

Abstract
Background and Purpose
To minimize the variance in CBV measurements made with DSC-MRI, the optimal echo time must be calculated. Simulations can be used to determine the influence of TE on CBV but may not adequately recapitulate the in vivo heterogeneity of pre-contrast T2*, contrast agent (CA) kinetics, and biophysical basis of CA induced T2* changes. With multi-echo based DSC-MRI acquisitions, voxel-wise pre-and post-contrast T2* changes can be quantified and used to compute the optimal TEs for traditional single-echo acquisitions.
Materials and Methods
Eleven subjects with high-grade gliomas were scanned at 3T with a dual-echo DSC-MRI sequence to quantify CA induced T2* changes in this retrospective study. Optimized TEs were calculated using propagation of error analysis for high-grade glial tumors, normal appearing white matter (NAWM), and arterial input function (AIF) estimation.
Results
The optimal TE is a weighted-averaged of the T2* values that occur as a CA bolus transverses a voxel. The mean optimal TEs were 30.0 ± 7.4 ms for high-grade glial tumors, 36.3 ± 4.6 ms for NAWM, and 11.8 ± 1.4 ms for AIF estimation (repeated measures ANOVA p<0.001).
Conclusion
Greater heterogeneity was observed in the optimal TE values for high-grade gliomas and mean values of all three ROIs were statistically significant. The optimal TE for the AIF estimation is much shorter implying that quantitative DSC-MRI acquisitions would benefit from multiple echo acquisitions. In the case of a single-echo acquisition, the optimal TE prescribed should be 30-35 ms (without a preload) and 20-30 ms (with a standard full-dose preload).
Introduction
Dynamic susceptibility contrast (DSC) MRI is increasingly used to map cerebral blood volume (CBV) in brain tumor patients owing to its potential to predict treatment response, improve image-guided biopsies, and to differentiate post-treatment radiation effects and glioma progression.1–9
CBV is typically acquired using a dynamic susceptibility contrast (DSC) MRI by tracking the gadolinium-based contrast agent (CA) induced T2* changes over time. To optimally capture the MR signal changes due to the T2* changes, an optimal echo time (TE) must be prescribed during the acquisition. Previous studies have used simulations to determine optimal TEs for spin-echo (SE) based DSC-MRI10; however, it is to the best of our knowledge that an optimal TE has not been determined for a gradient-echo (GRE) based DSC-MRI. Recently, the American Society of Functional Neuroradiology (ASFNR) recommended GRE-based DSC-MRI for brain tumor imaging because of the higher signal to noise, better sensitivity and more uniform vessel size sensitivity compared to SE.11 Accordingly, it is important to determine an optimal TE for GRE-based DSC-MRI.
Optimal echo times have been previously suggested in the literature. Willats et al. have suggested that the optimal echo time should be on the order of expected T2* values before CA administration.12,13 In contrast, Boxerman et al. demonstrated, using propagation of error analysis, that the optimal echo time should be a weighted-average of the pre-contrast and post-contrast T2* values, although did not recommend a specific TE.10 It has also been noted that the optimal TE in a DSC experiment is most likely different for voxels used to identify the arterial input function (AIF) and normal appearing white matter (NAWM) due to the higher contrast agent concentration encountered within arteries and the associated potential signal saturation.14
While simulations and error analysis can be used to systematically investigate the influence of TE on CBV accuracy, they cannot recapitulate in vivo heterogeneity of pre-contrast T2*, CA kinetics, and biophysical basis of CA induced T2* changes. With multi-echo based DSC-MRI acquisitions, voxel-wise T2* values, before and after CA administration, can be quantified across tissue types by assuming a mono-exponential decay. The goal of this study was to combine quantitative multi-echo DSC-MRI T2* time curves with propagation of error analysis to compute the optimal GRE TEs for high-grade glial tumors, NAWM, and AIF estimation.
Materials and Methods
Theory
During the contrast agent (CA) bolus passage in a DSC-MR scan, the T2* of the perfused voxel changes over time. From the literature, it is assumed that this change in the transverse relaxation rate, ΔR2*(t) = 1/ΔT2*(t), is linear with CA concentration, and therefore the rCBV can be approximated by:
| (Eq. 1) |
Assuming a single echo acquisition, ΔR2*(t) is:
| (Eq. 2) |
Here R20* is the baseline apparent transverse relaxation rate before contrast arrival. The generalized signal equation, after contrast agent injection, for a spoiled gradient echo acquisition is:
| (Eq. 3) |
For simplification, the constant η includes all the terms that are independent of TE.
If we assume that the baseline (pre-contrast) signal points are acquired with sufficient signal-to-noise ratio (SNR), we note that the variance in the apparent transverse relaxation is mainly due to the variance in the signal over time. Applying propagation of error to Eq. 2, the variance in R2*(t) is:
| (Eq. 4) |
where k is a proportionality constant. Similar to the approach taken by Boxerman et al.10 the variance in a CBV measurement can then be determined by:
| (Eq. 5) |
Lastly, to determine the optimal TE that minimizes the variance in CBV measurements the derivative of Eq. 5 is taken with respect to TE and solved when equal to zero:
| (Eq. 6) |
The optimal TE can now be solved numerically from Eq. 6. Note that the optimal TE is, essentially, the weighted average of T2* values during the contrast agent passage (illustrated by Figure 1).
Figure 1.
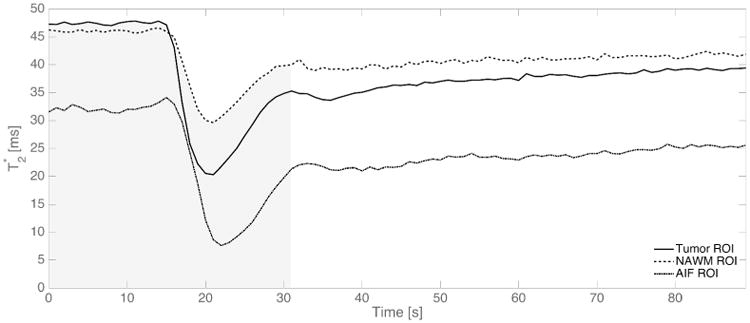
An example from one patient of the absolute T2* time curves for tumor (solid), NAWM (dash dash), and the AIF (dash dot) ROI. As described in Eq. 6, the optimal TE is proportional to the weighted average of absolute T2* values during the first pass (as indicated by the shaded gray area) of the contrast agent.
MRI Protocol
This manuscript is a retrospective analysis from two separate subject cohorts both approved by their institutional review board (IRB). Both cohorts of patients had World Health Organization grade III and IV primary high-grade gliomas undergoing preoperative imaging for surgical re-section. All patients exhibited contrast-enhancing lesions.
We analyzed two separate subject cohorts in order to evaluate optimal TE values in scans acquired with and without a contrast agent preload. In the clinic, a preload ranging from 0.025 to 0.1 mmol/kg is typically administered 6 minutes prior to the DSC imaging to reduce CA-induced T1 leakage effects. The first cohort of subjects was used for calculation of optimal TE (described in detail below) without a preload. The second cohort of subjects were scanned with multi-echo DSC-MRI for 7.5 minutes making it an ideal dataset to quantify T2* changes 6 minutes after contrast agent injection, mimicking a preload situation in the clinic. These results allowed us to understand how a preload would affect the calculated optimal TE.
The first subject cohort consisted of eleven datasets randomly selected from an on-going study (average age: 49.9 ± 12.9 years; 7 males, 4 females). Each subject was scanned on a single 3T MR imaging system (Signa HDx; GE Healthcare, Milwaukee, Wisconsin) using a dedicated 8-channel phased array brain coil. A 2D single-shot dual-echo spiral DSC sequence was used with the following parameters: TR/TE1/TE2 = 1000/5.6/28 ms, flip angle = 60 degrees, FOV = 22 × 22 cm, slice thickness = 5 mm, slice spacing = 0 mm, number of slices = 16, and an acquired matrix = 128 (frequency) × 128 (phase). Gadobenate dimeglumine (MultiHance; Bracco Diagnostics Inc., Germany) was administered at 0.1 mmol/kg (a standard dose), using a power-injector for each perfusion scan at a rate of 5 mL/s. The injection occurred 20 seconds after the start of the DSC scan, and the total length of the scan was 3 minutes. Lastly, T1-weighted spoiled gradient echo images were acquired (TR/TE = 6.7/2.8 ms, flip angle = 13 degrees, FOV = 32 × 24 cm2, slice thickness = 2 mm, acquired resolution = 0.51 × 0.51 × 2 mm3) after the perfusion scan to delineate enhancing tumor and NAWM region-of-interests (ROIs).
The second subject cohort consisted of five datasets (average age: 47.0 ± 7.2 years; 3 males, 1 female) acquired using a combined spin- and gradient-echo (SAGE) DSC sequence. Each subject was scanned on a single 3T MR imaging system (Achieva, Philips Healthcare, Best, Netherlands) using a 32-channel head coil. A 2D single-shot SAGE DSC sequence with used with the following parameters: 2 gradient-echo, 2 asymmetric spin-echo, and 1 true spin-echo, TR = 1800 ms, TE1 – TE5 = 8.8/26/55/72/90 ms, flip angle = 90 degrees, FOV = 24 × 24 cm2, slice thickness = 5 mm, slice spacing = 0 mm, number of slices = 15, and an acquired matrix = 76 (frequency) × 76 (phase). Partial Fourier encoding and SENSE (acceleration factors 0.73 and 2.0, respectively) were used to obtain acceptable echo times. Gadopentetate dimeglumine (Magnevist; Bayer AG., Germany) was administered at 0.1 mmol/kg (a standard dose), using a power injector at a rate of 4 ml/s. The injection occurred 60 seconds after the start of the DSC scan, and the total length of the scan was 7.5 minutes long. Lastly, 3D T1-weighted spoiled gradient echo images were acquired (TR/TE = 8.9/4.6 ms, flip angle = 9 degrees, FOV = 25.6 × 25.6 × 17.0 cm3, acquired resolution = 1 × 1 × 1 mm3) after the perfusion scan to delineate enhancing tumor and NAWM region-of-interests (ROIs).
Post Processing for Optimal TE calculation
The T1-weighted, anatomical data were co-registered to the DSC perfusion data using rigid registration with FMRIB Software Library (FSL).15 The DSC perfusion data were analyzed using MATLAB (Mathworks, Natick, Massachusetts).
From both the dual-echo spiral and SAGE DSC sequence, R2*(t) was calculated voxel-by-voxel by assuming a mono-exponential decay in T2*16:
| (Eq. 7) |
With this information the optimal TE was calculated by numerically solving Eq. 6 over the first-pass of CA. In order to determine the temporal duration of the first-pass, the mean whole brain (WB) ΔR2*(t) was first calculated to determine the mean peak time point. The slope of the WB ΔR2*(t) was then calculated. A positive slope indicated wash-in of CA, whereas a negative slope indicated wash-out, and a slope of 0 no change in CA. Starting at the peak time point, the time point in which the slope equaled 0 was identified and set as the end of the first passage. The first passage of CA was approximately 22.5 seconds from the time of injection across all subjects (see Fig. 1 for an illustrative example of the first-pass integration limits).
Three ROIs were used for analysis: tumor, NAWM, and voxels selected for AIF estimation. The tumor and NAWM ROI were selected using k-means clustering with data partitioned into four clusters using the T1-weighted, anatomical data (Supplementary Figure 1). The largest centroid value (brightest signal intensities) consisted of the enhancing tumor along with other unwanted regions such as fat around the skull and eyes. The enhancing tumor was manually selected slice by slice to separate it from the unwanted regions. The NAWM mask was determined by the second largest centroid value. Finally, voxels with the selected ROIs exhibiting a signal drop of at least 5 standard deviations from the baseline pre-contrast signal were used for analysis to ensure sufficient contrast-to-noise for the time curves. The AIF was identified on the DSC perfusion dataset using previously established automated algorithms.17,18 This automatic AIF algorithm typically selects AIF pixels in the internal carotid artery, vertebral artery, and middle cerebral artery. All ROI selections were approved by an investigator with over 15 years of experience in brain tumor imaging (C.C.Q).
In addition to the above measurements and calculations, we calculated T2* 6 minutes after the CA injection from the second cohort of subjects. The percent difference in T2* (1/R2*) between pre-contrast T2* (t = 0) and post-contrast (t = 6 minutes) was calculated to determine the potential effect of a standard dose (0.1 mmol/kg) preload on the measured baseline T2* values in a DSC scan. The estimated optimal TE with a preload was then calculated by scaling the calculated optimal TE without a preload by the percent difference in T2*.
Statistical Analysis
Mean optimal TE values were compared across tumor, NAWM, and AIF ROIs using a multivariate approach to a repeated measures analysis of variance (ANOVA) with post-hoc pairwise comparisons using paired t-tests. With 11 subjects, this study had an 80% power to detect a 0.94 standard deviation difference between a pair of ROIs with a two-side alpha = 0.05 paired t-test. To test for mean differences in the minimum T2* of the two cohorts of subjects imaged, a Student's unpaired t-test was performed. Statistical significance was detected for a p-value < 0.05.
Results
Figure 1 illustrates a typical T2* time curve for a single patient in the tumor, NAWM, and AIF. Figure 2 summarizes the baseline and minimum T2* along with the corresponding optimal TE across all 11 subjects from the first cohort of subjects. Mean optimal TE values (mean ± 1 standard deviation) were 30.0 ± 7.4 ms for tumor, 36.3 ± 4.6 ms for NAWM, and 11.8 ± 1.4 ms for AIF (repeated measures ANOVA p<0.001; post-hoc paired t-tests: tumor vs. NAWM p=0.005, tumor vs. AIF p<0.001, NAWM vs. AIF p<0.001). Tumor ROIs exhibited a wide range of optimal TE values as compared to healthy tissue. In all ROIs mean optimal TE values were closer to the minimum T2* than the baseline values.
Figure 2.
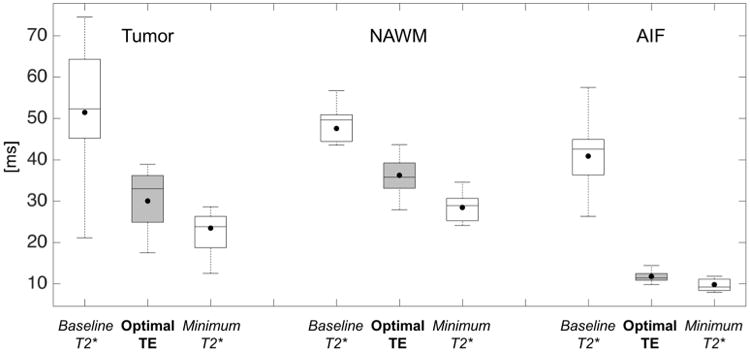
Boxplot representation of baseline and minimum T2* values (white boxplots) along with their respective calculated optimal TE (gray boxplots) in the brain tumor, NAWM, and AIF. Baseline T2* is defined as the T2* of the ROI before contrast arrival and minimum T2* is defined as the T2* value at the peak signal drop. Solid lines represent median values whereas solid dots represent means across subjects in these boxplots.
Results from the second cohort of subjects indicate that the mean tumor T2* was 35% lower than baseline 6 minutes after the CA injection. Additionally, the mean NAWM and AIF T2* were 15% and 10%, respectively, lower than baseline. Assuming each regions' respective percent decrease in T2* 6 minutes after CA injection and the optimal TE results from the first cohort of subjects presented above, the estimated mean optimal TE values with a standard preload dose were 19.5 ± 4.8 ms for tumor, 30.8 ± 3.9 ms for NAWM, and 10.6 ± 1.3 ms for AIF.
In order to apply the results of the second to the first cohort of subjects, the concentration of gadolinium between the populations must be similar. Since concentration of gadolinium is proportional to ΔR2* we estimated the similarity between cohorts by comparing the peak ΔR2* change. The mean peak ΔR2* for the first vs. second cohort of subjects was 22.9 ± 12.9 ms vs. 23.7 ± 10.8 ms for tumor (p-value = 0.90), 14.3 ± 4.2 ms vs. 12.9 ± 5.8 ms for the NAWM (p-value = 0.65), and 94.5 ± 18.3 ms vs. 103.2 ± 30.6 ms for the AIF (p-value = 0.40).
Discussion
This study determined the optimal TE for a typical single-echo DSC-MRI acquisition by minimizing the variance in CBV. Using error analysis, we determined that the optimal TE is a weighted-average of T2* values that occur before and after the CA passage and was found to be dependent upon ROI type.
For an imaging protocol employing no preload dose and a standard injection dose at 3T, the optimal TE in brain tumor is 30.0 ± 7.4 ms. The larger range of optimal TEs in the tumor regions is expected given the greater variability of blood volume values and CA-induced T2* leakage effects both within and across subjects.19 The optimal TEs for NAWM is roughly 20% longer (optimal TE = 36.3 ± 4.6 ms) than that found in the tumor. The optimal TE for the AIF is roughly 300% shorter (optimal TE = 11.8 ± 1.4 ms) than that found in tumor. For an imaging protocol employing both a standard preload and injection dose at 3T, we estimated the optimal TE in brain tumor to be 19.5 ± 4.8 ms. The estimated optimal TE for NAWM is roughly 65% longer (optimal TE = 30.8 ± 3.9 ms) than that found in the tumor. The optimal TE for the AIF is roughly 200% shorter (optimal TE = 10.6 ± 1.3 ms) than that found in tumor. Since a statistically significant difference was detected between the optimal TEs for each of the three regions for both imaging options (no preload and preload), multi-echo acquisitions are warranted for quantitative DSC-MRI studies requiring use of the AIF supporting previously hypothesizes in the literature.20
To quantify T2* values throughout the passage of CA in the selected ROIs, we analyzed data from dual-echo spiral acquisition. The dual-echo data is advantageous because the influence of CA-induced T1 changes that may be present in blood or in situations in which the blood brain barrier has been compromised are removed.16 Additionally, the calculation of T2* based on dual-echo data is computationally simple. While more echo times could potentially improve the T2* quantification, Stokes et al. have shown that T2* measurements derived from two echoes is consistent with those derived from a five echo acquisition.21 Our reported quantitative T2* values for NAWM (47.5 ± 6.8 ms) are within the range previously reported in literature: 48.4 ms21, 49 ms22, 50 ± 8 ms23, and 67.6 ± 11.0 ms20. However, comparison of the quantitative T2* values for the AIF in this study with those in literature (e.g. bulk arterial blood T2*) is difficult because the voxels used to estimate the AIF likely contain brain tissue and arteries due to partial volume effects. Nevertheless, our results indicate that a much shorter optimal echo time is needed for AIF estimation which is consistent with previously published observations.20
The optimal echo times reported in this study are specific to a field strength of 3T and the CA dose protocol (no preload and one standard dose of CA). At a different field strength, such as 1.5T, the optimal TE would be expected to lengthen. A preload of CA is typically administered prior to the DSC-MRI scan to decrease the CA induced T1 leakage effects. Such preloads could potentially decrease baseline T2* values due to residual CA in the blood and tumor tissue thereby shorting the optimal TE. To estimate the impact of a standard full-dose of preload, we retrospectively analyzed, in a separate cohort of 5 glioma patients, multi-echo DSC-MRI data that was acquired for a total of 7.5 minutes. We found that tumor T2* was 35% lower than baseline 6 minutes after the CA injection (additionally, NAWM was 15% and AIF was 10% lower than baseline). Assuming a 35% decrease in T2* with a preload, the optimal TE will be 35% shorter than a no preload dose scheme or an estimated 19.5 ± 4.8 ms for the tumor.
There were several limitations to this study. First, our results are specific to 3T and to both a standard preload and injection dose. Although T2* is expected to be longer at 1.5T than at 3T implying that the optimal TE would also increase, we are not able demonstrate this experimentally. For clinical sites using less than a standard dose for either the preload or injection dose, our results do not apply. However, our derivations and methodology for optimal TE can easily be applied to data acquired at any field strength or dosing scheme of interest. Second, as noted, a statistical difference was found between the optimal echo times between tumor, NAWM, and AIF. The extent of using a non-optimal echo time on CBV is unknown. The influence of TE on the accuracy of CBV can be explored both experimentally and through simulations, and is currently saved for future work. Third, we have calculated the optimal echo time in a small cohort of patients. However, power statistics did demonstrate that our sample size had an 80% power to detect a 0.94 standard deviation in our measurements. It is unlikely that additional patients would substantially (or practically) shift the calculated optimal TE values. Lastly, the estimation of the optimal TE from two separate cohorts to understand the effect of a preload on the optimal TE is not ideal. Calculation of the optimal TE from multi-echo DSC data acquired with a preload would have been ideal. However, clinically single-echo DSC-MRI is acquired with a preload, and changes in absolute T2* cannot be obtained from single-echo data for optimal TE calculation. When a multi-echo DSC acquisition is acquired in the clinic, a preload is typically not administered because the T1 leakage effects are eliminated. Additionally, our two separate cohorts used a standard dose injection of two different contrast agents. However, the calculated optimal TE values should not change significantly as the expected change in T2* due to its relaxation rate is similar22,23 across both contrast agents and we found no significant statistical differences in average gadolinium concentration between the two cohorts.
The results of this study demonstrate that for conventional single-echo, GRE based DSC-MRI, the optimal TE for CBV mapping in brain tumors and NAWM is 30-36 ms at 3T if no preload has been administered. It should be noted that the accuracy of the AIF will be diminished, to an unknown degree, due to the longer than optimal echo time. In this situation, CBV should only be calculated in the tumor and the NAWM. If multiple echo times can be prescribed than a shorter echo time of 10 ms should be prescribed for the AIF and a longer echo time of 30-36 ms should be prescribed for the brain tissue and tumor. Given the ASFNR's recommendation that a preload should be used for DSC-MRI studies in glioma patients, the error analysis and patient data described in this study provide experimental evidence that CBV estimates may benefit from lower echo times (∼20 ms) than the recommended value of 30 ms.
Supplementary Material
Supplementary Figure 1: An illustration of the ROI selection process for the tumor and NAWM ROIs as outlined within the Materials and Methods section.
Acknowledgments
We acknowledge Kelly Gardener and Samuel McGee for their valuable help.
Grant Support: We received funding for this project from NIH/NCI R01 CA158079.
References
- 1.Fink JR, Muzi M, Peck M, Krohn KA. Multimodality Brain Tumor Imaging: MR Imaging, PET, and PET/MR Imaging. J Nucl Med. 2015;56(10):1554–1561. doi: 10.2967/jnumed.113.131516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Boxerman JL, Ellingson BM, Jeyapalan S, et al. Longitudinal DSC-MRI for Distinguishing Tumor Recurrence From Pseudoprogression in Patients With a High-grade Glioma. Am J Clin Oncol. 2014;0(0):1–7. doi: 10.1097/COC.0000000000000156. [DOI] [PubMed] [Google Scholar]
- 3.Ellingson BM, Zaw T, Cloughesy TF, et al. Comparison between intensity normalization techniques for dynamic susceptibility contrast (DSC)-MRI estimates of cerebral blood volume (CBV) in human gliomas. J Magn Reson Imaging. 2012;35(6):1472–1477. doi: 10.1002/jmri.23600. [DOI] [PubMed] [Google Scholar]
- 4.Chaskis C, Stadnik T, Michotte A, Van Rompaey K, D'Haens J. Prognostic value of perfusion-weighted imaging in brain glioma: a prospective study. Acta Neurochir (Wien) 2006;148(3):277–285. doi: 10.1007/s00701-005-0718-9. [DOI] [PubMed] [Google Scholar]
- 5.Maia ACM, Malheiros SMF, da Rocha AJ, et al. Stereotactic biopsy guidance in adults with supratentorial nonenhancing gliomas: role of perfusion-weighted magnetic resonance imaging. J Neurosurg. 2004;101(6):970–976. doi: 10.3171/jns.2004.101.6.0970. [DOI] [PubMed] [Google Scholar]
- 6.Barajas RF, Chang JS, Segal MR, et al. Differentiation of recurrent glioblastoma multiforme from radiation necrosis after external beam radiation therapy with dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging. Radiology. 2009;253(2):486–496. doi: 10.1148/radiol.2532090007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hu LS, Baxter LC, Smith KA, et al. Relative Cerebral Blood Volume Values to Differentiate High-Grade Glioma Recurrence from Posttreatment Radiation Effect: Direct Correlation between Image-Guided Tissue Histopathology and Localized Dynamic Susceptibility-Weighted Contrast-Enhanced Perfusio. Am J Neuroradiol. 2009;30(3):552–558. doi: 10.3174/ajnr.A1377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Danchaivijitr N, Waldman AD, Tozer DJ, et al. Low-Grade Gliomas: Do Changes in rCBV Measurements at Longitudinal Perfusion-weighted MR Imaging Predict Malignant Transformation? Radiology. 2008;247(1):170–178. doi: 10.1148/radiol.2471062089. [DOI] [PubMed] [Google Scholar]
- 9.Rossi Espagnet MC, Romano A, Mancuso V, et al. Multiparametric evaluation of low grade gliomas at follow-up: comparison between diffusion and perfusion MR with 18 F-FDOPA PET. Br J Radiol. 2016;89(1066):20160476. doi: 10.1259/bjr.20160476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Boxerman JL, Rosen BR, Weisskoff RM. Signal-to-noise analysis of cerebral blood volume maps from dynamic NMR imaging studies. J Magn Reson Imaging. 1997;7(3):528–537. doi: 10.1002/jmri.1880070313. [DOI] [PubMed] [Google Scholar]
- 11.Welker K, Boxerman J, Kalnin A, et al. ASFNR recommendations for clinical performance of MR dynamic susceptibility contrast perfusion imaging of the brain. AJNR Am J Neuroradiol. 2015;36(6):E41–51. doi: 10.3174/ajnr.A4341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Willats L, Calamante F. The 39 steps: evading error and deciphering the secrets for accurate dynamic susceptibility contrast MRI. NMR Biomed. 2013;26(8):913–931. doi: 10.1002/nbm.2833. [DOI] [PubMed] [Google Scholar]
- 13.Thilmann O, Larsson EM, Björkman-Burtscher I, Ståhlberg F, Wirestam R. Effects of echo time variation on perfusion assessment using dynamic susceptibility contrast MR imaging at 3 tesla. Magn Reson Imaging. 2004;22(7):929–935. doi: 10.1016/j.mri.2004.01.079. [DOI] [PubMed] [Google Scholar]
- 14.Jochimsen TH, Newbould RD, Skare ST, et al. Identifying systematic errors in quantitative dynamic-susceptibility contrast perfusion imaging by high-resolution multi-echo parallel EPI. NMR Biomed. 2007;20(4):429–438. doi: 10.1002/nbm.1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Woolrich MW, Jbabdi S, Patenaude B, et al. Bayesian analysis of neuroimaging data in FSL. Neuroimage. 2009;45(1):S173–S186. doi: 10.1016/j.neuroimage.2008.10.055. [DOI] [PubMed] [Google Scholar]
- 16.Schmainda KM, Paulson ES, Prah DE. Multiparameter perfusion imaging with leakage correction. 2008 [Google Scholar]
- 17.Newton AT, Skinner JT, Quarles CC. Automatic AIF Estimation in Multi-echo DSC-MRI of Pediatric Patients -Avoiding The Noise Floor. Proc Intl Soc Mag Reson Med. 2013;21 [Google Scholar]
- 18.Mouridsen K, Christensen S, Gyldensted L, Ostergaard L. Automatic selection of arterial input function using cluster analysis. Magn Reson Med. 2006;55(3):524–531. doi: 10.1002/mrm.20759. [DOI] [PubMed] [Google Scholar]
- 19.Semmineh NB, Xu J, Skinner JT, et al. Assessing tumor cytoarchitecture using multiecho {DSC}-{MRI} derived measures of the transverse relaxivity at tracer equilibrium ({TRATE}) Magn Reson Med. 2014;784(September 2014):n/a–n/a. doi: 10.1002/mrm.25435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Newbould RD, Skare ST, Jochimsen TH, et al. Perfusion mapping with multiecho multishot parallel imaging EPI. Magn Reson Med. 2007;58(1):70–81. doi: 10.1002/mrm.21255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stokes AM, Quarles CC. A simplified spin and gradient echo approach for brain tumor perfusion imaging. Magn Reson Med. 2016;75(1):356–362. doi: 10.1002/mrm.25591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Weinmann HJ, Bauer H, Ebert W, et al. Comparative Studies on the Efficacy of MRI Contrast Agents in MRA. Acad Radiol. 2002;9(1):S135–S136. doi: 10.1016/s1076-6332(03)80419-1. [DOI] [PubMed] [Google Scholar]
- 23.Pintaske J, Martirosian P, Graf H, et al. Relaxivity of Gadopentetate Dimeglumine (Magnevist), Gadobutrol (Gadovist), and Gadobenate Dimeglumine (MultiHance) in human blood plasma at 0.2, 1.5, and 3 Tesla. Invest Radiol. 2006;41(3):213–221. doi: 10.1097/01.rli.0000197668.44926.f7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Figure 1: An illustration of the ROI selection process for the tumor and NAWM ROIs as outlined within the Materials and Methods section.