

Abstract
Angiofibrolipoma is a neoplasm composed of fibrocytes, capillaries and matured adipose tissues. It is a rare histopathologic variant of lipoma, characterized by matured adipocytes, blood vessels and dense collagenous tissues. It is an extremely rare tumor with very few cases reported in the literature. We are reporting a 9-year-old boy who presented with a right calf swelling noticed since birth, slowly increasing in size which became painful about a year prior to presentation (at about the age of 8 years). The mass extended from the popliteal fossa to the junction of the gastro-soleus. Mid calf circumference on the right was 44 cm and 24 cm on the left. Clinically there was no foot drop. He had neither preceding trauma nor fall. He had no systemic symptom. Pre-operative plain radiographs, incisional biopsy and other ancillary investigations were done. Histopathology result after excisional biopsy revealed angiofibrolipoma and postoperative clinical improvement was significant. To our knowledge, such a case has not been previously reported in the literature.
Key words: medicine, oncology, tumours, angiofibrolipoma
Introduction
Lipoma is a benign tumor composed of mature white adipocytes and is the most common soft tissue mesenchymal neoplasm in adults.1 It is well separated from surrounding tissues by a thin fibrous capsule.2-4 Lipoma can occur in any part of the body where adipose tissue is located, especially beneath the skin. However, 13% of cases occur in the head and neck region.2,3
The WHO classification of adipocytic tumors distinguishes lipomas based on their clinical and histopathological features into classic lipoma, angiolipoma, chondroid lipoma, and myolipoma spindle cell/pleomorphic lipoma.1 Histological variants of lipomas include fibrolipomas, angiolipomas, angiofibrolipomas, angiomyolipomas, and infiltrating angiolipomas.2,5,6 These classifications are based on the relationship between the fat, muscle, blood vessel, and connective tissues involved in the tumor structure. In this way, angiofibrolipomas are a mixture of mature adipocytes, vascular tissue and collagenous connective tissue.2,5,6 Angiofibro lipoma is a histological variant of lipoma, which usually presents as a solitary, subcutaneous, circumscribed lesion in the back, neck or shoulders.7 The growths are not encapsulated but are histologically distinct from surrounding tissues. They have low-to-moderate cellularity and are not clinically aggressive.5,8
Case Report
A 9-year-old boy presented with a history of right calf swelling noticed since birth which was slowly increasing in size. The swelling became painful about a year prior to presentation. He had no preceding history of trauma or fall. There was history of weight loss that was first noticed at the age of 7 years though weight loss was not marked. There was no pain from other parts of the body. There was no history of bone pain, jaundice, abdominal pain, chest pain or cough to suggest a metastatic lesion. There was no history of similar swelling in the siblings or parents. At presentation, essential findings were those of a young boy that was not pale, anicteric, with no significant lymph node enlargement. Musculoskeletal examination showed a 18×32 cm firm mass involving the upper 2/3 of the right leg posteriorly extending from the popliteal fossa down to the gastrosoleus junction with a punched out scar at the site of the previous incisional biopsy; which had been done prior to been planned for definitive management. The edges were poorly defined and tender on deep palpation. There was no clinical vascular deficit. Mid calf circumference on the right limb was 44 cm and 24 cm on the left. The mass was fixed to the underlying structure. The child maintained the ankle in an attitude of plantar-flexion. Attempt at standing plantigrade or placing the foot plantigrade resulted in pain, he therefore walked on his toes. Plain radiograph revealed a soft tissue mass at the posterior aspect of the right leg with no bone involvement (Figure 1).
Figure 1.

Plain x-ray of the patient before surgery shows an extensive soft tissue swelling.
Hematological parameters were within normal limits. Incisional, with later excisional biopsy were done. The excision was a marginal excision. Intra-operative findings were: i) a mass approximately 15×9×4 cm arising from the two heads of the gastronemius muscle at its origin in the popliteal fossa; ii) a yellowish-pink mass closely related to the posterior tibial artery at its origin in the fossa, the mass had to be dissected and removed piecemeal around the neurovascular bundle to prevent injury; iii) the soleus muscle had to be stripped off the gastronemius and the latter was detached at the gastrosoleus junction; iv) the cut surface of the mass was solid and yellowish with numerous ecchymotic patches (Figure 2).
Figure 2.
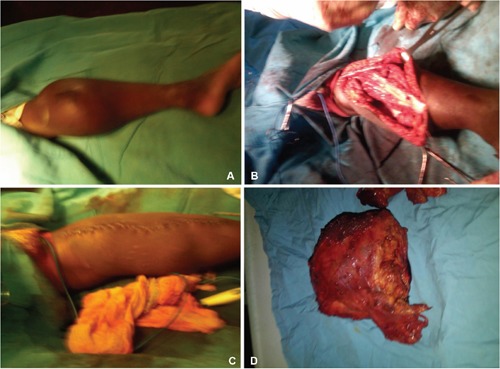
A) Patient on the operating table. Observe the scar of the earlier biopsy and the plantar-flexion of the ankle. B) Patient at excision. C) Patient after excision. D) Specimen at excision.
Histology showed fibrocollagenous tissue composed of adipose tissue and numerous thinwalled and congested vascular vessels. Also seen were chronic inflammatory cells, mainly lymphocytes and plasma cells. No evidence of malignancy seen in all the sections examined. Findings were consistent with angiofibrolipoma (Figure 3).
Figure 3.

Photomicrographs of the lesion.
Discussion
The etiology of angiofibrolipoma, like many neoplasms, is still unknown.2 However, implicated in its development are obesity, radiation, and a familial or genetic link, such as abnormality of chromosome 12 and trauma.2,9,10 Oral angiofibrolipoma has been reported in relation to trauma in a patient with prosthesis which developed 20 years after use of prosthesis.2 This protracted period of development was also supported in our case which has been noticed since birth before it was removed at the age of 9, as it has been found out that lipoma develop over several years.3 It is also worthy of note that the tumor in our case has been present since birth, a finding that has been associated in the literature with lipoblastoma; a lobulated, localized or diffuse tumor, resembling fetal adipose tissue.1 Angiolipoma is a close differential which however tends to occur more in the late teens and early twenties.1 Our patient is a 9-year old boy a finding which is also supported by the male preponderance in the incidence of lipoma and its variants.1 Examination findings depend on its site of occurrence. On the calf there may be swelling and tenderness which the index patient had. This may be attributable to the volume of the mass in the rather tight compartment. Important investigations include plain radio graph, CT Scan/MRI and incisional biopsy. The plain radiograph of the patient showed a huge soft tissue swelling with no bony involvement. The patient could not afford a CT Scan nor MRI. These would certainly have helped in the pre-operative planning. Mainstay of treatment for angiofibrolipoma and other variants of lipoma is surgical excision.1,3 Though recurrence is rare, there is need for follow up over a long period of time.1,3 The exception however is infiltrating angiolipoma, which has a recurrence rate of 35-50%.1,3,11 Conservative management may be observed if the tumour is not compromising vital structures, if it is not progressively increasing in size, and if cosmesis is not an issue. Our patient had a marginal excision and has been followed up for two years with no evidence of recurrence. The indication for the excision was increasing swelling, pain, and disability.
References
- 1.Fletcher CDM, Krishnan Unni K, Mertens F.World Health Organization classification of tumours: pathology and genetics tumours of soft tissue and bone. Lyon: IARC Press; 2002 [Google Scholar]
- 2.Brki A, Ozçamur C, Gürkan-Köseo lu B, Olgac V.Angiofibrolipoma of the buccal mucosa: a case report. J Oral Sci 2010;52:173-6 [DOI] [PubMed] [Google Scholar]
- 3.Auo HJ, Kang JM.Infiltrating angiolipoma of the nasopharynx: adjacent to an aberrant internal carotid artery. Auris Nasus Larynx 2009;36:247-50 [DOI] [PubMed] [Google Scholar]
- 4.Bandéca MC, de Pádua JM, Nadalin MR, et al. Oral soft tissue lipomas: a case series. J Can Dent Assoc 2007;73:431-4 [PubMed] [Google Scholar]
- 5.Liggett AD, Frazier KS, Styer EL.Angiolipomatous tumors in dogs and a cat. Vet Pathol 2002;39:286-9 [DOI] [PubMed] [Google Scholar]
- 6.Jacob A, Kneile J, Welling B.Angio fibro lipoma of the ear canal. Laryngoscope 2005;115:1461-2 [DOI] [PubMed] [Google Scholar]
- 7.Liu QL, Tian B, Zhang H, Qiao DS.Angiofibrolipoma of the spermatic cord. Asian J Androl 2009;11:746-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kershisnik W, McCarthy DJ, O’Donnell E.Angiofibrolipoma. A histologic variant of the lipoma. J Am Pediatr Med Assoc 1986;76:67-70 [DOI] [PubMed] [Google Scholar]
- 9.Enzinger FM, Weiss SW.Soft tissue tumors. 3rd ed.St Louis: Mosby; 1995. pp 384-405 [Google Scholar]
- 10.Merscher S, Marondel I, Pedeutour F, et al. Identification of new translocation breakpoints at 12q13 in lipomas. Genomics 1997;46:70-7 [DOI] [PubMed] [Google Scholar]
- 11.Ozer E, Schuller DE.Angiolipoma of the neck. Otolaryngol Head Neck Surg 2006;135:643-4 [DOI] [PubMed] [Google Scholar]