

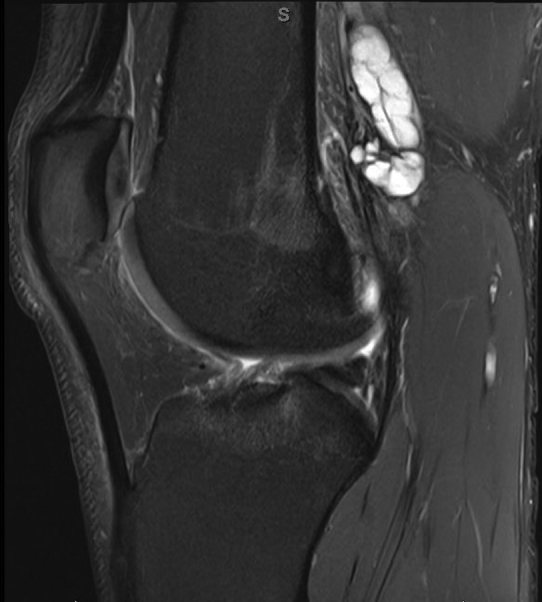
Popliteal artery adventitial cystic disease (ACD) is a rare cause of lower extremity claudication. This report describes a unique case of a 21-year-old college wrestler who presented with a 6-month history of left lower extremity lifestyle limiting claudication. The patient provided consent for publication of the images and case details. He had undergone an extensive workup by his sports medicine physician and was referred to our clinic after a magnetic resonance image of the left knee revealed a 1.6 × 1.5 × 4.6 cm multiloculated elongated cystic lesion arising from and compressing the left popliteal artery (A/cover). He was taken to the operating room for resection of the left popliteal artery mass and reconstruction with reversed ipsilateral greater saphenous vein from a prone approach. On the back table, on opening the artery, a multiloculated lesion was noted to be arising from within the lumen of the popliteal artery (B). This lesion was incised, and thick mucinous material was expressed from within lesion cavity (C). The patient did well postoperatively and had resolution of his claudication. The patient agreed to allow the authors to publish the case details and images.
Popliteal artery ACD affects 1 in 1200 patients with claudication.1 It affects males primarily, with a male-female ratio of 5:1.1 These patients are relatively young, with a typical age at diagnosis in the mid-30s.1 Currently, a developmental theory is generally accepted as the etiology of ACD.1 It proposes that mesenchymal mucin-secreting cells are implanted in the adventitia of the vessel during development.1 Affected patients typically present with short-distance calf claudication. Magnetic resonance imaging is considered the optimal diagnostic modality for ACD and can classically demonstrate an “hourglass” deformity in the popliteal artery. Management of ACD is determined by the luminal status of the popliteal artery and can be divided into nonresectional and resectional methods. Nonresectional methods include transluminal angioplasty, imaging-guided cyst aspiration, and operative cyst evacuation and excision.2 Resectional methods involve arterial resection and reconstruction. Recurrence of ACD can be seen in 15% of patients who underwent cyst evacuation and 6.7% of those undergoing resection.1,3,4 Overall, popliteal ACD is a rare curative cause for claudication in young patients without atherosclerotic risk factors.

From Midwestern Vascular Surgery Society
Footnotes
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the Journal policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Appendix.
Cover Image.
References
- 1.Bergan J.J. In: Vascular Surgery. 4th ed. Rutherford R.B., editor. WB Saunders; 1995. Adventitial cystic disease of the popliteal artery; pp. 883–888. [Google Scholar]
- 2.Rai S., Davies R.S., Vohra R.K. Failure of endovascular stenting for popliteal cystic disease. Ann Vasc Surg. 2008;23:410.e1–410.e5. doi: 10.1016/j.avsg.2008.01.014. [DOI] [PubMed] [Google Scholar]
- 3.Belmir H., Tijani Y., El Khloufi S., Sefiani Y., El Mesnaoui A., Lekehel B. Cystic adventitial disease of the popliteal artery. J Vasc Surg Cases Innov Tech. 2020;6:344–345. doi: 10.1016/j.jvscit.2020.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hernández Mateo M.M., Serrano Hernando F.J., Martínez López I., González Sánchez S., Hernando Rydings M., Saiz Jerez A., et al. Cystic adventitial degeneration of the popliteal artery: report on 3 cases and review of the literature. Ann Vasc Surg. 2014;28:1062–1069. doi: 10.1016/j.avsg.2013.09.013. [DOI] [PubMed] [Google Scholar]