

Abstract
Lack of diversity in IDD research is typically conceptualized only in terms of (1) recruitment of samples that do not appropriately represent the sociodemographics of the population, or (2) the limited number of researchers from historically marginalized backgrounds. Critically, the field also suffers from over-reliance on perspectives and social systems of dominant culture—both in how disability is regarded and in relation to other dimensions of identity and culture. These lenses lead to research findings that reinforce, rather than reduce, social inequities. We propose a framework that minimizes reliance on diagnostic categories, shifts from deficit- to person-centered-models, acknowledges people’s multiple identities, and includes self-advocates and diverse communities as partners in the research enterprise. The systems change necessary to support this framework is described.
Keywords: diversity, models of disability, intersectionality, bias, self-representation, advocacy, interprofessional education, bilingualism, race, disability justice
The long-standing inequities in this country’s institutions have been even more apparent as they have become centered in dialogue in the past three years. The systemic racism permeating society was brought into dramatic focus through continued senseless acts of violence against people of color and intolerance and cruelty directed at people, including children, seeking asylum and a better life in the U.S. In addition, people with intellectual and developmental disabilities (IDD) have continued to suffer discrimination in subtle and not so subtle ways (Emerson, 2021). The COVID-19 pandemic, for example, has had an outsized effect on people with IDD (Constantino et al., 2020), as well as on other historically marginalized groups, in part because of the overly politicized and antiquated nature of our healthcare and education systems. Calls for meaningful reform have grown louder as a result of these events.
In the field of IDD research, there is an increased attention to the voices of people with IDD, including around preferred language. In this paper, we use both person-first and identity-first language to respect the varied perspectives within the IDD community (Bottema-Beutel et al., 2021; Gernsbacher, 2017). In addition, funders of IDD research, such as the National Institutes of Health, have launched initiatives to better address issues of diversity, equity, and inclusion in research (https://www.nih.gov/ending-structural-racism/unite). Professional societies focused on IDD are also acting. For example, the theme of the 164th annual meeting of the American Association on Intellectual and Developmental Disabilities held in 2022 was “Dismantling Systemic Barriers: Reenvisioning Equity and Inclusion.” These actions are important, but not sufficient to sustain change.
As white, non-disabled researchers employed by institutions of higher education, we (the authors) acknowledge our positionality and the privileges conferred by our identities. We also acknowledge that much of our own research exemplifies the approaches and limitations we critique in this article. Yet, we recognize that the burden of having difficult conversations or transforming discriminatory systems should not always fall to those from historically marginalized groups. In the present article, we consider practices in the field that limit the benefits of research to people with IDD and counterproductively reinforce social inequities. These practices stem from systemic influences of the dominant culture related to how disability is regarded (e.g., ableism; social versus medical models of disability) and to other dimensions of identity and culture (e.g., racism). In light of these dominant practices and their tendency to be handled separately in the literature, we have curated strategies and priorities for the field from both a disability justice lens and a broader social justice lens to offer an integrated pathway forward toward more equitable and impactful IDD research.
Current State of IDD Research
Research on IDD cross-cuts professions, practice settings, and levels of analysis, bringing together a range of researchers, families, and professionals with a common goal of contributing to the well-being of intellectually disabled individuals. This common goal is approached through very different lenses, depending on the particular area of research: social or biological sciences; quantitative or qualitative traditions; embedded in the context of healthcare, education, or family systems. Despite these differences, inequitable societal systems influence all of this research, especially through society’s view of disability (ableism) and society’s marginalization of other identities (racism, xenophobia, sexism, homophobia, linguistic bias, and so on). Although disparities related to the conduct of research and disparities in the impact of that research have not been completely ignored, they have historically been addressed separately for disability and for factors such as race, ethnicity, and heritage language (Goode et al., 2014; Meade et al., 2014). In this section, we combine observations on disability-specific marginalization and other axes of marginalization as they impact the research process itself as well as the societal systems that should optimally support intellectually disabled individuals but are instead consistently characterized by disparities, such as healthcare and education. See Figure 1.
Figure 1.
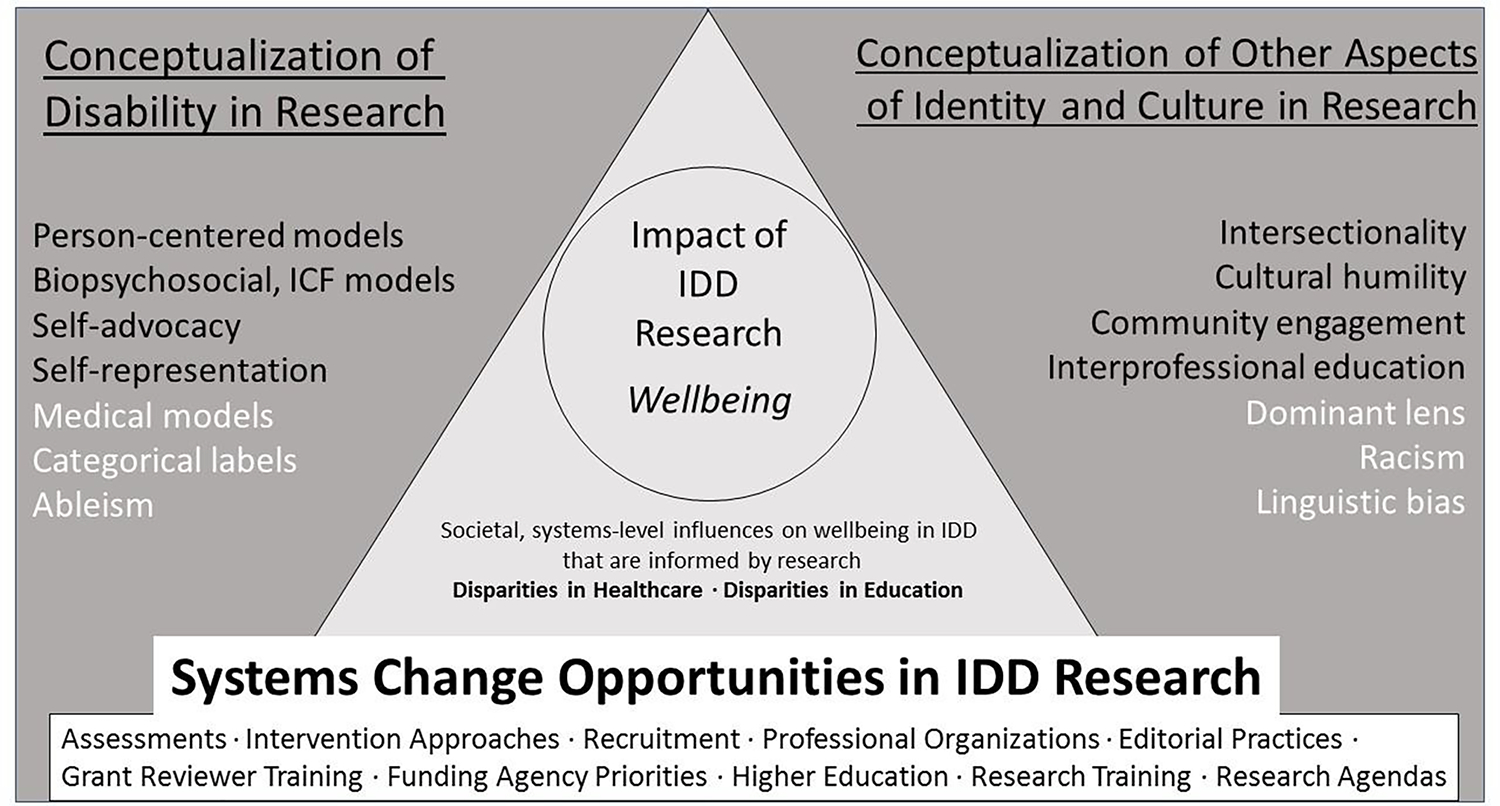
Framework for individual- and systems-level change to foster more equitable IDD research processes, to perturb systems that perpetuate IDD disparities in healthcare and education, and to increase equitable impact of research on wellbeing in intellectually disabled people.
Note that black text in the conceptualization panes shows models and strategies that increase equity; light text shows detractors from equity.
IDD = Intellectual and developmental disabilities
ICF = International Classification of Functioning, Disability, and Health
Models of Disability
Research on IDD is dominated by a medical model that relies on categorical diagnoses, such as intellectual disability (ID), autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder, and the like. This diagnostic system, which like physical health diagnoses, has become reified in the various systems that provide clinical care, education, and social services to individuals and families, such that the receipt of a diagnosis serves as the pathway to help (Casanova & Widman, 2021). Moreover, some diagnostic labels in the behavioral health arena are perceived as less stigmatizing and as better access points to services, such as ASD relative to ID. Indeed, when there have been calls to abandon diagnostic categories in general, or a specific diagnostic label such as ASD, the first argument often made against such an overhaul is that the categorical diagnosis, even if imperfect or inaccurate, is needed for accessing important clinical services (Callaghan & Sylvester, 2019; Shea et al., 2021).
Nonetheless, there are three important limitations of a categorical diagnostic approach to IDD. First, it has been argued that such diagnostic labels obscure heterogeneity that is important from both a mechanistic and clinical perspective. Abbeduto, McDuffie, and Thurman (2014) made this argument as regards research into the high co-occurrence of the ASD diagnosis among individuals with fragile X syndrome (FXS). They pointed to considerable empirical research showing that the categorical label of ASD neglected differences between individuals with FXS and autistic individuals without FXS, as well as differences among individuals with FXS. Abbeduto et al. further argued that the ASD categorical label in FXS was actually an impediment to understanding the nature of the supports needed to achieve optimal outcomes in those with FXS. This argument against overreliance on categorical ASD diagnosis in FXS can be extended to other conditions, such as Down syndrome (Dimachkie Nunnally et al., 2021). Interestingly, there have been calls to abandon the ASD categorical approach more generally in favor of an approach that recognizes the multidimensional nature of the support needs of autistic individuals (Harris, 2011; London, 2007; London, 2014).
This limitation of the medical model and its categorical diagnostic approach extends beyond behavioral definitions such as ASD and ID to include conditions defined by genetic etiology, such as Down syndrome and FXS. Although the heterogeneity within such genetic conditions is often acknowledged, that heterogeneity is most often studied relative to a limited number of biological factors (e.g., the presence of mosaicism in Down syndrome, X-activation ratio in females with FXS) or “background” genes (Boggs et al., 2022; Hagerman et al., 2018; Roper et al., 2020), rather than to the highly variable and complex social and environmental contexts in which these individuals live. Moreover, there is often an implicit assumption of fundamental, qualitative differences at a psychological or behavioral level between these etiological conditions, as seen in studies that compare and contrast these conditions with the goal of identifying their unique phenotypic features (Abbeduto, McDuffie, Thurman, & Kover, 2016). This assumption is also seen in attempts to create condition-specific curricula or therapies rather than programs based on the common supports needed across conditions (Reilly, 2012). As technologies such as whole genome sequencing become more affordable, additional rare genetic causes of IDDs will continue to be identified as in recent discoveries around SYNGAP1, ADNP, FOXG1, and CDLK5. Understandably, gene-specific, parent-led foundations emerge with each new discovery for the purposes of advocacy and raising funds for research. These foundations are a powerful and highly beneficial force in advancing research. At the same time, however, they reify the categorical approach, which can be an impediment for developing therapeutics and supports that address shared needs, especially in this era of precision medicine. Taken together, whether for behavior or genetics, overemphasis on categorical labels might simultaneously obscure meaningful differences and similarities among individuals.
Second, the medical model and its attendant categorical approach to diagnosis also has as its foundation an implied comparison to a normative, preferred, more highly valued state. In the case of physical health conditions, such as cancer, the comparison is to a healthy (i.e., a non-cancerous state). As IDD self-advocates have pointed out, extension of the medical model to IDD implies that people who are assigned an IDD diagnosis are not only different from average or expected, but also less valued, are defective, or somehow represent a less desirable class of human beings and, importantly, that these individuals are the source of their own challenges (Bottema-Beutel, Kapp, Lester, Sasson, & Hand, 2021; Burks-Abbott, 2022; Dwyer, Ryan, Williams, & Gassner, 2022). Self-advocates and others who argue against this ableist approach point to the ways in which a variety of descriptions with highly negative connotations are applied to people with an IDD diagnosis as evidence of the biases of the medical model; for example, the use of phrases such as the “epidemic” or “tsunami” to describe the increase in prevalence estimates of autism in recent decades (Dwyer et al., 2022). It is also reasonable to argue that the biases inherent in the medical model extend beyond language and shape policies that prevent self-determination and limit access to participation in “normative” experiences such as attending regular education K-12 classes, having access to postsecondary educational programs, or having the right to employment that provides a living wage.
Third, the medical model shapes research approaches (e.g., through an emphasis on identifying differences between diagnostic groups) and research interpretations (e.g., through an emphasis on deficits); however, there are other models that can serve as a basis for IDD research (Ojeda & San-Juan, 2022). In contrast to medical, categorical models of disability, the social model of disability, which acknowledges the restrictions imposed by society when accommodations are not made, and the neurodiversity movement have been integral in shifting the dialogue around neurodevelopmental diagnoses (Dwyer et al., 2022; McClimens, 2003). The term neurodiversity suggests that variations in brain and behavior are natural and valid ways of being, thereby highlighting the social and cultural aspects of diagnoses, with attitudes and barriers imposed by society causing impairment, rather than differences in development or behavior (Casanova & Widman, 2021). The neurodiversity movement has led to changes in language/labeling (e.g., neurotypical rather than typically developing) and in the discourse around whether different ways of being should be cured or accepted. The perspectives of individuals with IDD are critical in such conversations, although there are differing perspectives within the IDD community regarding this topic (Chapman & Viet, 2020). Researchers, largely steeped in entrenched systems, have been slow to truly hear these dialogues and update their language and the framing of their research.
Beyond the medical and social models of disability, some have proposed hybrid models of disability that acknowledge individuals’ needs but do so with respect and without imposing judgment (e.g., the biological gradient model; Casanova & Widman, 2021; Nelson, 2021). Other models that may be useful for researchers on IDD to take up include the International Classification of Functioning, Disability, and Health (ICF) and other biopsychosocial models of disability (Buntinx & Schalock, 2010; Meade et al., 2014; Westby & Washington, 2017). The ICF model, for example, not only acknowledges disability, but also activities, participation, and personal and environmental contextual factors, giving an explicit nod to culture (WHO, 2007). Awareness of the pervasiveness of the medical model of disability and its alternatives will open doors for research approaches that center, rather than pathologize, people with IDDs.
Dominant Culture Pervades: Participants and Researchers
We believe that the field also suffers from an over-reliance on perspectives and social systems of the dominant culture that leads to research findings that reinforce rather than reduce social inequities. That over-reliance is a direct result of who is involved in research: participants and researchers, predominantly from dominant culture backgrounds.
Representation in Research.
There continues to be a lack of attention to recruitment of diverse samples into research in the IDD field (McDonald et al., 2022). Indeed, race and ethnicity are often not even reported in published studies related to disabilities (Pierce et at al., 2014; Machalicek et al., 2008; Nguy et al., 2022; Steinbrenner et al., 2022), which is likely because the samples are not at all diverse. This is despite the availability of tools to systematically examine race and ethnicity reporting in published research (e.g., GAP-REACH; Lewis-Fernandez et al., 2013). When race and ethnicity are reported, the samples studied are mostly comprised of individuals who identify as white and the relationships among the variables of interest and race and ethnicity are seldom examined (Pierce et al., 2014). Moreover, this lack of attention to race and ethnicity occurs even in studies in which these factors could a priori be expected to have a substantial impact on the outcomes and relationships of interest (Machalicek et al., 2008). Recent attention to QuantCrit (quantitative critical race theory) has highlighted the ways in which traditional quantitative approaches to research and data analysis have perpetuated systemic racism (Castillo & Gillborn, 2022). Other dimensions of diversity beyond race and ethnicity, such as gender identity, language background/multilingual status, or cultural background are arguably even less likely to be reported or examined.
The failure to recruit diverse samples is due in large part to a reliance on culturally limited methods to recruit participants into research. First, a major source of recruitment is through clinics and health systems, especially those affiliated with universities. Unfortunately, individuals of color, individuals from low-resourced communities, individuals who speak a language other than English, individuals from refugee and immigrant communities do not have the same access to health care as do individuals from the dominant culture (Fiscella et al., 2002; Robertson et al., 2019; Willink et al., 2021). These individuals are thus underrepresented in the medical settings that are a major source of recruitment. An example is the consortium of clinics that was created to develop clinical care standards, improve access to care by supporting the opening of new clinics, and support research on FXS. Although this effort has been highly successful in many respects and beneficial to many families, the patient population served on the whole is only 10% Hispanic/Latinx and 12% non-white (Sherman et al., 2017). Second, in the case of research focused on relatively rare etiologic groups, such as single-gene conditions associated with autism, a major source of recruitment is the various local and national support and advocacy groups, many of which have been launched by families or by the clinicians who serve affected individuals. Here too, however, it seems that these groups are largely constituted by, and reach, individuals from the dominant culture. Indeed, an informal survey indicates that few of these groups compile data on the sociodemographic characteristics of their memberships; however, a review of the leadership boards of virtually any of these groups or attendance at the conferences they sponsor makes abundantly clear their lack of diversity.
In addition to the sources of recruitment, the approach generally taken for recruitment continues to favor engagement of individuals from the dominant culture. In particular, the creation of registries whether at the local university level or at a national level depends on potential participants placing a high value on research whether for themselves, their communities, or society in general and actively searching for research opportunities. Many communities outside of the dominant culture, however, are unlikely to see research as safe or valuable. We have only to point to high-profile research abuses involving African American and Black citizens, such as the Tuskegee Airman studies or the nonconsensual use of genetic material from Henrietta Lacks, to understand the hesitation of these communities to participate in research, especially when the commitment is as open-ended as in the case of enrolling in a registry rather than a specific research project (Washington, 2008). Further, requests for genomic data from individuals with intellectual disabilities, especially relevant to precision medicine, may reflexively raise concerns for many people by harkening back to the pseudoscience of eugenics, which sought to limit the rights of individuals with disabilities and others deemed unworthy of reproducing (Miller & Levine, 2013; Sabatello et al., 2019).
More generally, we researchers are often transactional and one-sided in our approach to recruitment, which is especially problematic against the backdrop of a mistrust of research and researchers. In particular, the first contact a researcher has with many individuals may be through the latter’s receipt of an unsolicited study flier or informed consent form. This can be seen as “we need something from you even though you don’t know us and have no reason to believe we care about your welfare.” We also often have limited success even when we reach out through entities that serve diverse communities, such as the public-school system. Many individuals from historically marginalized groups, however, may also have experienced bias and discrimination from those entities, as in the case of Black families who see their children disciplined at higher rates than white children in school and both over- and under-identified for special education, adding another reason to mistrust the researcher’s overture (Skiba et al., 2011; Morgan et al., 2017; Robinson & Norton, 2019).
Implicit Bias and Research Priorities.
It is also important to recognize that each of our lived experiences provides us as scientists a lens through which we identify research questions that interest us and that we prioritize. In the case of researchers who are members of the dominant culture, the lens may be less likely to lead us to address questions of relevance and high priority to historically marginalized groups. Although the experiences of individuals with IDD are influenced by countless social and contextual factors, including culture, ethnicity, gender, among others, these factors are understudied (Skinner & Weisner, 2007). For example, racial bias in diagnostic practices in clinical settings (Mandell et al., 2007; 2009), disciplinary practices in public education (Skiba et al., 2011), and interactions between patients and professionals may hold less intrinsic interest, on average, to scientists from the dominant cultural group than to those whose lived experiences include daily examples of bias directed against them and their communities. As another example, scientists from the dominant culture may be less interested in, or less certain of how to study, the occurrence of gender identity questioning among individuals with IDD or in the efficacy of clinical practices to support individuals with IDD as they explore their gender identity (e.g., Corbett et al., 2022).
All this is not to say, of course, that members of the dominant culture do not or cannot address issues about race, ethnicity, and gender in their research on IDD; however, we believe that such issues are less likely to be “on the radar” of researchers without those lived experiences. These cultural gaps in knowledge suggest a need to recruit into the field a more diverse workforce of scientists, including those whose lived experiences will provide them and their colleagues a broader cultural lens. There is also a need, however, to include as regular components of training for researchers and related professionals (a) the opportunity to recognize their own implicit, or unconscious, biases, how to address microaggressions, and how to push for structural changes that increase equity (Onyeador et al., 2021; see also INSAR’s repository of anti-racist resources, https://www.autism-insar.org/page/Repository), (b) how to collaborate within an interdisciplinary and multicultural team (Dibble & Gibson, 2013), and (c) how to create partnerships with self-advocates and diverse communities (Morgan et al., 2021; Stahmer et al., 2019). Such training initiatives are needed because researchers without lived experiences are less likely to identify the cultural framing and need for decolonization of constructs relevant to IDD that have been defined using WEIRD (western, education, industrialized, rich, democratic; Henlich et al., 2010) assumptions (e.g., the case of joint attention; Bard et al. 2021).
Further, Dwyer et al. (2022) point out that research on IDD is typically conducted with the goal of identifying weaknesses, challenges, and impairments rather than also identifying strengths that can be leveraged. Related to this is the need to integrate self-advocacy and neurodiversity with assessment and intervention frameworks (Brown et al., 2021; Leadbitter et al., 2021; Nelson, 2021; Schuck et al., 2021). The same is true for integrating social models of disability with special education practices (Gallagher et al., 2021). Research priorities and the interpretation of findings are constrained by the theoretical framing held by researchers, which is why considering these frameworks and integrating across perspectives is so important.
Systemic Bias in the Research Process Reinforces Inequities
As researchers in the field of IDD, our goal is to generate evidence that will change practices and policies in ways that support quality of life and wellbeing for individuals with IDD and their families. In spite of this motivation, many research practices and tools preserve social inequities and perpetuate marginalization (Morgan et al., 2021).
Measurement tools.
Many norm-based standardized assessments (e.g., intelligence tests, achievements tests, developmental screeners, diagnostic interviews and structured observational procedures) commonly used in research and clinical practice have been developed in ways that are most consistent with the schema, scripts, and behavioral patterns of the dominant culture (Helms, 2006; Williams, 2022). In the U.S., for example, verbal items on tests of intelligence are typically written to reflect the dialects of English that are most common to middle- to upper-income individuals in Northern regions of the country. As a result, individuals who speak other regional dialects (e.g., those common in the Southern U.S.) or a dialect more common in other cultural groups (e.g., African American or Black English) may be at a disadvantage from the beginning because they will be less familiar with items or particular wording used. More generally, standardized assessments are typically constructed in ways that assume and value concepts and experiences that may be common in the dominant culture but less so in other communities; again, potentially putting some groups at a disadvantage at the outset (Shuttleworth-Edwards, 2016). Even when attempts are made to create alternate versions of these tests adapted to other cultural groups, the adaptation is often quite perfunctory. Spanish-language versions of standardized assessments, for example, are often simply translated into a single dialect of Spanish, which fails to recognize the heterogeneity of language among Spanish speakers, and there is no attempt to assess the appropriateness of the actual item content for the Spanish-speaking community, which can include individuals who have varying degrees of experience with dominant U.S. culture (Bevan, Liu, Wallis, & Pinto-Martin, 2020; del Hoyo et al., 2021).
One example central to the definition of intellectual disability is adaptive behavior, which refers to the ability to meet naturally occurring social demands and complete personal activities of daily living. This construct is culturally bound, and tests of adaptive behavior are typically created through the lens of the dominant culture. As a result, these assessments can underestimate the competence of individuals from marginalized groups, such as Black autistic youth (Ratto et al., 2016), or fail to account for cultural differences in the behaviors that are seen as adaptive or valued (Taverna et al., 2011). Indeed, most standardized tests are constructed from the perspective of Western cultural values, which can disadvantage individuals from non-Western cultures, including those who reside in the U.S. or other Western countries but retain the values and practices of their culture of origin (Chen et al., 2022; Taverna et al., 2011).
These biases are not limited to standardized assessments. Experimenter-created tasks and materials likewise are typically constructed from the researcher’s own experiential lens and, combined with the limited diversity in the IDD research workforce, it is likely that those measures too will be biased in ways that can disadvantage marginalized communities. Recently developed outcome measures may have stronger psychometric properties and are better suited to evaluate efficacy of new treatments for individuals with IDD (Berry-Kravis et al., 2013; Budimirovic et al., 2017; Esbensen et al., 2017); however, these measures are largely limited to English-only versions, which leads to the exclusion of a growing proportion of the IDD population from participation in treatment studies (del Hoyo Soriano et al., 2021).
This state of affairs in measure use and development means that many measures yield results that may not be representative of the skills and abilities of participants with IDD from marginalized groups, may incorrectly exclude individuals from studies because they do not meet eligibility standards set by the measures, or may assign individuals incorrectly to a diagnostic category. These problems limit the value of research and are likely to perpetuate the negative consequences of these test biases that have been well documented in healthcare and educational practices, such as the inadequate assessment and overdiagnosis of Black children with ID (Kim et al., 2021; Schmidt et al., 2022).
Treatments and supports.
A similar set of problems characterizes research designed to develop behavioral treatments or other supportive interventions. In this area of research, most evidence-based interventions are typically developed and tested on English speakers from the dominant culture (Vargas London et al., 2022). This may reflect in part the previously noted failure to recruit individuals from historically marginalized groups into research in general, as well as the lack of linguistically and culturally appropriate measures. It may also reflect, however, more limited resources to meet the practical demands of participation in an intervention study for some families from historically marginalized groups (such as travel to a university site; participating during the workday, which could mean loss of pay; arranging costly childcare for other children; Lakes et al., 2009; Tomeras & Kjobli, 2017; Vargas London et al., 2022). Additionally, the long-term commitment of being in a treatment study may not be realistic for families with limited resources and constraints on their time that are out of their control. Whatever the source, the result is that evidence-based practices in healthcare and education settings emerge largely from research with non-diverse samples, which raises questions about their generalizability and appropriateness for individuals from non-dominant cultures.
Additionally, the typical approach to meeting the needs of individuals and families from historically marginalized groups is to take interventions that have been shown to be efficacious for the dominant culture and then make adaptations for other cultural groups, although there are exceptions (e.g., Magana et al., 2020). At best, this means that these non-dominant groups must wait longer for interventions that meet their needs. It is also possible, however, that the adaptation process may not be fully successful, and certainly there will be some cultural groups for whom no adaptations will be attempted, perhaps because the size of the non-dominant community is seen as too small to justify the cost and effort of adaptation or because of an inability of researchers to understand their needs. To this point, there are relatively few open-ended opportunities for individuals with IDD of any cultural background to share their experiences and give guidance on affirming supports and priorities for quality of life—a gap which additional qualitative research could fill (e.g., Atherton et al. 2021). Under the current circumstances, many individuals with IDDs will experience interventions that are a poorer fit for them than for their dominant-culture peers.
In summary, the field of IDD research has a serious generalizability problem. The measures we use, the treatments and supportive interventions we develop, the ways in which we recruit participants, and even the research questions we ask (and fail to ask) generate findings that are optimized for the dominant culture. There is considerable evidence that individuals with IDD from historically marginalized groups have less access to high quality healthcare services, education, and social supports than do those from the dominant culture (Kim et al., 2021; Leigh et al., 2016; Robertson et al. 2019). As such, inequitable practices in research in IDD not only fail to reduce disparities in healthcare or education for people with IDD, but may actually exacerbate those healthcare and education disparities, which is clearly counter to the goal of improving wellbeing in intellectually disabled people.
Pathways Forward: A Framework for Systemic Change
Shifting IDD research toward more equitable priorities, practices, and outcomes is possible by implementing strategies that utilize critical reflection, centering the experiences and voices of individuals with IDD, and making structural changes to the systems that are the foundation of research (e.g., professional training, graduate education). In this section, we integrate topics and actions from disability perspectives and perspectives on other disparities and marginalization, as shown in Table 1 and Figure 1.
Table 1.
Actions to Foster Equity in IDD Research Processes and Impact
| Individual-level Actions | |
|---|---|
|
| |
| Engage in critical self-reflection and increase cultural humility, through understanding implicit bias, increasing linguistic and cultural competence, and recognizing systems of bias and oppression | |
| Avoid ableist language and perspectives | |
| Self-educate on the history of disability justice and research abuses | |
| Utilize person-centered or biopsychosocial models of disability (e.g., ICF) | |
| Acknowledge the cultural framing of constructs related to IDD | |
| Include self-advocates in all phases of research | |
| Learn how to support meaningful, inclusive participation in research through universal design for learning practices | |
| Use qualitative methodologies to understand the priorities of people with IDD and their desired, affirming supports | |
| Select research topics that are priorities of people with disabilities | |
| Select research topics that acknowledge the intersecting and multiple identities of people with disabilities | |
| Learn how to build partnerships and create genuine collaborations in diverse communities | |
| Consider community-engaged scholarship as an approach | |
| Build research teams composed of diverse experiences, backgrounds, and perspectives (e.g., multicultural, multilingual teams) | |
| Seek out education or training for communicating with AAC/AT users | |
| Measure, analyze, and interpret social and cultural contributors to well-being in IDD, including race and ethnicity | |
| Address intersectionality in research design, analysis, and interpretation | |
| Learn how to create plain language, usable translations of research findings for dissemination to the communities who participated in the research | |
| Systems-level Actions | |
| Support the creation of culturally and linguistically appropriate assessments | |
| Support the creation of culturally and linguistically appropriate and affirming interventions | |
| Prioritize development of interventions that support common needs across diagnostic categories | |
| Earmark funding for research priorities of people with IDD | |
| Change funding mechanisms to support partnership-building in diverse communities and dissemination efforts past research completion | |
| Fund training and re-specialization for research topics and approaches | |
| Incentivize teams and collaborations with diverse experiences and skillsets | |
| Train and re-train grant reviewers to value diverse teams, person-centered frameworks, community partnerships, and methodologies that center those with IDD | |
| Train and re-train editorial board members to examine personal biases and to expect measurement and interpretation of social and cultural contributors to wellbeing in IDD | |
| Recruit, fund, and train the next generation of researchers to take actions and approaches to increase equity in IDD research | |
| Leverage interprofessional education and collaboration across professional organizations | |
Intersectionality and Person-Centered Approaches
We each have multiple identities, or multiple dimensions of our identity (Crenshaw, 1989; Morgan et al., 2021). These identities include various socially constructed categories such as race, ethnicity, and gender, as well as roles such as parent, researcher, etc. Most of us would argue that we are not defined solely or even primarily by one of these categories or roles. Instead, we view ourselves as the sum of those identities. We also recognize that the primacy of these categories and roles in determining our behavior, experiences, and goals may change at various points in our lives or in different circumstances. We probably also believe that we have some agency in defining our own identities relative to these constructs and roles. It is noteworthy, therefore, that we in the IDD research field appear comfortable defining the participants in our studies solely by their IDD diagnostic label, assuming that label is the most important determinant of their identity and ignoring all their other identities and the complex ways in which those identities shape their lived experiences.
The consequences of this unidimensional categorical view of people with IDD are clear in research, from framing research questions to selecting assessments to developing supports (Brown et al. 2021). Take gender identity as an example. Decades of research address the ways in which gender is socialized in neurotypical children (Fagot et al., 2000), and yet, gender differences and gender socialization have been studied relatively rarely in the field of IDD. Moreover, the studies of gender and IDD that do exist have largely focused on gender in terms of biological sex and on whether there are ability differences or differences in so-called challenging behavior between males and females with IDD (McClintock et al., 2003). This has led to a very limited understanding of the potentially unique ways in which gender identity emerges in people with IDD. Importantly, this has also led to relatively few efforts at developing supports for youth with IDD who are gender diverse. It is now clear, however, that adolescents with disabilities, including autistic youth, can benefit from support around gender identity and expression, with depression and other negative consequences if support is not forthcoming (Corbett et al., 2022). In short, our uni-categorical view of identity in IDD research has left us with important gaps in our evidence base to the detriment of our ability to support the wellbeing of individuals with IDD.
More generally, there is a naivete and an arrogance that is exemplified by this uni-categorical view in which IDD is assumed to be the most important determinant or descriptor of an individual’s identity. It is highly likely that individuals with IDD have very different lived experiences depending on the other dimensions of their identity (Andrews et al., 2019). There is considerable evidence, for example, that individuals from historically marginalized racial and ethnic groups, such as Black and Latinx individuals, are diagnosed with autism and thus receive services at a later age than their white counterparts (Habeyeb et al., 2022; Jo et al., 2015; Mandell et al., 2022; Miller et al. 2022). Moreover, even after diagnosis, access to clinical services is more limited for those from these marginalized groups (Angell et al., 2018; Zeleke et al., 2019). No doubt, these racially and ethnically correlated experiences of, and interactions with, the healthcare system lead to different developmental trajectories for Black and Latinx autistic individuals relative to their autistic peers from the dominant culture. The factors affecting diagnosis and access to services may also be different for individuals with different gender identities. Disciplinary practices in schools, including for students in special education, also differ according to race and ethnicity (e.g., Black students, whether with an identified disability or not, are more likely to be disciplined or expelled for what is seen as disruptive behavior by school personnel), which may have consequences for many aspects of subsequent development (Naser, Brann, & Noltemeyer, 2021; Skiba et al., 2011). Finally, it is possible that despite the primacy that our field affords the label of IDD, factors such as race and ethnicity, may be more important determinants of the lived experiences of many individuals. In fact, there is considerable evidence that a host of environmental factors, such as exposure to pollution, some types of insecticide, maternal stress and infections during pregnancy, and nutrition, all play a role in creating risk for IDDs (Lukens & Eyo, 2022), and these factors are correlated with poverty and, because of systemic racism, race and ethnicity.
Reliance on IDD categorical labels as the primary identity for the participants in research also continues to perpetuate a view of these individuals as different from, and less than, individuals whom we designate as typically developing (Gallagher et al., 2014). Acknowledging this devaluation allows an opportunity to consider disability on a continuum rather than always through categorization (McClimens, 2003). In fact, many decades of IDD research have largely found few qualitative differences between people with IDD and the rest of the population; instead, it appears that there are quantitative differences on various dimensions of ability such as language, memory, etc. Nonetheless, we as researchers and certainly many people in society at large view individuals with the IDD label as variously needing to be protected rather than supported in making their own life choices (e.g., participating in romantic relationships) or altered so as to be more “normal.” Researchers feel confident in defining what optimal behavior or preferred developmental patterns are for individuals with IDD. This paternalism and “othering” of individuals with the IDD label has also created social systems that actively deny them normative experiences, such as competitive wage employment and postsecondary education and, in the not too distant past, was used to justify forced sterilization during the eugenics movement (Miller & Levine, 2013).
Abandoning the uni-categorical IDD view and recognizing the multiple identities of people with IDD will be challenging from a research perspective and will require new conceptual frameworks, research designs, and methods of measurement. Doing so, however, will lead to a better understanding of how to support the wellbeing and quality of life of people with IDD, and to challenge systemic barriers to equity in healthcare and education settings for all. Relative to categorical framings, biopsychosocial frameworks offer a paradigm shift. Integrating models, such as the ICF and other person-centered approaches, with assessment and intervention would support a change in conceptualization of disability that acknowledges intersectionality, culture, and systemic influences on outcomes (Buntinx & Schalock, 2010; Meade et al., 2014; Roy et al. 2021; Westby & Washington, 2017). This reframing is emerging in work on IDD in disciplines such as nursing, mental health, and dentistry (Ingham et al., 2008; Wilson & Watson, 2022; Wilson et al., 2020). Educational research and practice feature shifts to universal design for learning and culturally sustaining pedagogy, thereby demonstrating how to center intellectually disabled individuals (Smith & Lowry, 2017; Waitoller & King Thorius, 2016). Precision medicine is another framework that has the potential to reduce disparities through tailored supports, provided that the framework takes into account not only (increasingly accessible) genetic information, but also environmental, and personal background factors (Sabatello, 2018). Abandoning the uni-categorical approach would lead us as researchers to view intellectually disabled people as individuals with multiple, intersectional identities in their cultural contexts and to view them as potential partners in the research enterprise, a point to which we now turn.
Participatory Research, Self-Representation, and Defining Research Agendas
There has been a growing emphasis on including self-advocates, family members, and community leaders as partners in research on disabilities (Maye et al., 2021; Pukki et al. 2022). Such partnerships have been increasingly common in the field of autism research (Girolamo, Rice, & Ghali, under review) and more generally, within the fields of implementation science, which is concerned with bringing evidence-based practices to scale under real-world constraints, and community-engaged scholarship, which co-creates research agendas through mutually beneficial relationships. These partnerships position disabled people as members of the research team, rather than subjects of study. Despite barriers to participation, people with disabilities are interested in contributing to study designs and believe that participants and researchers should be partners (Sabatello et al., 2019). Unfortunately, people with cognitive or communication challenges are less likely to be represented in self-advocacy opportunities; this is termed a partial representation problem, and it creates a challenge and an opportunity for IDD research (McCoy et al., 2020). The challenge is that additional efforts on the part of the researcher are needed to achieve self-representation and collaboration in research for IDD. The payoff is sizable: these partners have input into all stages of the research enterprise, from identifying high priority areas of investigation in terms of community needs to helping with dissemination efforts that translate research findings into forms that are understandable and more immediately useful to practitioners, policy makers, and people with IDD (Beechey, 2022). Thus, involvement of people with IDD in the research process itself increases equity related to disability specifically and to other aspects of marginalization by integrating self-representation and cultural representation into the framing and impact of the research.
Some researchers may resist these partnerships, arguing that people with IDD cannot understand the complexity of the research enterprise. We believe that this argument, first, shows a lack of respect for people with IDD and the public more generally, and second, reflects the lack of training that most researchers have in the process of effectively communicating their research. That IDD researchers need to improve their communication in this regard brings to mind the double empathy problem, which refers to the fact that non-autistic researchers lack insight into autistic culture while perseverating on autistic people’s lack of social insight (Milton, 2012). Researchers may also lack experience communicating with AAC users or assistive technology users, may not be fluent in signed languages, such as ASL, or otherwise might not share the linguistic or communicative background of their community partners or participants. For monolingual and monocultural researchers, collaborative teams that bring diverse skillsets may be critical to successful partnerships. Training on inclusive research practices, universal design, and respectful community engagement, for example, could help researchers develop the skills needed to hold up their side of research and community partnerships with people with IDD.
Researchers may also be resistant to a partnership approach because they worry that self-advocates and other members of the public will disagree with them about the value of a particular study or research topic. Indeed, researchers need to be prepared to accept critique and make adjustments. Researchers would also benefit from recognizing the pernicious consequences of the eugenics movement of the past and, therefore, the need to address the legitimate concerns of the potential uses of genetic data held by self-advocates. For example, researchers have worried that autistic self-advocates, many of whom assert that autism is not a disorder but rather an instance of natural variation in the human condition and a dimension of individual difference, would be against genetic research. In fact, these researchers would likely point to the Spectrum10K project on the genetics of autism in the United Kingdom (https://spectrum10k.org/) that was halted temporarily because the research team failed to get input from the autistic community. Similarly, the neurodiversity movement has led to a “cure vs. acceptance debate” in which the perspectives of individuals with IDD are critical, although there are differing perspectives even within the IDD community (Bottema-Beutel et al. 2021; Chapman & Viet, 2020). Here too, however, researchers would be better served and their findings more likely to be valued by self-advocates and the public if they worked with self-advocates to communicate to the public how the research is consistent with a neurodiversity view of IDD—and then co-create the next set of research questions.
Shifting from a transactional to a partnership approach, however, requires more than simply tolerating this approach. It will require training researchers so that they (a) understand and can address the factors that prevent diverse communities of people with IDD from participating in research (Goode et al., 2014); (b) know how to support the participation of these diverse audiences in decision-making interactions, which will include learning how to make accommodations in meetings, methods of communication, and timelines for decisions (https://rootedinrights.org/how-to-make-your-virtual-meetings-and-events-accessible-to-the-disability-community/; https://nisonger.osu.edu/learn-to-zoom/;https://ncapps.acl.gov/docs/SupportingMeetingAccessibility_NCAPPS_200519.pdf); and (c) know how to create relationships that extend beyond the boundaries of a single study, so that self-advocates view the researchers as true members of, and participants, in their community. Along these lines, researchers might consider qualitative research traditions, including but not limited to photovoice (Atherton et al., 2021; Wang & Burris, 1997), and technological tools, such as inclusive speech recognition (e.g., projectunderstood.ca), to better understand, include, and prioritize the perspectives of people with IDD.
Partnership approaches will change not only the process, but also the topics and priorities of research related to IDD. Utilizing theoretical frameworks that are person-centered will facilitate that change as well. This includes ICF and capability approach lenses that deliberately emphasize decision making and agency (Trani et al., 2011). These person-centered models will also facilitate dialogue across professions in how to determine research priorities to improve wellbeing in IDD and to be responsive to the co-constructed priorities of intellectually disabled individuals (Buntinx & Schalock, 2010). Through participatory, community-engaged research, the research agenda can be set by those with relevant lived experiences.
Although partnership is labor-intensive, there is a growing effort to create materials, roadmaps, stakeholder networks/databases, and toolkits to support implementation of a partnership approach. Particularly noteworthy here are efforts led by Goode and her colleagues, who have created materials to assist researchers and self-advocates: https://centerforstartservices.org/Truth-and-Reconciliation-Project. McDonald and colleagues (2022) have focused on methods for removing barriers and supporting the participation of adults with IDD in research as reporters of their experiences, challenges, and achievements (as opposed to reliance on caregivers and other informants). Further, the International Society for Autism Research hosts a community-collaborator interface with which researchers can post ads for stakeholder input.
It is incumbent on the field to make the systems-level changes needed to foster and reward these approaches to research. Indeed, funding models that encourage or even require partnership with individuals with IDD would shift the field. Partnership takes time and not all traditional sponsorship for research programs reward or sufficiently fund those components of community collaboration. Funding bodies, such as the National Institutes of Health, will need to provide the time and money in funded projects for researchers to build partnerships with self-advocates and within historically marginalized communities, especially in new areas of research or for researchers new to topics or approaches. Researchers will also need funds, time, and training to disseminate their findings in nontechnical and usable formats to communities after the research is completed. This partnership building and dissemination could be supported in specialized grants or “traditional” grants could be funded at higher levels or for longer periods of time. At the same time, these funding bodies should require metrics to assess the success of a researcher’s partnerships and dissemination efforts. Further systems changes include training reviewers of grant applications to properly evaluate and recognize the value of participatory research, for sponsors to prioritize funds for self-representation, and publishers to reduce inequalities in publication processes, such as by encouraging editorial board membership by self-advocates so that they shape the ultimate message produced by the research (see Autism in Adulthood as a model; Roberts et al., 2021).
Interprofessional Growth and Collaboration at Individual and Systems Levels
As researchers shift to creating partnerships with people with IDD and other non-scientists from diverse communities, they will need to adjust their own perspectives and styles to enter into genuine, productive, and culturally and linguistically competent interactions with these partners (Rhagavan & Small, 2004). How can cultural and linguistic competence and humility be achieved in a way that is tractable? Researchers can begin by acknowledging the ways in which their own cultural and linguistic lens, and the power and privilege that come from being a member of an academic or professional setting, affect their behavior and shapes their interactions with others. The term cultural competence means approaching interactions with the community in ways that are responsive to their beliefs, attitudes, language and patterns of behavior (https://acl.gov/about-acl/authorizing-statutes/developmental-disabilities-assistance-and-bill-rights-act-2000). The term linguistic competence refers to adapting communications to ensure they can be understood by the target audience, which can include changing the complexity or form of a message based on a person’s language preference, background, or ability or a translation of the message to a person’s heritage language. Researchers should also spend time understanding the culture and language of their potential partners. Hiring staff from the community of interest or staff who speak the language of that community helps to ensure productive interactions and demonstrates the value placed on cultural and linguistic competence. As partnerships with people with IDD and others in community are launched, it is critical that researchers are willing to listen to, and learn from, those partners so that study questions, research methods, recruitment materials, and dissemination efforts are developed appropriately.
Research on IDD is not unique in being influenced by systems of oppression. Many of the same factors can be seen at play in the history of policies and practices in special education, social work, applied behavior analysis, nursing, speech-language pathology, and other allied health fields and professions. These shared burdens of ableism, racism, and dominant-culture means-and-ends are apparent in the narratives produced by research and in the impacts of that research on the lives of individuals with IDD.
This ubiquity of bias points to two constraints and opportunities for the field. First, it must be recognized that the long-standing and well documented inequities in healthcare, education, criminal justice, and economic mobility for historically marginalized groups are also at play in research on IDD. The field functions as it does because of systemic bias that is prone to promoting ableism and prioritizing the needs and perspectives of the dominant culture. Reducing those inequalities and that bias around IDD will require both individual- and systems-level change. Changing systems is grueling work that requires action, persistence, and a willingness to be uncomfortable. Obtaining systems change hinges on commitment of not only minoritized researchers and self-advocates, but also researchers without marginalized backgrounds.
Second, because the inequity in research on IDD can be traced to oppressive systems, pathways forward do not need to be generated from scratch. Lessons, strategies, and practices can be borrowed from, adapted to, and co-developed in adjacent fields through interdisciplinary research, training efforts, and other professional activities (Cooper et al., 2022). Many groups of professionals are grappling with their roles in inequitable research and service enterprises from nurses to BCBAs to SLPs to special educators (Camarata 2022; Donaldson, 2021; Machalicek et al., 2021; Morris, 2022). One shared consideration for these disciplines is how the next generation of researchers and professionals is recruited and trained, and how those already in the field can “re-train” in equitable practices. Having professionals and researchers engage in equity-minded conversations and changes, with organizations and institutions providing guidance and modeling action, will contribute to individual- and system-level changes needed (Buntinx & Schalock, 2010). Those changes might include professional training opportunities, updated curricula in undergraduate and graduate programs, revised accreditation standards, and accompanying funding and infrastructure. Collaborative problem-solving, cross-training, and interdisciplinary approaches to increasing equity in research on IDD are likely to be worthwhile, efficient, and effective action steps to addressing systemic problems.
Conclusion
Fully realizing equitable IDD research will come with (will drive and be driven by) systemic changes. The actions of individuals in their own research practices are important, but so are the ways in which individuals push to change the norms of research processes. Training the next generation of researchers and practitioners to value self-advocacy, to recognize bias, and to champion equity-minded research will be important. The systematic inequities that characterize healthcare and education cannot be ignored, as they are at the basis of many of the disparities observed in the lives of individuals with IDD and the basis of many of the sources of inequity that show up in the research enterprise. Research in IDD has the potential to perturb healthcare and educational disparities. Doing so would accelerate the extent to which this research contributes to the wellbeing of intellectually disabled people.
Research in IDD can move towards equity by updating its conceptualizations of disability, updating its conceptualizations of culture and other identities, and tackling systemic change within the research process itself. Centering the experiences and voices of intellectually disabled people and acknowledging all their identities and contexts are key. Interprofessional collaboration and training will also serve the field well. No community of professionals is immune from the impacts of systemic racism, ableism, sexism, and other bias. Sharing strategies to reinvent systems, including recruitment of a diverse research workforce, provision of training in linguistic and cultural competence, incentivizing and prioritizing IDD research designed to address inequities in access to high quality healthcare and education, and in a person-centered framework, is critical for beginning to produce the changes needed in IDD research.
Now is the time to disrupt systems of marginalization, from how ID is framed, how research related to IDD is conducted, and what is prioritized. These ideas are not new, but they are worth repeating and declaring paramount (Jones & Mandell, 2020). Although there is much work to do, an equitable research enterprise for IDD is achievable. It is also the only way research on IDD can meet its goal to serve all those with IDD.
Acknowledgements:
SK acknowledges grant support from the National Institutes of Health (R21 DC017226), as well as conversations with many colleagues, including in the NeuDLL Lab and UW SPHSC. LA acknowledges grant support from the National Institutes of Health (P50HD103526) as well as conversations and interactions with key colleagues, including Janice Enriquez, Michele Ono, Mercedes Piedra, Patrick Dwyer, Susan Rivera, Hendry Ton, Tawara Goode, Angela Thurman, Christine Wu Nordahl, and the MIND Institute Diversity, Equity, and Inclusion Committee.
References
- Abbeduto L, McDuffie A, Thurman A, & Kover ST (2016). Language development in individuals with intellectual and developmental disabilities: From phenotypes to treatments. In Hodapp RM & Fidler D (Eds.), International Review of Research in Developmental Disabilities, pp. 74–118. New York: Academic Press. [Google Scholar]
- Angell A, Empey A, & Zuckerman K (2018). A review of diagnosis and service disparities among children with autism from racial and ethnic minority groups in the United States. International review of research in developmental disabilities, 55, 145–180. [Google Scholar]
- Andrews EE, Forber-Pratt AJ, Mona LR, Lund EM, Pilarski CR, & Balter R (2019). # SaytheWord: A disability culture commentary on the erasure of “disability”. Rehabilitation psychology, 64(2), 111. [DOI] [PubMed] [Google Scholar]
- Atherton G, Edisbury E, Piovesan A, & Cross L (2021). Autism through the ages: A mixed methods approach to understanding how age and age of diagnosis affect quality of life. Journal of Autism and Developmental Disorders, 1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bard KA, Keller H, Ross KM, Hewlett B, Butler L, Boysen ST, & Matsuzawa T (2021). Joint Attention in Human and Chimpanzee Infants in Varied Socio‐Ecological Contexts. Monographs of the Society for Research in Child Development, 86(4), 7–217. [DOI] [PubMed] [Google Scholar]
- Bevan SL, Liu J, Wallis KE, & Pinto-Martin JA (2020). Screening instruments for developmental and behavioral concerns in pediatric Hispanic populations in the United States: a systematic literature review. Journal of Developmental & Behavioral Pediatrics, 41(1), 71–80. [DOI] [PubMed] [Google Scholar]
- Boggs AE, Schmitt LM, McLane RD, Adayev T, LaFauci G, Horn PS, … & Erickson CA. (2022). Optimization, validation and initial clinical implications of a Luminex-based immunoassay for the quantification of Fragile X Protein from dried blood spots. Scientific Reports, 12(1), 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bottema-Beutel K, Kapp SK, Lester JN, Sasson NJ, & Hand BN (2021). Avoiding ableist language: Suggestions for autism researchers. Autism in Adulthood. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown HM, Stahmer AC, Dwyer P, & Rivera S (2021). Changing the story: How diagnosticians can support a neurodiversity perspective from the start. Autism, 25(5), 1171–1174. [DOI] [PubMed] [Google Scholar]
- Buntinx WH, & Schalock RL (2010). Models of disability, quality of life, and individualized supports: Implications for professional practice in intellectual disability. Journal of Policy and Practice in Intellectual Disabilities, 7(4), 283–294. [Google Scholar]
- Callaghan T, & Sylvester S (2019). Autism spectrum disorder, politics, and the generosity of insurance mandates in the United States. PloS one, 14(5), e0217064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camarata S (2022). Balancing Respect for Individuals, Human Rights, Neurodiversity, and Positive Behavioral Support in Intervention Research for a Spectrum of Autistic People. Journal of Speech, Language, and Hearing Research, 65(4), 1607–1609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casanova EL, & Widman CJ (2021). A sociological treatment exploring the medical model in relation to the neurodiversity movement with reference to policy and practice. Evidence & Policy: A Journal of Research, Debate and Practice, 17(2), 363–381. [Google Scholar]
- Castillo W, & Gillborn D How to “QuantCrit:” Practices and Questions for Education Data Researchers and Users. https://www.edworkingpapers.com/sites/default/files/ai22-546.pdf
- Chapman R, & Veit W (2020). Representing the autism spectrum. The American Journal of Bioethics, 20(4), 46–48. [DOI] [PubMed] [Google Scholar]
- Chen M, Nah YH, Waschl N, Poon K, & Chen P (2022). Developing and piloting a computerized adaptive test for a culturally appropriate measure of adaptive behavior. Journal of Psychoeducational Assessment, 40(2), 238–254. [Google Scholar]
- Cooper SM, Hurd NM, & Loyd AB (2022). Advancing scholarship on anti‐racism within developmental science: Reflections on the special section and recommendations for future research. Child Development, 93(3), 619–632. [DOI] [PubMed] [Google Scholar]
- Corbett BA, Muscatello RA, Klemencic ME, West M, Kim A, & Strang JF (2022). Greater gender diversity among autistic children by self-report and parent-report. Autism, 13623613221085337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Constantino JN, Sahin M, Piven J, Rodgers R, Tschida J. The Impact of COVID-19 on Individuals With Intellectual and Developmental Disabilities: Clinical and Scientific Priorities. Am J Psychiatry. 2020. Nov 1;177(11):1091–1093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crenshaw K Demarginalizing the intersection of race and sex: a black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. U. Chi. Legal Forum. 1989; 1989(1):139–167 [Google Scholar]
- Dibble R, & Gibson C (2013). Collaboration for the common good: An examination of challenges and adjustment processes in multicultural collaborations. Journal of Organizational Behavior, 34(6), 764–790. [Google Scholar]
- Dimachkie Nunnally A, Nguyen V, Anglo C, Sterling A, Edgin J, Sherman S, … & Thurman AJ. (2021). Symptoms of autism spectrum disorder in individuals with Down syndrome. Brain sciences, 11(10), 1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donaldson AL (2021). Disability in Speech and Hearing Sciences: Reflections on Representation. Perspectives of the ASHA Special Interest Groups, 6(3), 513–519. [Google Scholar]
- Dwyer P (2022). The Neurodiversity Approach (es): What Are They and What Do They Mean for Researchers?. Human Development, 1–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dwyer P, Ryan JG, Williams ZJ, Gassner DL. First Do No Harm: Suggestions Regarding Respectful Autism Language. Pediatrics. 2022. Apr 1;149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emerson E (2021). Social and Environmental Determinants of Health Among People With Disabilities. In Oxford Research Encyclopedia of Global Public Health. [Google Scholar]
- Fagot B, Rodgers C, & Leinbach MD (2012). Theories of gender socialization. In The developmental social psychology of gender (pp. 79–104). Psychology Press. [Google Scholar]
- Fiscella K, Franks P, Doescher MP, & Saver BG (2002). Disparities in health care by race, ethnicity, and language among the insured: findings from a national sample. Medical care, 52–59. [DOI] [PubMed] [Google Scholar]
- Gallagher DJ, Connor DJ, & Ferri BA (2014). Beyond the far too incessant schism: Special education and the social model of disability. International Journal of Inclusive Education, 18(11), 1120–1142. [Google Scholar]
- Gernsbacher MA (2017). Editorial perspective: The use of person‐first language in scholarly writing may accentuate stigma. Journal of Child Psychology and Psychiatry, 58(7), 859–861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goode TD, Carter-Pokras OD, Horner-Johnson W, & Yee S (2014). Parallel tracks: Reflections on the need for collaborative health disparities research on race/ethnicity and disability. Medical care, 52(10 0 3), S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Habayeb S, Kenworthy L, De La Torre A, & Ratto A (2021). Still Left Behind: Fewer Black School-Aged Youth Receive ASD Diagnoses Compared to White Youth. Journal of Autism and Developmental Disorders, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagerman RJ, Protic D, Rajaratnam A, Salcedo-Arellano MJ, Aydin EY, & Schneider A (2018). Fragile X-associated neuropsychiatric disorders (FXAND). Frontiers in Psychiatry, 9, 564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris JC (2011). Brain and behavior in fragile X syndrome and idiopathic autism. Archives of General Psychiatry 68, 230–231. [DOI] [PubMed] [Google Scholar]
- Helms JE (2006). Fairness is not validity or cultural bias in racial-group assessment: A quantitative perspective. American Psychologist, 61(8), 845. [DOI] [PubMed] [Google Scholar]
- Henrich J, Heine SJ, & Norenzayan A (2010). The weirdest people in the world? Behavioral and Brain Sciences, 33(2–3), 61–83. [DOI] [PubMed] [Google Scholar]
- Ingham B, Clarke L, & James IA (2008). Biopsychosocial case formulation for people with intellectual disabilities and mental health problems: a pilot study of a training workshop for direct care staff. The British Journal of Development Disabilities, 54(106), 41–54. [Google Scholar]
- Jo H, Schieve LA, Rice CE, Yeargin-Allsopp M, Tian LH, Blumberg SJ, … & Boyle CA. (2015). Age at autism spectrum disorder (ASD) diagnosis by race, ethnicity, and primary household language among children with special health care needs, United States, 2009–2010. Maternal and child health journal, 19(8), 1687–1697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones DR, & Mandell DS (2020). To address racial disparities in autism research, we must think globally, act locally. Autism, 24(7), 1587–1589. [DOI] [PubMed] [Google Scholar]
- Kim ET, Franz L, Fannin DK, Howard J, & Maslow G (2021). Educational classifications of autism spectrum disorder and intellectual disability among school‐aged children in North Carolina: Associations with race, rurality, and resource availability. Autism Research, 14(5), 1046–1060. [DOI] [PubMed] [Google Scholar]
- Lakes KD, Kettler RJ, Schmidt J, Haynes M, Feeney-Kettler K, Kamptner L, Swanson J, & Tamm L (2009). The CUIDAR early intervention parent training program for preschoolers at risk for behavioral disorders: An innovative practice for reducing disparities in access to service. Journal of Early Intervention, 31(2), 167–178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leadbitter K, Buckle KL, Ellis C, & Dekker M (2021). Autistic self-advocacy and the neurodiversity movement: Implications for autism early intervention research and practice. Frontiers in Psychology, 782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leigh JP, Grosse SD, Cassady D, Melnikow J, & Hertz-Picciotto I (2016). Spending by California’s Department of Developmental Services for persons with autism across demographic and expenditure categories. PLoS One, 11(3), e0151970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis-Fernández R, Raggio GA, Gorritz M, Duan N, Marcus S, Cabassa LJ, … & Hinton DE. (2013). GAP-REACH: A checklist to assess comprehensive reporting of race, ethnicity, and culture in psychiatric publications. The Journal of nervous and mental disease, 201(10), 860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- London E (2007). The role of the neurobiologist in redefining the diagnosis of autism. Brain Pathology, 17(4), 408–411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- London EB (2014). Categorical diagnosis: a fatal flaw for autism research?. Trends in Neurosciences, 37(12), 683–686. [DOI] [PubMed] [Google Scholar]
- Lukens JR & Eyo UB (2022). Microglia and neurodevelopmental disorders. Annual Review of Neuroscience, 45, 425–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Machalicek W, Strickland-Cohen K, Drew C, & Cohen-Lissman D (2021). Sustaining personal activism: Behavior analysts as antiracist accomplices. Behavior Analysis in Practice, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Machalicek W, O’Reilly M, Beretvas N, Sigafoos J, Lancioni G, Sorrells A, et al. (2008). A review of school-based instructional interventions for students with autism spectrum disorders. Research in Autism Spectrum Disorders, 2, 395–416. [Google Scholar]
- Magaña S, Lopez K, Salkas K et al. A Randomized Waitlist-Control Group Study of a Culturally Tailored Parent Education Intervention for Latino Parents of Children with ASD. J Autism Dev Disord 50, 250–262 (2020). [DOI] [PubMed] [Google Scholar]
- Mandell DS, Ittenbach RF, Levy SE, Pinto-Martin JA. Disparities in diagnoses received prior to a diagnosis of autism spectrum disorder. J Autism Dev Disord. 2007;37(9):1795–1802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mandell DS, Wiggins LD, Carpenter LA, et al. Racial/ethnic disparities in the identification of children with autism spectrum disorders. Am J Public Health. 2009; 99(3):493–498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maye M, Boyd BA, Martínez-Pedraza F, Halladay A, Thurm A, & Mandell DS (2021). Biases, barriers, and possible solutions: Steps towards addressing autism researchers under-engagement with racially, ethnically, and socioeconomically diverse communities. Journal of autism and developmental disorders, 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClimens A. (2003). The organization of difference: People with intellectual disabilities and the social model of disability. Mental retardation, 41(1), 35–46. [DOI] [PubMed] [Google Scholar]
- McClintock K, Hall S, & Oliver C (2003). Risk markers associated with challenging behaviours in people with intellectual disabilities: a meta‐analytic study. Journal of Intellectual Disability Research, 47(6), 405–416. [DOI] [PubMed] [Google Scholar]
- McCoy MS, Liu EY, Lutz AS, & Sisti D (2020). Ethical advocacy across the autism spectrum: Beyond partial representation. The American Journal of Bioethics, 20(4), 13–24. [DOI] [PubMed] [Google Scholar]
- McDonald KE, Gibbons C, Conroy N, & Olick RS (2022). Facilitating the inclusion of adults with intellectual disability as direct respondents in research: Strategies for fostering trust, respect, accessibility and engagement. Journal of Applied Research in Intellectual Disabilities, 35(1), 170–178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meade MA, Mahmoudi E, & Lee SY (2015). The intersection of disability and healthcare disparities: a conceptual framework. Disability and rehabilitation, 37(7), 632–641. 10.3109/09638288.2014.938176 [DOI] [PubMed] [Google Scholar]
- Miller PS, & Levine RL (2013). Avoiding genetic genocide: understanding good intentions and eugenics in the complex dialogue between the medical and disability communities. Genetics in Medicine, 15(2), 95–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milton DE (2012). On the ontological status of autism: the ‘double empathy problem’. Disability & Society, 27(6), 883–887. [Google Scholar]
- Morgan PL, Farkas G, Cook M, Strassfeld NM, Hillemeier MM, Pun WH, & Schussler DL (2017). Are Black children disproportionately overrepresented in special education? A best-evidence synthesis. Exceptional Children, 83(2), 181–198. [Google Scholar]
- Morgan EH, Rodgers R, Tschida J. Addressing the Intersectionality of Race and Disability to Improve Autism Care. Pediatrics. 2022. Apr 1;149(Suppl 4):e2020049437M. Doi: 10.1542/peds.2020-049437M. [DOI] [PubMed] [Google Scholar]
- Miller HL, Thomi M, Patterson RM, & Nandy K (2022). Effects of Intersectionality Along the Pathway to Diagnosis for Autistic Children With and Without Co-occurring Attention Deficit Hyperactivity Disorder in a Nationally-Representative Sample. Journal of Autism and Developmental Disorders, 1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miranda Ojeda R, & San-Juan D (2022). Letter to the Editor Concerning “Evolution and Medical Implications of Neurodiversity: Where Must We Go?”. Journal of Autism and Developmental Disorders, 1–2. [DOI] [PubMed] [Google Scholar]
- Morris MA (2022). Striving Toward Equity in Health Care for People With Communication Disabilities. Journal of Speech, Language, and Hearing Research, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naser SC, Brann KL, & Noltemeyer A (2021). A brief report on the promise of system 2 cues for impacting teacher decision-making in school discipline practices for Black male youth. School Psychology, 36(3), 196. [DOI] [PubMed] [Google Scholar]
- Nelson RH (2021). A critique of the neurodiversity view. Journal of Applied Philosophy, 38(2), 335–347. [Google Scholar]
- Nguy B, Quique YM, Cavanaugh R, & Evans WS (2022). Representation in Aphasia Research: An Examination of US Treatment Studies Published Between 2009 and 2019. American Journal of Speech-Language Pathology, 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onyeador IN, Hudson SKT, & Lewis NA Jr (2021). Moving beyond implicit bias training: Policy insights for increasing organizational diversity. Policy Insights from the Behavioral and Brain Sciences, 8(1), 19–26. [Google Scholar]
- Pierce NP, O’Reilly MF, Sorrells AM et al. Ethnicity Reporting Practices for Empirical Research in Three Autism-Related Journals. J Autism Dev Disord 44, 1507–1519 (2014). [DOI] [PubMed] [Google Scholar]
- Pukki H, Bettin J, Outlaw AG, Hennessy J, Brook K, Dekker M, … & Yoon WH. (2022). Autistic perspectives on the future of clinical autism research. Autism in Adulthood, 4(2), 93–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raghavan R, & Small N (2004). Cultural diversity and intellectual disability. Current Opinion in Psychiatry, 17(5), 371–375. [Google Scholar]
- Ratto AB, Anthony BJ, Kenworthy L, Armour AC, Dudley K, & Anthony LG (2016). Are non-intellectually disabled black youth with ASD less impaired on parent report than their white peers?. Journal of autism and developmental disorders, 46(3), 773–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reilly C (2012). Behavioural phenotypes and special educational needs: is aetiology important in the classroom?. Journal of Intellectual Disability Research, 56(10), 929–946. [DOI] [PubMed] [Google Scholar]
- Roberts SO, Bareket-Shavit C, Dollins FA, Goldie PD, & Mortenson E (2020). Racial inequality in psychological research: Trends of the past and recommendations for the future. Perspectives on psychological science, 15(6), 1295–1309. [DOI] [PubMed] [Google Scholar]
- Robertson J, Raghavan R, Emerson E, Baines S, & Hatton C (2019). What do we know about the health and health care of people with intellectual disabilities from minority ethnic groups in the United Kingdom? A systematic review. Journal of Applied Research in Intellectual Disabilities, 32(6), 1310–1334. [DOI] [PubMed] [Google Scholar]
- Robinson GC, & Norton PC (2019). A decade of disproportionality: A state-level analysis of African American students enrolled in the primary disability category of speech or language impairment. Language, Speech, and Hearing Services in Schools, 50(2), 267–282. [DOI] [PubMed] [Google Scholar]
- Roper RJ, Hawley L, & Goodlett CR (2020). Influence of allelic differences in Down syndrome. Progress in Brain Research, 251, 29–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roy A, Courtenay K, Odiyoor M, Walsh P, Keane S, Biswas A, … & Munir K. (2021). Setting priorities for people with intellectual disability/intellectual developmental disorders across the lifespan: a call to action by the World Psychiatric Association. BJPsych International, 18(3), 54–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabatello M (2018). Precision medicine, health disparities, and ethics: the case for disability inclusion. Genetics in Medicine, 20(4), 397–399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabatello M, Chen Y, Zhang Y, & Appelbaum PS (2019). Disability inclusion in precision medicine research: a first national survey. Genetics in Medicine, 21(10), 2319–2327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt J, Harris B, McClain MB, & Benallie KJ (2022). Evaluating psychometric properties of common autism educational identification measures through a culturally and linguistically responsive lens. Psychology in the Schools. [Google Scholar]
- Schuck RK, Tagavi DM, Baiden KM, Dwyer P, Williams ZJ, Osuna A, … & Vernon TW. (2021). Neurodiversity and Autism Intervention: Reconciling Perspectives Through a Naturalistic Developmental Behavioral Intervention Framework. Journal of Autism and Developmental Disorders, 1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shea LL, Koffer Miller KH, Verstreate K, Tao S, & Mandell D (2021). States’ use of Medicaid to meet the needs of autistic individuals. Health Services Research, 56(6), 1207–1214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherman SL, Kidd SA, Riley C, Berry-Kravis E, Andrews HF, Miller RM, … & Brown WT. (2017). FORWARD: a registry and longitudinal clinical database to study fragile X syndrome. Pediatrics, 139(Supplement_3), S183–S193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shuttleworth-Edwards AB (2016). Generally representative is representative of none: Commentary on the pitfalls of IQ test standardization in multicultural settings. The Clinical Neuropsychologist, 30(7), 975–998. [DOI] [PubMed] [Google Scholar]
- Skiba RJ, Horner RH, Chung CG, Rausch MK, May SL, & Tobin T (2011). Race is not neutral: A national investigation of African American and Latino disproportionality in school discipline. School psychology review, 40(1), 85–107. [Google Scholar]
- Skinner D, & Weisner TS (2007). Sociocultural studies of families of children with intellectual disabilities. Mental Retardation and Developmental Disabilities Research Reviews, 13(4), 302–312. [DOI] [PubMed] [Google Scholar]
- Smith SJ, & Lowrey KA (2017). Applying the universal design for learning framework for individuals with intellectual disability: The future must be now. Intellectual and Developmental Disabilities, 55(1), 48–51. [DOI] [PubMed] [Google Scholar]
- Soriano LDH, Bullard L, Alvarez CH, Thurman AJ, Abbeduto L. Using telehealth-delivered procedures to collect a parent-implemented expressive language sampling narrative task in monolingual and bilingual families with Autism Spectrum Disorder: A pilot study. Front Rehabilit Sci. 2021. Nov;2:716550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stahmer AC, Vejnoska S, Iadarola S, Straiton D, Segovia FR, Luelmo P, Morgan EH, Lee HS, Javed A, Bronstein B, Hochheimer S, Cho E, Aranbarri A, Mandell D, Hassrick EM, Smith T, Kasari C. Caregiver Voices: Cross-Cultural Input on Improving Access to Autism Services. J Racial Ethn Health Disparities. 2019. Aug;6(4):752–773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinbrenner JR, McIntyre N, Rentschler LF, Pearson JN, Luelmo P, Jaramillo ME, Boyd BA, Wong C, Nowell SW, Odom SL, Hume KA. Patterns in reporting and participant inclusion related to race and ethnicity in autism intervention literature: Data from a large-scale systematic review of evidence-based practices. Autism. 2022. Jan 22:13623613211072593. doi: 10.1177/13623613211072593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taverna L, Bornstein MH, Putnick DL, & Axia G (2011). Adaptive behaviors in young children: A unique cultural comparison in Italy. Journal of cross-cultural psychology, 42(3), 445–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tommeras T, & Kjobli J (2017). Family resources and effects on child behavior problem interventions: A cumulative risk approach. Journal of Child and Family Studies, 26(10), 2936–2947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trani JF, Bakhshi P, Bellanca N, Biggeri M, & Marchetta F (2011). Disabilities through the Capability Approach lens: Implications for public policies. Alter, 5(3), 143–157. [Google Scholar]
- Vargas Londono F, Lim N, Barnett MR et al. Training Culturally Diverse Caregivers to Decrease Their Child’s Challenging Behaviors: A Systematic Review and Meta-analysis. J Autism Dev Disord (2022). [DOI] [PubMed] [Google Scholar]
- Waitoller FR, & King Thorius KA (2016). Cross-pollinating culturally sustaining pedagogy and universal design for learning: Toward an inclusive pedagogy that accounts for dis/ability. Harvard Educational Review, 86(3), 366–389. [Google Scholar]
- Wang C, & Burris MA (1997). Photovoice: Concept, methodology, and use for participatory needs assessment. Health Education & Behavior, 24(3), 369–387. [DOI] [PubMed] [Google Scholar]
- Washington HA (2008). Medical Apartheid: The dark history of medical experimentation on black americans from colonial times to the present. New York: Harlem Moon. [Google Scholar]
- Westby C, & Washington KN (2017). Using the International Classification of Functioning, Disability and Health in assessment and intervention of school-aged children with language impairments. Language, Speech, and Hearing Services in Schools, 48(3), 137–152. [DOI] [PubMed] [Google Scholar]
- World Health Organization (WHO Workgroup for development of version of ICF for Children & Youth). (2007). Classification of Functioning, Disability and Health–Children and Youth Version (ICF-CY). Geneva, Switzerland: Author. [Google Scholar]
- Willink A, Assi L, Nieman C, McMahon C, Lin FR, & Reed NS (2021). Alternative Pathways for Hearing Care May Address Disparities in Access. Frontiers in digital health, 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson NJ, Collison J, Feighan SJ, Howie V, Whitehead L, Wiese M, … & Lewis P. (2020). A national survey of nurses who care for people with intellectual and developmental disability. Australian Journal of Advanced Nursing, 37(3), 4–12. [Google Scholar]
- Wilson NJ, & Watson J (2022). Toward a systems-led, biopsychosocial framework to underpin oral health supports: commentary on “Evolution of oral status in adults with intellectual and developmental disabilities: A longitudinal study”(Figueira et al., 2021). Research and Practice in Intellectual and Developmental Disabilities, 1–6. [Google Scholar]
- Zeleke WA, Hughes TL, & Drozda N (2019). Disparities in diagnosis and service access for minority children with ASD in the United States. Journal of autism and developmental disorders, 49(10), 4320–4331. [DOI] [PubMed] [Google Scholar]