

Abstract
改良唇-牙-牙槽嵴上颌全口种植义齿分类法是根据牙槽嵴宽度和高度将上颌无牙颌分为3类。Ⅰ类,牙槽嵴宽度高度均适宜,适合种植固定义齿修复;Ⅱ类,牙槽嵴宽度对于种植体足够但是对唇颊支撑不足,适合于固定活动联合修复;Ⅲ类,牙槽嵴高度或宽度不足以支撑种植体植入,需要植骨,或采用穿颧种植体等特殊方式种植,或者采用传统全口义齿修复。第Ⅰ类根据牙槽嵴高度不同又分为2个亚类:第Ⅰ类1亚类,牙槽嵴高度完全没有丧失,适合冠桥式义齿修复;第Ⅰ类2亚类,牙槽嵴高度有部分丧失,适合复合式义齿修复。本设计分类旨在帮助术者在术前明确患者是否适合种植,以及适合采用种植固定义齿还是种植活动义齿修复,有利于更好地选择适应证,减少并发症,获得更好的长期效果。
Keywords: 种植体支持义齿, 上颌无牙颌, 分类
Abstract
According to the width and height of the maxillary alveolar ridge, the maxillary edentulous jaws can be divided into three categories by using modified lip-tooth-ridge (MLTR) classification. Class Ⅰ is characterized by sufficient bone available for implants in the vertical and horizontal aspects and is suitable for fixed implant-supported prostheses. Class Ⅱ is characterized by sufficient bone amount available for implants in a horizontal aspect but insufficient for lip support and is suitable for a fixed detachable implant-supported prosthesis. Class Ⅲ is characterized by inadequate amount of bone for implants (with vertical or horizontal components) and is suitable for the use of zygomatic implants or traditional complete denture. Patients belonging to Class Ⅰ can be further classified into two sub-categories according to the height of the alveolar ridge. The first subclass is characterized by minimal bone deficiency and is suitable for a conventional implant-supported “crown and bridge” prosthesis. The second subclass is characterized by a larger vertical deficiency than that of the first subclass and is suitable for implant-supported hybrid prosthesis. The MLTR classification system can help the dentist to determine whether the patient is suitable for implanting dentures and whether fixed denture or removable denture is appropriate for the patient, select indications, reduce complications, and achieve long-term results.
Keywords: implant-supported prosthesis, maxillary edentulous, classification
种植技术为无牙颌患者提供了更多的修复方案,包括多种修复方法:冠桥式种植义齿、复合式种植义齿、固定活动联合种植义齿等[1]。在临床应用时,具体方案的选择需要考虑众多因素,包括美观、发音、自洁、患者配合程度、骨吸收状况、力学分布以及长期的功能稳定等[2]–[5]。这些因素中,牙槽嵴吸收状况及分布是选择种植体支持的修复方案时最主要的考虑内容。按照牙槽嵴吸收程度及前后向分布对上颌无牙颌进行分类的方法有多种[1],[5]–[9]。随着倾斜种植体和上颌窦提升技术的广泛应用,后牙区种植已经变得更加普及,此时颊舌向牙槽嵴吸收状况及与理想牙齿位置和口唇之间的相互关系对上颌种植体支持的修复方案选择起到了更加重要的作用[3]。2017年,Adrien Pollini等根据这三者之间的关系提出了唇-牙-牙槽嵴分类(the lip-tooth-ridge classification,LTR)[10],给临床医生带来了很多便利。在临床应用中,笔者感觉到LTR分类仍可以进一步改进,因此笔者根据临床实际需求提出了改良唇-牙-牙槽嵴分类(the modified-lip-tooth-ridge classification,MLTR)法,简述如下:与LTR分类法一样,先根据美学分析确定理想切缘及龈缘位置和唇颊丰满度,此位置不要受现有牙槽嵴和残余天然牙的影响,然后以能否提供唇颊丰满度和理想牙位置支持以及能否容纳种植体作为标准来衡量牙槽嵴的宽度和高度[3],[10]。由于牙槽嵴宽度是决定适合固定还是活动义齿修复的关键因素,所以根据患者牙槽嵴宽度进行基本分类,可以分为3类(图1)。
图 1. 上颌无牙颌MLTR分类,3个主分类及2个亚类的示意图.

Fig 1 The MLTR classification of the maxillary edentulous, the sketch maps of the three main categories and two sub-categories
A:MLTR-Ⅰ类1亚类;B:MLTR-Ⅰ类2亚类;C:MLTR-Ⅱ类;D:MLTR-Ⅲ类。
1. MLTR的分类原则
1.1. MLTR-Ⅰ类
牙槽嵴宽度和高度能容纳适宜的种植体,在牙槽嵴高度范围内能为唇颊提供足够的支撑。牙槽嵴的唇颊侧不需要借助基托获得唇颊丰满度,修复体能够形成适宜的穿龈外形,支持理想的牙位置。此时可以采用固定义齿修复。在MLTR-Ⅰ类中,根据牙槽嵴高度不同可以分为两个亚类。
1.1.1. MLTR-Ⅰ类1亚类
牙槽嵴宽度、高度足够,患者只有牙缺失,牙槽嵴及黏膜等软组织无明显丧失,适合冠桥式修复;一般前牙切缘到龈缘距离为7~10 mm[10],理想龈缘距离牙槽嵴顶距离小于4 mm[11]–[12](图2)。
图 2. MLTR-Ⅰ类1亚类,冠桥式种植义齿修复.

Fig 2 The classification MLTR-Ⅰ, sub-categories 1, and the implant-supported “crown and bridge” prosthesis
冠桥式修复要求种植体植入、穿龈方式与传统的单牙缺失种植冠或桥一致,需准确的种植体植入位置和良好的穿龈外形;如果穿龈外形美观,即使是高位笑线,对多数患者也不存在美观问题[13]。
1.1.2. MLTR-Ⅰ类2亚类
牙槽嵴宽度足够,高度出现吸收,患者有牙缺失并伴有牙槽嵴和软组织缺损,需行复合式义齿修复(图3)。复合式义齿可恢复缺失牙、缺损的牙槽嵴和黏膜组织,其特点是体积较大,清洁较困难,建议采用螺丝固位,方便后期复查。由于修复体边缘不美观,一般修复体边缘不能暴露,修复体边缘应当位于笑线的根方。当笑线较高时,可以根据情况将修复体边缘通过降低骨高度达到笑线的根方以上。由于修复体边缘不外露,不需要根据美观需求进行种植体定位,也不需要获取美观的穿龈外形,只要具备良好的自洁功能即可。
图 3. MLTR-Ⅰ类2亚类,复合式种植义齿修复.

Fig 3 The classification MLTR-Ⅰ, sub-categories 2, and the implant-supported hybrid prostheses
1.2. MLTR-Ⅱ类
牙槽嵴宽度和高度虽能容纳适宜种植体,但在牙槽嵴高度范围内牙槽嵴宽度不足以对唇颊产生足够的支撑,不能形成理想的穿龈外形,需要在牙槽嵴唇颊侧使用基托以获得唇颊丰满度,带有唇颊侧基托的义齿需要摘戴清洁,适合用固定活动联合义齿修复。
1.3. MLTR-Ⅲ类
牙槽嵴宽度或者高度不能容纳种植体,如果不使用植骨技术则不能行常规种植技术修复,只能使用穿颧种植体[1],[14]或传统全口义齿的方法进行修复。
2. 关于MLTR分类的补充说明
临床医生可以通过植骨或去骨的方式实现MLTR各分类之间的转化。如部分牙槽嵴靠近冠方宽度不足,而根方宽度足够,为MLTR-Ⅱ类;如果术中将高度降低至牙槽嵴宽度足够,则转化为MLTR-Ⅰ类2亚类;如果通过植骨增加靠近冠方牙槽嵴的宽度,则可转化为MLTR-Ⅰ类1亚类(图4)。MLTR-Ⅲ类可以通过植骨或者去骨转化为MLTR-Ⅱ类甚至Ⅰ类。MLTR-Ⅱ类可以转化为Ⅰ类,但是大量植骨的最终效果存在不确定性,需要慎重对待[15]。
图 4. MLTR-Ⅱ类可以通过植骨或者降低骨高度转化为MLTR-Ⅰ类.
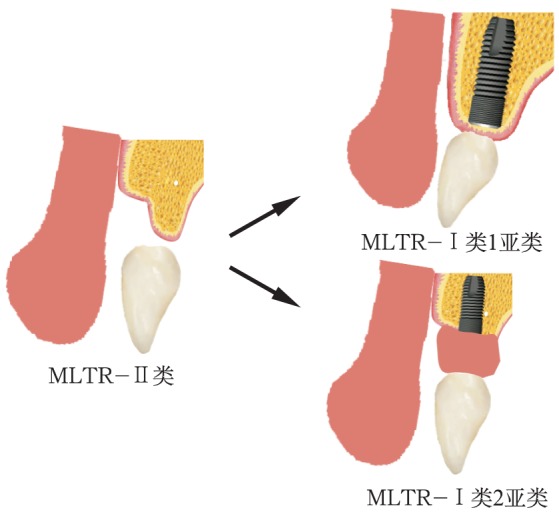
Fig 4 The MLTR-Ⅱ classification could transfer to MLTR-Ⅰ by the alveolar bone augmentation or removal
临床上全口种植患者在分类设计阶段,很多患者口内仍有天然牙存在,此时需要术前预估拔牙种植后牙槽嵴的吸收量,根据预计可保存的牙槽嵴进行MLTR分类。一般拔牙后牙槽嵴外形改变的时间集中在6~12个月内,颊舌向吸收量5~7 mm(相当于原宽度的50%)。牙槽嵴在拔牙后3个月内的吸收量最多[16],颊舌向为4~5 mm,垂直向为1~2 mm[17]–[18]。如果牙槽嵴完整,采用适宜的即刻种植即刻修复技术,可将外形轮廓改变量减少至0.4 mm[19];如果牙槽嵴薄弱或不规则,可根据需要进行牙槽嵴修整。
MLTR分类实际上是针对每个部位的颊舌向骨吸收情况进行分类。同一患者的不同区域可能属于不同分类。不同区域对修复体有不同的要求,一般在前牙区主要考虑美观和自洁,需结合笑线位置综合考虑;后牙区主要侧重修复体的受力及自洁。对部分前牙区牙槽嵴宽度不足的患者,可考虑前牙区使用改良盖嵴式设计而不作种植,只在后牙区进行种植[20]。前牙区大范围改良盖嵴式设计对患者自我清洁和维护能力的要求较高,而前牙区单臂悬梁会对合力分布控制的要求较高,需要谨慎选择。
MLTR-Ⅱ类患者可以采用种植覆盖义齿修复。牙槽嵴高度会影响到颌间间距,颌间间距会影响种植体相连的附着体的选择。如果切缘到牙槽嵴顶间距离在12 mm以上可以采用杆卡固位方式;距离为10~12 mm可选择球帽或者套筒冠修复;距离为8~10 mm,可以选用Locator或者磁性附着体修复(图5);如果距离低于8 mm,常需要去骨以获得足够的修复间隙[21],否则会造成修复困难。
图 5. 种植固定可摘义齿联合修复,带有4个Locator的覆盖义齿.

Fig 5 A fixed detachable implant-supported prosthesis: the overdenture with 4 Locators
上:覆盖义齿戴入前;下:覆盖义齿戴入后。
3. MLTR分类在临床上的应用
以1名典型病例介绍MLTR分类在临床上的应用。患者为已经拔牙3个月的无牙颌患者,要求种植修复(图6)。按照MLTR分类法,首先判断患者牙槽嵴能否容纳适宜的种植体,如果无法种植或者无法植骨后种植,归为MLTR-Ⅲ类;如果能够种植则归为MLTR-Ⅰ类或者Ⅱ类,具体分类再根据牙槽嵴的宽度和高度进一步判断。
图 6. 患者治疗前口内观.

Fig 6 The patients' intraoral view before treatment
左:上颌;右:下颌。
本病例牙槽嵴宽度和高度可以容纳种植体,因此需要进一步判断具体的分类。按照常规总义齿制取印模,灌制模型(图7A),制作暂基托和蜡堤,确定颌位关系以及唇丰满度(图7B、图8),将暂基托的颊侧基托降低至患者能够接受的唇丰满度,按照传统全口义齿方法确定理想的切缘、龈缘和笑线位置,并获得患者的认可,利用显影剂将这几个位置在暂基托蜡堤上或者已经完成试排牙的暂基托上标出(图7C、D),然后拍摄锥形束CT(cone beam computed tomography,CBCT)进行具体分析(图9)。
图 7. 制取印模,确定颌位关系及唇丰满度.

Fig 7 Making the impression, determine the relationship of the jaws and the convexity of the lip
A:常规制取上下颌全口印模,灌制模型;B:常规制作暂基托蜡堤确定颌位关系,并尽可能降低唇侧基托高度;C:利用标记物标记切缘、龈缘、笑线等位置;D:利用标记物标记拟植入种植体的位置。
图 8. 确定颌位关系时患者正面观(左)和侧面观(右).

Fig 8 Patients' front view (left) and side view (right) when determining the relationship of jaws
图 9. 以CBCT影像12牙位颊舌向横断面为例,可以看到笑线、穿龈位置、牙槽骨宽度和高度等信息.
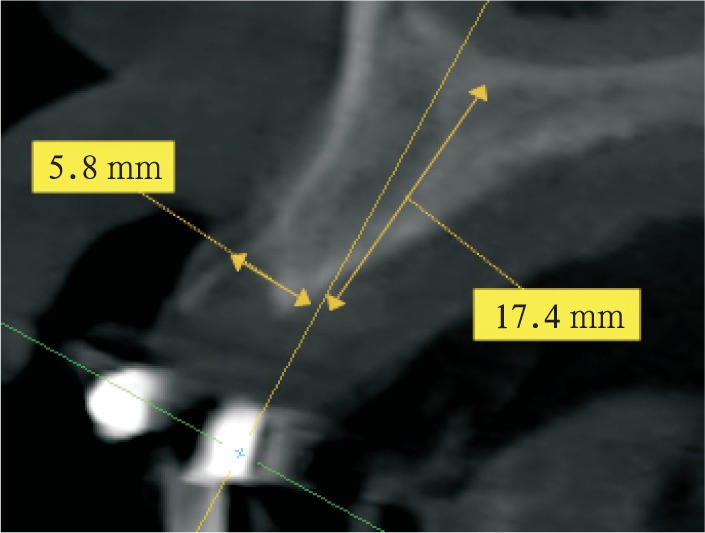
Fig 9 As an example, from the cross section of the cheek and tongue of the 12 teeth in the CBCT image, the smile line, gum position, width and height of alveolar bone could be seen
本病例最小唇侧基托边缘位于前牙区牙槽嵴的冠方,前牙区牙槽嵴宽度可以支撑口唇凸度,但龈缘位置距离牙槽嵴顶距离大于4 mm,不是单纯的牙缺失,为MLTR-Ⅰ类2亚类;与患者讨论后决定采用复合式义齿修复。 采用微创技术进行上下颌种植手术(图10A),放置多基基台,制作临时修复体(图10B、D),待3个月种植体骨结合完成后,完成最终修复(图10C、E和图11)。
图 10. 6枚种植体植入上颌完成即刻修复及最终修复.

Fig 10 Six implants had been put into the upper jaw and the temporary and final prostheses had been finished
A:上颌植入6枚种植体;B:戴入上颌临时修复体;C:戴入正式修复体;D:戴入临时修复体后曲面断层片;E:戴入正式修复体后曲面断层片。
图 11. 戴入正式修复体后正面观(左)及侧面观(右).

Fig 11 The front view (left) and side view (right) with the final prostheses
4. 讨论
设计种植支持的上颌全口义齿时,最关键的问题有两个,一是能否行种植术,二是适合固定还是活动义齿修复。原LTR分类法侧重于解剖结构,分为没有缺损、垂直方向缺损、水平方向缺损和组合缺损。MLTR分类法根据临床需求进行分类,首先判断牙槽嵴是否容纳适宜的种植体。如果不能容纳种植体,为MLTR-Ⅲ类;如果能容纳种植体,且其宽度可以支撑唇丰满度和理想的牙位置,为MLTR-Ⅰ类,可采用种植固定修复;根据牙槽嵴高度是否有丧失,又可分为2个亚类。如果能够容纳种植体,但是宽度不足以支撑唇颊软组织,不能获得良好的修复体自洁形态,则为MLTR-Ⅱ类,需要采用固定活动联合修复。
上颌前牙区牙齿缺失后颊舌向变化往往较后牙区明显,而且前牙区需要考虑更多的美学因素,因此前牙区MLTR分类对于最终种植方案选择起到了更加重要的作用,应当重点考虑。
临床上很多情况下种植支持的固定修复很难完全兼顾发音、口唇支撑和口腔卫生维护等全部的条件[22],种植体支持的固定义齿使用率实际上少于固定活动联合义齿。在一项回顾性研究[4]中也证实了这一观点。Bern大学2006—2009年间对43名患者进行了种植体支持的义齿修复,冠桥式修复患者为2.3%,复合式为20.9%,69.8%患者采用了覆盖义齿修复,7%患者不能采用种植修复[4]。
MLTR分类中一项重要的判断指标是唇侧基托是否需要以及其伸展范围,需要考虑唇颊软组织的支撑效果和修复体的可清洁能力。修复体这种能力一般受到种植体位置、颊侧软硬组织厚度,以及理想修复体龈缘及颊面外形的影响。在临床上有两个参数可以进行衡量,一个参数为伪牙龈角(angulation of artificial gingiva)[23],指的是人工牙龈颊舌面与牙槽嵴颊面延长线的夹角;另一个参数称为ProsthProfile[4],指的是牙龈缘到种植体颊侧缘的连线与 平面的夹角。一般伪牙龈角小于45°适合固定义齿修复,大于45°时适合活动义齿修复;ProsthProfile大于45°适合冠桥式义齿修复,30°~45°适合复合式义齿修复,小于30°适合固定活动联合修复(覆盖义齿)[4]。如果伪牙龈角过大,或者ProsthProfile过小,会导致患者自洁困难,部分患者会感觉到上唇运动受限。
平面的夹角。一般伪牙龈角小于45°适合固定义齿修复,大于45°时适合活动义齿修复;ProsthProfile大于45°适合冠桥式义齿修复,30°~45°适合复合式义齿修复,小于30°适合固定活动联合修复(覆盖义齿)[4]。如果伪牙龈角过大,或者ProsthProfile过小,会导致患者自洁困难,部分患者会感觉到上唇运动受限。
MLTR分类不是替代原有的系统诊断和分析,种植体前后向的分布仍然是全口种植设计中需要重点考虑的内容。MLTR分类主要侧重分析种植体与理想牙齿、唇颊舌之间的位置关系,帮助分析什么情况可以使用种植修复,什么情况适合种植固定义齿,什么情况适合种植固定活动联合修复。良好充分的术前分析可帮助临床医生更好地选择适应证,减少并发症,获得更好的长期效果。MLTR分类法是基于一定临床技术水平和患者的全身和局部状况,尤其是在患者主动配合能力的基础上提出的,在临床应用中,医生要充分考虑自身的临床技能和患者情况,尤其是主动配合能力,选择最佳的种植修复方案。
Acknowledgments
本文图2所示病例的修复部分由北京大学口腔医院王新知医师提供,本文修复体制作由北京大学口腔医院技工室王乔技师和李曼技师完成,特此致谢!
References
- 1.Bedrossian E, Sullivan RM, Fortin Y, et al. Fixed-prosthetic implant restoration of the edentulous maxilla: a systematic pretreatment evaluation method[J] J Oral Maxillofac Surg. 2008;66(1):112–122. doi: 10.1016/j.joms.2007.06.687. [DOI] [PubMed] [Google Scholar]
- 2.Sadowsky SJ, Fitzpatrick B, Curtis DA. Evidence-based criteria for differential treatment planning of implant restorations for the maxillary edentulous patient[J] J Prosthodont. 2015;24(6):433–446. doi: 10.1111/jopr.12226. [DOI] [PubMed] [Google Scholar]
- 3.Zitzmann NU, Marinello CP. Treatment plan for restoring the edentulous maxilla with implant-supported restorations: removable overdenture versus fixed partial denture design[J] J Prosthet Dent. 1999;82(2):188–196. doi: 10.1016/s0022-3913(99)70155-1. [DOI] [PubMed] [Google Scholar]
- 4.Avrampou M, Mericske-Stern R, Blatz MB, et al. Virtual implant planning in the edentulous maxilla: criteria for decision making of prosthesis design[J] Clin Oral Implants Res. 2013;24(Suppl A100):152–159. doi: 10.1111/j.1600-0501.2011.02407.x. [DOI] [PubMed] [Google Scholar]
- 5.Bidra AS, Agar JR. A classification system of patients for esthetic fixed implant-supported prostheses in the edentulous maxilla[J] Compend Contin Educ Dent. 2010;31(5):366–368, 370, 372-374. [PubMed] [Google Scholar]
- 6.Papadimitriou DE, Salari S, Gannam C, et al. Implant-prosthodontic classification of the edentulous jaw for treatment planning with fixed rehabilitations[J] Int J Prosthodont. 2014;27(4):320–327. doi: 10.11607/ijp.3791. [DOI] [PubMed] [Google Scholar]
- 7.John V, Gossweiler M. Implant treatment planning and rehabilitation of the anterior maxilla: part 1[J] J Indiana Dent Assoc. 2001;80(2):20–24. [PubMed] [Google Scholar]
- 8.Maló P, Nobre Md, Lopes A. The rehabilitation of completely edentulous maxillae with different degrees of resorption with four or more immediately loaded implants: a 5-year retrospective study and a new classification[J] Eur J Oral Implantol. 2011;4(3):227–243. [PubMed] [Google Scholar]
- 9.Jensen OT. Complete arch site classification for all-on-4 immediate function[J] J Prosthet Dent. 2014;112(4):741–751. doi: 10.1016/j.prosdent.2013.12.023. [DOI] [PubMed] [Google Scholar]
- 10.Pollini A, Goldberg J, Mitrani R, et al. The lip-tooth-ridge classification: a guidepost for edentulous maxillary arches. Diagnosis, risk assessment, and implant treatment indications[J] Int J Periodontics Restorative Dent. 2017;37(6):835–841. doi: 10.11607/prd.3209. [DOI] [PubMed] [Google Scholar]
- 11.Kan JY, Rungcharassaeng K, Umezu K, et al. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans[J] J Periodontol. 2003;74(4):557–562. doi: 10.1902/jop.2003.74.4.557. [DOI] [PubMed] [Google Scholar]
- 12.Hermann JS, Buser D, Schenk RK, et al. Biologic width around titanium implants. A physiologically formed and stable dimension over time[J] Clin Oral Implants Res. 2000;11(1):1–11. doi: 10.1034/j.1600-0501.2000.011001001.x. [DOI] [PubMed] [Google Scholar]
- 13.Al-Johany SS, Alqahtani AS, Alqahtani FY, et al. Evaluation of different esthetic smile criteria[J] Int J Prosthodont. 2011;24(1):64–70. [PubMed] [Google Scholar]
- 14.Maló P, Nobre Mde A, Lopes A, et al. Five-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded zygomatic implants placed extra-maxillary[J] Eur J Oral Implantol. 2014;7(3):267–281. [PubMed] [Google Scholar]
- 15.Milinkovic I, Cordaro L. Are there specific indications for the different alveolar bone augmentation procedures for implant placement? A systematic review[J] Int J Oral Maxillofac Surg. 2014;43(5):606–625. doi: 10.1016/j.ijom.2013.12.004. [DOI] [PubMed] [Google Scholar]
- 16.Chen ST, Wilson TG, Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes[J] Int J Oral Maxillofac Implants. 2004;19(Suppl):12–25. [PubMed] [Google Scholar]
- 17.Mecall RA, Rosenfeld AL. Influence of residual ridge resorption patterns on implant fixture placement and tooth position. 1[J] Int J Periodontics Restorative Dent. 1991;11(1):8–23. [PubMed] [Google Scholar]
- 18.Schropp L, Wenzel A, Kostopoulos L, et al. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study[J] Int J Periodontics Restorative Dent. 2003;23(4):313–323. [PubMed] [Google Scholar]
- 19.Tarnow DP, Chu SJ, Salama MA, et al. Flapless postextraction socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change—a retrospective cohort study[J] Int J Periodontics Restorative Dent. 2014;34(3):323–331. doi: 10.11607/prd.1821. [DOI] [PubMed] [Google Scholar]
- 20.Block MS. Maxillary fixed prosthesis design based on the preoperative physical examination[J] J Oral Maxillofac Surg. 2015;73(5):851–860. doi: 10.1016/j.joms.2014.12.027. [DOI] [PubMed] [Google Scholar]
- 21.Phillips K, Wong KM. Space requirements for implant-retained bar-and-clip overdentures[J] Compend Contin Educ Dent. 2001;22(6):516–518, 520, 522. [PubMed] [Google Scholar]
- 22.McGarry TJ, Nimmo A, Skiba JF, et al. Classification system for complete edentulism. The American college of prosthodontics[J] J Prosthodont. 1999;8(1):27–39. doi: 10.1111/j.1532-849x.1999.tb00005.x. [DOI] [PubMed] [Google Scholar]
- 23.Maló P, Nobre Mde A, Lopes I. A new approach to rehabilitate the severely atrophic maxilla using extramaxillary anchored implants in immediate function: a pilot study[J] J Prosthet Dent. 2008;100(5):354–366. doi: 10.1016/S0022-3913(08)60237-1. [DOI] [PubMed] [Google Scholar]