

Abstract
Objective
Carotid endarterectomy (CEA) is the gold standard surgical procedure for managing carotid stenosis due to atherosclerosis and reducing the risk of ischemic stroke. This bibliometric analysis summarizes the most-cited articles on CEA and highlights the contributing articles to today’s evidence-based practice.
Methods
A title-specific search using the Scopus database was used to perform the search. Pertinent article-based, journal-based, and author-based parameters were obtained for review.
Results
A total of 6,824 articles were published between 1970 and 2020. The top 100 most-cited articles accumulated a total of 54,153 citations with an average citation count (CC) of 541, with only a 4.53% self-citation rate for all authors. The publication trends peaked between 1997 and 2010, in which two-third of the highly cited works were published. The most prolific categories with top citations are the clinical, indications, and management, in a descending order. There were 41 published Randomized Controlled Trials (RCT) in the most-cited list.
Conclusions
Citation analysis on carotid endarterectomy has witnessed a marked shift in the publication trends from studying the outcome and complications to comparing carotid stenting with endarterectomy. This analysis is a good introductory article to physicians interested in this topic, as it summarizes the highly impactful articles and enlists the most-cited RCT on CEA.
Keywords: Carotid artery stenosis, Carotid endarterectomy, Stroke, Bibliometric analysis, Citation analysis
INTRODUCTION
Carotid endarterectomy (CEA) is a surgical technique where an atheromatous plaque is dissected and removed from the carotid intima-media space, to prevent an ischemic stroke. The first CEA was performed by Raul Carrea in 1951 [7]. The utility of CEA in preventing stroke was proven by various RCTs and is considered the gold standard in managing extracranial carotid atherosclerotic disease [4,11,14].
After the proper introduction and definition of bibliometric analysis type studies in 1969, it has gained wide acceptance and popularity by the scientific community [15]. Bibliometric analysis is a study of the most impactful articles to their respective fields, based on article and journal citometric evaluation. In addition, it summarizes the chronological trends of the most impactful publications to interested readers. Evidence-based studies are carefully reviewed to demonstrate contemporary evidence-based approaches to a disease for physicians in related medical specialties. Many citation analyses were published in neurosurgery; herein, we are presenting the first bibliometric study of the most cited publications on CEA [3,5,6].
MATERIALS AND METHODS
The bibliometric based search on the most-cited articles on CEA was performed using the Scopus database in June 2020. A title-specific keyword-based search with no restriction to the time of publication was executed. The search keyword was “Carotid Endarterectomy.” The identified studies were ranked based on their citation count in descending order and the most-cited 100 articles were selected for further analysis.
Information of interest to bibliometric analysis were obtained which included twelve parameters. The article’s citation count, articles citation count, authors H-index, Journal’s Source Normalized Impact Per Paper (SNIP), Journal’s SCImago Journal Rank (SJR), journal’s Impact Factor (IF), article’s title, contributing authors, specialty of the most contributing authors, contributing journal, corresponding author’s affiliation, and country of contribution. The obtained 100 top studies on CAE were categorized into the following five categories: clinical, clinicoradiological, complications, management, and management indications. Since this study did not incorporate any patients or patient information, an IRB was not required.
RESULTS
The Scopus bibliometric based search showed that 6,824 articles were published between 1970 and 2020 on CEA. The top 100 most cited articles were published between 1970 and 2016. The top-100 articles received an accumulative citation count of 54,153 and an average citation count of 541 citations per paper (Table 1). The identified rate of self-citation among all authors in the top100 articles; accounted for 4.53% from the overall citation count. The publication trends on CEA were continually active between 1997 and 2010 comprising the time for twothird of the top-cited articles publication time (Fig. 1) Clinical studies and studies on the management indications were the most studied category in approximately two-third of the most-cited articles on CEA (Fig. 2).
Table 1.
The top 100 most-cited articles on CEA
| Rank | Authors | Title | Year | Journal | CC | CY |
|---|---|---|---|---|---|---|
| 1st | Taylor D.W. et al. | Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis | 1991 | New England Journal of Medicine | 7064 | 243.58 |
| 2nd | Michael D. Walker. et al. | Endarterectomy for asymptomatic carotid artery stenosis | 1995 | JAMA: The Journal of the American Medical Association | 4643 | 185.72 |
| 3rd | Barnett H.J.M. et al. | Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis | 1998 | New England Journal of Medicine | 2692 | 122.36 |
| 4th | Warlow C. et al. | Randomised trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST) | 1998 | Lancet | 2601 | 118.22 |
| 5th | Yadav J.S. et al. | Protected carotid-artery stenting versus endarterectomy in high-risk patients | 2004 | New England Journal of Medicine | 2348 | 146.75 |
| 6th | Brott T.G. et al. | Stenting versus endarterectomy for treatment of carotid-artery stenosis | 2010 | New England Journal of Medicine | 1931 | 193.1 |
| 7th | Halliday A. et al. | Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: Randomised controlled trial | 2004 | Lancet | 1856 | 116 |
| 8th | Mas J.L. et al. | Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis | 2006 | New England Journal of Medicine | 1293 | 92.35 |
| 9th | Ringleb P.A. et al. | 30 day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial | 2006 | Lancet | 1192 | 85.14 |
| 10th | Rothwell P.M. et al. | Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis | 2003 | Lancet | 1154 | 67.88 |
| 11th | Hobson R.W. et al. | Efficacy of carotid endarterectomy for asymptomatic carotid stenosis | 1993 | New England Journal of Medicine | 1117 | 41.37 |
| 12th | Rothwell P.M. et al. | Endarterectomy for symptomatic carotid stenosis in relation to clinical subgroups and timing of surgery | 2004 | Lancet | 1081 | 67.56 |
| 13th | Ederle J. et al. | Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (international carotid stenting study): An interim analysis of a randomised controlled trial | 2010 | The Lancet | 951 | 95.1 |
| 14th | Mayberg M.R. et al. | Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis | 1991 | JAMA: The Journal of the American Medical Association | 765 | 26.37 |
| 15th | Ferguson G.G. et al. | The north american symptomatic carotid endarterectomy trial: Surgical results in 1415 patients | 1999 | Stroke | 764 | 36.38 |
| 16th | Barnett H.J.M. | Original contributions north american symptomatic carotid endarterectomy trial: Methods, patient characteristics, and progress | 1991 | Stroke | 751 | 25.89 |
| 17th | Sundt Jr. T.M. et al. | Correlation of cerebral blood flow and electroencephalographic changes during carotid endarterectomy. With results of surgery and hemodynamics of cerebral ischemia | 1981 | Mayo Clinic Proceedings | 611 | 15.67 |
| 18th | Eckstein H.H. et al. | Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: A multinational, prospective, randomised trial | 2008 | The Lancet Neurology | 603 | 50.25 |
| 19th | Gurm H.S. et al. | Long-term results of carotid stenting versus endarterectomy in high-risk patients | 2008 | New England Journal of Medicine | 601 | 50.08 |
| 20th | Halliday A. et al. | 10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): A multicentre randomised trial | 2010 | The Lancet | 491 | 49.1 |
| 21st | Mas J.L. et al. | Endarterectomy Versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S) trial: results up to 4 years from a randomised, multicentre trial | 2008 | The Lancet Neurology | 467 | 38.916 |
| 22nd | Taylor D.W. et al. | Low-dose and high-dose acetylsalicylic acid for patients undergoing carotid endarterectomy: A randomised controlled trial | 1999 | Lancet | 442 | 21.04 |
| 23rd | Spencer M.P. et al. | Detection of middle cerebral artery emboli during carotid endarterectomy using transcranial doppler ultrasonography | 1990 | Stroke | 438 | 14.6 |
| 24th | Naylor A.R. et al. | Randomized study of carotid angioplasty and stenting versus carotid endarterectomy: A stopped trial | 1998 | Journal of Vascular Surgery | 438 | 19.90 |
| 25th | Wennberg D.E. et al. | Variation in carotid endarterectomy mortality in the medicare population: Trial hospitals, volume, and patient characteristics | 1998 | Journal of the American Medical Association | 430 | 19.54 |
| 26th | Gray-Weale A.C. et al. | Carotid artery atheroma: Comparison of preoperative B-mode ultrasound appearance with carotid endarterectomy specimen pathology | 1988 | Journal of Cardiovascular Surgery | 423 | 13.21 |
| 27th | Biller J. et al. | Guidelines for carotid endarterectomy: A statement for healthcare professionals from a special writing group of the stroke council, american heart association | 1998 | Circulation | 421 | 19.13 |
| 28th | Moore W.S. et al. | Guidelines for carotid endarterectomy: A multidisciplinary consensus statement from the ad hoc committee, american heart association | 1995 | Stroke | 416 | 16.64 |
| 29th | Bonati L.H. et al. | New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: A substudy of the International Carotid Stenting Study (ICSS) | 2010 | The Lancet Neurology | 410 | 41 |
| 30th | Chaturvedi S. et al. | Carotid endarterectomy - an evidence-based review: Report of the therapeutics and technology assessment subcommittee of the american academy of neurology | 2005 | Neurology | 399 | 26.6 |
| 31st | Moneta G.L. et al. | Correlation of North American Symptomatic Carotid Endarterectomy Trial (NASCET) angiographic definition of 70% to 99% internal carotid artery stenosis with duplex scanning | 1993 | Journal of Vascular Surgery | 379 | 14.03 |
| 32nd | Winslow C.M. et al. | The appropriateness of carotid endarterectomy | 1988 | New England Journal of Medicine | 364 | 11.375 |
| 33rd | Rothwell P.M., Warlow C.P. | Prediction of benefit from carotid endarterectomy in individual patients: A risk-modelling study from (ECST) | 1999 | Lancet | 342 | 16.28 |
| 34th | Brooks W.H. et al. | Carotid angioplasty and stenting versus carotid endarterectomy: Randomized trial in a community hospital | 2001 | Journal of the American College of Cardiology | 341 | 17.94 |
| 35th | Brown M.M. | Short-term outcome after stenting versus endarterectomy for symptomatic carotid stenosis: A preplanned meta-analysis of individual patient data | 2010 | The Lancet | 332 | 33.2 |
| 36th | Sundt Jr. T.M., Sandok B.A., Whisnant J.P. | Carotid endarterectomy. Complications and preoperative assessment of risk | 1975 | Mayo Clinic Proceedings | 314 | 6.97 |
| 37th | Brott T.G. et al. | Long-term results of stenting versus endarterectomy for carotid-artery stenosis | 2016 | New England Journal of Medicine | 302 | 75.5 |
| 38th | Rothwell P.M., Slattery J., Warlow C.P. | Clinical and angiographic predictors of stroke and death from carotid endarterectomy: Systematic review | 1997 | British Medical Journal | 299 | 13 |
| 39th | Sharbrough F.W. et al. | Correlation of continuous electroencephalograms with cerebral blood flow measurements during carotid endarterectomy | 1973 | Stroke | 295 | 6.27 |
| 40th | Rothwell P.M., Slattery J., Warlow C.P. | A systematic review of the risks of stroke and death due to endarterectomy for symptomatic carotid stenosis | 1996 | Stroke | 285 | 11.87 |
| 41st | Piepgras D.G. et al. | Intracerebral hemorrhage after carotid endarterectomy | 1988 | Journal of Neurosurgery | 284 | 8.87 |
| 42nd | Jackson L.A. et al. | Isolation of Chlamydia pneumoniae from a carotid endarterectomy specimen | 1997 | Journal of Infectious Diseases | 282 | 12.26 |
| 43rd | Riles T.S. et al. | The cause of perioperative stroke after carotid endarterectomy | 1994 | Journal of Vascular Surgery | 261 | 10.03 |
| 44th | Gasecki A.P. et al. | Long-term prognosis and effect of endarterectomy in patients with symptomatic severe carotid stenosis and contralateral carotid stenosis or occlusion: Results from NASCET | 1995 | Journal of Neurosurgery | 259 | 10.36 |
| 45th | NASCET investigators | Clinical alert: Benefit of carotid endarterectomy for patients with high-grade stenosis of the internal carotid artery. National Institute of Neurological Disorders and Stroke, Stroke and Trauma Division | 1991 | Stroke | 257 | 8.86 |
| 46th | Chambers B.R., Donnan G.A. | Carotid endarterectomy for asymptomatic carotid stenosis. | 2005 | Cochrane Database of Systematic Reviews (online) | 248 | 16.53 |
| 47th | Samra S.K. et al. | Evaluation of a cerebral oximeter as a monitor of cerebral ischemia during carotid endarterectomy | 2000 | Anesthesiology | 248 | 12.4 |
| 48th | Jordan Jr. W.D. et al. | Microemboli detected by transcranial Doppler monitoring in patients during carotid angioplasty versus carotid endarterectomy | 1999 | Cardiovascular Surgery | 239 | 11.38 |
| 49th | Slattery J. | Endarterectomy for moderate symptomatic carotid stenosis: Interim results from the MRC european carotid surgery trial | 1996 | Lancet | 236 | 9.83 |
| 50th | Bonati L.H. et al. | Long-term outcomes after stenting versus endarterectomy for treatment of symptomatic carotid stenosis: The International Carotid Stenting Study (ICSS) randomised trial | 2015 | The Lancet | 236 | 47.2 |
| 51st | Silver F.L. et al. | Safety of stenting and endarterectomy by symptomatic status in the Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST) | 2011 | Stroke | 235 | 26.11 |
| 52nd | Bond R., Rerkasem K., Rothwell P.M. | Systematic review of the risks of carotid endarterectomy in relation to the clinical indication for and timing of surgery | 2003 | Stroke | 234 | 13.76 |
| 53rd | Mantese V.A. et al. | The carotid revascularization endarterectomy versus stenting trial (CREST): Stenting versus carotid endarterectomy for carotid disease | 2010 | Stroke | 226 | 22.6 |
| 54th | Lal B.K. et al. | Restenosis after carotid artery stenting and endarterectomy: A secondary analysis of CREST, a randomised controlled trial | 2012 | The Lancet Neurology | 225 | 28.125 |
| 55th | David O.W. et al. | Results of a randomized controlled trial of carotid endarterectomy for asymptomatic carotid stenosis | 1992 | Mayo Clinic Proceedings | 225 | 8.03 |
| 56th | Thompson J.E., Austin D.J., Patman R.D. | Carotid endarterectomy for cerebrovascular insufficiency: Long-term results in 592 patients followed up to thirteen years | 1970 | Annals of surgery | 220 | 4.4 |
| 57th | Morgenstern L.B. et al. | The risks and benefits of carotid endarterectomy in patients with near occlusion of the carotid artery | 1997 | Neurology | 216 | 9.39 |
| 58th | Toole J.F. et al. | Original contributions study design for randomized prospective trial of carotid endarterectomy for asymptomatic atherosclerosis | 1989 | Stroke | 214 | 6.90 |
| 59th | Coward L.J., Featherstone R.L., Brown M.M. | Safety and efficacy of endovascular treatment of carotid artery stenosis compared with carotid endarterectomy: A cochrane systematic review of the randomized evidence | 2005 | Stroke | 214 | 14.26 |
| 60th | Yadav J.S. et al. | Angioplasty and stenting for restenosis after carotid endarterectomy: Initial experience | 1996 | Stroke | 212 | 8.83 |
| 61st | Spencer M.P. | Transcranial doppler monitoring and causes of stroke from carotid endarterectomy | 1997 | Stroke | 212 | 9.21 |
| 62nd | McKinlay S.M. | Carotid Revascularization Using Endarterectomy or Stenting Systems (CaRESS) phase I clinical trial: 1-year results | 2005 | Journal of Vascular Surgery | 211 | 14.06 |
| 63rd | Debakey M.E. | Successful carotid endarterectomy for cerebrovascular insufficiency: Nineteen-year follow-up | 1975 | JAMA: The Journal of the American Medical Association | 210 | 4.66 |
| 64th | Naylor A.R. et al. | A systematic review of outcomes following staged and synchronous carotid endarterectomy and coronary artery bypass | 2003 | European Journal of Vascular and Endovascular Surgery | 210 | 12.35 |
| 65th | Schnaudigel S. et al. | New brain lesions after carotid stenting versus carotid endarterectomy: A systematic review of the literature | 2008 | Stroke | 210 | 17.5 |
| 66th | Zierler R.E. et al. | Carotid artery stenosis following endarterectomy | 1982 | Archives of Surgery | 209 | 5.5 |
| 67th | O'donnell T.F. et al. | Correlation of B-mode ultrasound imaging and arteriography with pathologic findings at carotid endarterectomy | 1985 | Archives of Surgery | 207 | 5.91 |
| 68th | Sundt Jr T.M. et al. | Cerebral blood flow measurements and electroencephalograms during carotid endarterectomy | 1974 | Journal of Neurosurgery | 206 | 4.47 |
| 69th | Moritz S. et al. | Accuracy of cerebral monitoring in detecting cerebral ischemia during carotid endarterectomy: A comparison of transcranial Doppler sonography, near-infrared spectroscopy, stump pressure, and somatosensory evoked potentials | 2007 | Anesthesiology | 203 | 15.61 |
| 70th | Ogasawara K. et al. | Intracranial hemorrhage associated with cerebral hyperperfusion syndrome following carotid endarterectomy and carotid artery stenting: Retrospective review of 4494 patients | 2007 | Journal of Neurosurgery | 202 | 15.5 |
| 71st | Brooks W.H. et al. | Carotid angioplasty and stenting versus carotid endarterectomy for treatment of asymptomatic carotid stenosis: A randomized trial in a community hospital | 2004 | Neurosurgery | 198 | 12.37 |
| 72nd | Rothwell P.M. et al. | Treating individuals 3: From subgroups to individuals: General principles and the example of carotid endarterectomy | 2005 | Lancet | 192 | 12.8 |
| 73rd | Featherstone R.L., Brown M.M., Coward L.J. | International Carotid Stenting Study (ICSS): Protocol for a randomised clinical trial comparing carotid stenting with endarterectomy in symptomatic carotid artery stenosis | 2004 | Cerebrovascular Diseases | 191 | 11.93 |
| 74th | Easton J.D., Sherman D.G. | Stroke and mortality rate in carotid endarterectomy: 228 consecutive operations | 1977 | Stroke | 188 | 4.37 |
| 75th | Meyer F.B. et al. | Emergency carotid endarterectomy for patients with acute carotid occlusion and profound neurological deficits | 1986 | Annals of Surgery | 186 | 5.47 |
| 76th | McCrory D.C. et al. | Predicting complications of carotid endarterectomy | 1993 | Stroke | 185 | 6.8 |
| 77th | Cebul R.D. et al. | Indications, outcomes, and provider volumes for carotid endarterectomy | 1998 | Journal of the American Medical Association | 183 | 8.31 |
| 78th | Bonati L.H. et al. | Long-term risk of carotid restenosis in patients randomly assigned to endovascular treatment or endarterectomy in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): Long-term follow-up of a randomised trial | 2009 | The Lancet Neurology | 183 | 16.63 |
| 79th | Gaunt M.E. et al. | Clinical relevance of intraoperative embolization detected by transcranial Doppler ultrasonography during carotid endarterectomy: A prospective study of 100 patients | 1994 | British Journal of Surgery | 183 | 7.03 |
| 80th | Wade J.G. et al. | Effect of carotid endarterectomy on carotid chemoreceptor and baroreceptor function in man | 1970 | New England Journal of Medicine | 180 | 3.6 |
| 81st | Payne D.A. et al. | Beneficial effects of clopidogrel combined with aspirin in reducing cerebral emboli in patients undergoing carotid endarterectomy | 2004 | Circulation | 180 | 11.25 |
| 82nd | Reigel M.M. et al. | Cerebral hyperperfusion syndrome: A cause of neurologic dysfunction after carotid endarterectomy | 1987 | Journal of Vascular Surgery | 178 | 5.39 |
| 83rd | Hertzer N.R. et al. | A prospective study of vein patch angioplasty during carotid endarterectomy: Three-year results for 801 patients and 917 operations | 1987 | Annals of Surgery | 176 | 5.33 |
| 84th | Hertzer N.R. et al. | Early outcome assessment for 2228 consecutive carotid endarterectomy procedures: The cleveland clinic experience from 1989 to 1995 | 1997 | Journal of Vascular Surgery | 174 | 7.56 |
| 85th | Tu J.V. et al. | The fall and rise of carotid endarterectomy in the United States and Canada | 1998 | New England Journal of Medicine | 174 | 7.90 |
| 86th | Thompson J.E., Patman R.D., Talkington C.M. | Asymptomatic carotid bruit: Long-term outcome of patients having endarterectomy compared with unoperated controls | 1978 | Annals of Surgery | 172 | 4.09 |
| 87th | Ederle J. et al. | Endovascular treatment with angioplasty or stenting versus endarterectomy in patients with carotid artery stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): Long-term follow-up of a randomised trial | 2009 | The Lancet Neurology | 171 | 15.54 |
| 88th | Levi C.R. et al. | Transcranial Doppler detected cerebral microembolism following carotid endarterectomy. High microembolic signal loads predict postoperative cerebral ischaemia | 1997 | Brain | 170 | 7.39 |
| 89th | Hays R.J., Levinson S.A., Wylie E.J. | Intraoperative measurement of carotid back pressure as a guide to operative management for carotid endarterectomy | 1972 | Surgery | 170 | 3.54 |
| 90th | Bernstein M., Fleming J.F.R., Deck J.H.N. | Cerebral hyperperfusion after carotid endarterectomy: A cause of cerebral hemorrhage | 1984 | Neurosurgery | 168 | 4.66 |
| 91st | McKinlay S. et al. | Carotid Revascularization Using Endarterectomy or Stenting Systems (CARESS): Phase I clinical trial | 2003 | Journal of Endovascular Therapy | 167 | 9.82 |
| 92nd | Ennix C.L. et al. | Improved results of carotid endarterectomy in patients with symptomatic coronary disease: An analysis of 1,546 consecutive carotid operations | 1979 | Stroke | 166 | 4.04 |
| 93rd | Blaser T. et al. | Risk of stroke, transient ischemic attack, and vessel occlusion before endarterectomy in patients with symptomatic severe carotid stenosis | 2002 | Stroke | 166 | 9.2 |
| 94th | Barnett H.J.M., Meldrum H.E., Eliasziw M. | The appropriate use of carotid endarterectomy | 2002 | CMAJ | 166 | 9.2 |
| 95th | Cowan Jr. J.A. et al. | Surgeon volume as an indicator of outcomes after carotid endarterectomy: An effect independent of specialty practice and hospital volume | 2002 | Journal of the American College of Surgeons | 166 | 9.2 |
| 96th | Hannan E.L. et al. | Relationship between provider volume and mortality for carotid endarterectomies in New York State | 1998 | Stroke | 165 | 7.5 |
| 97th | Goldstein L.B. et al. | Multicenter review of preoperative risk factors for endarterectomy for asymptomatic carotid artery stenosis | 1998 | Stroke | 163 | 7.40 |
| 98th | Solomon R.A. et al. | Incidence and etiology of intracerebral hemorrhage following carotid endarterectomy | 1986 | Journal of Neurosurgery | 163 | 4.79 |
| 99th | Hobson II, R.W. | CREST (Carotid Revascularization Endarterectomy Versus Stent Trial): Background, design, and current status | 2000 | Seminars in Vascular Surgery | 161 | 8.05 |
| 100th | Rothwell, P.M., Slattery, J., Warlow, C.P. | A systematic comparison of the risks of strokeand death due to carotid endarterectomy for symptomatic and asymptomatic stenosis | 1996 | Stroke | 160 | 6.6 |
CEA, carotid endarterectomy; CC, citations count; CY, citations per year
Fig. 1.
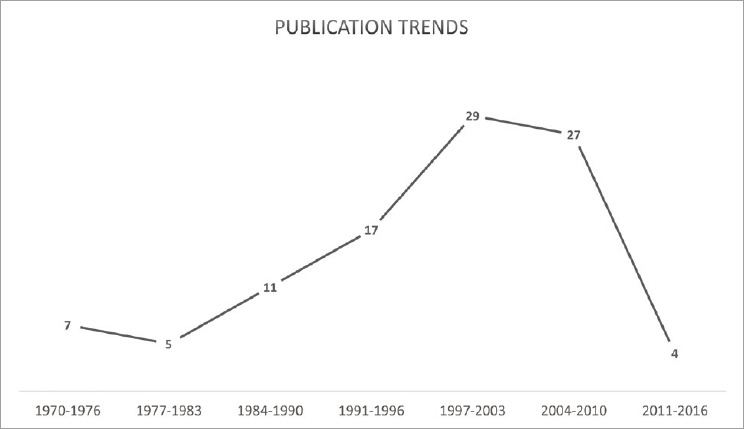
Line chart demonstrating the chronological trend with the highest publication in the years 1997-2003.
Fig. 2.
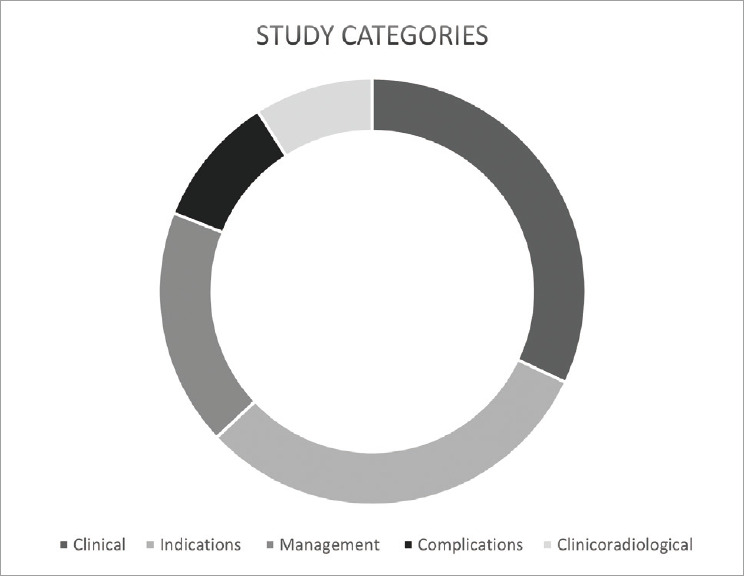
Pie chart with study categories of publications mostly concentrated on the clinical and indications categories.
The number 1 article on CEA is a RCT authored by Taylor et al., 1991 in New England Journal entitled “Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis” in which it received 7064 citations and 243 citations per year. The bibliometric based search has identified 41 clinical trials on carotid endarterectomy. The most prolific author was Barnett, H.J.M a neurologist in which he authored 11 articles in the top 100 list (Fig. 3). The University College London was the most active participating institute by producing 15 articles on the list (Fig. 4). Assessment of journals showed that Stroke was the most active journal by publishing 22 articles in the list (Fig. 5). The United States of America was the source of publication in 56 articles on the list (Fig. 6).
Fig. 3.
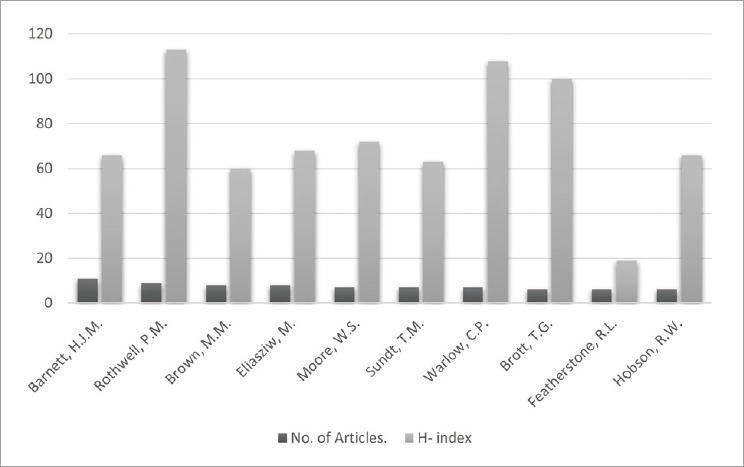
Bar chart of the most contributing authors in carotid endarterectomy.
Fig. 4.
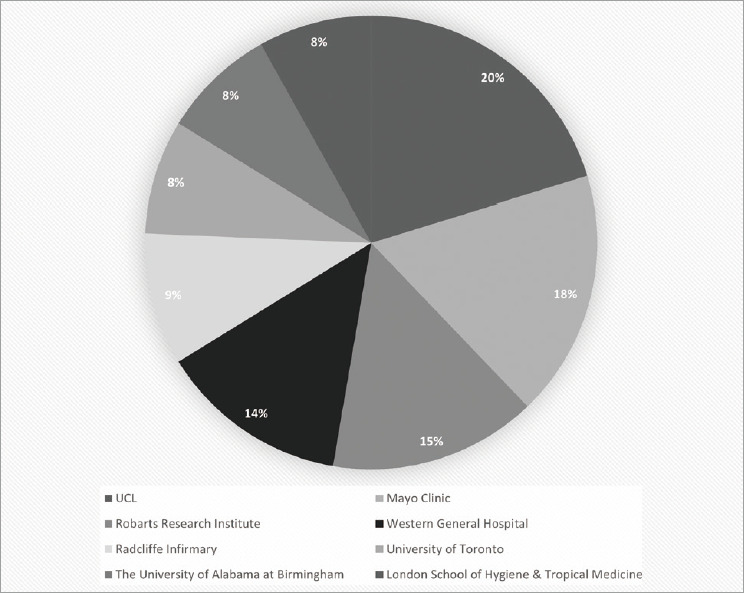
Pie chart demonstrating the top contributing institutions in carotid endarterectomy.
Fig. 5.
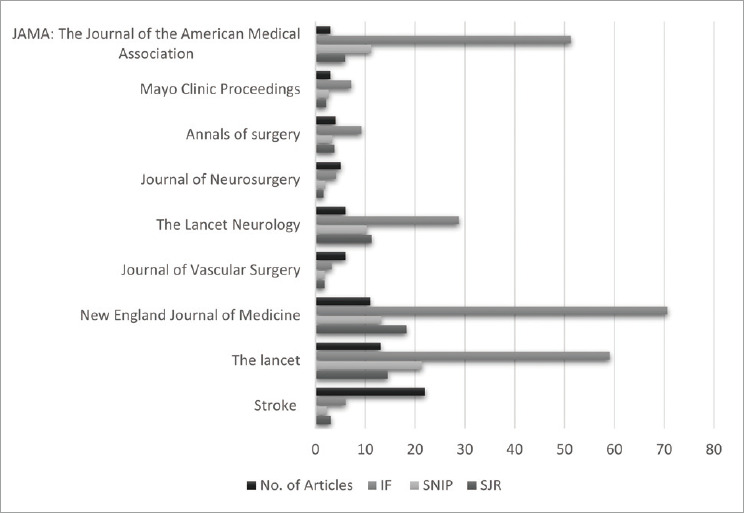
Bar chart demonstrating the top contributing journals in publishing articles of carotid endarterectomy.
Fig. 6.
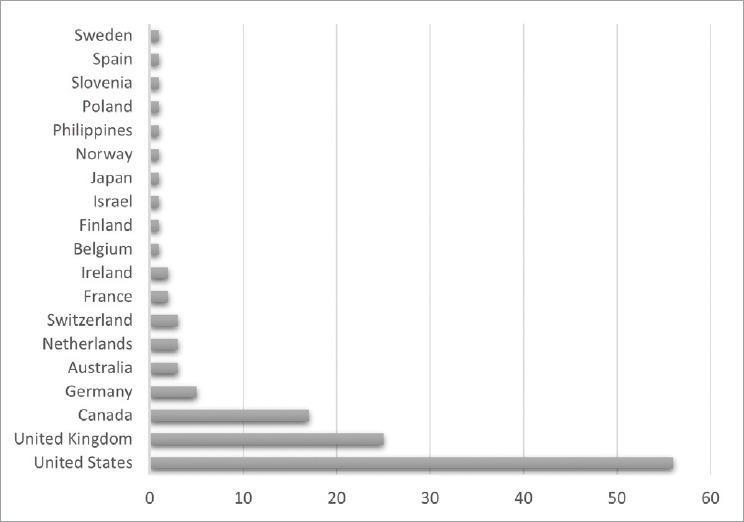
Bar chart demonstrating the most contributing countries in publishing carotid endarterectomy studies.
DISCUSSION
During the 1970s, publications were mainly focused on the short and long-term outcomes of CEA, complications of the procedure, and the usefulness of CEA in patients with asymptomatic carotid atherosclerosis. In the 1980s, more publications were focused on the short and long-term complications of CEA, especially cerebral hyperperfusion with the ensuing intracerebral hemorrhage, and the recurrence of carotid atherosclerosis post CEA. In addition, some articles studied the efficacy and outcome of emergency CEA. The 1990s witnessed a major shift geared by the production of major RCT, primarily analyzing the indications and outcomes of CEA in symptomatic and asymptomatic carotid atherosclerosis. In contrast, the 21st century was flourishing with more RCTs that compared the outcomes and complications between CEA and carotid stenting. Various systematic review and meta-analyses studies were published in the 21st century, comparing the efficacy of CEA to medical management, and comparing CEA to endovascular treatment.
The highest cited article in the top 100 list, and the indications category, is an RCT with 7064 Citations Count (CC) and 243 Citations per Year (CY) is “Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis” by the North American Symptomatic Carotid Endartrectomy Trial Collaborators in 1991 published by the New England Journal of Medicine. The trial resulted in significant findings that most vascular surgeons and neurosurgeons adopted the results. The aggregate risk of any ipsilateral stroke at two years was 9% in patients who underwent CEA, and 26% in patients who received best medical management; the absolute risk reduction was 17±3.5% (p-value=<0.001). The overall risk of fatal or major ipsilateral was 13.1% in medically treated patients and 2.5% in patients who underwent CEA; the absolute risk reduction was 10.6±2.6% (p-value=<0.001) [12].
The second highest cited article, and the second highest in the indications category, with 4643 CC and 185 CY is “Endarterectomy for Asymptomatic Carotid Artery Stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study’’ by Walker et al., 1995 in the Journal of the American Medical Association. The trial randomized patients into an aspirin-treated group with medical risk factor management, and a CEA-treated group. Risk reduction of the cumulative 5-year risk of ipsilateral stroke and any perioperative stroke and death was noted to be 5.1% for the CEA group, and 11% for the medical management group (aggregate risk reduction of 53%). The authors concluded that CEA is indicated for patients ≤75 years, with asymptomatic carotid atherosclerosis who have a ≥60% stenosis and ≤3% risk of perioperative morbidity and mortality will have a lower 5-year aggregate risk of ipsilateral stroke [21].
Clinical category
The clinical category has the highest number of publications, with multiple RCTs. From 1970-2010s, studies were mainly reviewing and assessing the outcome and complications of CEA, relative to medical management and carotid stenting. The highest article in the category (ranked 20th overall), with 491 CC and 49.1 CY, is “10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): A multicentre randomised trial” by Halliday et al., 2010 in Lancet. The study incorporated asymptomatic patients with carotid atherosclerosis and were randomized to immediate CEA group and deferral CEA group. The stroke risk at 5-years was 4.1% in the immediate CEA group, and 10% in the deferred CEA group; the 10-year stroke risk was 10.8% and 16.9% in the immediate and deferred CEA groups, respectively. Ratio of the stroke incidence rate was 0.54 (95% CI: 0.43 – 0.68; p-value=<0.0001) [10].
The second highest article in the category (ranked 25th overall), with 430 CC and 19 CY, is “Variation in carotid endarterectomy mortality in the medicare population: Trial hospitals, volume, and patient characteristics” by Wennberg et al., 1998 in the Journal of the American Medical Association. The authors reviewed the 30-day perioperative mortality rate in the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the Asymptomatic Carotid Atherosclerosis Study (ACAS), compared to Medicare-insured patients treated in hospitals that did and didn’t participate in the trial. They demonstrated a mortality rate of 1.4% at trial hospitals, 1.7% in non-trial high volume hospitals, 1.9% in non-trial average volume hospitals, and 2.5% in non-trial low volume hospitals. The authors concluded that Medicare-insured patients had a higher mortality rate, even in hospitals who participated in NASCET and ACAS. Therefore, they advised caution in inferring trial’s mortality rate to the general everyday practice hospitals [22].
Indications category
The indications category has the highest number of RCTs, with the main goal of comparing CEA and carotid stenting. The third highest cited article in the category (ranked 3rd overall), with 2692 CC and 122 CY, is “Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis” by Barnett et al., 1998 in the New England Journal of Medicine. Patients were categorized into mild (<50%) and moderate (50-69%) carotid stenosis and were divided into CEA-treated group and medical management alone group. Patients with moderate stenosis had a 15.7% 5-year risk of any ipsilateral stroke, versus 22.2% in patients with medical management alone (p-value=0.045). Conversely, patients with mild stenosis didn’t have a notable difference between the CEA group (14.9%) and the medical management group (18.7%; p-value=<0.16). Hence, a moderate benefit of CEA is seen in patients with moderate stenosis [1].
The fourth highest cited article in this category (ranked 4th overall), with 2601 CC and 118 CY, is “Randomised trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST)” by Warlow et al., 1998 in Lancet. The authors randomized patients with carotid stenosis to CEA-treated group and control group with delay of CEA. The 3-year risk of major stroke or mortality was 26.5% for the control group, and 14.9% for the CEA group. The conclusion of the study was that CEA is indicated for patients with >80% stenosis, as the morbidity of non-operation is higher than the risk of surgery; with taking consideration to the age and gender of the patient [9].
The fifth highest cited article in the indication category (ranked 5th overall), with 2348 CC and 146 CY, is “Protected carotid-artery stenting versus endarterectomy in high-risk patients’’ by Yadav et al., 2004 in the New England Journal of Medicine. Patients were randomized to CEA-treated group and stent with an emboli protection device group. Results showed non-inferiority of carotid stenting with emboli protection device (cumulative incidence of 12.2%), compared to CEA-treated group (cumulative incidence of 20.1%; non-inferiority p-value=0.004) [23].
Management category
The management first started with publications in the correlation of electroencephalogram (EEG) and cerebral blood flow intraoperatively in detecting intraoperative cerebral ischemia. Later, studies focused on the use of intraoperative doppler ultrasound in identifying cerebral ischemia. Many authors focused on medication use with CEA to reduce stroke risk, such as the use of high vs. low dose aspirin, or the combination of aspirin and clopidogrel. Some studies reviewed the association of mortality and surgeon’s volume. The highest cited article in the category (ranked 17th overall), with 611 CC and 15 CY, is “Correlation of cerebral blood flow and electroencephalographic changes during carotid endarterectomy: with results of surgery and hemodynamics of cerebral ischemia” by Sundt et al., 1981 in Mayo Clinic Proceedings. The study found that EEG had a positive correlation with cerebral blood flow, and the authors concluded a good prediction of postoperative outcome based on intraoperative EEG fluctuations [19].
The second highest cited article in the category (ranked 22nd overall), with 442 CC and 21 CY, is “Low-dose and high-dose acetylsalicylic acid for patients undergoing carotid endarterectomy: A randomized controlled trial” by Taylor et al., 1999 in Lancet. The authors found that low dose aspirin (81 and 325 mg) was associated with a lower risk of myocardial infarction, stroke, and mortality within 30 days and 3 months of CEA than high dose group (650 mg and 1300 mg) [20].
The highest cited article in the 21st century (ranked 47th overall), with 248 CC and 12 CY, is “Evaluation of a cerebral oximeter as a monitor of cerebral ischemia during carotid endarterectomy” by Samra et al., 2000 in Anesthesiology. The authors measured regional cerebral oxygen saturation in patients who developed neurological deficits compared to those with no neurological deficits during carotid occlusion in CEA. There was a noticeable 20% reduction threshold in oxygen saturation before developing neurological symptoms (p=.0002) [17].
Complications category
The complications category assessed the association of cerebral hyperperfusion to intracerebral hemorrhage. The highest cited article (ranked 36th overall), with 314 CC and 6.9 CY, is “Carotid endarterectomy. Complications and preoperative assessment of risk” by Sundt et al., 1975 in Mayo Clinic Proceedings. The authors divided the preoperative risk of myocardial infarction and residual mild to severe stroke based on neurological status, with medical and angiographic. Group 1 (1% risk) are patients with no neurological deficits and no medical or angiographic risk factors. Group 2 (2%) are patients with no neurological deficits and no medical risk factors, but with angiographic risk factors. Group 3 (7%) are patients with no neurological deficits; however, they have medical risk factors, with or without angiographic risk factors. Group 4 (10%) are patients who have neurological deficits [16].
The second highest cited article in the category (ranked 40th overall), with 285 CC and 11 CY, is “A systematic review of the risks of stroke and death due to endarterectomy for symptomatic carotid stenosis” by Rothwell et al., 1996 in Stroke. The finding of this systematic review demonstrated a 1.62% mortality and 5.64% of stroke or mortality [16].
The highest cited article in the 21st century (ranked 70th overall), with 202 CC and 15 CY, is “Intracranial hemorrhage associated with cerebral hyperperfusion syndrome following carotid endarterectomy and carotid artery stenting: Retrospective review of 4494 patients” by Ogasawara et al., 2007 in the Journal of Neurosurgery. All patients who underwent CEA and carotid artery stenting (CAS) who developed intracranial hemorrhage (ICH) were collected and studied. ICH developed at a rapid setting in the CAS group (12 hours) compared to the CEA group (6 days). Interestingly, inadequate blood pressure control was found to be significantly associated with ICH in CEA (P=.016) compared to CAS [13].
Clinicoradiological category
Multiple articles were published in this category which have correlated the pathological finding in carotid atherosclerosis using ultrasound and angiogram. In addition, there were multiple RCTs that studied the utility of ultrasound in predicting the degree of stenosis calculated on angiography. The highest cited article in the category (ranked 23rd overall), with 438 CC and 14 CY, is “Detection of middle cerebral artery emboli during carotid endarterectomy using transcranial doppler ultrasonography” by Spencer et al., 1990 in Stroke. Transcranial ultrasound of the middle cerebral artery proved to be efficacious in detecting emboli from the carotid artery, when correlated with the postoperative neurological status [18].
The second highest cited article in this category (ranked 26th overall), with 423 CC and 13 CY, is “Carotid artery atheroma: Comparison of preoperative B-mode ultrasound appearance with carotid endarterectomy specimen pathology” by Gray-Weale et al., 1988 in Journal of Cardiovascular Surgery. The authors demonstrated the correlation between ultrasound detection of heterogeneous signals and intraplaque hemorrhage and ulceration on pathological specimens (p-value<0.001) [8].
The highest cited article in the 21st century (ranked 29th overall), with 410 CC and 41 CY, is “New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a substudy of the International Carotid Stenting Study (ICSS)” by Bonati et al., 2010 in Lancet Neurology. Patients who underwent CAS were found to have a higher likelihood of ischemic changes on MRI at 1 day (p<.0001) and 1 month (p=.0003) post-stenting compared to CEA, and thus, confirms the notion that ischemic stroke is associated with CAS [2].
LIMITATIONS
Bibliometric review is a purely quantitative measure of the scientific community’s recognition rather than the reflection of the article’s impact in its respective field. Therefore, the usage of bibliometric in conjunction with peer reviewed articles provides a comprehensive overview on a certain topic. Inherited limitations exist in bibliometric studies which includes the citation accumulation overtime for old studies which can be counteracted by the use of the citation per year. Another limitation is the self-citation by authors which was minimal in our citation analysis on CEA (4.53%). Articles published after 2010 are focused on the comparison of CAS to CEA, hence, contemporary studies on CEA is lacking. Lastly, the coverage of the Scopus databases have an extensive citation tracking for articles published between 1970 and 2020 in which articles published prior to that might be underrepresented.
CONCLUSIONS
The CEA chronological trends have witnessed an initial surge in the short and long-term outcomes, and complications following CEA. Then multiple RCTs emerged in studying the indications of CEA in symptomatic and asymptomatic carotid atherosclerosis. The latest articles and RCTs focused on comparing CEA and carotid stenting. The topic of carotid atherosclerosis contains various RCTs that define the current evidence-based approach to this disease. The temporal trends and the most-cited articles and the published RCT are highlighted in this rich evidence-based guide article for today’s clinicians.
Footnotes
Disclosure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
REFERENCES
- 1.Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998 Nov;339:1415–25. doi: 10.1056/NEJM199811123392002. [DOI] [PubMed] [Google Scholar]
- 2.Bonati LH, Jongen LM, Haller S, Flach HZ, Dobson J, Nederkoorn PJ, et al. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a substudy of the International Carotid Stenting Study (ICSS) Lancet Neurol. 2010 Apr;9(4):353–62. doi: 10.1016/S1474-4422(10)70057-0. [DOI] [PubMed] [Google Scholar]
- 3.Burak Atci I, Yilmaz H, Samanci MY. The top 50 most-cited articles on low-grade glioma: a bibliometric analysis. Br J Neurosurg. 2019 Apr;33(2):171–5. doi: 10.1080/02688697.2018.1549314. [DOI] [PubMed] [Google Scholar]
- 4.Chambers BR, Donnan GA. Carotid endarterectomy for asymptomatic carotid stenosis. Cochrane Database Syst Rev. 2005 Oct;2005(4):CD001923. doi: 10.1002/14651858.CD001923.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Elarjani T, Almutairi OT, Alhussinan M, Alturkistani A, Alotaibi FS, Bafaquh M, et al. Bibliometric analysis of the top 100 most cited articles on craniosynostosis. Childs Nerv Syst. 2021 Feb;37(2):587–97. doi: 10.1007/s00381-020-04858-2. [DOI] [PubMed] [Google Scholar]
- 6.Elarjani T, Almutairi OT, Alhussinan M, Alzhrani G, Alotaibi FE, Bafaquh M, et al. Bibliometric Analysis of the Top 100 Most Cited Articles on Cerebral Vasospasm. World Neurosurg. 2021 Jan;145:e68–82. doi: 10.1016/j.wneu.2020.09.099. [DOI] [PubMed] [Google Scholar]
- 7.Friedman SG. The first carotid endarterectomy. J Vasc Surg. 2014 Dec;60:1703–8. doi: 10.1016/j.jvs.2014.08.059. [DOI] [PubMed] [Google Scholar]
- 8.Gray-Weale AC, Graham JC, Burnett JR, Byrne K, Lusby RJ. Carotid artery atheroma: comparison of preoperative B-mode ultrasound appearance with carotid endarterectomy specimen pathology. J Cardiovasc Surg (Torino) 1988 NovDec;29(6):676–81. [PubMed] [Google Scholar]
- 9.Group ECSTC. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998 May;351(9113):1379–87. [PubMed] [Google Scholar]
- 10.Halliday A, Harrison M, Hayter E, Kong X, Mansfield A, Marro J, et al. 10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): a multicentre randomised trial. Lancet. 2010 Sep;376(9746):1074–84. doi: 10.1016/S0140-6736(10)61197-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moore WS, Barnett HJ, Beebe HG, Bernstein EF, Brener BJ, Brott T, et al. Guidelines for carotid endarterectomy. A multidisciplinary consensus statement from the ad hoc Committee, American Heart Association. Stroke. 1995 Jan;26(1):188–201. doi: 10.1161/01.str.26.1.188. [DOI] [PubMed] [Google Scholar]
- 12.v. Barnett HJM, Taylor DW, Haynes RB, Sacket DL, Peerless SJ, et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991 Aug;325(7):445–53. doi: 10.1056/NEJM199108153250701. [DOI] [PubMed] [Google Scholar]
- 13.Ogasawara K, Sakai N, Kuroiwa T, Hosoda K, Iihara K, Toyoda K, et al. Intracranial hemorrhage associated with cerebral hyperperfusion syndrome following carotid endarterectomy and carotid artery stenting: retrospective review of 4494 patients. J Neurosurg. 2007 Dec;107(6):1130–6. doi: 10.3171/JNS-07/12/1130. [DOI] [PubMed] [Google Scholar]
- 14.Orrapin S, Rerkasem K. Carotid endarterectomy for symptomatic carotid stenosis. Cochrane Database Syst Rev. 2017 Jun;6(6):CD001081. doi: 10.1002/14651858.CD001081.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pritchard A. Statistical bibliography or bibliometrics? Journal of Documentation. 1969 Jan;25(4):348–9. [Google Scholar]
- 16.Rothwell PM, Slattery J, Warlow CP. A systematic review of the risks of stroke and death due to endarterectomy for symptomatic carotid stenosis. Stroke. 1996 Feb;27(2):260–5. doi: 10.1161/01.str.27.2.260. [DOI] [PubMed] [Google Scholar]
- 17.Samra SK, Dy EA, Welch K, Dorje P, Zelenock GB, Stanley JC. Evaluation of a cerebral oximeter as a monitor of cerebral ischemia during carotid endarterectomy. Anesthesiology. 2000 Oct;93(4):964–70. doi: 10.1097/00000542-200010000-00015. [DOI] [PubMed] [Google Scholar]
- 18.Spencer MP, Thomas GI, Nicholls SC, Sauvage LR. Detection of middle cerebral artery emboli during carotid endarterectomy using transcranial Doppler ultrasonography. Stroke. 1990 Mar;21(3):415–23. doi: 10.1161/01.str.21.3.415. [DOI] [PubMed] [Google Scholar]
- 19.Sundt TM, Jr, Sharbrough FW, Piepgras DG, Kearns TP, Messick JM, Jr, O’Fallon WM. Correlation of cerebral blood flow and electroencephalographic changes during carotid endarterectomy: with results of surgery and hemodynamics of cerebral ischemia. Mayo Clin Proc. 1981 Sep;56(9):533–43. [PubMed] [Google Scholar]
- 20.Taylor DW, Barnett HJ, Haynes RB, Ferguson GG, Sackett DL, Thorpe KE, et al. Low-dose and high-dose acetylsalicylic acid for patients undergoing carotid endarterectomy: a randomised controlled trial. ASA and Carotid Endarterectomy (ACE) Trial Collaborators. Lancet. 1999 Jun;353(9171):2179–84. doi: 10.1016/s0140-6736(99)05388-x. [DOI] [PubMed] [Google Scholar]
- 21.Walker MD, Marler JR, Goldstein M, Grady PA, Toole JF, Baker WH, et al. Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA. 1995 May;273(18):1421–8. [PubMed] [Google Scholar]
- 22.Wennberg DE, Lucas FL, Birkmeyer JD, Bredenberg CE, Fisher ES. Variation in carotid endarterectomy mortality in the Medicare population: trial hospitals, volume, and patient characteristics. JAMA. 1998 Apr;279(16):1278–81. doi: 10.1001/jama.279.16.1278. [DOI] [PubMed] [Google Scholar]
- 23.Yadav JS, Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004 Oct;351:1493–501. doi: 10.1056/NEJMoa040127. [DOI] [PubMed] [Google Scholar]