

Abstract
The majority of ingested foreign bodies pass of their own accord without causing any adverse impact on the patient, while others present a greater management dilemma. We present a case of a 36-year-old man admitted to the hospital with a 10-day history of colicky abdominal pain following voluntary ingestion of multiple pairs of vinyl gloves. The plain-film abdominal X-ray confirmed small bowel obstruction and gastric bezoar. After failed conservative management he opted for endoscopic retrieval. Following exposure to stomach acid the gloves had lost their structural integrity becoming hard, sharp and brittle. As a result endoscopic removal was abandoned due to the risk of traumatic injury to the oesophagus. A midline laparotomy was performed and the gloves were retrieved via enterotomy. While many foreign bodies are suitable for endoscopic extraction this case demonstrates that the retrieval of vinyl gloves is unlikely to be successful due to significant chemical change.
Background
Accident and emergency and surgical departments are frequently confronted with ingestion of a foreign body. The majority of objects pass of their own accord without causing adverse impact on the patient, while others present a greater management dilemma. It is important to be aware of the potential for seemingly innocuous objects to undergo chemical transformation from a benign substance into something harmful when in contact with the acidic environment of the stomach. We present a case of a 36-year-old man who ingested multiple pairs of vinyl gloves.
Case presentation
A 36-year-old man self-referred to accident and emergency with a 10-day history of colicky abdominal pain following voluntary ingestion of multiple pairs of surgical gloves. The initial onset of pain began 3 days after ingestion and progressed in severity, prompting his hospital attendance. He reported generalised cramping abdominal pain, initially intermittent, but becoming more constant by the time of presentation. Associated symptoms included anorexia, nausea, vomiting and decreased bowel movements. The patient had recently been released from prison, where he had ingested the gloves in pairs each time he lost in a game of cards. Each pair of gloves was carefully folded into a small pellet which was then ingested with the aid of water. His only significant medical history was an established diagnosis of schizophrenia, which was well controlled on Seroquel. On examination he was found to have generalised abdominal tenderness with guarding on deep palpation in the epigastrium.
Investigations
Routine admission bloods were unremarkable. The plain film abdominal X-ray showed small bowel obstruction and gastric bezoar prompting his admission to the general surgical unit (figure 1). After a period of observation with no significant clinical improvement a CT Scan was performed in order to determine the nature of the obstruction. This revealed a small bowel obstruction to the mid ileum with a transition point at an area of impacted debris with luminal collapse distal to the obstruction. Prominent debris was noted in the stomach and there was no evidence of free intra-abdominal gas to signify a perforation (figure 2).
Figure 1.

Abdominal X-ray showing gastric bezoar and small bowel obstruction.
Figure 2.
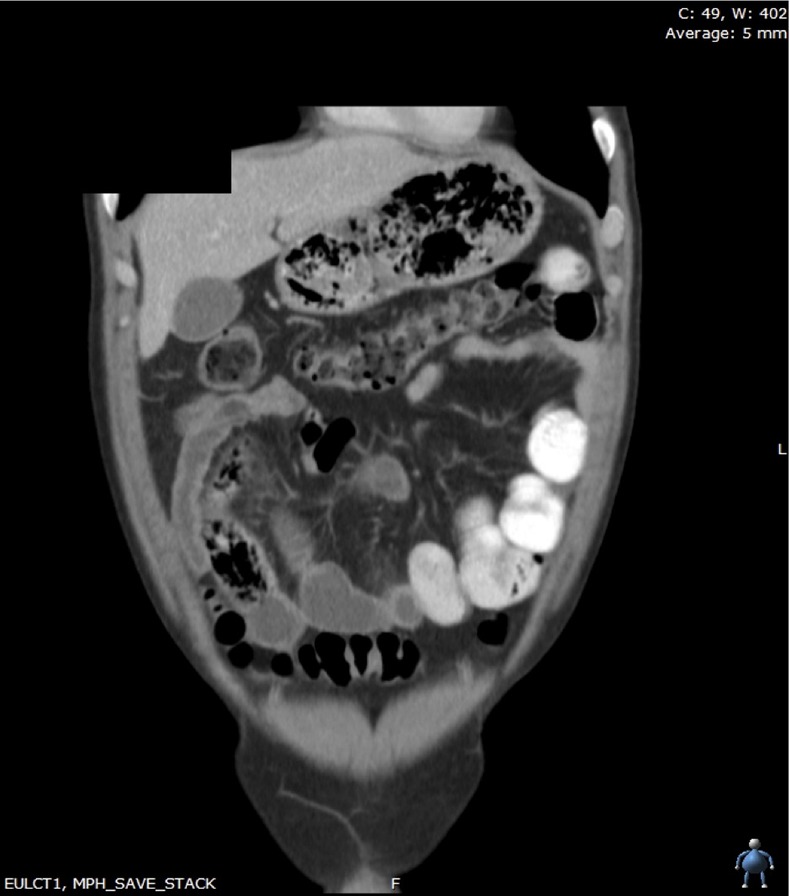
A CT scan showing significant gastric debris and dilated small bowel loops.
Treatment
Given that the patient was passing flatus, he was initially managed conservatively with laxatives and close clinical monitoring and a follow-up plain abdominal X-ray, in line with current views on the management of benign foreign body ingestion. However, on the third day of his admission (13 days from ingestion of foreign bodies) the patient continued to have abdominal distention, progressing to absolute constipation and a CT scan was performed. This confirmed failure of conservative management with significant debris remaining in the stomach and small bowel obstruction.
The patient was consented for gastroscopy and removal of the foreign body and proceeded to the theatre. At gastroscopy it was possible to visualise multiple gloves within the stomach; however, following exposure to stomach acid, the gloves had lost their structural integrity becoming hard, sharp and brittle. As a result of this change it was difficult to gain satisfactory purchase on the gloves and it was felt that continued attempts at endoscopic removal would risk substantial traumatic injury to the oesophagus and potential perforation. Following an appropriate time interval to allow for recovery from sedation the outcome of endoscopy was discussed with the patient and he was consented for a laparotomy to retrieve the remaining foreign bodies. A midline laparotomy was performed and 22 pairs of vinyl gloves were removed. Two pairs were identified in the terminal ileum and removed via enterotomy with the remaining gloves removed via gastrotomy. In addition, the patient had also ingested a Chelsea Football Club badge and a large clothing label both of which were removed from the stomach. An oesophagogastroduodenoscopy was performed prior to closure to ensure there were no remaining objects.
Outcome and follow-up
Postoperatively the patient developed a paralytic ileus, which resolved with conservative management. He remained clinically well and following several days of observation was discharged home with follow-up in the surgical outpatient clinic.
Discussion
Ingestion of foreign bodies is common. Successful management will depend on the nature of the object and its location within the gastrointestinal tract.1 Areas of anatomical narrowing (cricopharyngeus, lower oesophageal sphincter, pylorus, ileocaecal valve and the anus) are common sites of impaction, with objects in the oesophagus requiring prompt retrieval due to their potential risk of perforation and airway obstruction.1–3 Foreign body ingestion is most commonly seen in the paediatric population by accidental means or in association with pica. However, intentional ingestion of foreign bodies has been reported in adults were mental health issues, intoxication, incarceration and attempted evasion of drug possession are seen as risk factors in its occurrence.1 3–7 When the object in question is known to be within the stomach, management strategies include a conservative watch and wait approach, endoscopic retrieval and surgical intervention.1–3 8 Endoscopic retrieval is often successful and should be considered first-line management in a patient failing to pass the offending material; however, sharp objects have a higher failure rate with endoscopy due to potential trauma caused by its removal.8 9 We report a case of vinyl glove ingestion in order to highlight the importance of considering chemical transformation by stomach acid on an ingested foreign body. Vinyl glove ingestion is rare having been reported exclusively in children with pica or vulnerable adults with extensive mental health issues.10 11 Ours is the first reported case of vinyl glove ingestion due to gambling misadventure. Polyvinyl chloride or vinyl is a multipurpose plastic used in the manufacture of protective gloves. When ingested vinyl gloves undergo chemical transformation, likely a result of cross bridging of polymers, similar to the process of rubber vulcanisation. This leads to the development of sharp edges causing impaction, intestinal obstruction and potential perforation of the gastrointestinal tract.10 11 While many foreign bodies are suitable for endoscopic extraction this case demonstrates that the retrieval of vinyl gloves is unlikely to be successful due to significant chemical change.10 11 Endoscopy may still have a role in the management of such cases by confirming the presence of chemical transformation. However, when a chemical change has occurred we would recommend timely surgical intervention given the potential risks of intestinal injury or perforation with conservative management or endoscopic retrieval.
Learning points.
Contact with stomach acid has the potential to transform seemingly innocuous objects from a benign substance into something harmful.
Patients presenting with a history of vinyl or other plastic object ingestion should not be dismissed without adequate imaging and correlation with clinical history.
Endoscopic retrieval of vinyl gloves following a significant period of exposure to the acidic stomach environment is unlikely to be successful due to significant chemical change.
Patients presenting with the above should undergo early endoscopy and should be informed of, and consented for, the failure of endoscopic retrieval requiring laparotomy.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Kay M, Wyllie R. Pediatric foreign bodies and their management. Curr Gastroenterol Rep 2005;7:212–18 [DOI] [PubMed] [Google Scholar]
- 2.Arana A, Hauser B, Hachimi-Idrissi S, et al. Management of ingested foreign bodies in childhood and review of the literature. Eur J Pediatr 2001;160:468–72 [DOI] [PubMed] [Google Scholar]
- 3.Bisharat M, O'Donnell ME, Gibson N, et al. Foreign body ingestion in prisoners: the belfast experience. Ulster Med J 2008;7:110–14 [PMC free article] [PubMed] [Google Scholar]
- 4.Budnick LD. Toothpick related injuries in the United States, 1979 through 1982. JAMA 1984;252:796–7 [PubMed] [Google Scholar]
- 5.Danford DE, Huber AM. Pica among mentally retarded adults. Am J Ment Defic 1982;87:141–6 [PubMed] [Google Scholar]
- 6.Voitk AJ. Acute abdomen in severely mentally retarded patients. Can J Surg 1987;30:195–6 [PubMed] [Google Scholar]
- 7.Siriwardana HP, Ammori BJ. Laparoscopic removal of a large gastric bezoar in a mentally retarded patient with pica. Surg Endosc 2003;17:834. [DOI] [PubMed] [Google Scholar]
- 8.Velitchkov NG, Grigorov GI, Losanoff JE, et al. Ingested foreign bodies of the gastrointestinal tract: retrospective analysis of 542 cases. World J Surg 1996;20:1001–5 [DOI] [PubMed] [Google Scholar]
- 9.Mosca S, Manes G, Martino R, et al. Endoscopic management of foreign bodies in the upper gastrointestinal tract: report on a series of 414 adult patients. Endoscopy 2001;3:692–6 [DOI] [PubMed] [Google Scholar]
- 10.Kamal I, Thompson J, Paquette DM. The hazards of vinyl glove ingestion in the mentally retarded patient with pica: new implications for surgical management. Can J Surg 1999;42:201–4 [PMC free article] [PubMed] [Google Scholar]
- 11.Stringel G, Parker M, McCoy E. Vinyl glove ingestion in children: a word of caution. J Pediatr Surg 2012;47:996–8 [DOI] [PubMed] [Google Scholar]