

Abstract
Diabetic macular edema (DME) remains an important cause of visual loss in patients with diabetes mellitus. Although photocoagulation and intensive control of systemic metabolic factors have been reported to achieve improved outcomes in large randomized clinical trials (RCTs), some patients with DME continue to lose vision despite treatment. Pharmacotherapies for DME include locally and systemically administered agents. We review several agents that have been studied for the treatment of DME.
1. Introduction
Diabetic macular edema (DME) is one of the most common causes of visual loss in patients with diabetes mellitus [1]. The pathophysiology of DME involves dilated capillaries, retinal microaneurysms, and loss of pericytes, with eventual impairment of the blood-retinal barrier (BRB) [2]. Breakdown of the BRB results in fluid leakage into the extracellular space, which disrupts macular structure and function on a cellular level [3, 4]. A technique for visualizing molecules leaked through the outer BRB in a diabetic rodent model has recently been described, which should increase our understanding of this process [5].
This leakage may be analyzed in terms of physical forces [6]. Starling's Law states that the net flow of fluid across a vessel wall is increased by hydrostatic pressure within the lumen of the vessel and decreased by oncotic pressure within the lumen. In diabetic patients, hydrostatic pressure may be increased because of systemic hypertension and retinal ischemia, increasing the likelihood of exudation. This problem is exacerbated because increased hydrostatic pressure may lead to dilatation and tortuosity of retinal arterioles, capillaries, and venules, which increases vessel wall tension and further disruption of the BRB according to LaPlace's Law [7]. Other factors may also contribute to this edema, such as osmotic stress leading to Muller cell swelling, such as that reported with retinal detachment [8].
The pathogenesis of DME is at this time poorly defined, but is believed to involve angiogenesis, inflammation, and oxidative stress [9]. Hyperglycemia is reported to lead to capillary endothelial damage and alterations in leukocyte function [10]. In addition, hyperglycemia has been reported to activate oxidative stress agents, such as advanced glycation endproducts and the protein kinase C (PKC) pathway [11]. Various inflammatory mediators appear to play a role in promoting DME, including vascular endothelial growth factor (VEGF) [12], placental growth factor (PlGF) [13], and hepatocyte growth factor (HGF) [14].
The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) reported that approximately 14% of patients with type 2 diabetes developed DME over a 10-year period [15]. More recently, the 10-year incidence of DME in a Spanish population of patients with type 1 diabetes was reported as approximately 11% [16]. Reported risk factors for diabetic retinopathy and DME include duration of diabetes, as well as the severity of hyperglycemia, hypertension, and hyperlipidemia [17].
Intensive control of systemic factors, including blood sugar, blood pressure, and serum lipids, has been reported to reduce complications of diabetic retinopathy in patients with type 1 [18] and type 2 [19] diabetes. Macular photocoagulation was demonstrated as a treatment for clinically significant macular edema (CSME) by the Early Treatment Diabetic Retinopathy Study (ETDRS) in 1985 [20]. Newer clinical trials using intravitreal pharmacotherapies have reported many favorable outcomes. The current paper will review the literature and various randomized clinical trials (RCTs) on emerging pharmacotherapies for the treatment of DME.
2. Ocular Agents
2.1. Corticosteroids
Corticosteroids may have multiple mechanisms of action in the treatment of DME. In addition to their anti-inflammatory properties, corticosteroids have been reported to reduce the activity of VEGF [21]. Intravitreal triamcinolone acetonide (IVTA) has been reported for the treatment of DME (Figure 1) (Table 1). Currently, there are at least four preparations reported in clinical studies: Kenalog-40 (Bristol-Myers Squibb, Princeton, NJ, USA); preservative-free triamcinolone acetonide from compounding pharmacies; Triesence (Alcon, Fort Worth, TX, US); and Trivaris (Allergan, Irvine, CA, USA).
Figure 1.
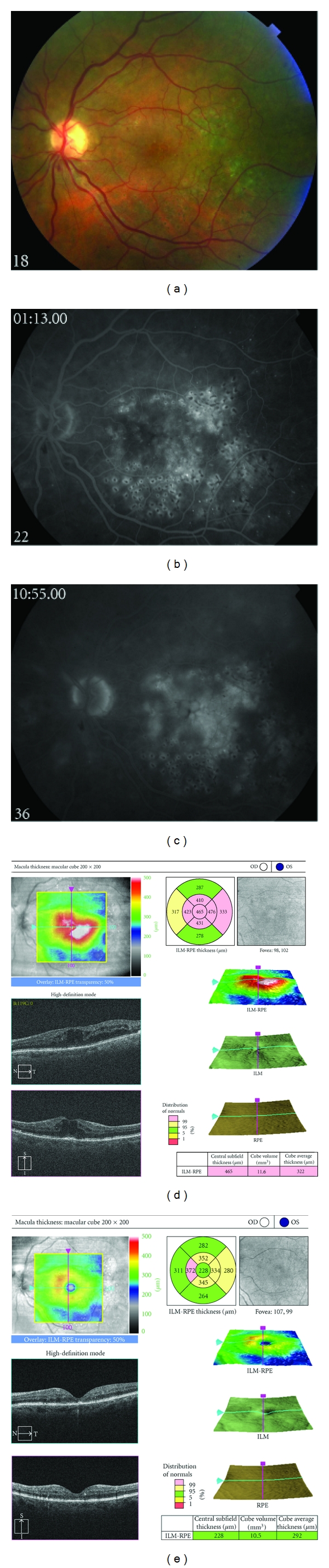
(a) Fundus photograph, left eye, of a patient with persistent diabetic macular edema following focal/grid photocoagulation. (b) Early phase fluorescein angiograph, left eye, demonstrating abnormal hyperfluorescence in the macula. (c) Late phase fluorescein angiograph, left eye, demonstrating profuse leakage consistent with angiographic macular edema. (d) Spectral domain optical coherence tomograph, left eye, demonstrating cystoid macular edema. (e) Following treatment with intravitreal triamcinolone acetonide, 4 mg in 0.1 mL, spectral domain optical coherence tomography demonstrates marked improvement in cystoid macular edema.
Table 1.
Selected clinical trials of corticosteroids in treatment of diabetic macular edema.
| Agent (no. patients) | Main outcomes | Reference |
|---|---|---|
| Intravitreal triamcinolone (693) | Less favorable outcomes versus photocoagulation at 24 and 36 months | [22, 23] |
| Peribulbar triamcinolone (109) | Less favorable outcomes versus intravitreal triamcinolone at 34 weeks | [28] |
| Fluocinolone acetonide implant (Retisert) (197) | Effective treatment of DME at 36 months, but high risks of cataract and glaucoma | [32] |
| Fluocinolone acetonide implant (Iluvien) (956) | Generally favorable results at 24 months | [34] |
| Dexamethasone drug delivery system (Ozurdex) (171) | Generally favorable results at 90 days | [36] |
The Diabetic Retinopathy Clinical Research Network (DRCR) protocol B compared two doses (1 and 4 mg) of IVTA versus photocoagulation for DME [22]. For most patients, photocoagulation produced more favorable outcomes than did IVTA at 24 months of followup. Similar results were reported at 3-year followup [23]. The most common complications of IVTA are cataract formation [24] and increased intraocular pressure (IOP) [25]. Pseudoendophthalmitis [26] and infectious endophthalmitis occur much less commonly. The rate of infectious endophthalmitis after IVTA is low in reported series. For example, in an analysis of two large RCTs (from the DRCR network and the Standard Care Versus Corticosteroid for Retinal Vein Occlusion (SCORE) trials), the rate of endophthalmitis after IVTA was 0.05% [27].
A triamcinolone-eluting intravitreal implant (I-vation, SurModics, Inc., MN, USA) for the treatment of DME was suspended in a phase 2b RCT after the publication of the DRCR network results showing a benefit of laser photocoagulation over IVTA in treatment of DME [22].
In order to reduce the risk of complications associated with IVTA, the use of peribulbar triamcinolone was investigated. In a single-center, prospective trial, peribulbar triamcinolone demonstrated lesser efficacy than did IVTA [28]. The DRCR reported that peribulbar triamcinolone did not significantly benefit patients with mild DME and visual acuity of 20/40 or better [29].
To reduce the need for repeated intravitreal injections, several extended-release corticosteroid delivery systems have been studied. A fluocinolone-acetonide- (FA-) eluting intravitreal implant (Retisert, Bausch and Lomb, NY, USA) has received FDA approval for the treatment of chronic, noninfectious posterior segment uveitis [30]. This is a nonbiodegradable device that releases 0.59 μg/day of FA into the vitreous cavity. It must be implanted in an operating room or similar setting. In an RCT, the effects of the device versus photocoagulation for DME were studied. At one year, DME was resolved by clinical examination and optical coherence tomography (OCT) in 57% of patients with the FA implant versus 20% of patients with photocoagulation. There were no statistically significant differences in final visual acuity between the two groups [31]. At 3 years, patients randomized to receive the FA implant had persistent treatment of macular edema, but 95% of phakic eyes developed significant cataract, and about one-third of eyes had IOP above 30 mm Hg [32].
A smaller fluocinolone acetonide-eluting device (Iluvien, Alimera Sciences, Alpharetta, GA, USA) may be administered through a 25-gauge device in a clinic setting. The Famous (Pharmacokinetic and Efficiency Study of Fluocinolone Acetonide Inserts in Patients with DME) study compared 0.2 versus 0.5 μg/day fluocinolone injection devices in patients with persistent DME despite at least one previous focal/grid laser therapy [33]. There was a mean improvement of 5 letters in visual acuity in both groups at 3-month followup. The number of patients in the trial was too small to determine whether there were clinically meaningful differences in results obtained from the two doses.
The Fluocinolone Acetonide for Macular Edema (FAME) study comprised 2 phase 3 RCTs assessing the efficacy and safety of 0.2 μg/day (low dose) and 0.5 μg/day (high dose) inserts in patients with DME with persistent edema despite at least one macular laser treatment [34]. The primary study endpoint was defined as improvement in visual acuity by 15 or more letters at 2 years. At 24 months, the primary endpoint was achieved in 28.7% and 28.6% of low- and high- dose insert groups compared with 16.2% in the sham group. Elevated intraocular pressure requiring incisional surgery occurred in 3.7%, 7.6%, and 0.5% of the low-dose, high-dose, and sham groups, respectively.
The dexamethasone drug delivery system (DDS) [Ozurdex, Allergan, Irvine, California] is a biodegradable, sustained-release device approved by the US FDA for the treatment of macular edema associated with retinal vein occlusion and noninfectious posterior segment uveitis. A phase 2 RCT in patients with persistent macular edema secondary to various etiologies, including DME, showed that the dexamethasone DDS produced improvements in visual acuity, macular thickness, and fluorescein leakage that were sustained for up to 6 months [35]. In an RCT, the safety and efficacy of the dexamethasone DDS in the treatment of DME was studied [36]. Patients with persistent macular edema (at least 90-day duration) were randomized to treatment with 700 μg or 350 μg of dexamethasone DDS or observation. At 3 months, visual acuity improved by 10 letters or more in 30% of eyes in the 700 μg group, 20% of eyes in the 350 μg group, and 12% of eyes in the observation group. A more recent study reported that the dexamethasone DDS improved visual acuity and macular edema in previously vitrectomized eyes with diffuse DME [37].
2.2. Vascular Endothelial Growth Factor Antagonists
VEGF appears to play an important role in the pathogenesis of diabetic retinopathy [38]. In animal models, injection of VEGF causes breakdown of the BRB [39], and elevated levels of VEGF cause macular edema [40]. An oral nonselective blocker of VEGF receptor was found to reduce DME, suggesting that VEGF antagonists may provide benefit in treatment of DME [41]. Four intravitreal anti-VEGF agents are currently available commercially, although none is FDA-approved for the treatment of DME (Table 2).
Table 2.
Selected clinical trials of VEGF antagonists in treatment of diabetic macular edema.
| Agent (no. patients) | Main outcomes | Reference |
|---|---|---|
| Pegaptanib (260) | More favorable outcomes versus sham at 2 years | [43] |
| Bevacizumab | ||
| DRCR phase II (121) | More favorable outcomes versus photocoagulation at 3 weeks | [45] |
| BOLT study (80) | More favorable outcomes versus photocoagulation at 1 year | [46] |
| Ranibizumab | ||
| READ-2 study (126) | More favorable outcomes versus photocoagulation at 2 years | [53] |
| DRCR protocol I (691) | Ranibizumab with photocoagulation more favorable than photocoagulation alone at 2 years | [54] |
| RESTORE study (345) | Ranibizumab with or without photocoagulation more favorable than photocoagulation alone at 1 year | [57] |
| RISE/RIDE studies (377) | More favorable outcomes versus sham at 2 years | [59] |
| RESOLVE study (151) | More favorable outcomes versus sham at 1 year | [60] |
| Aflibercept | ||
| DA VINCI study (219) | More favorable outcomes versus photocoagulation at 1 year | [66] |
2.2.1. Pegaptanib
Pegaptanib (Macugen, Eyetech Pharmaceuticals, Palm Beach Gardens, FL, USA) is a pegylated aptamer that targets the VEGF165 isoform. Pegaptanib is approved by the FDA for the treatment of neovascular age-related macular degeneration (AMD) and was the first anti-VEGF medication reported to have efficacy in the treatment of DME. The Macugen Diabetic Retinopathy Study Group conducted a phase 2 RCT of pegaptanib for fovea-involving DME [42]. After 36 weeks of followup, the pegaptanib-treated eyes had better visual acuity, more reduction in central retinal thickness, and less need for laser photocoagulation compared to the sham group. More recently, a phase 2/3 RCT reported that pegaptanib therapy was associated with improved visual outcomes in patients with DME for up to 2 years [43].
2.2.2. Bevacizumab
Bevacizumab (Avastin, Genentech, Inc., South San Francisco, CA, US) is a full-length recombinant humanized antibody against all isoforms of VEGF-A. Bevacizumab is approved by the FDA for the systemic treatment of metastatic colorectal cancer, metastatic breast cancer, and nonsmall cell lung cancer [44]. The agent is used commonly as an off-label intravitreal injection (Figure 2). The DRCR network conducted a randomized study of 121 eyes with DME over a 12-week period [45]. There were five treatment arms: focal photocoagulation, 2 consecutive 1.25 mg bevacizumab injections, 2 consecutive 2.5 mg bevacizumab injections, 1.25 mg bevacizumab followed by sham injection, and combination of photocoagulation with 2 consecutive 1.25 mg bevacizumab injections. The groups that received two bevacizumab injections without laser had a significant improvement in visual acuity over the laser-only group. There were no detectable differences between the 1.25 mg and 2.5 mg doses. The single injection group had no advantage over the laser-only group. The combination of laser and bevacizumab had comparable results to the laser-only group with a trend toward worse short-term vision than eyes that received two bevacizumab injections. The DRCR is currently planning an RCT to compare bevacizumab to ranibizumab in the treatment of DME.
Figure 2.

(a) Fundus photograph, right eye, of a patient with persistent diabetic macular edema following focal/grid photocoagulation. (b) Spectral domain optical coherence tomograph, right eye, demonstrates cystoid macular edema and subretinal fluid. (c) Following additional focal/grid photocoagulation and treatment with intravitreal bevacizumab, 1.25 mg in 0.1 mL, fundus photography demonstrates marked improvement in diabetic macular edema. (d) Follow-up spectral domain optical coherence tomography demonstrates marked improvement in intraretinal and subretinal fluid.
In the BOLT (Bevacizumab Or Laser Therapy in the Management of DME) study, repeated intravitreal bevacizumab injections were compared with modified ETDRS photocoagulation in patients with persistent DME. A total of 80 patients with center-involving DME and at least one prior photocoagulation without evidence of advanced macular ischemia were included. Patients were randomized to 2 arms: intravitreal bevacizumab (injections at baseline, 6- and 12-week followup with subsequent injections every 6 weeks based on OCT-guided retreatment protocol) or photocoagulation (at baseline with subsequent retreatment every 4 months if clinically indicated by ETDRS guidelines). At 12 months, bevacizumab had a greater treatment effect than did photocoagulation. The bevacizumab arm gained a median of 8 ETDRS letters, whereas the photocoagulation group lost a median of 0.5 ETDRS letters. Approximately 31% of patients in the bevacizumab arm versus 7.9% of patients in the laser arm gained ≥10 ETDRS letters (P = 0.01). The decrease in central macular thickness was significantly more in the bevacizumab group compared to the photocoagulation group [46]. There was no progression of macular ischemia in either treatment group [47].
2.2.3. Ranibizumab
Ranibizumab (Lucentis, Genentech, Inc. South San Francisco, CA, USA) is a recombinant humanized monoclonal antibody fragment that binds all isoforms of VEGF-A with high affinity. Ranibizumab is FDA-approved for the treatment of neovascular AMD and retinal vascular occlusion [48–51]. The Ranibizumab for Edema of the Macula in Diabetes (READ-2) study randomized 126 eyes with DME to 3 groups: ranibizumab only (injection at baseline, months 1, 3, and 5); photocoagulation (at baseline and at 3 months if needed); combined ranibizumab and photocoagulation (photocoagulation and ranibizumab at baseline, and ranibizumab at 3 months if needed) [52]. Patients randomized to ranibizumab only showed a significantly better visual outcome at 6 months compared with the other 2 groups. For patients with data available at 6 months, improvement of 3 lines or more in vision occurred in 22% of patients in the ranibizumab-only arm, none in the photocoagulation-only arm, and 8% in combined arm. At 24 months, the study reported that intravitreal ranibizumab provided persistent treatment benefits [53].
DRCR protocol I evaluated ranibizumab and IVTA in combination with photocoagulation by randomizing patients into four arms: ranibizumab with prompt (within one week) photocoagulation, IVTA with prompt photocoagulation, sham injection with prompt photocoagulation, and ranibizumab with photocoagulation deferred for at least 24 weeks [54]. The treatment protocol included a baseline treatment followed by intravitreal study medication or sham injection retreatments every 4 weeks through the 12-week visit. After the 16-week visit, retreatment was at the investigator's discretion according to web-based predetermined criteria. Ranibizumab with prompt or deferred photocoagulation resulted in more favorable visual acuity and central macular thickness outcomes compared with photocoagulation alone at 1 and 2 years of followup. In ranibizumab-treated eyes, the results were similar whether photocoagulation was given with the first injection or deferred for at least 24 weeks. IVTA combined with photocoagulation did not result in better visual outcomes compared with photocoagulation alone. In pseudophakic eyes, the IVTA with prompt photocoagulation group had similar visual outcomes to the 2 ranibizumab groups, suggesting that cataract formation may have affected the visual acuity outcomes in phakic eyes treated with IVTA. Two-year visual outcomes were similar to 1-year results and reinforced the conclusion that ranibizumab with prompt or deferred photocoagulation should be considered for patients with vision impairment of worse than 20/32 secondary to DME [55]. This study utilized a web-based algorithm to determine treatment decisions; in clinical practice, this may not be feasible, but the general approach may be emulated [56].
The RESTORE phase 3 study reported that ranibizumab monotherapy or combined with laser photocoagulation provided superior visual acuity gain over standard photocoagulation in the treatment of DME [57]. The one-year results showed that 37% of patients treated with ranibizumab 0.5 mg alone, and 43% of those treated with ranibizumab plus laser therapy, gained vision improvement of 10 letters or more compared to 16% of patients treated with laser alone. At one year, no difference was detected between the ranibizumab and ranibizumab plus laser arms.
A recent study showed that the addition of one IVTA injection or two ranibizumab injections to eyes receiving focal laser treatment for DME and panretinal photocoagulation is associated with significantly better visual acuity and decreased macular edema by 14 weeks [58]. However, these improvements were not maintained when study subjects were followed for 56 weeks for safety outcomes.
Two additional phase 3 RCTs (RISE and RIDE) were conducted to evaluate the efficacy, durability, and long-term safety of monthly ranibizumab injections in patients with center-involving DME. The primary efficacy outcome was the proportion of subjects who gained more than 15 letters in visual acuity compared with baseline at 24 months. Patients were randomized 1 : 1 : 1 to receive monthly injections of 0.3 mg ranibizumab, 0.5 mg ranibizumab, or sham. These studies were not designed to compare the two doses of ranibizumab, but each dose against the sham injection. At 24 months, RISE met its primary endpoint with statistically significant improvements in vision in ranibizumab-treated patients compared to sham injections [59].
The safety and efficacy of 2 concentrations of intravitreal ranibizumab in the treatment of DME were compared in the RESOLVE phase 2 trial [60]. Subjects were randomized to receive 3 monthly injections with either 0.3 or 0.5 mg ranibizumab or placebo. Treatment was then administered on an as-needed basis, depending on the response to initial treatment. If edema persisted, then the dose of ranibizumab was doubled after 1 month. Photocoagulation after 3 injections was given if needed. When the pooled data from the double-dose ranibizumab group (n = 77) were compared with the sham group (n = 32), there were statistically significant improvements in vision and central macular thickness.
In contrast to intravitreal corticosteroids, cataract progression associated with intravitreal VEGF antagonists has not been identified. Some patients do sustain IOP elevation following repeated injections of VEGF antagonists [61], but this effect does not appear to be as strong as that associated with intravitreal corticosteroids. In most published series, the rate of endophthalmitis following treatment with intravitreal anti-VEGF injections is about 0.03% per injection [62–64]. The incidence and severity of systemic and ocular adverse events that are associated with repeated intravitreal injections of two doses of ranibizumab (0.5 mg versus 2.0 mg) in subjects with DME are being investigated in READ-3 study.
2.2.4. Aflibercept
Aflibercept, or VEGF trap-eye, (Eylea, Regeneron, Tarrytown, NY, USA), is a recombinant fusion protein with activity against all VEGF-A isoforms and PlGF that is FDA-approved for the treatment of neovascular AMD and has been shown to have short-term efficacy in the treatment of DME [65]. The DA-VINCI study assessed the efficacy and safety of intravitreal aflibercept versus laser photocoagulation in the treatment of DME. Patients were randomized to one of the following treatment arms: 0.5 mg aflibercept every 4 weeks, 2 mg aflibercept every 4 weeks, 2 mg aflibercept every 8 weeks, 2 mg aflibercept as needed, or photocoagulation. At 24 weeks, the mean change in BCVA for aflibercept arms ranged from +8.5 to +11.4 letters compared to the mean change of +2.5 letters in the laser-treated eyes (P < 0.01). There was no statistical significant difference between the aflibercept arms. Anatomic effects (mean change in central retinal thickness) ranged from −127 μm to −195 μm in aflibercept arms compared to −68 μm in laser-treated eyes at 24 weeks (P < 0.01). At 52 weeks, the mean change in BCVA for aflibercept arms ranged from +9.7 to +13.1 letters compared to the mean change of −1.3 letters in the laser-treated eyes (P < 0.01) [66]. In this study population, intravitreal aflibercept produced significant improvements in visual acuity and retinal thickness as compared to laser photocoagulation at both 24 and 52 weeks. At this time, aflibercept is not approved by the US FDA for the treatment of DME.
2.3. Vitreolysis
The vitreous has been implicated as a cause of DME by several mechanical and physiological mechanisms, including macular traction and concentration of vasopermeable factors in the macular region [67]. A recent prospective trial by DRCR network evaluated visual and anatomical outcomes of pars plana vitrectomy (PPV) without concomitant cataract surgery for DME in eyes with moderate vision loss and vitreomacular traction. Retinal thickening was improved in most eyes, but visual acuity results were less consistent with improvement of ≥10 letters in 38%, and worsening by ≥10 letters in 22% at 6 months [68]. In a subsequent analysis, the DRCR reported that better visual outcomes were associated with worse baseline visual acuity and in eyes in which an epiretinal membrane was removed [69].
Enzymatic vitreolysis with or without PPV has been studied in the treatment of DME. Intravitreal hyaluronidase (Vitrase, ISTA Pharmaceuticals, Irvine, CA, USA) has shown evidence of safety and efficacy in reducing vitreous hemorrhage secondary to different etiologies, including proliferative diabetic retinopathy (PDR), although it has not received FDA approval for this indication [70, 71].
Induction of a posterior vitreous detachment (PVD) may be beneficial in the treatment of DME [72]. Enzymes that may have efficacy in creating a PVD include hyaluronidase, plasmin, chondroitinase, and dispase [73]. Autologous plasmin has been used by itself or as adjunct to PPV in the treatment of DME [74, 75]. Microplasmin is a recombinant human protein derived from the yeast Pichiapastoris. It is a truncated form of the human protein plasmin with intact protease activity. The Microplasmin Intravitreous Injection (MIVI) trial was a phase 2 RCT that evaluated the safety and efficacy of intravitreal microplasmin in facilitating the creation of a total PVD in patients scheduled for PPV [76]. The study showed that microplasmin injection at a dose of 125 μg led to a greater likelihood of induction of PVD than placebo. Patients receiving microplasmin were significantly more likely to have resolution of vitreomacular traction and not to require PPV.
2.4. Other Ocular Agents
Other ocular agents have been studied as treatments for DME (Table 3). Animal models have demonstrated an important role for inflammation in diabetic retinopathy [77]. In early stages of diabetic retinopathy, there is upregulation of cyclo-oxygenase-2 (COX-2) that leads to elevated prostaglandin production and increased expression of VEGF with increased risk of vascular leakage and retinal neovascularization [78]. High doses of aspirin and intermediate doses of COX-2 inhibitors (celecoxib) have shown to be beneficial in early stages of experimental diabetic retinopathy [79]. Periocular celecoxib-containing microparticles have shown to inhibit elevation of VEGF for as long as 60 days in animal models [80]. A recent multicenter clinical trial failed to show any visual function benefits with celecoxib treatment in DME, although, there was a suggestive effect of celecoxib in reducing fluorescein leakage [81].
Table 3.
Selected Other Ocular Agents in Treatment of Diabetic Macular Edema.
| Agent (# patients) | Main Outcomes | Reference |
|---|---|---|
| Celecoxib (86) | Unfavorable outcomes versus photocoagulation at 2 years | [81] |
| Nepafenac (1) | Some evidence of efficacy in case report | [83] |
| Etanercept (7) | Some evidence of efficacy in pilot study | [85] |
| Infliximab (4) | Some evidence of efficacy in pilot study | [87] |
| Mecamylamine (23) | Some evidence of efficacy in pilot study | [90] |
Nepafenac (Nevanac, Alcon, Ft. Worth, TX, USA), an FDA-approved topical nonsteroidal anti-inflammatory drug (NSAID), is a prodrug that is converted to amfenac in the anterior chamber [82]. In a pilot study, nepafenac has shown some efficacy in the treatment of DME [83]. The DRCR is currently beginning a phase 2 RCT studying the use of topical nepafenac to treat nonclinically significant DME.
Etanercept (Enbrel, Amgen, Inc. Thousand Oaks, CA, USA and Wyeth, Madison, NJ, USA), a recombinant fusion protein with activity against TNF-α, is FDA-approved for the treatment of psoriatic disease [84]. Intravitreal etanercept has shown some evidence of efficacy against refractory DME [85].
Infliximab (Remicade, Centocor, Horsham, PA, USA) is another TNF-α antagonist that is FDA-approved for the treatment of Crohn's disease [86]. A pilot study showed benefits from systemic infliximab in treatment of DME [87]. A pilot study of intravitreal infliximab is continuing.
Stimulation of nicotinic acetylcholine (nACh) receptors on vascular endothelial cells promotes angiogenesis and vascular permeability in animal models [88, 89]. A recent multicenter phase 1/2 clinical trial evaluated the safety and bioactivity of topical mecamylamine, an antagonist of nACh receptors, in patients with DME [90]. Mecamylamine drops were well tolerated. The study suggested that administration of topical mecamylamine may have heterogeneous effects in patients with DME. The heterogeneous response may be secondary to variable expression of nACh receptor subtypes on endothelial cells.
A pilot study has reported a short-term positive response to intravitreal erythropoietin in a group of patients with chronic DME unresponsive to other therapies [91].
3. Systemic Agents
Various systemic agents have been studied in the treatment of DME (Table 4). Activation of protein kinase C (PKC) may play an important role in the development and progression of diabetic retinopathy [92–98]. Ruboxistaurin (Arxxant, Eli Lilly and Company, Indianapolis, IN, USA) is a selective antagonist of PKC βI and PKC βII [99]. The PKC-Diabetic Retinopathy Study (PKC-DRS) reported that ruboxistaurin was associated with a reduced incidence of moderate visual loss (doubling of the visual angle) [100]. The PKC-DRS 2 reported that ruboxistaurin was associated with a reduced incidence of sustained moderate visual loss (for 6 months) [101]. The PKC-DME Study (PKC-DMES) reported some evidence that ruboxistaurin was associated with reduced progression of DME, although this was a secondary endpoint [102]. Ruboxistaurin has not received approval from the USA FDA.
Table 4.
Selected Systemic Agents in Treatment of Diabetic Macular Edema.
| Agent (# patients) | Main Outcomes | Reference |
|---|---|---|
| Ruboxistaurin (686) | Did not meet primary outcome measure at 30 months | [102] |
| Fenofibrate (9795) | Favorable outcomes versus placebo at average of 5 years | [104] |
| Rosiglitazone (30) | Some evidence of efficacy at 3 months, but also may worsen DME in some patients | [107] |
Fenofibrate is a fibric acid derivative with pleiotropic effects that is used as a lipid-modifying agent [103]. The fenofibrate intervention and event lowering in diabetes (FIELD) study, a large RCT, showed that treatment with fenofibrate reduces the need for laser treatment in patients with PDR and DME [104].
Rosiglitazone (Avandia, GlaxoSmith Klein, Research Triangle Park, NC, US) is a peroxisome proliferator-activated γ ligand that is used in the treatment of type 2 diabetes [105]. Treatment with rosiglitazone has been shown to reduce the rate of progression to PDR [106], however, in some patients, it may be associated with increased risk of DME [107].
4. Summary Statement
For decades, standard treatments for DME have included tighter control of systemic metabolic factors, as well as photocoagulation. However, some patients continue to lose vision despite these therapies, which has led to the investigation of various pharmacotherapies for DME. At this time, both intravitreal corticosteroids and intravitreal anti-VEGF agents are widely used in clinical settings. The role of combination therapies (both various medications with each other as well as medications with photocoagulation) is yet to be determined. As we continue to collect data from current and future RCTs, management strategies for DME will continue to evolve.
Acknowledgments
This work was partially supported by NIH Center Grant P30-EY014801 and by an unrestricted grant to the University of Miami from Research to Prevent Blindness, NY, NY, USA. S. G. Schwartz is a consultant for Alimera Sciences and Bausch + Lomb, and holds intellectual property licensed to IC Labs. H. W. Flynn, Jr. is a consultant for Alcon Laboratories, Allergan, Pfizer, and Santen.
References
- 1.Klein R, Knudtson MD, Lee KE, Gangnon R, Klein BEK. The Wisconsin Epidemiologic Study of diabetic retinopathy XXIII: the twenty-five-year incidence of macular edema in persons with type 1 diabetes. Ophthalmology. 2009;116(3):497–503. doi: 10.1016/j.ophtha.2008.10.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ciulla TA, Amador AG, Zinman B. Diabetic retinopathy and diabetic macular edema: pathophysiology, screening, and novel therapies. Diabetes Care. 2003;26(9):2653–2664. doi: 10.2337/diacare.26.9.2653. [DOI] [PubMed] [Google Scholar]
- 3.Knudsen ST, Bek T, Poulsen PL, Hove MN, Rehling M, Mogensen CE. Macular edema reflects generalized vascular hyperpermeability in type 2 diabetic patients with retinopathy. Diabetes Care. 2002;25(12):2328–2334. doi: 10.2337/diacare.25.12.2328. [DOI] [PubMed] [Google Scholar]
- 4.Rotsos TG, Moschos MM. Cystoid macular edema. Journal of Clinical Ophthalmology. 2008;2:919–930. doi: 10.2147/opth.s4033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Xu HZ, Le YZ. Significance of outer blood-retina barrier breakdown in diabetes and ischemia. Investigative Ophthalmology & Visual Science. 2011;52:2160–2164. doi: 10.1167/iovs.10-6518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gardner TW, Antonetti DA, Barber AJ, LaNoue KF, Levison SW. Diabetic retinopathy: more than meets the eye. Survey of Ophthalmology. 2002;47(supplement 2):S253–S262. doi: 10.1016/s0039-6257(02)00387-9. [DOI] [PubMed] [Google Scholar]
- 7.Kristinsson JK, Gottfredsdóttir MS, Stefánsson E. Retinal vessel dilatation and elongation precedes diabetic macular oedema. British Journal of Ophthalmology. 1997;81(4):274–278. doi: 10.1136/bjo.81.4.274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wurm A, Pannicke T, Iandiev I, et al. Changes in membrane conductance play a pathogenic role in osmotic glial cell swelling in detached retinas. American Journal of Pathology. 2006;169(6):1990–1998. doi: 10.2353/ajpath.2006.060628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ehrlich R, Harris A, Ciulla TA, Kheradiya N, Winston DM, Wirostko B. Diabetic macular oedema: physical, physiological and molecular factors contribute to this pathological process. Acta Ophthalmologica. 2010;88(3):279–291. doi: 10.1111/j.1755-3768.2008.01501.x. [DOI] [PubMed] [Google Scholar]
- 10.Morigi M, Angioletti S, Imberti B, et al. Leukocyte-endothelial interaction is augmented by high glucose concentrations and hyperglycemia in a NF-kB-dependent fashion. Journal of Clinical Investigation. 1998;101(9):1905–1915. doi: 10.1172/JCI656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005;54(6):1615–1625. doi: 10.2337/diabetes.54.6.1615. [DOI] [PubMed] [Google Scholar]
- 12.Shams N, Ianchulev T. Role of vascular endothelial growth factor in ocular angiogenesis. Ophthalmology Clinics of North America. 2006;19(3):335–344. doi: 10.1016/j.ohc.2006.05.005. [DOI] [PubMed] [Google Scholar]
- 13.Miyamoto N, de Kozak Y, Jeanny JC, et al. Placental growth factor-1 and epithelial haemato-retinal barrier breakdown: potential implication in the pathogenesis of diabetic retinopathy. Diabetologia. 2007;50(2):461–470. doi: 10.1007/s00125-006-0539-2. [DOI] [PubMed] [Google Scholar]
- 14.Cai W, Rook SL, Jiang ZY, Takahara N, Aiello LP. Mechanisms of hepatocyte growth factor-induced retinal endothelial cell migration and growth. Investigative Ophthalmology and Visual Science. 2000;41(7):1885–1893. [PubMed] [Google Scholar]
- 15.Klein R, Klein BEK, Moss SE, Cruickshanks KJ. The Wisconsin epidemiologic study of diabetic retinopathy XV: the long term incidence of macular edema. Ophthalmology. 1995;102(1):7–16. doi: 10.1016/s0161-6420(95)31052-4. [DOI] [PubMed] [Google Scholar]
- 16.Romero-Aroca P, Baget-Bernaldiz M, Fernandez-Ballart J, et al. Ten-year incidence of diabetic retinopathy and macular edema. Risk factors in a sample of people with type 1 diabetes. Diabetes Research and Clinical Practice. 2011;94(1):126–132. doi: 10.1016/j.diabres.2011.07.004. [DOI] [PubMed] [Google Scholar]
- 17.Rodriguez-Fontal M, Kerrison JB, Alfaro DV, Jablon EP. Metabolic control and diabetic retinopathy. Current Diabetes Reviews. 2009;5(1):3–7. doi: 10.2174/157339909787314176. [DOI] [PubMed] [Google Scholar]
- 18.Diabetes Control and Complication Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The New England Journal of Medicine. 1993;329:977–986. doi: 10.1056/NEJM199309303291401. [DOI] [PubMed] [Google Scholar]
- 19.UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. UKPDS 33. Lancet. 1998;352:837–853. [PubMed] [Google Scholar]
- 20.Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study report number 1. Archives of Ophthalmology. 1985;103:1796–1806. [PubMed] [Google Scholar]
- 21.Nauck M, Roth M, Tamm M, et al. Induction of vascular endothelial growth factor by platelet-activating factor and platelet-derived growth factor is downregulated by corticosteroids. American Journal of Respiratory Cell and Molecular Biology. 1997;16(4):398–406. doi: 10.1165/ajrcmb.16.4.9115750. [DOI] [PubMed] [Google Scholar]
- 22.Diabetic Retinopathy Clinical Research Network. A randomized trial comparing intravitreal triamcinolone acetonide and focal/grid photocoagulation for diabetic macular edema. Ophthalmology. 2008;115:1447–1449. doi: 10.1016/j.ophtha.2008.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Beck RW, Edwards AR, Aiello LP, et al. Three-year follow-up of a randomized trial comparing focal/grid photocoagulation and intravitreal triamcinolone for diabetic macular edema. Archives of Ophthalmology. 2009;127(3):245–251. doi: 10.1001/archophthalmol.2008.610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chu YK, Chung EJ, Kwon OW, Lee JH, Koh HJ. Objective evaluation of cataract progression associated with a high dose intravitreal triamcinolone injection. Eye. 2008;22(7):895–899. doi: 10.1038/sj.eye.6702802. [DOI] [PubMed] [Google Scholar]
- 25.Smithen LM, Ober MD, Maranan L, Spaide RF. Intravitreal triamcinolone acetonide and intraocular pressure. American Journal of Ophthalmology. 2004;138(5):740–743. doi: 10.1016/j.ajo.2004.06.067. [DOI] [PubMed] [Google Scholar]
- 26.Moshfeghi DM, Kaiser PK, Bakri SJ, et al. Presumed sterile endophthalmitis following intravitreal triamcinolone acetonide injection. Ophthalmic Surgery Lasers and Imaging. 2005;36(1):24–29. [PubMed] [Google Scholar]
- 27.Bhavsar AR, Ip MS, Glassman AR. The risk of endophthalmitis following intravitreal triamcinolone injection in the DRCRnet and SCORE clinical trials. American Journal of Ophthalmology. 2007;144(3):454–456. doi: 10.1016/j.ajo.2007.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bonini-Filho MA, Jorge R, Barbosa JC, Calucci D, Cardillo JA, Costa RA. Intravitreal injection versus sub-tenon’s infusion of triamcinolone acetonide for refractory diabetic macular edema: a randomized clinical trial. Investigative Ophthalmology and Visual Science. 2005;46(10):3845–3849. doi: 10.1167/iovs.05-0297. [DOI] [PubMed] [Google Scholar]
- 29.Chew E, Trauber S. Diabetic Retinopathy Clinical Research Network, triamcinolone acetonide with and without focal photocoagulation for mild diabetic macular edema: a pilot study. Ophthalmology. 2007;114:1190–1196. doi: 10.1016/j.ophtha.2007.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jaffe GJ, Martin D, Callanan D, Pearson PA, Levy B, Comstock T. Fluocinolone acetonide implant (Retisert) for noninfectious posterior uveitis. Thirty-four-week results of a multicenter randomized clinical study. Ophthalmology. 2006;113(6):1020–1027. doi: 10.1016/j.ophtha.2006.02.021. [DOI] [PubMed] [Google Scholar]
- 31.Fluocinolone acetonide ophthalmic- Bausch & Lomb: fluocinolone acetonide envision TD implant. Drugs RD. 2005;6(2):116–119. doi: 10.2165/00126839-200506020-00007. [DOI] [PubMed] [Google Scholar]
- 32.Montero JA, Ruiz-Moreno JM. Intravitreal inserts of steroids to treat diabetic macular edema. Current Diabetes Reviews. 2009;5(1):26–32. doi: 10.2174/157339909787314211. [DOI] [PubMed] [Google Scholar]
- 33.Campochiaro PA, Hafiz G, Shah SM, et al. Sustained ocular delivery of fluocinolone acetonide by an intravitreal insert. Ophthalmology. 2010;117(7):1393–1399. doi: 10.1016/j.ophtha.2009.11.024. [DOI] [PubMed] [Google Scholar]
- 34.Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4):626–635. doi: 10.1016/j.ophtha.2010.12.028. [DOI] [PubMed] [Google Scholar]
- 35.Kuppermann BD, Blumenkranz MS, Haller JA, et al. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Archives of Ophthalmology. 2007;125(3):309–317. doi: 10.1001/archopht.125.3.309. [DOI] [PubMed] [Google Scholar]
- 36.Haller JA, Kuppermann BD, Blumenkranz MS, et al. Randomized controlled trial of an intravitreous dexamethasone drug delivery system in patients with diabetic macular edema. Archives of Ophthalmology. 2010;128(3):289–296. doi: 10.1001/archophthalmol.2010.21. [DOI] [PubMed] [Google Scholar]
- 37.Boyer DS, Faber D, Gupta S, et al. Dexamethasone intravitreal implant for treatment of diabetic macular edema in vitrectomized patients. Retina. 2011;31(5):915–923. doi: 10.1097/IAE.0b013e318206d18c. [DOI] [PubMed] [Google Scholar]
- 38.Vinores SA, Youssri AL, Luna JD, et al. Upregulation of vascular endothelial growth factor in ischemic and non-ischemic human and experimental retinal disease. Histology and Histopathology. 1997;12(1):99–109. [PubMed] [Google Scholar]
- 39.Derevjanik NL, Vinores SA, Xiao WH, et al. Quantitative assessment of the integrity of the blood-retinal barrier in mice. Investigative Ophthalmology and Visual Science. 2002;43(7):2462–2467. [PubMed] [Google Scholar]
- 40.Ozaki H, Hayashi H, Vinores SA, Moromizato Y, Campochiaro PA, Oshima K. Intravitreal sustained release of VEGF causes retinal neovascularization in rabbits and breakdown of the blood-retinal barrier in rabbits and primates. Experimental Eye Research. 1997;64(4):505–517. doi: 10.1006/exer.1996.0239. [DOI] [PubMed] [Google Scholar]
- 41.Campochiaro PA. Reduction of diabetic macular edema by oral administration of the kinase inhibitor PKC412. Investigative Ophthalmology and Visual Science. 2004;45(3):922–931. doi: 10.1167/iovs.03-0955. [DOI] [PubMed] [Google Scholar]
- 42.Cunningham ET, Jr., Adamis AP, Altaweel M, et al. A phase II randomized double-masked trial of pegaptanib, an anti-vascular endothelial growth factor aptamer, for diabetic macular edema. Ophthalmology. 2005;112(10):1747–1757. doi: 10.1016/j.ophtha.2005.06.007. [DOI] [PubMed] [Google Scholar]
- 43.Sultan MB, Zhou D, Loftus J, Dombi T, Ice KS. A phase 2/3, multicenter, randomized, double-masked, 2-year trial of pegaptanib sodium for the treatment of diabetic macular edema. Ophthalmology. 2011;118(6):1107–1118. doi: 10.1016/j.ophtha.2011.02.045. [DOI] [PubMed] [Google Scholar]
- 44.Yang JC, Haworth L, Sherry RM, et al. A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. New England Journal of Medicine. 2003;349(5):427–434. doi: 10.1056/NEJMoa021491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Diabetic Retinopathy Clinical Research Network. A phase II randomized clinical trial of intravitreal bevacizumab for diabetic macular edema. Ophthalmology. 2007;114:1860–1867. doi: 10.1016/j.ophtha.2007.05.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Michaelides M, Kaines A, Hamilton RD, et al. A prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study). 12-month data: report 2. Ophthalmology. 2010;117(6):1078–1086. doi: 10.1016/j.ophtha.2010.03.045. [DOI] [PubMed] [Google Scholar]
- 47.Michaelides M, Fraser-Bell S, Hamilton R, et al. Macular perfusion determined by fundus fluorescein angiography at the 4-month time point in a prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (bolt study): report 1. Retina. 2010;30(5):781–786. doi: 10.1097/iae.0b013e3181d2f145. [DOI] [PubMed] [Google Scholar]
- 48.Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. New England Journal of Medicine. 2006;355(14):1419–1431. doi: 10.1056/NEJMoa054481. [DOI] [PubMed] [Google Scholar]
- 49.Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. New England Journal of Medicine. 2006;355(14):1432–1444. doi: 10.1056/NEJMoa062655. [DOI] [PubMed] [Google Scholar]
- 50.Campochiaro PA, Heier JS, Feiner L, et al. Ranibizumab for macular edema following branch retinal vein occlusion. Six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1102–1112. doi: 10.1016/j.ophtha.2010.02.021. [DOI] [PubMed] [Google Scholar]
- 51.Brown DM, Campochiaro PA, Singh RP, et al. Ranibizumab for macular edema following central retinal vein occlusion. Six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1124–1133. doi: 10.1016/j.ophtha.2010.02.022. [DOI] [PubMed] [Google Scholar]
- 52.Nguyen QD, Shah SM, Heier JS, et al. Primary end point (six months) results of the ranibizumab for edema of the mAcula in diabetes (READ-2) study. Ophthalmology. 2009;116(11):2175–2181. doi: 10.1016/j.ophtha.2009.04.023. [DOI] [PubMed] [Google Scholar]
- 53.Nguyen QD, Shah SM, Khwaja AA, et al. Two-year outcomes of the ranibizumab for edema of the mAcula in diabetes (READ-2) study. Ophthalmology. 2010;117(11):2146–2151. doi: 10.1016/j.ophtha.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 54.Diabetic Retinopathy Clinical Research Network, Elman MJ, Aiello LP, et al. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2010;117(6):1064–1077. doi: 10.1016/j.ophtha.2010.02.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Elman MJ, Bressler NM, Qin H, et al. Expanded 2-year follow-up of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2011;118(4):609–614. doi: 10.1016/j.ophtha.2010.12.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Aiello LP, Beck RW, Bressler NM, et al. Rationale for the diabetic retinopathy clinical research network treatment protocol for center-involved diabetic macular edema. Ophthalmology. 2011;118(12):e5–e14. doi: 10.1016/j.ophtha.2011.09.058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;118(4):615–625. doi: 10.1016/j.ophtha.2011.01.031. [DOI] [PubMed] [Google Scholar]
- 58.Googe J, Brucker AJ, Bressler NM, et al. Randomized trial evaluating short-term effects of intravitreal ranibizumab or triamcinolone acetonide on macular edema after focal/grid laser for diabetic macular edema in eyes also receiving panretinal photocoagulation. Retina. 2011;31(6):1009–1027. doi: 10.1097/IAE.0b013e318217d739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Brown DM, Nguyen QD, Rubio RG, et al. Ranibizumab for diabetic macular edema (DME): 24-month efficacy and safety results of RISE—a phase 3 randomized controlled trial. ARVO abstract 6647, 2011.
- 60.Massin P, Bandello F, Garweg JG, et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE study): a 12-month, randomized, controlled, double-masked, multicenter phase II study. Diabetes Care. 2010;33(11):2399–2405. doi: 10.2337/dc10-0493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Good TJ, Kimura AE, Mandava N, Kahook MY. Sustained elevation of intraocular pressure after intravitreal injections of anti-VEGF agents. British Journal of Ophthalmology. 2011;95(8):1111–1114. doi: 10.1136/bjo.2010.180729. [DOI] [PubMed] [Google Scholar]
- 62.Schwartz SG, Flynn HW, Jr., Scott IU. Endophthalmitis after intravitreal injections. Expert Opinion on Pharmacotherapy. 2009;10(13):2119–2126. doi: 10.1517/14656560903081752. [DOI] [PubMed] [Google Scholar]
- 63.Moshfeghi AA, Rosenfeld PJ, Flynn Jr. HW, et al. Endophthalmitis after intravitreal anti-vascular endothelial growth factor antagonists: a six-year experience at a university referral center. Retina. 2011;31(4):662–668. doi: 10.1097/IAE.0b013e31821067c4. [DOI] [PubMed] [Google Scholar]
- 64.McCannel CA. Meta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents: causative organisms and possible prevention strategies. Retina. 2011;31(4):654–661. doi: 10.1097/IAE.0b013e31820a67e4. [DOI] [PubMed] [Google Scholar]
- 65.Do DV, Nguyen QD, Shah SM, et al. An exploratory study of the safety, tolerability and bioactivity of a single intravitreal injection of vascular endothelial growth factor Trap-Eye in patients with diabetic macular oedema. British Journal of Ophthalmology. 2009;93(2):144–149. doi: 10.1136/bjo.2008.138271. [DOI] [PubMed] [Google Scholar]
- 66.Do DV, Schmidt-Erfurth U, Gonzalez VH, et al. The da VINCI study: phase 2 primary results of VEGF trap-eye in patients with diabetic macular edema. Ophthalmology. 2011;118(9):1819–1826. doi: 10.1016/j.ophtha.2011.02.018. [DOI] [PubMed] [Google Scholar]
- 67.Harbour JW, Smiddy WE, Flynn HW, Jr., Rubsamen PE. Vitrectomy for diabetic macular edema associated with a thickened and taut posterior hyaloid membrane. American Journal of Ophthalmology. 1996;121(4):405–413. doi: 10.1016/s0002-9394(14)70437-4. [DOI] [PubMed] [Google Scholar]
- 68.Diabetic Retinopathy Clinical Research Network Writing Committee, Haller JA, Qin H. Vitrectomy outcomes in eyes with diabetic macular edema and vitreomacular traction. Ophthalmology. 2010;117:1087–1093. doi: 10.1016/j.ophtha.2009.10.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Flaxel CJ, Edwards AR, Aiello LP, et al. Factors associated with visual acuity outcomes after vitrectomy for diabetic macular edema: diabetic retinopathy clinical research network. Retina. 2010;30(9):1488–1495. doi: 10.1097/IAE.0b013e3181e7974f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Kuppermann BD, Thomas EL, De Smet MD, Grillone LR. Pooled efficacy results from two multinational randomized controlled clinical trials of a single intravitreous injection of highly purified ovine hyaluronidase (Vitrase) for the management of vitreous hemorrhage. American Journal of Ophthalmology. 2005;140(4):573–584. doi: 10.1016/j.ajo.2005.04.018. [DOI] [PubMed] [Google Scholar]
- 71.Kuppermann BD, Thomas EL, De Smet MD, Grillone LR. Safety results of two phase III trials of an intravitreous injection of highly purified ovine hyaluronidase (Vitrase) for the management of vitreous hemorrhage. American Journal of Ophthalmology. 2005;140(4):585–597. doi: 10.1016/j.ajo.2005.06.022. [DOI] [PubMed] [Google Scholar]
- 72.Lopez-Lopez F, Rodriguez-Blanco M, Gómez-Ulla F, Marticonera J. Enzymatic vitreolysis. Current Diabetes Reviews. 2009;5(1):57–62. doi: 10.2174/157339909787314220. [DOI] [PubMed] [Google Scholar]
- 73.Gandorfer A. Enzymatic vitreous disruption. Eye. 2008;22(10):1273–1277. doi: 10.1038/eye.2008.29. [DOI] [PubMed] [Google Scholar]
- 74.Diaz-Llopis M, Udaondo P, Arevalo F, et al. Intravitreal plasmin without associated vitrectomy as a treatment for refractory diabetic macular edema. Journal of Ocular Pharmacology and Therapeutics. 2009;25(4):379–384. doi: 10.1089/jop.2008.0118. [DOI] [PubMed] [Google Scholar]
- 75.Azzolini C, D’Angelo A, Maestranzi G, et al. Intrasurgical plasmin enzyme in diabetic macular edema. American Journal of Ophthalmology. 2004;138(4):560–566. doi: 10.1016/j.ajo.2004.05.024. [DOI] [PubMed] [Google Scholar]
- 76.Benz MS, Packo KH, Gonzalez V, et al. A placebo-controlled trial of microplasmin intravitreous injection to facilitate posterior vitreous detachment before vitrectomy. Ophthalmology. 2010;117(4):791–797. doi: 10.1016/j.ophtha.2009.11.005. [DOI] [PubMed] [Google Scholar]
- 77.Johnson EIM, Dunlop ME, Larkins RG. Increased vasodilatory prostaglandin production in the diabetic rat retinal vasculature. Current Eye Research. 1999;18(2):79–82. doi: 10.1076/ceyr.18.2.79.5386. [DOI] [PubMed] [Google Scholar]
- 78.Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. New England Journal of Medicine. 1994;331(22):1480–1487. doi: 10.1056/NEJM199412013312203. [DOI] [PubMed] [Google Scholar]
- 79.Joussen AM, Poulaki V, Mitsiades N, et al. Nonsteroidal anti-inflammatory drugs prevent early diabetic retinopathy via TNF-alpha suppression. The FASEB Journal. 2002;16(3):438–440. doi: 10.1096/fj.01-0707fje. [DOI] [PubMed] [Google Scholar]
- 80.Amrite AC, Ayalasomayajula SP, Cheruvu NPS, Kompella UB. Single periocular injection of celecoxib-PLGA microparticles inhibits diabetes-induced elevations in retinal PGE2, VEGF, and vascular leakage. Investigative Ophthalmology and Visual Science. 2006;47(3):1149–1160. doi: 10.1167/iovs.05-0531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Chew EY, Kim J, Coleman HR, et al. Preliminary assessment of celecoxib and microdiode pulse laser treatment of diabetic macular edema. Retina. 2010;30(3):459–467. doi: 10.1097/IAE.0b013e3181bcf1a0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Gamache DA, Graff G, Brady MT, Spellman JM, Yanni JM. Nepafenac, a unique nonsteroidal prodrug with potential utility in the treatment of trauma-induced ocular inflammation: I. Assessment of anti- inflammatory efficacy. Inflammation. 2000;24(4):357–370. doi: 10.1023/a:1007049015148. [DOI] [PubMed] [Google Scholar]
- 83.Hariprasad SM, Callanan D, Gainey S, He YG, Warren K. Cystoid and diabetic macular edema treated with nepafenac 0.1% Journal of Ocular Pharmacology and Therapeutics. 2007;23(6):585–590. doi: 10.1089/jop.2007.0062. [DOI] [PubMed] [Google Scholar]
- 84.Ducharme E, Weinberg JM. Etanercept. Expert Opinion on Biological Therapy. 2008;8(4):491–502. doi: 10.1517/14712598.8.4.491. [DOI] [PubMed] [Google Scholar]
- 85.Tsilimbaris MK, Panagiotoglou TD, Charisis SK, Anastasakis A, Krikonis TS, Christodoulakis E. The use of intravitreal etanercept in diabetic macular oedema. Seminars in Ophthalmology. 2007;22(2):75–79. doi: 10.1080/08820530701418243. [DOI] [PubMed] [Google Scholar]
- 86.Targan SR, Hanauer SB, van Deventer SJH, et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor α for Crohn’s Disease. New England Journal of Medicine. 1997;337(15):1029–1035. doi: 10.1056/NEJM199710093371502. [DOI] [PubMed] [Google Scholar]
- 87.Sfikakis PP, Markomichelakis N, Theodossiadis GP, Grigoropoulos V, Katsilambros N, Theodossiadis PG. Regression of sight-threatening macular edema in type 2 diabetes following treatment with the anti-tumor necrosis factor monoclonal antibody infliximab. Diabetes Care. 2005;28(2):445–447. doi: 10.2337/diacare.28.2.445. [DOI] [PubMed] [Google Scholar]
- 88.Villablanca AC. Nicotine stimulates DNA synthesis and proliferation in vascular endothelial cells in vitro. Journal of Applied Physiology. 1998;84(6):2089–2098. doi: 10.1152/jappl.1998.84.6.2089. [DOI] [PubMed] [Google Scholar]
- 89.Heeschen C, Jang JJ, Weis M, et al. Nicotine stimulates angiogenesis and promotes tumor growth and atherosclerosis. Nature Medicine. 2001;7(7):833–839. doi: 10.1038/89961. [DOI] [PubMed] [Google Scholar]
- 90.Campochiaro PA, Shah SM, Hafiz G, et al. Topical mecamylamine for diabetic macular edema. American Journal of Ophthalmology. 2010;149(5):839–851. doi: 10.1016/j.ajo.2009.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Li W, Sinclair SH, Xu GT. Effects of intravitreal erythropoietin therapy for patients with chronic and progressive diabetic macular edema. Ophthalmic Surgery Lasers and Imaging. 2010;41(1):18–25. doi: 10.3928/15428877-20091230-03. [DOI] [PubMed] [Google Scholar]
- 92.Park JY, Takahara N, Gabriele A, et al. Induction of endothelin-1 expression by glucose an effect of protein kinase C activation. Diabetes. 2000;49(7):1239–1248. doi: 10.2337/diabetes.49.7.1239. [DOI] [PubMed] [Google Scholar]
- 93.Park CW, Kim JH, Lee JW, et al. High glucose-induced intercellular adhesion molecule-1 (ICAM-1) expression through an osmotic effect in rat mesangial cells is PKC-NF-χB-dependent. Diabetologia. 2000;43(12):1544–1553. doi: 10.1007/s001250051567. [DOI] [PubMed] [Google Scholar]
- 94.Xia P, Inoguchi T, Kern TS, Engerman RL, Oates PJ, King GL. Characterization of the mechanism for the chronic activation of diacylglycerol-protein kinase C pathway in diabetes and hypergalactosemia. Diabetes. 1994;43(9):1122–1129. doi: 10.2337/diab.43.9.1122. [DOI] [PubMed] [Google Scholar]
- 95.Aiello LP. The potential role of PKC β in diabetic retinopathy and macular edema. Survey of Ophthalmology. 2002;47(supplement 2):S263–S269. doi: 10.1016/s0039-6257(02)00391-0. [DOI] [PubMed] [Google Scholar]
- 96.Donnelly R, Idris I, Forrester JV. Protein kinase C inhibition and diabetic retinopathy: a shot in the dark at translational research. British Journal of Ophthalmology. 2004;88(1):145–151. doi: 10.1136/bjo.88.1.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Nishizuka Y. The molecular heterogeneity of protein kinase C and its implications for cellular regulation. Nature. 1988;334(6184):661–665. doi: 10.1038/334661a0. [DOI] [PubMed] [Google Scholar]
- 98.Aiello LP, Bursell SE, Clermont A, et al. Vascular endothelial growth factor-induced retinal permeability is mediated by protein kinase C in vivo and suppressed by an orally effective β-isoform-selective inhibitor. Diabetes. 1997;46(9):1473–1480. doi: 10.2337/diab.46.9.1473. [DOI] [PubMed] [Google Scholar]
- 99.Jirousek MR, Gillig JR, Gonzalez CM, et al. (S)-13-[(dimethylamino)methyl]-10,11,14,15-tetrahydro-4,9:16,21- dimetheno-1H,13H-dibenzo[e,k]pyrrolo[3,4-h][1,4,13]oxadiazacyclohexadecene- 1,3(2H)-dione (LY333531) and related analogues: isozyme selective inhibitors of protein kinase Cβ . Journal of Medicinal Chemistry. 1996;39(14):2664–2671. doi: 10.1021/jm950588y. [DOI] [PubMed] [Google Scholar]
- 100.The PKC-DRS Study Group. The effect of ruboxistaurin on visual loss in patients with moderately severe to very severe nonproliferative diabetic retinopathy: initial results of the protein kinase C β inhibitor diabetic retinopathy study (PKC-DRS) multicenter randomized clinical trial. Diabetes. 2005;54(7):2188–2197. doi: 10.2337/diabetes.54.7.2188. [DOI] [PubMed] [Google Scholar]
- 101.PKC-DRS2 Group, Aiello LP, Davis MD, et al. Effect of ruboxistaurin on visual loss in patients with diabetic retinopathy. Ophthalmology. 2006;113(12):2221–2230. doi: 10.1016/j.ophtha.2006.07.032. [DOI] [PubMed] [Google Scholar]
- 102.The PKC-DMES Study Group. Effect of ruboxistaurin in patients with diabetic macular edema: thirty-month results of the randomized PKC-DMES clinical trial. Archives of Ophthalmology. 2007;125(3):318–324. doi: 10.1001/archopht.125.3.318. [DOI] [PubMed] [Google Scholar]
- 103.Keating GM, Croom KF. Fenofibrate: a review of its use in primary dyslipidaemia, the metabolic syndrome and type 2 diabetes mellitus. Drugs. 2007;67(1):121–153. doi: 10.2165/00003495-200767010-00013. [DOI] [PubMed] [Google Scholar]
- 104.Keech A, Mitchell P, Summanen P, et al. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): a randomised controlled trial. Lancet. 2007;370(9600):1687–1697. doi: 10.1016/S0140-6736(07)61607-9. [DOI] [PubMed] [Google Scholar]
- 105.Nolan JJ, Jones NP, Patwardhan R, Deacon LF. Rosiglitazone taken once daily provides effective glycaemic control in patients with Type 2 diabetes mellitus. Diabetic Medicine. 2000;17(4):287–294. doi: 10.1046/j.1464-5491.2000.00269.x. [DOI] [PubMed] [Google Scholar]
- 106.Shen LQ, Child A, Weber GM, Folkman J, Aiello LP. Rosiglitazone and delayed onset of proliferative diabetic retinopathy. Archives of Ophthalmology. 2008;126(6):793–799. doi: 10.1001/archopht.126.6.793. [DOI] [PubMed] [Google Scholar]
- 107.Ryan Jr. EH, Han DP, Ramsay RC, et al. Diabetic macular edema associated with glitazone use. Retina. 2006;26(5):562–570. doi: 10.1097/00006982-200605000-00011. [DOI] [PubMed] [Google Scholar]