

Abstract
Aim and Objective
Submandibular oncocytomas are rare benign salivary gland neoplasms, normally involves the parotid gland and few instances are stated in the submandibular gland region. As the clinical and histopathological features are overlapping to another salivary gland tumor like pleomorphic adenoma or warthin tumour, they are often misdiagnosed. They are typically found in patients aged 50–70 years with no gender preference. The aim of this paper is to assess the clinicopathological functions, diagnostic standards and treatment of submandibular gland oncocytomas via a series of three case reports.
Method and Results
We report a three case series of unilateral submandibular gland oncocytoma with female to male ratio 2:1, Size of tumor ranged from 1.8 to 10 cm, 2 cases have painless swelling and one involved tender mass. FNAC and CT scan confirmed the presence of an oncocytoma. The patient underwent unilateral submandibular gland resection and on follow up no evidence of any recurrence was identified.
Conclusion
Submandibular oncocytomas often present as solitary slow growing painless masses, which are firm on clinical examination. CT followed by fine-needle aspiration cytology (FNAC) would be the preferred diagnostic modalities. Due to its low rate of malignant transformation and recurrence, the best treatment is local resection with follow-up as necessary.
Keywords: Submandibular oncocytomas, Onkocytes, FNAC
Introduction
Oncocytoma is a rare Salivary gland benign tumour that normally happens with inside the parotid gland [1] and few instances are stated in the submandibular gland, as scientific presentation of oncocytoma is similar to pleomorphic adenoma or warthin tumour due to that it’s also misdiagnosed [1, 2]. The term oncocytoma is derived from the resemblance of a tumour cell to apparently normal cell which has been termed oncocytes. DuPlay in 1875 was first one to reported this tumor and term was first used by Schaefer [3, 4]. Histologically neoplasm consists of monotonous sheets of oncocytes, and epithelial cells and is characterised by an intensely eosinophilic and granular cytoplasm [4]. This tumour basically affected 50–70 years of age with gender preference and the parotid gland is the most common site, other sites encompass the minor salivary glands, specifically the buccal mucosa and upper lip and seldom arise with inside the submandibular gland region [4, 5]. There aren’t any clear aetiologies for the development of submandibular oncocytomas, despite the fact that few instances are associated with radiation exposure [6]. Synonyms for this tumour encompass oncocytic adenoma, oxyphilic granular-cell adenoma, and oxyphilic adenoma [7].
The aim of this paper is to assess the clinicopathological functions, diagnostic standards and treatment of submandibular gland oncocytomas via a series of three case reports. All the case reported in Military Hospital, India in year 2017 to 2020.
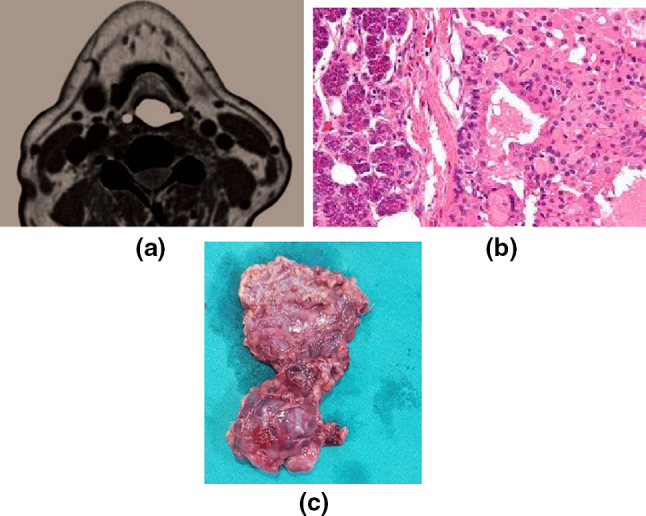
Case1: A 30-year-old patient pronounced with a major complaint of painless swelling at the right side of the face from the last 2 years that is developing constantly and achieving the present size of 10 × 6.5x3 cm in length (Fig. 1a). Clinically it is painless, non-tender, non-fluctuant, non-pulsatile swelling with regular margins, firm in consistency, does not adhere to the overlying skin or underlying structure and shows no signal of any facial palsy or numbness of the lower lip. Intraorally tongue is raised, restricted tongue movement, based on scientific findings the diagnosis of pleomorphic adenoma was made with differential analysis of warthins tumour or oncocytoma of the right submandibular gland. The NC and CECT of the face and neck show the presence of a huge heterogeneous lesion enhancing the right ground of the mouth and anteriorly extending into the right sublingual space, inferiorly displacement of the right anterior stomach of digastric muscle noted with well-defined lymph node measuring 10 mm in short axis diameter visible at right level II. CT carotid angiography was performed which indicates the facial artery is the primary arterial supply and no blood supply from the lingual artery. FNAC document indicates clusters of monotonous, polygonal, eosinophilic (oncocytic) epithelial cells with a low nuclear to cytoplasmic (N/C) ratio. The tumour cells had round nuclei and prominent nucleoli. There was no significant lymphoid population recognized, absence of mitosis or tumour necrosis (Fig. 1b). Cytologic functions were suggestive of submandibular oncocytoma. For definitive treatment and pathologic diagnosis Total submandibular gland excision was planned along with excision of level I and II lymph node along with maintenance of the vital structure (Fig. 1c).
Fig. 1.

Submandibular gland oncocytoma (a) well circumscribed mass 10 × 6.5x3 cm at right submandibular region; b Total submandibular gland excision and removal of level I and II lymph nodes (c) FNAC of the mass showing clusters of polygonal eosinophilic epithelial cells with low N/C ratio. d Histology of the submandibular oncocytoma reveals tumor is well circumscribed with a thin capsule and is composed of benign appearing oncocytes
Microscopically tumour indicates a well-circumscribed mass in multiple lobules. The lobules comprise cells in acini, nests and follicles, bordered by delicate fibrovascular septa. The cells are polygonal in shape, with spherical nuclei, granular eosinophilic cytoplasm, absence of mitosis. The tumour is bordered by subcutaneous tissue and reactive lymph nodes. Absence of any capsular breach. Features are consistent with an Oncocytoma (Fig. 1d). The patient was discharged on the fifth day after the surgical procedure. Follow-up was carried out for two years no recurrence was recognized. As far as our research goes nowhere in the literature this massive large submandibular gland oncocytoma measuring 10 × 6.5 × 3 cm in size is mentioned.
Case 2: A 63-year-old female presented with a history of pain and tender mass at the right submandibular region, no relevant past medical or personnel history. On physical exam, about 2 cm cm solid nodule was palpated in the right submandibular region. The CT imaging, confirmed a well-defined, homogeneously enhancing 1.8 × 1.5 cm mass in the inferior pole of the submandibular salivary gland (Fig. 2a). FNAC of the lesion has performed all features suggestive of submandibular oncocytoma. Right submandibular gland resection was performed. Microscopically, the tumour confirmed a well-circumscribed mass with a thin capsule The tumour was composed of monotonous epithelial cells with a low N/C ratio, considerable eosinophilic cytoplasm, and round nuclei with prominent nucleoli (Fig. 2b). The patient was discharged on the fifth day after the surgical procedure, and no recurrence was recognized after 1.5 years of follow-up.
Fig. 2.
Imaging and cytopathology of the submandibular oncocytoma. a CT scan showing a well-circumscribed mass at the right submandibular space (b) foci of oncocytes present at the tumor adjacent submandibular tissue, eosinophilic cytoplasm, and round nuclei with prominent nucleoli (c) Excised tumor mass
Case 3: A 52 years old female patient had long standing unilateral growth on left side of face size about 5 × 3 cm which is mild tender, non-fluctuant, non-pulsatile swelling with regular margins, firm in consistency, does not adhere to the overlying skin or underlying structures. FNAC of the lesion has performed all features suggestive of submandibular oncocytoma. Excision of tumour along with left submandibular gland resection was performed (Fig. 2c) and no recurrence was recognized after 2.5 years of follow-up.
Discussion
Oncocytoma is an unprecedented benign salivary gland tumour normally visible in the parotid gland (70%) followed by the minor salivary gland (26%) and rarely involves in the submandibular gland region [8, 9]. Submandibular oncocytoma is a rare benign tumour that arises primarily in the older age group among 50 to 75 age and women are more commonly involved [10]. It is usually present as a painless, enlarging mass generally three to five cm in size and appears as discrete, encapsulated that is sometimes nodular [11, 12]. Schaffer defined oncocytoma as “granular swollen cells” [12]. The father of oncocytes is Hamperl who referred to them as “onkocytes.” which in Greek means “increase in bulk,” swollen, enlarged [13]. Any tumour to be referred to as an oncocytoma, needs to be comprised solely of oncocytes which contain considerable eosinophilic cytoplasm [13, 14]. Oncocytoma because of its large size and growth pattern and the existence of malignant forms even though very rare is usually taken into consideration as neoplasm as opposed to nodular hyperplasia [15].
Histopathologically 03 distant types: ondocytosis, oncocytoma and oncocytic carcinoma. Oncocytoma has increased the mitochondria, large eosinophilic cytoplasm and distant cell membrane. The mitochondria can be angulated, semicircular, and ovoid with intently packed central sheaves of lamellar cristae. Electron dense glycogen deposits are located each within the cytoplasm in addition to within the mitochondrial substructure [16, 17].
The aetiology remains unknown because of its rare incidence; however, theory implicated the role of radiation in the pathogenesis of oncocytoma; however, no conclusive evidence exists [17] In parotid, region oncocytoma may be derived primarily from reserve cells in intercalated ducts as this is evident by immunohistochemistry, which indicates the presence of markers for human duct cells like CK7, CK8, and CK19. Submandibular gland oncocytosis may also have a comparable aetiology; however, no studies on this due to its rarity and research has mainly been targeted on parotid gland oncocytomas [17, 18].
Investigation executed is FNAC—features encompass uniform polygonal cytoplasm rich cell with eosinophilic and granulated cell, low N/C ratio, no mitotic changes and necrosis. Ultrasound isn’t always a completely effective investigation tool due to its inability to provide information about the encompassing structures. Technetium ninety-nine m pertechnetate scintigraphy is beneficial to assess gland mass. F18 FDG PET/CT assist in detecting the features of salivary gland malignancies due to the extent of invasion and spread of the tumour [18, 19]. CT has been established as the first-line image modality in the assessment of major salivary gland tumors. The common CT finding of the oncocytomas described in the literature is a well-defined mass showing homogeneous enhancement.
The differential diagnosis of oncocytoma consists of pleomorphic adenoma, warthins tumour, which may be distinguished on basis of histopathology characteristics, oncocytoma has the typical presence of monomorphic oncocytes without mitosis and necrosis with thin capsule while pleomorphic adenoma has thick capsule wall [20, 21]. Similarly, warthins tumor to be ruled out histologically by lack of lymphatic population as compared to oncocytoma [22]. As in line with the literature, Submandibular gland oncocytoma has a rare malignant capacity and the criteria for malignancy include capsular invasion, destructive growth, necrosis, vascular or neural invasion, lymph node and distant metastases and increased mitotic activity [23, 24]. None of our cases verified any of those features, and long term follow-up demonstrated no recurrences or metastases (Table 1).
Table 1.
Summary of clinical characteristics of submandibular oncocytoma
| S.no | Age/Sex | Sign /symptoms | Size | Laterality | Mode of diagnosis | Treatment | Follow up |
|---|---|---|---|---|---|---|---|
| 1 | 30/M | Painless enlarge mass | 10 × 6.5x3 cm | Unilateral right side | FNAC | Total Gland Excision and removal of level I and II lymph nodes | 3.5 years, no recurrence, alive |
| 2 | 63/F | Tender mass | 1.8 × 1.5 cm | Unilateral right side | FNAC | Excision of gland | 2 years, no recurrence, alive |
| 3 | 52/F | Long standing mass with no tenderness | 5 × 3 cm | Unilateral left side | FNAC | Excision of gland | 2.5 years, no recurrence, alive |
Presented three cases with female to male ratio 2:1, Size of tumor ranged from 1.8 cm to 10 cm, 2 cases have painless swelling and one involved tender mass. On follow up no evidence of any recurrence
The first line of treatment is surgical excision, the extent of excision is dictated by clinical and radiological examination [25, 26]. Submandibular oncocytoma has extremely low malignant potential Alternative treatment methods like chemotherapy and radiotherapy aren’t yet pronounced because of their uncommon origin. The possibilities of recurrence are due to incomplete excision and multinodular cases [27, 28].
Conclusion
We present a case series of submandibular oncocytoma, which is a rare benign tumor of salivary gland. A combined clinical, radiologic, and pathologic assessment of a patient who presents with a submandibular mass is essential in establishing an accurate diagnosis. Distinctive features of oncocytomas are best seen on preoperative FNAC and histology, which includes the presence of monotonous oncocytes with low N/C ratio and lack of mitoses and necrosis. The malignant potential of a benign oncocytoma is extremely low. Treatment is excision of the tumor along with total submandibular gland resection depend on the extent of tumor with appropriate follow-up as required.
Funding
The author declares no funding.
Declarations
Conflict of interest
There are no conflicts of interest.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, Govt/ Militaryhospital, India.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Beltaos E, Maurer WJ. Oncocytoma of the submaxillary salivary gland: report of a case. Arch Otolaryngol. 1966;84(2):193–197. doi: 10.1001/archotol.1966.00760030195014. [DOI] [PubMed] [Google Scholar]
- 2.Nakada M, Nishizaki K, Akagi H, Masuda Y, Yoshino T. Oncocytic carcinoma of the submandibular gland: a case report and literature review. J Oral Pathol Med. 1998;27(5):225–228. doi: 10.1111/j.1600-0714.1998.tb01946.x. [DOI] [PubMed] [Google Scholar]
- 3.Thompson LD, Wenig BM, Ellis GL. Oncocytomas of the submandibular gland: a series of 22 cases and a review of the literature. Cancer. 1996;78(11):2281–2287. doi: 10.1002/(SICI)1097-0142(19961201)78:11<2281::AID-CNCR3>3.0.CO;2-Q. [DOI] [PubMed] [Google Scholar]
- 4.Lee T-H, Lin Y-S, Lee W-Y, Wu T-C, Chang S-L. Malignant transformation of a benign oncocytoma of the submandibular gland: A case report. Kaohsiung J Med Sci. 2010;26(6):327–332. doi: 10.1016/S1607-551X(10)70047-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fernandez JR, Micas MM, Tello FJM, et al. Metastatic benign pleomorphic adenoma: report of a case and review of the literature. Med Oral Patol Oral Y Cir Bucal. 2008;13(3):193–196. [PubMed] [Google Scholar]
- 6.Knight J, Ratnasingham K. Metastasising pleomorphic adenoma: systematic review. Int J Surg. 2015;19:137–145. doi: 10.1016/j.ijsu.2015.04.084. [DOI] [PubMed] [Google Scholar]
- 7.Allevi F, Biglioli F (2014) Squamous carcinoma arising in a parotid Warthin’s tumour. BMJ Case Rep [DOI] [PMC free article] [PubMed]
- 8.Brandwein MS, Huvos AG. Oncocytic tumors of major salivary glands: a study of 68 cases with follow-up of 44 patients. Am J Surg Pathol. 1991;15(6):514–528. doi: 10.1097/00000478-199106000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Eneroth CM. Oncocytoma of major salivary glands. J Laryngol Otol. 1965;79:1064–1072. doi: 10.1017/S0022215100064811. [DOI] [PubMed] [Google Scholar]
- 10.Dibble PA, Sanford DM. Submaxillary oncocytoma: oxyphil-cell adenoma. Arch Otolaryngol Head Neck Surg. 1961;74(3):299–301. doi: 10.1001/archotol.1961.00740030306011. [DOI] [PubMed] [Google Scholar]
- 11.Mukai H, Sugihara K, Dohhara Y, Yamada K, Yamashita S. Malignant oncocytoma of the submandibular gland: report of a case. Jpn J Oral Maxillofac Surg. 1978;24:111–116. doi: 10.5794/jjoms.24.111. [DOI] [Google Scholar]
- 12.Goode RK, Corio RL. Oncocytic adenocarcinoma of salivary glands. Oral Surg Oral Medi Oral Pathol. 1988;65(1):61–66. doi: 10.1016/0030-4220(88)90193-4. [DOI] [PubMed] [Google Scholar]
- 13.Ziegler M, Maibach E-A, Ussmuller J. Malignant oncocytoma of the submandibular gland. LaryngoRhino Otol. 1992;71(8):423–425. doi: 10.1055/s-2007-997327. [DOI] [PubMed] [Google Scholar]
- 14.Sakthikumar KRV, Mohanty S, Dineshkumar K. Solitary oncocytoma of the submandibular salivary gland in an adolescent female: a case report. Indian J Otolaryngol Head Neck Surg. 2007;59:171–173. doi: 10.1007/s12070-007-0051-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Subramaniam RM, Durnick DK, Peller PJ. F-18 FDG PET/CT imaging of submandibular gland oncocytoma. Clin Nucl Med. 2008;33(7):472–474. doi: 10.1097/RLU.0b013e31817792b6. [DOI] [PubMed] [Google Scholar]
- 16.Dastaran M, Chandu A. Bilateral submandibular gland oncocytoma in a patient with multiple endocrine neoplasia 2B syndrome and neurofibromatosis type 1: An unusual case. Int J Oral Maxillofac Surg. 2011;40(7):764–767. doi: 10.1016/j.ijom.2011.02.017. [DOI] [PubMed] [Google Scholar]
- 17.Ziglinas P, Arnold A, Arnold M. Primary tumors of the submandibular glands: a retrospective study based on 41 cases. Oral Oncol. 2010;46:287–291. doi: 10.1016/j.oraloncology.2010.01.011. [DOI] [PubMed] [Google Scholar]
- 18.Volk TL, Scarpelli DG. Mictochondrial giagantism in the adrenal cortex following hypophysectomy. Lab Invest. 1966;15:707–715. [PubMed] [Google Scholar]
- 19.Ramakrishna B, Perakath R, Chandi SM. Malingant "multinodular" oncocytoma of parotid gland: a case report and literature review. Indian J Cancer. 1992;29:230–233. [PubMed] [Google Scholar]
- 20.Ackerman LV. Oncocytoma of the parotid gland. ArchPathol Lab Med. 1943;36:508–511. [Google Scholar]
- 21.Rauer WH, Bauer JD. Classification of glandular tumors of salivary glands: study of 143 cases. Arch Parhol Lah Med. 1953;55:328–346. [PubMed] [Google Scholar]
- 22.Taxy JB. Necrotizing squamous/mucinous metaplasia in oncocytic salivary gland tumors: a potential diagnostic problem. Am J Clin Parhol. 1992;97:40–45. doi: 10.1093/ajcp/97.1.40. [DOI] [PubMed] [Google Scholar]
- 23.Palmer TJ, Gleeson MJ, Eveson JW, Cawson RA. Oncocytic adenomas and oncocytic hyperplasia of salivary glands: a clinicopathological study of 26 cases. Histopathology. 1990;16(5):487–493. doi: 10.1111/j.1365-2559.1990.tb01549.x. [DOI] [PubMed] [Google Scholar]
- 24.Chan JKC, Tang SK, Tsang WYW, Lee KC, Batsakis JG. Histologic changes induced by fine needle aspiration. Adv Anat Puthol. 1996;3:71–90. doi: 10.1097/00125480-199603000-00001. [DOI] [Google Scholar]
- 25.Goode RK, Corio RL. Oncocytic adenocarcinoma of salivary glands. Oral Surg Oral Med Oral Pathol. 1988;65:61–66. doi: 10.1016/0030-4220(88)90193-4. [DOI] [PubMed] [Google Scholar]
- 26.Brandwein MS, Huvos AG. Oncocytic tumors of the major salivary glands: a study of 68 cases with follow-up of 44 patients. Am J Surg Parhol. 1991;15:514–528. doi: 10.1097/00000478-199106000-00002. [DOI] [PubMed] [Google Scholar]
- 27.Muramatsu T, Hashimoto S, Lee M-W, et al. Oncocytic carcinoma arising in submandibular gland with immunohistochemical observations and review of the literature. Oral Oncol. 2003;39(2):199–203. doi: 10.1016/S1368-8375(02)00031-3. [DOI] [PubMed] [Google Scholar]
- 28.Lee W-Y, Chang S-L. Fine needle aspiration cytology of oncocytic carcinoma of the submandibular gland with pre-existing oncocytoma: a case report. Cytopathology. 2010;21(5):339–341. doi: 10.1111/j.1365-2303.2009.00720.x. [DOI] [PubMed] [Google Scholar]