

Abstract
Background Reconstruction of large foot and ankle defects is a difficult task due to less available local soft tissue and more critical from functional point of view. To overcome the limitations associated with locoregional flaps and free flaps, reverse peroneal artery (RPA) flap was selected and its usefulness in reconstruction of distal large defects of the ankle and foot and its complications were studied.
Materials and Methods This is a prospective observational study done in 20 patients treated as cohort within 2 years and 8 months from January 2018 to August 2020. Large defects of foot and ankle were reconstructed with RPA flap and evaluated for its usefulness. Three cases were evaluated with computed tomography angiography postoperatively, to assess the vascular pattern.
Conclusion RPA flap is a versatile and very reliable flap for the reconstruction of large and distal defects of foot and ankle. It is safely done in children and in acute trauma without any major complications.
Keywords: reverse peroneal artery flap, reconstruction of foot and ankle defects, peroneal perforator fasciocutaneous flaps, reverse flow flaps, CT peripheral angiogram, peroneal artery communications
Introduction
Reconstruction of large foot and ankle defects is a difficult task due to less availability of local soft tissues. 1 2 Regional flaps like reverse sural artery (RSA) flap, 3 4 lateral supramalleolar artery flap, 5 perforator-based fasciocutaneous flap, perforator propeller flap, 6 7 and perforator plus flaps 8 are frequently used, while cross leg 9 and free flaps 10 11 are also recommended to reconstruct foot defects. Certain limitations of these flaps are as follows: RSA flap does not reach the distal third of the foot and the source vessel may be in the zone of injury. Lateral supramalleolar flap and perforator-based fasciocutaneous flaps cannot usually cover large and distal defects of the foot and are associated with complications like venous congestion. Limitation for cross leg flaps is that maintenance of odd position of legs together for 3 weeks and free flap needs expertise and infrastructure and are expensive. Reverse peroneal artery (RPA) flap 12 13 was selected to overcome the limitations associated with locoregional flaps; distant and free flaps in the reconstruction of large defects of the ankle and foot and their usefulness and complications were studied.
Materials and Methods
This is a prospective cohort study done between January 2018 and August 2020. The study included a total of 20 patients between 5 and 50 years of age, with large defects involving ankle and foot, requiring flap cover. These defects were reconstructed with RPA flaps. Due permission was obtained from the institutional ethical committee and informed consent was obtained from the patients.
Operative Procedure
The RPA flap was planned in patients in whom pulse was palpable in at least one of all the three major vessels at the level of the ankle, and color Doppler was performed to make sure the blood flow in three major vessels is adequate. Peroneal artery perforators were localized with a hand-held Doppler probe of 8 MHz. The perforators of the middle third leg with good signal were marked along a line joining the lateral malleolus and head of the Fibula. The flap axis is along the sural nerve, which is a line joining the midpoint of lateral malleolus and tendoachilles and mid-popliteal point. The flap was marked along the axis, keeping the superior border two fingers breadth from the popliteal crease, laterally up to lateral axial lines including marked peroneal perforators ( Fig. 1 ). The pivot point for flap transposition should be above the level of 5 cm from the tip of lateral malleolus to safeguard the distal communication between peroneal, posterior, and anterior tibial vessels ( Fig. 2 ).
Fig. 1.

Preoperative planning of reverse peroneal artery flap, P denotes the pivot point of the flap.
Fig. 2.

Normal communications of peroneal artery with anterior tibial and posterior tibial arteries. RPA, reverse peroneal artery.
Patients were operated under regional anesthesia in a semiprone position. The dissection of RPA flap was started along the medial border of the flap marking in subfascial plane, either including or sparing sural nerve (nerve-sparing RPA flap) until we reach the lateral border of Soleus muscle where we can identify the target peroneal perforators ( Fig. 3A ).
Fig. 3.

( A–F ) The various steps of the reverse peroneal artery flap.
Then the dissection was continued incising the lateral border of the flap that opens the lateral compartment of the leg. Peroneal muscles were identified and the peroneus brevis muscle was dissected from the fibula, and periosteum on fibula was incised just above the level of the middle peroneal perforator ( Fig. 3B and C ).
Subperiosteal dissection was done to identify and isolate the peroneal vessels. From the medial aspect, the middle peroneal perforator is traced to peroneal vessels. The peroneal vessels are then clamped proximal to the entry of the large middle peroneal perforator. The peroneal vessels were ligated, cut, and included into the flap after confirming the adequate distal perfusion of the foot and flap
The peroneal vessel was dissected along with perforators distally, disconnecting all of its muscular branches and preserving cutaneous branches up to the pivot point of the flap, which is 5 cm ( Fig. 3D above the tip of the lateral malleolus). The donor area was covered with a split-thickness skin graft ( Fig. 3E ).
In an islanded RPA flap ( Fig. 6 ), skin flaps were dissected in the subdermal plane on either side of the pedicle. After the flap elevation, skin flaps were used to close the donor area to avoid exposure of the gastrosoleus tendon. Postoperatively the limb is splinted in plaster of paris slab and nursed in the lateral position with limb elevation.
Fig. 6.

Series of cases where islanded reverse peroneal artery was done for dorsum of foot defects in patients including pediatric age group subjects.
The flap was monitored for venous congestion, discoloration, edema, and for any other complications. Patients were followed till the complete healing of the wound.
Computed tomography (CT) angiography of both lower limbs was done in three of the cases after the 10th postoperative day to identify the changes in vascular pattern in the flap and the reconstructed limb in comparison with the normal limb.
All of the interpolated RPA flaps were divided after 3 to 4 weeks. The demographic parameters such as age, sex of the patient, etiology, time of presentation, details of defect like site, size, extent and details of flap, location of the middle peroneal perforator from the tip of the lateral malleolus, and complications were noted down and tabulated.
Results
Out of the 20 patients in this study, 18 patients were male and 2 were female patients. Seven patients were children of less than 15 years of age. All had sustained injuries in road traffic accidents. The size of the defects ranged from 7 × 5 cm to 15 × 10 cm. The size of the flap for reconstruction ranged from 13 × 6 cm to 29 × 12 cm. The distance of the middle peroneal perforator from tip of the lateral malleolus ranged from 10 to 12 cm in children and 17 to 20 cm in adults. The pedicle length varied from 5 to 21 cm. The distance of the superior border of the flap from popliteal fossa ranged from 2 to 5 cm ( Table 1 ).
Table 1. Demographic details of cases included in the study.
| Case no. | Age/sex | Etiology | Site of defect | Pedicle length | Outcome/complication | Size of defect in cms | Size of the flap in cm |
|---|---|---|---|---|---|---|---|
| 1 | 23/M | RTA | Rt. foot | 20 | Good | 15 ×10 | 26 ×12 |
| 2 | 26/M | RTA | Rt. foot | 15 | Good | 13 ×11 | 28 × 13 |
| 3 | 22/M | RTA | Rt. foot | 18 | Marginal necrosis | 12 ×10 | 29 ×12 |
| 4 | 8/F | RTA | Rt. foot | 7 | Good | 11 × 6 | 18 × 7 |
| 5 | 14/M | RTA | Rt. foot and ankle | 9 | Good | 10 × 7 | 19 × 8 |
| 6 | 21/M | RTA | Rt. foot | 13 | Subflap collection | 12 × 6 | 20 × 7 |
| 7 | 25/M | RTA | Rt. foot | 18 | Good | 12 × 8 | 29 × 10 |
| 8 | 21/M | RTA | Rt. foot | 21 | Mild SSG loss | 11 × 10 | 29 × 12 |
| 9 | 20/M | RTA | Rt. foot | 17 | Good | 12 × 8 | 26 × 10 |
| 10 | 30/M | RTA | Rt. foot | 16 | Good | 13 × 7 | 28 × 8 |
| 11 | 23/M | RTA | Lt. foot and ankle | 13 | Good | 13 × 7 | 22 × 9 |
| 12 | 25/M | RTA | Lt. foot | 18 | Mild loss of SSG | 11 × 6 | 28 × 8 |
| 13 | 6/M | RTA | Rt. foot | 5 | Good | 8 × 6 | 14 × 7 |
| 14 | 11/M | RTA | Rt. foot | 7 | Good | 7 × 5 | 13 × 7 |
| 15 | 25/F | RTA | Rt. foot | 19 | Subflap collection | 14 × 7 | 26 × 8 |
| 16 | 50/M | RTA | Lt. sole | 16 | Marginal necrosis | 15 × 8 | 20 × 10 |
| 17 | 7/M | RTA | Rt. foot | 8 | Good | 10 × 5 | 18 × 7 |
| 18 | 5/M | RTA | Rt. foot | 5 | Mild loss of SSG | 7 × 5 | 13 × 6 |
| 19 | 30/M | RTA | Rt. foot and ankle | 17 | Good | 15 × 7 | 22 × 9 |
| 20 | 8/M | RTA | Rt. foot | 7 | Good | 8 × 5 | 16 × 7 |
Abbreviations: F, female; Lt, left; Rt, right; M, male; RTA, road traffic accident.
Fig. 5.

Dorsum of foot ( A and C ) along with ankle defects ( B ) reconstructed with reverse peroneal artery (RPA) flap. Far-right photos in A and B depict the follow-up pictures of the flap after 6 months of surgery. ( A ) Case 1—A 30-year-old male with posttraumatic defect over dorsum of foot with size 137 cm reconstructed, with RPA flap of size 28 8cm. Flap settled well. ( B ) Case 2—A 30-year-old male patient with posttraumatic defect over the dorsum of foot and ankle of size 157cm was reconstructed with RPA flap of size 229 cm. Flap settled well. ( C ) Case 3—A 25-year-old male patient with posttraumatic defect over dorsum of left foot of size 116 cm was reconstructed with RPA flap of size 288 cm. This patient had a minor loss of SSG over the donor site. ATA, anterior tibial artery; PTA, posterior tibial artery; PA, peroneal artery.
Islanded RPA flap was done in eight patients. All flaps survived and no venous congestion was observed in any of these flaps. Postoperatively, marginal necrosis of a few mm was seen in two patients that was managed conservatively. Loss of skin graft at the flap donor area was noted in three patients that healed in 4 weeks.
Three cases were evaluated with CT angiography study on the 10th postoperative day for case 1, 30th postoperative day for case 2, and 2 years postoperatively for case 3 to know the vascular pattern in the flap and in the limb. It was found that there was a significant increase of 0.4 mm internal diameter of peroneal artery in flap limb compared with normal limb. It was also noted that there was an increase in the internal diameter of communicating vessels connecting the peroneal artery with the branches of anterior tibial arteries and posterior tibial arteries in the foot and ankle region. Increase in the vascularity of flap was noted in all of the three patients ( Table 2 ) ( Fig. 4 ).
Table 2. CT angiography findings of increase in the internal diameter of flap feeder vessels and opening of communicating vessels between PA, ATA, and PTA (and their branches) in flap limb when compared with normal limb.
| Peroneal artery | ATA | PTA | Lateral malleolar artery | Lateral plantar artery | Communicating vessel between PA and PTA | |
|---|---|---|---|---|---|---|
| Case 1 (10th POD) | 0.51 | 0.51 | 0.29 | 0.9 | 0.12 | 1.26 mm |
| Case 2 (1 mo) | 0.3 | 0.37 | 1.4 | 0.9 | 0.12 | 1.94 mm |
| Case 3 (4 mo) | 0.55 | 0.2 | 0.4 | 0.1 |
Abbreviations: ATA, anterior tibial artery; CT, computed tomography; PTA, posterior tibial artery; PA, peroneal artery; POD, postoperative day.
Fig. 4.
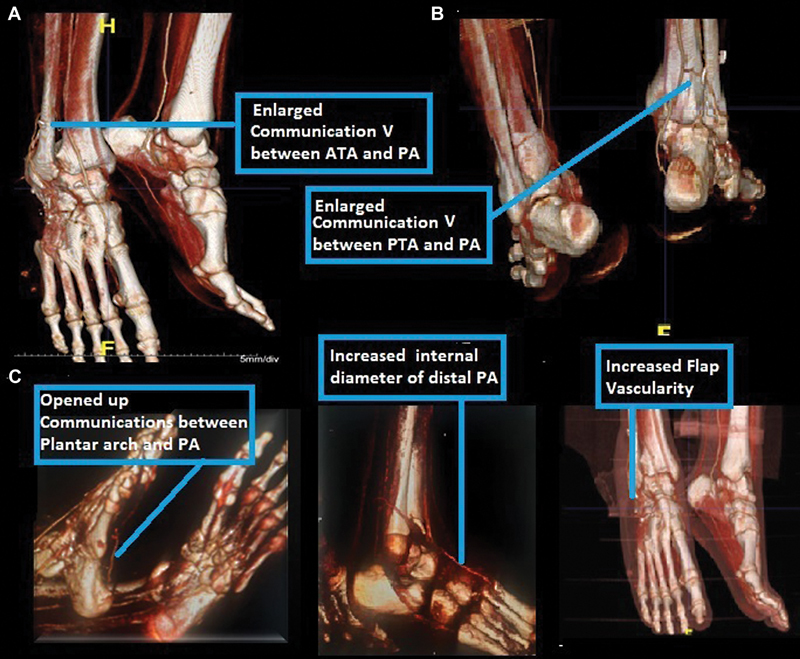
Postoperative findings in computed tomography angiography. Findings of the flap limb versus normal limb. RPA, reverse peroneal artery.
Discussion
Reconstruction of complex soft tissue defects around the ankle and foot is a big challenge.
Various reconstructive options have been recommended according to reconstructive ladder such as local cutaneous flaps, regional pedicled fasciocutaneous flaps, cross leg flaps, and free flaps 1 . Local flaps in the foot have a limitation of adequacy of tissue. Regional flaps were described like RSA flaps and its modifications. 4 Lateral supramalleolar flap, 5 fasciocutaneous flaps, 6 perforator propeller flaps, 7 and perforators plus flaps 8 are adequate to cover only medium-sized defects but not large distal defects of the foot. Bhandari et al 1 in their study analyzed all reconstructive procedures done for ankle and foot defects and found that RSA flap was reliable flap for the reconstruction of superficial noncomplicated soft tissue defects of ankle and up to midfoot region of moderate size.
Regional flaps like RSA flap were frequently used but were associated with complications like venous congestion and partial necrosis in high-risk group patients with comorbidities 14 15 Measures to increase coverage and decrease complications are of only limited usefulness. Baumeister et al 14 in their study showed that RSA flaps are not free from complications like venous congestion and partial flap necrosis in high-risk group patients. Large RSA flaps showed venous congestion leading to partial flap necrosis as studied by Grandjean et al. 16
RSA flap, fasciocutaneous flaps, and perforator propeller flaps from the same limb reach up to the proximal or middle of the foot but not up to base of toes. 13 However, we can follow the reconstructive elevator and choose free flap reconstruction 17 18 when expertise and infrastructure are available. Li et al 19 have concluded that free flaps play a major role in reconstruction of complex, large distal defects of the foot and ankle than pedicled flaps in their comparative study.
Cormack and Lamberty 20 21 described that peroneal artery supplies entire posterolateral aspect of calf region through its upper and middle perforators. By including the distal peroneal artery and all the perforators up to large middle perforator into the flap, the length dimension of the flap can be increased up to the popliteal crease, which facilitates the flap's distal most reach. 4 The venous drainage can be increased by including the short saphenous vein into the flap. Supercharging of this flap can be possible by including sural nerve and arterial plexus of vessels that will help in taking the whole skin in the calf region as the flap. This makes the RPA flap more robust, reliable and with inclusion of short saphenous vein and two big venae comitantes, the venous congestion will not be a problem.
Our study evaluates the RPA flap 12 22 for its feasibility of coverage of large defects of foot and ankle and its complications. The present technique of including the peroneal artery with large internal diameter along with its perforators in the flap acts as arterial supercharging of the flap and increased venous drainage via peroneal venae comitantes. This significantly increases the perfusion pressure in the flap taken from the upper third of the leg. With these advantages, flap from the upper leg achieves all the advantages of an axial pattern flow. As the flap can be extended up to popliteal crease with pivot point at 5 cm above the tip of lateral malleolus, flap has a long pedicle; hence, the flap can reach distal most part of dorsum or sole of the foot ( Fig. 7 ).
Fig. 7.

( A - D ) Case of road traffic accident with the patient sustain injury to plantar surfaces of both feet following which RSA flap was done for right foot and RPA flap was done for the left foot. Postoperative result in the bottom picture. RPA, reverse peroneal artery; RSA, reverse sural artery flap.
Islanded RPA flap was done as single stage in our study safely in eight patients. Exposure of tendoachilles at flap donor site was also avoided by doing an islanded RPA flap ( Fig. 6 ).
The incidence of venous congestion is very low with RPA flap. The flap can be designed of the size around 29 × 12 cm that could easily cover the largest of foot defects and can reach up to the base of the toes also. We used this flap to reconstruct large defects in seven children below 15 years of age in our study with good outcome establishing safety in children.
As the importance of the peroneal artery in arterial supply of the foot is minimal, the difficult reconstruction achieved with sacrifice of it with the RPA flap is not of any consequence. The increased amount of soft tissue transferred, the more distal reach, increased reliability, and ease of rotation compared with any other regional flap including the RSA flap helped us in the salvage of these limbs without the need of microvascular surgery. RPA flap effectively covers entire ankle and foot region just as effectively as free flap.
RPA flap done for 20 cases in our study was for posttraumatic defects due to road traffic accidents with good results, so established safety in acute trauma also.
CT angiography study done in three cases in postoperative period confirms that RPA flap has good reverse blood supply into distal peroneal artery from posterior tibial artery and anterior tibial artery through communicating vessels and plantar arch. The vessel caliber of peroneal artery and communicating vessel is increased after flap transfer ( Fig. 4).
We compared our study with the existing two studies in the literature by Tharayil and Patil 12 and Bhatt et al 13 ( Table 3 ).
Table 3. The comparison of the current study to other similar studies 4 5 .
| Study | Total flaps | No. of children <15 years | Etiology of defects | Site of defect | Reach of the flap | Complications | RPA flap modifications | CT angiography |
|---|---|---|---|---|---|---|---|---|
| Tharayil and Patil 12 | 22 | 2 (9%) | Variable trauma 50% |
Ankle and foot | Distal reach up to base of toes | Minor | Islanded and pedicled flaps | Not done |
| Bhatt et al 13 | 10 | Nil | All cancer cases No trauma |
Ankle and foot | Bases of toes | One case—fibula exposed | Both | Not done |
| Present study | 20 | 7 (35%) | Safe in major trauma | Dorsum of the foot in 19 and sole of the foot in one (1) but in extended proximally to ankle in 3 cases | Bases of the toes in and 1st web space in 2 cases. Covered entire width of dorsum and sole of the foot | Marginal necrosis of few mm | Peninsular (60%) and islanded (40%) | Increase in internal diameter of communicating vessels b/w PA, ATA, PTA |
Abbreviations: ATA, anterior tibial artery; PA, peroneal artery; PTA, posterior tibial artery; RPA, reverse peroneal artery; RSA, reverse sural artery flap; RTA, road traffic accident.
Conclusion
RPA flap from the calf region provides reliable cover for the defects involving the entire dorsum or sole of the foot. It can reach up to the bases of the toes with good wound healing without major complications. It can be done safely even in the pediatric age group, in acute trauma. It can be done as a single procedure by islanding it. Postoperative CT angiography demonstrated improved blood supply to flap by enlarged communications between peroneal and both anterior tibial vessels and posterior tibial vessels in the foot and ankle region.
Acknowledgments
I would like to thank Dr. V. Battacharya, former professor & HOD, BIMS, Varanasi, for his constant support and guidance. I would also like to thank Radiology Faculty Dr. Nadheem and Dr. Vijaya Kumari Whole Team Plastic-Surgery, OGH, my husband Dr. Srinivas S.S, Professor & HOD Neurosurgery, my son Dr. S. Ahlad, and my parents P.V.G . Krishna Rao, P. Parvathi Ratnam for their support.
Conflict of Interest None declared.
Patient Consent
The authors certify that they have obtained all appropriate patient consent forms.
References
- 1.Bhandari P S, Bath A S, Sadhotra L P, Singh M, Mukherjee M K. Management of soft tissue defects of the ankle and foot. Med J Armed Forces India. 2005;61(03):253–255. doi: 10.1016/S0377-1237(05)80167-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Godina M. Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg. 1986;78(03):285–292. doi: 10.1097/00006534-198609000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Follmar K E, Baccarani A, Baumeister S P, Levin L S, Erdmann D. The distally based sural flap. Plast Reconstr Surg. 2007;119(06):138e–148e. doi: 10.1097/01.prs.0000259203.79909.7e. [DOI] [PubMed] [Google Scholar]
- 4.Masquelet A C, Romana M C, Wolf G. Skin island flaps supplied by the vascular axis of the sensitive superficial nerves: anatomic study and clinical experience. Plast Reconstr Surg. 1992;89:1115–1121. doi: 10.1097/00006534-199206000-00018. [DOI] [PubMed] [Google Scholar]
- 5.Masquelet A C, Beveridge J, Romana C, Gerber C. The lateral supramalleolar flap. Plast Reconstr Surg. 1988;81(01):74–81. doi: 10.1097/00006534-198801000-00014. [DOI] [PubMed] [Google Scholar]
- 6.Pontén B. The fasciocutaneous flap: its use in soft tissue defects of the lower leg. Br J Plast Surg. 1981;34(02):215–220. doi: 10.1016/s0007-1226(81)80097-5. [DOI] [PubMed] [Google Scholar]
- 7.Andrei R, Popescu S A, Zamfirescu D. Lower limb perforator propeller flaps - clinical applications. Chirurgia (Bucur) 2014;109(03):299–309. [PubMed] [Google Scholar]
- 8.Luo Z, Lv G, Wei J. Comparison between distally based peroneal and posterior tibial artery perforator-plus fasciocutaneous flap for reconstruction of the lower extremity. Burns. 2020;46(01):225–233. doi: 10.1016/j.burns.2019.06.002. [DOI] [PubMed] [Google Scholar]
- 9.Stark R B. The cross-leg flap procedure. Plast Reconstr Surg (1946) 1952;9(03):173–204. doi: 10.1097/00006534-195203000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Acar M A, Güleç A, Aydin B K, Erkoçak ÖF, Yilmaz G, Şenaran H. Reconstruction of foot and ankle defects with a free anterolateral thigh flap in pediatric patients. J Reconstr Microsurg. 2015;31(03):225–232. doi: 10.1055/s-0034-1395888. [DOI] [PubMed] [Google Scholar]
- 11.Gupta A, Lakhiani C, Lim B H. Free tissue transfer to the traumatized upper extremity: risk factors for postoperative complications in 282 cases. J Plast Reconstr Aesthet Surg. 2015;68(09):1184–1190. doi: 10.1016/j.bjps.2015.05.009. [DOI] [PubMed] [Google Scholar]
- 12.Tharayil J, Patil R K. Reverse peroneal artery flap for large defects of ankle and foot: a reliable reconstructive technique. Indian J Plast Surg. 2012;45(01):45–52. doi: 10.4103/0970-0358.96584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bhatt Y C, Singh S, Doshi P, Vaghani S G. Reverseperoneal artery flap for large heel and sole defects: a reliable coverage. World J Plast Surg. 2017;6(02):212–219. [PMC free article] [PubMed] [Google Scholar]
- 14.Baumeister S P, Spierer R, Erdmann D, Sweis R, Levin L S, Germann G K.A realistic complication analysis of 70 sural artery flaps in a multimorbid patient group Plast Reconstr Surg 200311201129–140., discussion 141–142 [DOI] [PubMed] [Google Scholar]
- 15.Herlin C, Bekara F, Bertheuil N. Venous supercharging reduces complications and improves outcomes of distally based sural flaps. J Reconstr Microsurg. 2017;33(05):343–351. doi: 10.1055/s-0037-1598620. [DOI] [PubMed] [Google Scholar]
- 16.Grandjean A, Romana C, Fitoussi F. Distally based sural flap for ankle and foot coverage in children. Orthop Traumatol Surg Res. 2016;102(01):111–116. doi: 10.1016/j.otsr.2015.10.010. [DOI] [PubMed] [Google Scholar]
- 17.Battiston B, Antonini A, Tos P, Daghino W, Massazza G, Riccio M. Microvascular reconstructions of traumatic-combined tissue loss at foot and ankle level. Microsurgery. 2011;31(03):212–217. doi: 10.1002/micr.20863. [DOI] [PubMed] [Google Scholar]
- 18.Zhu Y L, He X Q, Wang Y, Lv Q, Fan X Y, Xu Y Q. Traumatic fore foot reconstructions with free perforator flaps. J Foot Ankle Surg. 2015;54(06):1025–1030. doi: 10.1053/j.jfas.2015.04.019. [DOI] [PubMed] [Google Scholar]
- 19.Li X, Cui J, Maharjan S, Lu L, Gong X. Reconstruction of the foot and ankle using pedicled or free flaps: perioperative flap survival analysis. PLoS One. 2016;11(12):e0167827. doi: 10.1371/journal.pone.0167827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cormack G, Lamberty B. Edinburgh: Churchill Livingstone; 1995. The Arterial Anatomy of Skin Flaps. [Google Scholar]
- 21.Taylor G I, Chubb D P, Ashton M W. True and 'choke' anastomoses between perforator angiosomes: part I. Anatomical location. Plast Reconstr Surg. 2013;132(06):1447–1456. doi: 10.1097/PRS.0b013e3182a80638. [DOI] [PubMed] [Google Scholar]
- 22.Li S J, Cheng H, Fang X. Modified reversed superficial peroneal artery flap in the reconstruction of ankle and foot defects following severe burns or trauma. Burns. 2017;43(04):839–845. doi: 10.1016/j.burns.2016.12.003. [DOI] [PubMed] [Google Scholar]