

Abstract
Aim
The aim of the study was to compare and evaluate the retention and antibacterial efficacy of posterior high strength glass ionomer cement and glass hybrid bulk-fill alkasite restorative material as a conservative adhesive restoration in children with mixed dentition.
Materials and methods
A total of 60 children of age 6–12 years with mixed dentition were selected and divided into group I (control group n = 30): posterior high strength glass ionomer cement and group II (experimental group n = 30): glass hybrid bulk-fill alkasite restorative material. Restorative treatment was carried out using these two materials. Retention of the material and salivary Streptococcus mutans and Lactobacillus species count was estimated at baseline, 1, 3, and 6 months. The collected data were statistically analyzed using International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS) software (version 20.0 Chicago, Illinois, USA)
Results
About 100% retention of glass hybrid bulk-fill alkasite restorative material, and 90% retention of posterior high strength glass ionomer cement was observed according to United State Public Health Criteria. The * signifies statistically significant results, i.e. p < 0.0001 reduction in salivary S. mutans colony count and Lactobacillus species colony count was seen in both groups at different time intervals.
Conclusion
Both the materials showed good antibacterial properties, but glass hybrid bulk-fill alkasite restorative showed better retention, that is, 100% when compared to posterior high strength glass ionomer cement, which showed 90% retention at the end of 6 months follow-up.
How to cite this article
Soneta SP, Hugar SM, Hallikerimath S, et al. An In Vivo Evaluation of Retention and Antibacterial Efficacy of Posterior High Strength Glass Ionomer Cement and Glass Hybrid Bulk-fill Alkasite Restorative Material as Conservative Adhesive Restoration in Children with Mixed Dentition: A Comparative Study. Int J Clin Pediatr Dent 2022;15(5):529-534.
Keywords: Antimicrobial, Children, Conservative adhesive restoration, Glass hybrid bulk-fill restorative material, Posterior high strength glass ionomer cement
Introduction
Oral health is an integral part of overall general health, which in turn is essential for the well-being of mankind. With globalization on the rise and in spite of foremost progress and advances in preventive dentistry, there is an ever-increasing rate of caries seen in children. Dental caries is the most common oral disease and is still a major public health burden in developing countries, affecting nearly 60–90% of children.1,2
The paradigm around the quintessential treatment and management of carious lesions has been altering. Conventional restorative approaches, with the school of thought on the complete removal of carious tooth surface followed by placement of a restoration, have been substituted by more biological and less invasive approaches, which focus on biofilm control and its disruption to arrest caries.3
The concept of conservative adhesive restoration has gained a lot of popularity in the recent past, along with its emphasis on the conservation of the tooth structure followed by the placement of adhesive restorative material. For this purpose, conventional high strength posterior glass ionomer cement is the basic ideal filling material of choice for conservative adhesive restoration in children due to its advantages of being esthetically acceptable, adhesive to the tooth, and release of fluoride. It is also simple, economical, does not require complicated dental equipment, and can be used in small conservative restorations. However, glass ionomer cements have certain disadvantages like poor mechanical properties, which are unsuitable for large posterior restorations in stress-bearing areas since their compressive strength is less compared to amalgam.4
Recently, a new basic tooth-colored filling material, glass hybrid bulk-fill restorative material—Cention N has been introduced with added advantages over amalgam, glass ionomer cement, and composite. The “alkasite” Cention N redefines the basic filling material with combined bulk placement, ion release, durability in a dual-curing, radiopaque, and capable of releasing acid-neutralizing ions. It's esthetic and satisfies the demands of both the dentists and the patients. Cention N thus can be a good alternative for restoring deciduous and permanent teeth in class I, II, and V tooth preparations.5
When the literature search was carried out, there were no studies carried out in the Indian scenario or worldwide to evaluate and compare the retention and antimicrobial efficacy of posterior high strength glass ionomer cement and glass hybrid bulk-fills alkasite restorative material as conservative adhesive restoration in children with mixed dentition. So, an attempt was made to carry out this research to evaluate and compare retention, and antimicrobial efficacy of posterior high strength glass ionomer cement and glass hybrid bulk-fill alkasite restorative material as conservative adhesive restoration in children with mixed dentition.
Materials and Methods
The study was conducted in the Department of Pediatric and Preventive Dentistry. Ethical clearance for the study was obtained from the Institutional Review Board. The sample size was derived based on the previous study with a confidence level of 85%, a probability of 0.05, and 15% attrition.6 A total of 60 sample sizes were selected. Children with mixed dentition with 1–2 decayed maxillary or mandibular first permanent molars with occlusal caries (class I) involving enamel or dentin (type I or type II conservative adhesive restoration) were included in the study. Children exhibiting proximal carious lesions, special children, and if the patient was on any medication were all excluded from our study. The selected samples were divided into two groups.
Group I (control group n = 30): Posterior high strength glass ionomer cement (GC Gold label H.S. posterior extra)
Group II (experimental group n = 30): Glass hybrid bulk-fill alkasite restorative material: (Ivoclar Vivadent, Leuven).
Written informed consent was obtained from the parent/guardian, and assent was taken from the child before the start of the procedure. Thereafter, case history followed by intraoral periapical radiographs was recorded.7 The saliva was collected for microbiological evaluation between 9 and 11 am8 to assess the baseline colony count of S. mutans and Lactobacillus species by using the suction method with sterile disposable syringes.9 The saliva was collected on four occasions to assess microbiological colony count at baseline, 1, 3, and 6 months (Figs 1 and 2).
Figs 1A to D.

Photograph showing the growth and colonization of S. mutans at different time intervals with glass hybrid bulk-fill alkasite restoration, (A) baseline; (B) 1 month; (C) 3 months; (D) 6 months
Figs 2A to D.

Photograph showing the growth and colonization of Lactobacillus species at different time intervals with posterior high strength glass ionomer cement restoration, (A) baseline; (B) 1 month; (C) 3 months; (D) 6 months
Before the start of the procedure, oral prophylaxis was performed, and all procedures, such as saliva collection, restoration, and postoperative assessment, were carried out by a single investigator to avoid any bias. The teeth selected for the study were isolated using a rubber dam followed by pumice prophylaxis on the sample tooth. The class I tooth preparation used high-speed round diamond points but followed the principle of minimally invasive dentistry to receive the restoration (posterior high strength glass ionomer cement/glass hybrid bulk-fill alkasite restorative material) (Figs 3 and 4).
Figs 3A to D.

Photograph showing procedure of restoration in posterior high strength glass ionomer cement (group I): (A) preoperative IOPA; (B) preoperative photograph; (C) cavity prepared; (D) postoperative photograph
Figs 4A to D.

Procedure of restoration in glass hybrid bulk-fill alkasite restorative material (group II): (A) preoperative IOPA; (B) preoperative photograph; (C) cavity prepared; (D) postoperative photograph
The postoperative evaluation of all the restorations was done and recorded in a master chart. Patients were given postoperative instructions not to drink or take water for 30 minutes and a soft diet for the next 24 hours. Patients were followed for review of retention for the restoration at 1, 3, and 6 months. Restorations were evaluated for checking retention of the restoration as per the United States Public Health Service (USPHS) Ryge criteria.10 The collected data were statistically analyzed using IBM SPSS software (version 20.0 Chicago, Illinois, USA).
Results
Statistical evaluation for the mean S. mutans and Lactobacillus species colony-forming units (CFU) among the two groups was analyzed using the dependent t-test was carried out, and the retention of the material was evaluated by using USPHS Ryge criteria, and percentile was calculated.
Retention
A total of 60 restorations were evaluated at 1, 3, and 6 months of recall. Both the materials showed similar retentiveness, that is, α restoration is intact and fully retained at 1 and 3 months, however at 6 months follow-up, 10% of posterior high strength glass ionomer cement restorations showed Bravo (B), that is, restoration is partially retained with some portion of the restoration still intact (Table 1 and Fig. 5).
Table 1.
Comparison of retention of the restorative material in posterior high strength glass ionomer cement (group I) and glass hybrid bulk-fill alkasite restoration (group II)
| Follow-up visit | Material used | Total | Retention | |||||
|---|---|---|---|---|---|---|---|---|
| α | (%) | B | (%) | Charlie | (%) | |||
| 1 month | Group I | 30 | 30 | 100 | – | – | – | – |
| Group II | 30 | 30 | 100 | – | – | – | – | |
| 3 months | Group I | 30 | 30 | 100 | – | – | – | – |
| Group II | 30 | 30 | 100 | – | – | – | – | |
| 6 months | Group I | 30 | 27 | 90 | 3 | 10 | – | – |
| Group II | 30 | 30 | 100 | – | – | – | – | |
Fig. 5.
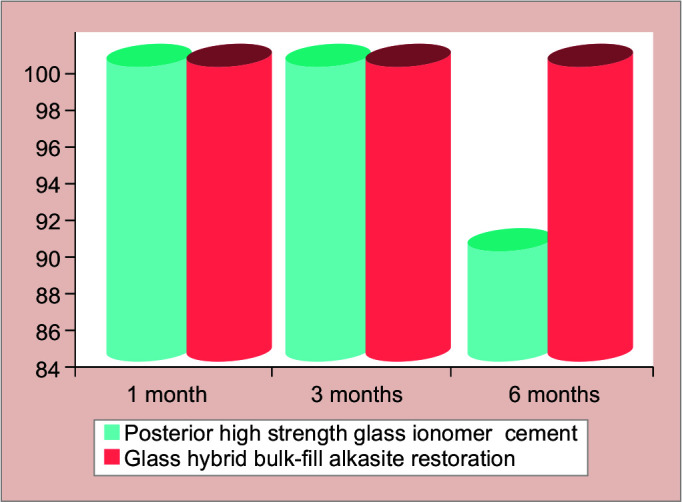
Intergroup comparison between two groups namely posterior high strength glass ionomer cement (group I) and glass hybrid bulk-fill alkasite restoration (group II) with respect to retention of the restorative material
Microbiological Evaluation
In posterior high strength glass ionomer cement (group I), the mean value of S. mutans colony count (×105 CFU/mL of saliva) was 3.53 ± 0.11 at baseline, which was reduced to 3.09 ± 0.28 (p = 0.0001*) at 1 month, it further reduced to 2.45 ± 0.27 (p = 0.0001*) at 3 months, and 2.51 ± 0.75 (p = 0.0001*) at 6 months this indicates a statistically highly significant reduction in S. mutans level. Thus, when compared to baseline, the reduction of S. mutans seen at 1-, 3-, and 6-months follow-up was 12.46, 30.67, and 29.05%, respectively (Table 2 and Fig. 6).
Table 2.
Difference between the mean S. mutans CFU/mL of saliva (×105 CFU/mL) in posterior high strength glass ionomer cement (group I) and glass hybrid bulk-fill alkasite restoration (group II) at baseline, 1-, 3-, and 6-month time points using dependent t-test
| Groups | Time points | Mean | Standard deviation | Mean difference | Standard deviation difference | % of change | t-value | p-value |
|---|---|---|---|---|---|---|---|---|
| Group I: Posterior high strength glass ionomer cement | Baseline | 3.53 | 0.11 | |||||
| 1 month | 3.09 | 0.28 | 0.44 | 0.29 | 12.46 | 8.2892 | 0.0001* | |
| Baseline | 3.53 | 0.11 | ||||||
| 3 months | 2.45 | 0.27 | 1.08 | 0.30 | 30.67 | 20.0990 | 0.0001* | |
| Baseline | 3.53 | 0.11 | ||||||
| 6 months | 2.51 | 0.75 | 1.03 | 0.76 | 29.05 | 7.3964 | 0.0001* | |
| Group II: Glass hybrid bulk-fill alkasite restoration | Baseline | 3.62 | 0.09 | |||||
| 1 month | 3.01 | 0.33 | 0.61 | 0.35 | 16.91 | 9.5080 | 0.0001* | |
| Baseline | 3.62 | 0.09 | ||||||
| 3 months | 1.91 | 0.78 | 1.71 | 0.76 | 47.27 | 12.3993 | 0.0001* | |
| Baseline | 3.62 | 0.09 | ||||||
| 6 months | 2.41 | 0.85 | 1.21 | 0.84 | 33.39 | 7.8663 | 0.0001* |
*Denotes statistically significant p < 0.05
Fig. 6.
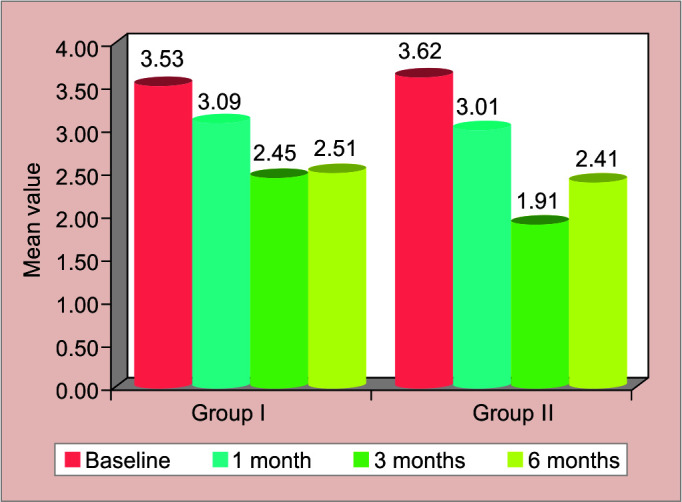
Difference between the mean S. mutans CFU/mL of saliva (×105 CFU/mL) in posterior high strength glass ionomer cement (group I) and glass hybrid bulk-fill alkasite restoration (group II) at baseline, 1, 3, and 6-month time points
In glass hybrid bulk-fill alkasite restoration material (group II), the mean value of S. mutans colony count (×105 CFU/mL of saliva) was 3.62 ± 0.09 at baseline, which was reduced to 3.01 ± 0.33 (p = 0.0001*) at 1 month, it further reduced to 1.91 ± 0.78 (p = 0.0001*) at 3 months, and at 2.41 ± 0.85 (p = 0.0001*) at 6 months this indicates a statistically highly significant reduction in S. mutans level. Thus, when compared to baseline, the reduction of S. mutans seen at 1, 3, and 6 months, follow-up was 16.91, 47.27, and 33.39%, respectively (Table 2 and Fig. 6).
In posterior high strength glass ionomer cement (group I), the mean value of Lactobacillus species colony count (×105 CFU/mL of saliva) was 3.42 ± 0.33 at baseline, which was reduced to 2.87 ± 0.17 (p = 0.0001*) at 1 month, it further declined to 2.36 ± 0.20 (p = 0.0001*) at 3 months, and 2.63 ± 0.32 (p = 0.0001*) at 6 months; this indicates a statistically highly significant reduction in Lactobacillus species level. Thus, when compared to baseline, the reduction of Lactobacillus species seen at 1-, 3-, and 6-months follow-up was 16.15, 31.02, and 23.01%, respectively (Table 3 and Fig. 7).
Table 3.
Difference between the mean Lactobacillus species CFU/mL of saliva (×105 CFU/mL) in posterior high strength glass ionomer cement (group I) and glass hybrid bulk-fill alkasite restoration (group II) at baseline, 1, 3, and 6-month time points using dependent t-test
| Groups | Time points | Mean | Standard deviation | Mean difference | Standard deviation difference | % of change | t-value | p-value |
|---|---|---|---|---|---|---|---|---|
| Group I: Posterior high strength glass ionomer cement | Baseline | 3.42 | 0.33 | |||||
| 1 month | 2.87 | 0.17 | 0.55 | 0.36 | 16.15 | 8.3410 | 0.0001* | |
| Baseline | 3.42 | 0.33 | ||||||
| 3 months | 2.36 | 0.20 | 1.06 | 0.41 | 31.02 | 14.3091 | 0.0001* | |
| Baseline | 3.42 | 0.33 | ||||||
| 6 months | 2.63 | 0.32 | 0.79 | 0.53 | 23.01 | 8.1670 | 0.0001* | |
| Group II: Glass hybrid bulk-fill alkasite restoration | Baseline | 3.59 | 0.08 | |||||
| 1 month | 2.86 | 0.18 | 0.72 | 0.17 | 20.13 | 22.7878 | 0.0001* | |
| Baseline | 3.59 | 0.08 | ||||||
| 3 months | 1.80 | 0.74 | 1.79 | 0.73 | 49.79 | 13.3258 | 0.0001* | |
| Baseline | 3.59 | 0.08 | ||||||
| 6 months | 1.95 | 0.98 | 1.64 | 0.97 | 45.61 | 9.2008 | 0.0001* |
*Denotes statistically significant p < 0.05
Fig. 7.

Difference between the mean Lactobacillus species CFU/mL of saliva (×105 CFU/mL) in posterior high strength glass ionomer cement (group I) and glass hybrid bulk-fill alkasite restoration (group II) at baseline, 1-, 3-, and 6-month time points
In glass hybrid bulk-fill alkasite restoration material (group II) mean value of Lactobacillus species colony count (×105 CFU/mL of saliva) was 3.59 ± 0.08 at baseline, which was reduced to 2.86 ± 0.18 (p = 0.0001*) at 1 month, it further reduced to 1.80 ± 0.74 (p = 0.0001*) at 3 months, and 1.95 ± 0.98 (p = 0.0001*) at 6 months this indicates statistically highly significant reduction Lactobacillus species level. Thus, when compared to baseline, the reduction of Lactobacillus species seen at 1, 3, and 6 months, follow-up was 20.13, 49.79, and 45.61%, respectively (Table 3 and Fig. 7).
Hence an inference from the above results can be drawn that glass hybrid bulk-fill alkasite restoration material (group II) has got superior retention and antibacterial property as compared to posterior high strength glass ionomer cement (group I).
Discussion
The incidence of dental caries has seen a rise with the increase in globalization. If there is a delay in the treatment of dental caries, it may not only affect the mastication but also may have deleterious psychological effects due to altered speech and smile of the child.
Treatment for dental caries implies the modern concept of minimal invasion. This technique has evolved from an increased understanding of the caries process and the development of adhesive and biomimetic restorative materials. The radical ideology of G.V. Black's “extension for prevention” has changed to Simonsen's “prevention of extension.”11
The present study compared the retention, and antibacterial efficacy of posterior high strength glass ionomer cement and glass hybrid bulk-fill alkasite restorative material for retention and its antibacterial property using a microbiological method under a randomized clinical trial setting.
In our study, the first permanent molar was used for restoration because this being the first permanent tooth to erupt in the oral cavity, is most commonly affected with dental caries. From a functional and developmental point of view, they have a key role in balanced occlusion. Loss of first permanent molars because of dental caries negatively affects both arches having adverse effects on occlusion. Also, early extraction of these teeth results in tilting of neighboring teeth to hollow spaces, supra-eruption of the teeth in the opposite arch, unilateral chewing, shift in the midline, and dental malocclusion. Furthermore, the dexterity of children at the age of eruption of first permanent molars is poor, and it is this tooth that is most commonly misunderstood as a primary tooth as it's the first permanent tooth to erupt. Hence to maintain standardization, only the first permanent molars have been selected.12
Children with mixed dentition between 6 and 12 years were included in the study with a mean age of 10.75 ± 1.14 years because, at this age, they are highly susceptible to dental caries and are undergoing multiple permanent tooth eruptions also, it has been noted that there is a high occurrence of pseudo pockets which in turn houses plaque and other bacterias. Saliva and plaque can be used for the estimation of S. mutans and Lactobacillus species count. Due to the ease of sampling and processing, unstimulated saliva was used in the study, which was collected from the floor of the mouth using a sterile disposable syringe to avoid any contamination.8,9
The choice of material for recovery in the treatment of caries among children is an extremely important task for a dentist as there is a huge arsenal of dental materials for restoration. Nevertheless, it is often difficult for a dentist to choose the best material for a specific clinical case.13 In our study, we have chosen posterior high strength glass ionomer cement, and glass hybrid bulk-fill alkasite restorative material due to its esthetic nature and adhesive property along with improved physical and mechanical properties.
The literature has shown fluoride ion release capacity, demineralizing inhibition potential, resistance to microleakage compressive strength, and tensile strength of glass hybrid bulk-fill alkasite restorative material, but it lacked clinical study that measured retention or antibacterial property.14–18 Hence in our study, we measured the clinical success based on the retention and antibacterial effectiveness of both materials. According to Ngo and Opsahl-Vital, posterior high strength glass ionomer cements have shown promising results in relation to retention.19 But our study has shown that glass hybrid bulk-fill alkasite restorative material showed better retentive properties than posterior high strength glass ionomer cements.
There have been studies in the past that have shown posterior high strength glass ionomer cement to have good antibacterial properties.20,21 In our study, when the antibacterial effectiveness was compared in relation to S. mutans and Lactobacillus species, it was seen that glass hybrid bulk-fill alkasite restorative material showed a better reduction in the microbial load from baseline to 1, 3, and 6 months when compared to posterior high strength glass ionomer cement.
Our study showed that glass hybrid bulk-fill alkasite restorative material had better antibacterial and retentive properties when compared to posterior high strength glass ionomer cements. However, a study with larger sample size and longer follow-up should be carried out in future for a better understanding of the results.
It also would be quite interesting to know and analyzing the relationship between S. mutans and Lactobacillus species and the success of different other minimal intervention restorative techniques.
Conclusion
Posterior high strength glass ionomer cements and glass hybrid bulk-fill alkasite restorative material showed good retention and antibacterial property, but the latter showed the better result. Hence, our study concludes that glass hybrid bulk-fill alkasite restorative material can be used as an adjunct to posterior high strength glass ionomer cements.
Clinical Significance
A wide variety of restorative materials are available for conservative adhesive restoration techniques; our study will serve as a clinical guide for optimal use and ease of selection of restorative material for conservative adhesive restoration in children with mixed dentition.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Petersen PE, Bourgeois D, Ogawa H, et al. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661–669. doi: 10.1590/S0042-96862005000900011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hugar SM, Kohli D, Badakar CM, et al. Comparative assessment of conventional composites and coloured compomers in permanent molars of children with mixed dentition: a pilot study. J Clin Diag Res. 2017;11(6):ZC69–ZC72. doi: 10.7860/JCDR/2017/25596.10083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Qin M, Liu HS. Clinical evaluation of a flowable resin composite and flowable compomer for preventive resin restorations. Oper Dent. 2005;30(5):580–587. [PubMed] [Google Scholar]
- 4.Cho SY, Cheng AC. A review of glass ionomer restorations in the primary dentition. J Can Dent Assoc. 1999;65(9):491–495. [PubMed] [Google Scholar]
- 5.Ivoclar Vivadent. Cention N (Scientific Documentation). Australia: Ivoclar Vivadent.; 2016. [Google Scholar]
- 6.Viechtbauer W, Smits L, Kotz D, et al. A simple formula for the calculation of sample size in pilot studies. J Clin Epidemiol. 2015;68(11):1375–1379. doi: 10.1016/j.jclinepi.2015.04.014. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. Oral Health Surveys: Basic Methods. 4th ed. Geneva: World Heatlh organization; 1997. [Google Scholar]
- 8.Navazesh M. Methods for collecting saliva. Ann N Y Acad Sci. 1993;694:72–77. doi: 10.1111/j.1749-6632.1993.tb18343.x. [DOI] [PubMed] [Google Scholar]
- 9.Dawes C. Circadian rhythms in human salivary flow rate and composition. J Physiol. 1972;220(3):529–545. doi: 10.1113/jphysiol.1972.sp009721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bayne SC, Schmalz G. Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin Oral Investig. 2005;9(4):209–214. doi: 10.1007/s00784-005-0017-0. [DOI] [PubMed] [Google Scholar]
- 11.MM J, NK B, A P. Minimal intervention dentistry–a new frontier in clinical dentistry. J Clin Diag Res. 2014;8(7):ZE04–ZE08. doi: 10.7860/JCDR/2014/9128.4583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ebrahimi M, Ajami Molook BA, Shirazi Sarraf AR, et al. Dental treatment needs of permanent first molars in Mashhad schoolchildren. J Dent Res Dent Clin Dent Prospec. 2010;4(2):52–55. doi: 10.5681/joddd.2010.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yeolekar TS, Chowdhary NR, Mukunda KS, et al. Evaluation of microleakage and marginal ridge fracture resistance of primary molars restored with three restorative materials: a comparative in vitro study. Int J Clin Pediatr Dent. 2015;8(2):108–113. doi: 10.5005/jp-journals-10005-1294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gupta N, Jaiswal S, Nikhil V, et al. Comparison of fluoride ion release and alkalizing potential of a new bulk-fill alkasite. J Conserv Dent. 2019;22(3):296–299. doi: 10.4103/JCD.JCD_74_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kaur M, Mann NS, Jhamb A, et al. A comparative evaluation of compressive strength of Cention N with glass ionomer cement: an in-vitro study. Int J Appl Dent Sci. 2019;5(1):5–9. [Google Scholar]
- 16.Iftikhar N, Devashish Srivastava B, et al. A comparative evaluation of mechanical properties of four different restorative materials: an in vitro study. Int J Clin Pediatr Dent. 2019;12(1):47–49. doi: 10.5005/jp-journals-10005-1592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mishra A, Singh G, Singh SK, et al. Comparative evaluation of mechanical properties of Cention N with conventionally used restorative materials—an in vitro study. Int J Prosth and Rest Dent. 2018;8(4):120–124. doi: 10.5005/jp-journals-10019-1219. [DOI] [Google Scholar]
- 18.Meshram P, Meshram V, Palve D, et al. Comparative evaluation of microleakage around class V cavities restored with alkasite restorative material with and without bonding agent and flowable composite resin: an in vitro study. Ind J Dent Res. 2019;30(3):403–407. doi: 10.4103/ijdr.IJDR_767_17. [DOI] [PubMed] [Google Scholar]
- 19.Ngo H, Opsahl-Vital S. Minimal intervention dentistry II: part 7. Minimal intervention in cariology: the role of glass-ionomer cements in the preservation of tooth structures against caries. Br Dent J. 2014;216(10):561–565. doi: 10.1038/sj.bdj.2014.398. [DOI] [PubMed] [Google Scholar]
- 20.Loyola-Rodriguez JP, Garcia-Godoy F, Lindquist R. Growth inhibition of glass ionomer cements on mutants Streptococci. Pediatr Dent. 1994;16(5):346–349. [PubMed] [Google Scholar]
- 21.Khere CH, Hiremath H, Sandesh N, et al. Evaluation of antibacterial activity of three different glass ionomer cements on Streptococcus mutans: an in-vitro antimicrobial study. Med Pharm Rep. 2019;92(3):288–293. doi: 10.15386/mpr-1113. [DOI] [PMC free article] [PubMed] [Google Scholar]