

Abstract
We sought to describe the association between HIV and blood pressure levels, and determined the extent to which this relationship is mediated by body weight in a cross-sectional study of HIV-infected and HIV-uninfected controls matched by age, gender, and neighborhood. We fit mixed-effects models to determine the association between HIV and BP and amount of effect of HIV on BP mediated through BMI. We analyzed data from 577 HIV-infected and 538 matched HIV-uninfected participants. HIV infection was associated with 3.3 mmHg lower SBP (1.2 to 5.3), 1.5 mmHg lower DBP (0.2 to 2.9), 0.3 m/s lower PWV (0.1 to 0.4), and 30% lower odds of hypertension (10 to 50%). BMI mediated 25% of the association between HIV and SBP. HIV infection was inversely associated with SBP, DBP and pulse-wave velocity. Comprehensive community-based programs to routinely screen for cardiovascular risk factors irrespective of HIV status should be operationalized in HIV-endemic countries.
BACKGROUND
Survival of HIV infected persons over the years has increased due to successful scale-up of antiretroviral therapy (ART)1 with life expectancy of people living with HIV approaching that of HIV-uninfected individuals.2–5 This has created an aging HIV population with elevated risk of hypertension and cardiovascular disease.6–8 In fact, several studies have shown that risk of cardiovascular disease is higher in HIV infected patients than HIV uninfected.9,10
Epidemiological studies report conflicting associations between HIV and hypertension/blood pressure (BP) levels with some studies reporting lower BP levels,11–13 a few reporting comparable levels8,14–16 and others report higher BP levels in HIV-infected individuals.17,18 A recent systematic review of studies in sub-Saharan Africa reported lower prevalence of hypertension in HIV-infected individuals compared with the general populations.12 Other scholars have examined Pulse Wave Velocity (PWV) as a novel measure of subclinical atherosclerosis and a precursor to clinical hypertension.19 Here again, the reported associations between PWV and HIV are mixed.20,21
However, these studies had several major limitations. First, most of the prior studies only adjusted for traditional cardiovascular risk factors such as age, and gender but had limited data on life style factors such as physical activity, smoking, alcohol use, socioeconomic status, and stress, raising the potential for unmeasured confounding.22–24 Second, some of these studies included body weight as a potential confounder, whereas it is more likely to be a mediator of the effect of HIV on blood pressure.11 Finally, most of these studies were conducted in rural areas, and are therefore not representative of the rapidly growing urban populations where cardiovascular disease risk tends to be much higher.25
Therefore, we conducted a cross-sectional study of HIV and cardiovascular risk factors in an urban population in Uganda to better understand the relationships between HIV and blood pressure and pulse-wave velocity. We also investigated the potential role of body weight in mediating the effect of HIV on blood pressure.
METHODS
Study population
We conducted a matched cross-sectional study in Mbarara municipality, Uganda between June and October 2015 to recruit HIV-infected persons and age, gender, and neighborhood matched HIV-uninfected controls known as the Aging and Cardiovascular diseases in HIV patients of East Africa (ACHIEvA) study. These matching factors were chosen a-priori as important determinants of both HIV and blood pressure.
We used the electronic databases of the Makerere University Joint AIDS Program (MJAP)/Mbarara Municipal Council (MMC) Health Center IV and the Mbarara University/Mbarara Regional Referral Hospital Immune Suppression Syndrome (ISS) clinic to identify adults aged 40 years or older who had visited the clinic within the past 6 months and lived in one of the 3 divisions of Mbarara municipality (Kakoba, Kamukuzi, and Nyamitanga). We abstracted identifier and contact information and expected dates for subsequent clinic visits to maximize chances of finding selected HIV-infected person. Once contact was established, a visit in their households to perform interviews and measurements was arranged based on their earliest convenience.
To recruit matched HIV-uninfected controls, we randomly chose a household in the same neighborhood as the index HIV patient and selected an adult resident who was of the same gender and in the same 5-year age category as the HIV-infected participant. In Mbarara, the distinction of household members from non-residents is blurred. We therefore considered a household member as anyone who had had at least 3 meals in a household on at least three consecutive days in the past 6 months. If there were more than one potential matches in the same household, we used the Kish method26 to select one of them. In the event that a selected matched individual was not home at the time of the visit, 3 attempts on separate days, including evenings on week days and weekends were made before sampling another household for a match.
If a selected household had no eligible individual, we visited the immediate neighboring household until an eligible participant was found. We excluded pregnant women since this causes physiological derangement metabolic parameters, mentally incapacitated people as these people would respond to survey questions inappropriately, and limb or spinal physically incapacitated people would not be able to stand for anthropometric measurements.
Ethics Statement
All participants provided informed consent before enrollment into the study and separate consent for release of HIV care data was obtained from HIV infected participants. The head of MJAP/MMC clinic, director of the ISS clinic, office of the town clerk, and respective administrative heads of Mbarara municipality granted permission to carry this study.
The ethics review committees at Mbarara University of Science & Technology, Harvard T. H. Chan School of Public Health, and Uganda National Council of Science and Technology approved the study.
Data collection
Measurement of covariates
Trained research assistants conducted interviews using electronic devices to capture household asset ownership, stress in life and work using the perceived stress tool,27 and physical activity using a validated physical activity questionnaire for sub-Saharan Africa.28 The questionnaire also captured information on smoking history (age of starting, duration and intensity of smoking and efforts to quit), alcohol intake using the Alcohol Use Disorders Identification Test (AUDIT-C) questionnaire,29 history of diagnosis and/or management of cardiovascular disease and its risk factors (hypertension, diabetes mellitus, dyslipidemia), and a list of current medications.
Waist and hip circumferences were measured by standard procedures30 with a participant standing using a tape (seca 201, Hanover, USA), weight was measured using standardized scales (seca 762, Hanover, USA) and height was measured using a roll-up measuring stadiometers (seca 206, Hanover, USA). Height, waist and hip circumferences were measured to the nearest 0.1 cm and weight was measured to the nearest kilogram. The plausible ranges for the anthropometric measurements were set as 0.5 to 1.5 for waist-to-hip ratio, 100 to 200 cm for height, and 30 to 150 kg for weight. Values outside of these ranges were set to missing. We used height and weights to calculate body mass (BMI) as weight (in kilograms) divided by the square of height (in meters), and categorized BMI as underweight (<18.5 Kg/m2), normal weight (18.5 to 24.9 Kg/m2), overweight (25 to 29.9 Kg/m2), or obese (>30 Kg/m2).
We collected spot urine specimen and measured urine sodium and creatinine (Humastar200™, Human Diagnostics Worldwide, Wiesbaden, Germany) and estimated 24-hour urinary sodium excretion using the Kawasaki formula.31 Laboratory tests were performed at Mbarara Regional Referral Hospital laboratory which has standardized internal quality control protocols and participates in external quality control programs by the National Health Laboratory Service.
Blood pressure and pulse wave velocity measurements
Blood pressure (BP) was measured using a digital upper arm sphygmomanometer (Omron® BP710N 3 series, Omron Healthcare Inc., Bannockburn, USA) with small (<21 cm), normal (22 to 32 cm), and large cuffs (35 to 44 cm). The participant was seated in a chair and allowed to rest for 5 minutes before three measurements were performed with 3-minutes intervals. We used the average of the second and third measurements to determine the blood pressure of each participant. We set a range of 70 to 270 mmHg as plausible values for systolic blood pressure (SBP) and 30 to 150 mmHg for diastolic blood pressure (DBP). We defined hypertension as having a systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or self-reported use of antihypertensive medications.32
We performed two measurements of carotid-femoral pulse wave velocity (PWV) using a handheld device (Arteriograph, TensioMed® Arteriograph™ TL2, Budapest, Hungary) with the participant in supine position. The device estimates PWV by measuring the time-lag between the two peaks in the blood pressure wave and combining this information with the distance between jugular notch and symphysis pubis that the operator measures with a tape. During each measurement, PWV was estimated for each pulse wave during eight seconds and if the standard deviation of the estimated PWVs was larger than 1 m/s, the recording was discarded and a repeat measurement performed as recommended by the manufacturer;33 up to 5 attempts were made to obtain a valid measurement.
Statistical analysis
We used principle component analysis (Supplementary Table 1 and 2) to generate an assets index score based on household utilities and assets34 and perceived stress questionnaire responses to derive composite measures with highest discriminatory capabilities. Participants were divided into quintiles of these scores.
We described population characteristics, exposures, and outcomes by HIV- status and compared the distributions between HIV-infected and matched HIV-uninfected participants in univariate analyses using t-test for continuous variables, chi-square tests for categorical variables, and trend test using median values of categories for ordinal variables. We categorized participants with hypertension into: undiagnosed; diagnosed and untreated; diagnosed and treated but not controlled; diagnosed, treated and controlled, with the latter defined by having SBP<140 and DBP<90 mmHg.
We used a-priori knowledge to select potential confounders (Figure 4): age, gender, asset index, marital status, smoking, alcohol consumption, and perceived stress score that were postulated to affect the association of HIV and blood pressure. Hierarchical linear mixed effects regression models were used to determine the participant-level association between HIV and blood pressure (systolic and diastolic blood pressures separately) and PWV, adjusted participant matching and interviewer-related differences in measurement of subjective risk factors.35 In addition, we fit a conditional logistic regression model to determine association between HIV and hypertension status. We also performed a subgroup analysis to estimate the adjusted odds of prevalent hypertension by separating the HIV-infected participants into those with shorter (< 3years) or longer (≥3 years) duration of ART.
Figure 4.
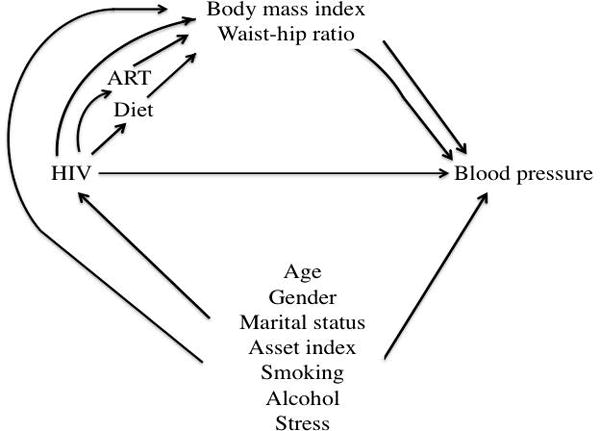
Directed Acyclic Graph for the relationship between HIV and blood pressure, ACHIEvA study 2015
We examined whether BMI (categorized as ≥ 25 kg/m2 and < 25kg/m2 as reference value) and waist-hip ratio (continuous scale) mediated the effects of HIV on SBP and PWV. Direct and indirect effects were estimated using parametric regression models.36,37 We fit two models, one for BMI as a mediator conditional on HIV and potential confounders and a model for SBP conditional on HIV, BMI and potential confounders with interaction between HIV and BMI. We used bootstrapping to compute bias-corrected confidence intervals.37 The percentage of mediation was quantified as (indirect effect/total effect) × 100.
All statistical analyses were conducted using Stata 13.0 (StataCorp, College Station, TX).
RESULTS
At time of study, 1659 records of people living with HIV in the clinic databases were eligible for inclusion. We randomly abstracted 909 records and among these, 184 had no telephone contacts, 54 people had moved out of study area by time of survey and 28 had changed their telephone numbers.
A total of 1347 households were visited, 24 people declined to participate, 9 had mental incapacitation, 2 were physically incapacitated, 10 were found to be younger than under 40 years, 4 were pregnant, and 10 had time constraints though they were interested.
We enrolled 697 HIV-infected persons and 591 matched HIV-uninfected persons. All people living with HIV were taking ART except 24 who were not previously diagnosed. After excluding 21 participants who had missing data on confounders [smoking (N=1), BMI (N=4), waist circumference (N=3), and physical activity (N=13)] (Figure 1), the final study population consisted of 1115 participants (577 HIV-infected and 538 matched HIV-uninfected). The prevalence of hypertension was higher among the HIV-uninfected compared to the HIV-infected participants (28.8% vs 21.5%). Also, there was no statistical difference in median age in both groups with HIV-infected having a median age 45 (InterQuartile Range (IQR) 42 to 49) years and HIV-uninfected median age 46 (IQR 43 to 50) years (Table 1).
Figure 1.
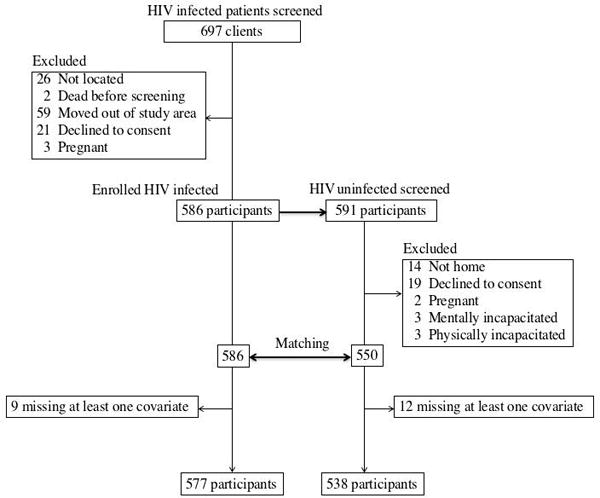
Participant selection process, ACHIEvA study 2015
Table 1.
Study characteristics by HIV status, ACHIEvA study 2015 (n=1115)
| Characteristic | HIV-infected, n (%) | Matched HIV uninfected, n (%) | p-value |
|---|---|---|---|
| Women | 326 (57) | 305 (56) | 0.958 |
| Age, median (IQR) | 45 (42, 49) | 46 (43, 50) | 0.0821 |
| Age groups | 0.020* | ||
| 40 – 44 | 246 (42.6) | 178 (33.1) | |
| 45 – 49 | 190 (32.9) | 211 (39.2) | |
| 50 – 54 | 72 (12.5) | 80 (14.9) | |
| 55 – 60 | 45 (7.8) | 36 (6.7) | |
| > 60 | 25 (4.2) | 33 (6.1) | |
| Employment status | < 0.001 | ||
| Self-employed | 337 (58.4) | 348 (64.7) | |
| Government or non-professional | 73 (12.6) | 62 (11.5) | |
| Private employer | 84 (14.6) | 37 (6.9) | |
| Unemployed | 83 (14.4) | 91 (16.9) | |
| Marital status | <0.001 | ||
| Married or cohabiting | 303 (52.5) | 415 (77.1) | |
| Separated or divorced | 144 (25.0) | 71 (13.2) | |
| Widowed or widower | 119 (20.6) | 48 (8.9) | |
| Single | 11 (1.9) | 4 (0.7) | |
| Religion | 0.009 | ||
| Catholic | 178 (30.8) | 152 (28.2) | |
| Anglican | 276 (47.8) | 232 (43.1) | |
| Muslim | 73 (12.6) | 107 (19.9) | |
| Pentecostal | 46 (8.0) | 42 (7.8) | |
| Other | 4 (0.7) | 5 (0.9) | |
| Smoking status | 0.069* | ||
| Never smoker | 423 (73.3 | 415 (77.1) | |
| Current smoker | 61 (10.6) | 58 (10.8) | |
| Former smoker | 93 (16.1) | 65 (12.1) | |
| Alcohol consumption | 0.855* | ||
| 0 g/week | 371 (64.3) | 367 (68.2) | |
| <20 g/week (women) & <40 g/week (men) | 90 (15.6) | 57 (10.6) | |
| 20 to 39g/week (women) & 40 to 59 g/week (men) | 20 (3.5) | 16 (3.0) | |
| ≥ 40g/week (women) & ≥ 60g/week (men) | 96 (16.6) | 98 (18.2) | |
| Perceived stress score (quintiles) | 0.067* | ||
| 1st | 96 (16.6) | 127 (23.6) | |
| 2nd | 112 (19.4) | 111 (20.6) | |
| 3rd | 136 (23.6) | 88 (16.4) | |
| 4th | 121 (21.0) | 104 (19.3) | |
| 5th | 112 (19.4) | 108 (20.1) | |
| Asset index | < 0.001* | ||
| Poorest | 131 (22.7) | 90 (16.7) | |
| Poorer | 118 (20.4) | 106 (19.7) | |
| Average | 126 (21.8) | 97 (18.0) | |
| Richer | 113 (19.6) | 110 (20.5) | |
| Richest | 89 (15.4) | 135 (24.1) | |
| METS hours/week | 0.142* | ||
| 0 | 237 (41.1) | 220 (40.9) | |
| 1 – 3 | 102 (17.7) | 75 (13.9) | |
| 3 – 10 | 127 (22.0) | 114 (21.2) | |
| 10 – 20 | 61 (10.6) | 65 (12.1) | |
| > 20 | 50 (8.7) | 64 (11.9) | |
| Clinical | |||
| Body mass index category | |||
| Underweight (<18.5) | 56 (9.7) | 26 (4.8) | < 0.001* |
| Normal (18.5 – <25) | 301 (52.2) | 210 (39.0) | |
| Overweight (25 – <30) | 131 (22.7) | 169 (31.4) | |
| Obese (≥30) | 89 (15.4) | 133 (24.7) | |
| Waist circumference (both genders) | 87 (12.6) | 91 (12.4) | < 0.001 |
| Waist circumference, men (≥ 102 cm)* | 11 (4.4) | 29 (12.4) | < 0.004 |
| Waist circumference, women (≥ 88 cm)* | 190 (58.3) | 202 (66.2) | 0.040 |
| Waist - hip ratio (WHR) (both genders) | 0.88 (0.1) | 0.89 (0.1) | 0.059 |
| Waist – hip ratio, men (≥ 0.90)* | 97 (38.6) | 120 (51.5) | 0.004 |
| Waist – hip ratio, women (≥ 0.85)* | 218 (66.9) | 205 (67.2) | 0.927 |
| Systolic blood pressure, mean (SD)$ | 123 (18.3) | 127 (17.8) | < 0.001 |
| Diastolic blood pressure, mean (SD)$ | 76 (11.5) | 78 (12.3) | 0.027 |
| Antihypertensive medication | 49 (8.5) | 45 (8.4) | 0.685 |
| Prevalent hypertension** | 124 (21.5) | 155 (28.8) | |
| Pulse wave velocity (PWV), m/s | 7.8 (1.4) | 8.0 (1.4) | 0.013 |
| Arterial stiffness #(age stratified) | 10 (1.9) | 5 (1.0) | 0.241 |
| Laboratory | |||
| Serum Hb A1c (%), mean (SD) | 5.8 (4.3) | 6.7 (5.1) | 0.005 |
| Serum Hb A1c (> 6.5 %), n (%) | 200 (36.4) | 164 (28) | 0.002 |
| Serum HDL cholesterol (all), mg/dL, mean (SD) | 58.5(19.9) | 55.3(15.0) | 0.01 |
| Serum LDL cholesterol (all), mg/dL, mean (SD) | 103 (34.5) | 110 (35.1) | 0.004 |
| Serum triglycerides (all), mg/dL, mean (SD) | 175 (99.9) | 181 (91.6) | 0.341 |
| Serum total cholesterol (all), mg/dL, mean (SD) | 188 (73.9) | 182 (52.2) | 0.207 |
| Urine sodium excretion, g/24hours, mean (SD) | 8.40 (3.3) | 7.96 (3.1) | 0.040 |
Abbreviations: SD: Standard deviation; IQR: Interquartile range; METS: Metabolic equivalents; HbA1c: glycated hemoglobin; HDL: High-density lipoprotein cholesterol; LDL: Low density lipoprotein cholesterol.
Pulse wave velocity measurements n= 1026 (530 HIV-infected and 496 uninfected), glycated hemoglobin n= 865 (448 HIV-infected and 417 HIV-uninfected), Serum LDL and Triglycerides n= 899 (464 HIV-infected and 435 HIV-uninfected), serum cholesterol and HDL n= 811 (420 HIV-infected and 391 HIV-uninfected), and urine sodium excretion estimation n= 890 (462 HIV-infected and 428 HIV-uninfected).
Trend test: WC,
WHR: WHO thresholds for substantially increased cardiovascular disease risk;
Blood pressure: Average of same sitting 2nd and 3rd blood pressure measurements;
Arterial stiffness: European[47] cutoffs for Arterial stiffness: PWV >11 m/s for age 20–40 years; PWV > 12 m/s for age 41–59
Hypertension defined as SBP ≥140 mmHg, DBP ≥90 mmHg, and/or self-reported anti-hypertensive drug use.
Ninety one percent (524/577) of HIV-infected participants had been taking antiretroviral therapy for median duration of 4.8 years (IQR 2.6 to 7.6) with a median nadir CD4 cell count of 206 cells/mL (IQR 104 to 307) at time of ART initiation. Though none of the HIV-infected participants had been initiated on a protease inhibitor (PI)-based ART regimen, we found 3 % (N=17) were taking PI-based regimen at time of this study (Table 3).
Table 3.
Characteristics of HIV infected participants, ACHIEvA study 2015
| Characteristic | N=577 |
|---|---|
| Taking antiretroviral therapy (ART) (n, %) | 528 (91.5) |
| HIV not initiated ART | 24 (4.2) |
| Previously undiagnosed (n, %) | 25 (4.3) |
| Follow-up duration (months) before ART initiation, (Median, IQR) | 4 .3 (1.4, 24.9) |
| Follow-up duration (years) after ART initiation, (Median, IQR) | 4.8 (2.6, 7.6) |
| Age (in years) at ART initiation (Median, IQR) | 40 (37, 45) |
| Systolic blood pressure at ART initiation (Mean, SD) | 116 (18) |
| Diastolic blood pressure at ART initiation (Mean, SD) | 73 (10) |
| Body mass index at ART initiation (Mean, SD) | 22.9 (9.1) |
| CD4 cell counts (cells/mL) at ART initiation (Median, IQR) | 163 (62, 251) |
| CD4 cell counts (cells/mL) at time of study (Median, IQR) | 479 (338, 656) |
| Changed ART regimen during follow-up (n, %) | 149 (28) |
| Duration on baseline regimen, years (Median, IQR)** | 2.4 (0.5, 3.3) |
| Participants initiated on Protease inhibitors at ART initiation (n, %) | 0 (0) |
| Participants taking Protease inhibitors at time of study (n, %) | 17 (3) |
| Participants initiated on Stavudine at ART initiation (n, %) | 87 (16) |
| Participants taking Stavudine at time of study (n, %) | 9 (2) |
Among those who have at least one change in drug regimen
Note: 25 participants were diagnosed with HIV during study and had no HIV data and 28 had been diagnosed with HIV but were not receiving care during ACHIEvA study.
Thirty six percent of HIV-uninfected controls and 28% of HIV-infected participants had serum glycated hemoglobin > 6.5 % (p=0.002), defined as diabetes mellitus. HIV-infected participants had a mean serum LDL cholesterol of 103 (SD ± 34.5) mg/dL levels versus 110 (SD ± 35.1) mg/dL for uninfected controls (p =0.004) (Table 1). The mean systolic blood pressure was 123 mmHg (SD ± 18.3) among HIV-infected participants and 127 mmHg (SD ± 17.8) among HIV-uninfected controls. A total of 276 participants were found to have hypertension, 119 men (50 HIV-infected and 69 HIV-uninfected controls) and 157 women (71 HIV-infected and 86 HIV-uninfected controls).
After adjusting for potential confounders, HIV infection was associated with a 3.3 mmHg lower SBP (95% confidence interval (CI) 1.2 to 5.3), 1.5 mmHg lower DBP (95% CI 0.2 to 2.9), 0.3 m/s slower PWV (95% CI 0.1 to 0.4), and 30% lower odds of hypertension (95% CI 10% to 50%). In addition, increasing alcohol consumption was associated with higher SBP (p value for test of trend 0.003) and DBP (p value for test of trend 0.002) whereas increasing physical activity was associated with lower SBP (p value for test of trend 0.040) and pulse wave velocity (p value for test of trend 0.001) (Table 2).
Table 2.
Adjusted mean difference for systolic and diastolic blood pressure and pulse wave velocity, and adjusted odds ratios (95% CI) for hypertension prevalence, ACHIEvA study 2015
| Characteristic | * Systolic blood pressure (mmHg) | † p-value | * Diastolic blood pressure (mmHg) | † p-value | Pulse wave velocity (m/s) | † p-value | ** Hypertension | † p-value |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| N=1115 | N=1115 | N=1115 | N=1115 | |||||
| HIV-uninfected | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| HIV-infected | −3.3 (−5.3, −1.2) | 0.002 | −1.5 (−2.9, −0.2) | 0.027 | −0.3 (−0.4, −0.1) | 0.002 | 0.7 (0.5, 0.9) | 0.022 |
| Marital status | 0.337 | 0.511 | 0.060 | 0.744 | ||||
| Married | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| Separated/divorced | −3.1 (−5.9, 0.2) | −0.8 (−2.7, 1.0) | 0.1 (−0.1, 0.4) | 0.6 (0.3, 1.3) | ||||
| Widowed | −0.9 (−4.0, 2.2) | −1.0 (−3.1, 1.1) | 0.2 (−0.1, 0.5) | 0.9 (0.4, 1.8) | ||||
| Single | −1.7 (−10.4, 7.1) | 0.7 (−5.1, 6.6) | 0.2 (−0.5, 0.9) | 2.0 (0.3, 14.4) | ||||
| Employment | 0.113 | 0.138 | 0.046 | 0.047 | ||||
| Self-employed | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| Government/NGO | 1.6 (−1.7, 5.0) | −0.03 (−2.3, 2.2) | 0.1 (−0.1, 0.4) | 1.3 (0.6, 3.1) | ||||
| Private employer | 1.9 (−1.5, 5.4) | 1.7 (−0.5, 4.0) | 0.0 (−0.2, 0.3) | 1.4 (0.6, 3.4) | ||||
| Unemployed | 1.6 (−1.4, 4.7) | 0.8 (−1.2, 2.8) | 0.3 (0.1, 0.6) | 1.7 (0.8, 3.5) | ||||
| Religion | 0.528 | 0.353 | 0.856 | 0.904 | ||||
| Catholic | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| Anglican | 1.6 (−0.9, 4.0) | 0.4 (−1.2, 2.0) | 0.1 (−0.1, 0.3) | 1.5 (0.8, 2.8) | ||||
| Muslim | 3.1 (−0.3, 6.5) | 0.7 (−1.6, 2.9) | 0.2 (0.1, 0.5) | 1.1 (0.5, 2.5) | ||||
| Pentecostal | −0.7 (−4.9, 3.5) | −2.5 (−5.3, 0.3) | −0.2 (−0.5, 0.2) | 1.2 (0.4, 3.6) | ||||
| Other | 1.1 (−10.7, 12.9) | −1.4 (−9.2, 6.5) | −0.3 (−1.3, 0.6) | 0.8 (0.1, 7.0) | ||||
| Smoking status | 0.098‡ | 0.686‡ | 0.355‡ | 0.580‡ | ||||
| Never smoker | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| Current smoker | −2.7 (−6.3, 0.9) | −2.8 (−52, 0.4) | −0.1 (−0.4, 0.2) | 0.3 (0.1, 0.9) | ||||
| Former smoker | 2.7 (−0.4, 5.8) | −0.3 (−2.3, 1.8) | −0.1 (−0.4, 0.1) | 0.9 (0.4, 2.1) | ||||
| Alcohol consumption|| | 0.003‡ | <0.002‡ | 0.549‡ | 0.610‡ | ||||
| 0 g/week | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| <20 g/week (women) & <40 g/week (men) | −0.6 (−3.9, 2.6) | −0.4 (−2.5, 1.8) | −0.2 (−0.5, 0.1) | 1.0 (0.5, 2.1) | ||||
| > 20 g/week (women) & > 40 g/week (men) | 5.3 (2.4, 8.2) | 3.6 (1.7, 5.6) | −0.0 (−0.2, 0.2) | 1.7 (0.8, 3.4) | ||||
| Perceived stress (quintiles) | 0.842‡ | 0.083‡ | 0.802‡ | 0.545‡ | ||||
| 1st | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| 2nd | −0.9 (−4.2, 2.3) | 0.5 (−1.7, 2.6) | −0.0 (−0.3, 0.2) | 0.5 (0.3, 1.2) | ||||
| 3rd | 0.4 (−2.9, 3.7) | 0.2 (−1.9, 2.4) | −0.0 (−0.3, 0.2) | 0.7 (0.3, 1.6) | ||||
| 4th | 0.2 (−3.1, 3.5) | 1.2 (−1.9, 2.4) | 0.1 (−0.2, 0.4) | 0.8 (0.3, 1.8) | ||||
| 5th | −1.0 (−4.3, 2.2) | 1.8 (−0.4, 3.9) | −0.0 (−0.3, 0.2) | 1.0 (−0.3, 2.4) | ||||
| Asset index | 0.275‡ | 0.173‡ | 0.014‡ | 0.055‡ | ||||
| Average | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| Poorest | 0.5 (−2.9, 3.8) | 0.5 (−1.8, 2.8) | −0.1 (−0.4, 0.2) | 0.6 (0.3, 1.7) | ||||
| Poorer | 0.6 (−2.6, 3.8) | 0.2 (−1.9, 2.4) | −0.0 (−0.3, 0.2) | 0.7 (0.3, 1.6) | ||||
| Richer | 0.1 (−3.1, 3.4) | −0.2 (−2.3, 2.0) | 0.1 (−0.2, 0.3) | 0.9 (0.4, 2.1) | ||||
| Richest | 1.6 (−1.7, 4.9) | 2.0 (−0.2, 4.2) | 0.2 (−0.1, 0.4) | 1.4 (0.6, 3.2) | ||||
| METS hours/week | 0.040‡ | 0.321‡ | 0.001‡ | 0.507‡ | ||||
| 0 | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | ||||
| 1 – 3 | −1.5 (−4.5, 1.6) | −0.1 (−2.9, 2.0) | 0.1 (−0.2, 0.3) | 1.0 (0.5, 2.0) | ||||
| 3 – 10 | −1.1 (−3.9, 1.6) | −1.3 (−3.2, 0.5) | −0.2 (−0.4, 0.1) | 1.0 (0.5, 1.9) | ||||
| 10 – 20 | −5.1 (−8.7, −1.6) | −2.7 (−5.1, −0.4) | −0.6 (−0.9, −0.4) | 1.0 (0.4, 2.6) | ||||
| > 20 | −1.9 (−5.6, 1.8) | 0.7 (−1.8, 3.1) | −0.2 (−0.5, 0.1) | 0.5 (0.2, 1.5) | ||||
Average of same sitting 2nd and 3rd blood pressure measurements.
Hypertension defined as SBP ≥140 mmHg, DBP ≥90 mmHg, and/or self-reported anti-hypertensive drug use
chi-square test unless otherwise specified
Test of trend based on median value within each category
Definition based on number of days consumed alcohol over the past 30 days and the average number of drinks per drinking session
In subgroup analyses, we found that HIV-infected participants taking ART ≥ 3 years had a slightly lower prevalence of hypertension (18.4% (81/440)) compared with those on ART for < 3 years (21% (26/124)). We also estimated the adjusted odds of prevalent hypertension by separating the HIV-infected participants into those with shorter (< 3years) or longer (≥3 years) duration of ART. We found that both groups had lower odds of hypertension compared with HIV-uninfected participants and the difference between the two groups were not statistically significant as indicated by a point estimate for one group falling within the 95% confidence interval for the other.
The indirect effect of HIV infection through BMI led to a 0.8 mmHg lower SBP (95% CI 0.3 to 1.5), equivalent to 25% of the total association between HIV and SBP. The corresponding proportion mediated by waist-hip ratio was only 6% (Figure 2. Panel B).
Figure 2.
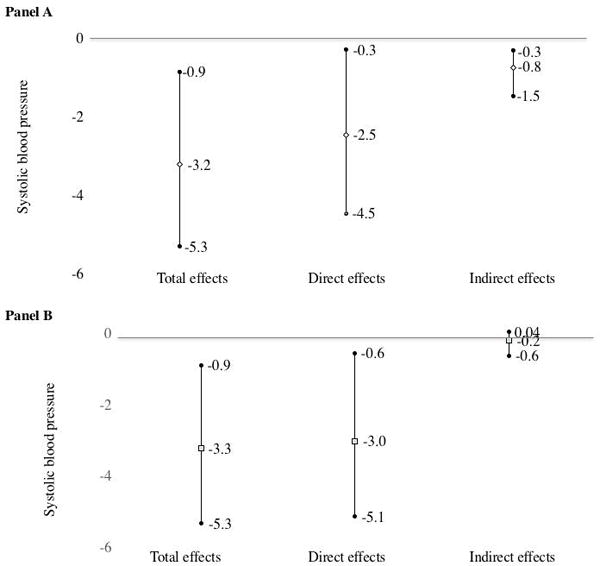
Total, direct, and indirect effects of HIV on systolic blood pressure with respect to body mass index (Panel A) and waist-hip ratio (Panel B), ACHIEvA study 2015
The relationship between HIV infection and hypertension care was complex and varied by gender: HIV-infected hypertensive participants had a higher chance of having been previously diagnosed (44% vs 28% in men, 56% vs 48% in women). Among men, HIV-infected participants who were diagnosed with hypertension had a higher chance of being treated (77% vs 47%) and among those treated, HIV-infected participants had a higher chance of being controlled (29% vs 11%) compared with HIV-uninfected counterparts. Among women, HIV-infected hypertensive participants were less likely to be treated (80% vs 88%) and among those treated, HIV-infected participants were less likely to be controlled (34% vs 61%) (Figure 3).
Figure 3.
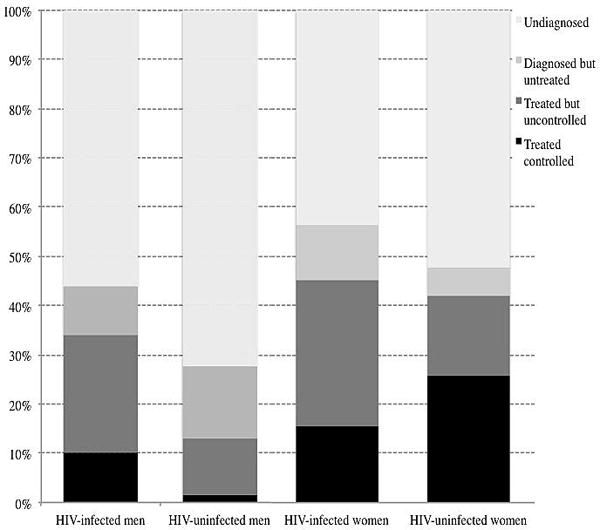
Hypertension awareness, treatment, and control by HIV status and gender, ACHIEvA study 2015
DISCUSSION
We found an inverse relationship between HIV and blood pressure, pulse wave velocity and odds of hypertension in this population of adults from an urban site in Uganda. Our results are similar to those reported in a meta-analysis of studies in Sub-Saharan Africa which found that HIV infection was associated with lower systolic and diastolic blood pressures.12 We postulate that this result could be explained by phenomenon of cardiovascular autonomic dysfunction that leads to the low blood pressure levels in HIV-infected persons irrespective of level of immunosuppression.38,39 Furthermore, HIV-infected patients in our study population tended to have an advanced HIV disease at entry into HIV care and might have had comorbid opportunistic infections that could lower their blood pressure levels directly or through weight loss.40 Conversely, other studies have found that HIV-infection with ART is associated with higher BP compared with HIV-uninfected persons with a similar sex and age distribution.7,17 The discrepancy between these results and our observation could be due to the rare (< 2%) use of protease inhibitors (PIs) in our study population. These agents are known to increase blood pressure levels7,41 and induce metabolic complications.17
We found that HIV infection was associated with lower PWV (arterial stiffness) compared to age, sex, and neighborhood-matched HIV-uninfected controls.42 This finding is in contrast to a few previous reports that found that HIV-infected patients under ART had higher PWV compared to HIV-infected not taking ART or HIV-uninfected matched controls.43,44 Most of our HIV-infected participants were not on PIs that have been shown to be pro-atherogenic and had suppressed viral replication at the time of study. The combined effect of low use of PIs and suppressed viral replication may have resulted in lower systemic inflammation and endothelial dysfunction leading to reduced arterial stiffness in HIV-infected participants.20 Furthermore, in our study cardiovascular risk factors such as obesity, physical inactivity, and dyslipidemia were more prevalent in the HIV-uninfected controls than the HIV-infected participants. This suggests traditional cardiovascular risk factors other than HIV-related characteristics are responsible for atherosclerosis and hypertension in HIV.10,45
We found that body mass index mediated a quarter of the association between HIV and systolic blood pressure. This confirms our expectation that lower body weight in HIV-infected patients is associated with lower blood pressure and is also consistent with the previous reports of increase in BP and body weight after initiation of ART.40,45,46 We did not find any prior studies that investigated the role of body mass index in mediating the effects of HIV on blood pressure to compare to ours.
As expected, we found that in both genders, hypertensive HIV-infected participants were more aware of their hypertension status and were more likely to be on treatment as compared to HIV-uninfected participants. However, among women, control rates were lower for HIV-infected participants. Although these differences are not statistically significant, they point to better chances of diagnosis and treatment for hypertension among HIV-infected participants but the overall rates are still suboptimal. The differences in prevalence rates of awareness, treatment, and control between HIV-infected and uninfected participants might be partly attributable to the differences in health seeking behaviors of HIV-infected and HIV-uninfected people47 as well as differences in resources (medical staff, facilities, and supplies) available in general health facilities compared to HIV care facilities48. Strategies to integrate HIV care with other health programs have focused primarily on tuberculosis, sexually transmitted infections, malaria, and reproductive health49,50 and there is only limited experience on integrating cardiovascular disease prevention into HIV care. A recent report from South Africa found that integrating non-communicable diseases care into HIV care is cost-effective and leads to improved functional ability and health status in HIV-infected patients.51
Our study has several strengths. HIV-infected participants were sampled from comprehensive databases of all patients receiving treatment in 2 of the 3 HIV-clinics in Mbarara, covering most of the diagnosed patients in the area. HIV-uninfected participants were selected from the same neighborhood which greatly reduces the potential for confounding by location of residence and socioeconomic status. In addition to blood pressure, we measured pulse wave velocity as an indicator of early atherosclerosis, which has not been investigated with respect to HIV-status in sub-Saharan Africa. We used a rigorous and standard BP measurement protocol and collected information on many lifestyle and socioeconomic factors using standard and validated questionnaires. However, our results should be interpreted with some limitations in mind. Although we collected data on many potential confounders, there is always a potential for unmeasured confounding and residual confounding due to measurement error in the selected confounders. As most of the participants were on ART, we were not able to examine the impact of ART on blood pressure and hypertension as a mediator of the effect of HIV infection. In addition, there was little variability in ART regimens in our study population, precluding analysis of impact of different ART regimens on BP.
In conclusion, HIV infection was associated with lower systolic blood pressure, pulse-wave velocity and odds of hypertension. Although HIV infection was associated with a higher chance of diagnosis and treatment of hypertension, and better control rates among men, it was associated with worse control rates among women. To improve cardiovascular disease care among HIV patients, health-centered services should be combined with community-level approaches to improve the reach and cost-effectiveness of preventive interventions. Such health care models remain largely untapped in HIV-endemic countries such as Uganda.
Supplementary Material
Acknowledgments
The authors would like to thank the staff at the Immune Suppression Syndrome (ISS) clinic and Mbarara Municipal Council health IV, Medexpert Ltd Budapest (Hungary) for providing Arteriogram devices. Study staff: Abia Begumisa, Agnes Alupo, Boaz Niwamanya, Chris Mugume, Christine Kazungu, Daniel Nabimanya, Daphine K. Atwine, Elizabeth Ninsiima, Emily Ashaba, Emmanuel Ndyabahika, Gertrude Kyarimpa, Harriet Akidi, Hope Namanya, Jonath Tumusiime, Jovita Kyosiimire, Martin Kiwe, Mary Tumweshengyereze, Milliam Korukiiko, Opherous Oshabahebwa, Patrick Oroma, Phionah Ampaire, Resty Nalugya, Ronald Mwesigye, Thelema B. Kateeba, and Tony Engwau.
Sources of funding: This study was supported by the Bernard Lown Scholars in Cardiovascular Health Program and a pilot grant through the Center for the Global Demography of Aging (National Institute of Health: AG024409) at Harvard T. H Chan School of Public Health. The funders had no role in study design, conduct, data analysis, or production of manuscript.
Footnotes
Disclosure of Previous Presentations: None
DR. SAMSON OKELLO (Orcid ID : 0000-0001-7377-6094)
Financial Disclosure: The authors have no financial or other potential conflict of interest with regard to this manuscript.
Author Contributions: S.O, P.U, A.K, E.B, W.R.M, and G.D, conceptualized and designed the study; S.O and P.U analyzed the data. S.O wrote the first draft of the manuscript. S.O, P.U, A.K, E.B, A.K, G.A, W.R.M, and G.D, contributed to the write-up and edited the manuscript. All authors approved the manuscript.
References
- 1.UNAIDS. Global Report 2012: UNAIDS Report on the Global AIDS Epidemic. 2013 ebookpartnership.com.
- 2.Mills EJ, Bakanda C, Birungi J, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Annals of internal medicine. 2011;155(4):209–216. doi: 10.7326/0003-4819-155-4-201108160-00358. [DOI] [PubMed] [Google Scholar]
- 3.Floyd S, Molesworth A, Dube A, et al. Population-level reduction in adult mortality after extension of free anti-retroviral therapy provision into rural areas in northern Malawi. PLoS One. 2010;5(10):e13499. doi: 10.1371/journal.pone.0013499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Johnson LF, Mossong J, Dorrington RE, et al. Life expectancies of South african adults starting antiretroviral treatment: collaborative analysis of cohort studies. PLoS medicine. 2013;10(4):e1001418. doi: 10.1371/journal.pmed.1001418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bor J, Herbst AJ, Newell M-L, Bärnighausen T. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment. Science. 2013;339(6122):961–965. doi: 10.1126/science.1230413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nduka CU, Stranges S, Bloomfield GS, et al. A plausible causal link between antiretroviral therapy and increased blood pressure in a sub-Saharan African setting: A propensity score-matched analysis. International Journal of Cardiology. 2016 doi: 10.1016/j.ijcard.2016.06.210. [DOI] [PubMed] [Google Scholar]
- 7.Seaberg EC, Munoz A, Lu M, et al. Association between highly active antiretroviral therapy and hypertension in a large cohort of men followed from 1984 to 2003. Aids. 2005;19(9):953–960. doi: 10.1097/01.aids.0000171410.76607.f8. [DOI] [PubMed] [Google Scholar]
- 8.Baekken M, Os I, Sandvik L, Oektedalen O. Hypertension in an urban HIV-positive population compared with the general population: influence of combination antiretroviral therapy. Journal of hypertension. 2008;26(11):2126–2133. doi: 10.1097/HJH.0b013e32830ef5fb. [DOI] [PubMed] [Google Scholar]
- 9.Durand M, Sheehy O, Baril J-G, Lelorier J, Tremblay CL. Association between HIV infection, antiretroviral therapy, and risk of acute myocardial infarction: a cohort and nested case–control study using Quebec’s public health insurance database. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2011;57(3):245–253. doi: 10.1097/QAI.0b013e31821d33a5. [DOI] [PubMed] [Google Scholar]
- 10.Triant VA, Lee H, Hadigan C, Grinspoon SK. Increased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus disease. The Journal of Clinical Endocrinology & Metabolism. 2007;92(7):2506–2512. doi: 10.1210/jc.2006-2190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schutte AE, Schutte R, Huisman HW, et al. Are behavioural risk factors to be blamed for the conversion from optimal blood pressure to hypertensive status in Black South Africans? A 5-year prospective study. International journal of epidemiology. 2012:dys106. doi: 10.1093/ije/dys106. [DOI] [PubMed] [Google Scholar]
- 12.Dillon DG, Gurdasani D, Riha J, et al. Association of HIV and ART with cardiometabolic traits in sub-Saharan Africa: a systematic review and meta-analysis. International journal of epidemiology. 2013;42(6):1754–1771. doi: 10.1093/ije/dyt198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Scholten F, Mugisha J, Seeley J, et al. Health and functional status among older people with HIV/AIDS in Uganda. BMC Public Health. 2011;11(1):886. doi: 10.1186/1471-2458-11-886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bergersen B, Sandvik L, Dunlop O, Birkeland K, Bruun J. Prevalence of hypertension in HIV-positive patients on highly active retroviral therapy (HAART) compared with HAART-naive and HIV-negative controls: results from a Norwegian study of 721 patients. European Journal of Clinical Microbiology and Infectious Diseases. 2003;22(12):731–736. doi: 10.1007/s10096-003-1034-z. [DOI] [PubMed] [Google Scholar]
- 15.Khalsa A, Karim R, Mack WJ, et al. Correlates of prevalent hypertension in a large cohort of HIV-infected women: Women’s Interagency HIV Study. AIDS. 2007;21(18):2539–2541. doi: 10.1097/QAD.0b013e3282f15f7b. [DOI] [PubMed] [Google Scholar]
- 16.Jericó C, Knobel H, Montero M, et al. Hypertension in HIV-infected patients: prevalence and related factors. American journal of hypertension. 2005;18(11):1396–1401. doi: 10.1016/j.amjhyper.2005.05.016. [DOI] [PubMed] [Google Scholar]
- 17.Gazzaruso C, Bruno R, Garzaniti A, et al. Hypertension among HIV patients: prevalence and relationships to insulin resistance and metabolic syndrome. Journal of hypertension. 2003;21(7):1377–1382. doi: 10.1097/01.hjh.0000059071.43904.dc. [DOI] [PubMed] [Google Scholar]
- 18.Schouten J, Wit FW, Stolte IG, et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study. Clinical Infectious Diseases. 2014;59(12):1787–1797. doi: 10.1093/cid/ciu701. [DOI] [PubMed] [Google Scholar]
- 19.Ikonomidis I, Lekakis J, Papadopoulos C, et al. Incremental value of pulse wave velocity in the determination of coronary microcirculatory dysfunction in never-treated patients with essential hypertension. American journal of hypertension. 2008;21(7):806–813. doi: 10.1038/ajh.2008.172. [DOI] [PubMed] [Google Scholar]
- 20.Echeverría P, Bonjoch A, Moltó J, et al. Pulse wave velocity as index of arterial stiffness in HIV-infected patients compared with a healthy population. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2014;65(1):50–56. doi: 10.1097/QAI.0b013e3182a97c17. [DOI] [PubMed] [Google Scholar]
- 21.Maia-Leite LH, Catez E, Boyd A, et al. Aortic stiffness aging is influenced by past profound immunodeficiency in HIV-infected individuals: results from the EVAS-HIV (EValuation of Aortic Stiffness in HIV-infected individuals) Journal of hypertension. 2016;34(7):1338–1346. doi: 10.1097/HJH.0000000000000957. [DOI] [PubMed] [Google Scholar]
- 22.Althoff K, Gange S. A critical epidemiological review of cardiovascular disease risk in HIV-infected adults: the importance of the HIV-uninfected comparison group, confounding, and competing risks. HIV medicine. 2013;14(3):191–192. doi: 10.1111/hiv.12007. [DOI] [PubMed] [Google Scholar]
- 23.Grotto I, Huerta M, Sharabi Y. Hypertension and socioeconomic status. Current opinion in cardiology. 2008;23(4):335–339. doi: 10.1097/HCO.0b013e3283021c70. [DOI] [PubMed] [Google Scholar]
- 24.Leng B, Jin Y, Li G, Chen L, Jin N. Socioeconomic status and hypertension: a meta-analysis. Journal of hypertension. 2015;33(2):221–229. doi: 10.1097/HJH.0000000000000428. [DOI] [PubMed] [Google Scholar]
- 25.Sliwa K, Acquah L, Gersh BJ, Mocumbi AO. Impact of socioeconomic status, ethnicity, and urbanization on risk factor profiles of cardiovascular disease in Africa. Circulation. 2016;133(12):1199–1208. doi: 10.1161/CIRCULATIONAHA.114.008730. [DOI] [PubMed] [Google Scholar]
- 26.Le KT, Brick JM, Diop A, Alemadi D. Within-household sampling conditioning on household size. International Journal of Public Opinion Research. 2013;25(1):108–118. [Google Scholar]
- 27.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of health and social behavior. 1983:385–396. [PubMed] [Google Scholar]
- 28.Sobngwi E, Mbanya JC, Unwin NC, Aspray TJ, Alberti KG. Development and validation of a questionnaire for the assessment of physical activity in epidemiological studies in Sub-Saharan Africa. Int J Epidemiol. 2001;30(6):1361–1368. doi: 10.1093/ije/30.6.1361. [DOI] [PubMed] [Google Scholar]
- 29.Bradley KA, DeBenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcoholism: Clinical and Experimental Research. 2007;31(7):1208–1217. doi: 10.1111/j.1530-0277.2007.00403.x. [DOI] [PubMed] [Google Scholar]
- 30.Consultation WE. Waist circumference and waist-hip ratio. Report of a WHO Expert Consultation Geneva: World Health Organization. 2008:8–11. [Google Scholar]
- 31.Mente A, O’Donnell MJ, Dagenais G, et al. Validation and comparison of three formulae to estimate sodium and potassium excretion from a single morning fasting urine compared to 24-h measures in 11 countries. Journal of hypertension. 2014;32(5):1005–1015. doi: 10.1097/HJH.0000000000000122. [DOI] [PubMed] [Google Scholar]
- 32.Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. Jama. 2003;289(19):2560–2571. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- 33.TensioMed. ArterioGraph User’s Manual. In: Arteriograph T, editor. TensioMed Arteriograph. Budapest, Hungary: TensioMed; 2011. pp. 5–02. [Google Scholar]
- 34.Filmer D, Pritchett LH. Estimating wealth effects without expenditure Data—Or tears: An application to educational enrollments in states of india*. Demography. 2001;38(1):115–132. doi: 10.1353/dem.2001.0003. [DOI] [PubMed] [Google Scholar]
- 35.Himelein K. Interviewer effects in subjective survey questions: evidence from Timor-Leste. International Journal of Public Opinion Research. 2015:edv031. [Google Scholar]
- 36.MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annual review of psychology. 2007;58:593. doi: 10.1146/annurev.psych.58.110405.085542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Emsley R, Liu H. PARAMED: Stata module to perform causal mediation analysis using parametric regression models. Statistical Software Components. 2013 [Google Scholar]
- 38.Nzuobontane D, Ngu BK, Christopher K. Cardiovascular autonomic dysfunction in Africans infected with human immunodeficiency virus. Journal of the Royal Society of Medicine. 2002;95(9):445–447. doi: 10.1258/jrsm.95.9.445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mattana J, Siegal FP, Sankaran RT, Singhal PC. Absence of age-related increase in systolic blood pressure in ambulatory patients with HIV infection. The American journal of the medical sciences. 1999;317(4):232–237. doi: 10.1097/00000441-199904000-00004. [DOI] [PubMed] [Google Scholar]
- 40.Feigl AB, Bloom DE, Danaei G, et al. The effect of HIV and the modifying effect of anti-retroviral therapy (ART) on body mass index (BMI) and blood pressure levels in Rural South Africa. PLoS One. 2016;11(8):e0158264. doi: 10.1371/journal.pone.0158264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chow DC, Souza SA, Chen R, Richmond-Crum SM, Grandinetti A, Shikuma C. Elevated blood pressure in HIV-infected individuals receiving highly active antiretroviral therapy. HIV clinical trials. 2003;4(6):411–416. doi: 10.1310/5E7Q-PGWB-16UE-J48U. [DOI] [PubMed] [Google Scholar]
- 42.Papita AM, Albu A, Fodor D, Bondor C, Itu C, Cârstina D. Markers of preclinical vascular disease and left ventricular diastolic dysfunction in patients with HIV infection. Medical ultrasonography. 2012;14(1):10. [PubMed] [Google Scholar]
- 43.Lekakis J, Ikonomidis I, Palios J, et al. Association of highly active antiretroviral therapy with increased arterial stiffness in patients infected with human immunodeficiency virus. American journal of hypertension. 2009;22(8):828–834. doi: 10.1038/ajh.2009.90. [DOI] [PubMed] [Google Scholar]
- 44.Schillaci G, De Socio GV, Pucci G, et al. Aortic stiffness in untreated adult patients with human immunodeficiency virus infection. Hypertension. 2008;52(2):308–313. doi: 10.1161/HYPERTENSIONAHA.108.114660. [DOI] [PubMed] [Google Scholar]
- 45.Okello S, Kanyesigye M, Muyindike WR, et al. Incidence and Predictors of Hypertension in Adults with HIV Initiating Antiretroviral Therapy in Southwestern Uganda. Journal of hypertension. 2015;33(10):2039. doi: 10.1097/HJH.0000000000000657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Palacios R, Santos J, Garcia A, et al. Impact of highly active antiretroviral therapy on blood pressure in HIV-infected patients. A prospective study in a cohort of naive patients. HIV medicine. 2006;7(1):10–15. doi: 10.1111/j.1468-1293.2005.00333.x. [DOI] [PubMed] [Google Scholar]
- 47.Crawford TN, Sanderson WT, Breheny P, Fleming ST, Thornton A. Impact of non-HIV related comorbidities on retention in HIV medical care: does retention improve over time? AIDS and Behavior. 2014;18(3):617–624. doi: 10.1007/s10461-013-0524-y. [DOI] [PubMed] [Google Scholar]
- 48.Mayosi BM, Benatar SR. Health and health care in South Africa—20 years after Mandela. New England Journal of Medicine. 2014;371(14):1344–1353. doi: 10.1056/NEJMsr1405012. [DOI] [PubMed] [Google Scholar]
- 49.Hermans SM, Castelnuovo B, Katabira C, et al. Integration of HIV and TB services results in improved TB treatment outcomes and earlier, prioritized ART initiation in a large urban HIV clinic in Uganda. Journal of acquired immune deficiency syndromes (1999) 2012;60(2):e29. doi: 10.1097/QAI.0b013e318251aeb4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hope R, Kendall T, Langer A, Bärnighausen T. Health systems integration of sexual and reproductive health and HIV services in sub-Saharan Africa: a scoping study. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2014;67:S259–S270. doi: 10.1097/QAI.0000000000000381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Levitt NS, Steyn K, Dave J, Bradshaw D. Chronic noncommunicable diseases and HIV-AIDS on a collision course: relevance for health care delivery, particularly in low-resource settings—insights from South Africa. The American journal of clinical nutrition. 2011;94(6):1690S–1696S. doi: 10.3945/ajcn.111.019075. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.