

Abstract
Sweet's syndrome is a well-known entity in the field of dermatology. It has presented itself in myriad forms, well-recorded in literature. Our patient presented with a sudden eruption of nontender molluscoid pseudovesicles distributed over the neck and forearms alone. A complete diagnostic work up for the same did not give any clue regarding an underlying systemic ailment, responsible for the dermatosis. This case is being presented because of this extremely rare morphology of Gomm-Button disease.
Keywords: Molluscoid pseudovesicles, nontender, Sweet's syndrome
What was known?
Idiopathic Sweet's syndrome (SS) usually has a female preponderance
Edematous pseudovesicles is the hallmark morphology of lesions in SS
Lesions in SS, generally have an asymmetric and generalized distribution
Constitutional symptoms usually precede the cutaneous manifestations in SS.
Introduction
Sweet's syndrome (SS) presenting in a localized and symmetric pattern is a very rare phenomenon. There have, however, been, a few case reports for the same. SS per se was first reported in 1964 by Robert Douglas Sweet.[1] Though classically presenting as tender pseudovesicles, SS may demonstrate numerous topographic variations, which could be quite confusing for the diagnosing dermatologist.
Case Report
A 45-year-old farmer from Nepal presented to the Department of Dermatology with complaints of an abrupt onset of an asymptomatic cutaneous eruption involving the neck and both the forearms since the past 5 days. The lesions were smaller earlier which had progressively increased in size over the past 5 days to reach the current status. There were no associated constitutional symptoms and no history of contact with cattle or sheep. He was not receiving any other medications. There were no associated comorbidities. On inspection, papules and plaques of varying sizes with a striking central umbilication were identified involving the forearms and neck that gave an illusion of vesiculation [Figures 1–3]. Some of the lesions over the neck had a crust overlying the depressed center [Figures 4 and 5]. On palpation, these lesions were firm and nontender. Gram staining of the tissue obtained from one of the papules after needle extirpation was inconclusive. A skin biopsy from these lesions showed absence of epidermal changes with a dense inflammatory neutrophilic dermal infiltrate along with dermal edema as the hallmark finding, without evidence of vasculitis [Figures 6–8]. Laboratory parameters revealed a hemoglobin level of 14 g/dl, a total white blood cell count of 13,000 cells/mm3 with 89% neutrophils, and a normal peripheral smear. His renal and hepatic profiles were normal, and imaging studies of the abdomen and pelvis were insignificant. A urine analysis for Bence-Jones protein was negative. A throat swab culture only grew normal throat flora. With these findings, the patient was diagnosed as SS and started on 20 mg of Prednisolone once daily for 2 weeks and 100 mg of dapsone once at bedtime for 2 weeks. Patient was asked to follow-up after 2 weeks. However, the patient was lost to follow-up.
Figure 1.

Fleshy pseudovesicles with central umbilication seen on the right forearm of our patient
Figure 3.

Molluscoid pseudovesicles over the nape of the neck
Figure 4.

Juicy plaques with a central depression and an overlying crust seen on the right side of the neck
Figure 5.

Similar lesions on the left side of the neck as seen in Figure 4. To note here again, is the striking symmetric distribution of the nuchal lesions
Figure 6.
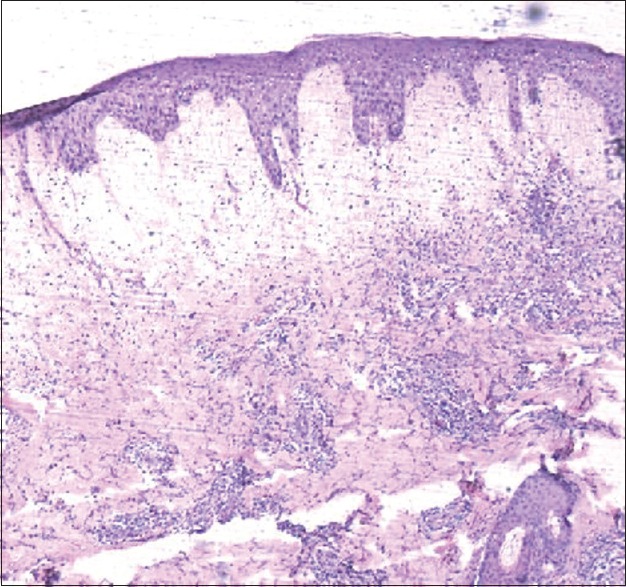
Section of the plaque on the right forearm demonstrating dermal edema and a dense dermal inflammatory infiltrate (H and E, ×10)
Figure 8.

Absence of vasculitis on microscopy (H and E, ×40)
Figure 2.

Over the left forearm, a plaque with the characteristic central umbilication seen, closely mimicking the lesions encountered in molluscum contagiosum. Furthermore, to note here is the symmetric pattern of lesion arrangement
Figure 7.

Same section showing a dense inflammatory infiltrate composed of neutrophils around the blood vessels and also diffusely distributed (H and E, ×20)
Discussion
Sweet's syndrome is the prototypical neutrophilic dermatosis, generally characterized by fever, an increase in the neutrophilic count along with tender pseudovesicles distributed over the body in an asymmetric manner.[2,3] Etiologically, three types of SS have been described, namely the idiopathic, paraneoplastic, and the drug-induced type of SS.[4] As mentioned earlier, localized SS is a very rare manifestation of the disease. There have, however, been reports of the occurrence of SS localized to specific sites of the body though, some of which have presented with very unusual morphologic patterns, as shown by Sommer et al.[5] who described palmoplantar pustulosis as the sole finding in a SS patient, Verma et al.[6] demonstrating the occurrence of SS confined to the photo exposed sites alone, Verma[7] who elucidated a rare recurrent bullous eruption localized to the flexural aspect of both the forearms in a SS patient and Brechtel et al.[8] who reported a localized facial presentation of SS manifesting as an inflammatory lesion with a central depression superimposed with several pustules on the surface of the plaque. A variant of SS referred to as neutrophilic dermatosis of the dorsal hands (NDDH) is a specific entity confined only to the dorsa of the hands and has been extensively reviewed in literature by Galaria et al.,[9] Takahama and Kanbe,[10] Cook et al.,[11] Baz et al.,[12] and Walling et al.[13] NDDH usually presents as edematous and violaceous plaques and papulonodules on the radial aspect of the dorsal surface of both hands. Another localized presentation of SS has been described by Bubna et al.[14] wherein pseudovesicles restricted to the palms and soles alone, was described. Our patient presented with molluscoid pseudovesicles distributed over the neck and forearms only, which is a very rare morphologic pattern witnessed in SS and to the best of our knowledge has not been previously described. Second, our patient lacked the usual constitutional symptoms that herald SS, which made the diagnosis a challenge. Third, as no systemic association with SS could be identified in our patient, he was further sub-classified as a case of idiopathic SS, which again is a rarity in male patients, who usually present with the paraneoplastic or the drug-induced variant of SS. The hallmark finding in our patient was the central depression in all the pseudovesicles examined. The other possibilities, we kept in mind after clinically examining our patient, were, atypical erythema multiforme, histioid leprosy,[15] milker's nodule, cowpox, and ecthyma contagiosum, but these were eventually ruled out. Hence, to conclude, we see that SS is a dermatosis that could be a great mimicker just like leprosy and syphilis and therefore when faced with diagnostic dilemmas in these kinds of atypical presentations, it would be worthwhile considering SS as a differential diagnosis.
What is new?
Idiopathic Sweet's syndrome (SS) may even occur in males though highly uncommon
The absence of constitutional symptoms does not necessarily rule out the diagnosis of SS
The plaques encountered in SS could even be asymptomatic.
Molluscoid lesions seen in SS is a very rare morphologic pattern encountered and to the best of our knowledge is being reported for the 1st time in literature
Localized patterns of SS are not so rare as previously thought.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Cohen PR, Kurzrock R. Sweet's syndrome revisited: A review of disease concepts. Int J Dermatol. 2003;42:761–78. doi: 10.1046/j.1365-4362.2003.01891.x. [DOI] [PubMed] [Google Scholar]
- 2.Sweet RD. Acute febrile neutrophilic dermatosis-1978. Br J Dermatol. 1979;100:93–9. doi: 10.1111/j.1365-2133.1979.tb03573.x. [DOI] [PubMed] [Google Scholar]
- 3.Cohen PR, Almeida L, Kurzrock R. Acute febrile neutrophilic dermatosis. Am Fam Physician. 1989;39:199–204. [PubMed] [Google Scholar]
- 4.Cohen PR. Sweet's syndrome – A comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:34. doi: 10.1186/1750-1172-2-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sommer S, Wilkinson SM, Merchant WJ, Goulden V. Sweet's syndrome presenting as palmoplantar pustulosis. J Am Acad Dermatol. 2000;42:332–4. doi: 10.1016/s0190-9622(00)90105-1. [DOI] [PubMed] [Google Scholar]
- 6.Verma R, Vasudevan B, Pragasam V, Mitra D. Unusual Presentation of Idiopathic Sweet's Syndrome in a photodistributed pattern. Indian J Dermatol. 2014;59:186–9. doi: 10.4103/0019-5154.127682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Verma SB. Recurrent bilaterally symmetrical bullous Sweet's Syndrome: A rare and confusing entity. Indian J Dermatol. 2012;57:483–5. doi: 10.4103/0019-5154.103070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brechtel B, Haas N, Czarnetzki BM. Localized Sweet syndrome. Hautarzt. 1994;45:858–60. doi: 10.1007/s001050050186. [DOI] [PubMed] [Google Scholar]
- 9.Galaria NA, Junkins-Hopkins JM, Kligman D, James WD. Neutrophilic dermatosis of the dorsal hands: Pustular vasculitis revisited. J Am Acad Dermatol. 2000;43:870–4. doi: 10.1067/mjd.2000.109286. [DOI] [PubMed] [Google Scholar]
- 10.Takahama H, Kanbe T. Neutrophilic dermatosis of the dorsal hands: A case showing HLA B54, the marker of Sweet's syndrome. Int J Dermatol. 2010;49:1079–80. doi: 10.1111/j.1365-4632.2009.04422.x. [DOI] [PubMed] [Google Scholar]
- 11.Cook E, Epstein R, Miller R. A rare case of idiopathic neutrophilic dermatosis of the hands. Dermatol Online J. 2011;17:11. [PubMed] [Google Scholar]
- 12.Baz K, Yazici AC, Kaya TI, Ikizoglu G, Ulubas B, Apa DD, et al. Neutrophilic dermatosis of the hands (localized Sweet's syndrome) in association with chronic hepatitis C and sarcoidosis. Clin Exp Dermatol. 2003;28:377–9. doi: 10.1046/j.1365-2230.2003.01299.x. [DOI] [PubMed] [Google Scholar]
- 13.Walling HW, Snipes CJ, Gerami P, Piette WW. The relationship between neutrophilic dermatosis of the dorsal hands and sweet syndrome: Report of 9 cases and comparison to atypical pyoderma gangrenosum. Arch Dermatol. 2006;142:57–63. doi: 10.1001/archderm.142.1.57. [DOI] [PubMed] [Google Scholar]
- 14.Bubna AK, Veeraraghavan M, Anandan S, Rangarajan S. Palmoplantar pseudovesicles: An unusual presentation of Sweet's Syndrome. Indian J Dermatol. 2015;60:94–6. doi: 10.4103/0019-5154.147819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ghorpade A. Molluscoid skin lesions in histoid leprosy with pseudo-isomorphic Koebner phenomenon. Int J Dermatol. 2008;47:1278–80. doi: 10.1111/j.1365-4632.2008.03836.x. [DOI] [PubMed] [Google Scholar]