

Abstract
Purpose
The purpose of this research was to examine spatial and temporal aspects of articulatory control in children with apraxia of speech (CAS), children with speech delay characterized by an articulation/phonological impairment (SD) and typically developing controls (TD) during speech tasks that increase in word length.
Method
The participants included 33 children between three and seven years of age (11 CAS, 11 SD, and 11 TD). A motion capture system was used to track jaw, lower lip and upper lip movement during a naming task. Movement duration, velocity, displacement, and variability were measured from accurate word productions.
Results
Movement variability was significantly higher in the children with CAS as compared to participants in the SD and TD groups. Differences in temporal control were seen between both groups of speech-impaired children and the TD controls during accurate word productions. As word length increased, movement duration and variability differed between the CAS and SD children.
Conclusions
These findings provide evidence that movement variability distinguishes children with CAS from speakers with SD. Kinematic differences between the CAS and SD participants suggest that these groups respond differently to linguistic challenges.
Childhood apraxia of speech (CAS) is a complex disorder involving a core impairment in planning and/or programming of speech movements (ASHA, 2007). The American Speech Language and Hearing Association’s (ASHA) position statement on CAS highlights three features that are consistent with deficits in speech motor control: inconsistent errors on repeated syllable or word productions, impaired coarticulation patterns, and prosodic errors (ASHA, 2007). While these differentiating features implicate a deficit in articulatory control, questions remain as to the specific aspects of movement that are deficient in CAS. To address this knowledge gap, the current study examined oral articulator movement in children with idiopathic CAS, children with delayed speech development characterized by articulation and/or phonological errors (SD), and typically developing controls (TD). Specifically, we examined spatial and temporal parameters of articulator movement in an effort to identify whether movement characteristics distinguish these two groups of speech impaired children from one another, as well as from children with age appropriate speech production skills.
Many past studies have emphasized isolating one level of processing deficit in CAS (e.g. motor planning, programming, execution); however, the connection between different levels of processing is difficult to tease apart in a developing system where impairment at one level may impact the development of other levels of processing (Maassen, Nijland & Terband, 2010). Therefore, it has been proposed that research shift focus away from locating the core etiology of CAS with greater emphasis placed on the interactional nature of development (see Maassen et al., 2010 for a review). One approach to exploring the complex interaction between different levels of processing is to study speech production in the context of varied task demands. Thus, an additional goal of the present work was to compare articulatory control between speech impaired and typically developing children as they produced words that increased in length
Speech motor control in CAS
Researchers have used acoustic or kinematic methods to examine speech motor control in CAS (Bahr, 2005; Grigos & Kolenda, 2005; Moss & Grigos, 2012; Nijland et al., 2002; 2003a; Nijland, Maassen, & Van der Meulen, 2003b; Shriberg et al., 2003a; Shriberg, Green, Campbell, McSweeney & Scheer, 2003b; Skinder, Strand & Mignerey, 1999; Terband, Maassen, Van Lieshout & Nijland, 2011; Terband, Zaalen & Maassen, 2012). Results from several studies have provided evidence of deviant coarticulation patterns in children with CAS (Nijland et al., 2002; 2003a; 2003b). Nijland et al. (2002) investigated coarticulation in four to six-year-old children with CAS, typically developing children and adults during production of nonwords embedded in a carrier phrase. They reported that F2 values were higher and more variable in the CAS group than in the typically developing group. In addition, children with CAS produced lower F2 ratios than controls and had higher within-group and within-subject variability for F2 ratios. The authors concluded that both intrasyllabic and intersyllabic coarticulation differed in CAS, suggesting a deficit in syllabic planning. In a subsequent study, Nijland et al. (2003a) examined anticipatory coarticulation during repetition of phrases that consisted of identical phonetic contexts yet differed by syllable structure. Across syllable structures, intrasyllabic coarticulation and within-subject variability were higher in the CAS group than in the controls.
In addition to differences in coarticulation in CAS, there is acoustic evidence consistent with deficits in temporal control of speech. Children with CAS have been reported to produce longer acoustic durations of segments (Nijland et al., 2003a) and words (Bahr, 2005) than typically developing controls. Past research has also shown that the degree of variability in the duration of pause and speech events may differentiate children with CAS from children with other speech impairments (Shriberg et al., 2003b). In relation to lexical stress production, differences in the use of acoustic cues (i.e. frequency, amplitude and duration) to mark either lexical or sentential stress have been reported between children with CAS and typically developing controls (Skinder et al., 1999), as well as children with other speech sound disorders (Shriberg et al. 2003a). Collectively, these works provide support from acoustic analyses that CAS involves deficient speech motor processing.
Kinematic research has aimed to delineate patterns of articulatory control in children with CAS. Grigos and Kolenda (2010) used movement tracking to investigate longitudinal changes in jaw movement during a period of phonemic acquisition in a three-year-old child with CAS and a typically developing control group. The child with CAS was studied every two weeks over an eight month period until he began accurately and consistently producing the bilabial phonemes /p/, /b/ and /m/ in CVC word structures (i.e. bob, mom, pop). Changes in articulator movement over time included decreased variability (measured by the spatiotemporal index, STI, Smith, Goffman, Zelaznik, Ying & McGillem, 1995) and increased jaw velocity. By the final session, both velocity and variability fell within a 95% confidence interval established for the typically developing controls. There was a significant positive correlation between movement stability and consonant accuracy. The authors suggested that increased phoneme accuracy and consistency may have been facilitated by more refined articulatory control. This relationship between speech motor processes and perceptual indices of speech intelligibility was further explored in the present work in a larger cohort of children with CAS. We examined the hypothesis that children demonstrating the poorest segmental accuracy would show atypical speech motor performance during accurate speech production.
To date, few studies have compared articulatory control between children with CAS and children with other speech sound disorders (Terband et al., 2011; 2012; Moss & Grigos, 2012). Terband et al. (2011) used electromagnetic midsagittal articulography (EMMA) to examine lip, jaw, and tongue tip movement in five children with a speech sound disorder (SSD) characterized by phonological deficits, five children with subtype CAS and six typically developing children, all of whom were between the ages of six and nine years. Tongue, lower lip and jaw movement displacement were measured during a reiterative speech task (i.e., repeated productions of /pa:s/and /spa:/). The results showed larger lower lip amplitude in both the CAS and SSD groups in the absence of any differences in stability. This finding suggests the use of an adaptive strategy in which both groups increased movement amplitude to obtain stability equal to that of the controls. A direct relationship between amplitude and stability has been described in previous studies (Van Lieshout, Bose, Square & Steele, 2007; Van Lieshout, Rutjens & Spauwen, 2002) and is thought to reflect a control strategy in which amplitude changes result in greater stability by providing more precise afferent feedback. In a later study, Terband et al. (2012) investigated jaw movement in the coronal plane in 16 typically developing children, 18 young adults and five children with developmental speech disorders between four and seven years of age during the same reiterative speech task. Results showed that all children in the SSD group (which included participants with CAS) had greater lateral jaw movement and variability relative to normative data for at least one of the stimuli. The authors highlighted that lateral jaw movement of the child with a phonological disorder may have deviated from controls in average angle but was not characterized by higher instability. For the child with CAS, a deviant average movement angle was accompanied by greater instability. Taken together, these studies provide evidence that children with a range of speech sound disorders may demonstrate deviant speech motor control relative to typically developing children. What may differentiate children with CAS from other children with other speech impairments is the degree of instability across articulators and speech tasks, potentially indicating that children with CAS do not use the same strategies to minimize instability as other subtypes of speech sound disorders when articulatory and linguistic demands increase.
Another window into speech motor development in CAS is through the study of movement coordination. Moss and Grigos (2012) examined the relationship between lip and jaw movements in three to six-year-old children identified as either having CAS, a speech delay characterized by articulation and/or phonological deficits (SD), or typical speech and language development (TD) (6 participants per group). The peak correlation coefficient was obtained for each articulator pair (i.e. jaw/upper lip; jaw/lower lip; upper lip/lower lip) per production and was used as an index of spatial coupling, while the lag, or time required to achieve peak spatial coupling, was used as a measure of temporal coupling (Green, Moore, Higashikawa & Steeve, 2000). There were no significant differences in the peak coefficient and lag between articulator pairs in the children with CAS, SD and TD. There were group differences, however, in the variability of spatial-temporal coupling, as measured by the coefficient of variation of the peak coefficient and lag values. Both spatial and temporal coupling were shown to be more variable in the children with CAS as compared to the participants with SD. In addition, lip aperture STIs (Smith et al., 1995) were significantly higher in the CAS than SD group. These findings provide further evidence that children with CAS achieve accurate speech using a less stable motor plan than their peers with other speech impairments. Based upon these results and others described above, we predict that children with CAS will be differentiated from children with other speech sound disorders by articulator movements that are longer in duration, smaller in displacement, slower in velocity and greater in variability.
Effects of Word Length on Articulatory Control in Children
Task effects on articulator movement have been shown in young typically developing children producing different orofacial behaviors (Nip, Green & Marx, 2009). The influence of task complexity on speech output is particularly interesting to explore in children with CAS as they commonly display difficulties sequencing articulator movements, such that phonemes in isolation are often produced with greater accuracy than when embedded in longer sequences. This suggests that task demands, such as increased utterance length, may have specific effects on articulator movement in CAS. There is evidence that typically developing children and adolescents display increases in movement variability as utterance length increases (Sadagopan & Smith, 2008; Walsh, Smith & Weber-Fox, 2006). For instance, Sadagopan and Smith (2008) showed that, in children and adolescents, lip aperture variability was higher when “Buy Bobby a puppy” was embedded in a longer utterance than when produced in isolation; however, the young adults studied did not display differences in STI related to utterance length. Walsh et al. (2006) reported that children’s speech movements were of greater duration than those of the adults when producing nonwords that increased in length. Lip aperture and lower lip-jaw variability increased with word length in all speakers, although to a greater extent in the children than the adults.
Findings from Moss and Grigos (2012) suggest that word length may impact articulator movement to a greater extent in children with CAS than children with SD and TD. Significant group differences in lip aperture stability were found as the children produced one, two and three syllables words. Although the interaction between group and length was not significant, the CAS group demonstrated much larger effect sizes between one and two-syllable words, as well as between one and three-syllable words, as compared to the SD and TD groups. This result highlights the need for additional research to determine whether increases in speaking demands, such as changes in word length, have a greater impact on movement sequencing for children with CAS as compared to children with other speech sound disorders. As a means to further explore the relationship between speech motor and linguistic processes in CAS, the current work examined the production of stimuli that varied in word length. We hypothesized that manipulating word length itself, thus directly taxing the level of syllabic planning, would impact children with CAS to a greater extent than their peers.
Research questions
Many studies of speech motor control in CAS are limited by small sample sizes or the absence of a comparison group including children with other speech sound impairments. Moreover, studies involving children with CAS have not adequately examined the effect of increasing linguistic complexity on speech motor control or studied the relationship between speech motor processes and perceptual measures of speech intelligibility. The current study addressed these issues by investigating spatial and temporal aspects of articulatory control in a larger cohort of children with CAS, children with SD and TD controls during speech tasks that increased in linguistic complexity through changes in word length. The following research questions were explored:
Do characteristics of oral articulator movement (duration, displacement, velocity and variability) differ in children with CAS relative to SD and TD participants?
Do increases in word length influence oral articulator movement to a greater extent in children with CAS relative to SD, and TD participants?
Is there a relationship between measures of articulatory control and indices of speech intelligibility in children in the CAS, SD and TD groups?
Method
Participants
The participants were thirty-three children between the ages of 3 years 1 month and 7 years 7 months, which included 11 children diagnosed with apraxia of speech (CAS), 11 children diagnosed with an articulation and/or phonological impairment (SD), and 11 children with typically developing speech and language skills (TD). Eleven TD participants were selected from a larger cohort of 24 TD children, matching for chronological age as closely as possible. The mean age (standard deviation) per group was 4.7 years (1.2) for CAS, 5.2 years (1.4) for SD and 5.2 years (1.2) for TD. In light of the age discrepancy between the CAS group and children in the SD and TD groups (on average 7 months), all children displayed age appropriate receptive language and cognitive skills (discussed in detail below). Data were collected from 5 additional children, who after careful analysis, were identified as having characteristics of both CAS and dysarthria. The inclusion criteria specified that children in the CAS group could not display characteristics of dysarthria. As a result, these children were excluded from group comparisons. All participants were monolingual speakers of American English.
Standardized testing of speech, language, cognition and oral motor skills, as well as a hearing screening, was conducted. Table 1 displays standardized testing results. To ensure that language comprehension and cognition did not influence performance on the experimental protocol, inclusion in the study for all participants was dependent upon the following criteria: normal receptive language (> -1SD from mean) as measured by the Test of Early Language Development (TELD-3, Hresko, Reid & Hammill, 2007) and normal cognition (> -1SD from mean) as measured by the Columbia Mental Maturity Scale (CMMS, Burgmeister et al. 1972). This measure of cognitive functioning was chosen because it is a nonverbal test and performance was not influenced by speech production difficulties. The mean Receptive Language Quotient (RLQ) on the TELD-3 (standard deviation) per group was 109 (16) for CAS, 110 (12) for SD and 120 (9) for TD. The mean standard score on the CMMS (standard deviation) per group was 118 (18) for CAS, 111 (11) for SD and 121 (16) for TD. All participants passed a hearing screening at 25dB SPL at 500, 1000, 2000 and 4000Hz.
Table 1.
Formal and Informal Testing Results
| Age | TELD | CMMS ADS | GFTA | VMPAC | SPEECH SAMPLE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participant | (mos.) | Gender | RLQ | ELQ | %ile | SS | GMC | FOMC | SEQ | PCC | PVC | WWC | |
| CAS1 | 37 | M | 122 | 101 | 93 | 8 | 73 | 100 | 63 | 35 | 47 | 72 | 28 |
| CAS2 | 43 | M | 134 | 77 | 111 | 29 | 95 | 95 | 83 | 54 | 54 | 85 | 25 |
| CAS3 | 44 | F | 83 | 94 | 101 | 5 | 63 | 100 | 44 | 20 | 46 | 79 | 19 |
| CAS4 | 45 | M | 116 | 115 | 150 | 5 | 64 | 95 | 77 | 57 | 54 | 81 | 27 |
| CAS5 | 51 | M | 122 | 91 | 106 | 56 | 104 | 80 | 66 | 48 | 75 | 87 | 49 |
| CAS6 | 53 | M | 90 | 88 | 118 | 13 | 82 | 100 | 85 | 76 | 66 | 78 | 38 |
| CAS7 | 62 | M | 113 | 115 | 150 | 19 | 88 | 85 | 84 | 72 | 55 | 52 | 47 |
| CAS8 | 64 | M | 110 | 88 | 120 | 13 | 82 | 85 | 93 | 87 | 87 | 92 | 59 |
| CAS9 | 68 | M | 110 | 105 | 122 | <1 | 47 | 100 | 91 | 70 | 80 | 85 | 55 |
| CAS10 | 69 | M | 85 | 91 | 113 | 2 | 55 | 100 | 97 | 76 | 66 | 76 | 54 |
| CAS11 | 86 | M | 115 | 115 | 116 | 30 | 100 | 100 | 98 | 98 | 83 | 83 | 61 |
|
| |||||||||||||
| SD1 | 38 | F | 113 | 105 | 104 | 32 | 90 | 100 | 77 | 65 | 90 | 99 | 62 |
| SD2 | 49 | M | 125 | 124 | 103 | 2 | 53 | 85 | 83 | 61 | 65 | 88 | 43 |
| SD3 | 44 | F | 137 | 120 | 124 | 78 | 113 | 100 | 100 | 100 | 93 | 97 | 63 |
| SD4 | 58 | F | 95 | 102 | 105 | 66 | 110 | 100 | 74 | 100 | 90 | 93 | 68 |
| SD5 | 56 | M | 108 | 115 | 118 | 43 | 99 | 100 | 97 | 80 | 88 | 93 | 75 |
| SD6 | 63 | M | 110 | 112 | 130 | 79 | 112 | 100 | 99 | 100 | 90 | 95 | 73 |
| SD7 | 64 | M | 110 | 94 | 106 | 14 | 83 | 100 | 94 | 100 | 79 | 86 | 56 |
| SD8 | 72 | M | 110 | 97 | 106 | 27 | 98 | 100 | 95 | 98 | 83 | 99 | 67 |
| SD9 | 78 | M | 105 | 102 | 94 | 8 | 74 | 95 | 99 | 78 | 84 | 87 | 60 |
| SD10 | 79 | M | 100 | 97 | 118 | 9 | 77 | 100 | 100 | 100 | 74 | 89 | 62 |
| SD11 | 92 | F | 96 | 107 | 109 | 3 | 78 | 90 | 99 | 100 | 87 | 88 | 77 |
|
| |||||||||||||
| TD1 | 37 | M | 119 | 115 | 128 | 98 | 127 | 100 | 100 | 100 | 94 | 98 | 91 |
| TD2 | 49 | M | 122 | 112 | 108 | 41 | 99 | 100 | 100 | 100 | 80 | 87 | 84 |
| TD3 | 48 | F | 128 | 118 | 133 | 91 | 118 | 100 | 99 | 100 | 99 | 100 | 97 |
| TD4 | 58 | F | 119 | 112 | 128 | >87 | 117 | 100 | 99 | 83 | 92 | 89 | 95 |
| TD5 | 56 | M | 131 | 115 | 105 | 72 | 110 | 100 | 98 | 96 | 94 | 98 | 91 |
| TD6 | 66 | M | 130 | 118 | 128 | >83 | 113 | 100 | 100 | 100 | 98 | 99 | 98 |
| TD7 | 68 | M | 121 | 97 | 150 | >79 | 112 | 100 | 100 | 100 | 100 | 100 | 100 |
| TD8 | 69 | M | 118 | 94 | 130 | >79 | 112 | 100 | 99 | 100 | 99 | 100 | 99 |
| TD9 | 73 | M | 118 | 112 | 115 | 54 | 107 | 100 | 97 | 98 | 97 | 100 | 91 |
| TD10 | 82 | M | 110 | 102 | 107 | >64 | 110 | 100 | 99 | 100 | 100 | 99 | 98 |
| TD11 | 84 | M | 100 | 115 | 94 | >64 | 109 | 100 | 100 | 94 | 93 | 95 | 94 |
TELD: Test of Early Language Development-3 (RLQ = Receptive Language Quotient; ELQ = Expressive Language Quotient)
CMMS: Columbia Mental Maturity Scale (ADS = Age Deviation Score)
GFTA: Goldman-Fristoe Test of Articulation-2 (%ile = percentile; SS = standard score)
VMPAC: Verbal Motor Production Assessment for Children (GMC = Global Motor Control; FOMC = Focal Oral Motor Control; SEQ = Sequencing)
Speech Sample: PCC = Percentage of Consonants Correct; PVC = Percentage of Vowels Correct; WWC =Percentage of Whole Word Correct
Expressive language was evaluated through the expressive language subtest of the TELD-3. Children in the TD group were required to score no lower than one standard deviation below the mean on the expressive language subtest. As speech production skills may impact expressive language skills, this same criterion did not apply to performance on the expressive language subtest of the TELD-3 for children in the CAS and SD groups. The Verbal Motor Production Assessment for Children (VMPAC, Hayden & Square, 1999) was used to assess oral motor skills.
Speech production skills were examined using the Goldman Fristoe Test of Articulation (GFTA-2, Goldman, Fristoe 2000), a 100-word conversational speech sample and the sequencing subtest of the VMPAC. Information obtained from these speaking contexts was used to describe phonetic inventory, syllable structure, lexical stress, consonant and vowel accuracy, whole word accuracy, occurrence of phonological processes and error consistency. A phonetic inventory was judged to be reduced if a child did not produce phonemes acquired by 90% of children their age as reported by Smit, Hand, Freilinger, Bernthal and Bird (1990). The presence of a phonological process was confirmed using criteria from McReynolds and Elbert (1981), where a process needs to occur in at least 20% of the possible opportunities and have at least four opportunities to occur. Percentage of consonants correct (PCC), percentage of vowels correct (PVC) (Shriberg, Austin, Lewis, McSeeney & Wilson, 1997) and whole word accuracy were calculated from speech samples. Accuracy of whole word productions was examined by modifying published measures (i.e. Schmidt, Howard & Schmidt, 1983; Ingram & Ingram, 2001), which only identified segmental errors, to also include suprasegmental errors (i.e. inaccurate and equal lexical stress). The percentage of whole words correct (WWC) was determined by dividing the number of words produced without segmental or suprasegmental errors by the total number of intelligible words in the sample and then multiplying by 100. This whole word measure captures the broad impact of segmental and suprasegmental errors on word accuracy. PCC, PVC and WWC scores are shown in Table 1.
Differential Diagnosis
There is no definitive list of characteristics that distinguish children with CAS from those with other speech sound disorders (ASHA, 2007). Another challenge in the diagnosis of CAS is that characteristics seen in children with CAS may also be seen in children with other speech sound disorders. The diagnoses of CAS and SD in the present work were based on careful analysis of each participant’s speech production skills across three different speaking contexts: single word productions (GFTA-2), connected speech (conversational speech sample) and sound/syllable sequencing tasks (VMPAC). These analyses were separately performed by two ASHA certified speech language pathologists with expertise in pediatric motor speech disorders (the first and second authors). Assessing the presence of speech characteristics across different speaking contexts (e.g. single words, conversation and syllable sequencing tasks) is an essential component of a comprehensive examination, as poor performance on single-word testing alone is not sufficient for diagnosis of a motor speech impairment, such as CAS. Further, results from single word articulation tests can be misleading when scoring is not based on all phonemes included in the words and when difficulties seen during connected speech may not be evident during the production of isolated words. Our analyses identified whether children produced speech errors in more that one speaking context that were not age appropriate according normative data from Smit et al. (1990) and Hodson & Paden (1981). Participants who were later diagnosed with CAS or SD met one or more of the following criteria: (a) GFTA-2 standard scores below 85; (b) PCC below 85%; (c) WWC below 65% for children between the ages of 36 to 48 months and below 80% for children older that 48 months. Previous research on children with age appropriate articulation skills reported increases in whole word accuracy from 69% to 80% from 36 to 48 months and to 92% by 72 months (Schmidt et al., 1983). Diagnostic distinction between CAS and SD is specified below.
CAS group
Diagnostic classification for CAS was determined according to the presence of the three core features identified in the ASHA position statement (ASHA, 2007): (a) inconsistent consonant and vowel errors; (b) difficulties forming articulatory transitions between sounds and syllables; and (c) prosodic errors. Children diagnosed with CAS displayed these features in more than one speaking context and within at least three different words (or sounds/syllables in the sequencing task). Inconsistent errors were defined as consonant and vowel errors that differed across repeated productions of the same word (e.g. “hot” /hat/ produced as /ha/, /at/ or /ta/ by the same speaker).1 Difficulties forming articulatory transitions were characterized by poor sequencing of adjacent sounds and/or syllables, particularly when they included phonemes that were present in the child’s repertoire (e.g. difficulty combining the phoneme /b/ with different vowels, even though /b/ and the vowels are accurately produced in other contexts). Prosodic errors were identified as incorrect lexical and/or phrasal stress (e.g. producing a strong-weak structure as strong-strong or weak-strong). In addition to the three core features, children with CAS also demonstrated at least four of the following characteristics: metathesis, vowel errors, timing errors (e.g. difficulty differentiating between voiced and voiceless cognates), phoneme distortions, articulatory groping (e.g. visual struggle accompanying phoneme production), impaired volitional oral movement (e.g. excessive oral opening during an open/close sequence), reduced phonetic inventory and poorer expressive than receptive language skills. A participant was identified as using metathesis, vowel errors, timing errors, distortions and articulatory groping when such patterns were seen across two different speaking contexts and within at least three different words (or sounds/syllables in the sequencing task). Children in the CAS group exhibited normal structure of the oral-peripheral mechanism as determined by the VMPAC. The examiners were 100% reliable in identifying the presence of characteristics in the children with CAS.
SD group
All participants in the SD group were diagnosed with an articulation and/or phonological impairment. The diagnosis was based on measures of accuracy and intelligibility during single word testing, the connected speech sample and sequencing task. Deviant speech patterns seen in the SD group primarily included consonant/vowel substitutions, omissions, additions and distortions associated with an articulation impairment (e.g., interdental lisp, r-distortion), as well as systematic use of phonological processes (e.g., velar fronting, gliding) as seen in a phonological impairment. Several children displayed prosodic errors. A participant was identified as using substitutions, omissions, additions, distortions and prosodic errors when such patterns were seen across two different speaking contexts and within at least three different words (or sound/syllables in the sequencing task). None of the children included in the SD group displayed all three of the core features identified in the ASHA position statement associated with CAS (i.e. inconsistent errors, poor articulatory transitions and prosodic errors) (ASHA, 2007). Results of the VMPAC were analyzed to rule out motor speech and sequencing deficits, as well as to confirm that children in the SD group exhibited normal structure of the oral-peripheral mechanism. Speech characteristics displayed by children in the CAS and SD groups in each of the three speaking contexts are shown in Table 2. The examiners were 96% reliable in identifying the presence of characteristics in the children with SD.
Table 2.
Speech Characteristics of Participants Diagnosed with CAS and SD
| Age (mos.) |
Incon. Errors |
Mvt. Seq. Deficits |
Prosodic Errors |
Timing Errors |
Groping | Reduced Inventory |
Phon. Process. |
Vowel Errors^ |
Consonant Errors | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DIST* | SUB | ADD | OMM | ||||||||||
| CAS1 | 37 | + (2,3) | + (1,2,3) | + (1,2,3) | — | — | + (1,2) | + (1,2,3) | + (1,2,3) | — | + (1,2,3) | + (1,2,3) | + (1,2,3) |
| CAS2 | 43 | + (2,3) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (2,3) | + (1,2) | + (1,2,3) | + (1,2,3) | — | + (1,2,3) | — | + (1,2) |
| CAS3 | 44 | + (2,3) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (2,3) | + (1,2) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (2,3) | + (1,2,3) |
| CAS4 | 45 | + (2,3) | + (1,2,3) | + (1,2,3) | + (1,2) | + (2,3) | + (1,2) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (2,3) | + (1,2,3) |
| CAS5 | 51 | + (2,3) | + (1,2,3) | + (1,2,3) | + (1,2) | — | + (1,2) | + (1,2) | + (1,2,3) | + (1,2,3) | + (1,2,3) | — | + (1,2,3) |
| CAS6 | 53 | + (2,3) | + (1,2,3) | + (1,2,3) | + (1,2) | + (1,2,3) | + (1,2) | + (1,2) | + (1,2,3) | + (1,2) | + (1,2,3) | + (2,3) | + (1,2,3) |
| CAS7 | 62 | + (2,3) | + (1,2,3) | + (1,2,3) | — | — | + (1,2) | + (1,2) | + (1,2,3) | — | + (1,2,3) | + (2,3) | + (1,2,3) |
| CAS8 | 64 | + (2,3) | + (1,2,3) | + (1,2,3) | — | + (1,2,3) | + (1,2) | — | + (1,2,3) | + (2,3) | + (1,2,3) | + (1,2,3) | + (1,2,3) |
| CAS9 | 68 | + (2,3) | + (1,2,3) | + (1,2,3) | — | + (2,3) | + (1,2) | + (1,2) | + (1,2,3) | — | + (1,2,3) | + (1,2) | + (1,2) |
| CAS10 | 69 | + (2,3) | + (1,2,3) | + (1,2,3) | + (2,3) | + (1,2,3) | — | + (1,2) | + (1,2,3) | + (1,2,3) | + (1,2,3) | + (2,3) | + (1,2) |
| CAS11 | 86 | + (2,3) | + (1,2) | + (1,2,3) | + (1,2,3) | + (1,2,3) | — | — | + (1,2) | + (1,2,3) | + (1,2) | + (1,2) | + (1,2) |
|
| |||||||||||||
| SD1 | 38 | + (2,3) | — | + (1,2) | — | — | + (1,2) | + (1,2,3) | — | + (1,2,3) | — | + (1,2) | + (1,2) |
| SD2 | 49 | + (2,3) | + (2,3) | — | — | — | + (1,2) | + (1,2) | + (1,2) | — | + (1,2,3) | + (1,2,3) | + (1,2) |
| SD3 | 44 | — | — | + (1,2) | — | — | — | — | — | + (1,2) | + (1,2) | + (1,2) | + (1,2) |
| SD4 | 58 | — | — | — | + (1,2) | — | — | — | + (1,2) | — | + (1,2) | — | + (1,2) |
| SD5 | 56 | — | — | — | — | — | + (1,2) | + (1,2) | + (1,2) | — | + (1,2) | — | + (1,2) |
| SD6 | 63 | — | — | — | — | — | — | — | + (1,2) | + (1,2) | + (1,2) | — | + (1,2) |
| SD7 | 64 | — | — | — | + (1,2) | — | — | — | + (1,2) | — | + (1,2) | + (1,2) | + (1,2) |
| SD8 | 72 | — | — | — | + (1,2) | — | — | — | — | — | + (1,2) | + (1,2) | + (1,2) |
| SD9 | 78 | — | — | + (1,2) | — | — | — | + (1,2,3) | + (1,2) | — | + (1,2,3) | — | + (1,2) |
| SD10 | 79 | — | — | — | + (1,2) | — | — | — | + (1,2) | + (1,2) | + (1,2) | + (1,2) | + (1,2) |
| SD11 | 92 | — | — | — | + (1,2) | — | — | — | + (1,2) | + (1,2) | + (1,2) | + (1,2) | + (1,2) |
DIST= Distortions; SUB= Substitutions; ADD=Additions; OMM=Omissions
+ characteristic present
— characteristic absent
Including vocalic /r/ errors
Including /s/ lateralizations, interdentalizations and consonantal /r/ distortions
Context: 1= Single words; 2= Conversational speech sample; 3= Syllable sequencing task
TD group
The participants with typically developing speech and language skills had no reported histories of speech, language or hearing problems and/or neurological disorders. The TD children met the inclusionary criteria described above regarding cognition, receptive language and hearing. In addition, they demonstrated (a) normal structure and functioning of the oral mechanism as determined by the VMPAC (Hayden & Square 1999); (b) age appropriate articulation skills as measured by the conversational speech sample and GFTA-2; (c) age appropriate expressive language skills as measured by the TELD-3. The lower limit for performance on the GFTA-2 and the TELD-3 for the TD children was one standard deviation below the mean. We used normative data provided in Smit et al. (1990) and Hodson & Paden (1981) to determine whether articulation skills were age appropriate. Children with age-appropriate articulation and/or phonological errors, according to these criteria, were included in the TD group.
Instruments
A motion capture system (Vicon 460, Vicon Motion Systems, 2001) was used to track articulator movement in three dimensions. Twelve 3mm reflective markers were placed on the face to track lip and jaw movement and to account for head movement. Three markers were placed on the jaw and four markers on the lips to measure oral articulator movement. Five markers were placed on the nose, nasion and forehead to account for head movement and rotation. Lip markers were placed in the midline of the vermilion border of the upper lip, midline of the vermilion border of the lower lip and on the corners of the mouth. Vertical lip movement was tracked using the markers on the upper lip and lower lip. The system tracked reflective markers at a sampling rate of 120 frames per second. Video and audio recordings were made using a Sony digital video camera (Model DSC-T1) and a digital minidisc recorder (HHB50). Recordings were made in a sound attenuated audiometric booth. Testing and data collection were performed in the Motor Speech Laboratory in the Department of Communicative Sciences and Disorders at New York University.
Data Collection and Procedures
The children were seated in a chair in a sound attenuated booth. During the familiarization phase, the children were introduced to the characters Pop (an elderly male puppet), puppet (a dragon puppet) and puppypop (a puppy shaped as a lollipop). These particular words were chosen as they included the bilabial plosive /p/, which allowed for visualization of lip and jaw movement. A brief training session was used to familiarize the children with the characters and items, as well as to model appropriate responses. The experimenter elicited token productions while following a protocol, which specified the sequence to follow and the cues that could be used. Character names were embedded in a story retell game in which the children were asked to complete a sentence or respond to a question using one of the target words. For example, to elicit the utterance Pop the child was presented with a scenario where Pop was hungry and had to select a food choice, such as a banana. The clinician asked the child, Who will eat the banana? with the correct response being Pop. This approach was taken to elicit naturalistic productions of the target words. Model responses were provided if a child did not remember a character name, however, direct imitations were not included in the analyses. Each token was elicited between 10 and 15 times in a randomized order.
Analyses
Data analyses were performed in several ways. Transcription measures were computed from correct and incorrect production of tokens (pop, puppet, puppypop). Kinematic measures were based only on accurate word productions to ensure that any observed kinematic differences were due to underlying changes in speech motor control that were independent from articulation errors.
Transcription analysis
Two listeners transcribed all productions of pop, puppet and puppypop using narrow transcription. The percent agreement between listeners was 93%. Productions were eliminated if the listeners identified segmental or suprasegmental errors, unusual voice or fluency patterns and if all reflective markers were not visible for the entire utterance. The original data pool consisted of 902 productions, which included trials where reflective markers were visible for the entire utterance (CAS=312, SD=301, TD=289). These productions were analyzed for consonant (PCC) and vowel accuracy (PVC). In addition, consistency across repeated productions of the same word were examined using Percent Word Consistency (PWC). The PWC was calculated by comparing the number of different forms of the word produced by a participant (which included both correct and incorrect forms of the word) to the total number of productions of that particular token. This whole word measure examined the entire word form, rather than individual segmental errors. Preliminary findings showed that PWC differentiated error consistency in children with CAS and SD as compared to calculations that only examined erred productions or those that focused only on segmental accuracy (Case, Moss, & Grigos, 2012). The following formula was utilized for this calculation:
If a participant produced a token accurately more than eight times, the first eight accurate productions were selected for further analysis. Thus a maximum of 264 productions could be obtained from each experimental group (8 productions × 11 participants × 3 tokens). The resulting number of productions per group (pop, puppet, puppypop shown in parentheses) was 190 (76, 64, 50) for CAS, 231 (82, 73, 76) for SD and 227 (81, 79, 67) for TD participants. The number of productions varied per child (ranging from five to eight). One participant with CAS did not achieve any accurate productions of puppet. Several participants did not achieve any accurate productions of puppypop (3 CAS, 2 SD and 1 TD). Data for those tokens were then analyzed for the remaining participants in each group. Further, lip movement data were not obtained from three of the children with CAS who displayed hypersensitivity to placement of reflective markers on the upper and lower lip. The number of participants per group for each comparison is noted in the results and on all related figures.
Kinematic analysis
The nasion and forehead markers were used to determine the orientation and to account for vertical head movement and rotation. Upper lip and jaw movements were calculated by subtracting their y coordinates from stationary forehead points (UL – Forehead; J – Forehead). Lower lip displacement was measured as the vertical lower lip movement subtracted from the jaw (LL – J). Lip aperture was calculated as the vertical distance between the upper and lower lips. The jaw signal was subtracted from the mean jaw value, creating an origin. The same subtraction method was applied to the lower and upper lip signals. The right jaw marker was used to track jaw movement to reduce the error associated with chin surface tracking (Green, Wilson, Wang, & Moore, 2007). The acoustic signal was aligned with the kinematic trajectory for each production. Movement kinematics were examined using custom Matlab algorithms (version 7.5, Mathworks, 2007).
The jaw displacement trajectory was used to identify the onset and offset of movement for each trial. The threshold for movement onset was taken as the point 10 frames (.083s) prior to the initial peak closing displacement for the first consonant in each token. Movement offset was selected as the point ten frames (.083s) following the final opening displacement associated with the vowel in pop and final vowels in puppet and puppypop (Figure 1). The offset was chosen in this manner in order to be consistent across tokens since lip and jaw movement associated with /t/ in puppet cannot be measured using facial tracking technology. These onset and offset criteria were used to mark duration, displacement and velocity across the entire word. Total movement duration was measured as the time between the onset and offset points. Average jaw displacement was calculated as the mean peak-to-peak displacement of each open and closing movement across the utterance, excluding the final consonant. Similarly, average jaw velocity was calculated as the mean velocity across the utterance. Lip aperture was measured as the distance between the upper and lower lips.
Figure 1.
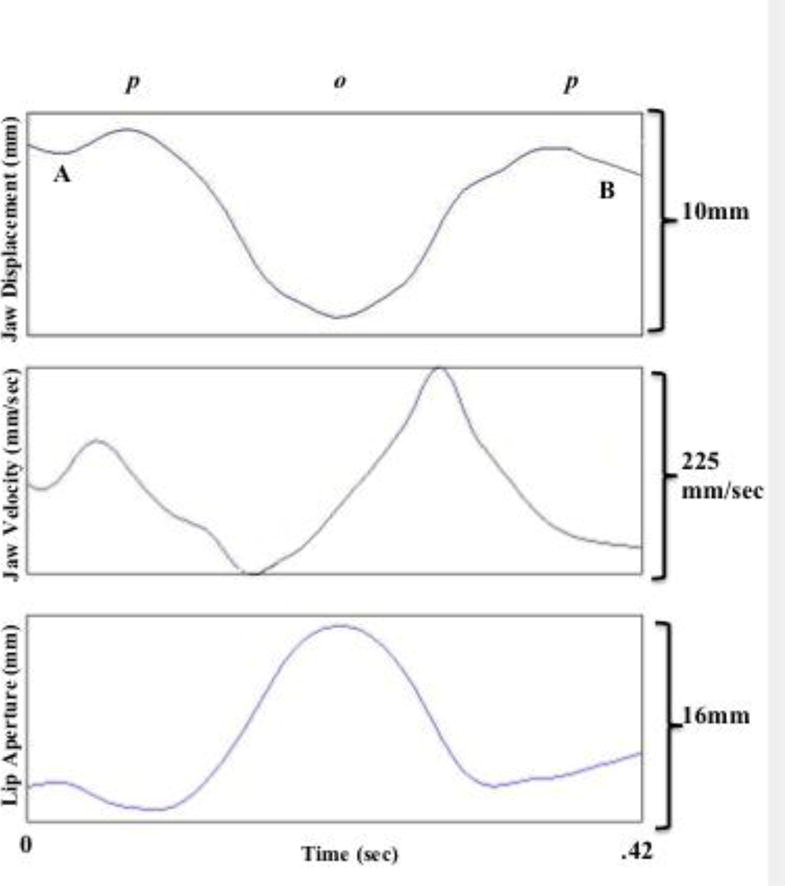
Kinematic traces of jaw displacement, jaw velocity and lip aperture corresponding to the utterance pop. Point A indicates the onset of movement in the jaw displacement trajectory and Point B marks the movement offset.
Spatiotemporal stability of jaw movement (jaw STI) was calculated using the spatiotemporal index (STI; Smith et al., 1995). To compute the STI, segmented displacement traces were normalized for amplitude and time. For each displacement trace, amplitude normalization was achieved by subtracting the mean of the displacement record and dividing by its standard deviation. Time normalization was achieved by using a cubic spline procedure to interpolate each waveform onto a time base of 1,000 points. The STI was then calculated to examine the stability of movement trajectories across repeated productions of target utterances. The STI was computed by calculating standard deviations at 2% intervals across repetitions of the time and amplitude normalized displacement traces. The STI is the cumulative sum of these 50 standard deviations and indicates the degree to which the set of trajectories converge onto one fundamental movement pattern (Smith, Johnson, McGillem & Goffman, 2000). Figure 2 displays normalized movement trajectories and STIs for a participant in each of the experimental groups.
Figure 2.

Normalized jaw movement trajectories and corresponding STIs associated with utterance puppypop produced by one participant each in the CAS, SD and TD groups.
Statistical Analysis
To measure the extent to which each of the outcome variables of interest differed across three groups (CAS, SD and TD) and different word lengths (one, two and three syllables), controlling for age effect, Analysis of Covariance with Repeated Measures was performed. The main effect of Group was treated as a between-subject effect and the main effect of Word Length was treated as a within-subject effect in this model. To control type-I error due to multiple pairwise comparisons, a post-hoc p-value adjustment (Tukey’s method) was conducted whenever applicable. Partial correlation analysis was used to quantify the correlation between various kinematic and transcription measures. The significance level of statistical tests is 5% unless otherwise mentioned. All statistical analyses were performed using SPSS version 20.
Results
Transcription measures were computed on 902 productions (CAS=312, SD=301, TD=289), which included both correct and incorrect productions of pop, puppet, puppypop. Kinematic measures were based only on accurate productions, which reduced the data pool to 648 utterances (CAS=190, SD=231, TD=227). As a result, the number of participants included in duration, jaw displacement, velocity and movement stability comparisons per token (pop, puppet, puppypop) was as follows: CAS (11, 10, 8), SD (11, 11, 9) and TD (11, 11, 10). The number of participants included in lip aperture comparisons was further reduced in the CAS group to 8 participants per token CAS (8, 8, 8).
Transcription
PCC, PVC and PWC were calculated for each participant from repeated productions of pop, puppet and puppypop. Mean PCC, PVC and PWC scores are shown in Table 3. High PCC, PVC and PWC scores reflect a greater percentage of consonant/vowel accuracy and consistency. As expected, consonant and vowel accuracy were lowest in the CAS group and highest in the TD group for all three tokens, with a significant between-subject effect of Group on PCC, F (2, 28) = 3.82, p = .034, η2 = 0.214 and PVC, F (2, 28) = 4.71, p = .017, η2 = 0.252. Post hoc tests revealed that PCC of the CAS group was significantly lower than both SD and TD groups, Mean differences = −12.14, p .039 and −14.58, p = .015, respectively. Similarly, PVC was significantly lower in the CAS group than SD and TD groups, Mean differences = −7.97, p = .032 and −10.43, p = .006, respectively. In contrast, PCC and PVC scores were not significantly different between the TD and SD groups. There was no significant within-subject effect of Word Length or Group by Word Length interaction for PCC and PVC. Further, there was no significant effect of age on PCC or PVC.
Table 3.
Mean (standard deviation) of Percentage of Consonants Correct (PCC), Percentage of Vowels Correct (PVC) and Percentage of Word Consistency (PWC)
| Measure | Group | pop | puppet | puppypop |
|---|---|---|---|---|
| PCC | CAS | 82.5 (15.9) | 88.3 (22.8) | 78.4 (33.1) |
| SD | 96.5 (4.2) | 97.6 (3.7) | 96.1 (7.7) | |
| TD | 98.9 (3.8) | 100 (0) | 98.5 (5.0) | |
| PVC | CAS | 89.3 (18.1) | 82.8 (27.9) | 86.0 (23.1) |
| SD | 94.4 (12.3) | 96.2 (7.3) | 97.7 (3.9) | |
| TD | 100 (0) | 100 (0) | 95.6 (9.9) | |
| PWC | CAS | 74.3 (15.4) | 76.5 (18.8) | 64.8 (23.8) |
| SD | 85.8 (14.0) | 82.8 (20.1) | 81.7 (21.7) | |
| TD | 97.7 (7.5) | 100 (0) | 88.6 (13.4) |
The CAS participants demonstrated the lowest PWC scores for all three tokens indicating that they produced a greater number of inconsistent errors than children in the other experimental groups. These observations were supported by a significant between-subject effect of Group on PWC, F (2, 28) = 11.45, p < .001, η2 = 0.45. Again, post hoc comparisons showed that PWC was significantly lower in the CAS than both SD and TD groups, mean difference = −10.38, p = .036 and −22.42, p < .001, as well as in the SD than TD group, mean difference = −12.04, p = .013. Similar to PCC and PVC, there was no significant within-subject effect of Word Length or Group by Word Length interaction. Finally, there was no significant effect of age on PWC.
Movement Kinematics
Movement Duration
Total movement duration was measured as the timing of jaw movement across the entire utterance and is displayed in Figure 3. As expected, duration increased with word length for all three experimental groups, resulting in a significant within-subject effect of Word Length on duration, F (2, 50) = 6.75, p < .01, η2 = 0.21. The effect of Group on movement duration did not reach statistical significance, F (2, 25) = 3.06, p =0.065, η2=0.197. Movement duration was longer for three syllable words than for one and two syllable words; the difference in duration was particularly prominent among the CAS and SD groups in comparison with the TD children. Movement duration associated with pop and puppet was longest for the SD participants, followed by the CAS then the TD children. In contrast, duration of puppypop was longest for the CAS group than the SD and TD groups. These observations were supported by a significant interaction between Group and Word Length, F (4, 50) = 2.875, p = .034, η2 = 0.19. The effect of age on movement duration was not significant.
Figure 3.
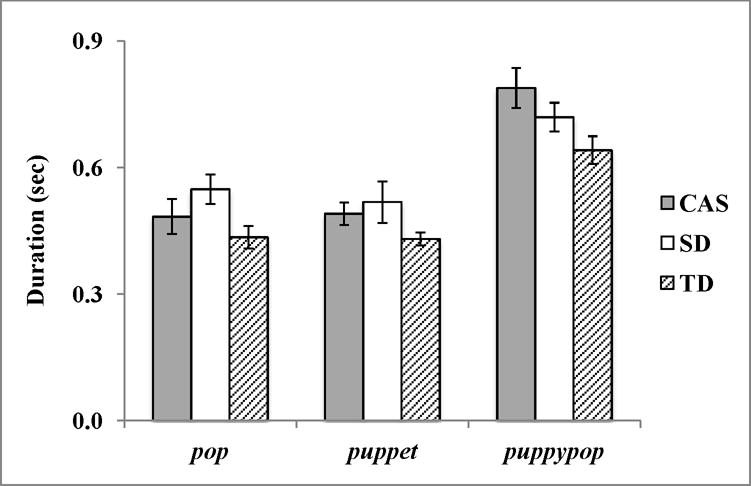
Mean total jaw movement duration and standard error associated with the production of pop, puppet and puppypop by participants in the CAS, SD and TD groups. Number of participants included per token (pop, puppet, puppypop) = CAS (11, 10, 8), SD (11, 11, 9) and TD (11, 11, 10).
Movement displacement
Average jaw displacement and lip aperture were calculated to examine the excursion of jaw and lip movement during the production of each word. Overall, jaw displacement and lip aperture were similar between the CAS, SD and TD groups. There was, however, a significant main effect of Word Length on jaw displacement, F (2, 50) = 3.541, p = .05, η2 = 0.101, and lip aperture, F (2, 48) = 3.567, p = .036, η2 = 0.129. The interaction between Group and Word Length was not significant. Across all three groups, when syllable number increased, movement excursion decreased. Post hoc testing showed that participants in all groups produced the shorter single syllable token pop with larger jaw and lip excursions as compared to the longer two and three syllable words puppet, mean difference in displacement = 6.21, p < .001; mean difference in lip aperture = 7.648, p < .001, and puppypop, mean difference in displacement = 6.88, p < .001; mean difference in lip aperture = 10.024, p < .001. Lastly, there was no significant effect of age on movement displacement or lip aperture. Figures 4a and 4b illustrate the findings for jaw displacement and lip aperture, respectively.
Figure 4.
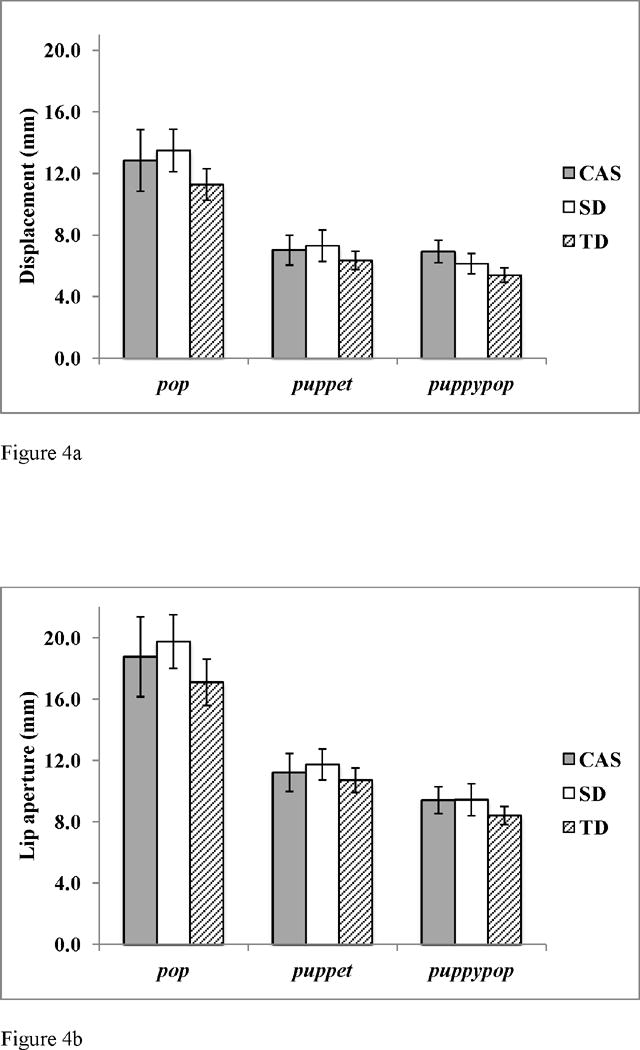
a: Mean average jaw displacement and standard error associated with the production of pop, puppet and puppypop by participants in the CAS, SD and TD groups. Number of participants included per token (pop, puppet, puppypop) = CAS (11, 10, 8), SD (11, 11, 9) and TD (11, 11, 10).
b: Mean average lip aperture and standard error associated with the production of pop, puppet and puppypop by participants in the CAS, SD and TD groups. Number of participants included per token (pop, puppet, puppypop) = CAS (8, 8, 8), SD (11, 11, 9) and TD (11, 11, 10).
Average Velocity
Average jaw movement velocity was calculated to examine the speed of jaw movement across word production. Similar velocity patterns were observed between children in the CAS, SD and TD groups for the three tokens. Thus, there were no significant main effects or interactions of Group or Word Length on average jaw velocity. The effect of age on velocity was not significant.
Movement stability
The spatiotemporal index (STI) was calculated to examine the stability of jaw movement trajectories across repeated productions of words. Mean STIs are shown in Figure 5. High STIs indicate greater spatiotemporal variability and low STIs represent more stability across movement trajectories. Jaw STIs were higher in the CAS group as compared to the SD and TD groups. This observation was supported by a significant between-subject effect of Group on jaw STI, F (2, 23) = 4.676, p < .05, η2=0.289. These findings indicate poorer spatiotemporal stability in the children with CAS than the children with SD and the TD controls. Post hoc comparisons revealed significantly higher jaw STIs in the CAS compared to the SD group, mean difference = 6.68; p = .006, and also the TD group, mean difference = 3.85; p = .03. There were no significant differences in jaw STIs between the SD and TD groups. The effect of age on movement stability was not significant.
Figure 5.
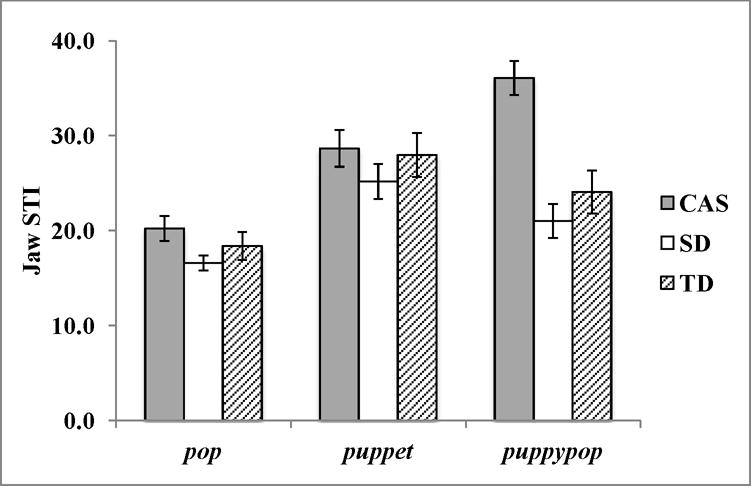
Mean jaw STI and standard error associated with the production of pop, puppet and puppypop by participants in the CAS, SD and TD groups. Number of participants included per token (pop, puppet, puppypop) = CAS (11, 10, 8), SD (11, 11, 9) and TD (11, 11, 10).
There was an influence of word length on movement stability, as STIs were lower for productions of pop as compared to puppet and puppypop. This finding was supported by a significant main effect of Word Length on STI, F (2, 46) = 5.424, p = .008, η2 = 0.191. Post hoc comparisons revealed significantly lower STIs for pop as compared to both puppet and puppypop, mean difference = −9.1 and −8.98, respectively, p < .001, but there was no significant difference between puppet and puppypop. As Figure 5 illustrates, STI values increased consistently from pop to puppet and to puppypop in the CAS group, suggesting a pattern of greater movement stability for shorter than longer words in the children with CAS. In contrast, STIs were higher in puppet than puppypop in the SD and TD participants. These findings were supported by a statistically significant interaction between Group and Word Length, F (4,46) = 6.852, p < .001, η2 = 0.373.
Relationship between transcription and kinematic measures
The relationship between indices of articulatory control (i.e., duration, stability) and measures reflective of speech intelligibility (i.e., PCC, PVC, PWC) were examined by computing Pearson partial correlations between these kinematic and transcription parameters while controlling for subjects’ age. Seven pairwise comparisons were made for each experimental group: PCC and STI, PVC and STI, PWC and STI, PCC and Duration, PVC and Duration, PWC and Duration, as well as Duration and STI, which adjusted the alpha level to .01. A significant positive correlation was found between PCC and Duration, r = .54, p < .01, among the CAS participants but not the SD or TD children. Correlations between PCC, PVC and STI were not significant in the CAS, SD or TD groups. There were no significant correlations between PWC and STI or Duration. Lastly, a significant positive correlation was found between Duration and STI in the children with CAS, r = .53, p < .01, but not the SD or TD groups.
Discussion
Temporal and spatial control in speech impaired children
The current study investigated articulatory control in children with CAS and SD, as well as participants with typically developing speech and language skills (TD), during the production of words that increased in length. We hypothesized that movement duration, displacement, velocity and variability would distinguish groups during accurate speech production. Our results partially supported these predictions and revealed that children in the CAS, SD and TD groups were differentiated by movement duration and variability. Regarding duration, both groups of speech-impaired children (CAS & SD) produced longer jaw movement durations than children in the TD group (across all three tokens). This result is consistent with research reporting longer acoustic durations in children with CAS than TD controls (Nijland et al., 2003a, Bahr, 2005). In addition, past work conducted in our laboratory (Grigos & Kolenda, 2010) revealed decreases in movement duration as a child with CAS produced words accurately and consistently over an eight-month period. The authors proposed that longer movement durations may have facilitated improved speech output. Although speaking rate was not directly measured in our present or past work, the movement duration findings from these experiments suggest that children with speech sound disorders may be reducing speaking rate as they achieve accurate speech. Reducing speech rate may allow these speakers to glean information derived from auditory feedback more easily (Terband & Maassen, 2010). Interestingly, longer movement durations have also been reported for children with specific language impairment (SLI) than TD controls (Goffman, 1999; 2004), a result that leaves us questioning whether increased duration represents a characteristic of children with speech and language impairment in general. Taken together, the findings above illustrate the need for additional research to examine whether differences in acoustic and kinematic timing between TD and speech/language impaired children reflect poor speech motor control or are adaptive strategies that support improved communication.
To further explore temporal patterns displayed by the children with CAS and SD, we examined the relationship between transcription and kinematic measures. PCCs (obtained from correct and incorrect productions) were significantly correlated with movement duration (obtained from correct productions) in the CAS group but not in the SD group, suggesting that increased duration facilitated segmental accuracy in the children with CAS. Severity of impairment and task demands are two factors that may have impacted these results. Formal and informal assessment revealed more speech errors in the CAS than SD children. Similarly, the transcription findings from the experimental task showed that the CAS and SD children were challenged to varying degrees. The children with CAS displayed lower PCCs on pop, puppet and puppypop than the SD group who performed close to ceiling (mean PCCs > 95), as is shown in Table 3. Further, the number and range of segmental errors produced by children in the CAS group were particularly striking given that all phonemes included in the tokens were early developing, were within each participant’s phonetic repertoire and were embedded within simple syllable structures. Thus, longer movement durations may have aided the children with CAS who displayed more severe speech deficits than children in the SD group. It is possible that the relationship between Duration and PCC would have been stronger in the SD group if the tokens included a wider range of phonemes within more complex syllable structures.
Interpretation of the temporal findings would not be complete without consideration of developmental changes in duration. Speech motor development in TD children is characterized by decreased movement duration with age (Goffman & Smith, 1999; Grigos & Patel, 2007; 2010; Smith & Goffman, 1998;). Given the participant age range in the present work (i.e. the TD controls were on average seven months older than the children with CAS), we considered the possibility that duration differences between the CAS and TD groups reflected this age difference. We do not believe that this is the case for several reasons. First, the SD children also produced longer movement durations as compared to the TD group and these groups (SD and TD) were more similar in mean age as compared with the CAS group. Second, there was no statistically significant effect of age on movement duration. Still, while age may not have contributed to group differences, it is possible that children with CAS represent a subset of less mature speakers. These children may not have had the same practice and feedback exposure as children of similar ages. To further investigate whether children with CAS display speech motor patterns that mirror those of less mature speakers, future studies should include a comparison group of younger TD children.
In contrast to the results for temporal control, there were no group differences in movement displacement. A significant length effect was found where all children produced the single syllable word pop with greater jaw and lip excursion than the longer words puppet and puppypop. These displacement findings appear to be confounded by vowel height where larger displacements associated with pop reflect the larger jaw openings required to produce the low-back vowel /a/. Although our dataset cannot rule out the vowel height effect on our displacement results (as measures of average displacement across the word were obtained), the fact that the relationship between displacement and stability changed with the articulatory challenges presented by the stimuli (whether vowel height or length) supports earlier research linking stability and displacement. The SD and TD groups produced puppypop with smaller displacements and a similar degree of movement stability relative to pop. Displacement decreased with word length in the CAS group as movement stability also decreased (i.e., higher STIs). Several researchers have suggested that increased amplitude may result in greater movement stability (Terband et al., 2011; Van Lieshout et al., 2002; 2007). Terband et al. (2011) proposed that amplitude adjustments assisted children with CAS to achieve STIs that were similar to the control participants. While we did not find group differences in displacement similar to those reported by Terband et al. (2011), this may be a result of task differences. We examined the production of real-words that increased in length where the longer words included vowels that varied in height and backness. In contrast, Terband et al. (2011) studied speech production within a reiterative speech task, where the stimuli included one vowel type. In relation to the present work, it is plausible that children with CAS may not have the refined motor skill necessary to modify displacement during challenging speaking tasks. In contrast, children with more mature speech motor skills, such as the participants in the TD and SD groups, may not need to increase movement displacement when producing multisyllabic words or words that include vowels of various heights. Given the task specific nature of speech motor control, understanding how task demands influence articulatory control is essential to unveiling deviant speech motor processes in CAS. This is discussed in greater detail below.
Poor movement stability in CAS
We hypothesized that children with CAS would produce more variable articulator movements than participants in the SD and TD groups during accurate word productions. Our findings supported this prediction as children with CAS produced targets with higher jaw STIs than children in the SD and TD groups, which is consistent with the notion that CAS is characterized by a higher degree of movement variability relative to children with an articulation and phonological impairment. The observation that children in the SD group had significantly lower STIs than participants in the CAS group suggests that they have more stable motor plans.
STI differences related to word length were only observed in the CAS group. As word length increased, jaw STIs increased in the CAS group. While the children with CAS accurately produced the longer three-syllable target, they did so with more variable articulator movements, reflecting poor movement stability. This result supports our previous findings, which showed that coordinative consistency differed between children with CAS and SD as measured by lip aperture STI (Moss & Grigos, 2012) and is consistent with research that has associated increased variability with CAS. Such studies involving children with CAS have identified high within subject variability of second formant values (Nijland et al., 2003a), decreased jaw movement variability as speech accuracy increased (Grigos & Kolenda, 2010), as well as high tongue tip movement variability (Terband et al., 2011). We also considered the average age difference (seven months) between the children with CAS as compared to the SD and TD groups in our interpretation of the current STI findings. Although it is well documented that movement stability increases with age in children (Green, Moore & Reilly, 2002; Grigos, 2009; Grigos, Saxman & Gordon, 2005; Sharkey & Folkins, 1985; Smith, Goffman & Stark, 1995; Smith & McLean-Muse, 1986; Watkin and Fromm, 1984), there was no statistically significant effect of age on STI in the current study. As mentioned above in regards to duration, future studies examining speech motor control in CAS should add a control group of younger typically developing children to investigate the importance of speaker experience and maturation. Given that the behavioral symptoms characteristic of CAS are not typical of less mature speakers (e.g., articulatory groping, inconsistent productions of the same word, prosodic errors.), we would anticipate that children with CAS would display different speech motor patterns from younger TD children. Additional research is warranted to examine this prediction in a larger cohort of children with CAS, as compared to age matched and younger TD controls.
Lastly, within group differences, and the potential impact of missing data, should be acknowledged when interpreting STI and duration findings. As noted above, data from three children with CAS (CAS2, CAS3, CAS6) were not included in all kinematic analyses, as they did not achieve accurate productions of puppet (CAS 2) and/or puppypop (CAS2, CAS3, CAS6). Their speech profiles (Tables 1 & 2) showed that they were among the more impaired children with CAS as they performed either at the midpoint or bottom half of the CAS group in terms of the number of speech characteristics they displayed, as well as on indices of connected speech accuracy (i.e. PCC and WWC). These participants were also in the younger half of their cohort (under five years of age). In contrast, speech profiles from the two SD participants with missing kinematic data for puppypop (SD1, SD11) differed in severity and these children were the youngest (SD1) and oldest (SD11) participants in the SD group. These results highlight some of challenges researchers contend with when studying speech motor control in speech-impaired children. It can be difficult to account for severity of impairment, the characteristics displayed by participants within the same diagnostic category, as well as for overlap in the diagnostic profiles of children who may clearly classify as CAS or SD. Further, researchers interested in examining speech motor control during accurate speech in children are faced with the task of collecting an adequate amount of interpretable data from experiments that tax the motor and linguistic systems. While we are cautious in over-interpreting the impact that these missing data may have had on our findings, we are left speculating whether group differences for duration and STI may have been even more distinct if these more severely impaired CAS participants were included in all analyses.
Influence of task demands on speech motor control in CAS
We predicted that increasing linguistic complexity, by increasing word length, would differentially impact articulator movement across groups. Our results for duration and movement stability lend support to this hypothesis, illustrating that the motor commands that underlie speech are shaped by task demands. As expected, increasing word length resulted in increased duration across all groups. This finding illustrates the challenge in producing a longer word, as has been documented in the literature (Sadagopan & Smith, 2008; Sasisekaran, Smith, Sadagopan & Weber-Fox, 2010; Walsh et al., 2006), as well as the increased time required to produce two and three-syllable tokens. Interestingly, the groups altered duration in different ways in response to task demands. The SD children displayed longer durations for one and two syllable words, as compared to the CAS and TD children. Children with CAS exhibited longer durations for three syllable words than the SD and TD participants. These findings may reflect a point of breakdown for the children with CAS between the production of two and three syllable words. Similarly, a significant increase in jaw STI between two and three syllable words was observed in the children with CAS but not in the SD and TD groups. The positive relationship between STI and duration in the CAS group suggests that strategies, such as increasing movement duration, may aide children with less stable speech motor skills to achieve accurate speech. From a clinical standpoint, the high degree of movement variability, seen during accurate productions of longer words by CAS children in the present work, may be related to the inconsistent errors that are characteristic of this population. We are also left wondering whether reduced stability of articulatory control may underlie the difficulties children with CAS have maintaining treatment gains and in generalizing phonemes across speaking contexts. Longitudinal studies of speech motor control in children with CAS are needed to reveal whether mature speech motor patterns emerge over time and to determine whether increased stability of articulatory control precedes maintenance of accurate speech.
Just as utterance length may impact performance and lead to speech breakdowns, children with CAS may utilize simple word structures to compensate for their motor deficits. Similarly, children with cleft palate were shown to avoid words that begin with phonemes that are difficult to produce, a strategy that also impacted their lexical development (Estrem & Broen, 1989; Willadsen, 2013). If children with CAS avoid more difficult productions, the consequences would be seen in their expressive output and potentially in their expressive competence. Consistent with this notion, the children with CAS in the present work demonstrated poorer performance on the expressive language portion of the TELD-2 than children in the SD and TD groups. Although the CAS children were also determined to have age appropriate receptive language skills based upon assessment with the TELD-2, this tool is a broad based language assessment and may not capture specific language deficits. Without a more comprehensive analysis of language performance, it is difficult to establish whether language factors may have contributed to speech motor performance in the children with CAS studied. In light of the evidence that children with SLI display deficits in articulatory control that are similar to those seen in the children with CAS in the present work (Goffman, 1999; 2004), future studies are needed to elucidate the complex relationship between speech and language in children with communication impairments.
Taken together, our findings illustrate the challenges in isolating a level of breakdown in speech motor processing in CAS. For instance, differences in temporal control between the speech impaired (CAS & SD) and TD children suggest problems at the motor programming level of speech processing in CAS and SD. Thus, the CAS and SD children may both have difficulty specifying temporal movement parameters. When these findings are viewed in relation to task demands, the children with CAS may also have difficulty adapting the motor plan to adjust to contextual factors. All groups were influenced by the demands placed on them as word length increased; however, the children with CAS displayed more deviant speech motor patterns when they produced three syllable words. Our findings support the claim that movement variability distinguishes children with CAS from speakers with SD, particularly as task demands increase. There are additional challenges placed on the speech production mechanism by anatomical and physiological maturation, as well as cognitive and linguistic development; the contribution of these factors to speech motor development in CAS warrants further exploration. In sum, these results support the shift towards exploring the interactional nature of development to fully understand speech motor processing in children with speech sound disorders (Maassen et al. 2010).
Conclusion
Although the nature of motor control deficits in CAS continues to be debated, a profile of the speech motor skills in CAS has begun to emerge, which is characterized most notably by increased variability. Our study also provides evidence that children with CAS and SD are impacted by task demands to different extents. This was most apparent in the high STIs seen in the CAS group in the production of longer words. While the children with CAS produced these words accurately, they used a less consistent motor plan to do so. We interpret this finding to suggest that speech motor deficits may underlie the speech production difficulties characteristic of CAS and may play a role in the challenges children with CAS display in achieving and maintaining accurate speech. Future research is warranted to develop an understanding of the source of such variability, as well as to explore whether speech motor processes are refined in response to intervention. The interaction between linguistic and motor factors in CAS also warrants further investigation in which semantic, syntactic and phonologic complexity are modified. Additional work in this area can further quantify speech motor performance in CAS which can contribute to the classification of speech production impairments overall.
Acknowledgments
This research was supported by a grant (R03DC009079) from the National Institute on Deafness and Other Communicative Disorders. The authors would like to acknowledge Julie Case, Hailey Small, Panagiota Tampakis, Penelope Elias and Jessica Storer for assistance with data collection and processing. We are grateful to the participants and their families for their cooperation and dedication to the project.
Footnotes
Inconsistent errors were identified in two speaking contexts, connected speech and the sequencing task, as repeated word productions were not obtained from the GFTA-2.
This is an author-produced manuscript that has been peer reviewed and accepted for publication in the Journal of Speech, Language, and Hearing Research (JSLHR). As the “Just Accepted” version of the manuscript, it has not yet undergone copyediting, proofreading, or other quality controls associated with final published articles. As the publisher and copyright holder, the American Speech-Language-Hearing Association (ASHA) disclaims any liability resulting from use of inaccurate or misleading data or information contained herein. Further, the authors have disclosed that permission has been obtained for use of any copyrighted material and that, if applicable, conflicts of interest have been noted in the manuscript.
References
- ASHA. Childhood Apraxia of Speech: Technical Report. American Speech-Language-Hearing Association; 2007. [Google Scholar]
- Bahr RH. Bahr 2005, Differential diagnosis of severe speech disorders using speech gestures. Topics in Language Disorders. 2005;25(3):254–265. [Google Scholar]
- Burgmeister B, Blum L, Lorge I. Columbia Mental Maturity Scale. The Psychological Corporation; 1972. [Google Scholar]
- Case J, Moss A, Grigos MI. Measuring error consistency in children with apraxia of speech; Poster presentation at the annual convention of the American Speech Language and Hearing Association; Atlanta, GA. 2012. [Google Scholar]
- Estrem T, Broen PA. Early speech productions of children with cleft palate. Journal of Speech, Language and Hearing Research. 1989;32:12–23. doi: 10.1044/jshr.3201.12. [DOI] [PubMed] [Google Scholar]
- Goffman L. Prosodic influences on speech production in children with specific language impairment and speech deficits: kinematic, acoustic, and transcription evidence. Journal of Speech, Language and Hearing Research. 1999;42(6):1499–517. doi: 10.1044/jslhr.4206.1499. [DOI] [PubMed] [Google Scholar]
- Goffman L. Kinematic differentiation of prosodic categories in normal and disordered language development. Journal of Speech, Language and Hearing Research. 2004;47(5):1088–102. doi: 10.1044/1092-4388(2004/081). [DOI] [PubMed] [Google Scholar]
- Goffman L, Smith A. Development and phonetic differentiation of speech movement patterns. Journal of Experimental Psychology: Human Perception and Performance. 1999;25(3):649–660. doi: 10.1037//0096-1523.25.3.649. [DOI] [PubMed] [Google Scholar]
- Goldman R, Fristoe M. Goldman-Fristoe Test of Articulation-2. Circle Pines, MN: American Guidance Service, Inc; 2000. [Google Scholar]
- Green JR, Moore CA, Higashikawa M, Steeve RW. The physiologic development of speech motor control: lip and jaw coordination. Journal of Speech, Language and Hearing Research. 2000;43:239–55. doi: 10.1044/jslhr.4301.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green JR, Moore CA, Reilly KJ. The sequential development of jaw and lip control for speech. Journal of Speech, Language and Hearing Research. 2002;45:66–79. doi: 10.1044/1092-4388(2002/005). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green JR, Wilson EM, Wang Y, Moore CA. Estimating mandibular motion based on chin surface targets during speech. Journal of Speech, Language and Hearing Research. 2007;50:928–939. doi: 10.1044/1092-4388(2007/066). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grigos MI. Changes in articulator movement variability during phonemic development: a longitudinal study. Journal of Speech, Language and Hearing Research. 2009;52(1):164–177. doi: 10.1044/1092-4388(2008/07-0220). [DOI] [PubMed] [Google Scholar]
- Grigos MI, Kolenda N. The relationship between articulatory control and improved phonemic accuracy in childhood apraxia of speech: a longitudinal case study. Clinical Linguistics and Phonetics. 2010;24(1):17–40. doi: 10.3109/02699200903329793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grigos MI, Patel R. Development of articulatory control of sentential focus in children. Journal of Phonetics. 2010;39:706–715. [Google Scholar]
- Grigos MI, Patel R. Articulator movement associated with the development of prosodic control in children. Journal of Speech, Language and Hearing Research. 2007;50:1–18. doi: 10.1044/1092-4388(2007/010). [DOI] [PubMed] [Google Scholar]
- Grigos MI, Saxman JH, Gordon AM. Speech motor development during acquisition of the voicing contrast. Journal of Speech, Language, and Hearing Research. 2005;48(4):739–752. doi: 10.1044/1092-4388(2005/051). [DOI] [PubMed] [Google Scholar]
- Hayden DA, Square PA. VMPAC: Verbal Motor Production Assessment for Children. San Antonio: Psychological Association; 1999. [Google Scholar]
- Hodson BW, Paden EP. Phonological processes which characterize intelligible and unintelligible speech in early childhood. Journal of Speech and Hearing Disorders. 1981;46:369–373. [Google Scholar]
- Hresko W, Reid D, Hammill D. Test of Early Language Development. Austin, TX: Pearson Assessment; 2007. [Google Scholar]
- Ingram D, Ingram KD. A Whole-Word Approach to Phonological Analysis and Intervention. Language, Speech and Hearing Services in Schools. 2001;32:271–283. doi: 10.1044/0161-1461(2001/024). [DOI] [PubMed] [Google Scholar]
- Math Works. MATLAB Version 7.2. [computer software] Natick, MA: 2007. [Google Scholar]
- Maassen B, Nijland L, Terband H. Developmental models of childhood apraxia of speech. In: Maassen B, Van Lieshout P, editors. Speech Motor Control: New Developments in Basic and Applied Research. Oxford: Oxford University Press; 2010. [Google Scholar]
- McReynolds LV, Elbert ME. Criteria for Phonological Process Analysis. Journal of Speech and Hearing Disorders. 1981;46:197–204. doi: 10.1044/jshd.4602.197. [DOI] [PubMed] [Google Scholar]
- Moss A, Grigos MI. Interarticulatory coordination of the lips and jaw in childhood apraxia of speech. Journal of Medical Speech Language Pathology. 2012;20(4):127–132. [PMC free article] [PubMed] [Google Scholar]
- Nijland L, Maassen B, van der Meulen S, Gabreels F, Kraaimaat FW, Schreuder R. Coarticulation patterns in children with developmental apraxia of speech. Clinical Linguistics & Phonetics. 2002;16(6):461–83. doi: 10.1080/02699200210159103. [DOI] [PubMed] [Google Scholar]
- Nijland L, Maassen B, van der Meulen S, Gabreels F, Kraaimaat FW, Schreuder R. Planning of syllables in children with developmental apraxia of speech. Clinical Linguistics and Phonetics. 2003a;17(1):1–24. doi: 10.1080/0269920021000050662. [DOI] [PubMed] [Google Scholar]
- Nijland L, Maassen B, van der Meulen S. Evidence of motor programming deficits in children diagnosed with CAS. Journal of Speech, Language and Hearing Research. 2003b;46(2):437–50. doi: 10.1044/1092-4388(2003/036). [DOI] [PubMed] [Google Scholar]
- Nip ISB, Green JR, Marx DB. Early speech motor development: Cognitive and linguistic considerations. Journal of Communication Disorders. 2009;42:286–298. doi: 10.1016/j.jcomdis.2009.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sadagopan N, Smith A. Developmental changes in the effects of utterance length and complexity on speech movement variability. Journal of Speech, Language & Hearing Research. 2008;51(5):1138–1151. doi: 10.1044/1092-4388(2008/06-0222). [DOI] [PubMed] [Google Scholar]
- Sasisekaran J, Smith A, Sadagopan N, Weber-Fox C. Nonword repetition in children and adults: Effects on movement coordination. Developmental Science. 2010;13(3):521–532. doi: 10.1111/j.1467-7687.2009.00911.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmitt LS, Howard BH, Schmitt JF. Conversational Speech Sampling in the Assessment of Articulation Proficiency. Language, Speech and Hearing Services in Schools. 1983;14:210–214. [Google Scholar]
- Sharkey SG, Folkins JW. Variability of lip and jaw movements in children and adults: implications for the development of speech motor control. Journal of Speech and Hearing Research. 1985;28(1):8–15. doi: 10.1044/jshr.2801.08. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Austin D, Lewis B, McSweeny J, Wilson D. The percentage of consonants correct (PCC) metric: Extensions and reliability data. Journal of Speech, Language, and Hearing Research. 1997;40:708–722. doi: 10.1044/jslhr.4004.708. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Campbell TF, Karlsson HB, Brown RL, McSweeny JL, Nadler CJ. A diagnostic marker for childhood apraxia of speech: the lexical stress ratio. Clinical Linguistics & Phonetics. 2003a;17(7):549–574. doi: 10.1080/0269920031000138123. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Green JR, Campbell TF, McSweeny JL, Scheer AR. A diagnostic marker for childhood apraxia of speech: the coefficient of variation ratio. Clinical Linguistics and Phonetics. 2003b;17(7):575–95. doi: 10.1080/0269920031000138141. [DOI] [PubMed] [Google Scholar]
- Skinder A, Strand EA, Mignerey M. Perceptual and acoustic analysis of lexical and sentential stress in children with developmental apraxia of speech. Journal of Medical Speech-Language Pathology. 1999;7(2):133–144. [Google Scholar]
- Smit AB, Hand L, Freilinger JJ, Bernthal JE, Bird A. The Iowa articulation norms project and its Nebraska replication. Journal of Speech & Hearing Disorders. 1990;55(4):779. doi: 10.1044/jshd.5504.779. [DOI] [PubMed] [Google Scholar]
- Smith A, Goffman L. Stability and patterning of speech movement sequences in children and adults. Journal of Speech, Language and Hearing Research. 1998;41:18–30. doi: 10.1044/jslhr.4101.18. [DOI] [PubMed] [Google Scholar]
- Smith A, Goffman L, Stark R. Speech motor development. Seminars in Speech and Language. 1995;16(2):87–98. doi: 10.1055/s-2008-1064112. [DOI] [PubMed] [Google Scholar]
- Smith A, Goffman L, Zelaznik HN, Ying G, McGillem C. Spatiotemporal stability and patterning of speech movement sequences. Experimental Brain Research. 1995;104(3):493–501. doi: 10.1007/BF00231983. [DOI] [PubMed] [Google Scholar]
- Smith A, Johnson M, McGillem C, Goffman L. On the assessment of stability and patterning of speech movements. Journal of Speech, Language and Hearing Research. 2000;43:277–286. doi: 10.1044/jslhr.4301.277. [DOI] [PubMed] [Google Scholar]
- Smith BL, McLean-Muse A. Articulatory movement characteristics of labial consonant productions by children and adults. Journal of the Acoustical Society of America. 1986;80(5):1321–1328. doi: 10.1121/1.394383. [DOI] [PubMed] [Google Scholar]
- Terband H, Maassen B. Speech Motor Development in Childhood Apraxia of Speech: Generating Testable Hypotheses by Neurocomputational Modeling. Folia Phoniatrica et Logopaedica. 2010;62:134–142. doi: 10.1159/000287212. [DOI] [PubMed] [Google Scholar]
- Terband H, Maassen B, Guenther FH, Brumberg J. Computational Neural Modeling of Speech Motor Control in Childhood Apraxia of Speech (CAS) Journal of Speech, Language, and Hearing Research. 2009;52:1595–1609. doi: 10.1044/1092-4388(2009/07-0283). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terband H, Maassen B, Van Lieshout P, Nijland L. Stability and composition of functional synergies for speech movements in children with developmental speech disorders. Journal of Communication Disorders. 2011;44(1):59–74. doi: 10.1016/j.jcomdis.2010.07.003. [DOI] [PubMed] [Google Scholar]
- Terband H, Zaalen Y, Maassen B. Lateral jaw stability in adults, children and children with developmental speech disorders. Journal of Medical Speech Langauge Pathology. 2012;20(4):112–120. [Google Scholar]
- Van Lieshout PHHM, Bose A, Square PA, Steele CM. Speech motor control in fluent and dysfluent speech production of an individual with apraxia of speech and Broca’s aphasia. Clinical Linguistics and Phonetics. 2007;21(3):159–188. doi: 10.1080/02699200600812331. [DOI] [PubMed] [Google Scholar]
- Van Lieshout PHHM, Rutjens CAW, Spauwen PMH. The Dynamics of Interlip Coupling in Speakers With a Repaired Unilateral Cleft-Lip History. Journal of Speech, Language, and Hearing Research. 2002;45:5–19. doi: 10.1044/1092-4388(2002/001). [DOI] [PubMed] [Google Scholar]
- Vicon Motion Systems. Vicon 460 [computer software] Los Angeles, California: 2001. [Google Scholar]
- Walsh B, Smith A, Weber-Fox C. Short-term plasticity in children’s speech motor systems. Developmental Psychobiology. 2006;48(8):660–674. doi: 10.1002/dev.20185. [DOI] [PubMed] [Google Scholar]
- Watkin KL, Fromm D. Labial coordination in children: Preliminary considerations. Journal of the Acoustical Society of America. 1984;75(2):629–632. doi: 10.1121/1.390494. [DOI] [PubMed] [Google Scholar]
- Willadsen E. Lexical selectivity in Danish toddlers with cleft palate. Cleft Palate Craniofacial Journal. 2013;50(4):456–65. doi: 10.1597/11-022. [DOI] [PubMed] [Google Scholar]