

Abstract
Confluent and reticulated papillomatosis (CARP) is a rare disorder mostly seen in young adults. It is characterized by persistent dull-brown, centrally confluent, peripherally reticulate macules and papules, which coalesce to form patches and plaques on the upper trunk and neck. It is commonly confused with pityriasis versicolor and acanthosis nigricans (AN). We report the case of a 15-year-old male with multiple pigmented confluent and reticulated patches and plaques on the neck, trunk, and chin for 3 years, which was successfully treated with oral minocycline, resulting in complete resolution of lesions within 2 weeks. The morphology of CARP resembles that of various other dermatological conditions such as AN and pityriasis versicolor, and, as a result, it is frequently misdiagnosed and mistreated, leading to social embarrassment for the patient. Therefore, it is prudent for dermatologists to carry out comprehensive clinical and histopathological assessments to facilitate prompt diagnosis and management of this condition.
Keywords: CARP, confluent and reticulated papillomatosis, pityriasis versicolor, acanthosis nigricans, minocycline
Introduction
Confluent and reticulated papillomatosis (CARP), which is also known as Gougerot-Carteaud syndrome, is an uncommon disorder of defective epidermal keratinization characterized by hyperkeratotic papules that may coalesce into confluent and reticulated plaques. It predominantly affects adolescents [1]. The etiology is unclear, but an aberrant host reaction to commensal organisms such as Malassezia furfur or Dietzia papillomatosis has been proposed [2]. CARP may masquerade as acanthosis nigricans (AN) or tinea versicolor, with few cases even showing an association with the latter [3]. We came across a case of a 15-year-old adolescent male with multiple asymptomatic pigmented lesions on the neck, upper back, chest, and chin for 3 years, which was misdiagnosed as pityriasis versicolor and AN. Treatment with oral minocycline led to successful resolution of lesions within 14 days.
Case History
A 15-year-old male presented at our outpatient department with a history of multiple, flat, hyperpigmented lesions on the neck, upper back, upper chest, and chin since the past 3 years. Lesions started on the nape of the neck, following a progressive course to involve the whole neck and upper back area. The patient complained of a rapid increase in the appearance of new lesions on the upper chest, presternal area, and chin area since the past 2 months. The lesions were asymptomatic. The patient had taken multiple unknown oral and topical medications with no effect on the size and number of lesions. There was no family history of similar lesions. His BMI was within the normal range. Dermatological examination revealed multiple hyperpigmented macules with mild scaling, which were confluent in the center and reticular toward the periphery over the neck, upper back, chest, and presternal region. Lesions over the nape of the neck and chin were hyperpigmented and verrucous (Figure 1). Differential diagnoses of CARP, AN, pityriasis versicolor, and macular amyloidosis were considered. Histopathological sections showed orthokeratotic hyperkeratosis, acanthosis, and low papillomatosis with few fungal spores in the stratum corneum. Sparse perivascular lymphocytic infiltrate was seen in the papillary and superficial dermis. Based on clinical and histopathological evaluation, a diagnosis of CARP was made (Figure 2).
Figure 1.

Multiple hyperpigmented macules, which are confluent at the center and reticulate at the periphery, involving the (A) chest and (C) upper back. A hyperpigmented and verrucous lesion with a reticular pattern over the (B) nape of the neck and (D) chin.
Figure 2.
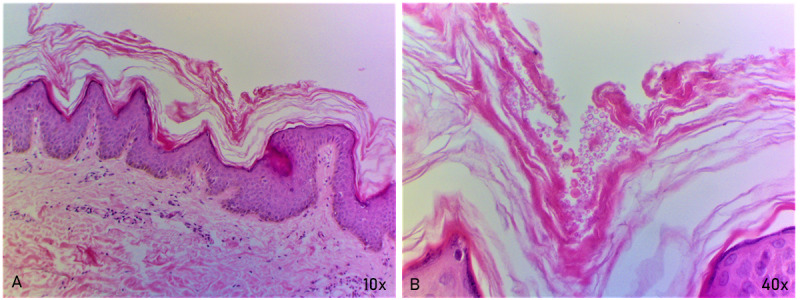
Histopathological assessment. (A) Skin section under low power (10× magnification) showing hyperkeratosis and acanthosis nigricans with low papillomatosis. The papillary dermis shows sparse perivascular lymphocytic infiltrate. (B) Few fungal spores are seen in the stratum corneum under high power (40× magnification).
Oral minocycline (100 mg once daily) was initiated for the patient, and follow-up evaluation was conducted after 14 days, which revealed complete clearing of lesions from all involved sites (Figure 3).
Figure 3.

Complete resolution of all lesions post 14 days of treatment with oral minocycline on the (A) chest, (B) back, (C) nape of the neck, and (D) chin.
Discussion
Principal Findings
CARP of Gougerot and Carteaud is a rare dermatosis seen usually in adolescents. It clinically manifests as persistent brown, scaly macules, papules, patches, or plaques. These lesions tend to be confluent at the center and become reticulated toward the periphery and are commonly located on the neck, interscapular, and intermammary regions and the axillae [4]. The etiopathogenesis of CARP is obscure till date, but data from few studies have hypothesized defective epidermal hyperkeratinization and an inherent tendency toward a hyperproliferative response to colonization by M furfur [5]. Recently, the presence of Dietzia spp in the skin has been proposed as an etiological factor in CARP. Other possible causes of CARP include endocrine abnormalities such as insulin resistance and hypothyroidism, a reaction to UV light, a variant of cutaneous amyloidosis, and genetic predisposition [1]. The histopathological characteristics of CARP include undulating basket-weave hyperkeratosis, focal acanthosis limited to the areas of elongated rete ridges, papillomatosis, and increased basal melanin pigmentation [6]. Occasionally, a mild perivascular lymphocytic infiltrate can be seen in the papillary dermis [5]. CARP is often clinically mistaken for pityriasis versicolor and usually shows no response to therapy with antifungal agents [7]. It was previously considered a clinical form of AN, but AN differs in location (axillae and neck in AN) and has a darker appearance than CARP [3,8]. Pseudoatrophoderma colli is a rare entity and is usually considered a variant of CARP. It clinically presents as atrophic and wrinkled lesions predominantly over the trunk and neck (thus named “colli”) [3].
The diagnostic criteria for CARP, as proposed by Davis et al [7] and Srinivas [9], require the following: (1) clinical presentation of scaly brown reticulated and papillomatous macules and patches; (2) the upper trunk and neck as the site; (3) negative potassium hydroxide staining of scales for spores and hyphae; (4) no response to antifungal agents; and (5) an excellent response to minocycline.
Jo et al [10] proposed a change to the original criteria, which are as follows: (1) clinical presentation of scaly brown macules and patches, some reticulated and papillomatous; (2) the upper trunk, neck, or flexures as the site; (3) negative potassium hydroxide staining or lack of response to antifungal treatment; and (4) an excellent response to antibiotic treatment.
The main differentiating features of CARP, AN, and pseudoatrophoderma colli are summarized in Table 1 [3].
Table 1.
Differentiating features between confluent and reticulated papillomatosis (CARP), acanthosis nigricans (AN), and pseudoatrophoderma colli.
| Features | CARP | AN | Pseudoatrophoderma colli |
| Age | Adolescents | Any age | 15-36 years |
| Gender | Male predominance | Equal distribution | Female predominance |
| Site | Upper trunk, neck, or flexures | Neck and axillae | Trunk and neck |
| Clinical presentation | Scaly brown macules and patches with some appearing reticulated and papillomatous | Velvety brown plaques | Atrophic and wrinkled lesions predominantly located on the trunk and neck |
| Microscopic features | Undulating basket-weave hyperkeratosis, papillomatosis, focal acanthosis limited to the areas of rete ridge elongation, and increased basal melanin pigmentation | Higher degree of acanthosis and papillomatosis than CARP and pseudoatrophoderma colli, and increased melanogenesis | Loosely thickened stratum corneum, stratum spinosum of variable thickness, irregular acanthosis, hypogranulosis, and mild dermal lymphocytic infiltrate |
| Treatment | Excellent response to minocycline | Improvement of insulin resistance, topical retinoids, ammonium lactate, and calcipotriene | Good response to minocycline |
A variety of treatments for CARP are available, among which oral minocycline (50-100 mg twice daily) is the treatment of choice. Recently, azithromycin (250-500 mg thrice per week) has been used, given its better safety profile than that of minocycline. Other less effective oral treatments options for CARP include isotretinoin, acitretin, and etretinate. Various topical agents have also been used, including selenium sulfide, ketoconazole cream, tacalcitol, tazarotene, tretinoin, and calcipotriene (calcipotriol) [1].
Conclusions
CARP is a rare dermatosis with a chronic and recurrent course, predominantly afflicting adolescents. Its etiology is controversial, but it is widely considered a disorder of keratinization. Its morphology resembles that of various other dermatological conditions such as AN and pityriasis versicolor, and, as a result, it is frequently misdiagnosed and mistreated, leading to social embarrassment for the patient. Therefore, it is prudent for dermatologists to carry out comprehensive clinical and histopathological assessments to facilitate prompt diagnosis and management of this condition. There is no standard therapy for CARP, but various therapeutic options are available such topical and systemic retinoids, oral antibiotics, topical antifungals, urea, calcipotriol, etc. Minocycline remains the first-line treatment for this condition as patients respond well to it and have minimal side effects.
Acknowledgments
DS was affiliated with the Department of Dermatology, Subharti Medical College and Hospital at Swami Vivekanand Subharti University, Meerut, India, at the time of the study and is currently affiliated with Naraina Medical College and Research Centre, Kanpur, India.
Abbreviations
- AN
acanthosis nigricans
- CARP
confluent and reticulated papillomatosis
Footnotes
Conflicts of Interest: None declared.
References
- 1.Scheinfeld N. Confluent and reticulated papillomatosis : a review of the literature. Am J Clin Dermatol. 2006;7(5):305–13. doi: 10.2165/00128071-200607050-00004.754 [DOI] [PubMed] [Google Scholar]
- 2.Yesudian P, Kamalam S, Razack A. Confluent and reticulated papillomatosis (Gougerot-Carteaud). An abnormal host reaction to Malassezzia furfur. Acta Derm Venereol. 1973;53(5):381–4. [PubMed] [Google Scholar]
- 3.Sudy E, Urbina F, Gubelin W, Misad C, Espinoza A. Pseudoatrophoderma colli: distinct entity or just a variant of confluent and reticular papilomatosis of Gougerot-Carteaud. Dermatol Online J. 2020 Oct 15;26(10):1–9. http://escholarship.org/uc/item/9q40r8v8 .13030/qt9q40r8v8 [PubMed] [Google Scholar]
- 4.Rao Tn, Guruprasad P, Sowjanya Cl, Nagasridevi I. Confluent and reticulated papillomatosis: successful treatment with minocycline. Indian J Dermatol Venereol Leprol. 2010;76(6):725. doi: 10.4103/0378-6323.72480. doi: 10.4103/0378-6323.72480.ijdvl_2010_76_6_725_72480 [DOI] [PubMed] [Google Scholar]
- 5.Hudacek KD, Haque MS, Hochberg AL, Cusack CA, Chung CL. An unusual variant of confluent and reticulated papillomatosis masquerading as tinea versicolor. Arch Dermatol. 2012 Apr;148(4):505–8. doi: 10.1001/archdermatol.2011.2812.148/4/505 [DOI] [PubMed] [Google Scholar]
- 6.Lim JH, Tey HL, Chong W. Confluent and reticulated papillomatosis: diagnostic and treatment challenges. Clin Cosmet Investig Dermatol. 2016;9:217–23. doi: 10.2147/CCID.S92051. https://europepmc.org/abstract/MED/27601929 .ccid-9-217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Davis MDP, Weenig RH, Camilleri MJ. Confluent and reticulate papillomatosis (Gougerot-Carteaud syndrome): a minocycline-responsive dermatosis without evidence for yeast in pathogenesis. A study of 39 patients and a proposal of diagnostic criteria. Br J Dermatol. 2006 Feb;154(2):287–93. doi: 10.1111/j.1365-2133.2005.06955.x.BJD6955 [DOI] [PubMed] [Google Scholar]
- 8.Jankowska-Konsur A, Maj J, Tupikowska M, Szepietowski JC. Confluent brownish papules and plaques on the neck, upper chest and back: a quiz. Confluent and reticulated papillomatosis of Gougerot and Carteaud. Acta Derm Venereol. 2013 Jul 06;93(4):493–494. doi: 10.2340/00015555-1504. https://www.medicaljournals.se/acta/content/abstract/10.2340/00015555-1504 . [DOI] [PubMed] [Google Scholar]
- 9.Srinivas S. Hypopigmented variant of confluent and reticulated papillomatosis. Indian J Paediatr Dermatol. 2016;17(3):245–246. https://journals.lww.com/ijpd/Fulltext/2016/17030/Hypopigmented_variant_of_confluent_and_reticulated.22.aspx . [Google Scholar]
- 10.Jo S, Park HS, Cho S, Yoon H. Updated diagnosis criteria for confluent and reticulated papillomatosis: a case report. Ann Dermatol. 2014 Jun;26(3):409–10. doi: 10.5021/ad.2014.26.3.409. https://europepmc.org/abstract/MED/24966649 . [DOI] [PMC free article] [PubMed] [Google Scholar]