

Abstract
This article analyzes the history of tobacco industry funding for the AIDS response – a largely ignored aspect of private donor involvement. Primary documents from the Legacy Tobacco Documents Library and from AIDS organizations are analyzed, alongside existing literature on the tobacco control and AIDS responses. Research on the tactics of transnational tobacco companies has documented how they have used various charitable causes to subvert tobacco control efforts and influence public health policy. This raises questions, which this paper seeks to answer, about if donations by tobacco companies to AIDS organizations have been used for similar means, and if so how AIDS organizations have responded to tobacco industry overtures. Two examples illustrate that tobacco companies initially tried to use the AIDS response to counter tobacco control measures: 1) During the 1990s Philip Morris, one of the largest corporate donors of the AIDS response in the US, used its connections with AIDS organizations to create competition for health resources, improve its reputation, and market tobacco products to the LGBT community; 2) In both Latin America and Sub-Saharan Africa, Philip Morris and British American Tobacco championed the AIDS response in order to delegitimize efforts to develop the WHO Framework Convention on Tobacco Control. However, from the late 1990s onwards, AIDS organizations began to refuse tobacco funding and partnerships - though these policies have been not comprehensive, as many tobacco companies still fund programs in Sub-Sahara Africa. The article concludes that tobacco companies aimed to exploit competition between health issues, and use the high profile AIDS response to improve their reputation and market access. However, AIDS organizations, adhering to broader health goals and drawing on extensive resources and networks, were able to shut the tobacco industry out of much of the response, though pockets of influence still exist. This demonstrates the importance of co-operation and policy convergence across health sectors, and suggests that tobacco control advocates, and other charitable sectors that receive funding from the tobacco industry, may be able to draw lessons from the experiences of AIDS organizations.
Keywords: HIV, AIDS, donors, corporations, WHO, tobacco industry
1. Introduction
This article analyzes the history of tobacco industry funding for the AIDS response – a largely ignored aspect of private donor involvement. Research on private donor involvement in the HIV/AIDS response to date has largely focused on the role of pharmaceutical companies (Flanagan & Whiteman 2007; Leisinger 2005; Lee & Kohler 2010), as well as the creation of public-private-partnerships to mobilize innovative financing (Ramiah & Reich, 2006; Buse & Harmer, 2007; Williams & Rushton, 2012). Meanwhile, the tobacco control literature only refers to AIDS initiatives in passing. An article on Philip Morris' (PM) attempts to generate legitimacy by working with health organizations refers to partnerships with AIDS Service Organizations (ASOs), but does not specifically discuss the dynamics between the tobacco industry and ASOs (McDaniel, 2006). Drabble (2000) documents how PM targeted lesbian, gay, bisexual and transgender (LGBT) communities with donations to related causes, but does not analyze the AIDS response in depth. Other research (Mamudu et al., 2008; Muggli & Hurt, 2003; Rimmer, 2005) briefly refers to tobacco industry sponsorship of specific AIDS events, but does not explore engagement in the AIDS response as an ongoing strategy employed by TTCs. Looking at other health sectors, this literature does document how TTCs have used charitable causes to subvert tobacco control efforts (Fookes et al. 2013; Mackenzie & Collin 2008). For example, in 1999, British American Tobacco (BAT) sponsored the creation of the Beijing Liver Foundation with the specific purposes of diverting government attention away from tobacco related illnesses (Muggli et al. 2008). This raises questions, which this paper seeks to answer, about if the donations by tobacco companies to the AIDS response were used for similar means. Furthermore, both the tobacco control and AIDS literature focuses on the role of tobacco companies as donors instead of organizations as recipients, and therefore fails to consider how organizations and charitable sectors targeted by tobacco funding respond to the ethical dilemma of receiving resources from an industry whose products are harmful to public health.
In order to contribute to filling these gaps in current research on private donors to the AIDS response and AIDS organizations' policies in regards to the tobacco industry, this article demonstrates how transnational tobacco companies (TTCs) initially tried to used the AIDS response to counter tobacco control measures, and then how actors in the AIDS response developed policies to restrict the participation of TTCs in global health. The article finds that TTCs aimed to exploit competition between health issues, and use the high profile AIDS response to improve their reputation and market access. However, AIDS organizations, adhering to broader health goals and drawing on extensive resources and networks, were able to shut the tobacco industry out of much of the response, though pockets of influence still exist. This demonstrates the importance of co-operation and policy convergence across health sectors.
In addition to contributing to the literature on AIDS funding, this article adds to understanding of the challenges of and opportunities for implementing Article 5.3 of the Framework Convention on Tobacco Control (FCTC), “on the protection of public health policies with respect to tobacco control from commercial and other vested interests of the tobacco industry.” The FCTC, introduced in 2003 and now signed by 168 states, aims to reduce tobacco related illness and death worldwide and limit the influence of the tobacco industry in public health policy. This article explores how AIDS organizations, as potential recipients of tobacco industry funding, make use of the norms embedded in the FCTC and influence its legitimacy. It suggests that tobacco control advocates, and other charitable sectors that receive funding from the tobacco industry, may be able to draw lessons from the experiences of AIDS organizations.
Following a brief description of the research methodology, the article provides two examples of tobacco industry involvement the AIDS response: Philip Morris' support for the early AIDS response in the United States (US), and Philip Morris' and British American Tobacco's efforts to delegitimize the WHO FCTC process by arguing that AIDS was a more important global health concern than tobacco control. It then documents the measures AIDS organizations took to restrict tobacco industry interference, and the limitations on these efforts, particularly in Sub-Sahara Africa. It concludes with policy implications for the AIDS response specifically, and global health governance more generally.
2. Methods
The research began with a review of secondary literature to identify key processes, actors, events and initiatives in the relationship between organizations involved in the AIDS response and tobacco industry. The Legacy Tobacco Documents Library, a collection of around 14 million industry documents that were released following US litigation, was then searched using keywords related to the global AIDS response including terms such as ‘National AIDS Fund’ and ‘Global Business Coalition’. The methodology and limitations of analyzing internal tobacco industry documents has been discussed elsewhere. Follow-up searches using a snowballing technique were conducted to further identify relevant industry actors (such as the Tobacco Growers' Association of Malawi) and campaigns (such as the Virginia Slims Legends Tour) involved in AIDS-related activities. Then the websites of the four largest tobacco companies' (Philip Morris, British American Tobacco, Imperial Tobacco and Japan Tobacco) were searched for the terms ‘HIV’ and ‘AIDS’. Reports on corporate social responsibility and charitable giving from these TTCs were correspondingly searched for any mention of HIV or AIDS.
The researchers then examined documents from AIDS organizations to identify policies related to engagement with TTCs. These queries were conducted first by searching the sites of those organizations mentioned in the tobacco industry documents (such as the Global Business Coalition and National AIDS Fund), and searching well known global AIDS organizations' (including UNAIDS, the Global Fund, and Funders' Concerned about AIDS) sites with the term ‘tobacco’ as well as the names of the largest tobacco corporations. In some cases more specific online searches were conducted to verify reference to specific events or partnerships. Two authors reviewed all materials independently to ensure relevant data were identified, interpreted appropriately and properly contextualized.
There were a number of limitations to the research. Many AIDS organizations have not kept historic policy documents or put them online. For example, records from some organizations, such as the Global Business Coalition on Health and National AIDS Fund, from the 1990s (when both worked closely with the tobacco industry) were not available. The restriction to online searches meant results were limited to what documents were made public. Furthermore, it is demonstrated that the TTCs destroyed many documents that should have been made available on the Legacy database (MacKenzie, Collin, & Lee, 2003). While this restricts analysis of why policies changed, existing documents present rationales that, when contextualized within the broader AIDS and tobacco control histories, generated a comprehensive narrative.
3. Fair Play? Philip Morris' support for the early AIDS response in the US
The initial response to AIDS in the US during the 1980s was characterized by conflicts between affected communities – mostly gay men and their allies – and repressive public reactions. When infections first appeared among young homosexual men homophobia combined with ignorance to generate a particularly oppressive and stigmatizing response (Fee, 1995). People Living with AIDS (PWAs) were denied health care, lost their jobs and were evicted from housing. Initial state action was slow and inadequate. US President Ronald Reagan did not mention the epidemic until 1985, and his first measures were to ban PWAs from entering the US and to promote sexual abstinence (Fee, 1995).
AIDS advocacy and self-help groups sprung up across the country demanding more progressive policies, and challenging homophobic and discriminatory attitudes. The Gay Men's Health Crisis, founded in 1981 in New York City, was the first formal PWA support group, and throughout the 1980s similar ASOs developed across the US (Knight, 2008). Membership largely consisted of middle class white males, who were well educated, articulate and professional. They rejected state sponsored campaigns that characterized them as statistical risk groups and as populations of disease carriers (Fee, 1994). Instead, they argued that the epidemic was not the result of their sexual orientations or behaviors, but the homophobia, stigma and discrimination that forces individuals to avoid information and medical care (Bayer & Fairchild, 2006). They took to the streets, staging “die-ins” in front of government and pharmaceutical offices, and coordinating national protests.
In one such case Act-Up, a political AIDS rights organization, decided to boycott Philip Morris Companies Inc. (PM), in 1990, when it found out that the TTC made donations to Senator Jessie Helms' campaigns for re-election (McGovern 1987), as well as his personal charity, the Jessie Helms Center (Lewis, 1989). Helms had promoted a particularly repressive response to AIDS, such as adding the Helms Amendment to the AIDS Appropriation Bill, which banned government funding for any AIDS education materials that “promote or encourage, directly or indirectly, homosexual activities” (US Senate, 1987). Act-Up made three demands of PM: that it stop funding Senator Helms; that it renounce its past support for Helms; and that it meet with Act-Up representatives to discuss PM's corporate responsibility to the LGBT community and AIDS response (Act-UP, 1990; Offen et al., 2005). In response, PM justified its donations to Helms as based on his representation of North Carolina, where PM ran a number of processing plants, as well as due to his support for the tobacco industry in general (PM, 1992). Helms had opposed the increase of taxes on cigarettes, as well as other proposals to regulate the tobacco industry (Maguire, 1993). PM refused to stop supporting Helms, but did increase funding to the AIDS response – illustrated by the temporary rise in donations to the National AIDS Fund in 1990 as depicted by Figure 1. Having secured this additional funding for the AIDS response, Act-Up called off the boycott (PM, 1992; Offen et al., 2005).
Figure 1. Philip Morris Contributions to the National Aids Fund (NAF 1996).
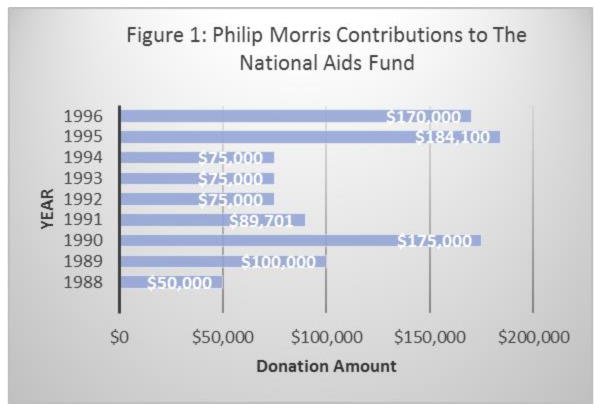
Over the next decade PM became one of the largest corporate donors to the National AIDS Fund. The fund had been created in 1988 to generate resources and provide support for ASOs, and received donations from a variety of sponsors, including the Ford Foundation and Elton John Foundation (NAF, 2007). One of the Fund's signature projects was Positive Helpings, a nutrition program for PWAs. Between 1996 and 2001, Positive Helpings distributed more than US$ 3 million from PM to food and meals programs serving PWAs. In addition to supporting the National AIDS Fund, PM donated to a wide range of AIDS organizations, including the Gay Men's Health Crisis, the Lutheran Church and the American Foundation for AIDS Research (PM, 1995). PM framed its support to the AIDS response as an extension of the company's contributions to the arts, stating, “For the Philip Morris family of companies, the AIDS epidemic of the 1980s hit close to home. Because of our support of the arts, we became aware of the devastating loss to the arts community wrought by the spread of this disease” (PM, 2000b). PM also explained support for AIDS nutrition programs, such as Positive Helpings, as an extension of Kraft's (a food corporation that was at the time a subsidiary of PM) programs, which prioritized nutrition related charitable giving.
In addition, PM hoped to use its relationships with ASOs to foster competition for resources that were being directed towards tobacco control. As evidence mounted regarding the harms of smoking and second-hand smoke, the US government increased funding to civil society organizations to conduct anti-smoking youth education and tobacco control advocacy. PM used the networks it had established through its AIDS programs to contest this support. In 1996, the company initiated a strategy entitled “Fair Play”, which aimed to limit the effectiveness of tobacco control advocates. Fair Play documents reveal a proposal to mobilize social activists, including those fighting AIDS, to compete with tobacco control groups for government funds. As suggested by Joshua Slavitt, PM Issues Manager:
An additional option would be to identify other groups who feel they are not receiving adequate federal or state funding for their programs. Examples could include, public literacy programs, AIDS research, programs to help the physically challenged, etc….This effort may lead to opportunities to encourage groups to divert federal or state funds away from tobacco control to other vital public programs during the appropriations process (Slavit, 1996).
PM planned to achieve this through “work with Corporate Contributions and other internal departments to identify individuals or organizations that can act as ‘emissaries’ to reach out to these groups” (Slavit, 1996). By letting AIDS and other organizations know how much state funding was going towards tobacco control groups, PM hoped to mobilize them to compete for funds and critique government priorities (PM, 1999).
PM also needed allies to help it counter negative publicity and improve its corporate image. The Commissioner of the Food and Drug Administration testified before US Congress in 1994 that, despite TTC assertions to the contrary, nicotine was indeed a highly addictive drug in tobacco. Lawsuits against the industry, mounted by several US states and whistle blowers, led to the release of internal industry documents revealing how TTCs had attempted to obscure evidence about the harms and addictive elements of smoking. Scholarly analysis and media reporting based on the revelations from these documents severely damaged the reputation of the tobacco companies (Ashley, 2003). By 2000, PM's own research indicated that it was one of the least trusted corporations in the US, and that a reputation management strategy was urgently needed (PM, 2000).
PM used AIDS fundraising events to improve its public image. For example, its largest AIDS fundraiser was the Virginia Slims Legends Tours – a series of tennis tournaments and all female musical performances. The tour raised approximately US$ 4 million for the National AIDS Funds between 1995 and 1998 (Rosenberg & Siegel, 2001). It also created opportunities for PM to share its message about smoking and the tobacco industry. PM provided instructions to representatives of the National AIDS Fund on how to respond to criticism about receiving tobacco funding. They were to state:
We're proud of our relationship with Philip Morris U.S.A. and Virginia Slims, and we support their belief in freedom of choice. Philip Morris, through its diverse food, beer and tobacco companies, has been very supportive of organizations that are leading the fight against AIDS. They were among the first corporations to assist in AIDS research, AIDS prevention/education and direct care for people with AIDS. The Virginia Slims brand has established a history of its own, through various promotions, that have benefited AIDS research over the years. Let's remember, AIDS does not discriminate and neither should we (PM, 1994).
The statement used phrasing that sought to unite the AIDS response with smokers' rights campaigns. The reference to freedom of choice refers to PM's frequent argument that smokers had the right to ‘choose’ to smoke, with tobacco control policies threatening that right (Balbach et al., 2005). In the context of an AIDS fundraiser, largely targeted at the LGBT community, this framing also reflected acceptance of sexual choice (Stevens et al., 2004). Similarly, reference to discrimination refers to the stigma attached to the virus, and echoes earlier campaigns by PM that smoking regulations discriminate against people who smoke. For example, in a press release from PM, the Vice President of Corporate Affairs is quoted as arguing that businesses need to “at least think before taking action that will discriminate against a large segment of their employees [i.e. smokers], their customers, and their vendors …. The time has come when smokers will not sit passively and have their rights trampled” (PR Newswire, 1988). PM's language around AIDS subtly mirrored pro-tobacco messaging. Furthermore, events such as the Virginia Slims Legends Tour presented PM as a good corporate citizen who was supporting an important community cause.
Such positive publicity also provided PM with lucrative marketing opportunities. Most American ASOs had strong connections to the LGBT community, who had, and continue to have, higher rates of smoking than the general public. A national household survey on drug abuse in 1990 found that 35% of gay men and 38% of lesbians had smoked cigarettes in the past month compared to 27% of men and 22% of women in the general sample (Drabble, 2000). Studies conducted across a range of contexts suggest LGBT populations have a higher smoking prevalence than the total population (Offen et al., 2008). Higher smoking rates are attributed to the additional levels of reported stress, and need for acceptance or desire for rebellion among LGTB youths. Smoking is also associated with the culture of ‘coming-out’ (Drabble, 1999). As LGBT communities have been shown to prefer brands that support LGBT related causes, supporting the AIDS response provided PM with a marketing advantage among a population group with higher smoking rates (Goebel, 1994; Drabble, 2000).
Noting the specific characteristics of the LGTB market, PM not only targeted LGTB smokers in traditional marketing campaigns, it also used AIDS initiatives to develop positive brand recognition (Smith & Malone, 2003). Between 1998 and 2002, PM paid for advertisements in Out Magazine that listed the top ten “Companies That Care” about LGTB community causes. The 2002 advertisement put PM in the top spot and celebrated PM's US$ 14 million in donations to AIDS-related organizations (Out Magazine, 1998 & 2002; Stevens et al., 2004). In 2002, PM ran a similar advertisement in PRIDE.02, ‘the Magazine for Gay Pride in the USA’, which noted that PM was one of the largest corporate contributors to the fight against AIDS. Such publicity presented PM as an ally in the AIDS response, seeking to generate a favorable reputation, and therefore market share, within the LGTB community (Stevens et al., 2004).
During the 1990s, ASOs were initially grateful for PM's support (Drabble, 2000). In 1990, federal US funding for AIDS programs was just $3.1 billion, which was grossly inadequate (Summers & Kates, 2004). Most ASOs depended on donations from private individuals, churches and charities to keep their doors open (Fee, 1994). Tobacco industry funding was the largest corporate grant for many American ASOs. Furthermore, tobacco funding provided more flexibility than government and foundation grants, allowing ASOs to design programs as they saw fit, and tobacco grants had substantially fewer reporting requirements. Grants from PM could be used for capital and administrative expenses, which was not typical of other corporate or foundation funding (Stone & Siegel, 2004). For example, PM provided money for general operating costs to the National Women and AIDS Project and Philadelphia Sciences Institute (PM, 1995). In return, the AIDS response provided PM with opportunities to divert attention and resources away from tobacco control, and to enhance its market position and messaging.
4. Targeting WHO's ‘Blind Spots’: TTCs use of AIDS as a diversion from global tobacco control
By the early 1990s awareness was increasing of growing AIDS epidemics in LMICs. In particular a generalized epidemic (as opposed to epidemics contain amongst specific population groups as was the case in most high income countries) was emerging in Sub-Sahara Africa. In South Africa, HIV prevalence among pregnant women climbed from less than 5% of the population in 1990 to nearly 30% in 1997 (UNAIDS, 1998). As treatment for those infected, and to prevent HIV transmission from mothers to infants, was not yet available in LMICs, due to the high cost and lack of health resources, increasing HIV infections were followed by mortality, orphaning and further devastating social impacts (Poku, 2006). AIDS epidemics in LMICs outside of Sub-Saharan Africa were less severe, but still caused widespread concern. AIDS rates in the Caribbean (1.82%) and South and South East Asia (0.61%) were lower than in Sub-Saharan Africa (7.4%), but higher than in North America (0.55%) and Western Europe (0.23%). As a result, there were predictions of burgeoning generalized epidemics in LMICs, and calls for scaling up a global response (UNAIDS, 1998; Pisani, 2008). Consequently, both the amount of funding for AIDS and number of organizations addressing the epidemic rapidly increased. Contributions from donor countries for the AIDS response rose from US$ 90 million in 1990 to US$ 1359 million in 2000 (Knight, 2008). In 1996, the United Nations Joint Program on AIDS was formed, and by the turn of the millennium discussions were underway to create innovative financing mechanisms for the AIDS response.
Much less attention was paid to the increasingly globalized use of tobacco products (Callard, 2008). As countries in North America and Western Europe implemented tobacco control measures and education activities, throughout the 1990s, smoking rates in what had been the largest markets for TTCs began to decline. Consumption in the US fell from approximately 750,000 cigarettes in 1981 to less than 500,000 in 2001 (WHO, 2008). In response, TTCs' shifted their focus to emerging markets in Asia, Africa and Latin America, where there were weaker regulations, growing populations and rising incomes (Lee, 2014). Initially, TTCs faced few barriers in restructuring their operations towards this globally oriented strategy. Tobacco control was still seen as primarily a domestic concern. The WHO Tobacco and Health Unit, located under the substance Abuse Program, collected and aggregated available data on tobacco use and its health consequences in members states, but was unable to do much else as it had only a handful of staff and limited budget (Lee, 2014). Meanwhile, domestic governments in LMICs were not overly concerned about increasing tobacco use. Though tobacco use was increasing in LMICs, the relatively delayed impacts of smoking (tobacco related illness often do not appear until decades after habits begin) meant that tobacco use did not present an imminent health threat (WHO, 2014). As many LMICs faced numerous health challenged related to lack of public health resources, and widespread poverty and infectious disease, tobacco control was not considered an urgent priority. As a result, TTCS were able to mitigate loses due to market contraction in high income countries by increasing sales in LMICs.
In order to create awareness about the growing disease burden from tobacco use in LMICs, public health advocates began organizing international events and campaigns. The 8th World Conference on Tobacco or Health (WCTOH), held in Buenos Aires in 1992, was the first tobacco conference held in a LMIC. The conference was described by Muggli et al as “a significant moment in globalizing tobacco control,” because it was the first meeting to concentrate on the dangers of second hand smoke and the effects of tobacco use in LMICs (2008, 2). Conference organizers advocated the introduction of tobacco control measures in LMICs comparable to those adopted in high-income countries.
Fearful of how such policies might impact its market expansion in LMICs, British American Tobacco (BAT) devised a planned to create a distraction from the WCTOH. Jorge R. Basso Dastugue, a representative from Nobleza-Piccardo, BAT's subsidiary in Argentina, proposed a strategy to counter the WCTOH by capitalizing on growing concerns around AIDS: “Being the disease of the century and a preventive disease, AIDS should be ‘public enemy No. 1’ because of its terminal consequences at every age. Facing the [sic] AIDS increasing importance in the world and in Argentina we believe this disease to be the sole matter cable [capable] [sic] of eclipsing the [WCTOH] Conference” (Dastugue, 1992). One of Dastugue's strategy documents, entitled Proposed Possible Action To Take Against [the WCTOH], suggested “to have groups fighting against AIDS claim this conference for their priority as compared to tobacco” (Dastugue, 1992. Further documents describe plans to generate competition for media and policy attention by sponsoring AIDS publicity events at the same time as the conference. Plans were proposed to bring in a “world known medical doctor” in order to divert press attention, and to have publicity films on AIDS be projected on large screens in different areas in the city at the same time as the WCTOH. In order to avoid questions about the timing of such campaigns, these promotions would not include information identifying BAT as the sponsor; instead BAT would provide the financing through a local AIDS foundation (Dastugue, 1992).
While it appears that not all planned activities were carried out, BAT did sponsor music concerts and soccer matches promoting AIDS awareness in Argentina at the same time as the WCTOH (Muggli & Hurt, 2003). The “world known doctor,” mentioned in Dastugue's plan may have been Luc Montagner, one of the discoverers of HIV, who visited Argentina at the same time as the WCOTH. The Buenos Aires newspaper, La Pensa (1992), reported on Montanger's visit, which coincided with the launch of the second phase of the National Program on AIDS by the Argentina Ministry of Health and Social Action. Such events fulfilled BAT's goal of creating competition between AIDS and tobacco control for media and political attention.
Despite such efforts by TTCs to subvert tobacco control efforts, WHO continued to promote the idea of a global convention on tobacco control. At the World Health Assembly (WHA) in 1992, the concept of an international legal instrument on tobacco control was put forward (Roemer et al., 2005). In 1995, WHO member states adopted WHA Resolution 48.11 calling for “an international strategy for tobacco control,” including the adoption of this international instrument. In 1996, Resolution 49.17 was adopted at the WHA, calling on all parties to fast track negotiations of the FCTC. In 1998, WHO Director-General Gro Harlem Brundtland made global tobacco control one of two cabinet-level priorities, and negotiations on the WHO FCTC commenced in 1999 (Lee, 2014).
Alongside these developments, BAT maintained the message advanced previously in Argentina – that global health cooperation should prioritize AIDS, not tobacco control. In a document entitled, The WHO Framework Convention on Tobacco Control: Our view, BAT argued that the convention:
Would impose an additional burden on many governments, which have already determined their own domestic policy needs. There are likely to be serious resource implications for many national governments, particularly in developing countries, which have already committed stretched resources to health policy matters they consider higher priority, such as HIV (BAT, 2000).
This messaging sought to discredit the WHO by questioning if its priorities aligned with those of LMICs. While AIDS was a growing concern in LMICs, as outlined above, in most countries outside of Sub-Saharan Africa there were arguably more pressing health matters as the majority of child and adult deaths continued to be caused by non-communicable diseases, many of which were related to the growing use of tobacco products, such as lower respiratory infections (WHO, 2003). However, BAT capitalized on the growing panic around AIDS, to question WHO policies and argue they neglected LMIC needs.
An important ally of this strategy was the industry front group the International Tobacco Growers Alliance (ITGA). Established in 1984 by the tobacco industry, the ITGA was a global agricultural lobby group on tobacco farming issues (Tobacco Tactics, 2014). While presenting itself as an independent collective of tobacco farmers, the ITGA received substantial funding from TTCs to create resistance to tobacco control efforts (Rimmer, 2005). In the late 1990s, BAT developed a plan to work with ITGA members in LMICs to lobby the WHO to direct greater attention to AIDS. A 1998 document outlines a strategy to, “Target WHO's blind spots on key primary health priorities, such as AIDS prevention and malaria. Working through African and Latin American members, ITGA will build actions with their governments to put pressure on WHO” (ITGA, 1998). In order to advance this strategy, ITGA members participated in AIDS related events and championed the need for greater AIDS resources from the WHO. Shabanji Opukah, BAT's Head of International Development Issues, wrote in an email that the ITGA Executive Director called him to report on the outcomes of a Southern African regional meeting:
The ITGA agreed to support fully a proposal for a pan African aids conference to be held in Zambia in September hosted by the health ministry at which they will discuss the aids scourge in Africa. The ITGA is going to present what their grower associations have been doing to support government and NGO efforts in combating AIDS in Africa and through that highlight the importance of tobacco to the economy whilst relegating it as an issues [sic] in the health priorities of these countries. Then [sic] idea is to use the forum to challenge and ridicule the WHO convention (Opukah, 1999).
By highlighting AIDS, the ITGA aimed to suggest that while the tobacco industry was addressing the epidemic and supporting the local economy, WHO priorities where misplaced and the FCTC would not benefit LMICs.
In order to further propagate this message, in 1999, BAT paid for representatives from the ITGA to meet with representatives from the WHO regarding the FCTC (Opukah, 1999b). An article about the meeting was published in the industry sponsored Tobacco Journal. It quoted the ITGA President, Richard Tate, as noting that while the ITGA disagreed with WHO over tobacco control, it encouraged it to increase its commitments to addressing AIDS and Malaria: “Many of our members are from developing countries and know the suffering and distresses caused by both diseases. This is the type of fundamental public health campaign that we applaud” (Hallmark, 1999). Another article on the meeting celebrated BAT's contributions to the AIDS response in Southern Africa: “In Zimbabwe, for example, tobacco farmers have set up one of the most extensive AIDS prevention programs in rural areas. Without their action, there would have been few resources available to combat this terrible scourge” (PR Newswire, 1999). This messaging showcased the contributions of the tobacco industry to the AIDS response, at the same time as suggesting WHO was not doing enough to address the epidemic because it was preoccupied with tobacco control.
The ITGA also championed AIDS at tobacco control related events. In 2000, PM paid for ITGA representatives from Malawi to attend a UN Economic and Social Council meeting on the FCTC in 2000. The Malawian delegates listed their goal in attending the meeting as to get the WHO to “reassess importance of tobacco growing for developing countries; put health priorities on real world basis, and go public where good work is taking place” (ITGA Malawi, 2000). The concept of refining health priorities “on a real world basis” reiterated the message that tobacco control was a concern primarily in high-income countries, while LMICs suffered from other health concerns, such as AIDS, which should be prioritized by WHO because of these countries' relative reliance on external assistance to address public health needs. The delegates reported to PM that they had advised the Malawian government representatives to present a similar message. Indeed the government of Malawi's subsequent statement on the FCTC, which was included in communications between the ITGA and PM as evidence of influence, expressed the belief “that the deaths due to Tobacco e.g. in Malawi are exaggerated, ignoring more important problems of Malaria and H.I.V. Aids” (quoted in ITGA Malawi, 2000). PM and BAT used networks with AIDS organizations and the ITGA to foster a discourse that capitalized on growing concerns about the AIDS epidemic at the expense of tobacco control.
5. “A Pact with the Devil”: Restricting TTC's Corporate Social Responsibility Opportunities
As evidence emerged on the higher smoking rates among LGBT populations in the US (as outlined above), AIDS organizations began questioning the motivations behind tobacco industry funding. The Coalition of Lavender Americans on Smoking and Health was supported by the Center for Disease Control, in 1996, to organize a conference, ‘Alive With Pleasure!’, which focused on the prevention of tobacco use and alcohol problems in the LGBT communities. The Coalition met with LGBT and AIDS organizations to discuss the health impacts of smoking and suspect practices of TTCs (Drabble, 1999). Their concerns were augmented by research showing that smoking was particularly harmful for PWAs and could impede treatment effectiveness (Furber et al., 2006). The findings created a link between anti-smoking campaigns and AIDS health care. Rather than there being a choice between tobacco control and AIDS, both issues were recognized as relevant health issues for ASOs and LGBT groups.
In response to growing awareness of smoking related diseases within the AIDS community, as well as wider public attention to the public relations tactics of tobacco companies, many ASOs and LGBT organizations demanded their boards refuse tobacco related funding. As early as 1991, a leader of Act-Up San Francisco argued in an editorial that receiving funding from PM, “represents us taking money from walking over the bodies of those killed by cigarettes … I would characterize this as a pact with the devil” (quoted in Yukins 1991). By the late 1990s such opinions had become widespread with the Coalition of Lavender Americans on Smoking and Health arguing, “We gay adults have a responsibility to start treating tobacco as a serious threat to our community. It's not some minor concern to be ignored while we focus on AIDS and breast cancer” (Drabble, 1999). In 1998 and 1999, the Coalition produced ‘The Ethics of Tobacco, Alcohol, & Pharmaceutical Funding: A Practical Guide for LGBT Organizations’, which advised against accepting tobacco funding, arguing it was a harmful form of indirect marketing. The Coalition encouraged ASOs to develop guidelines on what type of corporate funding they welcomed, and under what conditions. The Gay and Lesbian Medical Association developed, in 1998, one of the first such policies, stating that: “The Gay and Lesbian Medical Association will not accept direct funding from alcohol or tobacco manufactures or distributors” (quoted in Drabble, 2000). While not all AIDS related organizations made the choice to refuse TTC funding, it became increasingly common. A survey of ASOs in the US found that the most common reasons for refusing TTC funding was recognition that accepting tobacco money conflicted with organizational mandates related to improving population health, and due to concerns about public association between the organization and tobacco corporations – due to TTC's increasingly poor reputation (Stone & Spiegel, 2004). By linking health issues, ASOs recognized that tobacco control initiatives were not in competition with AIDS programs, as TTCs had suggested, but had similar overall health goals, which TTCs threatened.
It is notable that many ASOs adopted policies against receiving tobacco funding relatively early, compared to other charitable sectors; in developing such early policies ASO were earlier identifiers of the ethical issues raised by partnerships with the tobacco industry. ASOs were able to demonstrate leadership regarding the ethics of accepting tobacco industry funding for three reasons. First, as noted above, ASOs began to recognize that the holistic well-being of PWAs required consideration of health issues beyond those specifically related to the virus. Secondly, AIDS organizations benefited from an extensive global network of both grassroots organizations and global institutions that helped to disseminate concerns about the tobacco industry and resulting policies. Finally, by the late 1990s, resources for AIDS were increasing, rising from US$ 292 million spent globally in 1996 to US$ 4630 million in 2003 (Knight, 2008). Therefore, ASOs had access to more resources and greater flexibility around with whom they partnered with.
Rejection of tobacco funding trickled up from ASOs and partner organizations to global forums. During a 2002 retreat to establish the private sector delegation to the GFATM board, it was agreed that TTCs should not be allowed to be members. Meeting minutes from the retreat note that “there are certain industry sectors that could create conflict, such as tobacco industry representatives” (GFATM, 2002). In 2009, the GFATM formalized and expanded this policy, passing a board resolution that prohibited the fund from receiving donations or working in partnerships with TTCs (GFATM, 2010). UNAIDS developed ‘Guidelines on Working in Partnership with the Private Sector’, which recommend “not developing partnerships with entities in sensitive sectors such as tobacco, gambling and pornography” (2007). This stance was reiterated in a 2013 UNAIDS Lancet Commission Discussion paper on ‘How should the global health and AIDS architecture be modernized for the post-2015 development agenda?’ which noted the growing role of TTCs in LMICs, and the need to protect against this influence. It reads, “Public health goals, however, need to be safeguarded against private sector strategies, such as the efforts of tobacco companies to enlarge their markets in low- and middle-income countries” (2013). AIDS organizations were able to draw on their networks and new resources to advance policies against TTC interference in global health forums.
In 2011, the Global Business Coalition on Health (previously the Global Business Coalition on AIDS) decided to prohibit membership to parties with connections to the tobacco industry. It released a statement that read, “the membership of tobacco companies and their parent companies in the Coalition would be inconsistent with, and would contradict GBC's mission and vision.” This was significant as both PM and BAT had been long0time members of the Coalition. It is significant that the coalition developed this policy the same year it changed its name from the ‘Global Business Coalition on AIDS, TB and Malaria’ to ‘Global Business Coalition on Health’. As the organization widened its focus to broader health goals the divisions between health issues such as AIDS and tobacco related illness blurred. It became intolerable to for a health coalition to include members who profited from products that contributed to one of the most pressing global health crisis.
The GBC also noted that it had made the decision to restrict tobacco industry membership in order to align its policies with those of the WHO's FCTC, which strictly limited interactions and partnerships with the tobacco industry. The FCTC, signed by 168 states in 2003, included Article 5.3 on “the protection of public health policies with respect to tobacco control from commercial and other vested interests of the tobacco industry,” which recommended parties, “denormalize and, to the extent possible, regulate activities described as ‘socially responsible’ by the tobacco industry, including but not limited to activities described as ‘corporate social responsibility’.” Although the FCTC, as an intergovernmental treaty, was only binding for signatory states, measures regarding industry influence were adopted by non-state actors, including AIDS organizations, as justification for terminating partnerships with TTCs. The legitimacy of the convention, in turn, was strengthened by compliance of these organizations. Instead of AIDS distracting from the FCTC, as TTCs had hoped, the FCTC increased awareness among AIDS organizations about the need to limit TTC engagement and provided a framework through which to do so.
Furthermore, a number of prominent funders developed supportive policies to limit TTC involvement in global health. The Bill and Melinda Gates Foundation, one of the largest private donors in the global health field, established a policy of not providing funding to organizations that accepted resources from or had connections with the tobacco industry (BMGF, 2010). As the Gates Foundation also funded tobacco control initiatives, it noted that accepting funding from or working in partnership with organizations with links to the tobacco industry would be hypocritical to broader global health goals. In 2010, the foundation pulled funding from the International Research and Development Center (IDRC) – a research institute in Canada that supports organizations in LMICs to implement both AIDS and tobacco control programs – when it found out the Executive Director was also on the Board of Imperial Tobacco Canada. The Gates statement read, “The foundation was recently informed that the chair of the board of our partners, the International Development Research Centre (IDRC), has until recently also been a Director of Imperial Tobacco Canada, Ltd. We are deeply disappointed by this revelation and feel this conflict is unacceptable as we work to support meaningful tobacco control programs in Africa” (BMGF, 2010). This case, which was widely covered in the media, propagated the message that in order to access Gates resources organizations needed to sever all ties with the tobacco industry (see for example Blackwell, 2010; Market Wire, 2010). As the largest private donor to the global AIDS response, donating US$ 2.5 billion to AIDS programs in 2014, the Gates Foundation dwarfed TTC funding and could set the terms of partnerships for AIDS related organizations.
The widespread rejection of tobacco money by civil society organizations, institutions and other private actors in the AIDS response disseminated through global networks. Imperial Tobacco reported dismay, in 2005, when a West African charity it had historically provided funding to for AIDS programs refused its money. The TTC wrote in its Social Responsibility report, “Our efforts for further and more widespread action on AIDS have been impeded by the difficulty of finding a suitable partner to help us. We were saddened that the head office of an international NGO prevented their regional office from partnering us in several developing countries, solely on the grounds of accepting money from a tobacco company” (2005). Overall, by the late 1990s onwards, AIDS organization in the US and then globally turned away from tobacco funding. This was initially prompted by evidence of the harmful health effects of tobacco use on PWAs, but eventually was motivated by recognition of TTCs' use of the AIDS response to further its interest, and supported by the development of shared norms and greater resources. AIDS organizations were early recognizers of the ethical problems of involvement with TTCs. Their stance in turn proved supportive of the FCTC process and adoption of measures limiting industry influence in health programs and policy.
6. TTCs and AIDS in Sub-Saharan Africa
However, TTCs have not been completely shut out of the AIDS response. By 2007, Imperial Tobacco had found another AIDS organization – a French charity called Cinomade – to support in Cote D'Ivor, and continues to fund AIDS programs in Sub-Saharan Africa (Imperial Tobacco, 2007). BAT sponsors AIDS programs in Kenya, Nigeria and South Africa (BAT, 2014; ASH, 2007). Japan Tobacco funds AIDS programs in South Africa and Tanzania (JT, 2013), and Philip Morris gives extensively to AIDS projects in South Africa (PM, 2010; PM, 2011).
TTCs have continued to be active supporters of the AIDS response in Sub-Saharan Africa, despite resistance from some AIDS organizations and global policies discouraging such partnerships, for two reasons. First, the needs of AIDS initiatives in Sub-Saharan Africa remain greater than available resources. Global funding for the AIDS response in LMICs was US$ 19.14 billion in 2013, estimated to be nearly US$ 3 billion short of what will be needed by 2015 (Kates & Wexler, 2014). As a result of stagnated global health resources and continued insufficient domestic resources, many AIDS organizations remain desperate for funding (UNAIDS, 2014). Secondly, many Sub-Saharan African governments have not adopted comprehensive policies to restrict TTC influence. Some states, like Malawi and Zambia, have not signed and ratified the FCTC. Others, such as South Africa and Kenya, while imposing regulations on tobacco product advertising and marketing, do not regulate tobacco industry corporate social responsibility activities (ASH, 2007). The combination of dire need and relatively weak regulations in many Sub-Saharan African countries allow TTCs to continue to participate in the AIDS response.
As a result, TTCs continue to use AIDS projects to improve their image and reputation in Sub-Saharan Africa. They have even been celebrated for their contribution to the African AIDS response. In 2007, BAT sponsored an African–Middle East Conference on AIDS. At the conference the Nigerian Minister of Labor praised BAT's national work-force policy on AIDS, and called on other businesses to implement similar policies (John, 2007). Similarly, the Tanzanian Cigarette Company (a subsidiary of Japan Tobacco International) received a ‘Best Employer’ award in 2010, for AIDS and related programs for workers' health. With no recognition of the contradiction of giving a tobacco company a health related award, Japan Tobacco was commended by the Minister of Defense and National Security, and the Minister of Labor, Youth and Employment (Bitekeye, 2010). It can be argued that such events are contrary to Article 5.3 of the FCTC, which both Nigeria and Tanzania have ratified, because they create venues for government officials and TTC representatives to interact, failing to ‘de-normalize’ relationships between the government and tobacco industry (a recommendation under Article 5.3). Moreover, TTCs use such events and awards to enhance their reputation as ‘good’ corporate citizens, and to indirectly promote tobacco products despite advertising bans.
The continued participation of TTCs in the Sub-Saharan African AIDS response demonstrates that efforts to shut tobacco money and influence out have not been comprehensive. TTCs have redirected their resources where the AIDS response remains desperate for funding and where government tobacco control policies are weak. While TTCs claim to be supporting the AIDS response in Sub-Saharan Africa because of the dire need, and out of the desire to ensure the health of their employees, their past practices of using the AIDS response to subvert tobacco control efforts and market their products raises questions about the motivations behind their current AIDS programs.
Such questions are especially pertinent as rates of tobacco use are on the rise in many Sub-Saharan African countries. Cigarette consumption on the continent almost doubled from just over 40 billion in 1990 to nearly 80 billion in 2010 (Blecher & Ross, 2011). A great portion (9%) of boys smoke than in other developing regions such as South East Asia, and a greater portion of youth (both boys and girls) smoke compared to adults in Sub-Saharan Africa, indicating that smoking prevalence is likely to increase over the next decade (Blecher & Ross, 2011). Such trends suggest that tobacco control efforts are essential to preventing greater tobacco related illness and death in a region already struggling to address numerous other health challenges, such as AIDS.
7. Conclusion
During the early AIDS response in the US, PM provided funding to ASOs in order to support marketing campaigns targeted towards LGBT communities, to enhance its reputation during a time of declining public trust of TTCs, and to argue for the diversion of resources from tobacco control initiatives. TTCs then applied a similar strategy at the global level as the FCTC process accelerated. They capitalized on growing concern about the AIDS epidemics in LMICs – markets they were also expanding into – to argue that WHO should be focusing on AIDS not tobacco control. TTCs aimed to generate competition between health issues, for resources and policy attention, in order to subvert broader public health goals.
However, the collective decision by many AIDS organizations to refuse to let TTCs use the AIDS epidemic to their advantage, demonstrates that health networks can restrict negative or co-opting influences through co-operation. ASOs used information regarding the harms of smoking for PWAs and the suspect practices of TTCs to justify the termination of partnerships with TTCs. Through global networks and the creation of common policies, AIDS organizations pioneered policies that restricted the ability of TTCs to influence global health. These processes were supported by the presence of alternative funding options and a global normative framework. The FCTC, while not binding for non-state actors, provided a set of shared norms AIDS organizations could draw on.
Yet, TTCs remain active in the AIDS response in Sub-Sahara Africa where the gap between resources and needs remains great, and government tobacco control regulations are often weak. Here government ministers and TTCs representatives still share podiums to congratulate each other, while populations continue to suffer from both AIDS and smoking related diseases - two of the most common causes of illness and death worldwide (WHO, 2014).
The history of tobacco industry involvement in the AIDS response suggests a number of policy implications for the both the AIDS and tobacco control responses, as well as broader health governance. The first is that competition between health issues can be exploited by those whose interests run contrary to public health goals; TTCs used the AIDS epidemic to try a divert resources from tobacco. Therefore, it is by recognizing the links between health issues, and developing mutually supportive policies, such as those implemented by AIDS organizations that reflect Article 5.3 of the FCTC, that holistic health goals can be achieved. Secondly, other organizations may learn from and build on the policies regarding corporate donations from TTCs pioneered by AIDS organizations. Further research could consider how other organizations, or charitable sectors, that are targeted by funding from corporations that impeded other health goals, address such ethical dilemmas. Finally, AIDS organizations were able to restrict TTC influence where they were supported by sufficient financial resources and have a shared normative framework to draw upon. Therefore, efforts need to be made to replace TTC funding to the AIDS response in Sub-Saharan Africa with alternative resources, and to encourage states and organizations to implement policies that reflect Article 5.3 of the FCTC. Such coordination will benefit the AIDS response, tobacco control initiatives and, most importantly, those individuals and communities most affected by ill health.
Acknowledgments
This research is funded by the National Cancer Institute, US National Institutes of Health under award number R01-CA091021; The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the funders.
Contributor Information
Julia Smith, Postdoctoral Fellow in the Faculty of Health Sciences, Simon Fraser University, Burnaby, Canada.
Sheryl Thompson, Research Assistant in the Faculty of Health Sciences, Simon Fraser University, Burnaby, Canada.
Kelly Lee, Professor in Global Health in the Faculty of Health Sciences, Simon Fraser University, Burnaby, Canada and a Professor in Global Health Policy, Department of Global Health and Development, London School of Hygiene & Tropical Medicine.
References
- Act-Up. AIDS Activists Announce Boycott of Marlboro Cigarettes Legacy Tobacco Documents Library (Bates # 2024262561-2024262563) University of California; San Francisco: 1990. Apr 12, [Google Scholar]
- Action on Smoking and Health. BAT's African Footprint. 2007 Retrieved from http://www.ash.org.uk/information/tobacco-industry/bats-african-footprint.
- Ashley MJ. What the public thinks about the tobacco industry and its products. Tobacco Control. 2003;12(4):396–400. doi: 10.1136/tc.12.4.396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balbach E, Smith E, Malone R. How the health belief model helps the tobacco industry: individuals, choice, and “information”. Tobacco Control. 2005;15(4):37–43. doi: 10.1136/tc.2005.012997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BAT. Sustainability Report. 2014 Retrieved from http://www.bat.com/group/sites/UK__9D9KCY.nsf/vwPagesWebLive/DO964UGU/$file/Supporting_farmers'_livelihoods_-_The_opportunity_2014.pdf.
- BAT. The WHO Framework Convention on Tobacco Control, 2000 Documents Library (Bates # 760028654-760028657) University of California; San Francisco: 2000. [Google Scholar]
- BAT. Documents Library (Bates # 321324291-321324477) University of California; San Francisco: 1998. Sep 25, Corporate and Regulatory Affairs: Company Plan 1999 – 2001. [Google Scholar]
- BAT (undated): 8th International Conference on Tobacco and Health Proposed Possible Action to Take Against It Legacy Tobacco Documents Library (Bates number 321651588-321651593) University of California; San Francisco: [Google Scholar]
- Bayer R, Fairchild A. Changing the Paradigm For HIV Testing-The End of Exceptionalism. The New England Journal of Medicine. 2006;355(7):647–649. doi: 10.1056/NEJMp068153. [DOI] [PubMed] [Google Scholar]
- Bitekeye A. Tanzania: Cigarette Company Wins 2010 Best Employer Award. All Africa. 2010 Jul 3; Retrieved from http://allafrica.com/stories/201007051061.html.
- Blackwell R. Gates charity cuts funding to Canadian anti-smoking project in Africa. The Globe and Mail. 2010 Apr 12; Retrieved from http://www.theglobeandmail.com/news/world/gates-charity-cuts-funding-to-canadian-anti-smoking-project-in-africa/article1373518/
- Blecher E, Ross H. Tobacco Use in Africa: Tobacco Control Through Prevention. Oklahoma: American Cancer Society; 2011. [Google Scholar]
- Bill and Melinda Gates Foundation. AIDS Strategy Overview. 2014 Retrieved from http://www.gatesfoundation.org/What-We-Do/Global-Health/HIV.
- Bill and Melinda Gates Foundation. Statement Regarding IDRC Grant. 2010 Retrieved from http://www.gatesfoundation.org/Media-Center/Press-Releases/2010/04/Statement-Regarding-IDRC-Grant.
- MacKenzia R, Collin J. Philanthropy, politics and promotion: Philip Morris' “charitable contributions” in Thailand. Tobacco Control. 2008;17:284–285. doi: 10.1136/tc.2008.024935. [DOI] [PubMed] [Google Scholar]
- Dastugue J. 8th World Conference on Tobacco and Health British Legacy Tobacco Documents Library (Bates # 304058392-304058395) University of California; San Francisco: 1992. Jan 13, [Google Scholar]
- Dieleman JL, Graves CM, Templin T, Johnson E, Baral R, Leach-Kemon K. Global Health Development Assistance Remained Steady In 2013 But Did Not Align With Recipients' Disease Burden. Health Affairs. 2014;33(5):878–886. doi: 10.1377/hlthaff.2013.1432. [DOI] [PubMed] [Google Scholar]
- Drabble Laurie. The Ethics of Tobacco, Alcohol, & Pharmaceutical Funding A Practical Guide for LGBT Organizations. Washington D.C: Coalition of Lavender Americans on Smoking Health; 1999. [Google Scholar]
- Drabble Laurie. Alcohol, Tobacco, and Pharmaceutical Industry Funding: Considerations for Organizations Serving Lesbian, Gay, Bisexual, and Transgender Communities. Journal of Gay & Lesbian Social Services. 2000;11(1):1–26. [Google Scholar]
- Fee E. Understanding AIDS: Historical Interpretations and the Limits of Biomedical Individualism Interpretations. American Journal of Public Health. 1995;83(10):1477–1486. doi: 10.2105/ajph.83.10.1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flanagan W, Whiteman G. “AIDS is Not a Business”: A Study in Global Corporate Responsibility – Securing Access to Low-cost HIV Medications. Journal of Business Ethics. 2007;73(1):65–75. [Google Scholar]
- Fooks G, Gilmore A, Collin J, Holden C, Lee K. The Limits of Corporate Social Responsibility: Techniques of Neutralization, Stakeholder Management and Political CSR. Journal of Business Ethics. 2013;112(2):283–299. doi: 10.1007/s10551-012-1250-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furber AS, Maheswaran R, Newell JN, Carroll C. Is smoking tobacco an independent risk factor for HIV infection and progression to AIDS? A systemic review. Sexually Transmitted Infections. 2006;83(1):41–46. doi: 10.1136/sti.2005.019505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Global Business Coalition for Health. GBC Statement on Tobacco Industry Membership. 2011 Retrieved from http://archive.gbchealth.org/news-article/1551/
- Global Fund to Fight AIDS, TB and Malaria. Overview Of Corporate Risks Assigned To Committee Oversight. 2010 Retrieved from http://www.theglobalfund.org/en/board/meetings/twentyfirst/
- Global Fund to Fight AIDS, TB and Malaria. Private Sector Consultation Meeting. 2002 Retrieved from http://www.theglobalfund.org/documents/board/twg/Board_TWGPrivateSectorConsultMeetingRecommendations_Report_en/
- Goebel K. Lesbians and Gays Face Tobacco Targeting. Tobacco Control. 1994;3:65–67. [Google Scholar]
- Hallmark. Tobacco Growers Meet WHO for First Time Legacy Tobacco Documents Library (Bates # 321356911) University of California; San Francisco: 1999. Apr, [Google Scholar]
- Imperial Tobacco. Corporate Responsibility Review. 2005 Retrieved from http://www.imperial-tobacco.com/files/environment/cr2005/index.asp?pageid=57.
- Imperial Tobacco. Corporate Responsibility Review. 2007 Retrieved from http://files.the-group.net/library/itg/crreport2007/pdfs/itgcr07_cratimperialtobacco.pdf.
- ITGA. The case for additional industry support Legacy Tobacco Documents Library (Bates # 321324291-321324477) University of California; San Francisco: 1998. Sep 25, [Google Scholar]
- ITGA Malawi. The Economic Social Council Meeting Legacy Tobacco Documents Library (Bates # 321356066-321356132) University of California; San Francisco. New York: 2000. Aug 01, [Google Scholar]
- Japan Tobacco. Corporate Social Responsibility Report. 2013 Retrieved from http://www.jt.com/csr/report/pdf/report2013.pdf.
- John Moses. Nigeria: Minister Warns Against Stigma On AIDS in Workplace. Abuja. AllAfrica. 2007 Sep 25; Retrieved from allafrica.com/stories/200709250520.
- Kates J, Wexler A. Financing the Response to HIV in Low- and Middle-Income Countries: International Assistance from Donor Governments in 2013. Geneva: Kaiser Family Foundation and UNAIDS; 2014. [Google Scholar]
- Knight L. UNAIDS: The First 10 Years, 1996-2007. Geneva: UNAIDS; 2008. [Google Scholar]
- La Penza. Se Realizo el lanzamiento del programa ‘El SIDA esta aqui.’. 1992 Apr 03;:7. [Google Scholar]
- Lee K. The governance of global tobacco control. In: McInnes C, Le K, Rushton S, Kamradt-Scott A, Williams O, Roemer-Mahler A, editors. Transformations in Global Health Governance. London: Palgrave Macmillan; 2014. pp. 59–77. [Google Scholar]
- Lee M, Kohler J. Benchmarking and Transparency: Incentives for the Pharmaceutical Industry's Corporate Social Responsibility. Journal of Business Ethics. 2010;95(4):641–658. [Google Scholar]
- Leisinger K. The Corporate Social Responsibility of the Pharmaceutical Industry: Idealism without Illusion and Realism without Resignation. Business Ethics Quarterly. 2005;15(4):577–594. doi: 10.5840/beq200515440. [DOI] [PubMed] [Google Scholar]
- Lewis R. Dear Senator Helms Legacy Tobacco Documents Library (Bates # TI49492240-TI49492241) University of California; San Francisco: 1989. Jan 03, [Google Scholar]
- Lordan Gr, Ki Tang K, Carmignani F. Has AIDS displaced other health funding priorities? Evidence from a new dataset of development aid for health. Social Sciences and Medicine. 2011;73(3):351–355. doi: 10.1016/j.socscimed.2011.05.045. [DOI] [PubMed] [Google Scholar]
- MacKenzie R, Collin J, Lee K. The tobacco industry documents: an introductory handbook and resource guide for researchers. London: London School of Hygiene & Tropical Medicine; 2003. [Google Scholar]
- Maguire J. Thank You For Continuing To Be The Champion Of The Tobacco Industry Legacy Tobacco Documents Library (Bates # 518698402) University of California; San Francisco: 1993. Mar 10, [Google Scholar]
- Mamudu Hadii M, Hammond Ross, Glantz Stanton. Tobacco Industry Attempts to Counter the World Bank Report Curbing the Epidemic and Obstruct the WHO Framework Convention on Tobacco Control. Social Science & Medicine. 2008;67(11):1690–1699. doi: 10.1016/j.socscimed.2008.09.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Market Wire. Gates Foundation pulls funding from IDRC due to ties to Big Tobacco. 2010 Apr 12; Retrieved from http://www.marketwired.com/press-release/gates-foundation-pulls-funding-from-idrc-due-to-ties-to-big-tobacco-1146077.html.
- McCoy David, Kembhavi Gayatri, Patel Jinesh, Luintel Akish. The Bill & Melinda Gates Foundation's grant-making program for global health. The Lancet. 2009;373(9675):1645–1653. doi: 10.1016/S0140-6736(09)60571-7. [DOI] [PubMed] [Google Scholar]
- McDaniel PA. Philip Morris's Project Sunrise: Weakening Tobacco Control by Working with it. Tobacco Control. 2006;15(3):215–223. doi: 10.1136/tc.2005.014977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGovern P. The Tobacco Institute Check Request Legacy Tobacco Documents Library (Bates # TI49492257-TI49492258) University of California; San Francisco: 1987. [Google Scholar]
- Muggli M, Lee K, Gan Q, Ebbert J, Hurt RD. Efforts to Reprioritize the Agenda in China: British American Tobacco's Efforts to Influence Public Policy on Secondhand Smoke in China. Plos Med 5. 2008;12:1729–1736. doi: 10.1371/journal.pmed.0050251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muggli ME, Hurt RD. Tobacco Industry Strategies to Undermine the 8th World Conference on Tobacco or Health. Tobacco Control. 2003;12:195–202. doi: 10.1136/tc.12.2.195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NAF. Philip Morris Corporate Contributions Organization Details Legacy Tobacco Documents Library (Bates # 2041047771/2041047778) University of California; San Francisco: 1996. Feb 14, [Google Scholar]
- NAF. 2007 Annual Report. Washington D.C.: National AIDS Fund. 2007 Retrieved from http://www.lphi.org/LPHIadmin/uploads/2007_National_AIDS_-Fund_Annual_Report-50547.pdf.
- Offen N. The Parametric Boycott: A Tool for Tobacco Control Advocacy. Tobacco Control. 2005;14(4):272–277. doi: 10.1136/tc.2005.011247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Offen N, Smith E, Malone R. Is Tobacco a Gay Issue? Interviews with leaders of the lesbian, gay, bisexual and transgender community. Culture, Health & Sexuality. 2008;10(2):143–157. doi: 10.1080/13691050701656284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Opukah S. ITGA Legacy Tobacco Documents Library (Bates # 321357049) University of California; San Francisco: 1999. Jun 01, [Google Scholar]
- Opukah S. ITGA Meetings Legacy Tobacco Documents Library (Bates # 321357124) University of California; San Francisco: 1999. Feb 18, [Google Scholar]
- Out Magazine. Companies that Care. 1998 Retrieved from http://www.trinketsandtrash.org/detail.php?artifactid=4906&page=1.
- Pisani E. The Wisdom of Whores: Bureaucrats, Brothels, and the Business of Aids. London: Grata; 2008. [Google Scholar]
- PM. Legacy Tobacco Documents Library (Bates # 2023004617-2023004751) University of California; San Francisco: 1992. Briefing Book, Annual Meeting 1992. [Google Scholar]
- PM. NAF Statement RE Legacy Tobacco Documents Library (Bates # 2070055109-2070055113) University of California; San Francisco: 1994. Nov, [Google Scholar]
- PM. AIDS Related Grants Legacy Tobacco Documents Library (Bates # 2044025192-2044025202) University of California; San Francisco: 1995. Dec 14, [Google Scholar]
- PM. Philip Morris Companies Inc Corporate Affairs: Todays Topics Legacy Tobacco Documents Library (Bates # TI13601704) University of California; San Francisco: 1998. Jun 02, [Google Scholar]
- PM (1999/ 01/23) Sunrise Project Legacy Tobacco Documents Library (Bates # 2078018410-2078018475) University of California; San Francisco: [Google Scholar]
- PM (2000/06) Philip Morris Use Corporate Reputation: Benchmark Study Legacy Tobacco Documents Library (Bates # 2080986506-2080986528) University of California; San Francisco: [Google Scholar]
- PM. Charitable Donations. 2010 Retrieved from http://www.pmi.com/eng/about_us/corporate_contributions/pages/corporate_contributions.aspx.
- PM. Charitable Contributions. 2011 Retrieved from http://www.pmi.com/eng/about_us/corporate_contributions/pages/corporate_contributions.aspx.
- Poku N. AIDS in Africa: How the poor are dying. London: Polity Press; 2006. [Google Scholar]
- PR Newswire. Philip Morris Magazine Launches Ad Campaign Legacy Tobacco Documents Library (Bates # 2023257881) University of California; San Francisco: 1988. Jun 28, [Google Scholar]
- PR Newswire. Legacy Tobacco Documents Library (Bates # 321356987) University of California; San Francisco: 1999. Mar 2, Tobacco Growers Leaders Meet WHO. [Google Scholar]
- Ramiah I, Reich M. Building effective public–private partnerships: Experiences and lessons from the African Comprehensive AIDS Partnerships (ACHAP) Social Science & Medicine. 2006;63(2):397–408. doi: 10.1016/j.socscimed.2006.01.007. [DOI] [PubMed] [Google Scholar]
- Rimmer L. BAT in its own words. London: Action on Smoking and Health / Christian Aid / Friends of the Earth; 2005. [Google Scholar]
- Roemer R, Taylor A, Lariviere J. Origins of the WHO Framework Convention on Tobacco Control. American Journal of Public Health. 2005;95(6):936–938. doi: 10.2105/AJPH.2003.025908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenberg N, Siegel M. Use of Corporate Sponsorship as a Tobacco Marketing Tool: A Review of Tobacco Industry Sponsorship in the USA, 1995-99. Tobacco Control. 2001;10:239–246. doi: 10.1136/tc.10.3.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sridhar D, Batniji R. Misfinancing global health: a case for transparency in disbursements and decision making. The Lancet. 2006;372(964)(4):1185–1191. doi: 10.1016/S0140-6736(08)61485-3. [DOI] [PubMed] [Google Scholar]
- Slavitt J. Public Policy Plan Draft Legacy Tobacco Documents Library (Bates # 2070437692-2070437704) University of California; San Francisco: 1996. Dec 12, [Google Scholar]
- Smith Elizabeth A, Malone Ruth E. The Outing of Philip Morris: Advertising Tobacco to Gay Men. American Journal of Public Health. 2003;93(6):988–993. doi: 10.2105/ajph.93.6.988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith RA, editor. Global AIDS Politics, Policy and Activism: Persistent Challenges and Emerging Issues. 1-3. Santa Barbra: Praeger Publishers; 2013. [Google Scholar]
- Stevens P, Carlson L, Hinman J. An Analysis of Tobacco Industry Marketing to Lesbian, Gay, Bisexual, and Transgender (LGBT) Populations: Strategies for Mainstream Tobacco Control and Prevention. Health Promotion and Practice. 2004;5(3):129S–134S. doi: 10.1177/1524839904264617. [DOI] [PubMed] [Google Scholar]
- Stevens P, Carlson L, Hinman J. An Analysis of Tobacco Industry Marketing to Lesbian, Gay, Bisexual, and Transgender (LGBT) Populations: Strategies for Mainstream Tobacco Control and Prevention. Health Promotion and Practice. 2004;5(3):129–134. doi: 10.1177/1524839904264617. [DOI] [PubMed] [Google Scholar]
- Stone M, Siegel M. Tobacco Industry Sponsorship of Community-Based Public Health Initiatives: Why AIDS and Domestic Violence Organizations Accept or Refuse Funds. Journal of Public Health Management Practice. 2004;10(6):511–517. doi: 10.1097/00124784-200411000-00007. [DOI] [PubMed] [Google Scholar]
- Summers T, Kates J. Trends in U S Government Funding for AIDS Fiscal Years 1981 to 2004. Washington D.C: Kaiser Family Foundation; 2004. [Google Scholar]
- Tobacco Tactics. International Tobacco Growers Association. 2014 Retrieved from http://www.tobaccotactics.org/index.php/International_Tobacco_Growers_Association.
- UNAIDS; 1998. Global Report on the AIDS Epidemic. Retrieved from http://data.unaids.org/pub/Report/1998/19981125_global_epidemic_report_en.pdf. [Google Scholar]
- UNAIDS; 2007. Guidelines on Working in Partnership with the Private Sector. Retrieved from http://data.unaids.org/pub/manual/2007/unaids_guidelines_august2007_draft4_en.pdf. [Google Scholar]
- UNAIDS; Geneva: 2014. The Gap Report. Retrieved from http://www.unaids.org/en/resources/campaigns/2014/2014gapreport/gapreport. [Google Scholar]
- UNAIDS & the Lancet Commission. Geneva: 2013. How should the global health and AIDS architecture be modernized for the post-2015 development agenda? Retrieved from http://www.ucl.ac.uk/igh/events/Workshop-Report-UNAIDS. [Google Scholar]
- US Senate. AIDS Control Act. 1987 Retrieved from http://thomas.loc.gov/cgi-bin/bdquery/D?d100:11:./temp/∼bd5lnx::
- WHO. Framework Convention on Tobacco Control. 2003 Retrieved from http://www.who.int/fctc/text_download/en/
- WHO. World Report on Global Tobacco Epidemic. 2008 Retrieved from http://www.who.int/tobacco/mpower/mpower_report_full_2008.pdf.
- WHO. Geneva: 2014. Tobacco Free Initiative: Tobacco Facts. Retrieved from http://www.who.int/tobacco/mpower/tobacco_facts/en/ [Google Scholar]
- Williams O, Rushton S. Partnerships and foundations in global health governance. New York: Palgrave Macmillan; 2011. [Google Scholar]