

Abstract
Purpose:
Highly active antiretroviral therapy has significantly extended survival of human immunodeficiency virus (HIV) infected patients. These drugs suppress replication of HIV but at the same time, have many physical and mental side effects which may affect daily activities of the patients. The present study assessed if moderate intensity exercise program helped in enhancing the physical fitness and quality of life (QoL) in HIV positive females which may reduce the comorbidities associated with the disease and medications.
Aim and Objectives:
The aim of this study is to study the effects of moderate intensity physical training on physical fitness parameters and QoL in HIV positive females.
Methodology:
Post IEC approval, a randomized control, single-blinded, parallel group trial was conducted on 55 females (20 experimental HIV, 20 control HIV, 15 control normal) matching the selection criteria. Post informed consent, their muscular endurance, flexibility, aerobic capacity, and QoL was assessed. Moderate intensity physical exercises were given to experimental HIV and control normal 5 days/week for 8 weeks and subjects were reassessed for above parameters. Intragroup analysis was performed using paired t-test while inter-group was by one-way ANOVA with alpha set at ≤0.05.
Results:
Moderate-intensity exercises improved muscular endurance (P < 0.05), flexibility (P < 0.05), and aerobic capacity (P < 0.05)in experimental HIV and control normal group as compared to control HIV group. QoL in experimental HIV showed improvement in all the domains.
Conclusion:
Moderate-intensity exercises help improve the physical fitness as well as enhance the QoL in HIV positive females.
Key words: Endurance, human immunodeficiency virus, moderate intensity exercise, muscular strength, physical fitness, quality of life, VO2 max
INTRODUCTION
Human immunodeficiency virus (HIV) has become a serious health, economic, and social problem with 35.3 million people living with HIV globally and 2.6 million people only in India till the year 2012.[1,2,3,4] The first case of HIV in India was found in 1986 in a female sex worker of Calcutta.[2] Although the incidence of HIV infection was more among men, in the beginning, it is increasing in females as well.[3,4] Nowadays, patient with HIV/AIDS are increasing in number, partly due to improved screening, earlier diagnosis, better treatment methods such as antiretroviral therapy (ART), especially highly active ART (HAART), which has enhanced life span of HIV infected patient.[5,6,7] At the same time, there are many side effects associated with HAART.[8,9] Individuals infected with HIV and on HAART experience numerous co-morbidities such as muscle pain, fatigue joint pain, lack of sleep (insomnia), depression, dementia, lipodystrophy affecting multiple systems including the musculoskeletal, neurological and cardiorespiratory systems.[4,7,8,9,10] These symptoms affect their health and physical fitness which is necessary to perform day-to-day activities. Because of these symptoms, persons living with HIV experience a number of impairments, activity limitations, and participation restrictions, which affects their overall quality of life (QOL).[7,11,12,13,14] HIV infections are spreading in women continuously with almost 39% of females being infected by it.[14] There are biological, social, cultural, economical, political and legal factors, which make women more prone to the stigma and discrimination. Sometimes, women are prevented from learning about or using safer sex techniques. This leads to increase in the percentage of HIV among women.[15,16]
In India, women are considered the backbone of the home and the society. In the lower socioeconomic level of society, women do more hazardous manual labor than men which requires optimal fitness. While there are many newer avenues in the treatment of females infected with HIV,[11,17,18] there are few studies available to look at benefits of treatment on the physical function and capacity of these patients. Very little literature is available wherein aspects of treatment of HIV-induced population, other than their mere survival, are looked at. However, survival does not mean that the patient with HIV is merely alive, but what is equally important, is that it should look at aspects of physical and mental functioning as well as a sense of satisfaction of living. The purpose of the present study was to assess the effect of fitness training on improvement of fitness parameters and QoL in HIV positive females.
METHODOLOGY
A randomized, single-blinded, double control, parallel group trial was conducted post-Institutional Ethical Committee and University Postgraduate Research committee approval. Sample size was calculated using Sample size = (t value)2 × p × (1− p)/c where t value = 1.96 (95% confidence interval), P = 0.5 (% of getting picked), c = class interval. The sample size for the study was calculated by an effect size of 1.2 considering the aerobic capacity (VO2 Max) as the primary dependent outcome measure and was estimated at 16 per group for both the HIV groups. 72 females, who were diagnosed as being HIV positive, were approached through government hospitals and non-governmental organizations. The procedure of the study was explained to them. The study was conducted on 55 females (20 experimental HIV, 20 control HIV, 15 control normal) who were willing to participate. The 40 HIV positive females were of age group between 20 and 40 years, taking ART for 2–5 years, asymptomatic for any musculoskeletal or cardiovascular disease. Post informed consent from the participants, their muscular endurance, flexibility, aerobic capacity, and QoL were assessed. The HIV positive females were divided into two groups by random number table allocation method as Interventional HIV experimental group (Group 1) and noninterventional HIV control group (Group 2) by the 2nd investigator [Figure 1]. The 15 normal controls were healthy females; matched to Group 1 from the normal population, and was recruited for the Interventional normal control group (Group 3).
Figure 1.
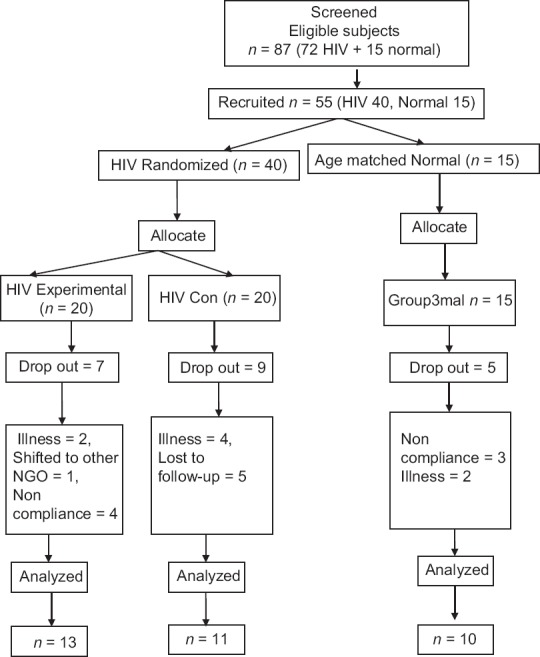
Consort flowchart
The baseline fitness parameters such as flexibility, muscular strength endurance, aerobic capacity (VO2 max) were assessed using sit and reach test,[19] push-ups, curl-ups[20,21] and squats test and shuttle run test[22,23] [Figures 2a, b, 3a, b, 4a, b and 5], respectively, by investigator 2. QoL was measured by using WHO-HIVQOL-BREF for Group 1 and 2 and WHOQOLBREF was used Group 3.[24] Group 1 and 3 were given moderate intensity exercise, that is, 50%–70% of VO2 max by investigator 1 which was at 5/10 level of the modified Borg scale, for 30 min a day, 5 days a week for 8 weeks.[25] Group 2 was not given any exercises and were advised to continue their routine level of daily tasks and activities. No activities of daily livings (ADL's) or diet modifications were advised to any groups.
Figure 2.

(a) Sit and reach test start position, (b) sit and reach end position
Figure 3.

(a) Push up start position, (b) push up end position
Figure 4.

(a) Curl up start position, (b) curl up end position
Figure 5.

Squats
Exercise protocol for Group 1 and 3 included following components:
-
WARM UP (Total time 5 min)[25]
Stretching of large muscle groups.15 s hold 5 repetitions.
Conditioning (total 20 min): Brisk walking of 50%–70% of VO2 max, push-ups, curl-ups and squats
Cool-down (5 min): Stretching of large muscle groups. Same as warm up.
Figure 6.

Paschimottanasan
Figure 7.

Bhujangasan
Figure 8.

Dhanurasan
Post 8 weeks intervention and completion of the recruited subjects, the time bound trial was terminated, and the above-mentioned parameters of Physical Fitness and QoL were reassessed.[27]
Statistical analysis
The obtained data were analyzed using Microsoft Excel 2007. Paired t-test was used for intragroup analysis and one-way ANOVA with single variable was used to compare between all three groups. α was set at P < 0.05 and power of the study (1-β) at 0.95. QoL was analyzed directly from the online software, and no other analysis was used for the same.[24]
RESULTS
From the Group 1, there were 7 dropouts (2 due to medical illness, 1 due to shifting and 4 due to low compliance) and thus 13 completed the study. In Group 2, there were 9 dropouts (4 due to illness and 5 were lost to follow-up), and thus 11 completed the study. In Group 3, there were 5 dropouts. No adverse reaction to exercise prescription was noted in any of the groups.
An improvement in the physical fitness was observed in both the HIV experimental and Normal control groups, whereas the HIV control group did not show any improvement at all, but in fact, possible disease-related deterioration was observed [Table 1].
Table 1.
Comparison between different groups for physical fitness parameters

The HIV positive experimental group showed an improvement in all the QoL parameters as compared to the HIV positive control group [Table 2].
Table 2.
Comparison between different groups for quality of life parameters

DISCUSSION
This study investigated the effect of equal moderate intensity fitness training on physical fitness parameters (muscular strength endurance, flexibility, aerobic capacity (VO2 peak) and QOL in HIV positive females and compared it with those of the normal females to check for the occurrence of exercises related benefits on health and QoL on both the groups.
According to Table 1, there is a significant increase in number of push-ups, curl ups, and squats performed in 1 min in Group 1 and Group 3 followed by 8 weeks of physical training. A normal human skeletal muscle undergoes an adaptive increase in mitochondrial enzyme level and the ability to oxidize pyruvate in response to endurance training.[28] Regularly performing endurance exercise induces major adaptations in skeletal muscle, as a result of the increase in mitochondria. The major metabolic consequences of the adaptations of muscle to endurance exercise are a slower utilization of muscle glycogen and blood glucose.[29] Endurance training also influences the enzyme system of the Krebs cycle electron transport chain, capillary supply, changes in key metabolic enzymes involved in fatty acid activation, and increased oxygen uptake in skeletal muscle and less lactate production during exercise of a given intensity.[30] It has also showed increase branching of neuromuscular synapse in normal individuals. These adaptations play an important role in the large increase in the ability to perform prolonged strenuous exercise that occurs in response to endurance exercise training. Exercise training seems to be mediated via peroxisome proliferators-activated receptor (PPAR)-co-activator (PGC-1α). Increased muscular activity induces PGC-1α production, which, in turn, protects skeletal muscle from atrophy by suppressing gene FoxO3 action and atrophy-specific gene transcription. In addition, muscle progenitor cell number and activity as measured by the amounts of MyoD, myogenin, and mRNAs, were increased.[30,31] Thus, moderate intensity exercising definitely offers benefits of strength and endurance enhancement in HIV-positive patients. In ART-associated complications, HIV-positive patients have to undergo premature aging.[29,31] A study carried out by Kusko et al., found that gene expression changes and phenotypic in muscle in an HIV model similar to that seen in aging.[32] There is an up regulation of genes associated with aging muscle prematurely expressed.[31] Hence, there is a reduction on muscle strength and endurance in Group 2.
Flexibility of the muscle gives good range of movement at joint and prevents it from musculoskeletal injuries. The stretch receptors located in the tendons (Golgi tendon organs) are sensitive to tension and prevent overstretching in the opposite way to the stretch reflex. An increase in tension from either a large muscle contraction or overstretching activates the Golgi tendon organ receptors, which, via the inverse stretch reflex, inhibit muscle contraction and induce relaxation. Thus, these receptors prevent the muscle from contracting in a way that damages itself.[33] A study done by Taylor et al. suggests that muscles and tendons also act viscoelastically in response to stretch.[34] Viscous properties are time or rate-change dependent, where the rate of deformation is directly proportional to the applied force and to the time of force application. This property is known as viscoelasticity. Therefore, stretching a muscle or group of muscles seems to induce muscle relaxation via either the inverse stretch reflex or the inherent viscoelastic property of the muscle.[35] In the present study, warm-up period of 10 min included stretching of larger muscle groups, hamstring, quadriceps, abdominals for 15 s hold and 5 repetitions.[35] According to Table 1, participants from experimental HIV and experimental normal both showed improved flexibility after the intervention of 8 weeks of stretching. This can be because of the immediate lengthening gained from stretching which is mostly temporary and can be accredited to transitory sarcomeric lengthening (actin/myosin) complex relaxation.[36] Other factors may have contributed to the changes observed, such as Golgi tendon organs and muscle spindle adaptation and increased stretched tolerance which may have allowed long-term effect of stretching leads to maintenance of the same.[37] HIV positive patients undergo muscle wasting because of cysteine glutamine imbalance and many others pathologies. This can lead to muscle weakness and may go shortness. This can be the reason for the deterioration in Group 2 which did not get any exercise program.
Aerobic fitness not only determines performance in a wide range of activities, but it is also a health parameter. Walking is the most accessible and easily regulated exercise that can enhance health and cardiorespiratory function.[38] Therefore, in this study, brisk walking at 2.4 mph for 20–30 min was given. As seen in Table 1, there is an improvement in VO2 peak in Group3. Free radicals are by-products of aerobic metabolism. They cause mild oxidative stress, which can act as a stimulant of physiological antioxidant systems and as a trigger for various physiological adaptations. Exercise training improves arterial compliance, baroreflex sensitivity, and autonomic profile in HIV positive individuals as well as reduces the traditional risk factors for cardiac disease.[38,39] A study done by Parker et al. in 1996 showed that there is an increase in functional capacity by 40% in cardiac rehab patient followed by 8 weeks of moderate endurance training.[40] The same effects could be considered even for HIV positive people. As seen earlier there are premature aging in HIV-positive patients. This may show effects of aging on cardiovascular system of HIV positive patients, like reduced aerobic capacity, increased energy expenditure. Therefore, Group 2 did not show significant improvement in VO2 max.
There is a significant improvement in physical domain score of Group 1 and Group 3 as compared to Group 2 [Table 2] This is probably because of improvement of muscular endurance and strength which has reduced their physical discomfort, pain, and fatigue. This might have improved their overall functional capacity.
There is an improvement in psychological domain in Group 1 and Group 3 which may be because of release of enkephalins, beta-endorphin, or other neuropeptides by the nervous system during exercise, which may help in relieving stress and depression.[41]
Level of independence domain showed more improvement in experimental groups as compared to control group. Level of independence includes mobility, ADL, dependence on medication or treatments and work capacity. This might be because of improved physical fitness to perform ADL efficiently.[42] There is an improvement in social relationship domain in Group 1. This is probably because it was a group therapy session, where they got an opportunity to come together interact with each other and improve and discuss their problems. This might improve their interpersonal relationship and social relationship. Group 2 also showed slight improvement in the same domain this is because of counseling session which was common for both the groups. Spiritual/religious/personal beliefs domain in WHOQOLHIV BREF questionnaire measured the spiritual, religious, and personal beliefs of the persons living with HIV. Positive attitude toward the life has improved in experimental group. This was observed probably because of group therapy that was imparted to the females, where the women in this study used to come together as leisure activity. Because of these activities, they started getting time to meet people, interact with them share their ideas and add-on to their available knowledge. They started planning recreational activities post session. There was an improvement in overall QOL score in Group 1 and Group 3 as a result of improved score in all the domains.[43]
There may be variations within the HIV positive groups and the normal group in regards to their socioeconomic statuses, lifestyles, and nutritional statuses, which was not considered in the present study. There were alterations in the choice of use of footwear in the Groups 1 and 2, including the choice of not wearing footwear during the testing of VO2 max. No uniformity could be made in this by the investigators due to ethical and economic issues involved.
CONCLUSION
Thus, the authors conclude that moderate intensity exercises for 8 weeks, 5 days week for 30 min does help to improve physical fitness parameters and enhance the QOL in HIV positive females and strongly recommend that exercises should be made a predominant part of HIV treatment program along with the HAART therapy.[44,45] Although the authors used walking as an aerobic exercise and push-ups, squats and curl-ups as anaerobic exercises, involvement in any form of supervised moderate-intensity exercises or activities including walking, swimming, cycling, strengthening by interval, suryanamaskar (Sun Salutation) training or circuit training would be beneficial.[46] Moderate-intensity exercises can gain not just a good physical fitness,[47] but can also enhance the QoL of a HIV-positive person[48] and make their life worth living because just surviving with HIV medications is not enough.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.UNAIDS Report on the Global AIDS Epidemic. 2013. [Last viewed on 2016 Jul 07]. Available from: http://www.files.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf .
- 2.Lakhashe S, Thakar M, Godbole S, Tripathy S, Paranjape R. HIV infection in India: Epidemiology, molecular epidemiology and pathogenesis. J Biosci. 2008;33:515–25. doi: 10.1007/s12038-008-0070-3. [DOI] [PubMed] [Google Scholar]
- 3.UNAIDS and WHO Epidemiological Fact Sheet on HIV/AIDS and Sexually Transmitted Diseases (India) [Last viewed on 2016 Jul 07]. Available from: http://www.data.unaids.org/publications/fact-sheets01/india_en.pdf .
- 4.Stanley S, Sethuramalingam V, Sathia S. Life Satisfaction and Pessimism in HIV positive people: A comparative study from India. Int J Psychosoc Rehabil. 2013;18:95–104. [Google Scholar]
- 5.Stages of HIV. U.S. Department of Health & Human Services. Revised 27 August, 2015. [Last viewed on 2016 Jul 07]. Available from: https://www.aids.gov/hiv-aids-basics/just-diagnosed-with-hiv-aids/hiv-in-your-body/stagesof-hiv/
- 6.WHO. Operations Manual for Staff at Primary Health Care Centres. [Last viewed on 2016 Jul 07]. Available from: http://www.who.int/hiv/pub/imai/om_appendix.pdf .
- 7.Kalra S, Kalra B, Agrawal N, Unnikrishnan A. Understanding diabetes in patients with HIV/AIDS. Diabetol Metab Syndr. 2011;3:2. doi: 10.1186/1758-5996-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Montessori V, Press N, Harris M, Akagi L, Montaner JS. Adverse effects of antiretroviral therapy for HIV infection. CMAJ. 2004;170:229–38. [PMC free article] [PubMed] [Google Scholar]
- 9.Havlir DV, Currier JS. Complications of HIV disease and antiretroviral therapy. Top HIV Med. 2006;14:27–35. [PubMed] [Google Scholar]
- 10.Hand GA, Lyerly GW, Jaggers JR, Dudgeon WD. Impact of aerobic and resistance exercise on the health of HIV-infected persons. Am J Lifestyle Med. 2009;3:489–499. doi: 10.1177/1559827609342198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.O'Brien K, Nixon S, Tynan AM, Glazier R. Aerobic exercise interventions for adults living with HIV/AIDS. Cochrane Database Syst Rev. 2010 Aug 4;8:CD001796. doi: 10.1002/14651858.CD001796.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anand D, Puri S, Mathew M. Assessment of quality of life of HIV-positive people receiving ART: An Indian Perspective. Indian J Community Med. 2012;37:165–9. doi: 10.4103/0970-0218.99918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wig N, Lekshmi R, Pal H, Ahuja V, Mittal CM, Agarwal SK. The impact of HIV/AIDS on the quality of life: A cross sectional study in north India. Indian J Med Sci. 2006;60:3–12. [PubMed] [Google Scholar]
- 14.Basu I, Jana S, Rotheram-Borus MJ, Swendeman D, Lee SJ, Newman P, et al. HIV prevention among sex workers in India. J Acquir Immune Defic Syndr. 2004;36:845–52. doi: 10.1097/00126334-200407010-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sharma A, Shah S, Marfatia YS. Discrimination faced by HIV positive females. Indian J Sex Transm Dis. 2005;26:70–2. [Google Scholar]
- 16.Paudel V, Baral KP. Women living with HIV/AIDS (WLHA), battling stigma, discrimination and denial and the role of support groups as a coping strategy: A review of literature. Reprod Health. 2015;12:53. doi: 10.1186/s12978-015-0032-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hand GA, Phillips KD, Dudgeon WD, William Lyerly G, Larry Durstine J, Burgess SE. Moderate intensity exercise training reverses functional aerobic impairment in HIV-infected individuals. AIDS Care. 2008;20:1066–74. doi: 10.1080/09540120701796900. [DOI] [PubMed] [Google Scholar]
- 18.O'Brien K, Nixon S, Glazier RH, Tynan AM. Progressive resistive exercise interventions for adults living with HIV/AIDS. Cochrane Database Syst Rev. 2004 Oct 18;4:CD004248. doi: 10.1002/14651858.CD004248.pub2. [DOI] [PubMed] [Google Scholar]
- 19.López-Miñarro PA, Andújar PS, Rodrñguez-Garcña PL. A comparison of the sit-and-reach test and the back-saver sit-and-reach test in university students. J Sports Sci Med. 2009;8:116–22. [PMC free article] [PubMed] [Google Scholar]
- 20.Diener MH, Golding LA, Diener D. Validity and reliability of a one-minute half sit-up test of abdominal muscle strength and endurance. Sports Med Train Rehab. 1995;6:105–19. [Google Scholar]
- 21.Faulkner RA, Sprigings EJ, McQuarrie A, Bell RD. A partial curl-up protocol for adults based on an analysis of two procedures. Can J Sport Sci. 1989;14:135–41. [PubMed] [Google Scholar]
- 22.Vaara JP, Kyröläinen H, Niemi J, Ohrankämmen O, Häkkinen A, Kocay S, et al. Associations of maximal strength and muscular endurance test scores with cardiorespiratory fitness and body composition. J Strength Cond Res. 2012;26:2078–86. doi: 10.1519/JSC.0b013e31823b06ff. [DOI] [PubMed] [Google Scholar]
- 23.Léger LA, Lambert J. A maximal multistage 20-m shuttle run test to predict VO2 max. Eur J Appl Physiol Occup Physiol. 1982;49:1–12. doi: 10.1007/BF00428958. [DOI] [PubMed] [Google Scholar]
- 24.Skevington SM, Lotfy M, O'Connell KA. WHOQOL Group. The World Health Organization's WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00. [DOI] [PubMed] [Google Scholar]
- 25.Whaley MH, Brubaker PH, Otto RM, Armstrong LE. ACSM's Guidelines for Exercise Testing and Prescription. 7th ed. Philladelphia: Lippincott Williams and Wilkins; 2006. [Google Scholar]
- 26.Ross A, Thomas S. The health benefits of yoga and exercise: A review of comparison studies. J Altern Complement Med. 2010;16:3–12. doi: 10.1089/acm.2009.0044. [DOI] [PubMed] [Google Scholar]
- 27.Gomes-Neto M, Conceição CS, Oliveira Carvalho V, Brites C. A systematic review of the effects of different types of therapeutic exercise on physiologic and functional measurements in patients with HIV/AIDS. Clinics (Sao Paulo) 2013;68:1157–67. doi: 10.6061/clinics/2013(08)16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nieman DC, Johanssen LM, Lee JW, Arabatzis K. Infectious episodes in runners before and after the Los Angeles Marathon. J Sports Med Phys Fitness. 1990;30:316–28. [PubMed] [Google Scholar]
- 29.Roubenoff R, Skolnik PR, Shevitz A, Snydman L, Wang A, Melanson S, et al. Effect of a single bout of acute exercise on plasma human immunodeficiency virus RNA levels. J Appl Physiol. 1999;86:1197–201. doi: 10.1152/jappl.1999.86.4.1197. [DOI] [PubMed] [Google Scholar]
- 30.Holloszy JO, Coyle EF. Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J Appl Physiol Respir Environ Exerc Physiol. 1984;56:831–8. doi: 10.1152/jappl.1984.56.4.831. [DOI] [PubMed] [Google Scholar]
- 31.Dröge W, Holm E. Role of cysteine and glutathione in HIV infection and other diseases associated with muscle wasting and immunological dysfunction. FASEB J. 1997;11:1077–89. doi: 10.1096/fasebj.11.13.9367343. [DOI] [PubMed] [Google Scholar]
- 32.Kusko RL, Banerjee C, Long KK, Darcy A, Otis J, Sebastiani P, et al. Premature expression of a muscle fibrosis axis in chronic HIV infection. Skelet Muscle. 2012;2:10. doi: 10.1186/2044-5040-2-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Smith CA. The warm-up procedure: To stretch or not to stretch. A brief review. J Orthop Sports Phys Ther. 1994;19:12–7. doi: 10.2519/jospt.1994.19.1.12. [DOI] [PubMed] [Google Scholar]
- 34.Taylor DC, Dalton JD, Jr, Seaber AV, Garrett WE., Jr Viscoelastic properties of muscle-tendon units. The biomechanical effects of stretching. Am J Sports Med. 1990;18:300–9. doi: 10.1177/036354659001800314. [DOI] [PubMed] [Google Scholar]
- 35.Knudson D. The biomechanics of stretching. J Exerc Sci Physiother. 2006;2:3–12. [Google Scholar]
- 36.Garrett WE, Jr, Califf JC, Bassett FH., 3rd Histochemical correlates of hamstring injuries. Am J Sports Med. 1984;12:98–103. doi: 10.1177/036354658401200202. [DOI] [PubMed] [Google Scholar]
- 37.Nelson RT, Bandy WD. Eccentric training and static stretching improve hamstring flexibility of high school males. J Athl Train. 2004;39:254–258. [PMC free article] [PubMed] [Google Scholar]
- 38.Golbidi S, Laher I. Exercise and the cardiovascular system. Cardiol Res Pract. 2012;2012:210852. doi: 10.1155/2012/210852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Dudgeon WD, Phillips KD, Bopp CM, Hand GA. Physiological and psychological effects of exercise interventions in HIV disease. AIDS Patient Care STDS. 2004;18:81–98. doi: 10.1089/108729104322802515. [DOI] [PubMed] [Google Scholar]
- 40.Parker ND, Hunter GR, Treuth MS, Kekes-Szabo T, Kell SH, Weinsier R, et al. Effects of strength training on cardiovascular responses during a submaximal walk and a weight-loaded walking test in older females. J Cardiopulm Rehabil. 1996;16:56–62. doi: 10.1097/00008483-199601000-00007. [DOI] [PubMed] [Google Scholar]
- 41.Howlett TA, Tomlin S, Ngahfoong L, Rees LH, Bullen BA, Skrinar GS, et al. Release of beta endorphin and met-enkephalin during exercise in normal women: Response to training. Br Med J (Clin Res Ed) 1984;288:1950–2. doi: 10.1136/bmj.288.6435.1950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Bopp CM, Phillips KD, Fulk LJ, Hand GA. Clinical implications of therapeutic exercise in HIV/AIDS. J Assoc Nurses AIDS Care. 2003;14:73–8. doi: 10.1177/1055329002239192. [DOI] [PubMed] [Google Scholar]
- 43.Ciccolo JT, Jowers EM, Bartholomew JB. The benefits of exercise training for quality of life in HIV/AIDS in the post-HAART era. Sports Med. 2004;34:487–99. doi: 10.2165/00007256-200434080-00001. [DOI] [PubMed] [Google Scholar]
- 44.Dolan SE, Frontera W, Librizzi J, Ljungquist K, Juan S, Dorman R, et al. Effects of a supervised home-based aerobic and progressive resistance training regimen in women infected with human immunodeficiency virus: A randomized trial. Arch Intern Med. 2006;166:1225–31. doi: 10.1001/archinte.166.11.1225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Mendes EL, Andaki AC, Amorim PR, Natali AJ, Brito CJ, Paula SO. Physical training for HIV positive individuals submitted to HAART: Effects on anthropometric and functional parameters. [Last cited on 2016 Aug 12];Rev Bras Med Esporte. 2013 19:16–21. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=s1577-86922013000100003&ing=en . [Google Scholar]
- 46.Vaiyapuri A, Ivor P, Jagatheesan A, Rajendran K. Effect of progressive resistance training on functional capacity, quality of life and CD4 count in people with HIV/AIDS. Int J Physiother Res. 2014;2:626–30. [Google Scholar]
- 47.Smith BA, Neidig JL, Nickel JT, Mitchell GL, Para MF, Fass RJ. Aerobic exercise: Effects on parameters related to fatigue, dyspnea, weight and body composition in HIV-infected adults. AIDS. 2001;15:693–701. doi: 10.1097/00002030-200104130-00004. [DOI] [PubMed] [Google Scholar]
- 48.Mutimura E, Stewart A, Crowther NJ, Yarasheski KE, Cade WT. The effects of exercise training on quality of life in HAART-treated HIV-positive Rwandan subjects with body fat redistribution. Qual Life Res. 2008;17:377–85. doi: 10.1007/s11136-008-9319-4. [DOI] [PMC free article] [PubMed] [Google Scholar]