

Abstract
Background
Hidden blood loss (HBL) after total hip arthroplasty (THA) would lead to many undesirable consequences. Traditional Chinese medicine (TCM) is now increasingly used for hidden blood loss. We performed this systematic review and meta-analysis to summarize the effect and safety of TCM treatment of HBL after THA.
Methods
We searched PubMed, Embase, Cochrane Library, CNKI, VIP, WanFang, and CBM for the updated articles published from the inception of each database to May, 2022, among which results such as abstracts, comments, letters, reviews, and case reports were excluded. The efficacy and safety of TCM treatment of HBL after THA were synthesized and discussed by the outcomes of total blood loss (TBL), hidden blood loss (HBL), hemoglobin (Hb), and hematocrit (HCT), and the incidence of adverse reactions.
Results
A total of 12 articles and 881 patients were included. There were 441 cases in the intervention group and 440 cases in the control group. Compared with the control group, the intervention group had more advantages in TBL (MD = −251.68, 95% CI = [−378.36, −125]; Z = 3.89, P < 0.00001), HBL (MD = −159.64, 95% CI = [−252.56, −66.71]; Z = 3.37, P=0.0008), Hb (MD = 11.39, 95% CI = [7.35, 15.43]; Z = 5.53, P < 0.00001), and HCT (MD = 2.87, 95% CI = [0.97, 4.78]; Z = 2.95, P=0.003), and had less incidence of adverse reactions (OR = −0.20, 95% CI = [−0.35, −0.05]; Z = 2.64, P=0.008).
Conclusion
TCM has advantages in the efficacy and safety of treating hidden blood loss after THA. The strength of the evidence of the research results is limited by the quality of the included literature, and more high-quality RCTs are needed to confirm.
1. Introduction
Total hip arthroplasty (THA) is the most commonly used and effective treatment for femoral neck fractures, hip arthritis, developmental dysplasia of the hip, and ischemic necrosis of the femoral head [1]. THA is always accompanied by blood loss, including intraoperative blood loss and postoperative blood loss, as well as some hidden blood loss (HBL) [2]. Sehat et al. [3]reported that HBL after THA was 49% of the total blood loss (TBL), since which surgeons learned that HBL plays an important role in surgery [4, 5].
HBL refers to the accumulation of blood in the joint cavity, or extravasation into the interstitial space, and the loss of hemoglobin (Hb) in the body caused by factors such as traumatic stress and other factors that induce hemolysis [6], of which the clinical manifestations are swelling, ecchymosis, and a significant decrease in Hb [7, 8]. It is one of the main causes of postoperative anemia in patients [9], which can affect the functional recovery and quality of life of the patient after surgery, and even increase the risk of infection and death, or extend the length of hospital stay [10]. Clinically, intraoperative and postoperative intravenous tranexamic acid (TXA) and other hemostatic drugs are often used to reduce HBL [5]. However, it has been reported that sometimes blood loss is not effectively controlled by these methods and with several complications [11]. There are increasing research studies reported using traditional Chinese medicine (TCM) theory to treat patients who suffer from blood loss according to symptoms and signs [12–14]. The main objective of this study was to evaluate the clinical efficacy and safety of TCM in treating HBL after THA.
2. Materials and Methods
2.1. Data Source
We searched PubMed, Embase, Cochrane Library, CNKI, VIP, WanFang, and CBM for the updated articles published from the inception of each database to May 1st, 2022. When duplicate publications were identified, we chose the most complete and recent trial. Two investigators (Z.Y. and X.W.) independently retrieved the related studies in the database and excluded duplicate publications. The combined text and medical subject heading (MeSH) terms were cross-searched using MeSH and free words as follows: (((Hidden blood loss[Title/Abstract]) AND ((((Hip Prosthesis Implantation[Title/Abstract]) OR (Hip Replacement, Total[Title/Abstract])) OR (Total Hip Arthroplasty[Title/Abstract])) OR (“Arthroplasty, Replacement, Hip”[Mesh]))) AND ((((Decoction[Title/Abstract]) OR (Tang[Title/Abstract])) OR (Fang[Title/Abstract])) OR ((“Medicine, Chinese Traditional”[Mesh]) OR ((Chung I Hsueh[Title/Abstract]) OR (Traditional Chinese Medicine[Title/Abstract]))))) AND ((randomized controlled trial [Publication Type] OR randomized [Title/Abstract] OR placebo [Title/Abstract]))
2.2. Inclusion and Exclusion Criteria
Inclusion criteria are as follows: (1) Type of Study: the study must be a randomized controlled trial (RCT); (2) Participants: patients receiving THA; (3) Intervention measures: the intervention group must be treated with TCM (decoction, capsule, ointment) or combined with western medicine, and the control group is treated only with western medicine; and (4) Outcomes: TBL, HBL, Hb, hematocrit (HCT), and incidence of adverse reactions.
Exclusion criteria are as follows: (1) studies are not RCTs; (2) patients not receiving THA; (3) incomplete or unidentified data; (4) duplicate publications; and (5) abstracts, reviews, case reports, and letters.
2.3. Study Selection and Data Extraction
Two independent researchers (Z.Y. and X.W.) read the title, abstract, and full text, screened the literature according to the inclusion and exclusion criteria, and cross-checked the results. If there is a disagreement, the third researcher (Y.L.X.) will be consulted. Extract data from the included literature, including first author, sample size of the study, gender, mean age or age range, intervention protocol, duration time, and outcomes.
2.4. Quality Assessment
The quality of the included studies was assessed by The Cochrane Risk Bias Tool in the Cochrane Handbook for Systematic Reviews of Interventions. The following messages were evaluated: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessments, incomplete outcome data, selective reporting, and other biases.
2.5. Statistical Analysis
RevMan5.4 and Stata15.0 software was used for statistical analysis. The included studies are tested for homogeneity. Pooled odds ratios (OR) and 95% confidence intervals (95% CI) were calculated to report dichotomous data, and mean differences (MD) with 95% CI were used to report continuous data. Statistical heterogeneity was considered present when P < 0.1 or I2 > 50%. When high heterogeneity existed, a random-effects model was used for meta-analysis. Sensitivity analysis was also used to analyze the source of heterogeneity. Publication bias was evaluated visually by funnel plots and considered significant when P < 0.05 in either Begg's test or Egger's test when the inclusion was more than 10 articles.
3. Results
3.1. Search Results
Our initial search yielded 85 articles in total, 32 of which were removed for duplication. After screening titles and abstracts, a further 17 items were taken away. 36 articles were reviewed, among which 12 were included in this meta-analysis [15–26]. No further study was identified by manual search. The flow diagram of study selection was shown in Figure 1.
Figure 1.

PRISMA flow diagram of the study selection process.
3.2. Study Characteristic
12 studies with a total of 881 subjects were included in the meta-analysis. The outcomes of the studies are shown as follows: TBL, HBL, Hb, HCT, and incidence of adverse reactions. The main characteristics of the 12 articles were summarized in Table 1.
Table 1.
Characteristics of the 12 studies included in the meta-analysis.
| Study | Sample size (IG/CG) | Gender (Men/Women) | Mean age or age range | Intervention Protocol | Duration time | Outcomes | |||
|---|---|---|---|---|---|---|---|---|---|
| IG | CG | IG | CG | IG | CG | ||||
| Cai2020 | 36/36 | - | - | 69.03 ± 5.64 | 70.39 ± 5.51 | Sanqi zhixue Decoction combined TXA | TXA | 7 days | ①②③④ |
| Ji2019 | 15/15 | 6/9 | 6/9 | 69.73 ± 0.79 | 70.87 ± 1.65 | Bazhen Decoction combined TXA | TXA | 14 days | ①②③ |
| Ke2017 | 30/30 | 11/19 | 14/16 | 71.1 ± 8.3 | 66.8 ± 10.1 | Taohong Siwu Decoction combined TXA | TXA | 7 days | ①② |
| Li2022 | 37/34 | 26/11 | 24/10 | 77.2 ± 7.7 | 79.6 ± 9.3 | Yiqi Huoxue ointment combined TXA | TXA | 7 days | ①②③④ |
| Ma2018 | 53/54 | 24/29 | 26/28 | 71.99 ± 7.29 | 72.03 ± 7.31 | Bazhen Decoction combined TXA | TXA | 14 days | ②③ |
| Miao2017 | 62/62 | 38/24 | 41/21 | 75.67 ± 8.32 | 73.72 ± 7.83 | Fuyuan Decoction | TXA | 7 days | ②③ |
| Qiu2018 | 30/30 | 20/10 | 22/8 | 64.25 ± 2.56 | 64.23 ± 2.54 | Yunnan Baiyao combined TXA | TXA | 7 days | ①②④ |
| Qiu2019 | 33/34 | 19/16 | 18/17 | 69.13 ± 3.26 | 68.62 ± 3.18 | Bazhen decoction combined TXA | TXA | 14 days | ①②③④ |
| Sheng2017 | 20/20 | 6/14 | 7/13 | 68.7 ± 5.33 | 70.7 ± 4.68 | Addition of Shiquan Dabu Decoction | Anti-infection and anticoagulation | 14 days | ①②③ |
| Wang2015 | 45/45 | 22/23 | 21/24 | 66.0 ± 6.7 | 66.2 ± 6.5 | Tanshinone Capsules | Low molecular weight heparin | 7 days | ①②③⑤ |
| Xiao2020 | 30/30 | 9/21 | 8/22 | 65.6 ± 4.8 | 66.2 ± 5.2 | Sanqi zhixue Decoction | No hemostatic drugs | 14 days | ①②③ |
| Zhou2019 | 50/50 | 20/30 | 22/28 | 52–70 | 50–70 | Chuanxi San combined TXA | TXA | 30 days | ② |
CG: control group; IG: intervention group “-”: not mentioned ① TBL, ② HBL, ③ Hb, ④ HCT, ⑤ Incidence of Adverse Reactions.
3.3. Quality of the Evidence
The results of the risk of bias assessment for all included studies are summarized in Figure 2. Randomization was used in all articles, six studies [15, 16, 19, 22, 25, 26] used the means of random number table, two studies [17, 20] grouped according to the odd-even number of admission case numbers, one study [23] used random and double-blind methods, one study [21] using the envelope method, were considered to have a low risk of bias in the random sequence generation domain. One study [18] grouped according to the treatment method was considered to have a high risk of bias in the random sequence generation domain and blinding of participants and personnel. One study [24] did not mention random methods were considered to have an unclear risk of bias. Two studies [23, 25] mentioned blinding of participation and outcome assessment were considered as low risk, while others were not mentioned, thus they were considered to have an unclear risk of bias. One study [21] had lost to follow-up cases and was considered high risk, and the rest of the studies were complete with data and considered as low risk. The selective reporting and other bias in the included articles resulted in an unclear risk of bias.
Figure 2.
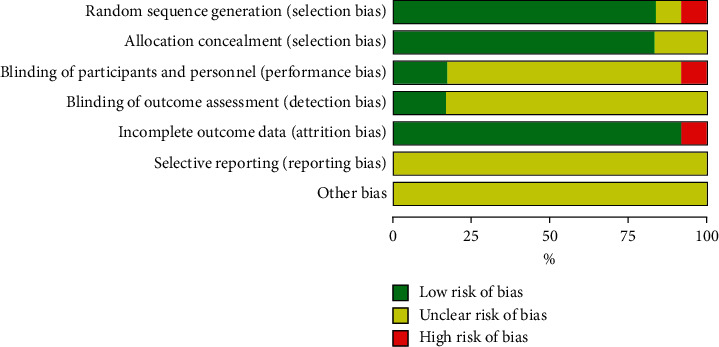
Risk of bias graph.
3.4. Outcome Measures
3.4.1. TBL
9 studies [15–18, 21–25] involving 550 participants reported the outcome of TBL. Heterogeneity test analysis suggested that there was heterogeneity (P < 0.00001, I2 = 98%). The sensitivity analysis was carried out one by one, and it was found that there was no significant change, thus the random effects model was used. The meta-analysis demonstrated there was a significant difference between the two groups (MD = -251.68, 95% CI = [−378.36, −125]; Z = 3.89, P < 0.00001) (Figure 3).
Figure 3.

Forest plots for TCM on TBL.
3.4.2. HBL
12 studies [15–26] involving 881 participants reported the outcome of TBL. Heterogeneity test analysis suggested that there was heterogeneity (P < 0.00001, I2 = 99%). The random effects model was used. The HBL in the intervention group was less than that in the control group (MD = -159.64, 95% CI = [−252.56, −66.71]; Z = 3.37, P=0.0008) (Figure 4(a)).
Figure 4.

(a) Forest plots for TCM on HBL. (b) Forest plots and subgroup analysis of duration time for TCM on HBL.
Subgroup analysis showed that TCM for tonifying qi and blood and TCM for activating blood stasis both have a significant difference in HBL (Figure 4(b)), which was consistent with the results reported in every study. However, both groups have high heterogeneity, which may be due to the differences in the duration and time of the research.
3.4.3. Hb
9 studies [15, 16, 18–21, 23–25] involving 661 participants reported the outcome of Hb. Heterogeneity test analysis suggested that there was heterogeneity (P < 0.00001, I2 = 88%). The sensitivity analysis was carried out one by one, and it was found that there was no significant change, thus the random effects model was used as well. The meta-analysis demonstrated there was a significant difference between the two groups (MD = 11.39, 95% CI = [7.35, 15.43]; Z = 5.53, P < 0.00001) (Figure 5).
Figure 5.
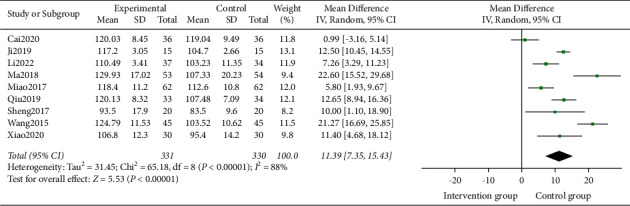
Forest plots for TCM on Hb.
3.4.4. HCT
4 studies [15, 18, 21, 22] compared HCT after TCM treatment with the control group, involving 270 participants. Heterogeneity test analysis suggested that there was heterogeneity (P=0.04, I2 = 64%). The sensitivity analysis was carried out one by one, and it was found that there was no significant change, thus the random effects model was used. The HCT in the intervention group was more than that in the control group (MD = 2.50, 95% CI = [1.28, 3.71]; Z = 4.03, P < 0.00001) (Figure 6).
Figure 6.

Forest plots for TCM on HCT.
3.4.5. Incidence of Adverse Reactions
One study [24] involving 90 participants reported the incidence of adverse reactions to TCM. The intervention group was safer than the control group (OR = −0.20, 95% CI = [−0.35, −0.05]; Z = 2.64, P=0.008) (Figure 7).
Figure 7.

Forest plots for incidence of adverse reactions.
3.5. Publication Bias
The publication bias of outcomes was evaluated using funnel plots based on the HBL of 12 studies. The funnel plot (Figure 8), which was asymmetrically distributed on both sides, and the Egger's test (P=0.001) of the HBL suggested that there was potential publication bias in the included studies.
Figure 8.

Funnel plots of the HBL.
4. Discussion
THA is recognized as one of the most effective surgical methods for the treatment of end-stage hip joint disease [27]. There are different degrees of hidden blood loss after surgery [28]. HBL refers to the effective circulation of hemoglobin and red blood cells entering the interstitial space after the operation, resulting in swelling of the affected limb which is not directly lost to the outside world. The hazards of hidden blood loss include postoperative anemia and complications such as slow wound healing, poor functional recovery, and increased risk of infection caused by anemia [29, 30]; increased risk of deep vein thrombosis in the lower extremities; increased probability of cardiovascular and cerebrovascular accidents; and subcutaneous ecchymosis [31]. Hidden blood loss falls into the category of “blood syndrome” in clinical Chinese medicine and can be traced back to “The Yellow Emperor's Classic of Internal Medicine.” It said: “injury of YANG-collateral leading to outwards bleeding…yin collateral impairment causing hematocheiza”.
The “yin collateral impairment” and “hematocheiza” described here are actually the same as the hidden blood loss described today. Blood circulating out of the vessels that cause swelling of the affected limb after the operation is called blood stasis. In this case, TCM thinks the bleeding cannot be stopped blindly but should remove blood stasis and stop it. In “A Treatise on Blood Troubles,” a famous classic TCM book on blood syndrome proposed four methods of treating blood syndrome: hemostasis, removing blood stasis, tranquilizing blood, and invigorating deficiency, which have been used by future generations to this day. Therefore, to treat blood syndrome, it is necessary to distinguish the cause of it. It could be caused by the stagnation of qi that blocks the normal flow of blood in the vessels, the deficiency of qi to promote blood circulation, or blood deficiency that leads to the inability to fill the vessels, so the flow rate slows down. Different etiologies and syndromes have different methods of differentiation and treatment.
This study systematically reviewed the clinical efficacy and safety of TCM in the treatment of HBL after THA. A total of 12 articles were included for the meta-analysis. The included studies used Bazhen Decoction, Tanshinone Capsules, Sanqi Zhixue Decoction, Taohong Siwu Decoction, Yiqi Huoxue ointment, Fuyuan Decoction, Yunnan Baiyao, Shiquan Dabu Decoction, and Chuanxi San to treat HBL. The prescriptions used are regulating qi and activating blood stasis to stop bleeding, tonifying qi and blood to stop bleeding, and all treatments were from the cause of blood syndrome. Therefore, the subgroup analysis showed that whether taking TCM for tonifying qi and blood or activating blood stasis, the HBL in the intervention group was smaller than the control group. The results of the meta-analysis showed that TCM has more advantages in TBL, HBL, Hb, HCT, and the incidence of adverse reactions after THA, and the difference is statistically significant.
Our review has several limitations. First, the sample size of this meta-analysis was relatively small. As a result, the unknown risk of bias caused by incomplete data could constrain our results. Second, due to the large heterogeneity of the included studies, only a random effect model can be adopted, which will have a certain impact on the results. Third, the intervention protocol varied significantly in the duration of treatment time, ranging from 7 to 30 days, and the type of intervention TCM varied from each other (capsule, decoction, ointment). At the same time, the control group received different interventions as well, which may be the reason for the high heterogeneity.
Despite these limitations, this meta-analysis provides information on the association between TCM and HBL after THA.
5. Conclusion
In conclusion, this article shows that TCM is more effective and safer than Western medicine in treating HBL after THA. Therefore, in the clinical treatment of HBL after THA, TCM should be added to the conventional treatment to improve the clinical efficacy. However, due to the small number of included studies and their low quality, our conclusions remain to be confirmed by further high-quality RCTs.
Acknowledgments
This project was supported by the National Natural Science Foundation of China (81974576).
Contributor Information
Yongliang Xia, Email: 20043077@zcmu.edu.cn.
Weifeng Ji, Email: jiweif@yeah.net.
Ethical Approval
Systematic review and meta-analysis will not require ethical approval.
Disclosure
Ze Yang and Xiang Wang are co-first authors.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
Ze Yang and Xiang Wang curated the data. Ze Yang, Xiang Wang, and Zheyun Xu were responsible for formal analysis. Ze Yang, Xiang Wang, Qike Xu, and Yongliang Xia handled the investigation. Ze Yang, Qike Xu, and Weifeng Ji were in charge of project administration. Xiang Wang, Zheyun Xu, Yongliang Xia, and Weifeng Ji were responsile for resource management. Ze Yang and Xiang Wang were responsile for software. Ze Yang, Zheyun Xu, and Yongliang Xia were responsile for supervision. Ze Yang, Zheyun Xu, and Yongliang Xia validated the data. Ze Yang and Xiang Wang visualized the data. Ze Yang and Xiang Wang wrote the original draft. Ze Yang, Qike Xu, and Weifeng Ji wrote the review and edited the manuscript.
References
- 1.Tanaka R., Shigematsu M., Motooka T., Mawatari M., Hotokebuchi T. Factors influencing the improvement of gait ability after total hip arthroplasty. The Journal of Arthroplasty . 2010;25(6):982–985. doi: 10.1016/j.arth.2009.06.009. [DOI] [PubMed] [Google Scholar]
- 2.Wang J. Q., Chen L. Y., Jiang B. J., Zhao Y. M. Oxidized regenerated cellulose can reduce hidden blood loss after total hip arthroplasty: a retrospective study. Journal of Investigative Surgery . 2019;32(8):716–722. doi: 10.1080/08941939.2018.1458166. [DOI] [PubMed] [Google Scholar]
- 3.Sehat K. R., Evans R., Newman J. H. How much blood is really lost in total knee arthroplasty?. Correct blood loss management should take hidden loss into account. The Knee . 2000;7(3):151–155. doi: 10.1016/s0968-0160(00)00047-8. [DOI] [PubMed] [Google Scholar]
- 4.Zhou Y., Fu X., Yang M., Ke S., Wang B., Li Z. Hidden blood loss and its possible risk factors in minimally invasive transforaminal lumbar interbody fusion. Journal of Orthopaedic Surgery and Research . 2020;15(1):p. 445. doi: 10.1186/s13018-020-01971-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sehat K. R., Evans R. L., Newman J. H. Hidden blood loss following hip and knee arthroplasty. Correct management of blood loss should take hidden loss into account. Journal of Bone and Joint Surgery British Volume . 2004;86-B(4):561–565. doi: 10.1302/0301-620x.86b4.14508. [DOI] [PubMed] [Google Scholar]
- 6.Liu X., Zhang X., Chen Y., Wang Q., Jiang Y., Zeng B. Hidden blood loss after total hip arthroplasty. The Journal of Arthroplasty . 2011;26(7):1100–1105. doi: 10.1016/j.arth.2010.11.013. [DOI] [PubMed] [Google Scholar]
- 7.Ghadimi K., Levy J. H., Welsby I. J. Perioperative management of the bleeding patient. British Journal of Anaesthesia . 2016;117(3):18–30. doi: 10.1093/bja/aew358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhou X. S. W. Z. K., Sun T. S. China’s orthopedic surgery accelerated rehabilitation-an expert in perioperative health management. Chinese Journal of Bone and Joint Surgery . 10(01):1–7. [Google Scholar]
- 9.Vles G. F., Corten K., Driesen R., van Elst C., Ghijselings S. G. Hidden blood loss in direct anterior total hip arthroplasty: a prospective, double blind, randomized controlled trial on topical versus intravenous tranexamic acid. Musculoskelet Surg . 2021;105(3):267–273. doi: 10.1007/s12306-020-00652-0. [DOI] [PubMed] [Google Scholar]
- 10.Smilowitz N. R., Oberweis B. S., Nukala S., et al. Association between anemia, bleeding, and transfusion with long-term mortality following noncardiac surgery. The American Journal of Medicine . 2016;129(3):315–323. doi: 10.1016/j.amjmed.2015.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wu J., Zhou Y. Q., Deng J. H., Han Y. G., Zhu Y. C., Qian Q. R. Ideal intraarticular application dose of tranexamic acid in primary total knee arthroplasty: a prospective, randomized and controlled study. Annals of Translational Medicine . 2020;8(21):p. 1353. doi: 10.21037/atm-20-3064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gan T., Liu Y. D., Wang Y., Yang J. Traditional Chinese Medicine herbs for stopping bleeding from haemorrhoids. Cochrane Database of Systematic Reviews . 2010;10 doi: 10.1002/14651858.CD006791.pub2.Cd006791 [DOI] [PubMed] [Google Scholar]
- 13.Shi S. Y., Zhou Q., He Z. Q., et al. Traditional Chinese medicine (Liang-Xue-Di-Huang decoction) for hemorrhoid hemorrhage: study protocol clinical trial (SPIRIT compliant) Medicine (Baltimore) . 2020;99(16) doi: 10.1097/md.0000000000019720.e19720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Xu S., Pang Q., Lin Z., Zhang N. Effect of integrated traditional Chinese and Western medicine therapy for acute hypertensive intracerebral hemorrhage: a meta-analysis. Artificial Cells, Nanomedicine, and Biotechnology . 2017;45(6):1186–1191. doi: 10.1080/21691401.2016.1215327. [DOI] [PubMed] [Google Scholar]
- 15.Cai L. M., Tan Z. C., Xiao S. Y., Ye Z. S., Zhang B. S., Yuan S. C. Clinical study on Sanqi Zhixue decoction for reducing blood loss in total knee arthroplasty. Journal of Guangzhou University of Traditional Chinese Medicine . 37(07):1252–1258. [Google Scholar]
- 16.Ji W. H., Shen J. R. Clinical observation on preventing from anemia after minimally invasive total hip replacement in elderly with the Bazhen decoction plus tranexamic acid. Traditional Chinese Medicine Clinical Research . 11(16):71–74. [Google Scholar]
- 17.Ke Z. Y., Shi J. W. Clinical observation of Taohong Siwu decoction in relieving swelling and pain of limbs after Total Hip replacement. Chinese Medical Sciences . 8(05):197–199. [Google Scholar]
- 18.Li S. B., Meng L., Zhang X. Y. Effect of Yiqi Huoxue ointment combined with tranexamic acid on perioperative occult blood loss and hemorheology in total hip replacement. Modern Journal of Integrated Traditional Chinese and Western Medicine . 31(01):57–61+80. [Google Scholar]
- 19.Ma S. C., Chen X. M., Qi Z. Y., Li Y. L. Effect of Bazhen decoction combined with perioperative blood management on elderly hip joint Observation of the intervention effect of replacement surgery. Guangxi Traditional Chinese Medicine . 41(05):35–37. [Google Scholar]
- 20.Miao J. J., Zhou H. L., Lu S. S., Li Y. Q. Effects of Fuyuan Decoction on implicit and rapid recovery after THA. Li Shizhen medicine and materia medica research . 28(9):2169–2171. [Google Scholar]
- 21.Qiu Q. H., Ma S. T., Li Y. P., Sun Z. Q., Wang K., Bo B. Influence of bazhen decoction on hidden blood loss after total hip replacement in elderly. Chinese Journal of Orthopedics and Traumatology . 27(01):27–30. [Google Scholar]
- 22.Qiu W. K., Xu W., Li L., Su Z. Y., Zhang Y. H. A comparative study of tranexamic acid and Yunnan Baiyao on reducing blood loss in total hip arthroplasty. Chinese Journal of Bone and Joint Injury . 33(06):565–567. [Google Scholar]
- 23.Sheng L. W., Zhou H., Fang Y. Y., Peng L., Dong G. Effect of addition of shiquan Dabu decoction on hidden blood loss after total hip replacement. China Modern Applied Pharmacy . 34(03):420–422. [Google Scholar]
- 24.Wang G. B., Dai H. D., Chen R. Y. Clinical effect of Tanshinone Capsules on invisible blood loss after total hip arthroplasty postoperative. Chinese Journal of Biochemical Medicine . 35(12):145–147. [Google Scholar]
- 25.Xiao S. Y., Cai L. M., Tan Z. C., Ye Z. S., Zhang B. S., Yuan S. C. Clinical study on Sanqi Zhixue tang for blood loss during perioperative stage of total hip arthroplasty. Journal Of New Chinese Medicine . 522020377530 [Google Scholar]
- 26.Zhou X. C., Xiang J., Hu M. F., Xia X. B. Chuanxi powder combined with tranexamic acid to prevent and treat 50 cases of hidden blood loss after total hip replacement. Chinese Journal of Orthopedics and Traumatology . 27(08):37–39. [Google Scholar]
- 27.Moerenhout K., Derome P., Laflamme G. Y., Leduc S., Gaspard H. S., Benoit B. Direct anterior versus posterior approach for total hip arthroplasty: a multicentre, prospective, randomized clinical trial. Canadian Journal of Surgery . 2020;63(5):E412–e417. doi: 10.1503/cjs.012019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wan R. R., Wang Y. L., Wu X. C., et al. Hidden blood loss and the influencing factors after laparoscopic cholecystectomy. ANZ Journal of Surgery . 2020;90(1-2):103–108. doi: 10.1111/ans.15502. [DOI] [PubMed] [Google Scholar]
- 29.Ban Z. T., Liu R. Z. Progress on hidden blood loss after lumbar interbody fusion. Zhong Guo Gu Shang . 2018;31(11):1077–1080. doi: 10.3969/j.issn.1003-0034.2018.11.018. [DOI] [PubMed] [Google Scholar]
- 30.Ye M., Zhou J., Chen J., Yan L., Zhu X. Analysis of hidden blood loss and its influential factors in myomectomy. Journal of International Medical Research . 2020;48(5) doi: 10.1177/0300060520920417.030006052092041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cai T., Chen D., Wang S., et al. Perioperative hidden blood loss in elderly cervical spondylosis patients with anterior cervical discectomy fusion and influencing factors. Geriatr Orthop Surg Rehabil . 2021;12 doi: 10.1177/21514593211002164.215145932110021 [DOI] [PMC free article] [PubMed] [Google Scholar]