

Abstract
Objective
The aim of this study was to compare the accuracy of cone beam CT (CBCT) with intraoral radiographs for detection of occlusal caries.
Methods
A set of 60 extracted teeth were imaged using a Sirona Galileos CBCT system (Sirona Dental Systems, Bensheim, Germany) and an intraoral Planmeca® system (Planmeca OY, Helsinki, Finland). Six observers looked at both modalities and used a five-point confidence scale to evaluate presence or absence of occlusal caries. Histology was used as the gold standard. Receiver operating characteristic analysis and weighted kappa statistics were used for statistical analysis. Differences in the area under the curve (AUC) values between observers and modalities were analysed using analysis of variance (ANOVA). Differences in sensitivity and specificity were analysed using the Wilcoxon test. Interobserver and intraobserver reliability was assessed by weighted kappa scores.
Results
The mean value and standard deviation of AUC was 0.719 ± 0.038 for CBCT and 0.649 ± 0.062 for the intraoral radiographs. The ANOVA results demonstrated that there was no significant difference between the modalities and the observers. The interobserver kappa for pairs of observers ranged from fair to substantial for bitewings (0.244–0.543) and CBCT (0.152–0.401). Four out of six observers reported higher sensitivity but lower specificity with CBCT. The Wilcoxon exact p-value showed no difference in sensitivity (0.175) or specificity (0.573) between the two modalities.
Conclusion
Based on the results we conclude that the Sirona CBCT unit cannot be used for the sole purpose of looking at occlusal caries.
Keywords: caries, cone beam computed, cone beam computed tomography, dental, tomography
Introduction
Over the last decade, the worldwide prevalence of dental caries has declined remarkably. However, even in populations with decreased caries prevalence, the proportion of occlusal caries has increased and accurately detecting incipient pit and fissure lesions remains a challenge.1
US dentists commonly diagnose occlusal caries using visual/tactile methods or visual inspection aided by radiographs. Bader et al found that visual-tactile methods have low sensitivity and moderate-to-high specificity in detecting occlusal lesions.2 Also, in a clinical setting, studies have reported no difference in performance between digital and conventional radiographs.3,4
The introduction of a new technology, tuned aperture CT, has also shown no promise in improving diagnosis of the primary caries.5-7 Studies have shown that some non-radiographic methods such as quantitative light induced fluorescence, electronic carie monitor, DIAGNOdent (KaVo Dental, Charlotte, NC), digital imaging fiberoptic transillumination or fiberoptic transillumination should be used as an adjunct to clinical decision making and serve primarily as a support tool for making preventive treatment plan decisions in conjunction with caries risk assessment.8,9
Although clinical diagnostic methods are highly specific with a low sensitivity, particularly for non-cavitated occlusal surfaces in vivo, means that new methods for caries diagnosis are required.10
The development of cone beam CT (CBCT) has been revolutionary in that this technology provides the dental clinician with an imaging modality capable of providing a three-dimensional (3D) representation of the maxillofacial skeleton with minimal distortion and radiation dosages up to 15 times lower than those of conventional CT scans. The specific aim for our study was to compare the accuracy of the Sirona Galileos CBCT system (Sirona Dental Systems, Bensheim, Germany) with intraoral bitewing radiographs in the diagnosis of occlusal caries. Our hypothesis was that there will be no difference in caries detection between the two modalities.
Materials and methods
Sample size
This was an in vitro study with a sample of 60 extracted premolar and molar teeth. Half the teeth were selected as test teeth and the other half were controls. The inclusion criteria for the test teeth was incipient occlusal caries as determined by either visual examination or a definite catch/tug back using the explorer. Any teeth that had large cavitated surfaces or restorations were excluded from the test sample. Some of these teeth also had proximal lesions but those surfaces were not included in our study. The teeth were collected from the departments of Periodontology, Prosthodontics and Oral and Maxillofacial Surgery.
Image acquisition
A human dried mandible with a set of teeth placed in wax was used to simulate the patient's dental structures and soft tissues. Each tooth was mounted individually in an extraction socket, created specifically for the experimental tooth. The mandible was surrounded by a plexiglass box to simulate soft tissues. Both the wax rim and the plexiglass box simulate soft tissue scatter. These teeth were imaged using the Galileos (Sirona) CBCT unit. The images were reconstructed into the “close-up view” which features 150 micron pixels. 60 separate scans were taken and these images were then reconstructed to different cross-sectional, axial and tangential views. Tangential is the Galileos term for a longitudinal view through the tooth, parallel to the mesiodistal dimensions of the teeth. The exposure parameters for the CBCT were set at 85 kVp and 21 mAs, with a total exposure time of 2–4 s.
The teeth were then imaged using a Planmeca (Planmeca Oy, Helsinki, Finland) intraoral source and a (Gendex Dental Systems, Hatfield, PA) photostimulable phosphor (PSP) imaging system. The exposure parameters for this system were set at 70 kVp and 3.2 s as the exposure time. After imaging, the teeth were sectioned using an IsoMet® low-speed saw (Buehler, Lake Bluff, IL) to establish the gold standard diagnosis. They were sectioned to 250 μm thin sections and viewed under a stereomicroscope. Of the 60 teeth, 27 teeth were determined by histology to have occlusal caries and the other 33 were without carious lesions.
Observation sessions
Six observers viewed all the images from both the modalities. The observers were not informed about the caries prevalence in the sample prior to evaluation. These observers were two radiologists, two radiology residents and two general dentists. They were asked to record the presence or absence of occlusal caries on a five-point confidence scale: 1 = caries definitely absent, 2 = caries probably absent, 3 = unsure if caries absent or present, 4 = caries probably present and 5 = caries definitely present. As this was an initial study, we did not carry out depth estimates of the carious lesions. The observers were given a short training session in using Galileos viewing software and were provided with an instruction brochure on how to observe the images. The observers were also allowed to manipulate the brightness and contrast of the PSP images. The intraoral images were viewed using Vixwin 2000 (version 1.11, Gendex). To standardize the viewing conditions all the images from both modalities were viewed using one computer (Lenovo ThinkVision™, IBM, Armonk, NY) in the radiology clinic. The images were displayed at a resolution of 1280 × 1024 pixels under dimmed lighting conditions.
The observers had the flexibility to scroll through the entire volume of images for each of the 60 teeth. The observers were asked to repeat their observations after 2 weeks in order to evaluate for intraobserver reliability. For this purpose a set of 20 teeth were randomly selected from the entire sample. Figure 1 shows occlusal caries in the close-up view using Sirona and the intraoral radiograph.
Figure 1.

(a) Close-up view of one of the test teeth using the Sirona Galileos cone beam CT system (Sirona Dental Systems, Bensheim, Germany). (b) Intraoral radiograph for one of the test teeth
Statistical methods
Receiver operating characteristic (ROC) curves were constructed for each observer and each modality. Diagnostic accuracy was expressed as the area under the curve (AUC). The difference in the AUC for the two modalities was compared using analysis of variance (ANOVA), controlling for observer. The data was dichotomized with scores of 1, 2 and 3 representing a negative finding (caries absent) and scores of 4 and 5 representing a positive finding (caries present). Using this dichotomization, the sensitivity and specificity of the two modalities were compared with the exact Wilcoxon rank-sum test. Interobserver and intraobserver reliability were assessed by weighted kappa scores. Analyses were done using SAS software (version 9.2, SAS Institute, Inc, Cary, NC).
Results
The diagnostic accuracy of the two radiographic systems was assessed using the ROC AUC (Figure 2). The means of the AUC for CBCT and intraoral radiographs were 0.72 and 0.65, respectively (Table 1). The difference between the modalities, controlling for observers, was not significant (p = 0.07).
Figure 2.
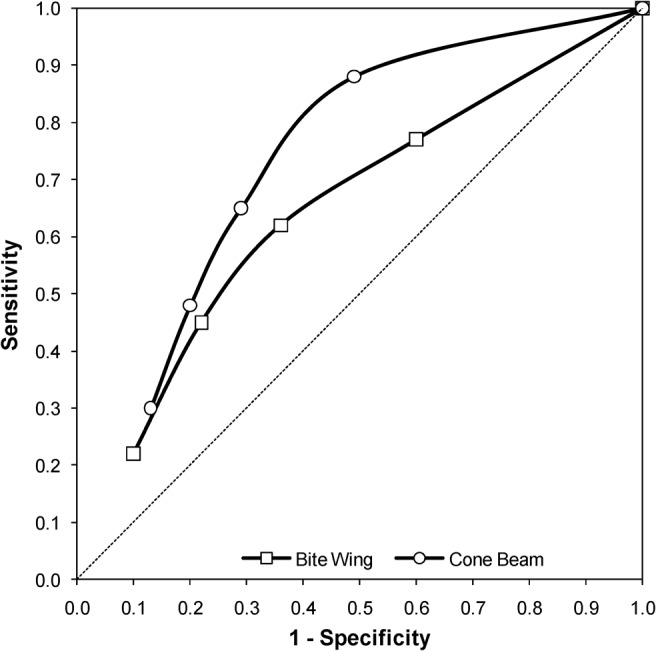
Receiver operating characteristic curves for bitewing and cone beam CT. Pooled data across observers
Table 1. Caries detection accuracy as measured by the area under the curve of a receiver operating characteristic (ROC) curve, sensitivity and specificity.
| Bite wing |
Cone beam CT |
|||||
| Observer | AUC | Sensitivity | Specificity | AUC | Sensitivity | Specificity |
| 1 | 0.635 | 66.67 | 63.34 | 0.669 | 77.78 | 51.52 |
| 2 | 0.646 | 77.78 | 48.48 | 0.703 | 74.07 | 66.67 |
| 3 | 0.700 | 51.85 | 78.79 | 0.690 | 70.37 | 54.55 |
| 4 | 0.736 | 62.96 | 78.79 | 0.769 | 66.67 | 69.70 |
| 5 | 0.556 | 51.85 | 54.55 | 0.751 | 51.85 | 84.85 |
| 6 | 0.622 | 62.96 | 51.52 | 0.737 | 81.48 | 63.64 |
| Mean | 0.649 | 62.35 | 62.58 | 0.720 | 70.37 | 65.16 |
| SD | 0.063 | 9.78 | 13.50 | 0.039 | 10.48 | 11.93 |
AUC, area under curve; SD, standard deviation.
The difference in sensitivity (Wilcoxon: p = 0.18) and specificity (Wilcoxon: p = 0.57) between the two modalities was not statistically significant. The interobserver kappa for pairs of observers ranged from fair to moderate [0.24–0.54, mean = 0.40, standard deviation (SD) = 0.09] for bitewings and slight to fair (0.15–0.40, mean = 0.28, SD = 0.06) for CBCT. The intraobserver kappa ranged from moderate to substantial for both bitewings (0.52–0.81, mean = 0.68, SD = 0.10) and CBCT (0.50–0.85, mean = 0.65, SD = 0.12). Four out of six observers reported higher sensitivity with CBCT. The mean and SD across observers for both modalities were calculated.
Discussion
The use of CBCT in dentistry for 3D imaging is becoming more widespread.11 Its potential to visualize minute changes in both the teeth and the surrounding structures is making it the modality of choice for an increasing number of diagnostic and treatment planning tasks. However, as CBCT is a new radiographic modality, its accuracy for various diagnostic tasks must be compared with existing well-established two-dimensional (2D) systems. The aim of the present study was to compare the accuracy of CBCT with intraoral radiographs in detecting occlusal caries.
Our present study concluded that there were no statistically significant differences between the Sirona Galileos CBCT (in the close-up or magnified mode) and conventional radiography for occlusal caries detection. In recent years, a number of studies have been carried out to establish the accuracy of CBCT for caries detection. A technology called local-CT (LCT) was investigated by van-Daatselaar et al12 and subsequently by Kalathingal et al.13 While van-Daatselaar et al found that under specific viewing modes LCT outperformed conventional 2D imaging using a PSP system, Kalathingal et al found no difference between the two modalities. However, Kalathingal et al did find that LCT was more accurate in assessing caries depth.
Accuracy studies of clinical CBCT systems evaluating occlusal/proximal caries have had varied results. Akdeniz et al14 compared the Accuitomo (3DX) CBCT (J Morita USA, Irvine, CA), Digora-fmxTM (Soredex, Tuusula, Finland) and Insight film (Eastman Kodak, Rochester, NY) for measuring depth of proximal caries lesions. The authors found that the Accuitomo images provided more accurate lesion depth estimates with less variation when compared with measurements performed on the sections of the tooth than the intraoral images and therefore suggested that CBCT appears to be a promising tool for monitoring small caries lesions. Tsuchida et al15 also assessed the accuracy of the 3D Accuitomo in evaluating incipient proximal caries and found that 3D Accuitomo could not enhance the accuracy in detecting the carious lesions.
In a study of non-cavitated teeth, a large field of view (FOV) CBCT performed poorer in detection of caries while a limited FOV CBCT had higher sensitivity only for occlusal caries compared with digital or conventional periapical radiographs.16
We used ROC analysis to evaluate the diagnostic performance of the two modalities. The analysis is made by comparing significant differences between the areas under the ROC curves that represent the competing modalities.17 An advantage of using ROC analysis is that it reflects the diagnostic performance more comprehensively than sensitivity and specificity, which are determined by only one cut-off point.18 It also provides the most meaningful approach to compare the diagnostic performance of two or more different imaging modalities because it distinguishes between the inherent capacities of the observers to under- and over-read when interpreting imaging and is used in many studies.19,20
In our study, AUC for CBCT and intraoral radiographs was 0.72 and 0.65, respectively. To interpret these results an area of 1 represents a perfect test and anything near 0.5 is a poor test result.21 Applying this standard to our results indicates that neither test could be considered very accurate.
The interobserver kappa for pairs of observers ranged from fair to moderate (0.24–0.54) for bitewings and slight to fair (0.15–0.40) for CBCT. When reporting kappa statistics, a perfect agreement would equate to κ = 1 and chance agreement would equate to 0.22 We had calibrated the observers prior to their observation sessions but there were some differences in the observers based on their experience and training with CBCT.
In conclusion, the data from this study support our hypothesis that there is no difference in the diagnostic accuracy of the Galileos CBCT system and intraoral PSP radiographs for the diagnosis of occlusal caries. Some may argue that CBCT could still be considered superior owing to its simplicity and the fact that it is an extraoral imaging modality. However it is to be noted that most of these are in vitro studies which are performed under “ideal” or well-controlled experimental settings. In our study specifically, we could not replicate the beam hardening artefacts or patient motion errors that could account for significant distortion in the image.
Beam hardening artefacts originate from metallic restorations, implants, endodontic restorative materials and create streaks of bright and dark bands and noisy projection reconstructions that project over adjacent teeth and render diagnosis difficult or unfeasible. In particular, the dark bands may convey the false impression of recurrent caries. Patient movement similarly decreases structure sharpness and definition, further complicating the diagnostic process.23
The spatial resolution and resultant detail perception would be considerably less for in vivo data considering many seconds of image acquisition.
The second issue with CBCT is related to patient dose. In a recent editorial by Farman,24 the principle of as low as reasonably achievable is still fundamental for diagnostic radiology and CBCT procedures should be reserved for selected cases. Diagnostic benefit and dose detriment tradeoffs are important considerations in choices of radiographic procedures. The effective dose of Sirona CBCT is 70 μSv, in line with the International Commission on Radiological Protection 2007 standards, compared with 5.0 μSv for a four-image posterior bitewings with PSP or F-speed film with rectangular collimation or 34.9 μSv for full-mouth radiographs with PSP storage or F-speed film with rectangular collimation.25,26 Also, a CBCT exam is more expensive compared with traditional intraoral images.
From the results of this study we concluded that using the Galileos CBCT for the sole purpose of diagnosing occlusal caries was not justified.
References
- 1.Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG. Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res 2006;40:194–201 [DOI] [PubMed] [Google Scholar]
- 2.Ismail A. Visual and visuo-tactile detection of dental caries. J Dent Res 2004;83:C56–66 [DOI] [PubMed] [Google Scholar]
- 3.Wenzel A. Digital radiography and caries diagnosis. Dentomaxillofac Radiol 1998;27:3–11 [DOI] [PubMed] [Google Scholar]
- 4.Wenzel A. Bitewing and digital bitewing radiography for detection of caries lesions. J Dent Res 2004;83:C72–75 [DOI] [PubMed] [Google Scholar]
- 5.Tyndall DA, Clifton TL, Webber RL, Ludlow JB, Horton RA. TACT imaging of primary caries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84:214–225 [DOI] [PubMed] [Google Scholar]
- 6.Shi XQ, Han P, Welander U, Angmar-Mansson B. Tuned-aperture computed tomography for detection of occlusal caries. Dentomaxillofac Radiol 2001;30:45–49 [DOI] [PubMed] [Google Scholar]
- 7.Abreu Júnior M, Tyndall DA, Platin E, Ludlow JB, Phillips C. Two- and three-dimensional imaging modalities for the detection of caries. A comparison between film, digital radiography and tuned aperture computed tomography (TACT). Dentomaxillofac Radiol 1999;28:152–157 [DOI] [PubMed] [Google Scholar]
- 8.Zandona AF, Zero DT. Diagnostic tools for early caries detection. J Am Dent Assoc 2006;137:1675–1684 [DOI] [PubMed] [Google Scholar]
- 9.Tam LE, McComb D. Diagnosis of occlusal caries: Part II. Recent diagnostic technologies. J Can Dent Assoc 2001;67:459–463 [PubMed] [Google Scholar]
- 10.Pitts N. Clinical diagnosis of dental caries: a European perspective. J Dent Educ 2001;65:972–978 [PubMed] [Google Scholar]
- 11.Mozzo P, Procacci C, Tacconi A, Tinazzi Martini P, Bergamo Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 1998. 11; 8:1558–1564 [DOI] [PubMed] [Google Scholar]
- 12.van Daatselaar A, Tyndall D, van derStelt P. Detection of caries with local CT. Dentomaxillofac Radiol 2003;32:235–241 [DOI] [PubMed] [Google Scholar]
- 13.Kalathingal SM, Mol A, Tyndall DA, Caplan DJ, Hill C. In vitro assessment of cone beam local computed tomography for proximal caries detection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:699–704 [DOI] [PubMed] [Google Scholar]
- 14.Akdeniz G, Gröndahl H, Magnusson B. Accuracy of proximal caries depth measurements: comparison between limited cone beam computed tomography, storage phosphor and film radiography. Caries Res 2006;40:202–207 [DOI] [PubMed] [Google Scholar]
- 15.Tsuchida R, Araki K, Okano T. Evaluation of a limited cone-beam volumetric imaging system: comparison with film radiography in detecting incipient proximal caries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:412–416 [DOI] [PubMed] [Google Scholar]
- 16.Tetradis S, Anstey P, Graff-Radford S. Cone beam computed tomography in the diagnosis of dental disease. J Calif Dent Assoc 2010;38:27–32 [PubMed] [Google Scholar]
- 17.Kantor M, Zeichner S, Valachovic R, Reiskin A. Efficacy of dental radiographic practices: options for image receptors, examination selection, and patient selection. J Am Dent Assoc 1989;119:259–268 [DOI] [PubMed] [Google Scholar]
- 18.Kositbowornchai S, Basiw M, Promwang Y, Moragorn H, Sooksuntisakoonchai N. Accuracy of diagnosing occlusal caries using enhanced digital images. Dentomaxillofac Radiol 2004;33:236–240 [DOI] [PubMed] [Google Scholar]
- 19.Tyndall DA, Ludlow JB, Platin E, Nair M. A comparison of kodak ektaspeed plus film and the siemens sidexis digital imaging system for caries detection using receiver operating characteristic analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:113–118 [DOI] [PubMed] [Google Scholar]
- 20.Akkaya N, Kansu O, Kansu H, Cagirankaya L, Arslan U. Comparing the accuracy of panoramic and intraoral radiography in the diagnosis of proximal caries. Dentomaxillofac Radiol 2006;35:170–174 [DOI] [PubMed] [Google Scholar]
- 21.Hintze H, Frydenberg M, Wenzel A. Influence of number of surfaces and observers on statistical power in a multiobserver ROC radiographic caries detection study. Caries Res 2003;37:200–205 [DOI] [PubMed] [Google Scholar]
- 22.Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa statistic. Fam Med 2005;37:360–363 [PubMed] [Google Scholar]
- 23.Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am 2008 Oct;52:707–730 [DOI] [PubMed] [Google Scholar]
- 24.Farman AG. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100:395–397 [DOI] [PubMed] [Google Scholar]
- 25.Ludlow J, Davies-Ludlow L, Brooks S, Howerton W. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology:CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac Radiol 2006;35:219–226 [DOI] [PubMed] [Google Scholar]
- 26.Ludlow JB, Davies-Ludlow LE, White SC. Patient risk related to common dental radiographic examinations: the impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculation. JADA 2008;139:1237–1243 [DOI] [PubMed] [Google Scholar]