

Abstract
Background and Objective:
To compare pneumatic retinopexy and scleral buckle for repair of primary rhegmatogenous retinal detachment.
Patients and Methods:
Retrospective analysis of 90 patients undergoing surgery for primary rhegmatogenous retinal detachment, with 46 patients undergoing pneumatic retinopexy (PR) compared with 44 patients undergoing scleral buckle procedure (SBP).
Results:
Both groups had similar baseline characteristics. Single surgery reattachment rate was 95.5% with SBP and 67% with PR (p=0.00057). Final reattachment rate was 100% with SBP and 97.8% with PR. A final visual acuity of 20/40 or better occurred in 89% with SBP and 72% with PR (p = 0.04). PR and SBP had a similar mean visual acuity if the primary procedure were successful, whereas those patients with unsuccessful PR had lower mean final acuities.
Conclusion:
This study demonstrates that SBP has a significantly higher rate of single surgery reattachment rate than PR along with improved final visual acuity. Initial success of PR may be an important predictor of final visual outcome.
Keywords: Primary rhegmatogenous retinal detachment, Retinal detachment, Pneumatic retinopexy, Scleral buckle
Background and Objective
Scleral buckling procedure (SBP) was pioneered by Charles Schepens in 1957 and revolutionized our treatment of patients with retinal detachment.1 In comparison to the 30–40% success rates initially reported by Gonin,2 scleral buckling has been reported to result in anatomic reattachment in up to 94% of uncomplicated retinal detachment cases.3 The surgery also offers significant longevity, with anatomic success lasting 20 years or more in the large majority of cases.4
Pneumatic retinopexy was introduced by Hilton and Grizzard in 1986. Pneumatic retinopexy allows surgeons to potentially avoid some of the difficulties associated with scleral buckling for select retinal detachments, including the need to go to the operating room, patient discomfort, and surgical complications such as diplopia.5,6 Initially, pneumatic retinopexy (PR) was advanced as a treatment option for uncomplicated, phakic superior detachments resulting from either singular breaks, or multiple breaks residing within a single clock-hour of the fundus, without proliferative vitreoretinopathy (PVR). Reported success rates have been variable and dependent upon patient selection, particularly for the treatment of inferior or more complex detachments.7,8
Limited studies have compared pneumatic retinopexy to scleral buckling in the primary treatment of retinal detachment. PR has gained popularity among retinal surgeons over the years,9,10 yet controversy still exists regarding its appropriate application. Selective inclusion criteria in the first retrospective study of PR may have contributed to a relatively high 91% success rate compared with subsequent studies.11 Recent uncontrolled retrospective studies have reported primary anatomic success rates of 54 – 83%, with final anatomic success rates of 98 – 100% of cases including subsequent reoperations.12,13,14 Studies comparing PR to SBP have demonstrated similar variability, with one study reporting lower rates of reattachment for PR,15 and another recent comparative study showing equivalent final anatomic and visual results.16 One large randomized controlled trial demonstrated final success rates that compared favorably to scleral buckling.17 A Cochrane review and meta-analysis of two randomized controlled trials including 218 eyes comparing PR to SB found PR may result in lower rates of reattachment and higher rates of recurrence than SB.18 More recently primary vitrectomy with intraocular gas and laser without scleral buckling has been popularized as a potentially favorable alternative to both scleral buckling and pneumatic retinopexy with the suggestion of higher initial primary reattachment rates presumably due to the concurrent release of vitreous traction and more optimized creation of the chorioretinal adhesion with laser. One large randomized study comparing scleral buckling with primary vitrectomy suggested that the latter technique was comparable or superior to the former depending on the clinical situation.19 Some recent studies of SBP have reported lower primary reattachment rates compared with historical results. Possible causes for this disparity may relate to the greater experience and facility of earlier generations of surgeons with the techniques of scleral buckling compared with those trained in an era in which other primary treatment options including PR and primary vitrectomy without scleral buckling 20,21
In this study, we retrospectively compare both single surgery and final anatomic and visual outcomes of scleral buckling surgery versus pneumatic retinopexy in a consecutive series of patients at a single institution.
Patients and Methods
Forty six consecutive patients undergoing pneumatic retinopexy treatment for uncomplicated rhegmatogenous retinal detachment between January 2002 and June 2009 by one of three surgeons were compared with a consecutive series of 44 patients undergoing scleral buckling by a single surgeon (MSB) during that same time period for a total of ninety patients. The retrospective study was conducted after approval from the Stanford University Human Subjects Institutional Review Board (Protocol number 16117, PI MSB). All research was performed in accordance with the Declaration of Helsinki, the Health Insurance Portability and Accountability Act (HIPAA), and all local, regional, and national laws. All procedures were performed at Stanford Hospital and Clinics by retina faculty members who each had numerous years of experience performing the procedure and regularly performed the procedure. Other patients with retinal detachment seen and treated during that time period were excluded if: (1) there was presence of grade C or higher proliferative vitreoretinopathy; (2) the patient had previously had pars plana vitrectomy surgery for any reason; or (3) follow up was shorter than 6 months.
Preoperative data included in the analysis based on previous studies22 included patient age, sex, eye involved, previous ocular surgery, history of trauma, presence/absence of symptoms, symptom duration prior to diagnosis, best corrected visual acuity (by pinhole vision or refraction), refractive error, detachment position, detachment size (in clock hours), macula status (attached or detached), number/location of retinal breaks/tears identified, and lens status, including presence or absence of previous capsular compromise and/or vitreous loss with cataract surgery.
Operative variables compiled included the type of anesthesia; the type of buckling elements used in the buckling group; the type of gas used for tamponade, if any (sulfur hexafluoride, perfluoropropane, or air); the use of a drainage sclerotomy during scleral buckling; method of chorioretinal adhesion (cryopexy or laser retinopexy); and any intraoperative complications.
Postoperative variables examined included initial and final postoperative retinal attachment status (defined in the 6 month postoperative period), the interval between initial and repeat surgeries if any, best corrected visual acuity, change in refractive error, and any postoperative complications requiring intervention (e.g., epiretinal membrane, ptosis repair, cataract, etc.).
Statistical analysis was performed using a one sided Fisher exact test using the Simple Interactive Statistical Analysis (SISA).23 The null hypothesis was rejected and statistical significance was found for a p-value less than 0.05.
Results
The baseline characteristics of the two groups are listed in Table 1 and were roughly comparable in sample size, age, gender, refractive error, and extent of retinal detachment including macular status. The patients were followed on average for more than 2 years, and over two-thirds of patients were myopic before surgery. The scleral buckle group tended to have a slightly shorter duration of detachment, excluding one chronic detachment (9.3 vs 7.7 days). Pre-operative visual acuities were slightly better in the scleral buckle group than the pneumatic group, although this was not statistically significant (p= 0.18). Both groups had the same average extent of detachment by number of clock hours. The PR patients tended to have more superior detachments and the SBP patients tended to have more inferior detachments.
Table 1:
Baseline characteristics of the patients who underwent PR and SBP, including sample size, age, gender, follow-up duration, lens status, refractive error, duration of detachment, and extent of retinal detachment including macular status.
| Pneumatic retinopexy (n= 46) | Scleral buckle (n=44) | |
|---|---|---|
| Age (mean, in years) | 57 | 51 |
| Gender (percent male) | 57% | 60% |
| Eye, right | 48% | 52% |
| Duration follow-up (mean, in months) | 27 | 29 |
| Myopia, percent | 67% | 73% |
| Percent macula-sparing | 72% | 77% |
| Duration of detachment (mean days) | 9.3 | 7.7* |
| (median days) | 5 | 1 |
| Extent of detachment (number clock hours) | 3.7 | 3.7 |
| Phakic | 70% | 80% |
| Location of detachment (percent) | ||
| Superior | 24% | 14% |
| Superotemporal | 37% | 30% |
| Superonasal | 15% | 7% |
| Temporal | 11% | 21% |
| Nasal | 7% | 5% |
| Inferior | 4% | 9% |
| Inferotemporal | 2% | 9% |
| Inferonasal | 0% | 5% |
Excludes 1 patient with symptoms for 1.5 years with chronic detachment.
The PR patients all received 100% C3F8 gas injection, typically 0.3 to 0.4 mL, but a few received up to 0.6 mL. 28% of the SBP patients had external drainage of subretinal fluid at the time of the surgery, and 61% had sterile air injected at the time of surgery.
As expected from having a very slightly greater proportion of patients with macula-sparing retinal detachments, the pre-operative visual acuity was slightly better in the SBP group (Table 2), with 68% of patients with a visual acuity of 20/40 or better, in contrast with 57% in the PR group, although this value was not statistically significant (p = 0.18). Twenty-eight percent of PR patients had visual acuity worse than 20/200, whereas only 11% of the SBP group had visual acuity worse than 20/200 pre-operatively. The final visual acuity was also better in the SBP group, with a logMAR visual acuity of 0.16 (Snellen equivalent of 20/30) versus 0.28 (Snellen equivalent of 20/40) and 89% achieving 20/40 or better as opposed to only 72% in the PR group, which was statistically significant (p= 0.04).
Table 2:
Visual acuity pre-operatively and final measured along with post-operative complications and recurrence of detachment in patients who underwent PR and SBP.
| Pneumatic retinopexy (n= 46) | Scleral buckle (n=44) | P value | |
|---|---|---|---|
| Pre-operative Best Corrected Visual Acuity | |||
| 20/20 to 20/40 | 57% | 68% | 0.18 |
| 20/50 to 20/200 | 15% | 21% | |
| < 20/200 | 28% | 11% | |
| Mean VA (logMAR) | 0.73 | 0.47 | |
| Mean VA (Snellen equivalent) | 20/100 | 20/60 | |
| Final measured Best Corrected Visual Acuity | |||
| 20/20 to 20/40 | 72% | 89% | 0.04* |
| 20/50 to 20/200 | 24% | 9% | |
| < 20/200 | 4% | 2% | |
| Mean VA (logMAR) | 0.28 | 0.16 | |
| Mean VA (Snellen equivalent) | 20/40 | 20/30 | |
| Recurrent retinal detachment (percent) | 33% | 4.5% | 0.00057* |
| Re-operation (percent) | 41% | 11% | 0.0012* |
| Reason for re-operation (non-detachment) | |||
| Vitrectomy for epiretinal membrane | 6.5% | 4.5% | |
| Ptosis repair | 0% | 2.3% | |
| Cataract surgery (1 combined with vitrectomy) | 4.4% | 0% | |
| Post-operative complications | |||
| Epiretinal membrane | 20% | 20% | |
| Cataract | 8.7% | 2.3% | |
| Corneal erosion | 2.2% | 4.5% | |
| Diplopia | 0% | 6.8% | |
| Ptosis | 0% | 4.5% | |
| Vitreous hemorrhage | 4.3% | 0% |
with bold font indicates statistical significance (p value < 0.05)
Abbreviations: VA = visual acuity
After SBP, 4.5% of patients suffered recurrent retinal detachment after the first intervention as opposed to 33% of those undergoing PR (p= 0.00057). 11% of SBP patients underwent any additional surgical procedure post-operatively in contrast to 41% in the PR group (p = 0.0012). Non-detachment related reasons for additional surgical procedures included vitrectomy for epiretinal membrane repair (6.5% of PR and 4.5% of SBP), 2.3% ptosis repair with SBP, and 4.4% cataract surgery with PR, one of which received both vitrectomy for epiretinal membrane and cataract surgery. The final rate of reattachment with one or more procedures was 100% with SBP and 97.8% with PR. Both PR and SBP had a 20% rate of epiretinal membrane formation (Table 2). Cataracts occurred more commonly with PR (8.7%) than with SBP (2.3%). The 3 cases of diplopia after SBP (6.8%) were managed with prism, and no cases of diplopia required surgical intervention or buckle removal. Corneal erosion occurred in both PR and SBP groups and was managed with antibiotic ointment and/or bandage contact lens. Ptosis occurred in 2 patients (4.5%) with SBP and was managed with surgery in 1 patient.
Plotting the visual acuity over time reveals that patients with a successful PR and SBP have similar visual acuity outcomes (Figure 1). Even after successful secondary surgical intervention, those patients who had an unsuccessful PR had a significantly worse visual outcome both initially after intervention and even after 1 year, with a logMAR visual acuity of 0.51 (Snellen equivalent of 20/65) versus 0.11 (Snellen equivalent of 20/25) for those patients with a successful PR.
Figure 1.
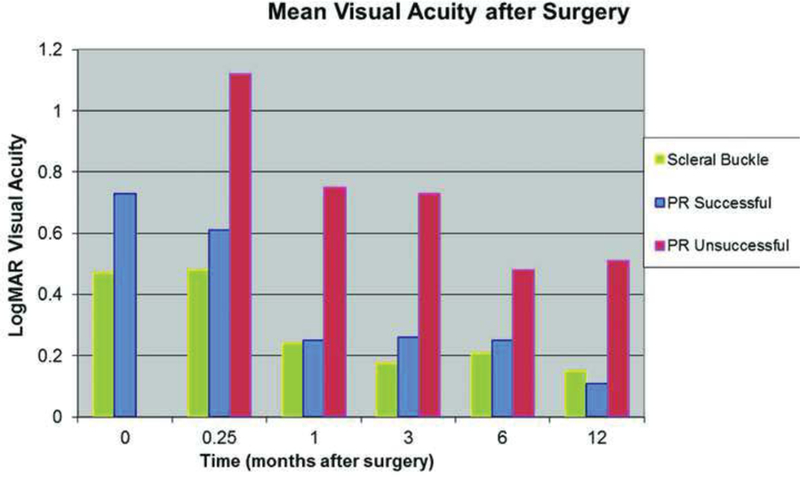
Mean logMAR visual acuity plotted over time in the year following retinal reattachment surgery demonstrates that patients with successful PR and SBP have similar visual acuity outcomes (blue and green bars). Patients who had an unsuccessful PR (red bar) had a significantly worse visual outcome even after 1 year, with a logMAR visual acuity of 0.51 (Snellen equivalent of 20/65) versus 0.11 (Snellen equivalent of 20/25) for those patients with a successful PR.
Discussion
This study retrospectively compares two different methods of primary rhegmatogenous retinal detachment repair, pneumatic retinopexy and scleral buckle. Factors evaluated include primary retinal reattachment rate, both primary and final anatomic success, and ensuing postoperative visual outcomes as a function of the primary procedure chosen. SBP had a significantly higher rate of single surgery reattachment rate, 95.5% versus 67% (p= 0.00057). The success rate of PR of 67% in our study is within the primary reattachment anatomic success spectrum of PR reported in the literature.12–14 The final visual acuity also appeared to be better in the SBP group with 0.12 logMAR difference. However, the SBP group also had more patients with macula-sparing retinal detachments, and thus had a baseline slightly better visual acuity. More patients who underwent SBP had a visual acuity of 20/40 or better, 89% SB versus 72% with PR, although this was not statistically significant (p= 0.18).
Evaluation of the mean visual acuity demonstrated that the patients with unsuccessful PR typically did not recover vision even after 1 year. However patients with failed PR also had worse pre-operative visual acuity, although this was not statistically significant. Given the retrospective nature of this study, alternatively this could have been due to numerous other factors, including subjective patient and/or physician preference. The small sample size of this study also limits the evaluation of these smaller subgroups as does the lack of patients undergoing primary vitrectomy as a treatment option.
This study suggests that stratification by initial success or failure of the PR may be a reliable predictor of final visual outcome. Anaya et al. suggested that failed pneumatic retinopexy may be a reflection of an intrinsically unfavorable reattachment prognosis whichever procedure was chosen primarily.24 This emphasizes both the importance as well as the challenges of appropriate patient selection in PR, since all patients who received PR were deemed by the surgeons to be good candidates for PR.
These data taken in conjunction with prior publications highlight the importance of clearly specifying the expected clinical outcomes for studies that purport to compare the efficacy of different procedural approaches to the treatment of retinal detachment. While final reattachment rates may not be different between various procedures such as scleral buckling versus pneumatic retinopexy or primary vitrectomy, initial rates may be quite different with subsequent impact on patient quality of life and cost. Additionally, rates of primary retinal reattachment by scleral buckling may vary widely due to differences in training. This could have significant impact on the sensitivity of well designed randomized clinical trials to detect differences in outcomes between different procedural approaches. In one large randomized clinical trial comparing scleral buckling versus primary vitrectomy, the final reattachment rates in phakic patients were good for both scleral buckle, taking into account one or more procedures at 96.7%, and vitrectomy at 96.6%.21 The rate of primary reattachment with scleral buckling alone was 63.6%, and was not significantly different from a rate of 63.8% with primary vitrectomy.21 In another randomized study, the rate of primary reattachment for scleral buckling alone was 75%.25 Both of those two rates of primary retinal reattachment for scleral buckling alone compare unfavorably with the frequency of primary retinal reattachment with one procedure in our study of 95.5%, or similar past studies, and make the conclusion of equipoise between scleral buckling and alternative procedures such as pneumatic retinopexy less compelling.
Both PR and SBP carry the risk of post-operative complications, which vary between the two procedures. The most common complication in our study was the development of an epiretinal membrane, which occurred in 20% of patients with both PR and SBP. SBP also carries the risk of diplopia, which is temporary in most cases. Persistent diplopia can typically be successfully managed through prisms, botulinum toxin injections, or strabismus surgery.26 In our series, 6.8% of patients who underwent SBP had diplopia, but all cases of diplopia were managed medically with prism. No cases of diplopia in our series were debilitating to patients and none required surgical intervention or buckle removal. In addition, SBP often induces a refractive change in patients. Encircling bands in adults has been demonstrated to result in a refraction change of 1 diopter after surgery, which is stable for at least 10 years.27 However, in pediatric patients, SBP results in less myopia 4 years after the surgery, which is thought to possibly be related to SBP affecting ocular growth.28 Many patients who receive SBP are myopic (73% in our study), and thus a mild refractive change was typically well-tolerated.
This study has several limitations. It is retrospective and thus subject to selection bias, although inclusion and exclusion criteria were strictly followed prior to enrollment in the outcome analysis. For example, lack of six-month follow-up was an exclusion criterion. Patients who underwent a successful procedure and did not return for follow-up postoperatively might have been lost to follow-up to a greater extent than those who initially failed to reattach. The patients in the study were not randomized, and thus the surgeons selected which patients received which procedure. Patients undergoing primary vitrectomy or vitrectomy and scleral buckling were excluded, although that procedure was not typically performed in most patients with uncomplicated retinal detachment at this institution during that time period. It is possible that macula-sparing and/or macula-threatening detachments may undergo SBP more frequently than PR because of a perceived superior single-procedure success rate in an eye with more visual potential. The study is limited by its size with ninety patients in the two groups combined, although each group is roughly a similar size. All the patients studied were treated consecutively during the same time period so it is less likely that there was selection bias in which patients were reported. Additionally, patient preference, surgeon comfort, post-operative positioning, and cost are additional factors to consider when selecting the appropriate procedure for a given patient.
In a 2015 survey of retina specialists, for a pseudophakic patient with a superior macula-sparing retinal detachment with one tear in a −3D myope, only 4% of US respondents would perform a SBP alone, 10% would perform a SB and vitrectomy, 58% would perform vitrectomy without SBP, and 28% would perform a PR.29 In one large retrospective study, whereas the total number of retinal reattachment procedures performed on Medicare Beneficiaries between 1997 and 2007 increased by 13%, the percentage of retinal reattachment procedures with vitrectomy increased 72% during that same time period. Simultaneously, the number of scleral buckling procedures without vitrectomy decreased by 69%.22 Cost-effectiveness analysis has found the weighted cost of pneumatic retinopexy to be $1961 to $3565 and the weighted cost of scleral buckle to be $4873.30 In another study, the rate of primary reattachment of 80.8% for both scleral buckling and vitrectomy with or without scleral buckling was higher than pneumatic retinopexy rate of 59.4%, although the rate of adverse outcomes was approximately two times higher in the vitrectomy group than the scleral buckling group.31 Our data and review of the literature continue to support the utility of scleral buckle in the management of uncomplicated retinal detachment as an important primary treatment option, and the need to continue to train residents and fellows in the performance of this time honored and valuable technique.
Acknowledgments
Funding was provided in part by the Heed Ophthalmic Foundation Fellowship Grant (YMP) and the National Eye Institute 4K12EY022299–4 (YMP).
Footnotes
Disclosure: None of the authors has any relevant conflicts of interest to disclose relating to the subject material in this manuscript.
References
- 1.Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedures. I. Surgical techniques and management. AMA Arch Ophthalmol 1957; 58:797–811. [DOI] [PubMed] [Google Scholar]
- 2.Rumpf J Gonin Jules. Inventor of the surgical treatment for retinal detachment. Surv Ophthalmol 1976; 21:276–84. [DOI] [PubMed] [Google Scholar]
- 3.Sodhi A, Leung LS, Do DV, et al. Recent trends in the management of rhegmatogenous retinal detachment. Surv Ophthalmol 2008; 53:50–67. [DOI] [PubMed] [Google Scholar]
- 4.Schwartz SG, Kuhl DP, McPherson AR, et al. Twenty-year follow-up for scleral buckling. Arch Ophthalmol 2002; 120:325–9. [DOI] [PubMed] [Google Scholar]
- 5.Lincoff H, Coleman J, Kreissig I, et al. The perfluorocarbon gases in the treatment of retinal detachment. Ophthalmology 1983; 90:546–51. [DOI] [PubMed] [Google Scholar]
- 6.Hilton GF, Grizzard WS. Pneumatic retinopexy. A two-step outpatient operation without conjunctival incision. Ophthalmology 1986; 93:626–41. [DOI] [PubMed] [Google Scholar]
- 7.Mansour AM. Pneumatic retinopexy for inferior retinal breaks. Ophthalmology 2005; 112:1771–6. [DOI] [PubMed] [Google Scholar]
- 8.Tornambe PE, Hilton GF, Kelly NF, et al. Expanded indications for pneumatic retinopexy. Ophthalmology 1988; 95:597–600. [DOI] [PubMed] [Google Scholar]
- 9.Benson WE, Chan P, Sharma S, et al. Current popularity of pneumatic retinopexy. Retina 1999; 19:238–41. [PubMed] [Google Scholar]
- 10.Snyder WB, Bloome MA, Birch DG. Pneumatic retinopexy versus scleral buckle. Preferences of Vitreous Society members, 1990. Retina 1992; 12:43–5. [PubMed] [Google Scholar]
- 11.Hilton GF, Kelly NE, Salzano TC, et al. Pneumatic retinopexy. A collaborative report of the first 100 cases. Ophthalmology 1987; 94:307–14. [PubMed] [Google Scholar]
- 12.Zaidi AA, Alvarado R, Irvine A. Pneumatic retinopexy: success rate and complications. Br J Ophthalmol 2006; 90:427–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kulkarni KM, Roth DB, Prenner JL. Current visual and anatomic outcomes of pneumatic retinopexy. Retina 2007; 27:1065–70. [DOI] [PubMed] [Google Scholar]
- 14.Rahat F, Nowroozzadeh MH, Rahimi M, Farvardin M, Namati AJ, Sarvestani AS, Sharifi F. Pneumatic retinopexy for primary repair of rhegmatogenous retinal detachments. Retina 2015;35(6):1247–55. [DOI] [PubMed] [Google Scholar]
- 15.McAllister IL, Meyers SM, Zegarra H, et al. Comparison of pneumatic retinopexy with alternative surgical techniques. Ophthalmology 1988; 95:877–83. [DOI] [PubMed] [Google Scholar]
- 16.Han DP, Mohsin NC, Guse CE, et al. Comparison of pneumatic retinopexy and scleral buckling in the management of primary rhegmatogenous retinal detachment. Southern Wisconsin Pneumatic Retinopexy Study Group. Am J Ophthalmol 1998; 126:658–68. [DOI] [PubMed] [Google Scholar]
- 17.Tornambe PE, Hilton GF. Pneumatic retinopexy. A multicenter randomized controlled clinical trial comparing pneumatic retinopexy with scleral buckling. The Retinal Detachment Study Group. Ophthalmology 1989; 96:772–83; discussion 84. [DOI] [PubMed] [Google Scholar]
- 18.Hatef E, Sena DF, Fallano KA, Crews J, Do DV. Pneumatic retinopexy versus scleral buckle for repairing simple rhegmatogenous retinal detachments. Cochrane Database Syst Rev 2015. May 7;5:CD008350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. ; Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology 2007;114(12):2142–54. [DOI] [PubMed] [Google Scholar]
- 20.Ramulu PY, Do DV, Corcoran KJ, et al. Use of retinal procedures in medicare beneficiaries from 1997 to 2007. Arch Ophthalmol 2010;128(10):1335–40. [DOI] [PubMed] [Google Scholar]
- 21.Day S, Grossman DS, Mruthyunjaya P, et al. One-year outcomes after retinal detachment surgery among medicare beneficiaries. Am J Ophthalmol 2010;150(3):338–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Adelman RA, Parnes AJ, Michalewska Z, Ducournau D; European Vitreo-Retinal Society (EVRS) Retinal Detachment Study Group. Clinical variables associated with failure of retinal detachment repair: the European vitreo-retinal society retinal detachment study report number 4. Ophthalmology 2014;121(9):1715–9. [DOI] [PubMed] [Google Scholar]
- 23.Uitenbroek DG. (1997). SISA Binomial Southampton: D.G. Uitenbroek; Retrieved December 10, 2016, from the World Wide Web: http://www.quantitativeskills.com/sisa/distributions/binomial.htm. [Google Scholar]
- 24.Anaya JA, Shah CP, Heier JS, Morley MG. Outcomes after Failed Pneumatic Retinopexy for Retinal Detachment. Ophthalmology 2016;123(5):1137–42. [DOI] [PubMed] [Google Scholar]
- 25.Moradian S, Ahmadieh H, Faghihi H, et al. Comparison of four surgical techniques for management of pseudophakic and aphakic retinal detachment: a multicenter clinical trial. Graefes Arch Clin Exp Ophthalmol 2016;254(9):1743–51. [DOI] [PubMed] [Google Scholar]
- 26.Farr AK, Guyton DL. Strabismus after retinal detachment surgery. Curr Opin Ophthalmol 2000; 11(3):207–10. [DOI] [PubMed] [Google Scholar]
- 27.Kawasaki T, Ideta H, Murata M, et al. Long-term changes in refraction following retinal detachment surgery. Jpn J Clin Ophthalmol 2000;54:909–912. [Google Scholar]
- 28.Sato T, Kawasaki T, Okuyama M, Ideta H. Refractive changes following scleral buckling surgery in juvenile retinal detachment. Retina 2003;23(5):629–35. [DOI] [PubMed] [Google Scholar]
- 29.Stone TW, ed. ASRS 2015 Preferences and Trends Membership Survey Chicago, IL: American Society of Retina Specialists; 2015. [Google Scholar]
- 30.Chang JS, Smiddy WE. Cost-Effectiveness of Retinal Detachment Repair. Ophthalmology 2014; 121(4):946–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Adelman RA, Parnes AJ, Ducournau D; European Vitreo-Retinal Society (EVRS) Retinal Detachment Study Group. Strategy for the management of uncomplicated retinal detachments: the European vitreo-retinal society retinal detachment study report 1. Ophthalmology 2013;120(9):1804–8. [DOI] [PubMed] [Google Scholar]