

Abstract
Objective
This study was designed to determine whether Black adolescents from disadvantaged backgrounds who have an unrelenting determination to succeed, would, as adults, show “skin-deep resilience” by faring well in psychosocial domains but also show a heightened chance of having a chronic disease, specifically type 2 diabetes.
Methods
Secondary data analyses were executed using Waves 1 and 4 of the United States Longitudinal Study of Adolescent and Adult Health (Add Health). At Wave 1, when participants were age 16, data were obtained on a behavioral style termed striving. Striving includes high aspirations, unwavering persistence, investment in education, and avoidance of activities that sidetrack success. At Wave 4, when participants were age 29, college graduation, personal income, symptoms of depression, and type 2 diabetes status were assessed.
Results
Black and non-Hispanic White youth who displayed striving during adolescence evinced, at age 29, a higher likelihood of college graduation, greater personal income, and fewer symptoms of depression than did non-strivers. Among Black participants, the findings were consistent with the “skin-deep resilience” pattern for type 2 diabetes. High-striving Black adolescents in the most disadvantaged families had a greater likelihood of developing type 2 diabetes during adulthood than did similar high-striving Black adolescents living in more privileged families. The skin-deep resilience pattern did not emerge among non-Hispanic White participants.
Conclusions
This study is the first to show that an unrelenting determination to succeed among Black adolescents from disadvantaged backgrounds forecasts an elevated risk of developing type 2 diabetes during adulthood.
A remarkable number of Black children and adolescents who experience a lifetime of exposure to economic hardship evince high levels of psychosocial competence that include planful self-regulation, academic achievement, and avoidance of behavioral or emotional problems.1 These children have been called resilient because their competence develops in the face of contextual adversity, enabling them to “beat the odds.” The pediatric resilience literature is characterized by the widespread assumption that, if children and youth who face major adversities are doing well by outward appearances—for example, if they excel academically and evince high levels of self-esteem—they have successfully negotiated those adversities. As interest in resilience has surged, a parallel literature has been developing; this literature suggests that, for low-SES Black youth, striving for success may act as a “double-edged sword,” facilitating academic success and psychosocial adjustment while undermining physical health. The first hints of this pattern came from a longitudinal study of African American youth growing up in rural areas in the southern portion of the United States.2 Most came from families who were working poor. A subgroup of resilient youth were identified at age 11, and at age 19 indicators of mental and physical health were assessed. Those who came from disadvantaged backgrounds but evinced high levels of academic success and self-control at age 11 also had few problems with aggression, conduct problems, or drug use at age 19. When indicators of physical health were examined, however, these psychosocially resilient young people from disadvantaged backgrounds were not faring well. Compared with rural African American youth from more advantaged family backgrounds, they produced more stress hormones (cortisol, epinephrine, norepinephrine), had higher blood pressure, and were more obese. Similar results emerged from a subsequent analysis of the same sample. These youth had attained academic success—they had graduated from high school and were attending college—despite coming from challenging neighborhoods with concentrated poverty. These youth were less likely to use drugs at age 20 years than were other participants. Despite their academic success, these youth showed poorer cardiometabolic health at age 20 years, as reflected in elevated stress hormones, blood pressure, and obesity, than did rural African American youth who were also attending college but who grew up in neighborhoods with lower poverty levels.3 The same pattern emerged again with a different longitudinal sample of rural African American youth who were followed from ages 17 to 22 years.4 Among all adolescents, planful self-control forecast better psychosocial outcomes, including less depression, drug use, and aggression. It also forecast, however, more rapid epigenetic aging of immune cells among Black youth from disadvantaged, but not from more advantaged, backgrounds. Together, these findings suggest that, for Black youth from disadvantaged backgrounds, resilience may be only “skin deep.”
These findings on skin-deep resilience raise several questions. First, because all of the data gathered thus farcome from studies of Black youth in the rural South, it is unclear whether the pattern is specific to these residents or is indicative of a more general phenomenon that crosses demographic and geographical lines. Second, the existing studies have used biomarkers to index health. Although biomarkers are useful as indicators of risk, they do not actually reflect disease. In this study, we examined the skin-deep resilience pattern to determine whether it would forecast a chronic disease—type 2 diabetes—which is prevalent in racial/ethnic minority populations and among persons living in economically disadvantaged circumstances.5 To address these questions, we conducted secondary analyses of data from Waves 1 and 4 of the U. S. National Longitudinal Study of Adolescent to Adult Health (Add Health). At Wave 1, adolescents completed extensive psychosocial assessments. From these data, a behavioral style common to resilient youth from disadvantaged circumstances was assessed.1 This style, termed striving, features the setting of high educational aspirations, determination and persistence in attaining goals, investment in school work, and avoidance of activities that could sidetrack goals and aspirations. Using these data, we asked whether the skin-deep resilience pattern would extend to a diverse national population and manifest an association with type 2 diabetes at the Wave 4 assessment, when the participants were adults.
Methods
Sample
The data were drawn from Waves 1 and 4 of the National Longitudinal Study of Adolescent Health (Add Health), a nationally representative sample of adolescents in grades 7 through 12 in the United States in 1995. The survey design has been described extensively elsewhere.6 Wave 1 (1994-1995) included 20,745 adolescents ages 11 to 20 years. The most recent wave of data collection (Wave 4) included 14,800participants (71% of the original sample), when respondents were 24 to 32 years of age. The analytic sample for this study constrained the ages of the study participants so that they were 15 to 17 years of age at Wave 1 and 29 to 31 years of age at Wave 4. This sample included 5366 individuals who self-identified as Black (n = 1431) or as White with no Hispanic heritage (n = 3935) and had complete data on all study variables at Waves 1 and 4. The mean ages of the target youth were 16.44 years (SD = 0.85) at Wave 1 and 29.32 years (SD = 0.91) at Wave 4. This sample included 47.9% male, 52.1% female, 26.7% Black, and 73.3% White participants. Compared with the study sample, participants at Wave 1 were less likely to live in poverty (17.2% vs. 15.2%), to receive public assistance (10.0% vs. 7.8%), or to have an unemployed primary caregiver (10.8% vs. 7.8%).
Measures
All questions in Add Health were constructed to meet the goals of the that study and were not drawn from existing measures.
Race
At Wave 1, adolescents reported their race/ethnicity. A dichotomous variable was created to assess Black (1) or White (0) ethnicity. Multiracial respondents were classified by their first choice of racial/ethnic category.
Gender
Gender was coded as male (1) or female (0).
Adolescent Disadvantage and Striving
Data on SES-related disadvantage and striving were collected at Wave 1 of Add Health. Table 1 presents the items used for each of the measures. Six standard indicators of SES-related disadvantage were assessed, with each risk factor scored dichotomously (0 if absent, 1 if present; Table 1, top; see 2, 7). Disadvantage was defined as the sum of the risk factors at the Wave 1 assessment. The resulting index ranged from 0 to 4, with 4 representing the presence of 4, 5, or 6 indicators (M = 0.87, SD = 1.13).
Table 1. Indicators of SES-related Disadvantage and Striving.
| Indicators | Description of composite variable | Response |
|---|---|---|
| SES-related Disadvantage | ||
| Family poverty | Family income below the poverty line | 0 = no; 1 = yes |
| Parental education | Either mother' or father' education level less than high school graduation | 0 = no; 1 = yes |
| Parental employment | Both parents were unemployed | 0 = no; 1 = yes |
| Single parent status | PC was single/never married, widowed, divorced, or separated | 0 = no; 1 = yes |
| Receipt of public assistance | Either parent received public assistance | 0 = no; 1 = yes |
| Economic hardship | PC reported not having enough money to pay bills | 0 = no; 1 = yes |
| Striving | ||
| Educational aspirations (items were averaged; median = 5) | On a scale of 1 to 5, where 1 is low and 5 is high, how much do you want to go to college? On a scale of 1 to 5, where 1 is low and 5 is high, how likely is it that you will go to college? |
1 = low to 5 = high |
| School engagement (items were averaged; median = 3) | How often did you have trouble: Paying attention in school? How often did you have trouble: Getting your homework done? |
1 = every day to 4 = never |
| Belief in hard work and optimism (items were standardized and averaged; median = 0) | How often did you feel hopeful about the future during the last week? When you get what you want, it's usually because you worked hard for it. |
0 = rarely to 3 = all of the time 1 = strongly disagree to 5 = strongly agree |
| Single-minded focus (items were averaged; median = 1.5) | During the past week, how many times did you:
|
0 = 5 or more times to 3 = not at all |
PC = primary caregiver.
The striving index was informed by the resilience literature.1 A striving index composed of four indicators was created: high educational aspirations, school engagement, belief in hard work and optimism, and a single-minded focus on success.1 Details of the indicators are presented at the bottom of Table 1. Four dichotomous indicators were created by performing a median split on each indicator; the indicators were then summed to form the striving index. Scores ranged from 0 to 4 (M = 2.05, SD = 1.09).
Young Adult Psychosocial Measures
At Wave 4, the young adults reported whether or not they had received a Bachelor's degree (coded as 0 or 1), were asked whether they had been diagnosed with depression by a mental health professional (coded as 0 or 1), and reported their average annual gross personal income.
Young Adult Type 2 Diabetes Status
At Wave 4, field researchers collected whole blood spots from a finger capillary prick onto filter paper that was dried and shipped to Flex Site Diagnostics (Palm City, Florida) for laboratory analysis of glycosylated hemoglobin (HbA1c).8 HbA1c is an integrated measure of blood glucose control over the preceding 2 to 3 months. Young adults also were interviewed and asked whether a health care provider ever told them that they have or had diabetes and age at the time of diagnosis. They were also asked about their use of prescription medications for type 2 diabetes during the past 4 weeks. Young adults were classified as having diabetes if they had a fasting glucose level ≥126 mg/dl, had a non-fasting glucose level ≥ 200 mg/dl, had an HbA1clevel ≥ 6.5%, self-reported a history of diabetes except during pregnancy, or used diabetes medication during the past 4 weeks. Of 5366 participants, 315 (5.9%) were classified as having diabetes (176 Black and 139 White).
Young Adult Body Mass Index
At Wave 4, trained field researchers obtained measurements of young adults' height and weight. This information was used to compute young adults' BMI, the ratio of weight in kilograms to height in meters squared.
Results
Preliminary Analyses
Table 2 presents descriptive statistics for the entire sample, the Black subsample, and the White subsample. At Wave 1, among the Black subsample, nearly 30% of the adolescents lived in families with incomes below the federal poverty level and 15.2% of the parents were unemployed. Among White participants, 10.8% of the adolescents lived in families with incomes below the federal poverty level and 6.4% of the parents were unemployed.
Table 2. Sample Characteristics.
| Variables (wave) | Whole Sample (N = 5366) | Black (n = 1431) | Whitea (n = 3935) |
|---|---|---|---|
| % or Mean (SD) | % or Mean (SD) | % or Mean (SD) | |
| Target gender (male) | 47.9% | 42.4% | 49.9% |
| Target age (W1) | 16.44 (0.85) | 16.42 (0.84) | 16.44 (0.86) |
| Disadvantage (W1) | 0.87 (1.13) | 1.39 (1.30) | 0.68 (0.99) |
| Family poverty | 15.2% | 28.3% | 10.8% |
| Parental education (< HS) | 17.4% | 21.4% | 16.4% |
| Parental unemployment | 8.8% | 15.2% | 6.4% |
| Single parent status | 29.4% | 51.1% | 21.5% |
| Receipt of public assistance | 7.8% | 15.2% | 5.2% |
| Inadequate income | 16.7% | 26.3% | 13.2% |
| Striving (W1) | 2.05 (1.09) | 2.19 (1.09) | 2.00 (1.09) |
| Educational aspirations | 50.7% | 52.1% | 50.2% |
| School engagement | 57.8% | 66.2% | 54.7% |
| Belief in hard work and optimism | 59.5% | 58.8% | 59.7% |
| Single-minded focus on success | 36.9% | 41.6% | 35.2% |
| Target age (W4) | 29.32 (0.91) | 29.33 (0.90) | 29.31 (0.91) |
| BMI (W4) | 29.07 (7.49) | 30.50 (8.34) | 28.54 (7.08) |
| Diabetes status (W4) | 5.9% | 12.3% | 3.5% |
| College degree (W4) | 34.3% | 29.4% | 36.1% |
| Personal annual income (W4) | 36.64 (48.01) | 31.62 (33.79) | 38.35 (51.86) |
| Depression (W4) | 18.9% | 13.5% | 20.9% |
W1 = Wave 1, age 16; W4 = Wave 4, age 29; HS = high school; BMI = body mass index.
White participants indicated that they had no Hispanic heritage.
Disadvantage and Striving at Age 16 and Psychosocial Outcomes at Age 29
The analyses in this section were designed to detect whether disadvantage or striving forecast college graduation, depression, or personal annual income. Two logistic regression models (for college graduation and depression) and a general linear model (for income) were used to examine these prospective associations. The models included main effects of Disadvantage, Striving, and race at age 16; the two-way interaction terms that included disadvantage × striving, disadvantage × race, and striving × race; and the three-way interaction of disadvantage × striving× race. Gender was included as a covariate. In all of the analyses, individual sample weights from Wave 1 and the Type = COMPLEX command of Mplus was used to account for oversampling by Add Health of smaller population groups and non-independence of observations among participants attending the same schools. The results of these analyses are presented in Table 3. Overall, a main effect of disadvantage at age 16 was associated with a lower likelihood of receiving a Bachelor's degree, a greater likelihood of a depression diagnosis, and a lower personal income at age 29. Main effects for striving also emerged for all the psychosocial outcomes. To the extent that participants reported high levels of striving at age 16, they were more likely to receive a Bachelor's degree, were less likely to be diagnosed with depression, and had higher personal income.
Table 3. Disadvantage, Striving, and Race as Predictors of Psychosocial Outcomes at Age 29.
| Predictors | College Degree | Personal Annual Income | Depression | |||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| b | [95% CI] | b | [95% CI] | b | [95% CI] | |
| 1. Gender, male | -0.155** | [-0.249, -0.061] | 17.338*** | [14.243, 20.433] | -0.475*** | [-0.566, -0.385] |
| 2. Disadvantage (age 16) | -0.531*** | [-0.596, -0.466] | -4.065* | [-7.784, -0.289] | 0.062* | [0.002, 0.122] |
| 3. Striving (age 16) | 0.345*** | [0.288, 0.401] | 3.549*** | [1.868, 5.229] | -0.112*** | [-0.167, -0.056] |
| 4. Race | -0.075 | [-0.297, 0.146] | -6.516*** | [-9.976, -3.056] | -0.337*** | [-0.482, -0.191] |
| 5. Disadvantage × Striving | -0.072 | [-0.151, 0.008] | -2.693 | [-5.812, 0.426] | 0.006 | [-0.050, 0.061] |
| 6. Disadvantage × Race | 0.286*** | [0.161, 0.411] | 1.195 | [-2.734, 5.124] | 0.026 | [-0.073, 0.125] |
| 7. Striving × Race | -0.046 | [-0.161, 0.069] | 0.766 | [-1.745, 3.277] | -0.019 | [-0.140, 0.102] |
| 8. Disadvantage × Striving × Race | 0.100 | [-0.005, 0.205] | 1.376 | [-1.985, 4.737] | -0.071 | [-0.195, 0.054] |
b = unstandardized regression coefficient, which represents the rate of change of the outcome variable (log odds of college degree, personal annual income, and depression) as a function of a change of one unit in the predictor variable with all other predictor variables held constant; CI = confidence interval.
p < .05.
p < .01.
p < .001.
A significant two-way interaction, disadvantage × race, emerged for college degree status. We examined this interaction by recalculating the regression lines (simple slopes) of disadvantage on college degree status separately for Black and White participants. Although disadvantage at age 16 was associated with a lower likelihood of receiving a Bachelor's degree for both Black (simple-slope = -0.184, 95%CI [-0.304, -0.064], p = .002) and White (simple-slope = -0.485, 95%CI [-0.542, -0.428], p< .001) participants, the association was more pronounced for White than for Black adults.
Testing the Skin-Deep Resilience Hypothesis with Type 2 Diabetes Status
The next set of analyses examined the skin-deep resilience prediction that strivers from disadvantaged backgrounds would, as young adults, be successful in psychosocial domains but would have poorer physical health as indicated by a heightened risk of having type 2 diabetes. This series of analyses predicted type 2 diabetes status at age 29 using a regression equation with four sequentially entered blocks of variables: (a) the covariates gender and BMI; (b) the main effects of disadvantage, striving, and race; (c) two-way interaction terms that included disadvantage × striving, disadvantage × race, and striving × race; and (d) the three-way interaction of disadvantage × striving× race. No main effects of disadvantage and striving were found; however, a disadvantage × striving × race interaction emerged (see Table 4, Model 1).
Table 4. Disadvantage, Striving, and Race as Predictors of Diabetes Status.
| Predictors | Diabetes Status (age 29) | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| Model 1 (whole sample, N = 5366) | Model 2 (Black, n = 1431) | Model 3 (Whitea, n = 3935) | ||||
|
|
|
|
||||
| b | [95% CI] | b | [95% CI] | b | [95% CI] | |
| 1. Gender, male | 0.043 | [-0.117, 0.204] | 0.142 | [-0.069, 0.353] | -0.014 | [-0.218, 0.191] |
| 2. BMI (age 29) | 0.031*** | [0.023, 0.038] | 0.020** | [0.006, 0.033] | 0.036*** | [0.026, 0.046] |
| 3. Disadvantage (age 16) | 0.007 | [-0.130, 0.143] | 0.072 | [-0.035, 0.178] | 0.004 | [-0.121, 0.128] |
| 4. Striving (age 16) | 0.010 | [-0.083, 0.104] | 0.027 | [-0.112, 0.167] | 0.017 | [-0.080, 0.113] |
| 5. Disadvantage × Striving | -0.076 | [-0.186, 0.034] | 0.117* | [0.002, 0.233] | -0.071 | [-0.170, 0.029] |
| 6. Race | 0.610*** | [0.456, 0.765] | - | - | - | - |
| 7. Disadvantage × Race | 0.036 | [-0.132, 0.205] | - | - | - | - |
| 8. Striving × Race | -0.069 | [-0.248, 0.110] | - | - | - | - |
| 9. Disadvantage × Striving × Race | 0.188* | [0.035, 0.341] | - | - | - | - |
b = unstandardized regression coefficient, which represents the rate of change of the outcome variable (log odds of diabetes status) as a function of a change of one unit in the predictor variable with all other predictor variables held constant; CI = confidence interval; BMI = body mass index.
White participants indicated that they had no Hispanic heritage.
p < .05.
p < .01.
p < .001.
To determine whether the skin-deep resilience pattern was specific to Black participants, additional analyses were conducted to examine the two-way interaction between disadvantage and striving separately for the Black and the White subsamples. The results revealed a significant two-way interaction for the Black subsample (Table 4, Model 2) but not for the White subsample (Table 4, Model 3). To decipher this interaction among Black participants, we plotted the estimated prevalence of type 2 diabetes for low (-1.5 SD from the mean) and high (+1.5 SD from the mean) levels of disadvantage and striving. These results, depicted in Figure 1, show that the type 2 diabetes findings were consistent with the skin-deep resilience pattern. For Black participants in the most disadvantaged families in the sample, higher striving was associated with a greater likelihood of developing type 2 diabetes (predicted prevalence of 31.99%). This association went in the opposite direction for Black participants raised in the most privileged families in the sample. For them, striving conferred greater protection from developing type 2 diabetes (predicted prevalence of 18.29%). Additional comparisons showed that high strivers from the most disadvantaged families in the Black subsample were 2.10 times more likely to develop type 2 diabetes than were high strivers living in the most privileged families in the Black subsample. Together, these results support the skin-deep resilience pattern in which the predicted prevalence of type 2 diabetes during adulthood would be greatest among high-striving Black youth who lived in disadvantaged circumstances.
Figure 1.
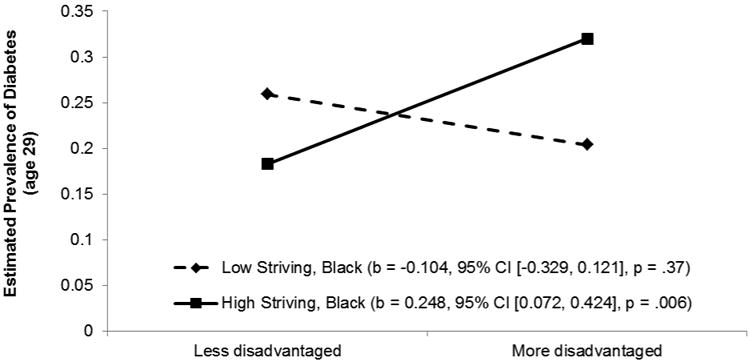
Diabetes status at age 29 as a function of disadvantage and striving at age 16 for the Black subsample.
Diabetes status was defined as fasting glucose ≥ 126 mg/dl, non-fasting glucose ≥ 200 mg/dl, HbA1c ≥ 6.5%, self-reported history of diabetes, or the use of diabetes medication during the past four weeks. The lines represent the regression lines for different levels of striving (low: 1.5 SD below the mean; high: 1.5 SD above the mean). Numbers in parentheses refer to simple slopes.
Additional analyses were executed to determine whether similar results would emerge when a more restricted definition of type 2 diabetes was used. This classification included blood glucose level, HbA1c level, and use of diabetes medication during the past 4 weeks. Of 5366 participants, 259 (4.8%) were classified as having diabetes (163 Black and 96 White participants). These analyses are presented in Table S1 and Figure S1 in the supplemental material available online. The results were identical to those reported previously.
Discussion
With a sample of Black adolescents from across the United States, the skin-deep resilience pattern emerged among high-striving youth from highly disadvantaged backgrounds. If, at age 16, these youth aspired to attend college, were highly goal directed and hardworking, and avoided activities that could sidetrack their goals and aspirations, then, at age 29, they were more likely to graduate from college, had greater personal resources, and were less likely to have symptoms of depression. The opposite pattern emerged for their health, as their chances of having type 2 diabetes were greater than those of similarly high-striving Black youth from more privileged backgrounds. This is the first demonstration that the skin-deep resilience pattern forecasts a heightened risk of developing a chronic disease. Diabetes reduces patients' quality of life and is a significant public health problem in the United States, with estimated financial costs of nearly $250 million annually (http:www.diabetes.org/advocacy/news-events/cost-of-diabetes.html). Hence, the 2.1-fold increased risk of developing diabetes among strivers from disadvantaged backgrounds is likely to have both individual and social ramifications.
The emergence of the skin-deep resilience pattern for type 2 diabetes among high-striving Black participants from disadvantaged backgrounds informs the health disparities literature. An unrelenting determination to succeed despite interpersonal, community, and institutional challenges is likely to occasion frequent activations of the HPA and SNS stress response systems.9 The hormonal end products of these systems, glucocorticoids and catecholamines, are elevated in Black youth who develop skin-deep resilience.2, 10 Frequent exposure to these hormones heightens inflammatory processes, which hasten the development of central obesity, insulin resistance, glucose intolerance, and type 2 diabetes.9 A follow-up study designed to include multiple waves of psychosocial, hormonal, inflammatory, and lifestyle data would be ideally suited to the identification of mechanisms responsible for the skin-deep resilience pattern.
For pediatric practice, the findings reported here emphasize the importance of surveillance and screening for early detection of indicators of skin-deep resilience in high- achieving Black youth from disadvantaged backgrounds. Helping these youth find a medical home would allow health-care professionals to perform regular and ongoing evaluations to detect early hints of the skin-deep pattern. Youth and their families could also be directed to school- and community-based resources that could assist the youth in developing resilience both “above and below the skin.” For example, participation in family-centered preventive interventions designed to enhance protective caregiving among disadvantaged African American families have been found to forecast reduced levels of proinflammatory cytokines11 and catecholamines,12 longer telomeres,13 and reduced epigenetic aging14 among youth and young adults. In addition, for older youth, colleges could provide cardiometabolic risk screenings and offer nutritional counseling and physical activity programs through student health services. This would facilitate the detection and treatment of emerging health problems before they become serious.
Some aspects of the study constitute possible limitations. First, the rate of diabetes was considerably lower among White adults (3.5%) than Black adults (12.3%). The low rate for White adults may have made detection of a skin-deep resilience pattern in that group difficult. Second, the items that comprised the striving index were developed specifically for the Add Health study and were collected from the study battery. Additional and refined measures should be used in future research. Because of sample size limitations, we were unable to examine the study questions with Latino or Asian participants. The possibility that skin-deep resilience emerges in these populations should be investigated in future research. Also, future research should examine change in type 2 diabetes by including a measure of it at Wave 1. Finally, research is needed to determine whether the skin-deep resilience pattern can be detected before adolescence. Can subgroups of children be identified who show this pattern in the early school years? Answers to this question will help to clarify the origins of chronic diseases such as type 2 diabetes. Despite these limitations, the results suggest that Black youth from disadvantaged backgrounds whose external behaviors appear to reflect resilience may be at risk for developing chronic diseases, such as type 2 diabetes.
Conclusions
The results of this study reveal that Black adolescents from disadvantaged backgrounds who have an unrelenting determination to succeed during adulthood fare well in terms of educational attainment, personal income, and symptoms of depression. The opposite pattern, however, emerged for their health, as their chances of having type 2 diabetes were heightened. Determined efforts during adolescence to “beat the odds” may exact an unanticipated toll on future health.
Supplementary Material
Figure S1. Diabetes status at age 29 as a function of disadvantage and striving at age 16 and of race.
Table S1. Disadvantage, Striving, and Race as Predictors of Diabetes Statusa
What's Known on This Subject
High-striving Black adolescents from disadvantaged backgrounds fare well in school and avoid drug use but are more likely to have outwardly undetectable wear and tear on their bodies that renders them vulnerable to negative health outcomes over the long term.
What This Study Adds
High-striving Black adolescents from disadvantaged backgrounds show a“skin-deep resilience” pattern during adulthood. They are more likely to graduate from college and have higher personal incomes but are also more likely to have type 2 diabetes.
Acknowledgments
Funding Source: Awards numbers R01 HD030588 and P30 DA027827 from the National Institutes of Health funded all phases of the study.
Abbreviations
- BMI
body mass index
- HbA1c
glycosylated hemoglobin
- SD
standard deviation
- SES
socioeconomic status
Footnotes
Financial Disclosure: The authors have indicated that they have no potential financial relationships relevant to this article to disclose.
Conflict of Interest: The authors have indicated that they have no potential conflicts of interest to disclose.
Contributors' Statement: Dr. Brody conceptualized and designed the study, drafted the initial manuscript, approved the final manuscript as submitted, and takes full responsibility for the final manuscript as submitted.
Dr. Yu conceptualized and designed the data analyses, made substantial intellectual contributions to the study, and approved the final manuscript as submitted.
Drs. Miller and Chen made substantial intellectual contributions to the study, critically reviewed the manuscript, and approved the final manuscript as submitted.
References
- 1.Brody GH, Kogan SM, Grange CM. Translating longitudinal, developmental research with rural African American families into prevention programs for rural African American youth. In: King RB, Maholmes V, editors. The Oxford handbook of poverty and child development. New York, NY: Oxford University Press-USA; 2012. pp. 553–570. [Google Scholar]
- 2.Brody GH, Yu T, Chen E, Miller GE, Kogan SM, Beach SRH. Is resilience only skin deep? Rural African Americans' preadolescent socioeconomic status-related risk and competence and age 19 psychological adjustment and allostatic load. Psychological Science. 2013;24(7):1285–1293. doi: 10.1177/0956797612471954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chen E, Miller GE, Yu T, Brody GH. The Great Recession and health risks in African American youth. Brain, Behavior, and Immunity. 2015 Dec 21; doi: 10.1016/j.bbi.2015.12.015. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Miller GE, Yu T, Chen E, Brody GH. Self-control forecasts better psychosocial outcomes but faster epigenetic aging in low-SES youth. Proceedings of the National Academy of Sciences of the USA. 2015;112(33):10325–10330. doi: 10.1073/pnas.1505063112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Piccolo RS, Yang M, Bliwise DL, Yaggi K, Araujo AB. Racial and socioeconomic disparities in sleep and chronic disease: Results of a longitudinal investigation. Ethnicity and Disease. 2013;23(4):499–507. [PMC free article] [PubMed] [Google Scholar]
- 6.Harris KM. An integrative approach to health. Demography. 2010;47(1):1–22. doi: 10.1353/dem.0.0091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rutter ML. Resilience: Some conceptual considerations. Journal of Adolescent Health. 1993;14(8):626–631. doi: 10.1016/1054-139x(93)90196-v. [DOI] [PubMed] [Google Scholar]
- 8.Nguyen QC, Whitsel EA, Tabor JW, Cuthbertson CC, Wener MH, Potter AJ, et al. Blood spot–based measures of glucose homeostasis and diabetes prevalence in a nationally representative population of young US adults. Annals of Epidemiology. 2014;24(12):903–909. doi: 10.1016/j.annepidem.2014.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Miller GE, Chen E, Parker KJ. Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychological Bulletin. 2011;137(6):959–997. doi: 10.1037/a0024768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chen E, Miller GE, Brody GH, Lei MK. Neighborhood poverty, college attendance, and diverging profiles of substance use and allostatic load in rural African American youth. Clinical Psychological Science. 2015;3(5):675–685. doi: 10.1177/2167702614546639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Miller GE, Brody GH, Yu T, Chen E. A family-oriented psychosocial intervention reduces inflammation in low-SES African American youth. Proceedings of the National Academy of Sciences of the USA. 2014;111(31):11287–11292. doi: 10.1073/pnas.1406578111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brody GH, Yu T, Chen E, Miller GE. Prevention moderates associations between family risks and youth catecholamine levels. Health Psychology. 2014;33(11):1435–1439. doi: 10.1037/hea0000072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Brody GH, Yu T, Beach SRH, Philibert RA. Prevention effects ameliorate the prospective association between nonsupportive parenting and diminished telomere length. Prevention Science. 2015;16(2):171–180. doi: 10.1007/s11121-014-0474-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brody GH, Yu T, Chen E, Beach SRH, Miller GE. Family-centered prevention ameliorates the longitudinal association between risky family processes and epigenetic aging. Journal of Child Psychology and Psychiatry. 2016;57(5):566–574. doi: 10.1111/jcpp.12495. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Diabetes status at age 29 as a function of disadvantage and striving at age 16 and of race.
Table S1. Disadvantage, Striving, and Race as Predictors of Diabetes Statusa