

Dear Editor,
With the advent of newer cataract techniques, there has been significant improvement in patients’ postoperative (PO) recovery. However, dependency on PO steroid eye drops poses challenges such as improper technique, contamination, compliance issues, and microtrauma to eye.[1] Subtenon depot corticosteroid injection is a well-accepted treatment option for various inflammatory eye diseases.[2] Subconjunctival triamcinolone acetonide (SCTA) depot injection at the end of phacoemulsification (less-drop approach) was suggested to avoid dependency on PO steroid drops.[1,3] Previous studies did not report any serious adverse event with this approach. Among 1129 eyes that underwent less-drop-approach cataract surgery, acute central serous chorioretinopathy (CSCR) was seen in three eyes (0.26%) following this novel approach at our center.
Case Reports
Patient demographics and clinical characteristics are presented in Table 1.
Table 1.
Showing the demographics, clinical characteristics, and mode of management in each patient
| Case | Age/Gender | Systemic illness | Eye | IOP | Type of surgery | Vision at diagnosis | SFCT | Modality of treatment | Final outcome | Follow up |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 66/M | Nil | LE | WNL | PE + anterior SCTA (6 mg/0.15 mL) | 6/9 | 422 µm | Focal laser | 6/6, Resolved CSCR | 4 months |
| 2 | 54/M | DM | RE | WNL | PE + anterior SCTA (6 mg/0.15 mL) | 6/6 | 441 µm | Stress relief | 6/6, Resolved CSCR | 2 months |
| 3 | 65/M | DM | RE | WNL | PE + anterior SCTA (4 mg/0.2 mL) | 6/9 p | 397 µm | Stress relief | 6/6, Resolved CSCR | 8 months |
M- male, DM- diabetes mellitus, PE=phacoemulsification, SCTA=sub-conjunctival triamcinolone, SFCT=sub foveal choroidal thickness, CSCR – central serous chorioretinopathy
Case 1
The patient presented with blurred vision left eye (OS) 1 month following the surgery. The best-corrected visual acuity (BCVA) for both eyes (OU) was 6/9. Anterior segment was unremarkable except for right eye (OD) nuclear sclerosis grade 2 and OS pseudophakia with subconjunctival steroid depot 6 mm from the superior limbus. OD fundus was normal, and OS revealed features of acute CSCR. Enhanced depth imaging-optical coherence tomography (EDI-OCT) OS showed neurosensory detachment at macula along with increased subfoveal choroidal thickness (SFCT) of 422 μm [Fig. 1a]. The patient was advised stress relief. At 1 month, CSCR was persistent [Fig. 1b]. Fundus fluorescein angiography (FFA) OS demonstrated two hyperfluorescent, ink-blot type of CSCR leaks supero-temporal to optic disc, which were treated with focal laser [Fig. 1c]. At 4 months, the BCVA OS improved to 6/6 partial with complete resolution of CSCR [Fig. 1d].
Figure 1.

(a) EDI-OCT at 1-month post-operative day (POD) showing OS acute CSCR. (b) EDI-OCT at 2-month POD showing none resolving CSCR. (c) FFA depicting normal OD and OS hyper fluorescent ink-blot pattern. (d) EDI-OCT at 4-month POD showing complete resolution of CSCR
Case 2
The patient presented with OD blurred vision 9 days following surgery. He was a computer professional by occupation. BCVA was 6/6 OD and 6/24 OS. Anterior segment was unremarkable with pseudophakia OD and immature cataract OS. Fundus OD showed acute CSCR and normal OS. EDI-OCT demonstrated vitreous echoes, increased SFCT (441 μm), and foveal and peri-foveal subretinal fluid [Fig. 2a]. At 2 months, there was complete and spontaneous resolution of vitreous echoes along with subretinal fluid on SD-OCT [Fig. 2b].
Figure 2.
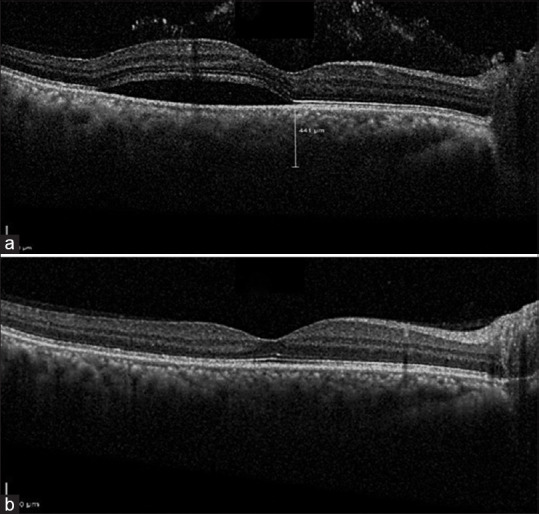
(a) OCT at 9 days POD showing OD acute CSCR. (b) OCT at 2 months POD showing complete resolution of OD CSCR
Case 3
The patient presented with blurred vision OD 2 weeks following surgery. On examination, BCVA OD was 6/9 partial and OS 6/6. Anterior segment was unremarkable except OU pseudophakia. Fundus showed OU peripapillary pachychoroid features with choroidal folds. The EDI-OCT identified an imminent CSCR OD with increased SFCT (397 μm) [Fig. 3a]. The patient was advised stress relief. At 1-month follow-up, BCVA OU was 6/6. However, EDI-OCT OD showed minimal increased schitic macular edema and imminent CSCR [Fig. 3b]. We decided to observe as the patient was asymptomatic. The patient reviewed back at 8 months postoperatively owing to the COVID-19 pandemic. The BCVA was 6/6 with resolved CSCR and mild peripapillary schitic edema [Fig. 3c].
Figure 3.

(a) OCT at 2 weeks POD showing OD parapapillary pachychoroid changes with imminent CSCR. (b) OCT at 6 weeks POD showing increased schitic edema along with imminent CSCR. (c) OCT at 8 months POD showing resolving CSCR and minimal schitic edema
Discussion
CSCR is characterized by localized serous detachment of the neurosensory retina with or without focal pigment epithelial detachments and altered retinal pigment epithelium (RPE). The pathogenesis of CSCR is still not clearly understood. It is proposed that increased choroidal hydrostatic pressure due to various risk factors can cause micro RPE breaks resulting in seepage of fluid into the subretinal space.[4] The known risk factors for CSCR include type A personality, smoking, obstructive sleep apnea, and various forms of steroid application. It is a known fact that steroids in any form are associated with an increased risk of developing of CSCR.
There has been a lot of interest in the recent past on the usage of SCTA at the end of phacoemulsification surgery to minimize the need of instilling tapering doses of steroid eye drops for 4–6 PO weeks. Shorstein et al.,[3] who pioneered this concept of less-drop approach, reported that the risk and safety profile of subconjunctival triamcinolone acetonide is similar to postoperative topical steroids. Lindholm et al.[5] suggested the use of perioperative SCTA (20 mg/0.5 mL) and intracameral cefuroxime to prevent ocular inflammation and macular edema in cataract patients. They observed a significant improvement in the postoperative aqueous flare and reduced central macular thickness (CMT) in the less-drop group (51 patients) when compared to the topical-steroid group (50 patients). Reddy et al.,[6] in their randomized controlled trial, did not observe any statistically significant difference in IOP, aqueous flare, and CMT between the less-drop group {(5 mg/0.5 mL) (200 patients)} and the topical-steroid group (200 patients).
Though different authors used different dosing regimens so far (20 mg/0.5 mL,[5] 5 mg/0.5 mL[6]), none of them reported CSCR as a complication following the less-drop approach in cataract surgery. However, CSCR following subtenon triamcinolone administration for other posterior segment lesions has been reported.[7] Despite using an acceptable dose of SCTA, we noted three cases of CSCR in 1129 eyes (0.26%) who underwent cataract surgery using the less-drop approach. To the best of our knowledge, this is the first case series of patients presenting with acute CSCR following SCTA given at the end of cataract surgery.
Interestingly, we noted thickened or pachychoroid in all three CSCR patients in our series. In recent times, CSCR has been included under the broader spectrum called pachychoroid-related disorders.[8] Apart from CSCR, pachychoroid spectrum includes pachychoroid pigment epitheliopathy, polypoidal choroidal vasculopathy, pachychoroid neovasculopathy, peripapillary pachychoroid syndrome, and focal choroidal excavation.[8] Hanumunthadu et al.[9] reported a significantly thickened choroid in acute CSCR (360.5 ± 94.7 μm) as compared to normal healthy eyes (277.8 ± 46.8 μm). Though there is no definitive cut off value for pachychoroid, most investigators consider values >300 μm as pathological.[8] Steroid-induced CSCR can be associated with thicker SFCT and multiple PED when compared to its idiopathic variant.[10] CSCR in our case series could have been triggered by the less-drop approach as these patients had clinically documented normal fundus preoperatively, did not have any known risk factors for CSCR, and CSCR was noted within a month following an uneventful cataract surgery.
Conclusion
We would like to convey that acute CSCR is rare but possible following the less-drop approach. However, larger prospective clinical trials are needed to ascertain the causality in the future. Preoperative OCT imaging to rule out pachychoroid might be critical in avoiding CSCR in this novel approach.
Ethics approval and consent to participate
Obtained.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Authors’ contributions
All authors contributed equally in data collection, manuscript writing, and critical revision.
Precis
Here we report a case series of three patients who developed acute central serous chorioretinopathy (CSCR) following cataract surgery using the less-drop approach. All patients showed pachychoroid features on enhanced depth imaging–optical coherence tomography (EDI-OCT). Preoperative EDI-OCT might help in identifying these patients who are prone for developing CSCR.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1. Shorstein NH, Myers WG. Drop-free approaches for cataract surgery. Curr Opin Ophthalmol. 2020;31:67–73. doi: 10.1097/ICU.0000000000000625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Helm CJ, Holland GN. The effects of posterior subtenon injection of triamcinolone acetonide in patients with intermediate uveitis. Am J Ophthalmol. 1995;120:55–64. doi: 10.1016/s0002-9394(14)73759-6. [DOI] [PubMed] [Google Scholar]
- 3. Shorstein NH, Liu L, Waxman MD, Herrinton LJ. Comparative effectiveness of three prophylactic strategies to prevent clinical macular edema after phacoemulsification surgery. Ophthalmology. 2015;122:2450–6. doi: 10.1016/j.ophtha.2015.08.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Guyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Ho A, Orlock D. Digital indocyanine green videoangiography of central serous chorioretinopathy. Retina. 1995;15:79–80. doi: 10.1001/archopht.1994.01090200063023. [DOI] [PubMed] [Google Scholar]
- 5. Lindholm JM, Taipale C, Ylinen P, Tuuminen R. Perioperative subconjunctival triamcinolone acetonide injection for prevention of inflammation and macular oedema after cataract surgery. Acta Ophthalmol. 2020;98:36–42. doi: 10.1111/aos.14175. [DOI] [PubMed] [Google Scholar]
- 6. Reddy JK, Chaitanya V, Shah N, Guduru VP, Khan S, Kuttupalayam S. Safety & efficacy of single subconjunctival triamcinolone 5 mg depot vs topical loteprednol post cataract surgery: Less drop cataract surgery. Int J Ophthalmol. 2019;12:774–8. doi: 10.18240/ijo.2019.05.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Dhanji S, Fung AT. Central serous chorioretinopathy secondary to subtenon triamcinolone injection: A new hypothesis for the mechanism. Clin Exp Ophthalmol. 2020;48:1007–9. doi: 10.1111/ceo.13807. [DOI] [PubMed] [Google Scholar]
- 8. Cheung CMG, Lee WK, Koizumi H, Dansingani K, Lai TYY, Freund KB. Pachychoroid disease. Eye (Lond) 2019;33:14–33. doi: 10.1038/s41433-018-0158-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hanumunthadu D, Van Dijk EHC, Dumpala S, Rajesh B, Jabeen A, Jabeen A, et al. Evaluation of choroidal layer thickness in central serous chorioretinopathy. J Ophthalmic Vis Res. 2019;14:164–70. doi: 10.4103/jovr.jovr_152_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Araki T, Ishikawa H, Iwahashi C, Niki M, Mitamura Y, Sugimoto M, et al. Central serous chorioretinopathy with and without steroids: A multicenter survey. PLoS One. 2019;14:e0213110. doi: 10.1371/journal.pone.0213110. [DOI] [PMC free article] [PubMed] [Google Scholar]