

Abstract
Behavioral flexibility—the ability to tailor motor actions to changing body-environment relations—is critical for functional movement. Navigating the everyday environment requires the ability to generate a wide repertoire of actions, select the appropriate action for the current situation, and implement it quickly and accurately. We used a new, adjustable barrier paradigm to assess flexibility of motor actions in 20 17-month-old (8 girls) and 14 13-month-old (7 girls) walking infants, and a comparative sample of 14 adults (8 women). Most participants were white, non-Hispanic, and middle class. Participants navigated under barriers normalized to their standing height (overhead, eye-, chest-, hip-, and knee-heights). Decreases in barrier height required lower postures for passage. Every participant altered their initial walking posture according to barrier height for every trial, and all but 2 13-month-olds found solutions for passage. Compared to infants, adults displayed a wider variety of strategies (squat-walking, half-kneeling, etc.), found more appropriate solutions based on barrier height (ducked at eye-height and low-crawled at knee-height), and implemented their solutions more quickly (within 4 seconds) and accurately (without bumping their heads against the barrier). Infants frequently crawled even when the barrier height did not warrant a low posture, displayed multiple postural shifts prior to passage and thus took longer to go, and often bumped their heads. Infants’ improvements were related to age and walking experience. Thus, development of flexibility likely involves the contributions of multiple domains—motor, perception, and cognition—that facilitate strategy selection and implementation.
Keywords: obstacle navigation, walking, crawling, motor development, perception, planning
What makes skills skillful? The hallmarks of skill are fluency and flexibility (Adolph & Hoch, 2019; Bernstein, 1996). Fluency is what makes skills beautiful, coordinated, smooth, and consistent. It is best exemplified by people’s ability to repeat highly practiced actions the same way over and over under uniform task constraints—like nailing basketball free throws, typing on a computer keyboard, or walking along a straight, unobstructed path.
Flexibility, in contrast, is what makes skills truly functional. It is the ability to tailor motor actions (even highly practiced actions like throwing, typing, and walking) to changing body-environment relations, or as Bernstein (1996) put it, “finding a motor solution for any situation and in any condition” (p. 21). Flexibility is imperative, not optional, because in most activities, task constraints are continually changing, not uniform. Flexibility is best exemplified by movements that are creative and generative, never performed exactly the same way as before—like shooting a basket while twisting midair to dodge opposing players, using a different hand configuration to type on a smaller keyboard or with a bandage on one finger, or modifying walking steps to navigate puddles, curbs, and oncoming pedestrians on a city sidewalk.
Thus, according to Bernstein (1996), flexibility requires movements to be (1) resourceful (constructed in the moment or selected from a wide range of solutions in the motor repertoire); (2) appropriate (rational and geared to the current situation); (3) quick (selected and implemented without wasted time or extraneous movements); and (4) accurate (implemented precisely without errors). In addition to the obvious motor requirements, flexibility implicates central psychological functions—motivation, perception, and cognition in a continual, interacting loop. Motivation instigates the search for appropriate solutions and weighs the relative costs among candidate solutions; perception obtains information about changing body-environment relations and guides subsequent actions; and cognition governs strategy choice and evaluates movement outcomes (Gibson, 1979; Hommel, 2003; Jeannerod, 1988; Kenward, Folke, Holmberg, Johansson, & Gredebäck, 2009; Kording & Wolpert, 2006; Siegler & Jenkins, 1989; von Hofsten, 2004).
Flexibility is evident in adult behavior. Adults display a wide range of locomotor solutions, each appropriate to particular variations in the terrain or their bodies, and they do so quickly and accurately. They seamlessly duck their heads to pass under low doorways while walking (Franchak & Adolph, 2012) or rolling in wheelchairs (Stoffregen, Yang, Giveans, Flanagan, & Bardy, 2009); they turn sideways to fit through narrow doorways (Comalli, Franchak, Char, & Adolph, 2013) and detour around apertures too narrow to squeeze through sideways (Hackney & Cinelli, 2013). Pregnant women (and adults wearing “pregnancy packs” or backpacks) adapt their gait and posture to the current status of their bellies/bodies for passing through narrow apertures (Franchak & Adolph, 2014; Regia-Corte & Wagman, 2008).
Walking infants also show evidence of flexibility, but their solutions become more resourceful, appropriate, quick, and accurate with age and walking experience (e.g., Adolph, 1997; Franchak & Adolph, 2012; Kretch & Adolph, 2013, 2017). Novice walkers, for example step right over the brink of impossibly high drop-offs, steep slopes, and narrow bridges and ledges, requiring rescue by an experimenter. Over weeks of walking experience, infants learn to discern safe from risky ground with adult-like precision. Experienced walkers modify their steps as they approach and cross challenging obstacles, and when the obstacle does not afford walking, they use alternative strategies (e.g., crawling, backing down on their bellies, sliding or scooting down sitting) or avoid going. Moreover, compared with novices, experienced walkers are quicker to determine whether and how to walk and their judgments are more accurate (i.e., they are less likely to walk and fall).
Despite extensive research on infants’ acquisition of flexibility in the development of locomotion (for reviews, see Adolph & Hoch, 2019; Adolph & Robinson, 2013; Adolph & Robinson, 2015), previous studies focused primarily on the target action: Do walking infants try to walk over the obstacle, under the barrier, or through the aperture (Franchak & Adolph, 2012; Schmuckler, 1996; van der Meer, 1997)? Although infants display a variety of alternative non-walking solutions (e.g., crawling, backing, scooting) to cope with slopes, drop-offs, bridges, and so on, prior work could not determine whether a particular alternative strategy was most appropriate for the current situation, or whether infants executed them quickly and accurately, because attempts often led to a fall. Anecdotally, infants sometimes correctly judged a slope as too steep or a drop-off as too high for walking but fell while trying to descend with an alternative strategy such as crawling, sliding, or backing (Adolph, 1997; McGraw, 1935).
Moreover, infant and adult walkers may weigh costs differently depending on the penalty for errors, the fun or frustration of different solutions, and the time and energy involved. In paradigms involving adjustable slopes, drop-offs, bridges, and ledges, the penalty for errors is falling, so infants often avoid going (Adolph & Hoch, 2019; Adolph & Robinson, 2013, 2015). But in paradigms where the penalty for error is entrapment (walking through narrow apertures), infants, like adults, are likely to try impossibly tight apertures and became wedged, suggesting that walkers weigh falling as more onerous than entrapment (Comalli et al., 2013; Franchak & Adolph, 2012). Infants sometimes fuss and cry out of frustration when they cannot find a solution to reach their goal (e.g., at the edge of an impossibly high drop-off), and they often enjoy implementing alternative solutions (e.g., sliding down slopes) even when the alternative is unnecessary (Adolph, 1997; Burnay & Cordovil, 2016; Tamis-LeMonda et al., 2008). What’s needed is a paradigm that encourages infants to attempt some form of locomotion on every trial without falling, allows for multiple solutions that are more or less appropriate depending on the status of an adjustable apparatus, and provides a means to assess the speed and accuracy of every solution. The current study did just that.
Current Study
We examined flexibility in infant locomotion in a new paradigm—while navigating under an overhead barrier set at different heights (Figure 1A). Rather than focusing only on walking behavior, our adjustable barrier paradigm allowed us to test all four of Bernstein’s criteria for flexibility: (1) resourcefulness, that is, displaying a wide variety of motor solutions across barrier heights, and (2) finding an appropriate solution for each barrier height, and implementing the solution (3) quickly and (4) accurately. For example, a barrier at walkers’ eye height affords multiple solutions—infants could duck their heads, squat down, crawl on hands and knees, and so on. Walking upright would not be possible and infants would bump their heads. Squatting or crawling are possible but would be grossly inefficient. Testing various postures before crossing is also possible but would involve extraneous movements and thus waste time and effort. Ducking is the most appropriate and rational solution and should be performed quickly and accurately, with the duck performed just at the moment of passage (ducking with a premature return to upright would result in a head bump).
Figure 1.
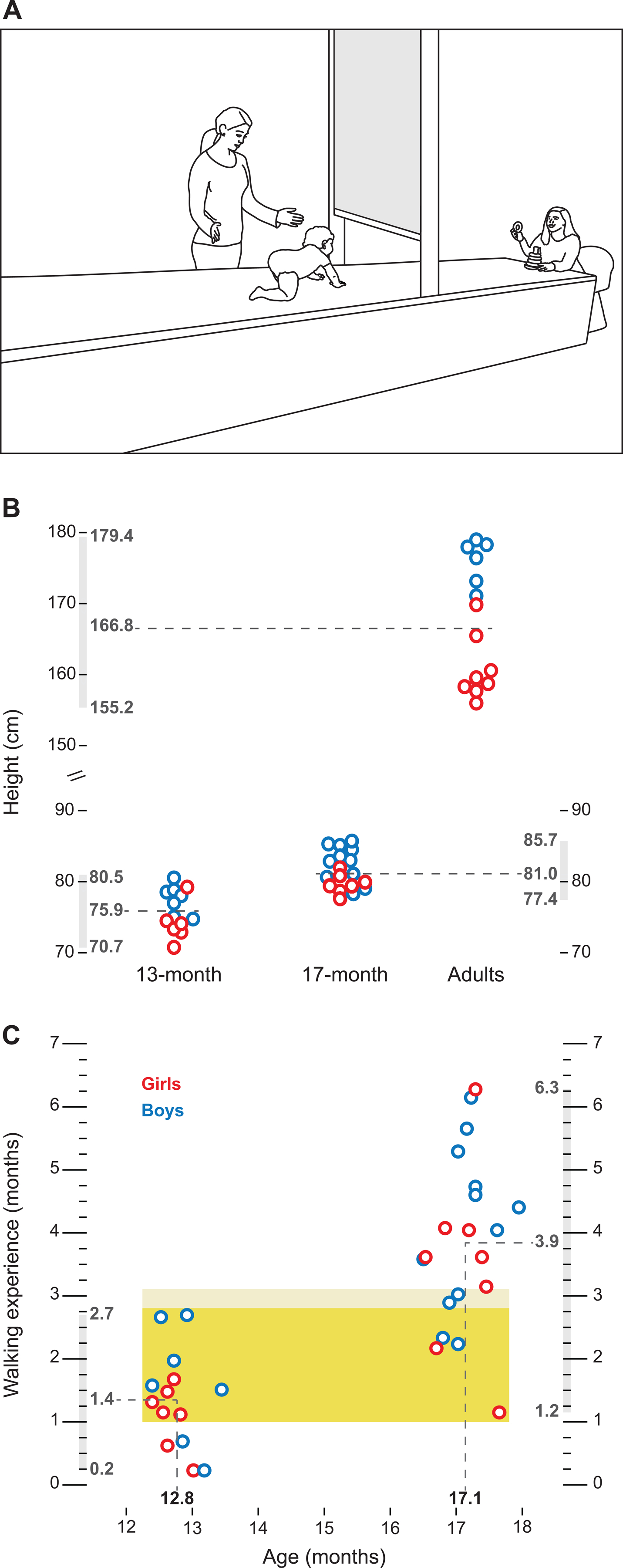
Apparatus and participants. (A) Adjustable overhead barrier. Participants walked on an elevated walkway. Between trials the barrier was adjusted to five heights (overhead-, eye-, chest-, hip-, or knee-height). Infants’ caregivers sat at the end of the walkway and encouraged infants to pass under the barrier to retrieve toys, snacks, and hugs. An experimenter followed alongside infants to ensure their safety on the raised walkway. Line drawing is the authors’ original artwork. (B) Standing height in infants and adults. Dashed lines denote group averages. Numbers on graph denote the mean, minimum, and maximum for each group. Barrier height was normalized to each participant’s standing height.(C) Infant age and walking experience. Each symbol represents a single infant (blue for boys, red for girls) and dashed lines denote group averages for age (x-axis) and walking experience (y-axis). Numbers on graph denote the mean, minimum, and maximum for each group. Dark yellow region denotes overlap in walking experience between the 13- and 17-month-olds. Light yellow region denotes 17-month-olds within 1 week of the 13-month-olds.
We designed each barrier height to require participants to lower their bodies to different extents for safe passage. On some trials, the barrier was far above participants’ heads, so normal upright walking was possible. But on other trials, we lowered the barrier to walkers’ eye-, chest-, hip-, or knee-height requiring them to lower their heads and/or torsos by ducking, squatting, kneeling, or various crawling postures. Given that all barrier heights afforded some form of locomotion and that the penalty for errors was relatively trivial (bumping the head on a padded barrier), we assumed that participants would not avoid passage at any barrier height.
We observed 13- and 17-month-old walking infants to test changes across age and walking experience. We focused on those age groups to ensure that the younger infants would have relatively little walking experience (Karasik, Tamis-LeMonda, & Adolph, 2014), whereas walking experience in the older infants would be within the range of previous studies with “experienced” walkers (Adolph, 1997; Franchak & Adolph, 2012). We also observed a comparison sample of adults to benchmark flexibility in mature walkers. Based on prior work, we predicted that infants, like adults, would perceive the relations between their bodies and the barrier height, but that the older, more experienced walking infants would show greater evidence of flexibility on all four criteria.
Method
The study was approved by the Institutional Review Board of New York University (Protocol Number: 10–6822, Study: Motor Development in Infants, Children, and Adults). The study was not preregistered, but all the data are openly shared with authorized Databrary researchers and video clips to illustrate the procedure and behavioral codes are publicly shared (see Data Availability).
Participants
As shown in Figure 1B, we tested 14 adults (M age = 24.3 years, 8 women), 20 17-month-olds (M age = 17.1 months, 8 girls), and 14 13-month-olds (M age = 12.8 months, 7 girls). Adults were recruited through word of mouth and compensated with $10 and souvenir photographs. Due to the limited height of the apparatus, adults taller than 180 cm were excluded from participation (Figure 1B). Most adults were white (64%), non-Hispanic (100%), and all were undergraduate or doctoral students. Families for the infant participants were recruited from hospitals in the New York City area, and they received a souvenir tote bag and photograph for participation. Most infants were white (71%), non-Hispanic (94%), and middle class; all were healthy and born at term. Data from 10 additional infants (2 13-month-olds, 8 17-month-olds) were excluded due to failure to complete >20% of trials or to fussiness (because infants fussed when we put them on the walkway, or they needed to be continuously held and soothed by the caregiver).
In a structured interview, parents reported the first day they saw their infant walk 3 meters (across a room) without stopping or falling using cell phone photos and videos, calendars, and baby books to support their memories (Adolph, Vereijken, & Shrout, 2003). Walking experience (from onset to test day) ranged from 0.2 – 2.7 months (M = 1.4) for the 13-month-olds and from 1.2 – 6.3 months (M = 3.9) for the 17-month-olds, t(32) = 6.16, p < .001. We originally aimed to observe 14 participants per group, who differed by age and walking experience (experienced young adults, experienced 17-month-olds, and novice 13-month-olds); prior work using linear mixed models suggested that N = 14 per group was sufficiently powered to detect a medium effect size of η2 = .06 for decisions to walk (Karasik, Tamis-LeMonda, & Adolph, 2016). However, as we collected data from the first 14 infants per age group, we realized that the 13-month-olds showed a relatively narrow range of walking experience as expected, but the 17-month-olds showed a wider range of walking experience than expected, and their experience overlapped the 13-month-olds (dark yellow band in Figure 1C) or was within 1 week (light yellow band in Figure 1C). Thus, we collected data from an additional 6 17-month-olds so that we could conduct follow-up analyses on the effects of walking experience with an age-held-constant design within the 17-month-olds; based on prior work (e.g., Cole, Gill, Vereijken, & Adolph, 2014; Franchak & Adolph, 2012; Kretch & Adolph, 2017), N = 20 was sufficiently powered for such within-age analyses. Moreover, in addition to creating one age group with varying walking experience, we could conduct follow-up analyses on the 14 infants in each age group who did not have overlapping walking experience.
Adjustable Barrier
Participants were tested on a wooden walkway (490 cm long × 98 cm wide × 64 cm high) with an adjustable overhead barrier (Figure 1A). The walkway was elevated to dissuade infants from detouring around the barrier. The wooden surface was covered with high-density foam to protect participants’ knees when crawling. The overhead barrier was a white vinyl window shade hung above an 86-cm wide doorway (as in Franchak & Adolph, 2012). The shade spanned the width of the doorway and was clearly visible. The shade was housed in vertical tracks along the sides of the doorway and a thin metal rod weighted the bottom to maintain a flat position. The rod was covered with foam to protect participants’ heads if they banged into the barrier (the foam was necessary to ensure infants’ safety because while piloting the procedure without the foam padding, some infants plowed so hard into the barrier that they “bounced” off).
The shade could be lowered in 1-cm increments from 185 – 0 cm above the surface of the walkway. As shown in the yellow panel of Figure 2A, the highest barrier height—overhead—was above all participants’ standing height (see variability of height across participants in Figure 1B). For adults, overhead was the highest possible barrier height (185 cm) and for infant walkers it was 130% of their standing height. We determined four lower barrier heights normalized to each participant’s standing height: 90% of standing height (approximately eye level), 70% (around chest height), 45% (around hip height), and 25% (around knee height).
Figure 2.
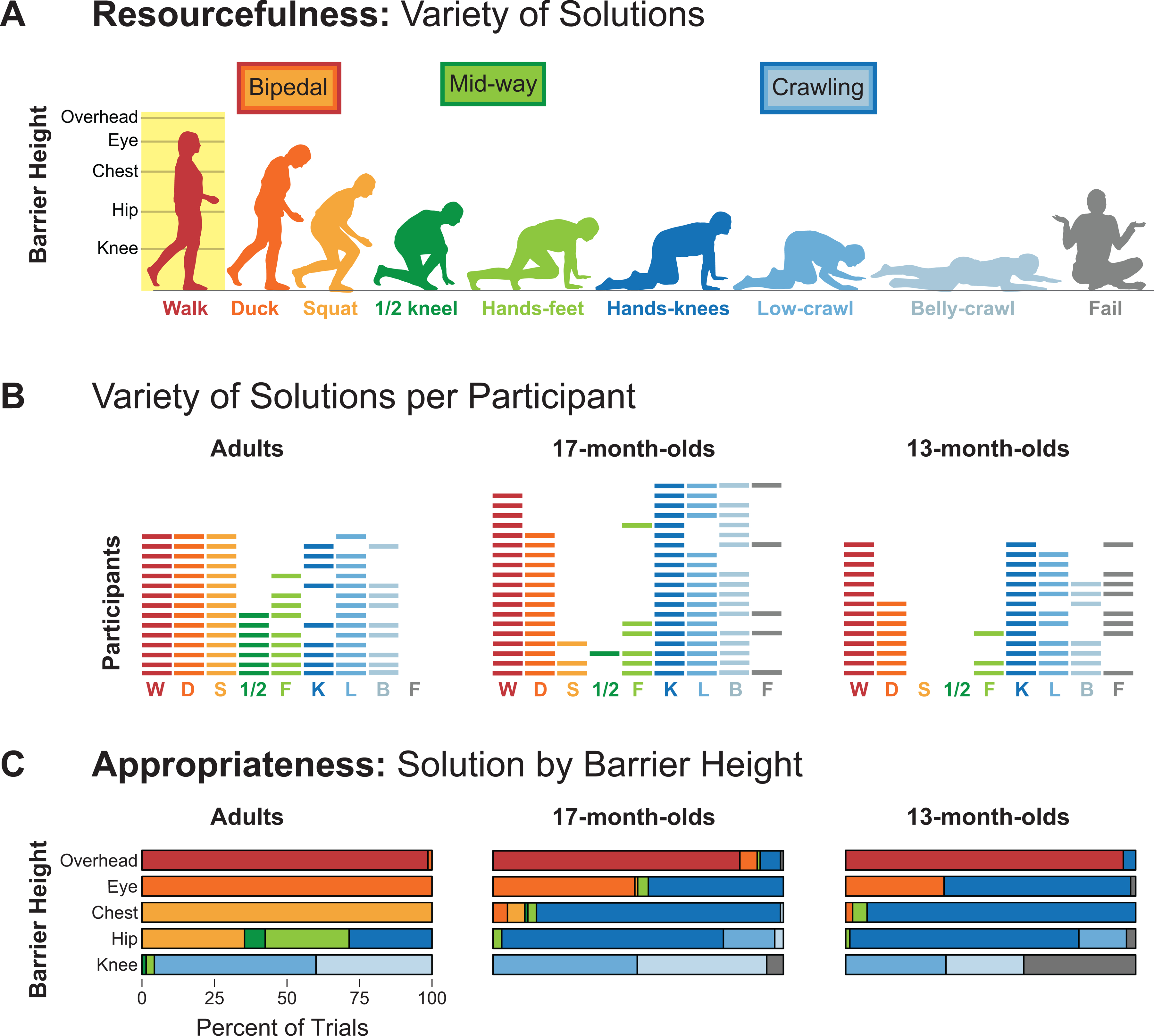
Solutions for passing under barriers. (A) Silhouettes show all observed locomotor solutions. Bipedal strategies were walking, ducking, and squat-walking; midway strategies were half-kneeling and hands-feet crawling; crawling strategies were hands-knees crawling, low crawling, and belly crawling; or participants could fail to find a solution for passage. Barrier heights are displayed against the silhouette of walking to illustrate body-scaled heights. Line drawing is the authors’ original artwork. (B) Variety of solutions used by each participant on at least one trial. Colors correspond to the silhouettes in (A). Each row represents a participant. Rows are ordered by the variety of solutions displayed. Empty spaces mean that the strategy was not displayed. Note, the 17-month-old who never walked on overhead barrier trials had 4 months of walking experience and he walked in the warm-up trials. (C) Appropriateness of strategy choice by barrier height. Stacked bars show the average percent of trials for each barrier height by age group.
Three cameras recorded participants’ actions: a stationary side camera captured participants’ movements as they passed through the doorway, a panning side camera tracked participants as they moved along the platform, and a stationary camera at the back of the apparatus recorded participants from behind. The three views were synced online into a single digital video file with a playback rate of 30 frames/second.
Procedure
Sessions lasted approximately 50 minutes in total for infants (25 minutes passing under the barrier), and 30 minutes in total for adults (15 minutes passing under the barrier). Adults wore clothes that did not restrict their movements, and infants wore a diaper and undershirt; all were barefoot. At the beginning of the session, the experimenter measured participants’ height to determine barrier heights. We measured adult’s standing height (155 – 179 cm) with a stadiometer, and we measured infant’s recumbent height from crown to heel (71 – 86 cm) on a measuring board (Figure 1B).
Participants received 5 blocks of 5 trials each––one trial per block at each barrier height––for a total of 25 trials. To maintain participants’ motivation, each trial block began with the overhead barrier, and the 4 lower barrier heights were randomized within each block. Due to infant fussiness on some trials, participants contributed 1089 trials instead of the 1200 expected. Thus, infants contributed to 3–5 (M = 4.8) overhead-barrier trials, 2–5 (M = 4.2) eye-barrier trials, 2–5 (M = 4.3) chest-barrier trials, 1–5 (M = 4.4) hip-barrier trials, 2–5 (M = 4.3) knee-barrier trials, and 2 13-month-old infants never contributed to knee-barrier trials. Adults contributed to all 25 trials.
Infant testing began with a few warm-up trials with no overhead barrier to get them comfortable with the game of crossing the raised walkway to their caregivers and a research assistant, who stood at the far side of the barrier and offered toys and snacks as enticements (see video clip: https://nyu.databrary.org/volume/1312/slot/54361). Every infant walked over the walkway on the warm-up trials. On barrier trials, caregivers and the assistant provided only general encouragement and did not tell infants how to pass under the barrier. At every barrier height, caregivers and enticements were visible under the barrier, and the adults behind the barrier emitted a continual stream of audible encouragements to “come here” or “get this toy/snack” On every trial, a highly trained experimenter followed alongside infants to ensure their safety.
Adults and infants began in a standing position approximately 1.5 m from the barrier. To prevent adults from planning their actions prior to the trial, adults faced away from the barrier at the start of each trial until the experimenter set the shade at the appropriate height and instructed them to turn around and proceed through the opening (see video clip: https://nyu.databrary.org/volume/1312/slot/54362). Adults were told that all trials were possible, and they should attempt all barrier heights. After adults passed through the doorway, the experimenter raised the shade to overhead, and adults walked back to the starting point. The experimenter carried infants back to the starting platform after each trial and the assistant changed the barrier height before the experimenter stood infants on the starting platform. Trials lasted until participants passed under the barrier or until 30s elapsed, whichever occurred first.
Data Coding and Processing
A primary coder scored the videos using Datavyu (datavyu.org), a computerized video coding tool, which time locks codes to the video and identifies the duration and type of user-defined events with frame accuracy. Prior work with adults and older children passing under barriers suggested that participants would display various bipedal strategies (walking, ducking/bowing, or squat-walking), crawling strategies (both hands and both knees touching the floor, and belly crawling), and “mid-way” strategies that were neither fully upright nor crawling (half-kneeling, hands/feet) for passage (Comalli, Persand, & Adolph, 2017). However, because prior work with infants was limited to barriers at standing height and higher (van der Meer, 1997), we were unsure what infants might do. Inspection of the videos resulted in a further distinction between hands/knees crawling and “low crawling.”
Thus, to determine the variety and appropriateness of solutions, for each trial, the coder scored the selected action for passage (as illustrated in Figure 2A, from left to right; see also video clip at https://nyu.databrary.org/volume/1312/slot/54362). Similar to Comalli et al. (2017), “bipedal” solutions were walking (fully upright), ducking (bending at the neck, trunk, or hips), and squat-walking (lowering the upper body without hands touching the floor and advancing with knees bent). “Mid-way” strategies were half-kneeling (putting one knee on the ground as a support point and advancing forward with the other foot—hands could occasionally touch the floor) and hands-feet crawling (advancing on two hands and two feet without the knees touching the surface). “Crawling” strategies were hands-knees crawling (crawling with reciprocal movements of hands and knees with an upright head position), low crawling (lowering the height of the quadruped position by bending at the elbows and ducking the head), and belly crawling (chest and/or belly to the ground and advancing forward with the arms or forearms while pushing with the legs or feet). In addition, infants sometimes failed to pass under (because infants could not find a solution or fell while doing so; see video clip at https://nyu.databrary.org/volume/1312/slot/54363).
To determine the quickness of participants’ solutions, the coder scored latency to success (from the moment the experimenter released infants on the starting platform or adults turned around until their buttocks passed under the barrier) and the total number of distinct postural shifts displayed before passing under the barrier (squatting, kneeling, sitting, return to upright, and the postures shown in Figure 2A; see video clip: https://nyu.databrary.org/volume/1312/slot/54364). To count as a shift, participants had to hold the posture for at least 0.5 s, take a step in the posture, or use the posture for passage. For example, if a participant walked straight through, the coder scored 0 postural shifts; if a participant transitioned smoothly from walking to crawling, the coder scored 1 shift; and if a participant shifted to squatting and held it for at least 0.5 s, then shifted to hands and knees and took a few steps, then sat for at least 0.5 s, and then finally crawled under the barrier, the total number of shifts was 4.
To determine the accuracy of participants’ solutions, the coder scored whether participants bumped their head on the barrier (either forehead or top of head). Coders distinguished initial bumps that occurred prior to passage from traveling bumps that occurred while passing under the barrier in the selected posture (see video clip: https://nyu.databrary.org/volume/1312/slot/54365). Initial bumps occurred when infants did not lower their heads at all or lowered too soon and returned to upright before arriving at the barrier. Traveling bumps occurred when infants lowered their heads but raised them while passing under the barrier or did not lower their heads sufficiently while passing under the barrier.
A second coder independently scored 25% of trials from each participant (randomly distributed across the session) to ensure inter-observer reliability. Coders agreed on ≥94% of instances for categorical variables (κs ≥ .91, ps < .001) and the correlation coefficient for trial duration was r(399) = .99, p < .001. To prevent coding drift, after every 3–4 sessions, the primary and secondary coders met to discuss disagreements. Often the disagreements were due to careless errors (typos, forgetting to set an offset time, etc.). Although the number of disagreements was low, to avoid propagating known errors in the final analyses, such disagreements were resolved through discussion. For the few instances that reflected true disagreements, the primary coder’s data were retained for the final analyses.
Statistical Analysis
We used Generalized Estimating Equations (GEE) to analyze the effects of the 5 barrier heights and 3 age groups on the resourcefulness, appropriateness, quickness, and accuracy of participants’ solutions. We used GEEs rather than ANOVAs because each participant’s trials were correlated, and the number of trials and successful crossings were not distributed evenly across barrier heights. We used an exchangeable covariance structure and Sidak corrections for multiple comparisons. Preliminary analyses showed no effects of sex, ts ≤ 1.71, ps ≥ .097, so this variable was collapsed in subsequent analyses.
To capitalize on the non-overlap in walking experience among 13- and 17-month-olds, we conducted separate follow-up analyses between the 13-month-olds and the 14 17-month-olds whose walking experience did not overlap the younger age group (white area of 17-month-olds in Figure 1C). Because the 17-month-olds showed such a wide range of walking experience, we also conducted additional follow-up analyses for them separately to test effects of walking experience with age held constant (using Pearson correlations). Finally, we performed separate analyses to examine changes between the first and last trial at the same barrier height for all age groups (using chi-squares for categorical measures and paired t-tests for continuous measures) to further investigate learning or perseveration and the impact of head bumps on subsequent trials at the same barrier height.
Data Availability
With participants’ permission, raw videos and coding spreadsheets from each session are shared with authorized investigators on Databrary (https://nyu.databrary.org/volume/1312). The coding manual, coding scripts, processed data, analysis scripts (https://nyu.databrary.org/volume/1312/slot/54360) and exemplar video clips are publicly available.
Results
Failure to Find a Solution
Although every age group found solutions to pass under the barriers, 13 infants (8 13-month-olds and 5 17-month-olds failed to find a solution on at least one trial). Most failed trials occurred at the lowest, knee-height barrier (21/25 failure trials). On the failure trials, infants fell on only 2 (both while walking toward the barrier) and bumped their heads on only 1, meaning that failures were not a consequence of an aversive experience. Indeed, postural shifts during these failed trials ranged from 1–9 (M = 3.84), suggesting that infants were searching for a solution, but failed to find one. In a typical instance, the baby switched from standing to squatting, to low-crawling, to kneeling, to standing again, to sitting, and then the trial timed out.
Overall, the average percentage of failure trials differed across age groups and barrier heights, Wald χ2 = 19.6, p = .001. At the knee-height barrier, adults never failed, and 17-month-old infants failed less frequently compared to 13-month-old infants, ps ≤ .013. No differences among groups were observed for the other barrier heights, ps ≥ .340.
Follow-up infant group analyses:
For the 13- and 17-month-old infants with non-overlapping walking experience, the average percentage of failed attempts differed between age groups and barrier heights, Wald χ2 = 11.69, p = .020. At the knee-height barrier, 17-month-olds failed less frequently compared to 13-month-olds, p = .004; but the two groups were similar for the other barrier heights, ps ≥ .129. For the 17-month-olds, we found no correlations between walking experience and failures at any barrier height, ps ≥ .126.
Changes across trials:
Overall, 17-month-old infants quickly learned to find a solution to pass under the knee-barrier height after their first failed attempt, whereas many 13-month-olds did not. For example, 4 17-month-olds failed on the first trial at knee-height but not on their last trial at that barrier height. In contrast, 4 13-month-olds failed at their first trial at knee-height and also failed on their last trial. A chi-square test confirmed differences in failures from the first to last trials between infant age groups, X2 (2, 16) = 6.49, p = .039.
Because all barrier heights were passable and adults never failed to negotiate any type of barrier, we excluded infants’ failed trials in analyses of resourcefulness, appropriateness, quickness, and accuracy of solutions.
Resourcefulness: Variety of Solutions
Participants displayed a variety of solutions for passage (shown in Figure 2A). These 8 locomotor actions were exhaustive although other actions were possible (bum shuffling, rolling, knee walking, etc.) and were displayed by adults and infants in other obstacle-navigation studies (Adolph, 1997; Comalli et al., 2017; Gill, Adolph, & Vereijken, 2009; Karasik et al., 2016; Kretch & Adolph, 2013, 2017). Figure 2B shows each participant’s variety of solutions for passage across the session. Each row is a participant and empty spaces denote that the participant did not display that action. Rows are ordered from least to most variety of actions (number of colors increases while moving down rows).
Adults exhibited the largest variety of locomotor solutions (4–8) across the session (M = 6.1). Compared to adults, infants were less likely to exhibit squat walking (light orange bars) and mid-way solutions—half kneeling (dark green bars) and hands-feet crawling (light green bars). The scarcity of these actions was most apparent in 13-month-olds. Seventeen-month-olds displayed 3–7 actions (M = 4.9), and 13-month-olds displayed 2–6 actions (M = 4.1). The GEE confirmed differences between adults and infants, Wald χ2 = 22.1, p < .001. Adults displayed more solutions compared to both infant groups, ps ≤ .009, and the variety of solutions was similar for 17- and 13-month-olds, p = .143.
Follow-up infant group analyses:
For the 13- and 17-month-olds with non-overlapping walking experience, 17-month-olds displayed a larger variety of solutions compared to 13-month-olds, Wald χ2 = 4.13, p = .042. Nonetheless, the variety of solutions did not change with walking experience for the 17-month-olds, p = .159.
Appropriateness: Solution by Barrier Height
Adults selected solutions in accordance with barrier height, lowering their bodies just enough to clear the barrier without touching the ground until absolutely necessary (note the large amount of red, orange, and yellow in Figure 2C). However, although both infant groups were able to negotiate the barrier, infants’ locomotor adjustments were not always appropriate. Infants lowered themselves all the way to the ground when the barrier height was lower than the overhead height (note the large amount of blue in Figure 2C).
With the overhead barrier, adults (M = 98.6% of trials), 17-month-olds (M = 85.0% of trials), and 13-month-olds (M = 95.7% of trials) mostly walked (without ducking). With the barrier at eye height, every adult ducked. In contrast, infants ducked on only Ms = 48.9% and 33.9% of trials, and hands-knees crawled on Ms = 46.5% and 66.1% of trials, for 17- and 13-month-olds, respectively. With the barrier at chest height, every adult squat-walked. In contrast, infants mostly crawled (Ms = 84.0% and 92.6% of trials for 17- and 13-month-olds, respectively). With the barrier at hip height, adults displayed a variety of actions—squat-walked (M = 35.4% of trials), half-knee crawled (M = 7.14%), hand-feet crawled (M = 28.9%), and hands-knees crawled (M = 28.6%)—whereas infants continued to hands-knees crawl (Ms = 76.3% and 81.6% for 17- and 13-month-olds, respectively). At knee height, all groups mostly low crawled or belly-crawled (Ms = 95.7% and 100% for adults and infants, respectively). Thus, the GEE showed a significant age by barrier height interaction for the proportion of trials in which participants chose bipedal and mid-way strategies to navigate under the barrier (red and green shaded actions in Figure 2A), Wald χ2 = 828.9, p < .001. Compared to infants, adults exhibited more bipedal and mid-way strategies for eye-, chest-, and hip-heights, ps < .001. The proportion of bipedal and mid-way strategies was similar across barrier heights for the two infant groups, ps ≥ .334.
Follow-up infant group analyses:
For the 13- and 17-month-olds with non-overlapping walking experience, the proportion of bipedal and mid-way strategies remained scarce (i.e., both groups chose crawling strategies equally often), Wald χ2 = 2.38, p = .123. The GEE revealed a main effect of barrier height, Wald χ2 = 603.59, p < .001, indicating that both infant groups displayed more bipedal and mid-way strategies with overhead, eye-, and chest-height barriers compared to knee-height, ps ≤ .005. For the 17-month-olds, the proportion of upright and midway strategies increased with walking experience at eye-height, p = .042, but was not correlated at the lower barrier heights, ps ≥ .286.
Changes across trials:
Adults persisted with their selected solutions for every barrier height. Infants persisted for all but the eye- and hip-height barriers. At eye-height, selected solutions remained consistent for slightly more than half of the infants in both groups, whereas the rest switched strategies between bipedal/midway to crawling strategies between the first and last trials. At hip-height, 17-month-olds perseverated with their first (crawling) strategy more often than did 13-month-olds. Thus, differences in switching solutions across trials between the infant age groups were not significant for any barrier height, X2s ≤ .71, ps ≥ .398, except for hip-height, X2 (1, 34) = 4.70, p = .030.
Quickness
We considered quickness in terms of how long it took participants to get through the barrier (latency for passage) and the total number of actions displayed prior to selection of the final locomotor action.
Latency for passage.
Adults were extremely quick to complete each trial. As shown in Figure 3A, trials for almost all barrier heights averaged less than 4 seconds and were only slightly longer for knee height where it was necessary to lower the body completely to the ground. Infants, especially 13-month-olds, took longer to pass under the barriers, and trial duration was particularly long for the lowest barrier heights. Thus, latency for passage differed across age groups and barrier height, Wald χ2 = 94.48, p < .001. For every barrier height, adults were faster (Ms = 2.79–4.33s) than infants, ps ≤ .003. Seventeen-month-olds (Ms = 3.67–7.54s) were faster than 13-month-olds (Ms = 5.01–12.3s) at every barrier height except knee-height, ps ≤ .029. With the barrier at knee height, 17- and 13-month-old infants were equally slow (Ms = 10.5s and 13.8s, respectively), p = .172.
Figure 3.
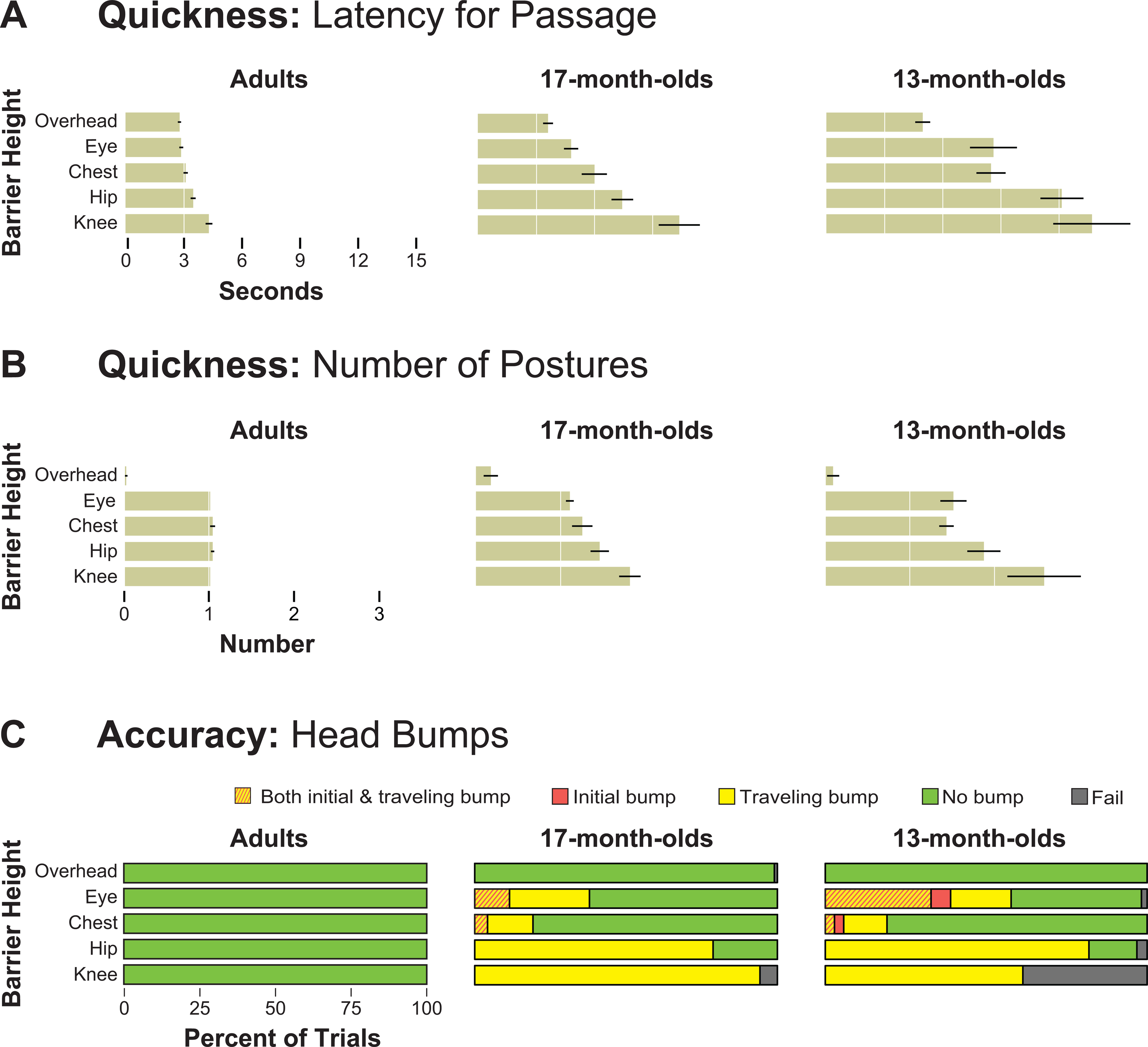
Quickness and accuracy of solutions. (A) Average latency across trials at each barrier height for each age group at each barrier height. Error bars denote standard errors. (B) Average number of postural shifts prior to passage for each age group at each barrier height. Error bars denote standard errors. Note, 1 adult ducked prior to squat-walking or hand-feet crawling on 1 trial each at chest- and hip-heights, respectively. And another adult squat-walked prior to hand-knees crawling at hip-height. (C) Head bumps for each age group at each barrier height. Green bars denote no head bumps; red bars denote initial head bumps; yellow bars denote traveling head bumps; and striped bars denote both initial and traveling head bumps.
To account for the effects of physical size on action duration, we normalized latency for passage by each individual’s height. Results replicated findings with non-normalized values. Thus, shorter durations in adults and 17-month-olds compared to 13-month-olds were not due to the older groups being taller and thus having longer legs and arms.
Follow-up infant group analyses:
For the two infant groups with non-overlapping walking experience, 17-month-olds were quicker at all barrier heights compared to 13-month-olds, Wald χ2 = 9.71, p = .002. Moreover, for both infant groups, trials were quicker with overhead, followed by eye and chest-height barriers, hip-height-barrier, and finally the knee-height barrier, ps < .001. However, for the 17-month-olds, we found no correlations between walking experience and latency for passage at any barrier height, ps ≥ .178.
Changes across trials:
Except for the slight decrease in latency for adults with the overhead barrier and for the 17-month-olds with hip- and knee-barrier heights (ts ≥ 2.13, ps ≤ .047), we found no significant differences in latency for passage between the first and last trial at any barrier height for any age group, ps ≥ .060.
Number of postural shifts.
Only one shift was necessary to navigate under barriers lower than overhead. Thus, multiple postural shifts incurred cost for passage latency. Excluding trials with the overhead barrier, postural shifts contributed to passage latency for infants, rs (≥194) ≥ .62, ps < .001, but not for adults, p = .280.
Adults were conservative in switching postures to navigate under the barrier, only transitioning to a different posture when necessary. As shown in Figure 3B, when the barrier was overhead, adults walked without any adjustments. For all other barrier heights, adults transitioned to another action only once, shifting seamlessly from walking to the chosen target action. Even when the barrier was at the lowest knee-height position, adults shifted to low crawling or belly crawling in one smooth transition.
Infants displayed a superfluous number of postural shifts (totals > 1, range = 1 to 11) while approaching all but the overhead barrier, and many actions (standing, squatting, sitting, kneeling) differed from the selected action for passage. Even at the overhead height, where shifting to another action was unnecessary, a few infants shifted posture prior to passage. Seventeen-month-olds shifted posture more than once on 25% of trials, and 13-month-olds shifted posture more than once on 37% of trials. Most multi-shift trials occurred at hip and knee heights (80% for 17-month-olds and 61% for 13-month-olds), meaning that most single-shift trials were at higher barrier heights. Moreover, of the multi-shift trials, infants’ initial postural shift differed from their selected action for passage on 96% of trials for 17-month-olds and 94% of trials for 13-month-olds.
The GEE confirmed differences in the number of postural shifts among age groups and barrier heights, Wald χ2 = 74.88, p < .001. For the overhead barrier, on average, adults and infants did not shift postures, ps ≥ .150. However, compared to the single transition adults displayed with the rest of the barrier heights, 17-month-olds shifted postures more frequently at eye-, hip- and knee-heights, ps ≤ .046, and 13-month-olds shifted postures more frequently at every barrier height, ps ≤ .002. Thirteen-month-olds (M = 1.50) displayed slightly more shifts than 17-month-olds (M = 1.11) at eye-height, p = .035. However, both infant groups displayed a similar number of postural shifts at the lower barriers (Ms = 1.26–2.56), ps ≥ .172.
Follow-up infant group analyses:
For the two infant groups with non-overlapping walking experience, 17-month-olds displayed fewer postural shifts at all barrier heights compared to 13-month-olds, Wald χ2 = 4.91, p < .001. Moreover, the GEE revealed a main effect of barrier height, Wald χ2 = 411.62, p < .001. For both infant groups, number of shifts was highest for knee-height, followed by hip-, chest- and eye-height barriers, and finally overhead, ps ≤ .003. However, for the 17-month-olds, walking experience was not correlated with the number of shifts at any barrier height, ps ≥ .255.
Changes across trials:
We compared the number of postural shifts between the first and last trial for every barrier height using paired-t-tests. We found no significant differences at any barrier height for any age group, ps ≥ .138.
Accuracy: Head Bumps
Initial head bumps never occurred in adults. Although infants could navigate under the barrier, most infants displayed initial head bumps (walked straight into the barrier) at least once, meaning they did not anticipate the impediment to walking—9/20 17-month-olds and 11/14 13-month-olds. Initial head bumps occurred mainly at eye-height (Ms = 11.5% and 40.7% of trials for 17- and 13-month-olds, respectively) and rarely at chest-height (3.0–5.7% of trials). As shown by the red bars and red-striped bars in Figure 3C, the proportion of these initial bumps differed across age groups and barrier heights (excluding the overhead barrier, where bumping was impossible), Wald χ2 = 43.50, p < .001. At eye-height, 17-month-olds displayed fewer initial bumps compared to 13-month-olds, p = .001.
Follow-up infant group analyses:
The difference in initial bumps remained among the 13- and 17-month-olds with non-overlapping walking experience. The GEE showed an interaction between group and barrier height, Walds χ2 = 10.98, p = .012. Seventeen-month-olds had fewer initial bumps compared to 13-month-olds at eye-height, p = .002, but no differences at other barrier heights, ps ≥ .726. However, for the 17-month-olds, we found no correlations between walking experience and the proportion of initial bumps at any barrier height, ps ≥ .331.
Changes across trials:
About half of the infants in each age group with initial head bumps at eye- and chest-heights did not bump their head on the last trial. The rest of the infants displayed initial bumps on intermediate trials and/or the last trial. Differences in initial head bumps from the first to last trials did not differ between age groups, X2s ≤ 3.73, ps ≥ .053.
Locomotor solutions after initial head bumps:
We analyzed infants’ selected solutions during trials with initial head bumps and the subsequent trial of the same barrier height. In these trials, infants in both age groups mostly persisted with the same locomotor solution despite experiencing an initial bump, and the frequency in persisting with the same solution did not differ between infant age groups, X2 (1, 33) =.85, p = .357. Of the few times when infants switched solutions, their selected solutions on subsequent trials were more appropriate (i.e., involved lowering their bodies) on 100% of trials for both 17- and 13-month-olds.
Adults never displayed traveling head bumps while passing under the barrier. In contrast, every infant displayed a traveling bump (bumped forehead or grazed top of head) at least once because they raised their heads too soon or did not adjust their posture sufficiently to clear the barrier. Thus, as shown by the yellow shaded bars in Figure 3C, the proportion of traveling bumps differed across age groups and barrier heights, Wald χ2 = 882.67, p < .001. At barrier heights where bumping was possible (excluding the overhead barrier), infants displayed more traveling bumps (Ms = 16.3–100%) compared to adults, ps ≤ .002. However, infant groups did not differ at any barrier height, ps ≥ .155. Moreover, infants bumped their head more on lower barrier heights compared to chest- and eye-height barriers, ps ≤ .001.
Follow-up infant group analyses:
For the two infant groups with non-overlapping walking experience, the proportion of traveling bumps was similar, Wald χ2 = 2.42, p = .491. Instead, the GEE revealed a main effect of barrier height, Wald χ2 = 564.84, p < .001, indicating that both groups of infants incurred more traveling bumps while going under the knee-height barrier, followed by the hip-height barrier, shoulder-height barrier, and finally the chest-height barrier, ps ≤ .001. Moreover, for the 17-month-olds, the proportion of traveling bumps was not correlated with walking experience at any barrier height, ps ≥ .189.
Changes across trials:
Traveling head bumps varied widely among infants in both age groups. For example, some infants showed evidence of learning across trials (traveling bumps on the first trial, but not on the last trial), some incurred traveling bumps on the first trial and on the last trial at that barrier height, and some showed traveling head bumps only on intermediate trials. Differences in traveling head bumps across trials between infant age groups were not significant at any barrier height, X2s ≤ 5.26, ps ≥ .072.
Locomotor solutions after traveling head bumps:
We analyzed infants’ selected solutions during trials with traveling head bumps and the subsequent trial at the same barrier height. As with initial head bumps, infants in both age groups mostly persisted with the same locomotor solution despite experiencing a traveling bump, X2 (1, 251) =.07, p = .798. Of the few times when infants switched solutions, their selected solutions on the subsequent trials were more appropriate (i.e., lowering their bodies), especially at higher barrier heights. Overall, we did not find differences between infant age groups in the frequency of switching to a lower strategy at any barrier height, X2s ≤ 1.53, ps ≥ .217.
Discussion
We examined the development of behavioral flexibility in younger and older infants (novice 13- and experienced 17-month-old walkers) and a comparison sample of adults. Whereas fluency is often an aesthetic desirable for motor skills, flexibility is a functional imperative because in most activities, task constraints are continually changing. Here, we used a new, adjustable, overhead barrier paradigm to test four critical aspects of flexibility—whether infants and adults show (1) a resourceful variety of solutions (2) tailored appropriately to the barrier height, and executed (3) quickly and (4) accurately (Bernstein, 1996). In our paradigm, all apertures were passable via multiple solutions, but each decrease in barrier height (from overhead to knee height) required a lower posture for passage. The penalty for errors was bumping the head on the barrier. Thus, flexible, seamless passage required participants to obtain and use perceptual information prior to passage, search for alternative solutions and weigh their relative costs, and discover and/or select the most appropriate solution for each barrier height. And, of course, participants required sufficient balance and coordination to implement the selected action.
Every participant altered their behavior based on barrier height at every trial, and except for 2 13-month-olds at knee-height, all found solutions for passage. Nevertheless, compared to infants, adults were more flexible on all four of Bernstein’s criteria. Adults (1) displayed a wide variety of bipedal (ducking, squat-walking), midway (half-kneeling, hands-feet crawling), and crawling solutions (hands-knees crawling, low crawling, belly crawling) across barrier heights; (2) found the most appropriate solution for each barrier height (e.g., squat-walked with the barrier at chest height and low-crawled with the barrier at knee height); and they implemented their solutions (3) quickly (within 4 seconds and shifted posture only when necessary), and (4) accurately (without bumping their heads).
In contrast, infants showed a narrower range of solutions, and consequently many solutions were inappropriate (e.g., hands-knees crawled rather than ducked at eye-height barrier). Moreover, infants were slower to find solutions and less accurate in implementing them. Infant improvements were related to age and walking experience.
Infant Solutions Were Resourceful, but Less So than Adults
Infants were less resourceful than adults in the sense that they displayed a narrower range of solutions. Some infants never ducked and most never squat-walked, half-kneeled, or hands-feet crawled, and 25% of 17-month-olds and 57% of 13-month-olds failed to find any solution for passage on at least one trial. Nonetheless, every infant was resourceful in the sense that they demonstrated a variety of solutions. Failure trials were rare (2.3% of 1089 trials) and many were due to infants’ first encounter with that barrier height. Even the two infants who failed to find solutions to pass under the knee-height barrier were savvy enough to switch from their upright posture to lower postures. In addition to their default walking posture (i.e., the posture infants used on warm-up trials with no overhead barrier), all but one 13-month-old demonstrated at least two alternative solutions, and all but one 17-month-old demonstrated at least three (see Figure 2B). In prior work with young, novice 12- and 13-month-old walkers on slopes and drop-offs, infants frequently showed no alternative strategies: They either walked over the edge and fell or avoided going (Adolph, 1997; Adolph & Eppler, 1998; Burnay et al., 2020; Karasik et al., 2014; Witherington, Campos, Anderson, Lejeune, & Seah, 2005).
So, why did infants demonstrate a greater variety of solutions in our overhead barrier paradigm? Put another way, why were young walkers better able to perceive the variety of affordances for navigating under low barriers compared with descending slopes and drop-offs (as in Adolph, 1997; Kretch & Adolph, 2013)? One possibility is that infants in the prior work did not realize that actions readily available in their repertoires (e.g., going down in crawling and sitting postures) were viable forms of locomotion for challenging slopes and drop-offs. Relatedly, overhead barriers may be more familiar to infants (in the form of tables and chairs that afford passage for crawling) relative to slopes and drop-offs. Alternatively, the visual salience of the overhead barrier right in front of their face may have prompted infants to lower themselves to the ground and thereby discover that crawling, low crawling, and belly crawling were viable solutions.
Infant Solutions Were Appropriate, but Less So than Adults
Studies of executive function show that young children demonstrate remarkable limitations in cognitive flexibility. For example, when 3-year-olds are asked to switch from sorting a set of cards by color to sorting the same cards by shape (or vice-versa), children perseverate and continue to sort the cards by the previous rule, despite explicit and repeated instructions to switch to the new rule (Kirkham, Cruess, & Diamond, 2003; Kloo, Perner, Kerschhuber, Dabernig, & Aichhorn, 2008; Zelazo, Frye, & Rapus, 1996). In contrast, we show that motor flexibility is present in young infants. Infants’ solutions were appropriate in the sense that actions were geared to barrier height, not randomly selected. Infant ducking and crawling were more frequent at the middle barrier heights (eye, chest, and hip heights) and low crawling and belly crawling were more frequent at the lowest knee-height barrier (Figure 2C). Similarly, the 17-month-olds never attempted hugely inefficient—but viable—solutions that their same-age counterparts regularly display on slopes and drop-offs such as scooting through the barrier in a sitting position or backing through the aperture feet first (Adolph, 1997; Adolph, Tamis-LeMonda, Ishak, Karasik, & Lobo, 2008; Karasik et al., 2014; Tamis-LeMonda et al., 2008). The discrepancy between the ability to switch behavior during our motor task and previously reported cognitive tasks might be that our stimuli change across trials and are clearly distinct (different barrier heights are easy to distinguish visually), which might facilitate infants to refocus their attention and inhibit their previous stimulus-response mapping. The stimuli in many cognitive tasks (cards with colors and shapes) do not change; what changes is what children are asked to do with the cards, which requires increased inhibitory control of the initial behavior (Diamond, Carlson, & Beck, 2010; Yerys & Munakata, 2006).
Nonetheless, infants’ solutions were less appropriate than those of adults. Infants did “too much” and persisted in doing so across trials. They crawled at eye- and chest-height when mid-way ducking and squat-walking strategies were more appropriate; they low-crawled and belly crawled at hip height when squat-walking, half-kneeling, and hands-feet crawling were more appropriate. Why this excess in low-to-the-ground strategies? Why the overkill? One possibility is that ducking, squat-walking, and half-kneeling were too difficult for infants to implement, especially for 13-month-olds whose upright balance is already precarious and leg strength and coordination is limited (Ivanenko, Dominici, Cappellini, & Lacquaniti, 2005; Ivanenko, Dominici, & Lacquaniti, 2007). Indeed, upright and mid-way strategies at eye-height increased with walking experience for the 17-month-olds. However, the fact that more than half of the infants in each age group demonstrated ducking suggests that this strategy may have been viable, but underused. Similarly, every infant was likely capable of hands-feet crawling, but most did not.
Alternatively, crawling is likely more familiar and habitual for infants than for adults. Although every baby was a walker, they likely use crawling for navigation on a daily or weekly basis. Not so for adults. Relatedly, infants may view hands-knees, low crawl, and belly crawling strategies as less costly compared to adults. Indeed, 5- to 6-year-old children are more likely than adults to hands-knees crawl and belly crawl to navigate bars placed strategically at heights (mid-calf to thigh) that allow both going under and over the bar (Comalli et al., 2017). Adults are biased to remain as upright as possible, even when increasing the cost of upright postures by adding ankle weights or starting in a crawling posture and when reducing the cost of crawling postures by padding the floor or adding a secondary task that requires crawling (Comalli et al., 2017).
More generally, the cost of motor actions may be less important to infants compared to adults. Human infants (just like infants of other mammalian species) expend energy needlessly in locomotor play (Mahler, Pine, & Bergman, 1975; Pellegrini, Dupuis, & Smith, 2007; Rheingold & Eckerman, 1970). They frequently walk with no end destination in sight or in mind (Hoch, Rachwani, & Adolph, 2020). They take just as many steps in an empty playroom as in a playroom filled with interesting toys designed to elicit locomotion (Hoch, O’Grady, & Adolph, 2019). Similarly, infant manual activity is exuberant and geared toward free exploration rather than efficient and geared toward cost reduction (Herzberg, Fletcher, Schatz, Tamis-LeMonda, & Adolph, in press).
Infants Were Slower to Find and Execute Solutions than Adults
Adults were uniformly fast at the overhead, eye-height, and chest-height barriers; their latency increased only at hip and knee heights, and the increase was slight, < 1s (read down first column in Figure 3A). Why so fast? Adults shifted posture only once at eye-height and lower barriers (read down first column in Figure 3B). The fact that every adult squat-walked at chest height (Figure 2B) with no increase in latency indicates that their slight increase in latency at chest, hip, and knee heights was due to the time to approach the barrier in a crawling posture. Thus, adults likely weigh the cost of increased time to passage while selecting a solution from their repertoires. Their bias to use bipedal and mid-way strategies likely incorporates (and mitigates) the cost of increased time for passage.
Infants were slower than adults at the overhead barrier height because of deficiencies in walking skill (infants walk more slowly), not because adults were taller and their legs were longer.. But infants’ latency increased at every lower barrier height (read down middle and last columns in Figure 3A). Why so slow, and why the increase? As with adults, the time to shift from upright to crawling postures incurs only a small increase in latency—not sufficient to explain infants’ dramatically increased latency at lower barrier heights. In prior work, older infants on slopes and drop-offs, frequently shifted seamlessly to an alternative posture with little increased cost to latency (Adolph, 1997; Karasik et al., 2014). Similarly, in the current study, the increased time to approach the barrier in a crawling posture does not explain the dramatic increase in latency across barrier heights.
Instead, latency increased so dramatically for infants because they displayed multiple shifts in posture prior to passage. Indeed, latency for passage and number of postural shifts were positively correlated. Infants’ first postural shift was rarely their final solution, indicating that babies did not immediately recognize how to navigate under the barrier. Instead, infants searched for a solution by shifting multiple times, often returning to upright or vacillating between two postures.
Why didn’t infants immediately recognize a viable solution for passage, especially at the lowest barriers when it should be clear that they needed to crawl? Most multi-shift trials occurred at the lowest barrier heights, where fewer strategies were viable and the requirement to crawl should be most apparent. Put another way, at eye and chest height where many more solutions were available in infants’ repertoires, they shifted immediately to their final (albeit inappropriate) solution of crawling. Possibly, the lowest barriers prompted infants to shift posture down to the floor. Now on the floor and close to the barrier, many actions were available (squatting, kneeling, sitting) that competed with strategies for passage. In addition, infants were sometimes compelled to explore the barrier by touching and pulling at it, and these exploratory actions also competed with strategies for passage. The final result was that these competing actions interfered with the process of strategy selection and incurred extraneous movements and wasted time.
Infants Were Less Accurate than Adults in Implementing Solutions
Adults never bumped their heads on the barrier, even when crossing barriers that required them to crawl (which is an action they rarely practice). In contrast, every infant bumped their head prior to or while navigating under the barrier. Initial head bumps occurred when infants walked straight into the barrier or because they lowered their heads prematurely and then raised them before the barrier. Traveling head bumps occurred because infants did not lower their heads sufficiently during passage. And infants did not learn from repeated bumps—infants mostly stuck with the same solution after experiencing a bump and thus bumped their heads over and over again. Possibly, infants misperceive the height of the barrier relative to their head height or misjudge the extent of ducking required. In particular, while crawling, view of the barrier is limited due to the horizontal position of the head (Franchak, Kretch, & Adolph, 2018; Kretch, Franchak, & Adolph, 2014). Likewise, infants display deficiencies in perceiving affordances for passage through apertures that varied in width (Brownell, Zerwas, & Ramani, 2007; Franchak & Adolph, 2012).
Alternatively, infants might not weigh the cost of head bumps as heavily as do adults. In some cases, infants bumped into the barrier so hard that they bounced backward (thus, we padded the edge of the barrier with foam). But in most cases, head bumps were relatively trivial and infants never cried and rarely appeared to notice the bump. Similarly, in prior work, infants repeatedly attempted to squeeze through impossibly narrow apertures that caused their heads to become wedged in the opening (Franchak & Adolph, 2012). Likewise, infants fall repeatedly during free play, despite head and torso impacts, and do not decrease their play with the objects and places implicated in the fall (Han & Adolph, 2021). Regardless, the head bumps provided infants with visceral perceptual feedback about affordances for clear passage.
Improvements Were Related to Infant Age and Walking Experience
Most outcome measures showed differences between the two infant groups. Compared to 13-month-olds, 17-month-olds exhibited fewer failures to find a solution for passage (and quickly learned from them); they were faster to find solutions, displayed fewer postural shifts prior to passage, and incurred fewer initial head bumps. The age groups did not differ in the frequency of traveling head bumps. Results replicate when comparing the two groups with nonoverlapping walking experience, indicating that improvements were driven by the 17-month-old, more experienced walkers. Moreover, experienced 17-month-olds exhibited a greater variety of solutions. Walking experience among the age-held-constant group (all 17-month-olds), which varied from 1.2 – 6.3 months, predicted only the proportion of upright and midway strategies at the eye-height barrier.
These findings suggest that infants’ improvements over time are due to age- and experience-related factors. Although we did not collect measures of perceptual or cognitive skills, the affordance of locomoting under a barrier is most likely a complex perceptual-motor and cognitive problem that integrates visual attention, height perception, and planning for appropriate strategy selection. Walking experience (a proxy for advanced motor skill) is also needed for quick and accurate implementation. Infants’ manual strategies with tools show similar findings—infants’ manual problem solving becomes more efficient and planful with age. For instance, 14-month-old infants reach with their preferred hand, disregarding the orientation of a spoon containing food, whereas older children anticipate the problem, alternating the hand to achieve an efficient grip (McCarty, Clifton, & Collard, 1999). Infants between 16 and 33 months of age also demonstrate more advanced spatial planning during object fitting (Jung, Kahrs, & Lockman, 2015). And infants’ success at opening everyday artifacts (e.g., twist-off containers) begin to emerge only at 18 months because children now know what to do and have the motoric ability to implement it (Rachwani, Tamis-LeMonda, Lockman, Karasik, & Adolph, 2020).
In the current study, every infant could have crawled under the lowest barriers, but many of the 13-month-olds did not. Every infant could have lowered their heads sufficiently in anticipation of the barrier height, but many of the 13-month-olds did not. Older, more experienced infants had the perceptual, motoric, and cognitive abilities to find a solution on almost every trial, select the most appropriate solution on eye- and knee-barrier heights, without wasted time and extraneous movements, and with accurate planning of action. To identify the key underlying skills, future studies should test the role of perceptual-motor and cognitive skills on behavioral flexibility.
Conclusions
Infants showed evidence of behavioral flexibility, but on Bernstein’s (1996) criteria, their actions were sub-optimal compared to adults, and older, more experienced infants generally fared better than younger, less experienced infants. Infants were less resourceful (displayed a narrower range of solutions), less able to select appropriate strategies (frequent use of “overkill” strategies), and less able to implement their strategies efficiently (slower to find and perform the solution) and accurately (without bumping their heads). Greater flexibility in older infants was likely due to improvements in their walking skill, perceptual-motor planning, and cognitive development. Thus, development of behavioral flexibility involves the contributions of multiple domains.
Acknowledgments
This research was supported by National Institute of Health and Human Development Grant R01-HD33486 to Karen E. Adolph. We gratefully acknowledge the infants and parents who participated. We thank the members of the NYU Infant Action Lab for assistance collecting and coding data.
Footnotes
With participants’ permission, videos and coding spreadsheets from each session are shared with authorized investigators on Databrary (https://nyu.databrary.org/volume/1312). The coding manual, coding scripts, processed data, analysis scripts (https://nyu.databrary.org/volume/1312/slot/54360), and exemplar video clips are publicly available. This study was not preregistered.
References
- Adolph KE (1997). Learning in the development of infant locomotion. Monographs of the Society for Research in Child Development, 62(3, Serial No. 251), 1–140. doi: 10.2307/1166199 [DOI] [PubMed] [Google Scholar]
- Adolph KE, & Eppler MA (1998). Development of visually guided locomotion. Ecological Psychology, 10, 303–321. [Google Scholar]
- Adolph KE, & Hoch JE (2019). Motor development: Embodied, embedded, enculturated, and enabling. Annual Review of Psychology, 70, 141–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adolph KE, & Robinson SR (2013). The road to walking: What learning to walk tells us about development. In Zelazo P (Ed.), Oxford handbook of developmental psychology (pp. 403–443). New York: Oxford University Press. [Google Scholar]
- Adolph KE, & Robinson SR (2015). Motor development. In Liben L & Muller U (Eds.), Handbook of child psychology and developmental science (7th ed., Vol. 2 Cognitive Processes, pp. 113–157). New York: Wiley. [Google Scholar]
- Adolph KE, Tamis-LeMonda CS, Ishak S, Karasik LB, & Lobo SA (2008). Locomotor experience and use of social information are posture specific. Developmental Psychology, 44, 1705–1714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adolph KE, Vereijken B, & Shrout PE (2003). What changes in infant walking and why. Child Development, 74, 474–497. [DOI] [PubMed] [Google Scholar]
- Bernstein NA (1996). On dexterity and its development. In Latash ML & Turvey MT (Eds.), Dexterity and its development (pp. 3–244). Mahwah, NJ: Erlbaum. [Google Scholar]
- Brownell CA, Zerwas S, & Ramani GB (2007). “So big”: The development of body self-awareness in toddlers. Child Development, 78, 1426–1440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burnay C, & Cordovil R (2016). Crawling experience predicts avoidance of real cliffs and water cliffs: Insight from a new paradigm. Infancy, 21, 677–684. [Google Scholar]
- Burnay C, R. C, Button C, Croft JL, Schofield M, Pereira J, & Anderson DI (2020). The effect of specific locomotor experiences on infants’ avoidance behavior on real and water cliffs. Developmental Science. doi: 10.1111/desc.13047 [DOI] [PubMed] [Google Scholar]
- Cole WG, Gill SV, Vereijken B, & Adolph KE (2014). Coping with asymmetry: How infants and adults walk with one elongated leg. Infant Behavior and Development, 37, 305–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Comalli DM, Franchak JM, Char A, & Adolph KE (2013). Ledge and wedge: Younger and older adults’ perception of action possibilities. Experimental Brain Research, 228, 183–192. doi: 10.1007/s00221-013-3550-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Comalli DM, Persand D, & Adolph KE (2017). Motor decisions are not black and white: Selecting actions in the ‘gray zone’. Experimental Brain Research, 235, 1793–1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond A, Carlson SM, & Beck DM (2010). Preschool children’s performance in task switching on the dimensional change card sort task: Separating the dimensions aids the ability to switch. Developmental Neuropsychology, 28, 689–729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, & Adolph KE (2012). What infants know and what they do: Perceiving possibilities for walking through openings. Developmental Psychology, 48, 1254–1261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, & Adolph KE (2014). Gut estimates: Pregnant women adapt to changing possibilities for squeezing through doorways. Attention, Perception, and Psychophysics, 76, 460–472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franchak JM, Kretch KS, & Adolph KE (2018). See and be seen: Infant-caregiver social looking during freely mobile play. Developmental Science, 21, e12626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson JJ (1979). The ecological approach to visual perception. Boston, MA: Houghton Mifflin. [Google Scholar]
- Gill SV, Adolph KE, & Vereijken B (2009). Change in action: How infants learn to walk down slopes. Developmental Science, 12, 888–902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney AL, & Cinelli ME (2013). Action strategies used by children to avoid two vertical obstacles in non-confined space. Experimental Brain Research, 229, 13–22. [DOI] [PubMed] [Google Scholar]
- Han D, & Adolph KE (2021). The impact of errors in infant development: Falling like a baby. Developmental Science, 24, e13069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herzberg O, Fletcher K, Schatz J, Tamis-LeMonda CS, & Adolph KE (in press). Infant exuberant object play at home: Immense amounts of time-distributed, variable practice. Child Development. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoch JE, O’Grady SM, & Adolph KE (2019). It’s the journey, not the destination: Locomotor exploration in infants. Developmental Science, 22, e12740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoch JE, Rachwani J, & Adolph KE (2020). Where Infants Go: Real-Time Dynamics of Locomotor Exploration in Crawling and Walking Infants. Child Dev, 91(3), 1001–1020. doi: 10.1111/cdev.13250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hommel B (2003). Acquisition and control of voluntary action. In Maasen WPGRS (Ed.), Voluntary action: An issue at the interface of nature and culture. Oxford: Oxford University Press. [Google Scholar]
- Ivanenko YP, Dominici N, Cappellini G, & Lacquaniti F (2005). Kinematics in newly walking toddlers does not depend upon postural stability. Journal of Neurophysiology, 94, 754–763. doi: 10.1152/jn.00088.2004 [DOI] [PubMed] [Google Scholar]
- Ivanenko YP, Dominici N, & Lacquaniti F (2007). Development of independent walking in toddlers. Exercise and Sport Sciences Reviews, 35, 67–73. [DOI] [PubMed] [Google Scholar]
- Jeannerod M (1988). The neural and behavioral organization of goal-directed movements. Oxford, England: Clarendon Press. [Google Scholar]
- Jung WP, Kahrs BA, & Lockman JJ (2015). Manual action, fitting, and spatial planning: Relating objects by young children. Cognition, 134, 128–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karasik LB, Tamis-LeMonda CS, & Adolph KE (2014). Crawling and walking infants elicit different verbal responses from mothers. Developmental Science, 17, 388–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karasik LB, Tamis-LeMonda CS, & Adolph KE (2016). Decisions at the brink: Locomotor experience affects infants’ use of social information on an adjustable drop-off. Frontiers in Psychology, 7, 797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenward B, Folke S, Holmberg J, Johansson A, & Gredebäck G (2009). Goal directedness and decision making in infants. Developmental Psychology, 45, 809–819. [DOI] [PubMed] [Google Scholar]
- Kirkham NZ, Cruess L, & Diamond A (2003). Helping children apply their knowledge to their behavior on a dimension-switching task. Developmental Science, 6, 449–467. [Google Scholar]
- Kloo D, Perner J, Kerschhuber A, Dabernig S, & Aichhorn M (2008). Sorting between dimensions: conditions of cognitive flexibility in preschoolars. Journal of Experimental Child Psychology, 100, 115–134. [DOI] [PubMed] [Google Scholar]
- Kording KP, & Wolpert DM (2006). Bayesian decision theory in sensorimotor control. Trends Cogn Sci, 10(7), 319–326. doi: 10.1016/j.tics.2006.05.003 [DOI] [PubMed] [Google Scholar]
- Kretch KS, & Adolph KE (2013). Cliff or step? Posture-specific learning at the edge of a drop-off. Child Development, 84, 226–240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kretch KS, & Adolph KE (2017). The organization of exploratory behaviors in infant locomotor planning. Developmental Science, 20, e12421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kretch KS, Franchak JM, & Adolph KE (2014). Crawling and walking infants see the world differently. Child Development, 85, 1503–1518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahler M, Pine F, & Bergman A (1975). The psychological birth of the human infant. New York: Basic Books. [Google Scholar]
- McCarty ME, Clifton RK, & Collard RR (1999). Problem solving in infancy: The emergence of an action plan. Developmental Psychology, 35, 1091–1101. [DOI] [PubMed] [Google Scholar]
- McGraw MB (1935). Growth: A study of Johnny and Jimmy. New York, NY: Appleton-Century Crofts. [Google Scholar]
- Pellegrini AD, Dupuis D, & Smith PK (2007). Play in evolution and development. Developmental Review, 27, 261–276. [Google Scholar]
- Rachwani J, & Adolph K (2021). Flexibility in Action: Development of Locomotion Under Overhead Barriers. Databrary. 10.17910/b7.1312. [DOI] [PMC free article] [PubMed]
- Rachwani J, Tamis-LeMonda CS, Lockman JJ, Karasik LB, & Adolph KE (2020). Learning the designed actions of everyday objects. Journal of Experimental Psychology: General, 149, 67–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Regia-Corte T, & Wagman JB (2008). Perception of affordances for standing on an inclined surface depends on height of center of mass. Experimental Brain Research, 191, 25–35. [DOI] [PubMed] [Google Scholar]
- Rheingold HL, & Eckerman CO (1970). The infant separates himself from his mother. Science, 168, 78–83. [DOI] [PubMed] [Google Scholar]
- Schmuckler MA (1996). Development of visually guided locomotion: Barrier crossing by toddlers. Ecological Psychology, 8, 209–236. [Google Scholar]
- Siegler RS, & Jenkins EA (1989). How children discover new strategies. Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Stoffregen TA, Yang C, Giveans MR, Flanagan M, & Bardy BG (2009). Movement in the perception of an affordance for wheelchair locomotion. Ecological Psychology, 21, 1–36. [Google Scholar]
- Tamis-LeMonda CS, Adolph KE, Lobo SA, Karasik LB, Dimitropoulou KA, & Ishak S (2008). When infants take mothers’ advice: 18-month-olds integrate perceptual and social information to guide motor action. Developmental Psychology, 44, 734–746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van der Meer ALH (1997). Visual guidance of passing under a barrier. Early Development and Parenting, 6, 149–157. [Google Scholar]
- von Hofsten C (2004). An action perspective on motor development. Trends in Cognitive Sciences, 8, 266–272. [DOI] [PubMed] [Google Scholar]
- Witherington DC, Campos JJ, Anderson DI, Lejeune L, & Seah E (2005). Avoidance of heights on the visual cliff in newly walking infants. Infancy, 7, 285–298. [DOI] [PubMed] [Google Scholar]
- Yerys BE, & Munakata Y (2006). When labels hurt but novelty helps: Children’s perseveration and flexibility in a card-sorting task. Child Development, 66, 1589–1607. [DOI] [PubMed] [Google Scholar]
- Zelazo P, Frye D, & Rapus T (1996). An age-related dissociation between knowing rules and using them. Cognitive Development, 11, 11–63. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
With participants’ permission, raw videos and coding spreadsheets from each session are shared with authorized investigators on Databrary (https://nyu.databrary.org/volume/1312). The coding manual, coding scripts, processed data, analysis scripts (https://nyu.databrary.org/volume/1312/slot/54360) and exemplar video clips are publicly available.