

Abstract
Statin induced pancreatitis has historically been considered a diagnosis of exclusion, with literature references typically in the form of case reports and observational studies. Recently, larger studies have challenged the correlations made by earlier case reports, and instead demonstrate a mild protective effect in statin users. We present a case report of likely statin induced pancreatitis in a 58-year-old male (which we have attributed to drug-drug interaction with resulting inhibition of hepatic cytochrome P450 enzymes) and have reviewed the apparent dichotomy in the available literature.
Keywords: Statin, Pancreatitis, CYP450, Inflammation, Toxic
Core tip: Statins may reduce the risk of developing an acute episode of pancreatitis through anti-inflammatory perturbation of the systemic inflammatory response pathway. However, it appears that these drugs may also carry a concomitant long-term risk of pancreatitis through a buildup of toxic metabolite/s.
INTRODUCTION
Drug-induced pancreatitis has historically been considered a relatively uncommon cause of acute pancreatitis, accounting for 1.4%-2% of all cases[1,2]. However, recent studies indicate that the diagnosis of drug-induced pancreatitis may be underestimated[3,4]. Among the many drugs that have been associated with pancreatitis, lipid-lowering agents-in particular, statins-have been increasingly reported as a cause of acute pancreatitis[5]. More recently, a large population based case control study and meta-analysis have called into question the prevailing consensus regarding the role of statins in the development of acute pancreatitis. This apparent dichotomy in the literature warrants that we re-examine what is known about the role of statins in acute pancreatitis. We present a case of a 58-year-old male incidentally found to have acute pancreatitis in the setting of background statin therapy.
CASE REPORT
A 58-year-old Caucasian male with a past medical history of traumatic brain injury at the age of five with a history of complex partial seizures and renal cell cancer status post right partial nephrectomy presented with syncope. His initial complete blood count (CBC) and electrolyte panel were normal. Head computer tomography (CT) was negative for any intracranial processes. The patient was subsequently managed for vaso-vagal syncope secondary to severe coughing spells. On the day of planned discharge the patient complained of vague pain in his right upper quadrant and epigastrium that had been progressively worsening for the past month. Physical exam revealed a negative Murphy’s sign and labs and imaging were ordered. The ultrasound was negative for gallstone disease, pericholecystic fluid and pericholecystic thickening. Liver function tests (LFTs), white blood cell count, serum creatinine and calcium levels were also within normal limits. Interestingly, lipase and amylase levels were noted to be elevated at 702 units/L (normal values 28-350 units/L) and 417 units/L (normal values 27-117 units/L), respectively. Triglyceride levels were found to be 317 mg/dL, which would unlikely account for an episode of acute pancreatitis (hypertriglyceridemia is typically considered a risk for pancreatitis when levels are > 1000 mg/dL)[6]. In addition, the patient denied any history of alcohol use. He did not have any travel outside of the United States. CT of the abdomen was performed and found to be consistent with an acute episode of pancreatitis without evidence of structural anomaly (Figure 1). After extensive review of his history and the relevant literature, we found that the patient was on three medications [valproic acid (class 1A), omeprazole (class 1B) and simvastatin (class 1A)] that could potentially cause pancreatitis[5]. In this patient’s case, venlafaxine (a potent inhibitor of neuronal serotonin and norepinephrine reuptake and weak inhibitor of dopamine reuptake) was started six weeks prior and is extensively metabolized by the same hepatic enzyme (CYP3A4) as simvastatin-which he had been taking for more than 10 years. Omeprazole is extensively metabolized by CYP2C19 with only minor contributions from CYP3A4 while valproic acid is not metabolized by CYP3A4. We accordingly held his simvastatin with subsequent decline in lipase levels and resolution of symptoms in the next 24-48 h.
Figure 1.
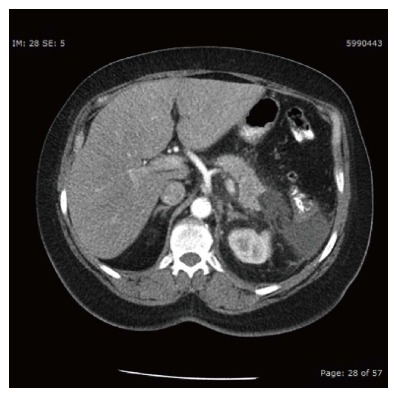
Cross-sectional view of computer tomography abdomen with contrast showing pancreatitis of the body and tail.
Notably, the standardized Naranjo Adverse Drug Reaction Probability Scale was used to assess the strength of the suspected link between acute pancreatitis and the above-mentioned drugs (venlafaxine, simvastatin, omeprazole and valproic acid) in this patient. In each case, we deduced the probability to be possible for an adverse drug reaction causing acute pancreatitis[7].
DISCUSSION
Although the mechanism of action of statin induced pancreatitis remains ill defined in the literature, an immune-mediated inflammatory response, direct cellular toxicity and metabolic effect have all been postulated as possible culprits[8]. Three case reports have identified drug-drug interaction as the most likely precipitant. Wong et al[9] documented a case of multiple organ toxicity, including acute pancreatitis, which was due to the interaction between lovastatin and erythromycin. Likewise, Abdul-Gaffar and El-Sombaty reported a case of acute pancreatitis with rhabdomyolysis due to the interaction between lovastatin and gemfibrozil[10]. Acute pancreatitis was also reported in the context of interaction between simvastatin and fenofibrate[11]. Interestingly, with regards to combined simvastatin and fenofibrate therapy, Stefanutti et al[12] reported no serious adverse effects in 45 patients using this double-drug regimen over a 12 mo period. The above data and previously reported cases of statin-induced pancreatitis during the last 2 decades are reported in Table 1.
Table 1.
Previously reported cases of statin-induced pancreatitis
| Ref. | Patient (age, yr/gender) | Associated drug/s | Drug rechallenge | Outcome |
| Abdul-Ghaffar et al[10] | 55/Female | Lovastatin and gemfibrozil | No | Complete recovery |
| Wong et al[9] | 73/Male | Lovastatin and erythromycin | Yes: no recurrence | Complete recovery |
| Belaïche et al[22] | 63/Male | Atorvastatin | No | Complete recovery |
| Tysk et al[13] | 36/Male | Fluvastatin | Yes: Recurrence | Complete recovery |
| McDonald et al[11] | 70/Male | Simvastatin and Fenofibrate | No | Fatal |
| Miltiadous et al[19] | 60/Male | Salicylate and Atorvastatin | No | Not available |
| Anagnostopoulos et al[20] | 56/Male | Pravastatin | Yes: Recurrence | Complete recovery |
| Singh et al[23] | 77/Female | Atorvastatin and Rosuvastatin | Yes; Recurrence with Rosuvastatin | Complete recovery |
| Antonopoulos et al[41] | 58/Male | Salicylate and Simvastatin | No | Complete recovery |
| Tsigreliset al[25] | 50/Female | Pravastatin | No | Complete recovery |
| Chintanaboinaet al[21] | 67/Female | Rosuvastatin | Yes: Recurrence | Complete Recovery |
| Current report | 58/Male | Simvastatin and Venlafaxine | No | Complete Recovery |
These cases are predicated on the inhibitory effect of these drugs on the oxidative metabolism of statins via the hepatic cytochrome P450 enzymes, in particular CYP3A4[13]. This is the mechanism that we have postulated in the case above. Venlafaxine is metabolized predominantly by CYP3A4 and was likely the reason that Simvastatin, which was being used for years, had precipitated an episode of acute pancreatitis. Interestingly, fibrates have also been found to inhibit the glucuronidation and non-CYP3A-mediated oxidation of statins[14]. It is important to note that in the case presented above, other more common causes of acute pancreatitis such as alcohol, mechanical ampullary obstruction via gallstones, hypercalcemia, hypertriglyceridemia, post-endoscopic retrograde cholangiopancreatography (ERCP) and trauma were initially ruled by history, laboratory tests and gallbladder ultrasound. CT of the abdomen also excluded congenital pancreatic anomaly-which is rather unlikely to have primary occurrence in the 6th decade of life. Initial workup for other less common causes such as autoimmune (IgG4 related) pancreatitis, vasculitis from systemic lupus erythematosis and polyarteritis nodosa was negative.
As an aside, it is noted that the patient above had right partial nephrectomy secondary to a history of renal cell carcinoma. While this has been shown to alter the pharmacokinetics (e.g., decrease in renal metabolism/excretion of drugs) in patients with resultant chronic kidney disease, the above patient did not have evidence of renal impairment and thus this condition was not expected to significantly impact renal drug metabolism[15,16].
Singh and Loke have postulated that there exists differences in the safety profiles of the various statins that may correlate with the degree to which they inhibit cytochrome P450 CYPA4 as well as the degree of their lipophilicity[17]. A subsequent meta-analysis demonstrating a lower incidence of adverse drug reactions with pravastatin (which is the only statin not metabolized by CYP3A4) versus with atorvastatin (which inhibits CYP3A4) gives credence to this idea[18]. Miltiadous et al[19] have also documented a case in which acute pancreatitis may have been caused by the interaction between atorvastatin and salicylates, however no possible mechanism of action has been put forward.
Understandably, reintroduction of the likely offending drug following the resolution of symptoms has been largely unfeasible due to the risk of recurrence. As such, their remains a dearth of concrete experimental evidence regarding the precise mechanism of action for the reported cases of statin-induced pancreatitis. Interestingly, the majority of documented instances in which statins have been reintroduced, demonstrate reproducibility of acute pancreatitis and/or symptoms consistent with this diagnosis[8,13,19-21]. However, these findings have not been universal as Belaiche and colleagues have documented a patient who tolerated pravastatin prior to and following an episode of atorvastatin-induced pancreatitis[22]. Furthermore, the latency period from initiation of treatment with a statin to onset of pancreatitis also varies between different statins, ranging from one day to several months[13]. Thus, there is lack of consensus in the literature regarding whether statins exert a class effect or carry distinct and individual risk profiles[13,22,23]. Observations from Singh et al[17] however suggest that statin induced pancreatitis rarely occurs early and most commonly occurs months to years after statins have been started. As one would expect, this predilection for later onset favors the buildup of toxic metabolite as an etiologic factor. A more recent cross-sectional study also found that statin use was more frequent among patients with idiopathic acute pancreatitis than in patients with other known etiologies of acute pancreatitis (e.g., alcohol and gallstone-induced). The inherent positive correlation does not however prove causality as it is noted that statin users were more likely to suffer from diabetes, obesity and dyslipidemia-which are all risk factors for acute pancreatitis[24].
A systematic review of observational studies and case reports yielded interesting results as statin-induced pancreatitis was found to have no correlation with the cumulative ingested dose of statins[17]. Analysis of the data revealed that the development of statin-induced pancreatitis was independent of duration of therapy even though it occurred more commonly months to years after treatment with statins. Although statins are generally used more frequently in older individuals, age of the patient was not found to be a major susceptibility factor[17]. It also appears that the majority of cases of statin-induced pancreatitis usually follow a relatively mild course with only a few severe or fatal cases reported[17,25]. This mirrors the natural history of other documented cases of drug-induced pancreatitis[1].
However, as noted above, lack of consensus regarding the precise causal link between statin use and the development of acute pancreatitis still exists. With regards to pathophysiology, acute pancreatitis involves local pancreatic inflammation as well as activation of the systemic inflammatory response system (SIRS)[26]. The latter system is characterized by the activation of multiple cellular processes and humoral cascades which supports the notion that acute pancreatitis results from an imbalance of pro-inflammatory and anti-inflammatory cytokines[27]. Thus, any targeted- intervention should, in theory, be capable of attenuating several arms of the inflammatory cascade. Statins have a diverse range of potent anti-inflammatory properties which are believed to modify the pathogenesis of acute pancreatitis. To this end, Almog et al[27] have proposed the following possible effects of statins as it relates to the inflammatory cascade: (1) statins could disrupt ligand receptor interaction step thereby hindering the SIRS cascade; (2) statins could blunt the acute-phase response and its immediate consequences; (3) statins could exert a protective effect on the elegant sequence of endothelial activation, dysfunction; and (4) apoptosis statins may also help create a favorable balance between constitutive nitric oxide synthase and inducible nitric oxide synthase so that maintenance of hemodynamic stability is favored[28-32].
In addition to the above theoretical benefits, Choi et al[33] have demonstrated an increase in Heat Shock Protein (HSP) 60 (HSPs are responsible for maintaining cellular homeostasis and help cells survive stress conditions by repairing damaged proteins)and decrease in the release of inflammatory mediators (e.g., IL-1beta, TNF-alpha and IL-6) when statins were used in rats with cholecystokinin-octapeptide (CCK)-induced pancreatitis. Subsequent animal studies have also demonstrated benefit of statin therapy in acute via reduction of IL-10 levels and myeloperoxidase activity[28]. Thus, these studies may indicate an anti-inflammatory role-via the modulation of various pro and anti-inflammatory cytokines-for statins in acute pancreatitis, however no long term protective benefit have been yet demonstrated.
In a population based case-control study involving three Danish counties, Thisted et al[34] found no strong causative effect of statins on the risk of developing acute pancreatitis. Instead, they found that former statin users (those patients who used statins greater than ninety days prior to hospital admission for acute pancreatitis) were at increased risk of acute pancreatitis. Furthermore, no increased risk among new users (those patients who filled their first statin prescription 0-90 d prior to hospital admission for acute pancreatitis) was shown, arguing against a direct short-term toxic effect of statins. These authors also cite a possible mild protective effect of statins as their results indicated an inverse relationship between the number of filled statin prescriptions and the risk of acute pancreatitis[34]. This finding does not lend support to the theory of a long-term accumulation of a toxic metabolite and may be mediated by the cholesterol and-to a lesser extent-triglyceride lowering effects of statins (it is noted that statins are not the first line therapy for hypertriglyceridemia)[34,35].
More recently, a meta-analysis conducted by Preiss et al[36] demonstrated that statin use was associated with a reduced risk of pancreatitis in patients with normal or mildly elevated triglyceride levels. This study also suggests a possible protective effect of statins, citing both the reduction of bile cholesterol levels and reduced risk of gallstone formation in statin users as corroborating evidence[37,38]. However, this meta-analysis is likely to be effected by multiple issues such as the failure of the trials to include pancreatitis as a primary end point, the lack of standardization when recording episodes of pancreatitis, the inability to examine specific causes of pancreatitis such as gallstones, and lack of access to individual-participant data. In addition, because exclusion criteria in the trials tended to exclude patients with marked hypertriglyceridemia, the findings may not be generalizable to that specific group of patients[36].
In light of the evolving evidence regarding statin induced pancreatitis, we believe that statins may reduce the risk of developing an acute episode of pancreatitis through anti-inflammatory perturbation of the systemic inflammatory response pathway. However, it appears that these drugs may also carry a concomitant long-term risk through a buildup of toxic metabolite/s. That being said, the overall mortality benefit of statin use (e.g., especially in patients with recent acute coronary syndrome and established coronary artery disease) clearly outweighs the risk of developing acute pancreatitis based on current evidence[39,40]. Further prospective double blinded trials with statin challenge and re-challenge are necessary to clarify the precise relationship between statin use and the development of acute pancreatitis.
COMMENTS
Case characteristics
A 58 years old male with presenting with sudden onset abdominal pain.
Clinical diagnosis
Characteristic epigastric abdominal pain and tenderness radiating to the back.
Differential diagnosis
Includes acute cholecystitis, gastroesophageal reflux disease, peptic ulcer disease and abdominal aortic dissection.
Laboratory diagnosis
Lipase and amylase levels were elevated at 702 units/L (normal values 28-350 units/L) and 417 units/L (normal values 27-117 units/L), respectively.
Imaging diagnosis
Computer tomography of the abdomen with contrast demonstrated inflammation of the body and tail of the pancreatitis highly suggestive of acute pancreatitis.
Treatment
The offending agent, which in this case was simvastatin, was discontinued in addition to bowel rest and pain control.
Related reports
Please refer to Table 1 for previously reported cases of statin-induced pancreatitis during the last 2 decades.
Experiences and lessons
Careful examination of drug profile and drug-drug interactions is necessary when other more common causes (e.g., gallstone disease, alcohol, etc.) of pancreatitis have been excluded.
Peer review
The authors report a case of pancreatitis during treatment with statin, quickly improved after stopping statin intake, and review literature concerning this topic. The manuscript is of sufficient interest, considering the limited knowledge currently available on the possible correlation between use of statins and pancreatitis.
Footnotes
P- Reviewer: Chow WK, Guarneri F, Sperti C, Stefanutti C, Shen SQ S- Editor: Song XX L- Editor: A E- Editor: Lu YJ
References
- 1.Lankisch PG, Dröge M, Gottesleben F. Drug induced acute pancreatitis: incidence and severity. Gut. 1995;37:565–567. doi: 10.1136/gut.37.4.565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Eland IA, van Puijenbroek EP, Sturkenboom MJ, Wilson JH, Stricker BH. Drug-associated acute pancreatitis: twenty-one years of spontaneous reporting in The Netherlands. Am J Gastroenterol. 1999;94:2417–2422. doi: 10.1111/j.1572-0241.1999.01367.x. [DOI] [PubMed] [Google Scholar]
- 3.Vinklerová I, Procházka M, Procházka V, Urbánek K. Incidence, severity, and etiology of drug-induced acute pancreatitis. Dig Dis Sci. 2010;55:2977–2981. doi: 10.1007/s10620-010-1277-3. [DOI] [PubMed] [Google Scholar]
- 4.Grendell JH. Editorial: drug-induced acute pancreatitis: uncommon or commonplace? Am J Gastroenterol. 2011;106:2189–2191. doi: 10.1038/ajg.2011.307. [DOI] [PubMed] [Google Scholar]
- 5.Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007;5:648–661; quiz 644. doi: 10.1016/j.cgh.2006.11.023. [DOI] [PubMed] [Google Scholar]
- 6.Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Sacks F, Murad MH, Stalenhoef AF. Evaluation and treatment of hypertriglyceridemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97:2969–2989. doi: 10.1210/jc.2011-3213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, Janecek E, Domecq C, Greenblatt DJ. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–245. doi: 10.1038/clpt.1981.154. [DOI] [PubMed] [Google Scholar]
- 8.Johnson JL, Loomis IB. A case of simvastatin-associated pancreatitis and review of statin-associated pancreatitis. Pharmacotherapy. 2006;26:414–422. doi: 10.1592/phco.26.3.414. [DOI] [PubMed] [Google Scholar]
- 9.Wong PW, Dillard TA, Kroenke K. Multiple organ toxicity from addition of erythromycin to long-term lovastatin therapy. South Med J. 1998;91:202–205. doi: 10.1097/00007611-199802000-00015. [DOI] [PubMed] [Google Scholar]
- 10.Abdul-Ghaffar NU, el-Sonbaty MR. Pancreatitis and rhabdomyolysis associated with lovastatin-gemfibrozil therapy. J Clin Gastroenterol. 1995;21:340–341. doi: 10.1097/00004836-199512000-00027. [DOI] [PubMed] [Google Scholar]
- 11.McDonald KB, Garber BG, Perreault MM. Pancreatitis associated with simvastatin plus fenofibrate. Ann Pharmacother. 2002;36:275–279. doi: 10.1345/aph.1A180. [DOI] [PubMed] [Google Scholar]
- 12.Stefanutti C, Bucci A, Di Giacomo S, Fraone N, Pace A, Mareri M, Musca A, Mammarella A. Efficacy, safety and tolerability of combined low-dose simvastatin-fenofibrate treatment in primary mixed hyperlipidaemia. Clin Drug Investig. 2004;24:465–477. doi: 10.2165/00044011-200424080-00005. [DOI] [PubMed] [Google Scholar]
- 13.Tysk C, Al-Eryani AY, Shawabkeh AA. Acute pancreatitis induced by fluvastatin therapy. J Clin Gastroenterol. 2002;35:406–408. doi: 10.1097/00004836-200211000-00010. [DOI] [PubMed] [Google Scholar]
- 14.Prueksaritanont T, Tang C, Qiu Y, Mu L, Subramanian R, Lin JH. Effects of fibrates on metabolism of statins in human hepatocytes. Drug Metab Dispos. 2002;30:1280–1287. doi: 10.1124/dmd.30.11.1280. [DOI] [PubMed] [Google Scholar]
- 15.Meyer JP, Delves GH, Sullivan ME, Keoghane SR. The effect of nephroureterectomy on glomerular filtration rate. BJU Int. 2006;98:845–848. doi: 10.1111/j.1464-410X.2006.06373.x. [DOI] [PubMed] [Google Scholar]
- 16.Shirasaki Y, Tsushima T, Nasu Y, Kumon H. Long-term consequence of renal function following nephrectomy for renal cell cancer. Int J Urol. 2004;11:704–708. doi: 10.1111/j.1442-2042.2004.00879.x. [DOI] [PubMed] [Google Scholar]
- 17.Singh S, Loke YK. Statins and pancreatitis: a systematic review of observational studies and spontaneous case reports. Drug Saf. 2006;29:1123–1132. doi: 10.2165/00002018-200629120-00004. [DOI] [PubMed] [Google Scholar]
- 18.Silva MA, Swanson AC, Gandhi PJ, Tataronis GR. Statin-related adverse events: a meta-analysis. Clin Ther. 2006;28:26–35. doi: 10.1016/j.clinthera.2006.01.005. [DOI] [PubMed] [Google Scholar]
- 19.Miltiadous G, Anthopoulou A, Elisaf M. Acute pancreatitis possibly associated with combined salicylate and atorvastatin therapy. JOP. 2003;4:20–21. [PubMed] [Google Scholar]
- 20.Anagnostopoulos GK, Tsiakos S, Margantinis G, Kostopoulos P, Arvanitidis D. Acute pancreatitis due to pravastatin therapy. JOP. 2003;4:129–132. [PubMed] [Google Scholar]
- 21.Chintanaboina J, Gopavaram D. Recurrent acute pancreatitis probably induced by rosuvastatin therapy: a case report. Case Rep Med. 2012;2012:973279. doi: 10.1155/2012/973279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Belaïche G, Ley G, Slama JL. [Acute pancreatitis associated with atorvastatine therapy] Gastroenterol Clin Biol. 2000;24:471–472. [PubMed] [Google Scholar]
- 23.Singh S, Nautiyal A, Dolan JG. Recurrent acute pancreatitis possibly induced by atorvastatin and rosuvastatin. Is statin induced pancreatitis a class effect? JOP. 2004;5:502–504. [PubMed] [Google Scholar]
- 24.Pulkkinen J, Kastarinen H, Kiviniemi V, Jyrkkä J, Juvonen P, Räty S, Paajanen H. Statin use in patients with acute pancreatitis and symptomatic gallstone disease. Pancreas. 2014;43:638–641. doi: 10.1097/MPA.0000000000000068. [DOI] [PubMed] [Google Scholar]
- 25.Tsigrelis C, Pitchumoni CS. Pravastatin: a potential cause for acute pancreatitis. World J Gastroenterol. 2006;12:7055–7057. doi: 10.3748/wjg.v12.i43.7055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bhatia M, Wong FL, Cao Y, Lau HY, Huang J, Puneet P, Chevali L. Pathophysiology of acute pancreatitis. Pancreatology. 2005;5:132–144. doi: 10.1159/000085265. [DOI] [PubMed] [Google Scholar]
- 27.Almog Y. Statins, inflammation, and sepsis: hypothesis. Chest. 2003;124:740–743. doi: 10.1378/chest.124.2.740. [DOI] [PubMed] [Google Scholar]
- 28.Almeida JL, Sampietre SN, Mendonça Coelho AM, Trindade Molan NA, Machado MC, Monteiro da Cunha JE, Jukemura J. Statin pretreatment in experimental acute pancreatitis. JOP. 2008;9:431–439. [PubMed] [Google Scholar]
- 29.Blanco-Colio LM, Tuñón J, Martín-Ventura JL, Egido J. Anti-inflammatory and immunomodulatory effects of statins. Kidney Int. 2003;63:12–23. doi: 10.1046/j.1523-1755.2003.00744.x. [DOI] [PubMed] [Google Scholar]
- 30.Kwak BR, Mach F. Statins inhibit leukocyte recruitment: new evidence for their anti-inflammatory properties. Arterioscler Thromb Vasc Biol. 2001;21:1256–1258. [PubMed] [Google Scholar]
- 31.Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor. Circulation. 2004;109:II2–I10. doi: 10.1161/01.CIR.0000129535.04194.38. [DOI] [PubMed] [Google Scholar]
- 32.Liappis AP, Kan VL, Rochester CG, Simon GL. The effect of statins on mortality in patients with bacteremia. Clin Infect Dis. 2001;33:1352–1357. doi: 10.1086/323334. [DOI] [PubMed] [Google Scholar]
- 33.Choi OS, Park SJ, Seo SW, Park CS, Cho JJ, Ahn HJ. The 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitor, lovastatin (statin) ameliorates CCK-induced acute pancreatitis in rats. Biol Pharm Bull. 2005;28:1394–1397. doi: 10.1248/bpb.28.1394. [DOI] [PubMed] [Google Scholar]
- 34.Thisted H, Jacobsen J, Munk EM, Nørgaard B, Friis S, McLaughlin JK, Sørensen HT, Johnsen SP. Statins and the risk of acute pancreatitis: a population-based case-control study. Aliment Pharmacol Ther. 2006;23:185–190. doi: 10.1111/j.1365-2036.2006.02728.x. [DOI] [PubMed] [Google Scholar]
- 35.Stein EA, Lane M, Laskarzewski P. Comparison of statins in hypertriglyceridemia. Am J Cardiol. 1998;81:66B–69B. doi: 10.1016/s0002-9149(98)00041-1. [DOI] [PubMed] [Google Scholar]
- 36.Preiss D, Tikkanen MJ, Welsh P, Ford I, Lovato LC, Elam MB, LaRosa JC, DeMicco DA, Colhoun HM, Goldenberg I, et al. Lipid-modifying therapies and risk of pancreatitis: a meta-analysis. JAMA. 2012;308:804–811. doi: 10.1001/jama.2012.8439. [DOI] [PubMed] [Google Scholar]
- 37.Duane WC, Hunninghake DB, Freeman ML, Pooler PA, Schlasner LA, Gebhard RL. Simvastatin, a competitive inhibitor of HMG-CoA reductase, lowers cholesterol saturation index of gallbladder bile. Hepatology. 1988;8:1147–1150. doi: 10.1002/hep.1840080531. [DOI] [PubMed] [Google Scholar]
- 38.Bodmer M, Brauchli YB, Krähenbühl S, Jick SS, Meier CR. Statin use and risk of gallstone disease followed by cholecystectomy. JAMA. 2009;302:2001–2007. doi: 10.1001/jama.2009.1601. [DOI] [PubMed] [Google Scholar]
- 39.Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene AM. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1504. doi: 10.1056/NEJMoa040583. [DOI] [PubMed] [Google Scholar]
- 40.Kjekshus J, Pedersen TR. Reducing the risk of coronary events: evidence from the Scandinavian Simvastatin Survival Study (4S) Am J Cardiol. 1995;76:64C–68C. doi: 10.1016/s0002-9149(99)80473-1. [DOI] [PubMed] [Google Scholar]
- 41.Antonopoulos S, Mikros S, Kokkoris S, Protopsaltis J, Filioti K, Karamanolis D, Giannoulis G. A case of acute pancreatitis possibly associated with combined salicylate and simvastatin treatment. JOP. 2005;6:264–268. [PubMed] [Google Scholar]