

Abstract
Purpose
To investigate a new intervention package aimed at increasing expressive word learning by school-age children with autism who have limited expressive vocabularies. This pilot investigation was intended to show proof of concept.
Method
Ten children between the ages of 6-10 years with educational diagnoses of autism and limited expressive vocabularies at the outset of the study participated. A multimodal intervention composed of speech sound practice and AAC was used to teach individualized vocabulary words that were selected based on initial speech sound repertoires and principles of phonotactic probability and neighborhood density. A multiple-probe design was used to evaluate learning outcomes.
Results
Five children showed gains in spoken- word learning across successive word sets (High Responders). Five children did not meet learning criteria (Low Responders). Comparisons of behaviors measured prior to intervention indicated that High Responders had relatively higher skills in receptive language, prelinguistic communication, vocal/verbal imitation, adaptive behavior and consonant productions.
Conclusions
The intervention package holds promise for improving spoken word productions for some children with autism who have limited expressive vocabularies. Further research is needed to better describe who may most benefit from this approach as well as investigate generalized benefits to untaught contexts and targets.
Despite promising results of intensive early interventions, approximately one third to one half of school-age children with autism do not use speech as a primary communication mode (National Research Council, 2001)(National Research Council, 2001). Remaining nonverbal past the age of 5 years has been considered a poor prognostic indicator for future language development (Billstedt, Carina Gillberg, & Gillberg, 2007; Picket, Pullara, O'Grady, & Gordon, 2009). Although there have been reports of individuals older than 5 acquiring speech (e.g., Picket, et. al., 2009), the characteristics of the successful individuals and the interventions employed are not fully understood. The present study is a pilot intervention aimed at teaching speech in combination with Augmentative or Alternative Communication (AAC) to a group of school-age children with autism diagnoses, and to describe characteristics that appeared to be associated with differential outcomes. The target population for this intervention is individuals who have very limited or minimal verbal skills-- for example, less than 20 words or stereotyped phrases produced in functional contexts (c.f., Kasari, Brady, Lord, & Tager-Flusberg, 2013).
Implications of Preschool Intervention Research for School-Aged Children
Most intervention studies aimed at teaching beginning speech and language skills to children with autism have focused on preschool ages or younger (Goods, Ishijima, Chang, & Kasari, 2013; Rogers et al., 2012; Vismara, Comlombi, & Rogers, 2009). The focus on ages 18 months – 5 years is logical given that this is the age range during which the need for direct language intervention becomes apparent. In addition, intensive interventions are implemented early in hopes of preventing further gaps in language development. However, results from early intensive interventions have been mixed. For example, the Early Start Denver Model (ESDM) is a comprehensive intervention that targets language skills as well as other cognitive and adaptive skills in young children with autism. In a randomized clinical trial study of toddlers with Autism Syndrome Disorders (ASDs), Dawson and colleagues (2010) found that ESDM delivered in the home by trained therapists to children between the ages of 18-30 months was significantly better than standard care in improving composite developmental scores on the Mullen scales of early learning (Mullen, 1995) and adaptive-behavior raw scores measured with the Vineland Adaptive behavior scale-2 (Sparrow, Cicchetti, & Balla, 2005). However, in a follow-up study that taught parents how to provide ESDM to children between 14-20 months with ASD, no significant child learning outcomes were reported after 12 weeks of intervention (Rogers et al., 2012). The authors speculated that more gains may have been detected if proximal measures directly linked to target behaviors had been used, in addition to the standardized test outcomes. In addition, post-hoc analyses found that children who didn't receive the Parent-Implemented ESDM received more services from community providers, which may have affected results.
Other studies have focused more specifically on communication outcomes. For example, Goods and colleagues (2013) demonstrated that a pilot intervention based on Joint Attention Symbolic Play Engagement and Regulation (JASPER) (Kasari, Gulsrud, Wong, Kwon, & Locke, 2010) led to gains in play skills and communicative gestures in children between the ages of 3-5 with ASD. However, this limited intervention (24 sessions) did not show changes in word productions.
In each of these studies, results were presented in terms of group comparisons, therefore it is difficult to determine individual responsiveness to the intervention. Warren et al (Warren et al., 2011) completed a meta-analysis with a wide age range of children with Autism Spectrum Disorders (ASD) and concluded that there is a need to better characterize subgroups of children who respond differentially to various intervention approaches. This type of characterization is difficult to complete when only group-level analyses are performed.
Thus, there is growing evidence for interventions directed to children between the ages of 18 months and 5 years. However, many of these strategies may not be appropriate for older, school-age children who remain nonverbal. Several of the approaches mentioned above rely on parent implementation and these approaches may not be feasible when children are attending full-day school programs. In addition, some intervention components, such as play, may need to be modified to be age-- as well as developmentally-- appropriate. Lastly, school age children who have not yet started talking may need more intensive interventions that target speech deficits while also teaching augmentative means of communication.
The Need for a Multimodal Approach
Most intervention research for nonverbal children with autism has focused on either AAC (Ganz et al., 2012; Mirenda & Bopp, 2003; Schlosser & Wendt, 2008) or speech (Rogers et al., 2006), but not both. Brady and colleagues followed the development of 42 children with autism between the ages of 3-6 and noted that children who remained nonverbal were unlikely to receive speech intervention when they reached elementary school (Brady, Thiemann-Bourque, Fleming, & Matthews, 2013). The fact that many children with autism remain nonverbal despite considerable efforts to improve communication suggests the need for an intensive intervention that combines components into one multimodal intervention package. Multimodal refers to the combined use of speech and AAC such as a speech generating device during intervention.
There is good reason that previous efforts have focused primarily on AAC. Speech is likely to remain difficult for some children with autism, whereas they may have more immediate communicative success with AAC. The main goal for AAC interventions is to improve expressive communication using AAC. However, some research studies have reported collateral improvements in speech following AAC. For example, collateral gains in speech were reported for some students following intervention with the Picture Exchange Communication System (PECS)(Bondy & Frost, 1994) (Carr & Felce, 2007; Flippin, Reszka, & Watson, 2010). Note that a wide age range of children have participated in the PECS studies. For example, the ages of the children in the Carr and Felce (2007) were between 3-7 years. Kasari and colleagues (2014) found that an intervention that added an SGD to a joint attention and play intervention resulted in significantly better communication outcomes, including speech outcomes, compared to the same intervention without the SGD. Children in the Kasari et al. (2014) study were between the ages of 5-8 and had minimal expressive verbal skills at the outset of intervention. Results were reported in terms of group differences, however, limiting the ability to determine speech gains by individual children, or skill sets that may be associated with relative differences in communication and speech outcomes.
The PECS studies and the Kasari et al. (2014) study referenced above measured speech outcomes but did not specifically target speech as a part of intervention. Studies directly targeting speech in school-age children with autism and minimal expressive vocabularies are difficult to find. For example, Rogers and colleagues directly taught participants speech skills using the PROMPT method (Rogers et al., 2006), but children were all below the age of 65 months. One study directly taught speech along with SGD use in a multimodal approach to children between the ages of 4-8, but participants had severe speech-sound disorders not associated with autism (King, Hengst, & DeThorne, 2013). Similar research is needed to investigate potential gains made by combining speech and AAC interventions for children with autism.
Multimodal approaches such as that used in the King et al. (2013) study have several potential advantages over approaches that focus on either AAC or speech alone. A combined multi-modal approach is designed to quickly improve communication success through AAC. AAC responses are learned more quickly than speech because they are easier to teach through physical prompts. Learning visually based responses is (typically) facilitated by presenting a fixed array of choices. In addition, participants obtain linguistic input from both AAC and speech models (Binger & Light, 2007; Harris & Reichle, 2004; Sevcik, Romski, Watkins, & Deffebach, 1995). In terms of speech gains, instead of waiting for collateral gains, some participants may benefit from directly teaching speech sounds that comprise targeted vocabulary within a multimodal approach. Speech gains are likely to come more slowly than AAC gains, but practicing the motor movements required for speech-sound productions may improve speech learning while also reinforcing word learning (Vihman, DePaolis, & Keren-Portnoy, 2014).
Teaching Contexts
The current study incorporated teaching contexts and strategies that have been shown to be effective in previous research—speech-sound practice using massed trials, joint book reading, interactive routines incorporating AAC, and receptive vocabulary trials. Massed-trial practice provides multiple opportunities, or trials, in succession, within a short period of time. This strategy can be particularly helpful for initial phases of learning (Heflin & Alberto, 2001). Repeated opportunities to practice and receive feedback for articulatory movements have been found to improve productions (Pomaville & Kladopoulos, 2013). Scripted communication routines are teaching contexts that provide multiple opportunities for communication within motivating activities such as playing a social game, or making and eating a snack, or more advanced thematic play routines (Goldstein, Wickstrom, Hoyson, Jamieson, & Odom, 1988; Kashinath, Woods, & Goldstein, 2006; Rollins, Wambacq, Dowell, Mathews, & Reese, 1998).
An additional teaching context that has been investigated in recent studies is Joint book reading. In joint book reading, an interventionist “reads” from a storybook, providing repeated exposures to targeted vocabulary paired with pictures (referents) (Bellon, Ogletree, & Harn, 2000; Fleury, Miramontez, Hudson, & Schwartz, 2013). Communication opportunities can be created by pausing during joint book reading to allow the child to respond with a specific vocabulary item or re-tell part of the book. Although studies have focused primarily on receptive vocabulary gains associated with joint book reading (Bellon et al., 2000; Hargrave & Sénéchal, 2000; Whitehurst, Falco, Lonigan, & Fischel, 1988), gains in vocabulary production have also been noted (King et al., 2013; Soto & Dukhovny, 2008).
Target Vocabulary Identification
Target vocabulary may be selected based on numerous criteria including frequency of use across contexts (Snodgrass, Stoner, & Angell, 2013), reinforcement value (Charlop-Christy, Carpenter, LeBlanc, & Kellet, 2002) or developmental appropriateness (Solomon-Rice & Soto, 2014). In the current study we took a different approach and selected vocabulary based on principles of phonotactic probability and word neighborhood (Storkel, 2001; Storkel, Maekawa, & Hoover, 2010), and in consideration of each child's speech sound repertoire. According to these principles, words that have higher frequency phonological forms (i.e., high probability) that are phonologically similar to many other words (i.e., high density) are easier to learn because these characteristics facilitate holding the word in working memory (Gathercole, Frankish, Pickering, & Peaker, 1999; Thomson, Richardson, & Goswami, 2005) as well as retrieving the word from long-term memory for production (German & Newman, 2004; Newman & German, 2005). Further, in accordance with these principles, children are more likely to learn and use words comprised of higher frequency phonological forms that are phonologically similar to many other words (e.g., cat) than low frequency forms that are phonologically similar to few other words (e.g., juice).
Research has also shown that children are more likely to learn new words if they contain phonemes that they consistently produce in spontaneous vocalizations (MacRoy-Higgins, Schwartz, Shafer, & Marton, 2013; Schwartz, Leonard, Messick, & Chapman, 1987). For example, if a child produces sounds /s/ and /d/ but not the sounds /l/ or /k/ during their vocalizations, learning to say /sad/ should be easier than learning to say /luck/. As described below under methods, in the current study we identified target vocabulary based on children's existing speech sound repertoires and principles of phonotactic probability and neighborhood density.
Predicting Response to the Intervention
This study was the first attempt to apply our multimodal intervention for word learning. Based on previous research with children with limited expressive vocabularies, we anticipated that not all participants would respond favorably (Odom et al., 2007). In addition to piloting procedures and determining if children learned to produce new words as a result of the intervention, we wanted to identify learner characteristics that may be associated with different outcomes. Numerous variables have been identified as predictive of language outcomes including developmental level, play, and level of joint attention (Kasari, Paparella, Freeman, & Jahromi, 2008; Rogers et al., 2006; Rogers, Hepburn, Stackhouse, & Wehner, 2003; Toth, Munson, N. Meltzoff, & Dawson, 2006); object interest (Sherer & Schreibman, 2005; Vivanti, Dissanayake, Zierhut, & Rogers, 2013); and nonverbal IQ (Thurm, Lord, Lee, & Newschaffer, 2007). Particularly relevant to the current study is research showing strong associations between expressive language and the following variables: imitation, receptive language and early social communication (Bopp & Mirenda, 2011; Poon, Watson, Baranek, & Poe, 2012; Rogers et al., 2006; Rogers et al., 2003). Past studies on predictive relationships have focused more on non-experimental studies demonstrating a longitudinal relationship between predictors and language outcomes. However, there are clinical implications of these studies, including identifying children who may respond better to one type of intervention compared to another.
Purpose of the Current Study
The current study was a pilot investigation aimed at demonstrating proof of concept for a new multi-modal intervention that combines AAC and speech sound practice for children with autism and minimal expressive vocabularies. Our purposes were (1) to determine if participants showed gains in spoken word production, (2) determine if gains were also made in receptive word learning, and (3) supposing that some but not all participants would show gains during intervention, compare the profiles of children who responded favorably to those who responded less favorably in an effort to identify possible predictors of response to this specific multi-modal intervention. As with any pilot study, an overarching goal was to determine if the results are promising enough to follow the research with a larger study.
Methods
Overview
Ten children with autism participated in a multi-modal intervention aimed at teaching new word production, and measuring comprehension of these new words. A single-subject design (multiple-probes across-sets-of-vocabulary words) was used to evaluate the success of the intervention package for each child. Target words were selected individually for each child based on the principles of phonotactic probability and neighborhood density. Specifically, words with high probability and high density were selected for each child. In addition, selected words had to include only sounds that were in the child's phonetic repertoire. Intervention sessions were between 45 min. to an hour each and occurred, on average, 4 days per week. Although the total length of intervention depended on the number of sessions to reach learning criteria, the range of the number of intervention sessions was 17 (for a child who did not learn any words) to 76. After all 10 participants finished participating in the intervention, we evaluated the relative success of individual participants in light of pre-intervention skills in adaptive behavior, receptive language, early communication, and imitation.
Participants
Ten children, nine of whom were boys, participated. The chronological ages of the children were between 7 years 5 months and 11 years 3 months at the time each child began participating in baseline sessions. A brief description of demographic information and communication status at the time of our initial assessment is summarized in Table 1.
Table 1. Participant Information for High and Low Responders.
| Child | Age | Consonants | VABS-C | VABS-M | PPVT-4 | CCS | Imitation-V |
|---|---|---|---|---|---|---|---|
| High Responders | |||||||
| 1 | 8;9 | 12 | 30 (28) | 25 | 23 (24) | – | 8 |
| 2 | 9;8 | 14 | 28 (26) | 18 | 24 (20) | 10 | 8 |
| 3 | 7;7 | 15 | 14 (28) | 20 | 13 (25) | 10 | 6 |
| 4 | 8;2 | 16 | 19 (28) | 30 | 17 (24) | 8.67 | 8 |
| 5 | 6;5 | 13 | – | – | 13 (27) | 10.33 | 8 |
| Low Responders | |||||||
| 6 | 10;11 | 15 | 21 (<20) | 37 | 20 (20) | 10 | 2 |
| 7 | 8;2 | 12 | 27 (31) | 18 | 7 (20) | 8 | 6 |
| 8 | 7;4 | 11 | 24 (33) | 35 | 6 (20) | 6.33 | 5 |
| 9 | 8;11 | 10 | 21 (26) | 33 | 3 (20) | 7.67 | 0 |
| 10 | 6;5 | 11 | 22 (37) | 32 | 4 (20) | 8 | 2 |
Note. VABS-C = Vineland Adaptive Behavior Scales Communication Domain; VABS-M = Vineland Adaptive Behavior Scales Maladaptive Behavior Index- high scores indicate increased maladaptive behaviors; PPVT-4 = Peabody Picture Vocabulary Test–4; CCS = Complexity of Communication Scale; Imitation-V = imitation of vocal/verbal/oral tasks. Age is age at start of data collection. Raw scores are reported; standard scores are presented in parentheses. CCS scores are based on a scale of 1-11 with 11 being highest. Imitation-V scores are number correct out of 8 from Early Steps Imitative Sequences Assessment. Child 4 is female.
All of the children were attending special programs for children with autism in a local school district and had educational diagnoses of autism. Each child had a confirmed diagnosis of autism, according to parent and school reports. Diagnoses were made by professionals not associated with the current research study, based on DSM IV criteria. Parents reported that their children were diagnosed by pediatricians when the children were between 1 and 5 years of age. Two children were diagnosed based on both the CARS and the Autism Diagnostic Observation Schedule (ADOS) (Lord, Rutter, DiLavore, & Risi, 1999) while 1 participant was diagnosed based only on the ADOS. Parents could not recall the instrument used to diagnose the remaining children. Participant 1 also had Down syndrome in addition to autism. Consensus clinical diagnoses such as this have been used to describe participants' autism status in past studies (e.g., Gray, Tonge, & Sweeney, 2008; L. Smith, Barker, Seltzer, Abbeduto, & Greenberg, 2012; Thiemann-Bourque, Brady, & Fleming, 2011), however, we are unable to describe autism severity across participants because we didn't apply a consistent autism measure to all participants.
Our goal was to recruit participants who met the following criteria for minimal expressive vocabulary: less than 20 spoken words produced spontaneously according to (1) teacher report; (2) parent report and (3) a language sample collected during our assessment process. All of the participants met the criteria for teacher report and for productions recorded during our language sample. However, mothers of Participants 1 and 2 indicated on the Vineland Adaptive Behavior Scales (VABS-2) that their child was able to say 50 different words. We included both of these children in the study because teachers indicated the children had vocabularies of less than 20 words, and no words were produced during a 30-minute language sample completed by our research staff. Given that our research design was based on data from individual subjects, with each child acting as their own control, we were able to evaluate children's progress relative to their own baselines without confounding results from other participants.
Measures
Assessment measures
The following measures were used to assess each child prior to baseline.
Vineland Adaptive Behavior Scale-Second Edition (VABS-2) (Sparrow et al., 2005)
We chose to use adaptive behavior instead of a measure of nonverbal cognitive development because we were unable to identify a standardized assessment that was appropriate for the ages and behaviors of our participants (see Kasari, Brady, Lord & Tager-Flusberg, 2013, for a discussion of testing difficulties).The VABS-2 is a measure of adaptive behavior for birth through age 90. It is completed through caregiver and/or teacher interview, covering four broad domains including communication, daily living skills, socialization, and motor skills. The Vineland also includes a maladaptive behavior domain that assesses problem behavior. Each subdomain and maladaptive behavior raw score has a v-scale score that corresponds to a standard score. Within the communication subdomain, questions are directed to assess development of receptive, expressive, and written language skills. The maladaptive behavior index assesses the presence of internalizing and externalizing behaviors. The VABS-2 was normed on a national sample of 3,695 individuals and represents population demographics (i.e., gender, ethnicity, region, and SES) matching the 2001 U.S. Census. The normative sample also included a representative number of individuals with disabilities, including relevant groups of individuals with speech-language impairments and intellectual disabilities. Reported test-retest reliability and content validity measures are high.
Peabody Picture Vocabulary Test-4
The Peabody Picture Vocabulary Test, Fourth Edition (PPVT-4) (Dunn & Dunn, 2007) was administered to all participants as a measure of single word vocabulary comprehension. The PPVT-4 norms are based on a representative sample of 3,540 people aged 2 years 6 months through 90 years and older and matching the U.S. Census for gender, ethnicity, region, and SES. Test-retest reliability coefficients and content validity measures for the PPVT-4 are high. Additionally, the demographic characteristics of the PPVT-4 special-population sample included relevant groups of children with identified language delays and intellectual disabilities. The PPVT-4 is administered by presenting test plates with 4 pictures on a grid. The individual being tested is asked to point to, or otherwise indicate, the picture that corresponds to one of the pictures, named by the tester.
Communication Complexity Scale (CCS)
The CCS is a scale describing levels of early communication development (Brady et al., 2012). Each child participated in a scripted assessment protocol consisting of 12 opportunities to initiate communication acts. Responses to each of the 12 opportunities were assigned a scaled score between 0 and 11 with 1 representing alerting behavior and 11 representing a multi-word utterance. Scores between 0 and 6 are pre-intentional; 7-9 are intentional but nonsymbolic and 10 -11 are symbolic. For each child, the scores of the three opportunities with the highest scores were then averaged to obtain the CCS scores reported in Table 1. Procedures for administering and scoring the CCS are provided in Brady et al. (2012).
Imitation
Imitation was assessed with an instrument developed by Rogers and colleagues (Rogers et al., 2003). This screening instrument contains 8 motor imitation tasks (e.g., clap hands) and 8 vocal/verbal items (e.g., say /ba/). Responses to the vocal/verbal items are presented in Table 1 because these responses are most closely related to our word-learning outcomes and because all of the children were able to imitate the motor imitation tasks.
Dependent measures
The following measures served as the primary measures of word learning.
Expressive probes
Pictures representing each target word were presented to the child, who was asked to name the picture, (e.g., “What's this?). No prompts were provided during these probes. Each word was presented five different times for a total of 25 trials. The order of words was randomized by shuffling the pictures before each session. A correct production was recorded if the child produced at least the initial consonant and vowel for a target word. For example, if the child said /mI/ when the picture of mitt was displayed, this production was scored “correct.” Our rationale for this definition was that deleting the final consonant is a common error in early word production (Dollaghan, 1985) and we were more concerned with the participant's attempts to correctly produce a target word, than their correct articulation of each sound in the word (c.f.,Storkel, 2001). Research assistants were able to reliably determine if the word was correct or not based on this definition.
Receptive probes
Computerized matching-to-sample procedures were used to assess receptive word learning prior to each intervention session. Sessions were presented on a laptop computer, and contained 20 trials, four for each word. For each test trial, a spoken vocabulary word (digitized speech recorded with the Proloquo2go app on an iPad) (Sennott & Bowker, 2009) was presented along with pictures on the touch-sensitive screen. Child 1 and 3 were provided with a three-choice array. Child 6 had a great deal of difficulty with the 3-choice array and we moved to a 2-choice array after 10 sessions. All the remaining children were presented with a 2-choice array. The spoken word was presented every 2 seconds until the child chose one of the pictures by touching it. The software automatically recorded the responses. No feedback was given as to the correctness of the response. The next trial began after a 1-second blank screen. The experimenter offered praise for participating in the task approximately once every 2 minutes on a random schedule.
Procedures
Speech sound identification
The multimodal intervention described below targeted vocabulary selected for each child, based on their extant repertoire of speech sounds. We used a digitized recording device (DLP; LENA™) to help us identify their speech sounds because participants could not participate in typical speech sound production assessment activities, such as a standardized articulation test. Using the DLP, we obtained a recording of 12 hours of spontaneous vocalizations, across 2 days. The recorder weighs approximately 2.5 ounces and fits into the front pocket of children's clothing specially designed to hold the device. It records the child's vocalizations and adult talk near the child within an approximate 6-10 foot radius (Thiemann-Bourque, Warren, & Brady, 2010). Participants received a recording packet at least one day prior to each scheduled recording date. The recording packet contained the DLP, clothing adapted with a pocket for the DLP, and instructional documents. Parents were instructed to turn on the DLP when the child woke up in the morning, insert it into the pocket of the clothing, and dress the child. Thereafter, they were to go about their normal daily activities. During the recording day, the recorder stayed on the child at all times except during baths and sleep periods. If the recorder was not on the child, parents were instructed to place it nearby within 6-feet and continue to record. Parents were asked not to turn off the recorder, but to leave it running continuously until the end of the day, at which time it would shut off automatically. The DLPs were picked up by a research assistant and brought to our research lab.
Audio recording data from the DLP were then uploaded to a computer and automatically processed using LENA software. The acoustical analysis software separates speech-related sounds from environmental sounds, and segments are identified as adult male, adult female, or child. Using the client manager software, child vocalizations were selected. LENA allows the acoustic information to be binned in specified amounts of time. We chose 5-minute increments and then selected the 10, 5- minute intervals with the highest rates of vocalizations recorded over the 12 hours. Next, a trained graduate student listened to these identified segments and transcribed each sound produced. Because the children were, for the most part, nonverbal, these vocalizations most often occurred during non-speech babbling productions. Thus, the DLP and LENA software increased our efficiency by facilitating our identification of periods of high frequency vocalizations that were later transcribed. The total number of different consonants transcribed for each child is listed in Table 1.
Target word selection
A set of target words was identified for each child using an existing set of consonant vowel consonant real words (Storkel, 2013). This existing corpus contained 1,396 real word CVCs. In the corpus, a real word was any CVC that appeared in an adult or a child corpus. For the current study, we pruned these 1,396 real words to only those that appeared in both the adult and child corpora, yielding a pool of 720 real words. Storkel (2013) provides measures of phonotactic probability and neighborhood density for each real word based on a child corpora. Words with high probability and high density sequences appear to be learned more rapidly than low probability and low density sequences, potentially facilitating word learning for the participants in the current study. Thus, these high probability and high-density words were targeted for treatment in the current study.
Phonotactic probability refers to the likelihood of occurrence of a sound sequence and can be represented by two measures: positional segment sum and biphone sum. Positional segment sum is the sum of the positional segment frequencies for each of the three sounds in the CVC. Positional segment frequency is computed by summing the log frequency of all the words in the corpus containing the target sound in the target word position and dividing by the sum of the log frequency of all the words in the corpus containing any sound in the target word position. Biphone sum is computed in the same way except that the focus is on an adjacent pair of sounds (i.e., CV or VC) rather than an individual sound. Neighborhood density refers to the number of words in the corpus that differ from a given word by a single sound substitution, deletion, or addition in any word position. For the 720 real words remaining in the pool, the two measures of phonotactic probability and one measure of neighborhood density were converted to a z score based on the mean and standard deviation of the items in the pool. Items that had negative z scores for any of the measures were removed from the pool. The remaining pool of potential targets consisted of 182 real word CVCs with high probability and high density.
For each individual child, the pool of 182 high probability and high density real words was further reduced based on the child's individual speech sound repertoire. That is, words in the pool that contained sounds that were not in the child's phonetic repertoire were removed from the pool for that specific child. Thus, the remaining pool for each child contained high probability and high density real words composed of sounds that the child produced as part of his/her phonetic repertoire. Thirty target words were identified for each child. The thirty selected words were then placed into six sets of five words each. Words were assigned to sets to provide a mixture of low and high frequency words (Storkel & Hoover, 2010) to ensure that there would be a range of items for each child to learn (e.g., words they may have heard before as well as words that they had never encountered). In addition, an attempt was made to create sets that were phonologically diverse with few words in the set sharing the same initial, medial, or final sound.
Sets were then randomly assigned to a treatment order. In terms of the number of sets actually treated, 4 children received treatment on 4 word sets; 2 children received treatment on 3 word sets; 3 children received treatment on 2 word sets and one child received treatment on only 1 set. This yields 145 treated words across children and sets, although note that some treated words were repeated across children. The appendix shows the treated word sets for each child. Characteristics of the treated words (i.e., word frequency, positional segment sum, biphone sum, and number of neighbors) was submitted to a 10 Participant x 4 Set ANOVA. Results showed no significant difference in word characteristics across participants, sets, or the interaction of participant and set, all F < 1.50, all p > 0.20, all ηp2 < 0.04. Across all participants and sets, the mean log frequency was 2.82 (SD = 0.86, range 1.00-4.69); the mean segment sum was 0.21 (SD = 0.03, range 0.17-0.29); the mean biphone sum was 0.013 (SD = 0.004, range 0.009-0.023); the mean number of neighbors was 20 (SD = 4, range 14-34).
Story creation
Once the set of words was identified for a child, a “story” that could be represented in a book and interactive routine was constructed. For example, based on the words: mitt, cap, bud, ten, and pin, a story was created about a game between two buds, where each child wore a special cap and a mitt, and after the buds scored a ten they earned a special pin.
A picture book depicting the story was created. Each target word was presented in the story 5 different times. Story books were illustrated with clip art and printed words were presented along the bottom of each page. Up to three short sentences appeared on each page. Symbols representing each target word were presented on an iPad equipped with Proloquo2go ™ software. The iPad was made available during an interactive teaching routine, described below under Intervention.
Research Design
In order to determine if participants showed gains in targeted spoken word productions, a multiple probe-across-word-sets design was used (Byiers, Reichle, & Symons, 2012; Kazdin, 1982). Six word sets (each set consisting of five real words) were identified for each child based on their phonetic repertoire and word characteristics (described above). Word sets were taught one at a time. Expressive probes for words in the set currently being taught were administered immediately prior to (i.e., on the same day as) each intervention session. These probes constituted the main outcome measure. In addition, probes for the next set to be taught were presented prior to initiating instruction on that set. Decisions regarding changes in experimental conditions were based on the results of these probes. Once a stable baseline was established for set 1, intervention began on set 1. A baseline was considered stable if at least two successive data points showed consistent (flat) performance, or if the performance declined. However, this rule for stable baselines was violated three times during the study due to experimenter error. Participant 1 only had 1 day of baseline for the first word set, and a rising baseline before the introduction of Set 2. Child 2 also showed a small increase immediately before intervention was introduced on Set 2.
The pass criterion for a word set was > 70% correct word approximations over three consecutive expressive probes. When students met this criterion, and also demonstrated a stable baseline on production probes for the next word set, instruction began on the next word set. If a child did not reach criterion after 14 or more intervention sessions for a word set, intervention was discontinued for that set. The baseline-treatment sequence was completed for 4 sets for Child 1, 2, 3, and 4. Due to lack of progress and time constraints, teaching was discontinued after 3 completed sets for Children 6 and 8, and 2 sets for Children 7 and 9, and 1 set for Child 10. Child 5 moved during the study, and had only two sets.
In addition, beginning with Child 2, we included maintenance probes for previously learned words and periodic probes of words that were never targeted for intervention (“control words”). Maintenance probes were identical to expressive word probes and were administered between 2 and 40 sessions following the final instruction session for a successfully learned word set. The purpose of control words was to provide additional evidence that increases in word learning were specific to the words targeted in intervention. Control words were selected for each child, in the same way as taught words, such that there were no differences in the word characteristics (i.e. phonotactic probability or neighborhood density) for control vs. taught words. Control words were probed in sets of five, in a manner identical to the expressive probes.
Multi-Modal Intervention Sessions
Following the Receptive and Expressive probes (described above under Measures), participants received the multimodal intervention for the word set they were currently learning. Multimodal refers to combined use of speech and a speech generating device during intervention. All components of the intervention were provided in the order listed below, within each intervention session.
Speech sound practice
Although children produced target phonemes during their babbling recorded with the digitized recording device, we wanted to provide additional practice for the sounds in the target words immediately prior to opportunities to use the target vocabulary during joint book reading and the interactive routine. Our theory was that this additional practice might increase the likelihood of correct productions during these activities and facilitate word learning. For example, for the word set mitt, cap, bud, ten and pin, children practiced the sounds /m/, /k/, /t/, /p/, and /n/. The interventionist, a speech-language pathologist, provided models, physical prompts and corrective feedback to assist in sound production. Each sound was practiced 5 times. Positive feedback (e.g., “good job”) was provided for correct sound approximations.
Joint book reading
The interventionist first read the story book that was created for the individualized set of words, emphasizing the target words and pointing to corresponding pictures. Next, she read the book with pauses before each target word (i.e, a cloze procedure as in Petersen, Gillam, Spencer, & Gillam, 2010). For example, one story begins with, “Bob and Joe are best buds!” On the second reading, the interventionist said, “Bob and Joe are best _____” and waited up to 5 seconds for the child to fill in the blank. If the child correctly filled in the blank the interventionist provided verbal praise and moved on to the next sentence in the story. If the child said a wrong word or didn't say any word, the interventionist provided the correct response and moved on to the next sentence in the story.
Interactive routines with iPad
Teaching routines followed a predicable structure with a script for each step in the routine (Kashinath et al., 2006; Snyder-McLean, Solomonson, McLean, & Sack, 1984). Routines also provided opportunities for children to produce target words at least 5 different times. In accordance with the script, the interventionist would first model selecting a target symbol on the iPad equipped with Proloquo2go software. The arrays contained the five target words. After the child participated in the routine several times, the interventionist began pausing before modeling the response in order to allow the child an opportunity to initiate the symbol selection. If the child did not select the symbol after 5 seconds, the interventionist selected it. Each symbol selection was associated with a tangible consequence that also led to the next step in the routine. For example, in a routine about a special game between buds, children needed to request the cap that was worn to play the game. The interventionist and child would walk to the shelf where the caps were located and say “Before we play the game we need to wear our _____.” After the child (or interventionist) selected the cap symbol and/or said “cap”, the child and interventionist put on their caps and went to the location where the game was played.
Receptive matching trials
At the end of each session, additional practice in associating the spoken word with the symbol was provided with another set of receptive matching trials on the laptop computer. These trials were identical to the receptive probe trials described above with the following exception—correct responses received a visual and auditory consequence on the computer and verbal praise by the interventionist.
Reliability
A second observer (a trained undergraduate student) was present for 22% of the baseline and intervention sessions (111 of 500, distributed across participants) to gather inter-observer agreement data for the dependent and independent variables. The second observer recorded responses (correct or incorrect) to the expressive probes. The second observer also recorded responses to the speech sound practice trials. Percent agreement was calculated as the number of agreements / agreements plus disagreements x 100. The percent agreement scores were very high for these variables—97% for the expressive probes and 97% for speech-sound practice. Receptive probe data were recorded directly from the computer and we did not perform reliability checks with the computer.
Procedural reliability for the independent variable was determined by asking the second observer to record whether or not the following intervention components were provided during intervention: 1) did the interventionist pause 5 seconds before each opportunity for an initiated symbol selection during joint book reading and interactive routines? 2) Did the interventionist model the correct response the designated number of times within joint book reading and the interactive routine? The percentage of teaching opportunities for which the interventionist included these components was high -- 99% for pauses, and 87% for modeling.
Results
Results will be presented according to our primary purposes: To determine if participants showed gains in (1) spoken word production and (2) receptive word learning, and (3) to compare profiles of children who responded favorably to those who did not respond as favorably to the intervention. The following section presents results pertaining to word learning outcomes.
Expressive Word Production
Results from the expressive word learning probes are presented in Figures 1-10. Each data point reflects the percent correct out of 25 expressive word production probe trials, collapsed across all 5 words in a set. Child 1 was the first child that participated. It is clear from Figure 1 that correct expressive word productions increased as each new set was introduced to Child 1. Unfortunately, only one baseline session was presented for the first word set and only two baseline sessions were presented for set 4. However, despite these limitations the pattern of responding is strong and consistent. Similarly, the data for child 2, 3 and 4 show increases across 4 different word sets. We were only able to complete two word sets for Child 5 due to time constraints, but the graph for child 5 shows increased production for both word sets compared to baseline. In addition, data from the control words showed that the gains recorded for Participants 1-5 were specific to the words targeted during intervention. Maintenance probes showed that word productions maintained at levels similar to those of the final intervention sessions.
Figure 1.
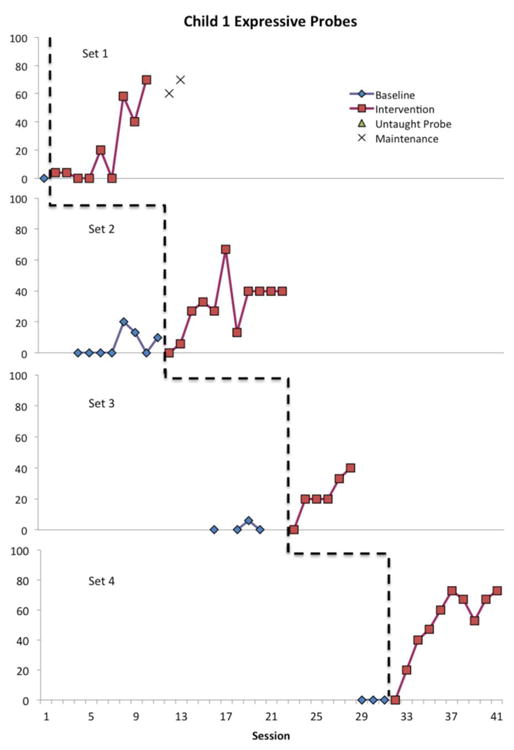
Multiple baselines across word sets for Child 1. Phase line indicates the beginning of intervention for the word set.
Figure 10.
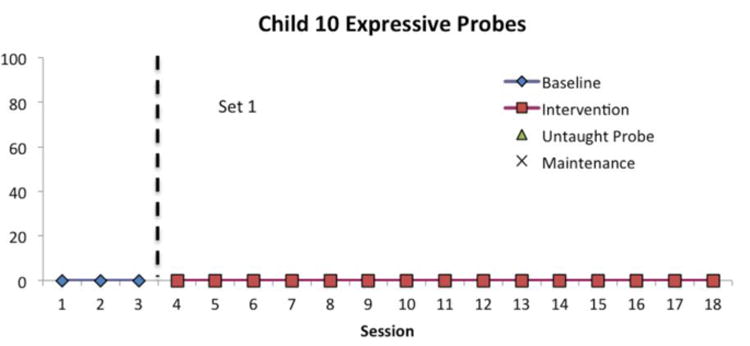
Multiple baselines across word sets for Child 10. Phase line indicates the beginning of intervention for the word set.
Child 6's data is shown in Figure 6. Although child 6 did not meet criterion for any of the word sets, he did show substantial progress over baseline production levels for each of three different word sets. Child 7 learned to say 1/5 words in each of 2 sets. Child 8 increased word production in set 1, although he did not meet criterion. Child 9 and child 10 showed essentially no progress, and hence we discontinued intervention after 2 sets for child 9 and 1 set for child 10.
Figure 6.

Multiple baselines across word sets for Child 6. Phase line indicates the beginning of intervention for the word set.
In addition to the graphic data display, we measured each child's changes from baseline to post treatment. We calculated confidence intervals for the effect sizes (ds) based on the differences between the mean percent correct over the last three days of intervention compared to baseline means. We used the method of Odgaard and Fowler (2010) to compute the noncentrality parameter for the upper and lower limits of the confidence interval based on dependent samples t-test values. These noncentrality parameters were then used to calculate the upper and lower effect size d for the confidence interval. This effect size confidence interval, along with the number of different words produced at a criterion of at least 80% correct over the last three days of intervention and the total number of treatment sessions are presented in Table 2. Effect sizes reflected large to very large effects for participants 1-6.
Table 2. Summary of Expressive Probe Data.
| Child | # Words Learned (Speech Only)/words taught | Total Treatment Sessions | Average Percent Correct Production Probes–Baseline | Average Percent Correct Production Probes–Treatment | 95% CI d |
|---|---|---|---|---|---|
| High Responders | |||||
| 1 | 15/20 | 36 | 3.06 | 52.75 | 2.50 - 5.96 |
| 2 | 17/20 | 62 | 12.83 | 73.25 | 4.03 - 7.88 |
| 3 | 14/20 | 63 | 3.47 | 65.50 | 1.81 – 4.80 |
| 4 | 17/20 | 55 | 1.08 | 79.92 | 3.88 - 9.49 |
| 5 | 7/10 | 18 | 29.57 | 77.67 | 1.28 - 5.58 |
| Low Responders | |||||
| 6 | 4/15 | 66 | 0.00 | 30.67 | 2.32 – 7.30 |
| 7 | 1/10 | 29 | 0.00 | 10.33 | .33 – 3.57 |
| 8 | 3/15 | 60 | 0.00 | 17.00 | .52– 2.97 |
| 9 | 0/10 | 31 | 0.00 | 0.00 | - |
| 10 | 0/5 | 15 | 0.00 | 0.00 | - |
Receptive Word Learning
Although the focus of this study was on expressive word production, we also measured receptive word learning as recorded with the computerized matching software. Words were considered “learned” on the receptive probes if children scored more than 80% correct over three consecutive sessions of the receptive matching probes. Table 3 shows changes for each child's receptive word learning. For the most part, the receptive data were similar to the expressive word data. That is, Participants 1-5 showed positive gains and met receptive criteria for most words learned expressively but Participants 6-10 did not.
Table 3. Summary of Receptive Probe data.
| Child | # Words learned1 | Total Treatment Sessions | Average Percent Correct Receptive Probes – Baseline | Average Percent Correct Receptive Probes – Treatment | 95% CI d |
|---|---|---|---|---|---|
| High responders | |||||
| 1 | 15/20 | 39 | 38.71 | 76.00 | 1.26 – 3.26 |
| 2 | 20/20 | 62 | 59.00 | 94.42 | 2.40 – 5.13 |
| 3 | 20/20 | 62 | 40.68 | 88.83 | 2.46 – 4.94 |
| 4 | 18/20 | 54 | 58.57 | 90.50 | 1.26 – 3.27 |
| 5 | 10/10 | 17 | 57.14 | 64.67 | -.26 – 2.70 |
| Low responders | |||||
| 6 | 4/15 | 66 | 38.60 | 54.89 | .09 – 2.03 |
| 7 | 3/10 | 29 | 58.14 | 41.17 | -2.84 - -.29 |
| 8 | 3/15 | 60 | 56.36 | 52.89 | -1.25 - .53 |
| 9 | 0/10 | 31 | 50.00 | 56.50 | -.52 – 1.82 |
| 10 | 0/5 | 11 | 55.67 | 46.67 | -2.47 - .91 |
Note: Children 1 and 3 had a three-choice array; Child 6 had three choices in baseline for the first set, and a three-choice array thereafter; the remaining children had a two-choice array throughout the study.
Words learned indicates the number of words meeting the 80% correct criterion on receptive probes.
Profiles of High and Low Responders
Participants 1-5 responded to the intervention with significant increases in expressive production of targeted words. We refer to these children as “High Responders.” As shown in Tables 2 and 3, Effect sizes for the “High Responders” were large in the full range of the confidence interval for both receptive and expressive probe data with the exception of Child 5 whose receptive effect size included zero in the confidence interval. Children in the Low Responders group did not meet expressive word learning criteria, although 3 children did show gains in producing some words. Effect size values in the Low Responders group contained zero or were small/moderate within the confidence interval. Child 6 was an exception to this with large effect sizes contained in the full 95% confidence interval for expressive language.
We reviewed the scores for each participant that were collected pre-baseline (see Table 1) to determine if there were differences in scores for children who were High vs. Low Responders to our intervention package. The children who responded best to our intervention (children 1-5) had higher scores on the PPVT-4, indicating better receptive vocabularies. In addition, they also had higher scores on the CCS with High Responders averaging 9.75 and Low Responders averaging 8.0, indicating more advanced prelinguistic communication in the high Responder group. This higher CCS score reflects more frequent use of communicative gestures and/or vocalizations during the scripted interaction. The overall imitation scores were not obviously different across children, a finding similar to Rogers and colleagues (2012). However, when we looked only at imitation for oral, vocal and verbal skills, we saw higher scores for the High-Responders with a mean of 7.6 while the Low Responders had a mean of 3.0. We also reviewed the number of different consonants recorded with the LENA recording system prior to intervention as a possible differentiating variable between high and low responders. The mean number of consonants was 14.0 for High Responders and 11.8 for Low Responders suggesting a possible relationship. Thus, high-responding children had relatively better scores on receptive vocabulary, prelinguistic communication, vocal/verbal imitation and consonant repertoires. However, these observations are merely suggestive due to small sample sizes.
Discussion
Results of this pilot investigation indicated that children with limited expressive vocabularies learned to say new words with a multimodal intervention package that combined AAC and speech sound practice for individually determined sets of words. Maintenance and control probe data indicated that the responses maintained and were specific to the targeted vocabulary for the four children for whom these data were collected. Given that all the participants had limited expressive vocabularies at the start of intervention, and were between the ages of 6 and 11 years, the gains made by the 5 High Responders are impressive. Currently, the predominant clinical practice for children with this profile is to abandon efforts to increase speech production. Moreover, there is little in the research literature to contraindicate this practice. Our results indicate that an intervention that focuses on speech plus AAC can have positive outcomes on speech for school-age children with autism and limited expressive vocabularies. Given that this was a relatively short-term intervention, and the duration of intervention sessions was only 45 minutes per day, these results are extremely promising.
To our knowledge, this study was also the first reported attempt to apply principles of phonotactic probability and neighborhood density to a word learning intervention for children with intellectual disabilities and limited expressive vocabularies. The vocabulary targeted by this approach may have been easier to learn to produce than other vocabularies, because of these word-learning principles. The approach we used may facilitate initial word learning that can help build a foundation for later functional spoken vocabulary.
Effect sizes for the high responders in our study were for the most part in the high to very high range and compared favorably to other interventions measuring gains in beginning word use by younger children with autism. For example, Rogers and colleagues reported a d of .84 for vocabulary comprehension and a d of .57 for vocabulary production for children who participated in their ESDM intervention. Kasari et al. (2014), reported effect sizes between .21 and .62 across different expressive communication measures for their group who experienced a combined JASPER and SGD treatment, compared to a treatment group of only JASPER (without the SGD). Thus, our multimodal intervention that includes intensive speech sound practice does seem to be effective for at least some children past the preschool age range. The specific emphasis on speech sound production differs from most interventions that have been used with preschool age children (e.g. Dawson et al., 2010; Goods et al., 2013). It is not known if the additional speech sound practice was a key ingredient of the intervention because all of the children experienced this component (and all of the components). Future research is needed to examine how different components, including speech sound practice contribute to overall outcomes.
Our results were not as positive for all participants, however. Five of the 10 participating children failed to meet our production criterion indicating that they failed to meet our learning criterion for any word sets (Low Responders). However, it is worth noting that three of these children did show increases in word productions over baseline levels, as indicated in Figures 6-8 and Table 2. Perhaps longer or more intense interventions would have improved responding by these three participants, and modifications such as these would be appropriate for clinical applications (outside of a research study). In addition, further analysis could focus on comparing the specific words that children learned to those they did not learn in an effort to identify commonalities in terms of the phonemes included and/or motivations associated with particular vocabulary.
Figure 8.
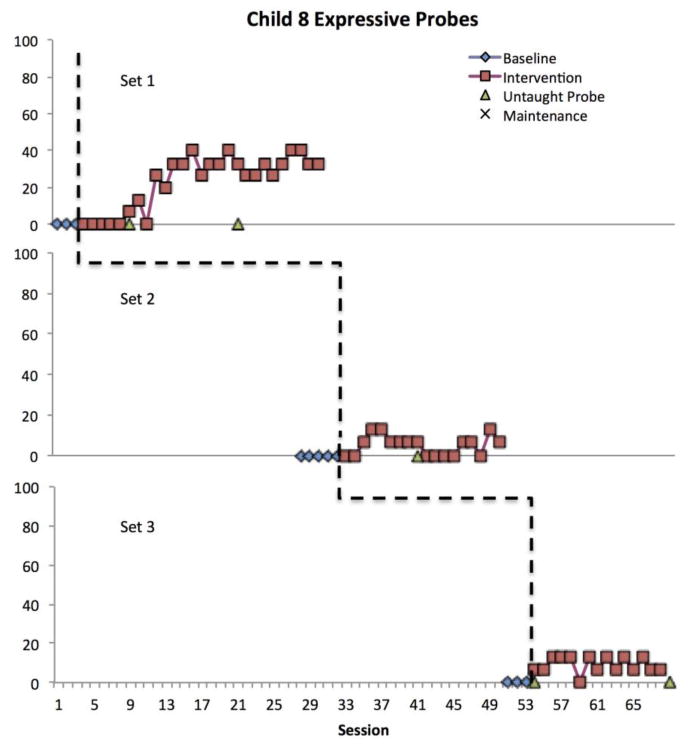
Multiple baselines across word sets for Child 8. Phase line indicates the beginning of intervention for the word set.
Perhaps the most important aspect of the current study is that we provided results for both children who did and children who did not respond well to our intervention, along with data about some important characteristics that appeared associated with differential outcomes. This type of information is critical for designing future research studies, and ultimately for clinical decision making (Yoder & Compton, 2004). Children with autism or autism symptoms and minimal verbal repertoires present clinicians with various skill repertoires. One goal of intervention research is to identify relative strengths and weaknesses in areas that may facilitate learning with a particular intervention approach.
We retrospectively compared High Responders' and Low Responders' initial skills in areas that have been linked to verbal outcomes (receptive language, prelinguistic communication, imitation, speech sound production and adaptive behavior) because the focus of the current study was on spoken word productions. Our review of differences in entry-level skills of High vs Low responders suggested the intervention may be most helpful for children who have at least some measureable receptive vocabulary, frequent use of intentional communication acts, imitate vocal/verbal sounds and oral movements, and have larger consonant repertoires (note we did not count or compare the size of vowel repertoires in this study). As discussed in the Introduction of this study, each of these skills has been linked to language learning outcomes and hence it is not surprising that they were also associated with different outcomes in our study. It is also noteworthy that Participants 1, 2, 3 and 5 had some correct responses (1-2 words) during baselines, which was not the case for Low Responders. Therefore some initial evidence of correct speech production appears to be predictive of early progress in a multimodal intervention. However, these observations are based on very small sample sizes and replication with larger samples who vary across these skills are needed to make more robust determinations of characteristics of High vs. low Responders. It may be useful to examine additional areas, such as play skills, that have been linked to communication outcomes in future studies.
Identifying children who respond best to different types of interventions could help maximize positive outcomes by selecting appropriate targets based on individual needs and entry behaviors. For example, in the current study, children who we ultimately described as Low Responders to our intervention package may have made more communication gains in an intervention that emphasized AAC along with prelinguistic social communication, without specific focus on speech sound production. In addition, it may prove beneficial to directly teach skills that are associated with better outcomes (e.g., receptive language, imitation) as part of a comprehensive communication intervention. However, speech gains made by our High Responding children provide evidence for continued speech-based interventions for some children with autism and limited expressive vocabularies.
The current study used a single subject research design which allowed review of the effectiveness across each child and evaluation of how individual skill sets related to different outcomes. This was very important because, if all the children's data had been combined, as in a between-groups design, the differences in relative effectiveness across children would have been lost. Future research that further delineates characteristics of responders will increase the generality to participants who are similar in terms of the dimensions associated with positive outcomes. However, as in all single subject design studies, the outcomes are only generalizable to participants of a given study or individuals highly similar to those participants. The detailed information about individual skills provides a basis for comparison that clinicians may refer to when evaluating the potential of a given intervention for use with their clients.
Limitations to the current study
Children in our study were taught a very limited set of vocabulary in contrived teaching environments, without any focus on generalized use of targeted vocabulary across contexts. While this is a limitation in terms of evaluating the clinical effectiveness of intervention outcomes, we propose that our findings be viewed in terms of “proof of concept” for our unique multimodal intervention package (T. Smith et al., 2007). Based on our results, further research is warranted that would include measures of generalization to functional communication targets, including generalized communication improvements to non-target vocabulary across communication modes. For experimental-control purposes, it was important in the current study to show that learning was limited to targeted vocabulary. A desirable outcome for future studies would be generalization to non-targeted words in addition to learning the words directly taught in intervention.
Another area for future research is determining the value of individual components of the intervention package. For example, one novel approach we used was to select vocabulary based on both a child's current speech sound repertoire and principles of phonotactic probability. This was based on our hypothesis that children would learn speech more readily under these conditions. However, we did not directly test this hypothesis and future investigations may want to compare word learning using different criteria for initial vocabulary selection. In the current study we only measured speech sound productions during baseline, and future investigations may also re-measure speech sound productions after intervention to determine if there is a change in this variable.
The lack of a consistent autism measure was another limitation to the current study. We relied on diagnoses performed by outside agencies using a variety of instruments. Therefore, we were not able to quantify the severity of autism in our participants. In future research it will be important to administer an assessment that could reflect autism severity across all participants, in order to determine the possible role of severity in predicting differential outcomes. Finally, the experimenter errors described under the methods section were limitations in the current study. Specifically, experimenter error resulted in baseline errors for one word set each for Child 1 and Child 2.
Conclusions
Results from this pilot investigation indicate that our multimodal intervention leads to increased spoken word productions for some school-age children with minimal verbal skills who attend educational programs for children with autism. Future studies are needed to more accurately describe the variables that are associated with positive outcomes, target use in naturalistic contexts and determine the relative contributions of different intervention components. Ultimately, results from this line of research may lead to increased emphasis on speech intervention in addition to AAC instruction for school-age children with autism and minimal verbal skills. Such a combined approach would seem optimal for promoting effective communication with the widest possible set of communication partners and across multiple environments.
Figure 2.
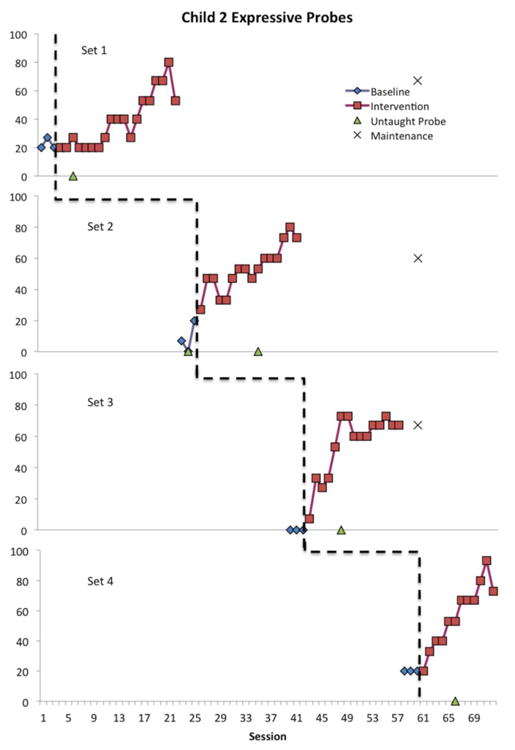
Multiple baselines across word sets for Child 2. Phase line indicates the beginning of intervention for the word set.
Figure 3.
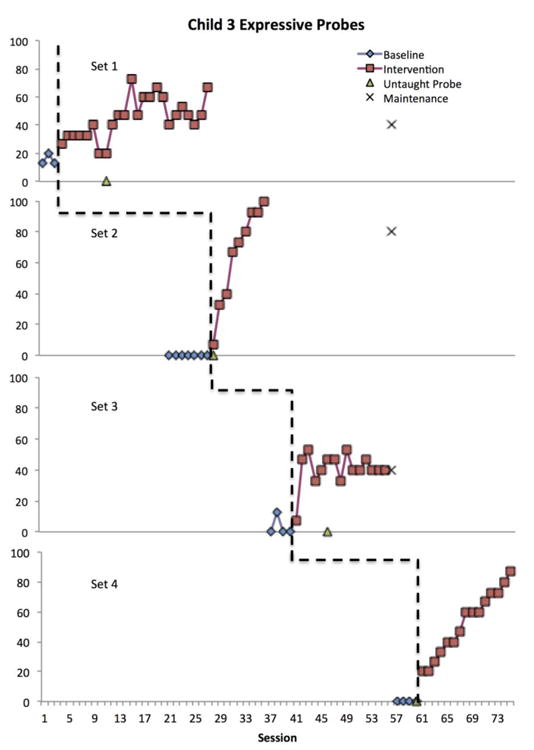
Multiple baselines across word sets for Child 3. Phase line indicates the beginning of intervention for the word set.
Figure 4.
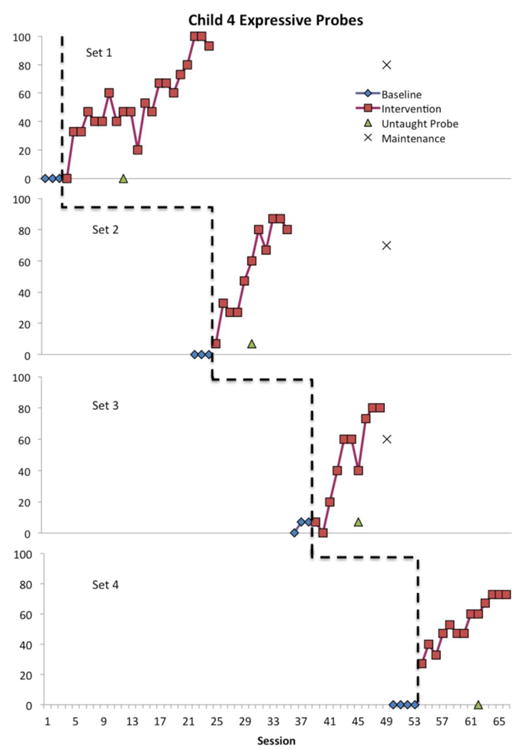
Multiple baselines across word sets for Child 4. Phase line indicates the beginning of intervention for the word set.
Figure 5.
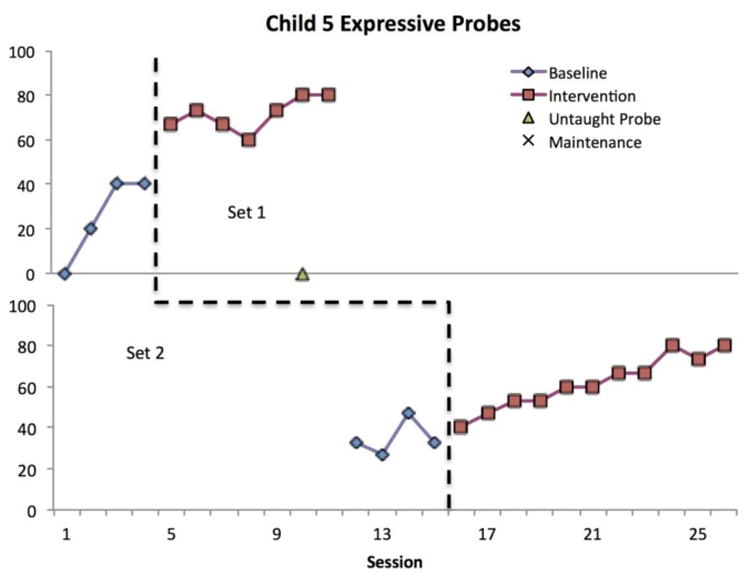
Multiple baselines across word sets for Child 5. Phase line indicates the beginning of intervention for the word set.
Figure 7.
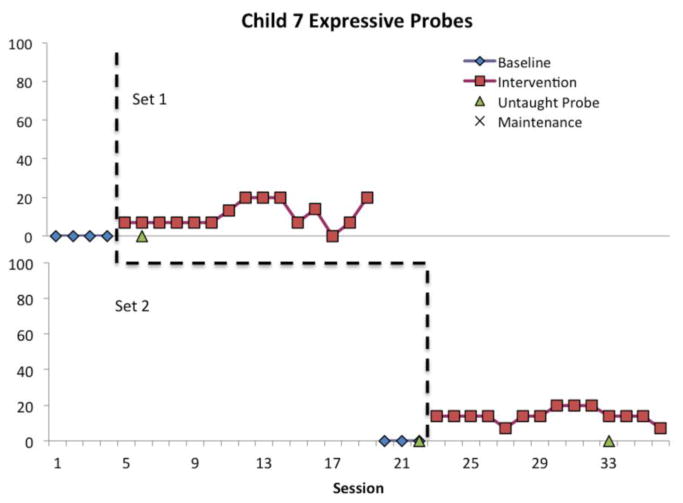
Multiple baselines across word sets for Child 7. Phase line indicates the beginning of intervention for the word set.
Figure 9.
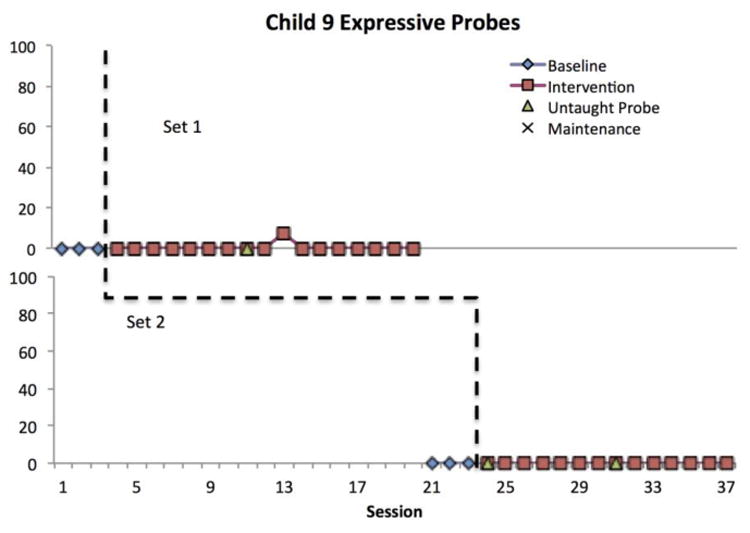
Multiple baselines across word sets for Child 9. Phase line indicates the beginning of intervention for the word set.
Acknowledgments
This research was supported by a Pilot Research grant from Autism Speaks and NIH grant NICHD P30 HD002528; NICHD 0070511; and T32 HD057844
Appendix A. Word lists for each participant
| Child 1 |
| Set 1: mitt, cap, bud, ten, pin |
| Set 2: pot, men, beat, pick, ton |
| Set 3: dead, pen, buck, met, bit |
| Set 4: hot, kick, mitt, tan, hid |
| Child 2 |
| Set 1: bag, head, mane, tick, sit |
| Set 2: bud, wet, dock, sing, fin |
| Set 3: hot, bun, kick, pad, seat |
| Set 4: ham, pine, mad, sick, cot |
| Child 3 |
| Set 1: bat, head, mane, tick, sing |
| Set 2: bun, mad, seat, wine, kick |
| Set 3: win, dad, king, met, coke |
| Set 4: bud, wet, cat, dock, tan |
| Child 4 |
| Set 1: coke, win, dad, bus, met |
| Set 2: hole, bun, kick, pad, seat |
| Set 3: pal, wet, dock, sing, fun |
| Set 4: bag, head, mane, sit, tick |
| Child 5 |
| Set 1: bag, head, mane, tick, sit |
| Set 2: pal, wet, dock, sing, fun |
| Child 6 |
| Set 1: bat, done, head, tick, mane |
| Set 2: buck, kit, had, ten, man |
| Set 3: back, wet, coat, dot, tin |
| Child 7 |
| Set 1: pan, mitt, bud, sing, nine |
| Set 2: bang, dad, sun, met. Pass |
| Child 8 |
| Set1: pen, dad, king, met, coke |
| Set 2: bat, fun, tick, mane, said |
| Set 3: pass, sing, tin, coat, fan |
| Child 9 |
| Set 1: bag, done, mane, gnat, head |
| Set 2: hot, mitt, bang, dad, win |
| Child 10 |
| Set 1: bang, dad, cop, pick, win |
Contributor Information
Nancy C. Brady, Department of Speech Language Hearing Sciences and Disorders, University of Kansas
Holly L. Storkel, Department of Speech Language Hearing Sciences and Disorders, University of Kansas
Paige Bushnell, Department of Speech Language Hearing Sciences and Disorders, University of Kansas.
R. Michael Barker, Schiefelbusch Institute of Lifespan Studies, University of Kansas.
Kate Saunders, Schiefelbusch Institute of Lifespan Studies, University of Kansas.
Debby Daniels, Department of Hearing and Speech, University of Kansas Medical Center.
Kandace Fleming, Schiefelbusch Institute of Lifespan Studies, University of Kansas.
References
- Bellon ML, Ogletree BT, Harn WE. Repeated Storybook Reading as a Language Intervention for Children with Autism. Focus on Autism & Other Developmental Disabilities. 2000;15(1):52. [Google Scholar]
- Billstedt E, Carina Gillberg I, Gillberg C. Autism in adults: symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. Journal of Child Psychology and Psychiatry. 2007;48(11):1102–1110. doi: 10.1111/j.1469-7610.2007.01774.x. [DOI] [PubMed] [Google Scholar]
- Binger C, Light J. The effect of aided AAC modeling on the expression of multi-symbol messages by preschoolers who use AAC. Augmentative and Alternative Communication. 2007;23(1):30–43. doi: 10.1080/07434610600807470. [DOI] [PubMed] [Google Scholar]
- Bondy AS, Frost LA. The picture exchange communication system. Focus on Autistic Behavior. 1994;9:1–19. [Google Scholar]
- Bopp KD, Mirenda P. Prelinguistic predictors of language development in children with autism spectrum disorders over four–five years. Journal of Child Language. 2011;38(03):485–503. doi: 10.1017/S0305000910000140. [DOI] [PubMed] [Google Scholar]
- Brady N, Fleming K, Thiemann-Bourque K, Olswang L, Dowden P, Saunders M, Marquis J. Development of the Communication Complexity Scale. American Journal of Speech-Language Pathology. 2012;21(1):16–28. doi: 10.1044/1058-0360(2011/10-0099). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brady N, Thiemann-Bourque K, Fleming K, Matthews K. Predicting language outcomes for children learning AAC: Child and environmental factors. Journal of Speech, Language & Hearing Research. 2013;56(5):1595–1612. doi: 10.1044/1092-4388(2013/12-0102). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byiers BJ, Reichle J, Symons FJ. Single-Subject Experimental Design for Evidence-Based Practice. American Journal of Speech-Language Pathology. 2012;21(4):397–414. doi: 10.1044/1058-0360(2012/11-0036). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr D, Felce J. Brief Report: Increase in Production of Spoken Words in Some Children with Autism after PECS Teaching to Phase III. Journal of Autism and Developmental Disorders. 2007;37(4):780–787. doi: 10.1007/s10803-006-0204-0. [DOI] [PubMed] [Google Scholar]
- Center NA. National Standards Report. Randolph, MA: National Autism Center; 2009. [Google Scholar]
- Charlop-Christy M, Carpenter M, LeBlanc L, Kellet K. Using the picture exchange communication system (PECS) with children with autism: Assessment of PECS acquisition, speech, social-communicative behavior and problem behavior. Journal of Applied Behavior Analysis. 2002;35(3):213–231. doi: 10.1901/jaba.2002.35-213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dawson G, Rogers S, Munson J, Smith M, Winter J, Greenson J, Varley J. Randomized, controlled trial of an intervention for toddlers with autism: The early start Denver model. Pediatrics. 2010;125(1) doi: 10.1542/peds.2009-0958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dollaghan C. Child meets word: “Fast mapping in preschool children”. Journal of Speech and Hearing Research. 1985;28:449–454. [PubMed] [Google Scholar]
- Dunn L, Dunn D. The Peabody Picture vocabulary Test-Fourth Edition (PPVT-4) San Antonio, TX: Psychological Corporation; 2007. [Google Scholar]
- Fleury VP, Miramontez SH, Hudson RF, Schwartz IS. Promoting active participation in book reading for preschoolers with Autism Spectrum Disorder: A preliminary study. Child Language Teaching and Therapy. 2013 doi: 10.1177/0265659013514069. [DOI] [Google Scholar]
- Flippin M, Reszka S, Watson L. Effectiveness of the Picture Exchange communication System (PECS) on Communication & Speech for Children with Autism Spectrum Disorders: A Metanalysis. American Journal of Speech-Language Pathology. 2010;19:178–195. doi: 10.1044/1058-0360(2010/09-0022). [DOI] [PubMed] [Google Scholar]
- Ganz JB, Earles-Vollrath TL, Heath AK, Parker RI, Rispoli MJ, Duran JB. A meta-analysis of single case research studies on aided augmentative and alternative communication systems with individuals with autism spectrum disorders. Journal of Autism & Developmental Disorders. 2012;42:60–74. doi: 10.1007/s10803-011-1212-2. [DOI] [PubMed] [Google Scholar]
- Gathercole SE, Frankish CR, Pickering SJ, Peaker S. Phonotactic influences of short-term memory. Journal of Experimental Psychology. 1999;25(1):84–95. doi: 10.1037//0278-7393.25.1.84. [DOI] [PubMed] [Google Scholar]
- German DJ, Newman RS. The Impact of Lexical Factors on Children's Word-Finding Errors. Journal of Speech, Language & Hearing Research. 2004;47(3):624–636. doi: 10.1044/1092-4388(2004/048). [DOI] [PubMed] [Google Scholar]
- Goldstein H, Wickstrom S, Hoyson M, Jamieson B, Odom SL. Effects of sociodramatic script training on social and communicative interaction. Education and Treatment of Children. 1988;11:97–117. [Google Scholar]
- Goods K, Ishijima E, Chang YC, Kasari C. Preschool Based JASPER Intervention in Minimally Verbal Children with Autism: Pilot RCT. Journal of Autism and Developmental Disorders. 2013;43(5):1050–1056. doi: 10.1007/s10803-012-1644-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray KM, Tonge BJ, Sweeney DJ. Using the Autism Diagnostic Interview-Revised and the Autism Diagnostic Observation Schedule with young children with developmental delay: Evaluating diagnostic validity. Journal of Autism and Developmental Disorders. 2008;38(4):657–667. doi: 10.1007/s10803-007-0432-y. doi:http://dx.doi.org/10.1007/s10803-007-0432-y. [DOI] [PubMed] [Google Scholar]
- Hargrave AC, Sénéchal M. A book reading intervention with preschool children who have limited vocabularies: the benefits of regular reading and dialogic reading. Early Childhood Research Quarterly. 2000;15(1):75–90. doi:http://dx.doi.org/10.1016/S0885-2006(99)00038-1. [Google Scholar]
- Harris M, Reichle J. The impact of aided language stimulation on symbol comprehension and production in learners with moderate cognitive disabilities. American Journal of Speech-Language Pathology. 2004;13(2):155–167. doi: 10.1044/1058-0360(2004/016). [DOI] [PubMed] [Google Scholar]
- Heflin LJ, Alberto PA. Establishing a Behavioral Context for Learning for Students with Autism. Focus on Autism & Other Developmental Disabilities. 2001;16(2):93. [Google Scholar]
- Kasari C, Brady N, Lord C, Tager-Flusberg H. Assessing the minimally verbal school-aged child with autism spectrum disorder. Autism Research. 2013;6(6):479–493. doi: 10.1002/aur.1334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Gulsrud A, Wong C, Kwon S, Locke J. Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism & Developmental Disorders. 2010;40(9):1045–1056. doi: 10.1007/s10803-010-0955-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Kaiser A, Goods K, Nietfeld J, Mathy P, Landa R, Almirall D. Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry. 2014;53(6):635–646. doi: 10.1016/j.jaac.2014.01.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Paparella T, Freeman S, Jahromi L. Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology. 2008;76(1):125–137. doi: 10.1037/0022-006X.76.1.125. [DOI] [PubMed] [Google Scholar]
- Kashinath S, Woods J, Goldstein H. Enhancing generalized teaching strategy use in daily routines by parents of children with autism. Journal of Speech, Language and Hearing Research. 2006;49(3):466–485. doi: 10.1044/1092-4388(2006/036). [DOI] [PubMed] [Google Scholar]
- Kazdin AE. Single-Case Research Designs. New York: Oxford University Press; 1982. [Google Scholar]
- King A, Hengst J, DeThorne L. Severe speech sound disorders: An integrated multimodal intervention. Language Speech and hearing Services in the Schools. 2013;44:195–210. doi: 10.1044/0161-1461(2012/12-0023). [DOI] [PubMed] [Google Scholar]
- Lord C, Rutter M, DiLavore PC, Risi S. Autism Diagnostic Observation Schedule-WPS Edition (ADOS-WPS) Los Angeles: Western Psychological Services; 1999. [Google Scholar]
- MacRoy-Higgins M, Schwartz RG, Shafer VL, Marton K. Influence of phonotactic probability/neighbourhood density on lexical learning in late talkers. International Journal of Language & Communication Disorders. 2013;48(2):188–199. doi: 10.1111/j.1460-6984.2012.00198.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mirenda P, Bopp K. “Playing the game”: Strategic competence in AAC. In: Light J, Beukelman DR, Reichle J, editors. Communicative competence for individuals who use AAC. 2003. pp. 401–437. [Google Scholar]
- Mullen E. Mullen scales of early learning: AGS edition. Circle Pines, MN: AGS; 1995. [Google Scholar]
- National Research Council. Educating children with autism: Committee on educational interventions for children with autism Division of behavioral and social sciences and education. Washington, DC: National Academy Press; 2001. [Google Scholar]
- Newman RS, German DJ. Life Span Effects of Lexical Factors on Oral Naming. Language & Speech. 2005;48(2):123–156. doi: 10.1177/00238309050480020101. [DOI] [PubMed] [Google Scholar]
- Odgaard EC, Fowler RL. Confidence intervals for effect sizes: Compliance and clinical significance in the Journal of Consulting and Clinical Psychology. Journal of Consulting and Clinical Psychology. 2010;78(3):287–297. doi: 10.1037/a0019294. doi:http://dx.doi.org/10.1037/a0019294. [DOI] [PubMed] [Google Scholar]
- Odom SL, Rogers S, McDougle CJ, Hume K, McGee G, Odom S, Blacher J. Early intervention for children with autism spectrum disorder. Handbook of developmental disabilities. 2007:199–223. [Google Scholar]
- Petersen DB, Gillam SL, Spencer T, Gillam RB. The Effects of Literate Narrative Intervention on Children With Neurologically Based Language Impairments: An Early Stage Study. Journal of Speech, Language & Hearing Research. 2010;53(4):961–981. doi: 10.1044/1092-4388(2009/09-0001). [DOI] [PubMed] [Google Scholar]
- Picket E, Pullara O, O'Grady J, Gordon B. Speech acquisition in older nonverbal individuals with autism. Cognitive and Behavioral Neurology. 2009;22(1):1–21. doi: 10.1097/WNN.0b013e318190d185. [DOI] [PubMed] [Google Scholar]
- Pomaville FM, Kladopoulos CN. The Effects of Behavioral Speech Therapy on Speech Sound Production With Adults Who Have Cochlear Implants. Journal of Speech, Language, and Hearing Research. 2013;56(2):531–541. doi: 10.1044/1092-4388(2012/12-0017). [DOI] [PubMed] [Google Scholar]
- Poon K, Watson L, Baranek G, Poe M. To What Extent Do Joint Attention, Imitation, and Object Play Behaviors in Infancy Predict Later Communication and Intellectual Functioning in ASD? Journal of Autism and Developmental Disorders. 2012;42(6):1064–1074. doi: 10.1007/s10803-011-1349-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers S, Estes A, Lord C, Vismara L, Winter J, Fitzpatrick A, Dawson G. Effects of a Brief Early Start Denver Model (ESDM)- based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry. 2012;5(10):1052–1065. doi: 10.1016/j.jaac.2012.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers S, Hayden D, Hepburn S, Charlifue-Smith R, Hall T, Hayes A. Teaching young nonverbal children with autism useful speech: A pilot studt of the Denver model and PROMPT interventions. Journal of Autism and Developmental Disorders. 2006;36:1007–1024. doi: 10.1007/s10803-006-0142-x. [DOI] [PubMed] [Google Scholar]
- Rogers S, Hepburn S, Stackhouse T, Wehner E. Imitation performance in toddlers with autism and those with other developmental disorders. Journal of Child Psychology and Psychiatry. 2003;44:763–781. doi: 10.1111/1469-7610.00162. [DOI] [PubMed] [Google Scholar]
- Rollins Pr, Wambacq I, Dowell D, Mathews L, Reese PB. An intervention technique for children with autistic spectrum disorder: Joint attentional routines. Journal of Communiction Disorders. 1998;31:181–189. doi: 10.1016/s0021-9924(97)00088-9. [DOI] [PubMed] [Google Scholar]
- Schlosser R, Wendt O. Effects of augmentative and alternative communication intervention on speech production in children with autism: A systematic review. American Journal of Speech Language Pathology. 2008;17:212–230. doi: 10.1044/1058-0360(2008/021). [DOI] [PubMed] [Google Scholar]
- Schwartz RG, Leonard LB, Messick C, Chapman K. The acquisition of object names in children with specific language impairment. Action context and word extension. 1987;8:233–244. [Google Scholar]
- Sennott S, Bowker A. Autsim, AAC, and Proloquo2Go. SIG 12 Perspectives on Augmentative and Alternative Communication. 2009;18:137–145. [Google Scholar]
- Sevcik R, Romski M, Watkins R, Deffebach K. Adult partner-augmented communication input to youth with mental retardation using the system for augmenting language. Journal of Speech, Language and Hearing Research. 1995;38:902–912. doi: 10.1044/jshr.3804.902. [DOI] [PubMed] [Google Scholar]
- Sherer MR, Schreibman L. Individual Behavioral Profiles and Predictors of Treatment Effectiveness for Children With Autism. Journal of Consulting and Clinical Psychology. 2005;73(3):525–538. doi: 10.1037/0022-006X.73.3.525. doi:http://dx.doi.org/10.1037/0022-006X.73.3.525. [DOI] [PubMed] [Google Scholar]
- Smith L, Barker ET, Seltzer MM, Abbeduto L, Greenberg JS. Behavioral phenotype of fragile X syndrome in adolescence and adulthood. American Journal on Intellectual and Developmental Disabilities. 2012;117:1–17. doi: 10.1352/1944-7558-117.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith T, Scahill L, Dawson G, Guthrie D, Lord C, Odom S, Wagner A. Designing Research Studies on Psychosocial Interventions in Autism. Journal of Autism and Developmental Disorders. 2007;37(2):354–366. doi: 10.1007/s10803-006-0173-3. [DOI] [PubMed] [Google Scholar]
- Snodgrass MR, Stoner JB, Angell ME. Teaching Conceptually Referenced Core Vocabulary for Initial Augmentative and Alternative Communication. Augmentative and Alternative Communication. 2013;29(4):322–333. doi: 10.3109/07434618.2013.848932. [DOI] [PubMed] [Google Scholar]
- Snyder-McLean LK, Solomonson B, McLean J, Sack S. Structuring joint action routines: A strategy for facilitating commuication and language development in the classroom. Seminars in Speech and Language. 1984;5(3):213–228. [Google Scholar]
- Solomon-Rice PL, Soto G. Facilitating Vocabulary in Toddlers Using AAC: A Preliminary Study Comparing Focused Stimulation and Augmented Input. Communication Disorders Quarterly. 2014 doi: 10.1177/1525740114522856. [DOI] [Google Scholar]
- Soto G, Dukhovny E. The Effect of Shared Book Reading on the Acquisition of Expressive Vocabulary of a 7 Year Old Who Uses AAC. Seminars in Speech and Language. 2008;29(2):133–145. doi: 10.1055/s-2008-1079127. [DOI] [PubMed] [Google Scholar]
- Sparrow S, Cicchetti D, Balla D. Vineland-II: Vineland adaptive bheavior scales, Second Edition. Minneapolis: Pearson; 2005. [Google Scholar]
- Storkel HL. Learning New Words: Phonotactic Probability in Language Development. Journal of Speech Language and Hearing Research. 2001;44:1321–1337. doi: 10.1044/1092-4388(2001/103). [DOI] [PubMed] [Google Scholar]
- Storkel HL. A corpus of consonant–vowel–consonant real words and nonwords: Comparison of phonotactic probability, neighborhood density, and consonant age of acquisition. Behavior Research Methods. 2013;45(4):1159–1167. doi: 10.3758/s13428-012-0309-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Storkel HL, Hoover JR. An on-line calculator to compute phonotactic probability and neighborhood density based on child corpora of spoken American English. Behavior Research Methods. 2010;42(2):497–506. doi: 10.3758/BRM.42.2.497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Storkel HL, Maekawa J, Hoover JR. Differentiating the Effects of Phonotactic Probability and Neighborhood Density on Vocabulary Comprehension and Production: A Comparison of Preschool Children With Versus Without Phonological Delays. Journal of Speech, Language & Hearing Research. 2010;53(4):933–949. doi: 10.1044/1092-4388(2009/09-0075). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thiemann-Bourque K, Brady N, Fleming K. Symbolic Play of Preschoolers with Severe Communication Impairments with Autism and Other Developmental Delays: More Similarities than Differences. Journal of Autism and Developmental Disorders. 2011:1–11. doi: 10.1007/s10803-011-1317-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thiemann-Bourque K, Warren S, Brady N. What We Can Learn from Counting Words: Applications and Implications of the Automatic Measurement of Natural Environments; Paper presented at the Society for Research on child Development, Montreal.2010. [Google Scholar]
- Thomson J, Richardson U, Goswami U. Phonological similarity neighborhoods and children's short-term memory: Typical development and dyslexia. Memory & Cognition. 2005;33(7):1210–1219. doi: 10.3758/BF03193223. [DOI] [PubMed] [Google Scholar]
- Thurm A, Lord C, Lee L, Newschaffer C. Predictors of language acquisition in preschool children with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2007;37:1721–1734. doi: 10.1007/s10803-006-0300-1. [DOI] [PubMed] [Google Scholar]
- Toth K, Munson J, Meltzoff AN, Dawson G. Early Predictors of Communication Development in Young Children with Autism Spectrum Disorder: Joint Attention, Imitation, and Toy Play. Journal of Autism and Developmental Disorders. 2006;36(8):993–1005. doi: 10.1007/s10803-006-0137-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vihman MM, DePaolis RA, Keren-Portnoy T. The Role of Production in Infant Word Learning. Language Learning. 2014;64(s2):121–140. doi: 10.1111/lang.12058. [DOI] [Google Scholar]
- Vismara LA, Comlombi C, Rogers SJ. Can 1 hour per week of therapy lead to lasting changes in young children with autism? Autism. 2009;13:93–115. doi: 10.1177/1362361307098516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vivanti G, Dissanayake C, Zierhut C, Rogers S. Brief Report: Predictors of Outcomes in the Early Start Denver Model Delivered in a Group Setting. Journal of Autism and Developmental Disorders. 2013;43(7):1717–1724. doi: 10.1007/s10803-012-1705-7. [DOI] [PubMed] [Google Scholar]
- Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glasser A, Veenstra-VanderWeele J. A Systematic Review of Early Intensive Intervention for Autism Spectrum Disorders. Pediatrics. 2011;127(5):e1303–e1311. doi: 10.1542/peds.2011-0426. [DOI] [PubMed] [Google Scholar]
- Whitehurst G, Falco F, Lonigan C, Fischel J. Accelerating language development through picture book reading. Developmental Psychology. 1988;24(4):552–559. [Google Scholar]
- Yoder P, Compton D. Identifying predictors of treatment response. Mental Retardation and Developmental Disabilities Research Reviews. 2004;10(3):162–168. doi: 10.1002/mrdd.20013. [DOI] [PubMed] [Google Scholar]