

Sir,
Supraclavicular approach to the subclavian vein is an underused and less commonly employed technique for unknown reasons than the traditional infraclavicular approach. There are definitive advantages of the former technique, which include: A well-defined insertion landmark (the clavisternomastoid angle); a shorter distance from skin to vein; a larger target area; a straighter path to the superior vena cava; less proximity to the lung; and fewer complications of pleural or arterial puncture.[1] In addition, the supraclavicular approach less often necessitates interruption of CPR or tube thoracostomy than the infraclavicular method.[2]
Since the original description of the supraclavicular approach to the subclavian vein described by Yoffa,[1] there were many modifications done to reduce the complications and to achieve greater success.[3,4] Evidence supporting the use of ultrasound-guided cannulation in subclavian venous access is sparse.[5]
We, in our institution, routinely identify the vessel by positioning the linear transducer (Sonosite®Titan™ with LHFL 38 high frequency 13-6 MHZ 38-mm linear array transducer) at the clavisternomastoid angle obtaining the short axis view of the subclavian vein [Figure 1] and marking the puncture site on the skin overlying the center of the vessel before cannulation. The cannula is inserted through out- of- plane approach at an angle of 10° medially from the sagittal plane and 35° posteriorly from the coronal plane [Figure 2], and after confirming the placement of the cannula in the vein by free aspiration of the venous blood, the guide wire and subsequent catheter is introduced.
Figure 1.
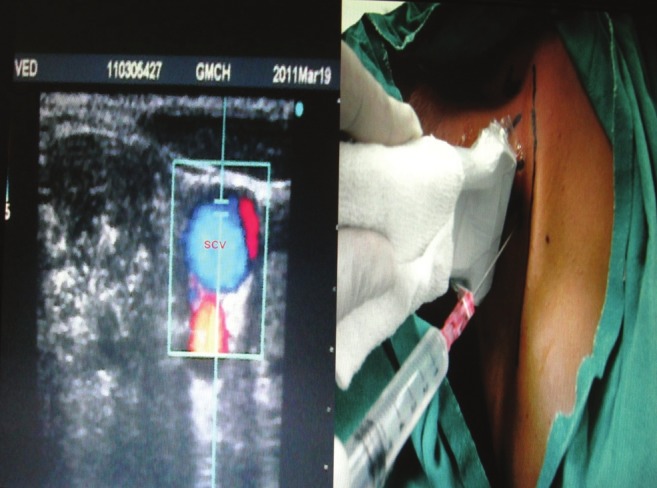
Supraclavicular short axis view of subclavian vein
Figure 2.

Modified approach for cannula insertion
While insertion of the guide wire, we sometimes encountered a problem of negotiating it past the likely area around clavicle where it frequently gets stuck and subsequently leads to difficult cannulation. The problem can be negated by gradually twisting the needle upside down with direction of the bevel rotated anticlockwise to an angle of 180° with constant gentle pressure applied over the guide wire [Figure 3]. By doing so, the bevel of the needle, which is originally facing upwards, which might leads to possibility of kinking of the guide wire, can be bypassed. The gentle constant pressure, which is applied over the guide wire, further directs it to follow the least resistance pathway along the vein.
Figure 3.
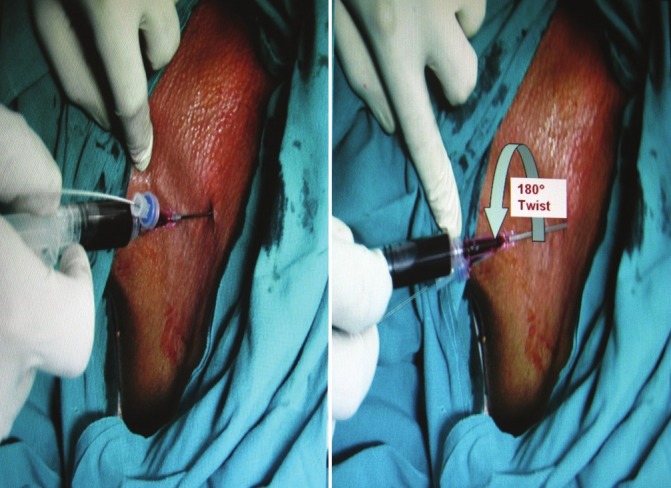
Upside down twist maneuver for guide wire insertion
For insertion of the cannula, we use modified approach,[6] in which the needle directs at an angle of 10° medially from the sagittal plane and 35° posteriorly from the coronal plane [Figure 2]. The risk of pnuemothorax, subclavian artery punctures, and pinch-off syndrome by catheters can be reduced by this approach.[6] While introducing the guide wire, there is sometimes resistance felt for insertion, even after upside down twist maneuver. This problem can be dealt by gently angulating the needle further medially in the sagittal plane (from 10° to nearly 45°) and anteriorly in the coronal plane (50° anterior angulation from the original angle, thus making an angle of 15° anterior from the coronal plane). The present direction of the needle is in concordance with the angulations seen in Yoffa technique[1] [Figure 4], thus now targeting the venous confluence of the subclavian and internal jugular vein instead of the previous subclavian vein.
Figure 4.

Yoffa Technique (Traditional approach) for cannula insertion
In nearly 100 cannulation, done in last 2 years, we have applied these simple troubleshooting maneuvers with excellent results though we do feel that further studies are warranted to evaluate and validate their efficacy.
References
- 1.Yoffa D. Supraclavicular subclavian venepuncture and catheterization. Lancet. 1965;2:614–7. doi: 10.1016/s0140-6736(65)90519-2. [DOI] [PubMed] [Google Scholar]
- 2.Dronen S, Thompson B, Nowak R, Tomlanovich M. Subclavian vein catheterization during cardiopulmonary resuscitation: A prospective comparison of the supraclavicular and infraclavicular percutaneous approaches. JAMA. 1982;247:3227–30. [PubMed] [Google Scholar]
- 3.Gorchynski J, Everett WW, Pentheroudakis E. A modified approach to supraclavicular subclavian vein catheter placement: The pocket approach. Cal J Emerg Med. 2004;5:50–4. [PMC free article] [PubMed] [Google Scholar]
- 4.MacDonnell JE, Perez H, Pitts SR, Zaki SA. Supraclavicular subclavian vein catheterization: Modified landmarks for needle insertion. Ann Emerg Med. 1992;21:421–4. doi: 10.1016/s0196-0644(05)82663-0. [DOI] [PubMed] [Google Scholar]
- 5.Silberzweig JE, Mitty HA. Central venous access: Low internal jugular vein approach using imaging guidance. AJR Am J Roentgenol. 1998;170:1617–20. doi: 10.2214/ajr.170.6.9609184. [DOI] [PubMed] [Google Scholar]
- 6.Jung CW, Seo JH, Lee W, Bahk JH. A novel supraclavicular approach to the right subclavian vein based on three-dimensional computed tomography. Anesth Analg. 2007;105:200–4. doi: 10.1213/01.ane.0000266469.63098.38. [DOI] [PubMed] [Google Scholar]