (for HLS, VOC, and GS) and ANCOVA (for OAHMQ) are presented in Tables 2 and 3. Overall results from the MANCOVA showed age, years post injury, injury level, and violent etiology were significant in Stage 1. After gender and race were included, both of which were significant, violent etiology became not significant. Finally, after years of education and household income were included, injury level also became not significant.
Table 2.
Multivariate analysis of covariance results of satisfaction with life
| Stage 1 | Stage 2 | Stage 3 | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| F statistic | P | F statistic | P | F statistic | P | |
| Overall satisfactiona | ||||||
| Age | 19.01 | <.0001 | 21.90 | <.0001 | 21.26 | <.0001 |
| Years post injury | 6.63 | .0002 | 7.26 | <.0001 | 7.30 | <.0001 |
| Injury level | 4.00 | .0075 | 2.89 | .0346 | 1.94 | .1217 |
| Ambulation | 2.08 | .1007 | 2.19 | .0876 | 1.26 | .2876 |
| Violent etiology | 4.63 | .0032 | 0.82 | .4818 | 1.22 | .3015 |
| Gender | - | - | 6.60 | .0002 | 6.46 | .0002 |
| Race | - | - | 14.95 | <.0001 | 5.67 | .0007 |
| Years education | - | - | - | - | 11.45 | <.0001 |
| Household income | - | - | - | - | 64.31 | <.0001 |
| Home life satisfactionb | ||||||
| Age | 8.27 | .0041 | 8.72 | .0032 | 7.47 | .0064 |
| Years post injury | 0.75 | .3857 | 0.89 | .3460 | 0.52 | .4722 |
| Injury level | 0.41 | .5228 | 0.81 | .3674 | 1.02 | .3135 |
| Ambulation | 3.42 | .0645 | 3.17 | .0751 | 0.61 | .4350 |
| Violent etiology | 5.00 | .0255 | 2.04 | .1531 | 0.72 | .3972 |
| Gender | - | - | 0.68 | .4094 | 1.29 | .2556 |
| Race | - | - | 2.50 | .1138 | 1.11 | .2913 |
| Years education | - | - | - | - | 0.23 | .6347 |
| Household income | - | - | - | - | 90.90 | <.0001 |
| Vocational satisfactionb | ||||||
| Age | 14.26 | .0002 | 16.83 | <.0001 | 14.74 | .0001 |
| Years post injury | 2.77 | .0961 | 2.27 | .1318 | 3.31 | .0692 |
| Injury level | 7.00 | .0082 | 3.74 | .0534 | 2.00 | .1572 |
| Ambulation | 4.61 | .0321 | 4.33 | .0376 | 2.44 | .1184 |
| Violent etiology | 11.22 | .0008 | 1.40 | .2369 | 1.31 | .2528 |
| Gender | - | - | 1.70 | .1926 | 0.64 | .4241 |
| Race | - | - | 23.90 | <.0001 | 0.74 | .3911 |
| Years education | - | - | - | - | 25.22 | <.0001 |
| Household income | - | - | - | - | 173.06 | <.0001 |
| Global satisfactionb | ||||||
| Age | 1.43 | .2313 | 1.74 | .1869 | 2.85 | .0919 |
| Years post injury | 5.28 | .0217 | 5.72 | .0170 | 7.25 | .0072 |
| Injury level | 0.09 | .7688 | 0.25 | .6169 | 0.10 | .7546 |
| Ambulation | 5.30 | .0215 | 6.00 | .0144 | 2.79 | .0949 |
| Violent etiology | 1.95 | .1624 | 2.02 | .1558 | 0.12 | .7337 |
| Gender | - | - | 2.99 | .0842 | 3.33 | .0682 |
| Race | - | - | 0.08 | .7733 | 7.50 | .0063 |
| Years education | - | - | - | - | 2.54 | .1111 |
| Household income | - | - | - | - | 72.00 | <.0001 |
Wilks lamda test of overall effect.
Type III sum of squares (SS).
Table 3.
Analysis of covariance results of Older Adult Health and Mood Questionnaire (OAHMQ)
| Stage 1 | Stage 2 | Stage 3 | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| OAHMQa | F statistic | P | F statistic | P | F statistic | P |
| Age | 3.09 | .0788 | 3.10 | .0784 | 4.56 | .0329 |
| Years post injury | 3.51 | .0612 | 3.52 | .0609 | 5.05 | .0248 |
| Injury level | 3.63 | .0570 | 3.61 | .0577 | 3.58 | .0587 |
| Ambulation | 2.18 | .1401 | 1.96 | .1622 | 3.98 | .0463 |
| Violent etiology | 6.61 | .0103 | 4.39 | .0364 | 0.73 | .3920 |
| Gender | - | - | 0.46 | .4995 | 1.84 | .1750 |
| Race | - | - | 0.51 | .4752 | 2.46 | .1170 |
| Years education | - | - | - | - | 11.28 | .0008 |
| Household income | - | - | - | - | 47.25 | <.0001 |
Type III sum of squares (SS).
Home Life Satisfaction (Table 2)
Age and violent etiology were significantly associated with HLS in Stage 1. Neither race nor gender was significant when added in Stage 2, and only age remained significant. Household income was significant in the third and final stage, although education was not. Age remained significant in Stage 3.
Vocational Satisfaction (Table 2)
In Stage 1, age, injury level, ambulatory status, and violent etiology were all significantly associated with VOC. Race was also significantly related to VOC in Stage 2, although gender was not related to VOC; violent etiology was no longer significant. Both years of education and household income were associated with VOC (Stage 3). However, after the addition of these 2 variables to the final model, race and ambulation were no longer significant. Age was the only other predictor that remained statistically significant in the final model.
Global Satisfaction (Table 2)
Years since injury and ambulatory status were significant predictors of GS (Stage 1). Neither race nor gender was significant in Stage 2, and there was no change in any of the control predictors. Household income was significant in the final model, although years of education was not. Although race did not enter into the equation in Stage 2, it was significant in the final model along with years since injury (ambulatory status dropped out of the final model).
Depression (Table 3)
Only violent etiology was significantly associated with the OAHMQ in Stage 1. Neither race nor gender was significant in Stage 2, but violent etiology remained significant. Both years of education and household income were significantly related to the OAHMQ. Additionally, age, years post injury, and ambulatory status were significantly associated with the OAHMQ in Stage 3.
DISCUSSION
We evaluated the mediation of SES on the relationships of race and gender with SWL and depression. There was partial support for the existence of mediational models. However, the findings provided mixed support for those observed in previous research.
Our first hypothesis suggested that Black participants would report lower SWL and higher depression scores than White participants, but this relationship would be mediated by years of education and income. There was partial support for this hypothesis. Two out of 3 satisfaction factors (VOC and HLS) were significantly correlated to race, but race was not associated with depression. As predicted, Black participants reported significantly lower VOC and HLS scores than White participants. Furthermore, these relationships disappeared after accounting for socioeconomic factors of education and income. It is not surprising that our data are consistent with the findings of racial trends in previous studies, considering that VOC encompasses finances, careers, and job opportunities.5,6,17,20 The reported number of years of education was not a significant mediator for HLS scores. This particular finding is inconsistent with the findings of prior studies, which included years of education as a mediating variable.2,10 It could be that separate dimensions of SWL (ie, VOC and HLS) have different mediating variables. Education was a mediator with regard to VOC, as would be expected since education is so strongly linked with vocation; however, education might not relate to HLS.
The predicted relationships did not hold for GS. In fact, race did not significantly enter into the equation and was only significant after the introduction of socioeconomic factors. Therefore, the condition for mediation that includes an initially significant relationship between the independent or predictor variable (race) and the dependent or outcome variable (GS) was not met. Nevertheless, years of education and income were clearly related to GS and, when considered, changed a nonsignificant relationship for race and GS into a significant relationship. Therefore, they served as suppressor variables rather than mediators, meaning that the association between race and GS was increased with the addition of SES variables. Even though there was no difference between race and GS preliminarily, the true association was brought out with the addition of SES.
Our second hypothesis of gender differences was completely rejected, as gender was not significantly associated with any of the 4 outcomes. This finding runs contrary to previous research suggesting women have significantly higher depression scores.2,7,21,24 The primary study, of which the current project is an extension,2 found consistent relationships between both race and gender and the odds of depressive diagnosis. This relationship was mediated by education and income for men (the race effect was no longer significant for men) and partially mediated for women, as Black women continued to have greater odds of a depressive disorder. One possible explanation is that all Blacks were grouped together in the previous research, whereas the current study only compared White and Black, non-Hispanic participants.
Implications
Our results showed that although racial disparities in SWL exist among persons with SCI, these disparities are mostly accounted for after controlling for socioeconomic indicators. These results highlight that the true disparities in SWL may be due to a lack of resources more than racial disparities. The effect of resources on health outcomes is an important issue and had been demonstrated to affect mortality after SCI.25 Furthermore, the existing effect of SES on the dependent outcomes would suggest that racial groups compensate for their lack of VOC through other potential means or sources, considering that disparities in SES are still present.
Limitations
Although this study provides valuable information, several limitations should be noted. First, information in this study was obtained through self-report. Our outcomes were subjective in measure, thus self-report is needed; several of our predictor variables were objective and could result in reporter error. Second, we were not able to assess race groups other than White and Black; therefore, our results may not be generalizable to other race groups. Third, this study focused on long-term outcomes, as defined by a minimum of 1 year post injury. Therefore, the findings do not generalize to the first year, which is the most difficult transitioning time. Fourth, we used the OAHMQ, which is a validated measure used in multiple studies, but we did not have a clinical diagnosis of depression. Last, these data were cross-sectional and do not demonstrate the effect of changes in socioeconomic variables on the outcomes.
Future research
SWL can be helpful for identifying themes in a person’s life that could be potential risks for depression. However, it is still not a discrete variable measuring the magnitude of risk a person has for depression. Furthermore, the measurement of SWL is difficult to gauge for comparison since one person’s view of his or her life, even under similar conditions, may be different from another person’s. Many benefits can come from identifying those aspects of life that a person holds in high value. Methods need to be discovered for measuring an individual’s own positive life factors so that emphasis can be placed during rehabilitation efforts and health care providers can offer the best patient care.
Conclusion
Relationships between race and overall SWL among persons with SCI are at least partially mediated by socioeconomic factors. Therefore, household income and, to a lesser extent, years of education should be considered when evaluating race differences in SWL after SCI.
Acknowledgments
The contents of this publication were developed under grants from the Department of Education, NIDRR, H133G050165, H133B090005, and H133A080064. However, these contents do not necessarily represent the policy of the Department of Education, and you should not assume endorsement by the Federal Government.
This publication was made possible by grant 1R01 NS 48117 from the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
- 1.Krause JS. Secondary conditions and spinal cord injury: a model for prediction and prevention. Top Spinal Cord Inj Rehabil. 1996;2(2):217–227. [Google Scholar]
- 2.Krause JS, Kemp B, Coker JL. Depression after spinal cord injury: relation to gender, ethnicity, aging, and socioeconomic indicators. Arch Phys Med Rehabil. 2000;81(8):1099–1109. doi: 10.1053/apmr.2000.7167. [DOI] [PubMed] [Google Scholar]
- 3.Dijkers MP. Quality of life in individuals with spinal cord injury: a review of conceptualization, measurement, and research findings. J Rehab Res Dev. 2005;42(suppl 3):87–110. doi: 10.1682/jrrd.2004.08.0100. [DOI] [PubMed] [Google Scholar]
- 4.van Koppenhagen CF, Post MW, van der Woude LH, et al. Changes and determinants of life satisfaction after spinal cord injury: a cohort study in the Netherlands. Arch Phys Med Rehabil. 2008;89(9):1733–1740. doi: 10.1016/j.apmr.2007.12.042. [DOI] [PubMed] [Google Scholar]
- 5.Krause JS, Saladin LK, Adkins RH. Disparities in subjective well-being, participation, and health after spinal cord injury: a 6-year longitudinal study. NeuroRehabil. 2009;24(1):47–56. doi: 10.3233/NRE-2009-0453. [DOI] [PubMed] [Google Scholar]
- 6.Krause JS. Subjective well-being after spinal cord injury: relationship to gender, race-ethnicity, and chronologic age. Rehabil Psychol. 1998;43(4):282–296. [Google Scholar]
- 7.Krause JS, Broderick LE, Broyles J. Subjective well-being among African-Americans with spinal cord injury: an exploratory study between men and women. NeuroRehabil. 2004;19(2):81–89. [PubMed] [Google Scholar]
- 8.Dijkers MP. Correlates of life satisfaction among persons with spinal cord injury. Arch Phys Med Rehabil. 1999;80(8):867–876. doi: 10.1016/s0003-9993(99)90076-x. [DOI] [PubMed] [Google Scholar]
- 9.Dowler R, Richards JS, Putzke JD, Gordon W, Tate D. Impact of demographic and medical factors on satisfaction with life after spinal cord injury: a normative study. J Spinal Cord Med. 2001;24(2):87–91. doi: 10.1080/10790268.2001.11753560. [DOI] [PubMed] [Google Scholar]
- 10.Krause JS, Broderick LE, Saladin LK, Broyles J. Racial disparities in health outcomes after spinal injury: mediating effects of education and income. J Spinal Cord Med. 2006;29:17–25. doi: 10.1080/10790268.2006.11753852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Krause JS, Broderick LE. Outcomes after spinal cord injury: comparisons as a function of gender and race and ethnicity. Arch Phys Med Rehabil. 2004;85:355–362. doi: 10.1016/s0003-9993(03)00615-4. [DOI] [PubMed] [Google Scholar]
- 12.DeNavas-Walt C, Proctor BD, Smith JC. [Accessed May 4, 2011.];Income, poverty, and health insurance coverage in the United States: 2007. 2008 http://www.census.gov/prod/2008pubs/p60-235.pdf.
- 13.Gaglia MA, Jr, Steinberg DH, Pinto Slottow TL, et al. Racial disparities in outcomes following percutaneous coronary intervention with drug-eluting stents. Am J Cardiol. 2009;103(5):653–658. doi: 10.1016/j.amjcard.2008.10.043. [DOI] [PubMed] [Google Scholar]
- 14.Krause JS, Brotherton S, Morrisette D, Newman S, Karakostas T. Does pain interference mediate the relationship of independence in ambulation with depressive symptoms after spinal cord injury? Rehabil Psychol. 2007;52(2):162–169. [Google Scholar]
- 15.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 16.Krause JS, Anson CA. Adjustment after spinal cord injury: relationship to gender and race. Rehabil Psychol. 1997;42(1):31–46. [Google Scholar]
- 17.Krause JS, Broderick LE. Outcomes after spinal cord injury: comparisons as a function of gender and race ethnicity. Arch Phys Med Rehabil. 2004;85:355–362. doi: 10.1016/s0003-9993(03)00615-4. [DOI] [PubMed] [Google Scholar]
- 18.Farmer MM, Ferraro KF. Are racial disparities in health conditional on socioeconomic status? Social Sci Med. 2005;60(1):191–204. doi: 10.1016/j.socscimed.2004.04.026. [DOI] [PubMed] [Google Scholar]
- 19.Krause JS. Dimensions of subjective well-being after spinal cord injury: an empirical analysis by gender and race/ethnicity. Arch Phys Med Rehabil. 1998;79(8):900–909. doi: 10.1016/s0003-9993(98)90085-5. [DOI] [PubMed] [Google Scholar]
- 20.Krause JS, Reed KS. Life satisfaction and self-reported problems after spinal cord injury: measurement of underlying dimensions. Rehabil Psychol. 2009;54(3):343–350. doi: 10.1037/a0016555. [DOI] [PubMed] [Google Scholar]
- 21.Kemp BJ, Adams BM. The Older Adult Health and Mood Questionnaire: a measure of geriatric depressive disorder. J Geriatr Psychiatry Neurol. 1995;8(3):162–167. doi: 10.1177/089198879500800304. [DOI] [PubMed] [Google Scholar]
- 22.Krause JS, Saunders LL, Reed KS, Coker J, Zhai Y, Johnson E. Comparison of the Patient Health Questionnaire and the Older Adult Health and Mood Questionnaire for self-reported depressive symptoms after spinal cord injury. Rehabil Psychol. 2009;54(4):440–448. doi: 10.1037/a0017402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kemp B, Krause J, Adkins R. Depression among African Americans, Latinos, and Caucasians with spinal cord injury: a exploratory study. Rehabil Psychol. 1999;44(3):235–247. [Google Scholar]
- 24.Fuhrer MJ, Rintala DH, Hart KA, Clearman R, Young ME. Depressive symptomatology in persons with spinal cord injury who reside in the community. Arch Phys Med Rehabil. 1993;74(3):255–260. [PubMed] [Google Scholar]
- 25.Krause JS, Zhai Y, Saunders LL, Carter RE. Risk of mortality after spinal cord injury: an 8-year prospective study. Arch Phys Med Rehabil. 2009;90(10):1708–1715. doi: 10.1016/j.apmr.2009.04.020. [DOI] [PMC free article] [PubMed] [Google Scholar]