

Abstract
Background
Enhancing Local Control (LC) of brain metastases is pivotal for improving overall survival, which makes the prediction of local treatment failure a crucial aspect of treatment planning. Understanding the factors that influence LC of brain metastases is imperative for optimizing treatment strategies and subsequently extending overall survival. Machine learning algorithms may help to identify factors that predict outcomes.
Methods
This paper systematically reviews these factors associated with LC to select candidate predictor features for a practical application of predictive modeling. A systematic literature search was conducted to identify studies in which the LC of brain metastases is assessed for adult patients. EMBASE, PubMed, Web-of-Science, and the Cochrane Database were searched up to December 24, 2020. All studies investigating the LC of brain metastases as one of the endpoints were included, regardless of primary tumor type or treatment type. We first grouped studies based on primary tumor types resulting in lung, breast, and melanoma groups. Studies that did not focus on a specific primary cancer type were grouped based on treatment types resulting in surgery, SRT, and whole-brain radiotherapy groups. For each group, significant factors associated with LC were identified and discussed. As a second project, we assessed the practical importance of selected features in predicting LC after Stereotactic Radiotherapy (SRT) with a Random Forest machine learning model. Accuracy and Area Under the Curve (AUC) of the Random Forest model, trained with the list of factors that were found to be associated with LC for the SRT treatment group, were reported.
Results
The systematic literature search identified 6270 unique records. After screening titles and abstracts, 410 full texts were considered, and ultimately 159 studies were included for review. Most of the studies focused on the LC of the brain metastases for a specific primary tumor type or after a specific treatment type. Higher SRT radiation dose was found to be associated with better LC in lung cancer, breast cancer, and melanoma groups. Also, a higher dose was associated with better LC in the SRT group, while higher tumor volume was associated with worse LC in this group. The Random Forest model predicted the LC of brain metastases with an accuracy of 80% and an AUC of 0.84.
Conclusion
This paper thoroughly examines factors associated with LC in brain metastases and highlights the translational value of our findings for selecting variables to predict LC in a sample of patients who underwent SRT. The prediction model holds great promise for clinicians, offering a valuable tool to predict personalized treatment outcomes and foresee the impact of changes in treatment characteristics such as radiation dose.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12911-024-02579-z.
Keywords: Local control, Brain metastases, SRT dose, Tumor volume, Local control factors
Introduction
Brain metastases represent the most common intracranial tumor in adults [1]. An estimated 20% of all patients with cancer will develop brain metastases [2]. Although brain metastases can occur from any cancer, the three most common primary tumors associated with brain metastases are lung (20–56% of patients), breast (5–20%) and melanoma (7–16%) [3]. Advances in the treatment of primary tumors have led to prolonged life expectancy and therefore increased the probability of developing brain metastases [1]. Although some patients who develop brain metastases remain asymptomatic, many patients show neurological symptoms including headaches, nausea, vomiting, dizziness, focal neurological deficits, epileptic seizures, behavioral changes, and cognitive impairment [3, 4]. The overall prognosis for patients with brain metastases remains poor [5]. Brain metastases account for a disproportionately high percentage of morbidity and mortality among patients with cancer [6], with dismal 2- and 5-year survival rates of 8.1% and 2.4% respectively after diagnosis [3].
Conventional local treatment options for brain metastases include surgical resection, Whole Brain Radiotherapy (WBRT), Stereotactic Radiotherapy (SRT), or a combination of these. Surgery is a treatment option for large metastatic brain lesions [7]. With WBRT, the entire brain, including healthy brain tissue, is irradiated with a fractionated treatment regimen. WBRT used to be the standard of care for multiple brain metastases. Since long-term adverse cognitive decline is a common neurotoxic effect in patients who have undergone WBRT, and SRT has become increasingly available, SRT is currently generally performed to avoid these cognitive side effects of WBRT [8, 9]. Some studies found SRT to be an effective treatment option for patients with multiple brain metastases [10–14]. As per the joint practice guidelines from the European Association of Neuro-Oncology (EANO) and the European Society for Medical Oncology (ESMO), SRT is recommended for patients with a limited number (1–4) of brain metastases and SRT may be considered for patients with a higher number of brain metastases (5–10) with a cumulative tumor volume < 15 ml [191]. SRT to the surgical cavity is a reasonable option for patients with one to two resected brain metastases [15]. The clinical trial of Brown et al. [192] showed that postoperative SRT is a superior alternative to WBRT for patients with a single brain metastasis.
Irrespective of the treatment type, LC of brain metastases remains an important clinical endpoint [16]. LC is defined as the freedom from the development of new lesions within the field treated with SRT or the absence of progression in preexisting metastases [17, 18]. The prediction of the LC of brain metastases after treatment has important practical implications for patients and clinicians. A predictive capability of the treatment outcome of brain metastases may provide a decision tool to clinicians for the effective management of patient care with the most desirable treatment outcome. If LC can be predicted, the treatment plan can be modified to improve LC by, for example, increasing the dose [19]. The complexity of predicting LC post-treatment remains, however, a critical challenge.
Machine learning, which entails a set of tools and structures to acquire information from data [20], has emerged as a promising avenue for predicting treatment outcomes [21, 22]. Machine learning presents important advantages in predictive performance and in the ability to account for complex interactions among inputs while scaling to data sets of very large sizes [23]. These models have shown great success in disease risk predictions based on historical clinical data. Recently, several studies relied on machine learning techniques to predict the response of brain metastases to SRT with high accuracy. Kawahara et al. [19], for instance, proposed a neural network model for predicting the local response of metastatic brain tumors to SRT. The study of Jaberipour et al. [24] investigated the effectiveness of pre-treatment quantitative Magnetic Resonance Imaging (MRI) and clinical features with machine learning techniques to predict local control in patients with brain metastasis treated with SRT. Jalalifar et al. [187] introduced a novel deep learning architecture to predict the LC in brain metastasis treated with SRT using pre-treatment MRI and standard clinical attributes.
However, the complexity of machine learning models and their limited interpretability pose challenges, particularly in biomedical and clinical areas where interpretability is crucial [27]. The inclusion of redundant features for training a machine learning model for the prediction of the local control of brain metastases will also degrade the performance of the model and increase the computation time. Additionally, the inclusion of redundant and irrelevant features reduces the model’s ability to generalize to unseen datasets. Feature selection is a crucial step in minimizing the problem of excessive and irrelevant features and enhancing model interpretability [28]. However, currently, there is lack of insight into the factors influencing local control of brain metastases irrespective of primary tumor types and treatment types. A systematic review of the factors influencing local control may provide the clinical insights needed to select the relevant factors.
Recognizing the importance of understanding the predictors of LC, our paper systematically reviews factors associated with LC of brain metastases. Unlike previous reviews confined to specific primary tumor types or treatment modalities [25, 26], our approach aims to provide a holistic overview of factors associated with LC, encompassing all treatment types, all primary tumor types and all characteristics associated with LC. The comprehensive nature of this review provides the foundation for machine learning model development.
Our study leverages the findings from our comprehensive review to perform feature selection for a Random Forest machine learning algorithm to predict LC specifically for the brain metastases patients treated with SRT group. Experimental results comparing different approaches showed that the Random Forest machine learning algorithm has better prediction performance than logistic regression in approximately 69% of the 243 real datasets [29], including 77 biological datasets, and the experiment compared the prediction performance of the Random Forest algorithm with that of logistic regression for a wide range of prediction outcomes. Also, the Random Forest algorithm performed better than other classification algorithms like support vector machines, K-nearest neighbors, and linear discriminant analysis [30]. Hence, we chose the Random Forest machine learning algorithm to find the importance of the factors and to predict LC for the SRT treatment group.
Our paper strives to bridge the gap between clinical insights and machine learning applications by providing a comprehensive overview of candidate predictors for LC of brain metastases. We use the Random Forest model as an illustrative example, highlighting the potential integration of machine learning in understanding and predicting treatment outcomes. This approach underscores the importance of unraveling predictors to pave the way for future advancements in personalized and effective cancer care.
Methods
Literature search
We conducted this systematic literature review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [190]. A systematic literature search was conducted to identify studies in which the LC of brain metastases was assessed for adult patients. EMBASE, PubMed, Web-of-Science, and the Cochrane Database were searched up to December 24, 2020. Inclusion criteria were studies investigating factors associated with LC of brain metastases. All studies investigating the LC of brain metastases were included irrespective of the primary tumor type. Also, there were no limitations based on the types of treatment.
Eligible studies were research papers, clinical studies, clinical trials, controlled trials, comparative studies, evaluation studies, journal articles, meta-analyses, and case series published since 2010, written in English. Systematic reviews and narrative reviews were also included in the search criteria.
Broad search terms were used to ensure that all studies investigating LC would be covered in the search. The studies were screened to select all those that included LC of brain metastases as an endpoint. Studies that did not have LC as an endpoint were excluded.
The inclusion and exclusion criteria in terms of PICOs (population, intervention, comparison, outcome) are presented in Supplementary Table 1 The search terms are presented in Supplementary Table 2 The inclusion, exclusion, and search terms were built by the first and second authors and reviewed by the other authors.
Study selection
All studies were screened by the first (HK) and second author (WDB) based on title and abstract. The full text was screened if it was unclear from the abstract whether the study met the inclusion criteria. Screening results from both authors were compared and cases of doubt were discussed. Consensus was reached in all cases.
Assessment of included studies
The important factors that were critically reviewed were the aim of the study, primary tumor type, primary and secondary endpoints, treatment type, and the factors associated with the LC of brain metastasis. From the papers that met the inclusion criteria, the significant factors associated with LC were noted. If both univariate and multivariate results were reported, all factors reaching significance in at least one of the two analyses were recorded. We also looked at non-significant univariate factors (neither significant in the univariate analysis nor the multivariate analysis) to report on contradictory findings about the association of a factor across different studies, as some significant factors in some studies might not be significant in others. If the outcome of the analysis was not clear (e.g., direction of the effect was not reported), the corresponding study was excluded.
Presentation of results
We first grouped studies based on primary tumor types. The three groups we created based on the primary tumor types were lung, breast, and melanoma. Studies that did not focus on a specific primary tumor type but included heterogeneous groups of patients with diverse primary cancer types were grouped based on treatment type. The groups we created based on the brain metastases treatment type were a surgery, an SRT, and a WBRT group. The results section visually depicts the significant factors associated with better and worse LC in each group. The factors not associated with LC and the factors for which there are mixed findings are not included in these figures but are added as text in the results section.
In the results section, we combined all results in the same direction for continuous variables like radiation dose, tumor volume, tumor size, and age. For example, some papers mention that a higher dose is associated with better LC whereas others mention that a lower dose is associated with worse LC. In the visual depictions, we have included higher dose under the list of factors associated with better LC and added the reference of all these papers.
Machine learning use case
We retrospectively collected the clinical data from 200 brain metastases patients from the Gamma Knife Center of the Elisabeth-TweeSteden Hospital (ETZ) at Tilburg, The Netherlands. The patients underwent Gamma Knife Radiosurgery (GKRS) at the Gamma Knife Center. This study was approved by the ETZ science office and by the Ethics Review Board at Tilburg University. We aimed to look for data on all the factors identified from the literature for the SRT group. Out of these factors, we collected the data for the variables for which data was available for analysis at ETZ. The patients for whom there was incomplete data for this subset of variables were excluded from the data set. The data were randomly split into training and testing data sets. For the treatment dose, we took the average value from the dose range. Similarly, we took the mean tumor volume across the metastases for patients with more than one brain metastasis. The data was normalized and supplied to the Random Forest classifier. The model was trained with the training data set and then tested with the test data set.
The performance of the model was evaluated by measuring the following metrics: classification accuracy, precision, recall, and Area Under the Receiver Operating Characteristic (ROC) Curve (AUC). The ratio of the number of correct predictions to the total number of input samples determines the accuracy of a machine learning algorithm. The precision is the ratio of true positive predictions to the total number of positive predictions made by the model, while recall is the ratio of true positive predictions to the total number of actual positives in the dataset. ROC is a graphical plot created by plotting the true positive rate vs. the false positive rate at various threshold settings. AUC refers to the area under the ROC curve.
K-fold cross validation was applied to the model. It provides a robust estimate of a model’s performance by partitioning the dataset into k subsets (folds) and iteratively training and evaluating the model on different combinations of training and validation sets. Cross-validation helps in obtaining a more reliable performance metric than a single train-test split. The different values used for K were 3, 5, and 10. The average accuracy, precision, recall and AUC across the different folds was calculated. We also extracted the importance of the various factors for predicting the LC from the trained model.
Results
Selected studies
The systematic literature search identified 6270 unique records (Fig. 1). After screening the title and abstract, 410 full texts were considered, and ultimately 159 studies were included in the review (Fig. 1).
Fig. 1.

PRISMA flowchart of the study selection
Study characteristics
The included 159 studies were heterogeneous, covering a wide range of primary cancer types and were distributed across the different treatment types available for brain metastases. The three groups that we created based on the primary tumor types were melanoma, breast cancer, and lung cancer. The significant factors associated with LC in these groups are presented as flowcharts in Figs. 2, 3, and 4. The different groups that we created based on the treatment types were a surgery, an SRT, and a WBRT group. The significant factors associated with LC in these groups are visually depicted in Figs. 5, 6, and 7. Within these figures, the factors are aggregated based on their characteristic type. The findings per group are discussed below. The studies which did not find any significant factors [31–43] were not included in these groups. Also, comparative studies that did not find any significant factors other than the treatment type [44–54] were not included in these groups and are not further discussed.
Fig. 2.

The factors associated with LC of Lung cancer brain metastases
Fig. 3.
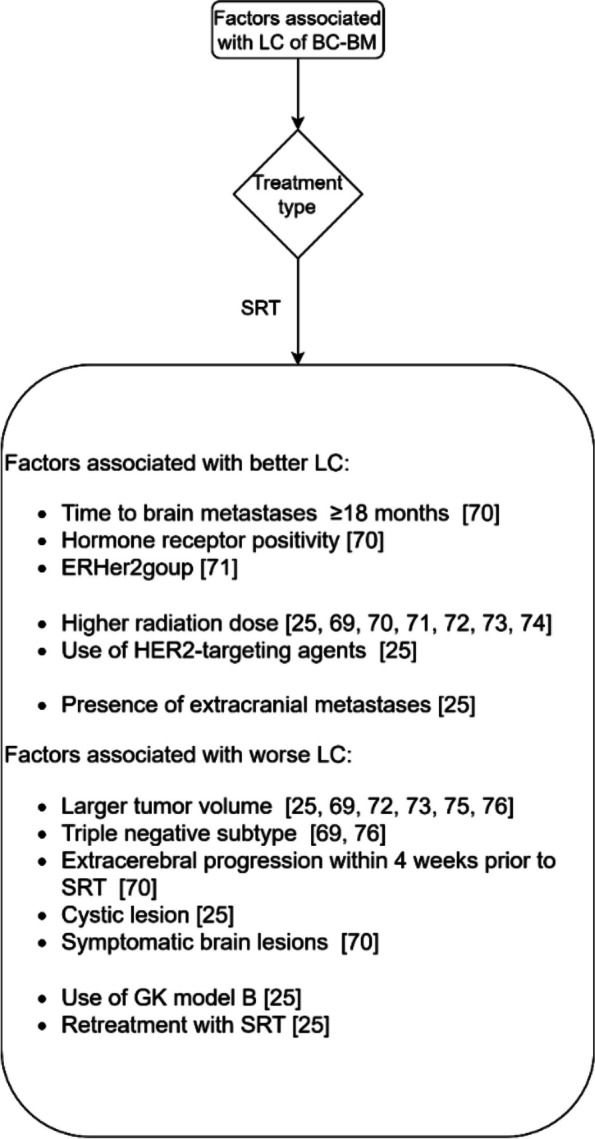
The factors associated with LC of breast cancer brain metastases
Fig. 4.

The factors associated with LC of melanoma brain metastases
Fig. 5.
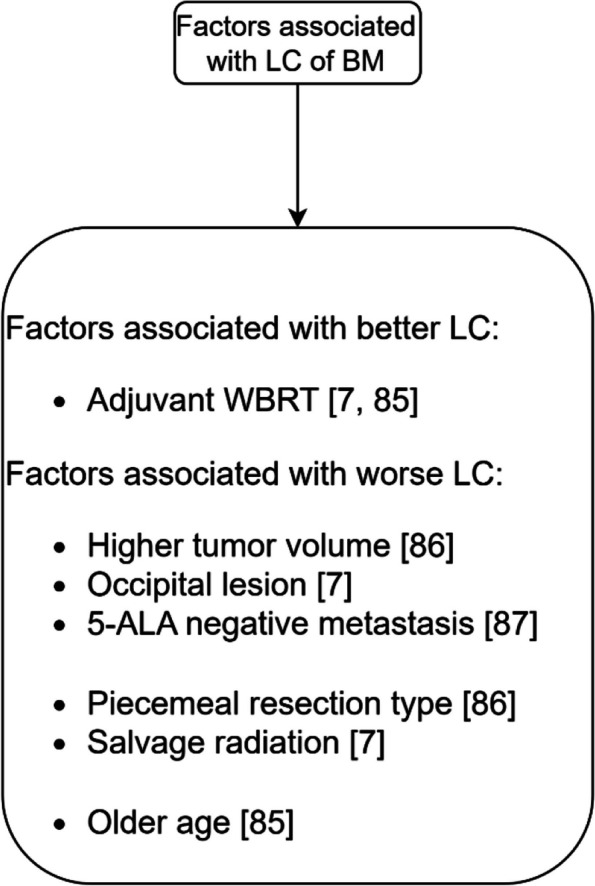
The factors associated with LC after surgery
Fig. 6.

The factors associated with LC after SRT
Fig. 7.

The factors associated with LC after WBRT
Primary tumor histology
Lung cancer brain metastases
Lung cancer is the leading cause of cancer-related death [16]. In addition, lung cancer is the most common malignancy giving rise to brain metastases, accounting for 40 to 60% of all cases of brain metastases [55]. Fig. 2 summarizes the factors associated with the LC of brain metastases from lung cancer. We distinguished the factors for Non-Small Cell Lung Cancer (NSCLC) from those for Small Cell Lung Cancer (SCLC).
NSCLC
The factors associated with LC for brain metastases from NSCLC after treatment with SRT are included in Fig. 2. There are no papers that discuss the LC factors after treatment with WBRT. The factors that were not associated with LC for NSCLC brain metastases after SRT are gender [16, 18, 57, 59, 60], chemotherapy [57, 60], Graded Prognostic Assessment (GPA) score [16, 18], and Recursive Partitioning Analysis (RPA) class [16, 18].
There are also factors for which there are contrasting findings: some studies found them to be associated with LC, whereas others showed that they are not associated with LC. In contrast with the studies reported in Fig. 2, other studies did not find an association with LC for location [16, 18, 60, 83], extracranial metastases [18], Karnofsky Performance Scale (KPS) score [18, 60], prior WBRT [57, 59], tumor volume [57], and prior craniotomy [57].
SCLC
Figure 2 also includes the factors that are associated with LC for brain metastases from SCLC after treatment with SRT or WBRT. In contrast with the study [67] reported in Fig. 2 that suggested that uncontrolled extracranial metastases are associated with worse LC, another study [68] suggested that presence of extracranial metastases are not associated with LC.
Breast cancer brain metastases
Breast Cancer (BC) is the second most common cause of brain metastases in approximately 30% of all women with brain metastases [69]. The incidence of brain metastases appears to be increasing, likely due to earlier diagnosis and prolonged survival with contemporary treatments of BC [69]. Fig. 3 summarizes the factors associated with the LC of brain metastases from BC.
For treatment with SRT, the factors that are not associated with LC are prior WBRT [25, 70, 71, 76], surgery prior to SRT [25, 70, 76], and age [25, 70, 73]. There are mixed findings about the association of Her2 positivity with the LC of brain metastases from BC [70, 71, 74]. There are also mixed findings about the association of the number of metastases with LC [25, 69].
In contrast with the studies reported in Fig. 3, one other study did not find an association with LC for radiation dose [76].
Only one study examined LC for BC brain metastases treated with WBRT. This study reported that a higher KPS score, and higher RPA class are associated with better LC.
Melanoma brain metastases
Thirty-four percent of patients with melanoma developed brain metastases in clinical studies [77]. With a median overall survival of 4.6 months, brain metastases are the leading cause of death in melanoma patients [77]. In addition, the management of melanoma brain metastases remains challenging because of its resistance to radiotherapy and chemotherapies [77].
The factors associated with the LC of melanoma brain metastases are shown in Fig. 4. Gender [81], age [81], location of brain metastases [81], and WBRT [79, 80] do not seem to be associated with LC of melanoma brain metastases after treatment with SRT.
In contrast with the studies reported in Fig. 4, other studies did not find an association with LC for tumor volume [79], tumor size [79], and SRT dose [80, 81] for treatment with SRT. There are mixed findings about the association of BRAF mutation with LC [78, 79, 82].
Treatment type
Surgery
Surgery is a treatment option for large metastatic brain lesions [7]. Fig. 5 summarizes the factors associated with LC after surgery.
The factors that are not associated with LC after surgical resection are gender [86], and KPS score [86].
Stereotactic radiotherapy
Figure 6 summarizes the factors associated with LC after treatment with SRT. The term SRT is used for both single fraction (also called Stereotactic Radiosurgery (SRS)) and fractionated stereotactic radiotherapy. Single fraction SRT (SRS) is a specialized radiation therapy that delivers a single, high dose of radiation directly to the tumor. Fractionated stereotactic radiotherapy delivers multiple, smaller doses of radiation over time. The studies on the factors associated with LC after SRT are sub-grouped into three categories namely: single fraction SRT (SRS), fractionated SRT, and SRT with surgery.
Single fraction SRT(SRS)
The factors that are associated with better LC after SRS are shown in Fig. 6, along with the factors that are associated with worse LC after SRS. The factors that are not associated with LC are chemotherapy [97, 98, 100, 126, 166], primary tumor status [100, 104, 124], GPA [127, 167], systemic treatment [95, 99, 106], time interval from primary tumor diagnosis to brain metastases [100, 110], use of targeted agents [106], energy index [8], DS-GPA [95, 110], and laterality [121, 167].
In contrast with the studies reported in Fig. 6, other studies did not find an association with LC after single fraction SRT (SRS) for dose [89, 102, 124, 125, 127, 166–168], tumor location [97, 98, 105–107, 109, 113, 121, 125, 129, 167], KPS [95, 96, 99, 101, 104, 110, 124, 126, 166, 167], primary tumor type [95–97, 99, 101, 107, 109, 111, 125, 127, 167, 168], tumor volume [8, 98, 100, 102, 104, 112, 128, 166, 167, 169], extracranial metastases [95–97, 99, 100, 166, 167], tumor size [95, 101, 168], WBRT [97, 100, 103, 104, 124], RPA class [95, 96, 100, 167], primary tumor location [105, 110, 117], breast cancer primary tumor type [103], conformity index [102, 119], number of fractions [100], presence of systemic metastases [110], and NSCLC primary tumor type [89].
There are mixed findings about the association of the number of metastases [95–98, 100, 103, 110, 112, 135, 166, 167], Paddick’s conformality index [113, 139, 169], prior WBRT [98, 99, 102, 107, 110, 111, 117, 121, 126, 166, 170], lung cancer primary tumor type [102, 103, 108] and age [89, 90, 95–99, 101–107, 110, 121, 124, 126, 127, 135, 166, 167, 170] with LC. There are also contrasting findings about the association of gender [95, 96, 98–103, 105, 106, 127, 133, 138, 166, 167] and melanoma histology [89, 98, 102, 103, 112, 120, 121, 126, 138] with LC.
Fractionated SRT
The factors that are associated with better LC after treatment with fractionated SRT are shown in Fig. 6. The figure also includes the factors that are associated with worse LC. The factor that is not associated with LC is systemic treatment [140].
There are mixed findings about the association of primary tumor histology with the LC of brain metastases [140, 146]. There are also mixed findings about the association of number of fractions with the LC of brain metastases [147, 171]. In contrast with the studies reported in Fig. 6, other studies did not find an association with LC for dose [158, 172].
SRT with surgery
Figure 6 also includes the factors that are associated with better and worse LC after treatment with SRT after surgery.
The factors that are not associated with LC are gender [150, 160], piecemeal excision [156], radioresistant primary tumor type [160, 163], and the time interval between surgery and SRS [152, 160].
There are mixed findings about the association of GPA score [155, 156] and the margin around the resection cavity [157, 173] with the LC of brain metastases.
In contrast with the studies reported in Fig. 6, other studies did not find a significant association between LC and tumor location [152, 160, 165], histology [150, 156, 165], age [150, 160], residual tumor [150], GPA [150], dose [165], number of metastases [160], tumor volume [165], and tumor size [165].
Whole brain radiation therapy
Figure 7 shows the factors associated with LC of brain metastases after treatment with WBRT. The WBRT treatment group is classified into two subgroups, namely: treatment with WBRT alone, and combination of WBRT with SRT.
In contrast with the studies reported in Fig. 7, other studies did not find an association with LC for age [175–180, 185], gender [174–176, 178–180], extracerebral metastases [174, 177, 179, 180, 185], extracranial metastasis [178], number of metastases [177, 178, 185], the interval from first diagnosis to WBRT [174, 177, 179], KPS [178, 185], primary tumor type [177, 179] and RPA class [185] for treatment with WBRT alone.
Combining WBRT with SRS was found to be associated with better LC when compared to treatment with WBRT alone. For this treatment combination, the factors not associated with LC are age [184], and gender [184].
Summary of results
Higher SRT radiation dose was found to be associated with better LC in lung cancer, breast cancer, and melanoma primary tumor groups. Also, in the SRT group (in which multiple primary tumor types were included), a higher dose was reported to be associated with better LC. Although few studies did not find any association of SRT radiation dose, many studies in the literature suggest that a higher SRT radiation dose is associated with better LC.
Table 1 summarizes the factors for which there is univocal evidence from the literature (meaning there is neither mixed nor contrasting findings) to suggest their association with better LC.
Table 1.
Factors that are associated with better LC
| Primary tumor/treatment group | Factors |
|---|---|
| Lung cancer (NSCLC) | Higher SRT radiation dose, larger conformality index, presence of EGFR mutations |
| Lung cancer (SCLC) | Higher SRT radiation dose |
| Breast cancer | Higher SRT radiation dose |
| Melanoma | Higher SRT radiation dose |
| WBRT | Higher KPS score, breast cancer primary tumor type, WBRT boost |
| SRT | Higher radiation dose, higher KPS score |
| Surgery | Adjuvant WBRT |
On the other hand, higher tumor volume seems to be associated with worse LC in the SRT group. Table 2 summarizes the factors for which there is univocal evidence from the literature to suggest their association with worse LC.
Table 2.
Factors that are associated with worse LC
| Primary tumor/treatment group | Factors |
|---|---|
| Lung cancer (NSCLC) | Larger tumor size, number of radiation shots |
| Breast cancer | Presence of triple-negative breast cancer subtype |
| Melanoma | Presence of intratumoral hemorrhage |
| WBRT | Higher RPA class |
| SRT | Higher tumor volume, larger tumor size, recurrent lesion |
This review showed that some of the significant factors in some studies are found to be non-significant in others. The factors for which there is such mixed evidence of their association with LC are a higher number of brain metastases for the breast cancer group, the presence of extracranial metastases and prior WBRT for the lung cancer group, a larger tumor size for the melanoma group, gender, and number of metastases for WBRT treatment group and prior WBRT, multifraction and number of metastases for SRT group.
Some factors are significant in some studies but found to be non-significant in a higher number of other studies. These factors for which there is only such weak evidence of their association with LC are female gender, older age for the WBRT treatment group, and breast cancer primary type, NSCLC primary tumor histology, a higher number of metastases, melanoma histology, and older age for the SRT group.
Machine learning use case
The list of all factors associated with LC after SRT for brain metastases from a diversity of primary cancers is illustrated in Fig. 6. Out of these factors, the variables for which data was available for analysis at ETZ were age, KPS score, number of brain metastases, average brain metastases volume, primary tumor type, presence of extracranial metastases, average treatment dose, prior WBRT, prior surgery, and prior SRS. The patients with incomplete data for this subset of variables were excluded from the data set. After this filtering, we had 135 patients with complete data. Table 3 summarizes the characteristics of these patients. The patient cohort was randomly partitioned into training and testing datasets, comprising 121 and 14 patients, respectively. A Random Forest model was trained iteratively on the training dataset and evaluated on distinct validation sets within the training data. The assessment of its classification accuracy revealed an average accuracy of 80% across the diverse folds utilized in the cross-validation procedure. The average precision and recall across the folds were 75% and 81.6% respectively. The AUC across the folds is depicted in Fig. 8. The average AUC across the three folds was 0.84. The most important factor as per the algorithm was the tumor volume followed by age and average SRT dose. The presence of prior WBRT was the least significant factor as per the algorithm (Fig. 9).
Table 3.
Patient characteristics
| Age (years) | |
| Average | 63 |
| Minimum | 39 |
| Maximum | 85 |
| Sex | |
| Male | 58 |
| Female | 77 |
| KPS | |
| 60 | 3 |
| 70 | 17 |
| 80 | 32 |
| 90 | 42 |
| 100 | 41 |
| Number of tumors | |
| 1 | 33 |
| 2-3 | 51 |
| 4-10 | 44 |
| >10 | 7 |
| Primary cancer | |
| Lung | 89 |
| Melanoma | 7 |
| Breast | 5 |
| Others | 34 |
| Presence of extracranial metastases | |
| Yes | 61 |
| No | 74 |
| Prior SRS | |
| Yes | 15 |
| No | 120 |
| Prior surgery | |
| Yes | 9 |
| No | 126 |
| Prior WBRT | |
| Yes | 8 |
| No | 127 |
| Tumor volume(mm3) | |
| Average | 16752 |
| Minimum | 88 |
| Maximum | 88029 |
| Average SRS dose(Gy) | |
| Average | 22.018 |
| Minimum | 14 |
| Maximum | 25 |
Fig. 8.

ROC curve for the prediction model
Fig. 9.

Variable importance for LC in decreasing order of significance
Discussion
The aim of this study was to conduct a comprehensive review of factors associated with LC of brain metastases, categorizing them across various primary tumor types and treatment modalities. By systematically analyzing a wide array of literature, we aimed to identify and present factors associated with LC, offering a holistic perspective. Additionally, we explored the translational potential of this knowledge in the context of machine learning, demonstrating its practical utility by applying insights to the stereotactic radiotherapy group.
One hundred and fifty-nine studies were included in the review. All the factors associated with LC of brain metastases were explored without restrictions on the primary tumor types, treatment types and study methodology. Also, we reviewed all the characteristics associated with LC and did not limit them to one type of characteristics, for instance treatment, patient, brain metastases or primary tumor characteristics. The studies were grouped based on primary tumor type. Studies that did not focus on a specific primary tumor type or included heterogeneous groups of patients with different primary cancers were grouped based on treatment type.
The results showed numerous significant factors for each group, underscoring the complexity of LC determinants. Notably, some factors showed significance in certain studies but not in others, highlighting the need for further investigation into factors contributing to these discrepancies, including patient, tumor, and treatment characteristics and their potential interactions. Additionally, differing international guidelines may have contributed to variations in study outcomes. The data from older studies show that a wide variety of SRT doses was used in the past [194, 195]. However, recently, national and international guidelines were developed to increase the homogeneity of the treatment [188, 189, 193]. Despite these recent guidelines, there are still minor differences between dosage guidelines across the countries. For instance, for a tumor with a volume of 20 cm3, the dosage guideline in US and UK is 15 Gy, while in Netherlands it is 18 Gy [188, 189, 193].
To illustrate the practical utility of our findings, we used the factors generally associated with LC for feature selection in a Random Forest machine learning algorithm for the SRT group. The list of factors identified in this review served as an input for us to extract the features for the algorithm. The resulting Random Forest model predicted the LC of brain metastases with an accuracy of 80% and an AUC of 0.84. The neural network model proposed by Kawahara et al. [19] for predicting the local response of metastatic brain tumors to SRT, built with 45 patient samples, provided a prediction accuracy of 78% for the evaluation dataset. The machine learning model trained with the clinical features of 100 patients in the study of Jaberipour et al. [24] reached a prediction accuracy of 63%. The prediction model developed by Jalalifar et al. [187] with clinical features of 99 patients had a prediction accuracy of 67.5%. The higher prediction accuracy of the Random Forest algorithm trained with the features selected from the systematic review utilized in this study suggests that our feature selection could help to increase the prediction accuracy of the machine learning algorithms. This prediction model holds promise for clinicians, offering a valuable tool to predict personalized treatment outcomes and to foresee the impact of changes in treatment characteristics such as dose, and prior brain treatments. As per the algorithm, the most important factor was tumor volume, while presence of prior WBRT was the least important factor.
Understanding the factors associated with LC is crucial, given its link to improved overall survival [186]. Our study advocates extending this approach for the SRT group to the other treatment and primary tumor groups described in this review. This could be the scope of a future study on this topic. Knowing the factors associated with the LC of brain metastases is imperative to predict the overall survival of the patients and in some cases to prolong survival if the factors are controllable. Moreover, the streamlined approach of using the identified factors has the potential to significantly facilitate and enhance efficiency in future machine learning studies, reducing time and computational costs during the data extraction and feature selection process. Limiting the number of features could also improve the interpretability of machine learning algorithms.
A limitation of this study is that we included only the clinical features for training the machine learning algorithm. The addition of imaging features from the pre-treatment MRI scans could increase the prediction performance of the machine learning algorithm. Also, for a more rigorous evaluation of the efficacy and robustness of the models, further investigations should be performed on larger patient cohorts, preferably with multi-institutional data. An external validation data set could also improve the generalizability of the prediction model.
In conclusion, our study expands clinical insights into LC in brain metastases and bridges a gap between traditional clinical understanding and advanced machine learning applications. The identified factors are a foundation for future advancements in predictive modeling and treatment optimization, fostering a more personalized and effective approach to cancer care.
Supplementary Information
Acknowledgements
Not applicable.
Abbreviations
- LC
Local Control
- BM
Brain Metastases
- WBRT
Whole brain radiotherapy
- SRT
Stereotactic radiotherapy
- DC
Distant Control
- OS
Overall Survival
- PFS
Progression-Free Survival
- iPFS
Intracranial Progression-Free Survival
- NSCLC
Non-Small Cell Lung Cancer
- SCLC
Small Cell Lung Cancer
- ECOG
Eastern Cooperative Oncology Group
- RPA class
Recursive Partitioning Analysis
- KPS score
Karnofsky Performance Scale
- GPA score
Graded Prognostic Assessment
- BC
Breast Cancer
- GK
Gamma Knife
- SRS
Stereotactic Radiosurgery
- GTV
Gross Tumor Volume
- PLR
Platelet-to-Lymphocyte Ratio
- ANC/ALC/NLR
Absolute Neutrophil Count/Absolute Lymphocyte Count/ratio
- TT/IT
Targeted or immunotherapy
- MRI
Magnetic resonance imaging
- EANO
European Association of Neuro-Oncology
- ESMO
European Society for Medical Oncology
- ROC
Receiver Operating Characteristic
- AUC
Area Under the Receiver Operating Characteristic Curve
Authors’ contributions
Conceptualization, H.K., W.d.B., K.G., P.H., and M.S.; Methodology, H.K. and W.d.B.; Formal Analysis, H.K.; Writing –Review & Editing, H.K., W.d.B., K.G., D.b.p.E., P.H., and M.S.; Supervision, W.d.B., and M.S.
Funding
This research is supported by KWF Kankerbestrijding and NWO Domain AES, as part of their joint strategic research programme: Technology for Oncology IL. The collaboration project is co-funded by the PPP Allowance made available by Health Holland, Top Sector Life Sciences & Health, to stimulate public-private partnerships.
Availability of data and materials
The data used for this study is available at ETZ and is accessible after approval from the ETZ Science office.
Declarations
Ethics approval and consent to participate
This study is part of the AI in Medical Imaging for novel Cancer User Support (AMICUS) project at Tilburg University. This project is approved by the Ethics Review Board at the Tilburg University.
The data did not contain any identifiable personal information, therefore the need for informed consent to participate was waived by the Institutional Review Board Elisabeth-TweeSteden Hospital (ETZ), Tilburg, The Netherlands (Study number : L1267.2021 - AMICUS).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Hemalatha Kanakarajan, Email: H.Kanakarajan@tilburguniversity.edu.
Margriet Sitskoorn, Email: M.M.Sitskoorn@tilburguniversity.edu.
References
- 1.Donofrio CA, Cavalli A, Gemma M, Riccio L, Donofrio A, Panni P, et al. Cumulative intracranial tumour volume prognostic assessment: a new predicting score index for patients with brain metastases treated by stereotactic radiosurgery. Clin Exp Metastasis. 2020;37:499–508. doi: 10.1007/s10585-020-10037-z. [DOI] [PubMed] [Google Scholar]
- 2.Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol. 2004;22:2865–72. doi: 10.1200/JCO.2004.12.149. [DOI] [PubMed] [Google Scholar]
- 3.Achrol AS, Rennert RC, Anders C, Soffietti R, Ahluwalia MS, Nayak L, et al. Brain metastases. Nat Reviews Disease Primers. 2019;5. [DOI] [PubMed]
- 4.Kaal EC, Niël CG, Vecht CJ. Therapeutic management of brain metastasis. Lancet Neurol. 2005;4:289–98. doi: 10.1016/S1474-4422(05)70072-7. [DOI] [PubMed] [Google Scholar]
- 5.Rastogi K, Bhaskar S, Gupta S, Jain S, Singh D, Kumar P. Palliation of brain metastases: analysis of prognostic factors affecting overall survival. Indian J Palliat Care. 2018;24:308–12. doi: 10.4103/IJPC.IJPC_1_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol. 2005;75:5–14. doi: 10.1007/s11060-004-8093-6. [DOI] [PubMed] [Google Scholar]
- 7.Chahal D, Lee DG, Toyota B. Survival and tumor recurrence in patients with brain metastases treated by surgical resection with or without adjuvant whole brain radiation therapy. J Radiation Oncol. 2015;5:213–9. doi: 10.1007/s13566-015-0242-3. [DOI] [Google Scholar]
- 8.Jani A, Rozenblat T, Yaeh AM, Nanda T, Saad S, Qureshi YH, et al. The energy index does not affect local control of brain metastases treated by Gamma Knife stereotactic radiosurgery. Neurosurgery. 2015;77:119–25. doi: 10.1227/NEU.0000000000000750. [DOI] [PubMed] [Google Scholar]
- 9.Abel RJ, Lederman A, Ji L, Chen T, Zada G, Liu C, et al. Stereotactic radiosurgery to the resection cavity for brain metastases: prognostic factors and outcomes. Int J Radiat Oncol*Biol*Physics. 2014;90:S331. doi: 10.1016/j.ijrobp.2014.05.1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Liu Q, Tong X, Wang J. Management of brain metastases: history and the present. Chin Neurosurgical J. 2019;5. [DOI] [PMC free article] [PubMed]
- 11.Hunter GK, Suh JH, Reuther AM, Vogelbaum MA, Barnett GH, Angelov L, et al. Treatment of five or more brain metastases with stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2012;83:1394–8. doi: 10.1016/j.ijrobp.2011.10.026. [DOI] [PubMed] [Google Scholar]
- 12.Bhatnagar AK, Flickinger JC, Kondziolka D, Lunsford LD. Stereotactic radiosurgery for four or more intracranial metastases. Int J Radiat Oncol*Biol*Physics. 2006;64:898–903. doi: 10.1016/j.ijrobp.2005.08.035. [DOI] [PubMed] [Google Scholar]
- 13.Kim GJ, Buckley E, Herndon JE, Allen K, Dale TS, Adamson J, et al. Outcomes in patients with 4 to 10 brain metastases treated with dose-adapted single-isocenter multitarget stereotactic radiosurgery: a prospective study. Adv Radiation Oncol. 2021;6:100760–0. doi: 10.1016/j.adro.2021.100760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Verhaak E, Schimmel WCM, Gehring K, Emons WHM, Hanssens PEJ, Sitskoorn MM. Health-related quality of life after Gamma Knife radiosurgery in patients with 1–10 brain metastases. J Cancer Res Clin Oncol. 2021;147:1157–67. doi: 10.1007/s00432-020-03400-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vogelbaum MA, Brown PD, Messersmith H, Brastianos PK, Burri S, Cahill D, et al. Treatment for brain metastases: ASCO-SNO-ASTRO Guideline. J Clin Oncol. 2022;40:492–516. doi: 10.1200/JCO.21.02314. [DOI] [PubMed] [Google Scholar]
- 16.Abraham C, Garsa A, Badiyan SN, Drzymala R, Yang D, DeWees T, et al. Internal dose escalation is associated with increased local control for non-small cell lung cancer (NSCLC) brain metastases treated with stereotactic radiosurgery (SRS) Adv Radiation Oncol. 2018;3:146–53. doi: 10.1016/j.adro.2017.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ha IB, Song JH, Jeong BK, Jeong H, Lee YH, Choi HS, et al. The usefulness of stereotactic radiosurgery for recursive partitioning analysis class II/III lung cancer patients with brain metastases in the modern treatment era. Medicine. 2019;98:e17390. doi: 10.1097/MD.0000000000017390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ko PH, Kim HJ, Lee JS, Kim WC. Tumor volume and sphericity as predictors of local control after stereotactic radiosurgery for limited number (1-4) brain metastases from nonsmall cell lung cancer. Asia-Pac J Clin Oncol. 2020;16:165–71. doi: 10.1111/ajco.13309. [DOI] [PubMed] [Google Scholar]
- 19.Kawahara D, Tang X, Lee CK, Nagata Y, Watanabe Y. Predicting the local response of metastatic brain tumor to Gamma Knife Radiosurgery by Radiomics with a machine learning method. Front Oncol. 2020;10:569461. doi: 10.3389/fonc.2020.569461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mendonça MOK, Netto SL, Diniz PSR, Theodoridis S. Chapter 13 - machine learning: review and trends. ScienceDirect. 2024;869–959. https://www.sciencedirect.com/science/article/abs/pii/B9780323917728000193?via%3Dihub.
- 21.Chen M, Hao Y, Hwang K, Wang L, Wang L. Disease prediction by Machine learning over big data from healthcare communities. IEEE Access. 2017;5:8869–79. doi: 10.1109/ACCESS.2017.2694446. [DOI] [Google Scholar]
- 22.Kohli PS, Arora S. Application of Machine Learning, in Disease Prediction, Communication. and Automation (ICCCA). 2018. 10.1109/ccaa.2018.8777449.
- 23.Stevens LM, Mortazavi BJ, Deo RC, Curtis L, Kao DP. Recommendations for reporting machine learning analyses in Clinical Research. Volume 13. Circulation: Cardiovascular Quality and Outcomes; 2020. [DOI] [PMC free article] [PubMed]
- 24.Jaberipour M, Soliman H, Sahgal A, Sadeghi-Naini A. A priori prediction of local failure in brain metastasis after hypo-fractionated stereotactic radiotherapy using quantitative MRI and machine learning. Sci Rep. 2021;11:21620. doi: 10.1038/s41598-021-01024-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Suzuki S, Inoue T, Ishido K. Factors influencing local tumor control after Gamma Knife Radiosurgery for intracranial metastases from breast cancer. J Clin Neurosci. 2016;33:154–8. doi: 10.1016/j.jocn.2016.03.037. [DOI] [PubMed] [Google Scholar]
- 26.Yuan M, Behrami E, Pannullo S, Schwartz TH, Wernicke AG. The relationship between tumor volume and timing of post-resection stereotactic radiosurgery to maximize local control: a critical review. Cureus. 2019;11:e5762. doi: 10.7759/cureus.5762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yu D, Wu H. Variable importance evaluation with personalized odds ratio for machine learning model interpretability with applications to electronic health records-based mortality prediction. Stat Med. 2023. 10.1002/sim.9642. [DOI] [PubMed]
- 28.Pudjihartono N, Fadason T, Kempa-Liehr AW, O’Sullivan JM. A review of feature selection methods for machine learning-based Disease Risk Prediction. Front Bioinf. 2022;2. [DOI] [PMC free article] [PubMed]
- 29.Couronné R, Probst P, Boulesteix A-L. Random forest versus logistic regression: a large-scale benchmark experiment. BMC Bioinformatics. 2018;19. [DOI] [PMC free article] [PubMed]
- 30.Chen R-C, Dewi C, Huang S-W, Caraka RE. Selecting critical features for data classification based on machine learning methods. J Big Data. 2020;7.
- 31.de la Peña C, Guajardo JH, Gonzalez MF, González C, Cruz B. CyberKnife Stereotactic Radiosurgery in brain metastases: a report from Latin America with literature review. Rep Practical Oncol Radiotherapy. 2018;23:161–7. doi: 10.1016/j.rpor.2018.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Fokas E, Henzel M, Engenhart-Cabillic R. A comparison of radiotherapy with radiotherapy plus surgery for brain metastases from urinary bladder cancer. Strahlenther Onkol. 2010;186:565–71. doi: 10.1007/s00066-010-2159-5. [DOI] [PubMed] [Google Scholar]
- 33.Fokas E, Henzel M, Hamm K, Surber G, Kleinert G, Engenhart-Cabillic R. Multidisciplinary treatment of brain metastases derived from colorectal cancer incorporating stereotactic radiosurgery: analysis of 78 patients. Clin Colorectal Cancer. 2011;10:121–5. doi: 10.1016/j.clcc.2011.03.009. [DOI] [PubMed] [Google Scholar]
- 34.Ahmed KA, Abuodeh YA, Echevarria MI, Arrington JA, Stallworth DG, Hogue C, et al. Clinical outcomes of melanoma brain metastases treated with stereotactic radiosurgery and anti-PD-1 therapy, anti-CTLA-4 therapy, BRAF/MEK inhibitors, BRAF inhibitor, or conventional chemotherapy. Annals Oncology: Official J Eur Soc Med Oncol. 2016;27:2288–94. doi: 10.1093/annonc/mdw417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Grandhi R, Kondziolka D, Panczykowski D, Monaco EA, Kano H, Niranjan A, et al. Stereotactic radiosurgery using the Leksell Gamma Knife perfexion unit in the management of patients with 10 or more brain metastases. J Neurosurg. 2012;117:237–45. doi: 10.3171/2012.4.JNS11870. [DOI] [PubMed] [Google Scholar]
- 36.Greto D, Scoccianti S, Compagnucci A, Arilli C, Casati M, Francolini G, et al. Gamma Knife Radiosurgery in the management of single and multiple brain metastases. Clin Neurol Neurosurg. 2016;141:43–7. doi: 10.1016/j.clineuro.2015.12.009. [DOI] [PubMed] [Google Scholar]
- 37.Akyurek S, Chang EL, Mahajan A, Hassenbusch SJ, Allen PK, Mathews LA, et al. Stereotactic radiosurgical treatment of cerebral metastases arising from breast Cancer. Am J Clin Oncol. 2007;30:310–4. doi: 10.1097/01.coc.0000258365.50975.f6. [DOI] [PubMed] [Google Scholar]
- 38.Alphonse-Sullivan N, Taksler GB, Lycan T, Weaver KE, McTyre ER, Shenker RF, et al. Sociodemographic predictors of patients with brain metastases treated with stereotactic radiosurgery. Oncotarget. 2017;8:101005–11. doi: 10.18632/oncotarget.22291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Marcrom SR, Foreman PM, Colvin TB, McDonald AM, Kirkland RS, Popple RA, et al. Focal management of large brain metastases and risk of leptomeningeal disease. Adv Radiat Oncol. 2020;5:34–42. doi: 10.1016/j.adro.2019.07.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Martinage G, Geffrelot J, Stefan D, Bogart E, Rault E, Reyns N et al. Efficacy and tolerance of post-operative hypo-fractionated stereotactic Radiotherapy in a large series of patients with brain metastases. Front Oncol. 2019;9. [DOI] [PMC free article] [PubMed]
- 41.Patel KR, Prabhu RS, Kandula S, Oliver DE, Kim S, Hadjipanayis C, et al. Intracranial control and radiographic changes with adjuvant radiation therapy for resected brain metastases: whole brain radiotherapy versus stereotactic radiosurgery alone. J Neurooncol. 2014;120:657–63. doi: 10.1007/s11060-014-1601-4. [DOI] [PubMed] [Google Scholar]
- 42.Cochran DC, Chan MD, Aklilu M, Lovato JF, Alphonse NK, Bourland JD, et al. The effect of targeted agents on outcomes in patients with brain metastases from renal cell carcinoma treated with Gamma Knife surgery. J Neurosurg. 2012;116:978–83. doi: 10.3171/2012.2.JNS111353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Press RH, Zhang C, Cassidy RJ, Ferris MJ, Zhong J, Steuer CE, et al. Targeted sequencing and intracranial outcomes of patients with lung adenocarcinoma brain metastases treated with radiotherapy. Cancer. 2018;124:3586–95. doi: 10.1002/cncr.31589. [DOI] [PubMed] [Google Scholar]
- 44.Tian L-J, Zhuang H-Q, Yuan Z-Y. A comparison between cyberknife and neurosurgery in solitary brain metastases from non-small cell lung cancer. Clin Neurol Neurosurg. 2013;115:2009–14. doi: 10.1016/j.clineuro.2013.06.006. [DOI] [PubMed] [Google Scholar]
- 45.Hasan S, Shah AH, Bregy A, Albert T, Markoe A, Stoyanova R, et al. The role of whole-brain radiation therapy after stereotactic radiation surgery for brain metastases. Pract Radiat Oncol. 2014;4:306–15. doi: 10.1016/j.prro.2013.09.006. [DOI] [PubMed] [Google Scholar]
- 46.Scheitler-Ring K, Ge B, Petroski G, Biedermann G, Litofsky NS. Radiosurgery to the postoperative Tumor Bed for Metastatic Carcinoma Versus Whole Brain Radiation after surgery. Cureus. 2016;8(11). [DOI] [PMC free article] [PubMed]
- 47.Churilla TM, Chowdhury IH, Handorf E, Collette L, Collette S, Dong Y, et al. Comparison of local control of brain metastases with stereotactic radiosurgery vs surgical resection. JAMA Oncol. 2019;5:243. doi: 10.1001/jamaoncol.2018.4610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kong D-S, Lee J-I, Im Y-S, Nam D-H, Park K, Kim J-H. Differential impact of whole-brain radiotherapy added to radiosurgery for brain metastases. Int J Radiat Oncol*Biol*Physics. 2010;78:385–9. doi: 10.1016/j.ijrobp.2009.08.027. [DOI] [PubMed] [Google Scholar]
- 49.Rades D, Veninga T, Hornung D, Wittkugel O, Schild SE, Gliemroth J. Single brain metastasis: whole-brain irradiation plus either radiosurgery or neurosurgical resection. Cancer. 2011;118:1138–44. doi: 10.1002/cncr.26379. [DOI] [PubMed] [Google Scholar]
- 50.Rades D, Hornung D, Veninga T, Schild SE, Gliemroth J. Single brain metastasis: radiosurgery alone compared with radiosurgery plus up-front whole-brain radiotherapy. Cancer. 2011;118:2980–5. doi: 10.1002/cncr.26612. [DOI] [PubMed] [Google Scholar]
- 51.Minniti G, Salvati M, Muni R, Lanzetta G, Osti MF, Clarke E, et al. Stereotactic radiosurgery plus whole-brain radiotherapy for treatment of multiple metastases from non-small cell lung cancer. Anticancer Res. 2010;30:3055–61. [PubMed] [Google Scholar]
- 52.Rades D, Dziggel L, Janssen S, Khoa M. Predictive Factors for Local Control and survival in patients with Cancer of unknown primary (CUP) irradiated for cerebral metastases. Anticancer Res. 2018;38:2415–18. [DOI] [PubMed]
- 53.OSTHEIMER C, BORMANN C, FIEDLER E, MARSCH W. Malignant melanoma brain metastases: treatment results and prognostic factors - a single-center retrospective study. Int J Oncol. 2015;46:2439–48. doi: 10.3892/ijo.2015.2970. [DOI] [PubMed] [Google Scholar]
- 54.Bougie E, Masson-Côté L, Mathieu D. Comparison between surgical resection and stereotactic radiosurgery in patients with a single brain metastasis from non–small cell lung cancer. World Neurosurg. 2015;83:900–6. doi: 10.1016/j.wneu.2015.01.029. [DOI] [PubMed] [Google Scholar]
- 55.Noel G, Medioni J, Valery C-A, Boisserie G, Simon JM, Cornu P, et al. Three irradiation treatment options including radiosurgery for brain metastases from primary lung cancer. Lung Cancer. 2003;41:333–43. doi: 10.1016/S0169-5002(03)00236-8. [DOI] [PubMed] [Google Scholar]
- 56.Johung KL, Yao X, Li F, Yu JB, Gettinger SN, Goldberg S, et al. A clinical model for identifying radiosensitive tumor genotypes in non–small cell lung cancer. Clin Cancer Res. 2013;19:5523–32. doi: 10.1158/1078-0432.CCR-13-0836. [DOI] [PubMed] [Google Scholar]
- 57.Lee C-C, Hsu SPC, Lin C-J, Wu H-M, Chen Y-W, Luo Y-H, et al. Epidermal growth factor receptor mutations: association with favorable local tumor control following Gamma Knife radiosurgery in patients with non–small cell lung cancer and brain metastases. J Neurosurg. 2020;133:313–20. doi: 10.3171/2019.4.JNS19446. [DOI] [PubMed] [Google Scholar]
- 58.Miller JA, Kotecha R, Ahluwalia MS, Mohammadi AM, Suh JH, Barnett GH, et al. The impact of tumor biology on survival and response to radiation therapy among patients with non–small cell lung cancer brain metastases. Pract Radiat Oncol. 2017;7:e263–73. doi: 10.1016/j.prro.2017.01.001. [DOI] [PubMed] [Google Scholar]
- 59.Garsa AA, Badiyan SN, DeWees T, Simpson JR, Huang J, Drzymala RE, et al. Predictors of individual tumor local control after stereotactic radiosurgery for non-small cell lung cancer brain metastases. Int J Radiat Oncol*Biol*Physics. 2014;90:407–13. doi: 10.1016/j.ijrobp.2014.05.047. [DOI] [PubMed] [Google Scholar]
- 60.Huang C-Y, Lee C-C, Yang H-C, Lin C-J, Wu H-M, Chung W-Y, et al. Radiomics as prognostic factor in brain metastases treated with Gamma Knife radiosurgery. J Neurooncol. 2020;146:439–49. doi: 10.1007/s11060-019-03343-4. [DOI] [PubMed] [Google Scholar]
- 61.Yomo S, Oda K. Impacts of EGFR-mutation status and EGFR-TKI on the efficacy of stereotactic radiosurgery for brain metastases from non-small cell lung adenocarcinoma: a retrospective analysis of 133 consecutive patients. Lung Cancer. 2018;119:120–6. doi: 10.1016/j.lungcan.2018.03.013. [DOI] [PubMed] [Google Scholar]
- 62.Ishihara T, Yamada K, Harada A, Isogai K, Tonosaki Y, Demizu Y, et al. Hypofractionated stereotactic radiotherapy for brain metastases from lung cancer. Strahlenther Onkol. 2016;192:386–93. doi: 10.1007/s00066-016-0963-2. [DOI] [PubMed] [Google Scholar]
- 63.Matsuyama T, Kogo K, Oya N. Clinical outcomes of biological effective dose-based fractionated stereotactic radiation therapy for metastatic brain tumors from non-small cell lung cancer. Int J Radiat Oncol*Biol*Physics. 2013;85:984–90. doi: 10.1016/j.ijrobp.2012.09.008. [DOI] [PubMed] [Google Scholar]
- 64.Badiyan SN, Ferraro DJ, Yaddanapudi S, Drzymala RE, Lee AY, Silver SA, et al. Impact of time of day on outcomes after stereotactic radiosurgery for non-small cell lung cancer brain metastases. Cancer. 2013;119:3563–9. doi: 10.1002/cncr.28237. [DOI] [PubMed] [Google Scholar]
- 65.Rava P, Sioshansi S, DiPetrillo T, Cosgrove R, Melhus C, Wu J, et al. Local recurrence and survival following stereotactic radiosurgery for brain metastases from small cell lung cancer. Pract Radiat Oncol. 2015;5:e37–44. doi: 10.1016/j.prro.2014.03.006. [DOI] [PubMed] [Google Scholar]
- 66.Kuremsky JG, Urbanic JJ, Petty WJ, Lovato JF, Bourland JD, Tatter SB, et al. Tumor histology predicts patterns of failure and survival in patients with brain metastases from lung cancer treated with Gamma Knife Radiosurgery. Neurosurgery. 2013;73:641–7. doi: 10.1227/NEU.0000000000000072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Suzuki R, Wei X, Allen PK, Welsh JW, Cox JD, Komaki R et al. Outcomes of re-irradiation for brain recurrence after prophylactic or therapeutic whole-brain irradiation for small cell lung Cancer: a retrospective analysis. Radiat Oncol. 2018;13. [DOI] [PMC free article] [PubMed]
- 68.Bohlen G, Meyners T, Kieckebusch S, Lohynska R, Veninga T, Stalpers LJA, et al. Short-course whole-brain radiotherapy (WBRT) for brain metastases due to small-cell lung cancer (SCLC) Clin Neurol Neurosurg. 2010;112:183–7. doi: 10.1016/j.clineuro.2009.11.004. [DOI] [PubMed] [Google Scholar]
- 69.Yang TJ, Oh JH, Folkert MR, Gupta G, Shi W, Zhang Z, et al. Outcomes and prognostic factors in women with 1 to 3 breast cancer brain metastases treated with definitive stereotactic radiosurgery. Int J Radiat Oncol*Biol*Physics. 2014;90:518–25. doi: 10.1016/j.ijrobp.2014.06.063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Weykamp F, El Shafie RA, König L, Seidensaal K, Forster T, Arians N et al. Validation of nine different prognostic grading indexes for Radiosurgery of Brain metastases in breast Cancer patients and development of an All-Encompassing Prognostic Tool. Front Oncol. 2020;10. [DOI] [PMC free article] [PubMed]
- 71.Armstrong K, Ward J, Dunne M, Rock L, Westrup J, Mascott CR et al. Linac-based radiosurgery for patients with brain oligometastases from a breast primary, in the Trastuzumab era-impact of Tumor phenotype and prescribed SRS dose. Front Oncol. 2019;9. [DOI] [PMC free article] [PubMed]
- 72.Yomo S, Hayashi M, Cho N. Impacts of HER2-overexpression and molecular targeting therapy on the efficacy of stereotactic radiosurgery for brain metastases from breast cancer. J Neurooncol. 2013;112:199–207. doi: 10.1007/s11060-013-1046-1. [DOI] [PubMed] [Google Scholar]
- 73.Matsunaga S, Shuto T, Kawahara N, Suenaga J, Inomori S, Fujino H. Gamma Knife surgery for metastatic brain tumors from primary breast cancer: treatment indication based on number of tumors and breast cancer phenotype. J Neurosurg. 2010;113(SpecialSupplement):65–72. doi: 10.3171/2010.8.GKS10932. [DOI] [PubMed] [Google Scholar]
- 74.Radawski JD, Zhang D, Nelson A, Grecula JC, Mayr NA, Gupta N, et al. Her2-enriched breast cancer brain metastases exhibit resistance to Gamma Knife radiosurgery: findings from a single institutional series review. J Radiation Oncol. 2012;1:283–90. doi: 10.1007/s13566-012-0026-y. [DOI] [Google Scholar]
- 75.Choi SW, Kwon DH, Kim CJ. Clinical outcome in Gamma Knife Radiosurgery for metastatic brain tumors from the primary breast cancer: prognostic factors in local treatment failure and survival. J Korean Neurosurg Soc. 2013;54:329. doi: 10.3340/jkns.2013.54.4.329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Resende Salgado L, Smith AW, Nehlsen A, Cohen A, Tseng T-C, Lin J-Y, et al. Biologic subtypes as a predictor of local control in patients with brain metastases from breast cancer after stereotactic radiosurgery. J Radiation Oncol. 2020;9:67–73. doi: 10.1007/s13566-020-00424-0. [DOI] [Google Scholar]
- 77.Hadi I, Roengvoraphoj O, Bodensohn R, Hofmaier J, Niyazi M, Belka C et al. Stereotactic radiosurgery combined with targeted/ immunotherapy in patients with melanoma brain metastasis. Radiat Oncol. 2020;15. [DOI] [PMC free article] [PubMed]
- 78.Kotecha R, Miller JA, Venur VA, Mohammadi AM, Chao ST, Suh JH, et al. Melanoma brain metastasis: the impact of stereotactic radiosurgery, BRAF mutational status, and targeted and/or immune-based therapies on treatment outcome. J Neurosurg. 2018;129:50–9. doi: 10.3171/2017.1.JNS162797. [DOI] [PubMed] [Google Scholar]
- 79.Gallaher IS, Watanabe Y, DeFor TE, Dusenbery KE, Lee CK, Hunt MA et al. BRAF Mutation is Associated with Improved Local Control of Melanoma Brain Metastases Treated with Gamma Knife Radiosurgery. Front Oncol. 2016;6. [DOI] [PMC free article] [PubMed]
- 80.Frakes JM, Figura NB, Ahmed KA, Juan T-H, Patel N, Latifi K, et al. Potential role for LINAC-based stereotactic radiosurgery for the treatment of 5 or more radioresistant melanoma brain metastases. J Neurosurg. 2015;123:1261–7. doi: 10.3171/2014.12.JNS141919. [DOI] [PubMed] [Google Scholar]
- 81.Matsunaga S, Shuto T, Yamamoto M, Yomo S, Kondoh T, Kobayashi T, et al. Gamma Knife Radiosurgery for metastatic brain tumors from malignant melanomas: a Japanese Multi-institutional Cooperative and Retrospective Cohort Study (JLGK1501) Stereotact Funct Neurosurg. 2018;96:162–71. doi: 10.1159/000489948. [DOI] [PubMed] [Google Scholar]
- 82.Fang P, Boehling NS, Koay EJ, Bucheit AD, Jakob JA, Settle SH, et al. Melanoma brain metastases harboring BRAF V600K or NRAS mutations are associated with an increased local failure rate following conventional therapy. J Neurooncol. 2017;137:67–75. doi: 10.1007/s11060-017-2695-2. [DOI] [PubMed] [Google Scholar]
- 83.Rades D, Heisterkamp C, Huttenlocher S, Bohlen G, Dunst J, Haatanen T, et al. Dose escalation of whole-brain radiotherapy for brain metastases from melanoma. Int J Radiat Oncol*Biol*Physics. 2010;77:537–41. doi: 10.1016/j.ijrobp.2009.05.001. [DOI] [PubMed] [Google Scholar]
- 84.Diao K, Bian SX, Routman DM, Yu C, Kim PE, Wagle NA, et al. Combination ipilimumab and radiosurgery for brain metastases: tumor, edema, and adverse radiation effects. J Neurosurg. 2018;129:1397–406. doi: 10.3171/2017.7.JNS171286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.McPherson CM, Suki D, Feiz-Erfan I, Mahajan A, Chang E, Sawaya R, et al. Adjuvant whole-brain radiation therapy after surgical resection of single brain metastases. Neurooncology. 2010;12:711–9. doi: 10.1093/neuonc/noq005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Patel AJ, Suki D, Hatiboglu MA, Abouassi H, Shi W, Wildrick DM, et al. Factors influencing the risk of local recurrence after resection of a single brain metastasis. J Neurosurg. 2010;113:181–9. doi: 10.3171/2009.11.JNS09659. [DOI] [PubMed] [Google Scholar]
- 87.Kamp MA, Fischer I, Bühner J, Turowski B, Cornelius JF, Steiger H-J, et al. 5-ALA fluorescence of cerebral metastases and its impact for the local-in-brain progression. Oncotarget. 2016;7:66776–89. doi: 10.18632/oncotarget.11488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Yomo S, Hayashi M. The efficacy and limitations of stereotactic radiosurgery as a salvage treatment after failed whole brain radiotherapy for brain metastases. J Neurooncol. 2013;113:459–65. doi: 10.1007/s11060-013-1138-y. [DOI] [PubMed] [Google Scholar]
- 89.Cummings M, Youn P, Bergsma DP, Usuki KY, Walter K, Sharma M, et al. Single-fraction radiosurgery using conservative doses for brain metastases: durable responses in select primaries with limited toxicity. Neurosurgery. 2017;83:437–44. doi: 10.1093/neuros/nyx427. [DOI] [PubMed] [Google Scholar]
- 90.Black PJ, Page BR, Lucas JT, Hughes RT, Laxton AW, Tatter SB, et al. Factors that determine local control with gamma knife radiosurgery: the role of primary histology. J Radiosurg SBRT. 2015;3:281–6. [PMC free article] [PubMed] [Google Scholar]
- 91.Skeie BS, Enger PØ, Ganz JC, Skeie GO, Parr E, Hatteland S, et al. Gamma Knife surgery of colorectal brain metastases: a high prescription dose of 25 gy may improve growth control. World Neurosurg. 2013;79:525–36. doi: 10.1016/j.wneu.2011.09.019. [DOI] [PubMed] [Google Scholar]
- 92.Ogino A, Hirai T, Serizawa T, Yoshino A. Gamma Knife surgery for brain metastases from uterine malignant tumor. World Neurosurg. 2020;139:e363–72. doi: 10.1016/j.wneu.2020.03.225. [DOI] [PubMed] [Google Scholar]
- 93.Murovic J, Ding V, Han SS, Adler JR, Chang SD. Impact of CyberKnife Radiosurgery on overall survival and various parameters of patients with 1–3 versus ≥ 4 brain metastases. Cureus. 2017;9(10). [DOI] [PMC free article] [PubMed]
- 94.Shaverdian N, Wang J, Levin-Epstein R, Schaue D, Kupelian P, Lee P, et al. Pro-inflammatory state portends poor outcomes with stereotactic radiosurgery for brain metastases. Anticancer Res. 2016;36:5333–8. doi: 10.21873/anticanres.11106. [DOI] [PubMed] [Google Scholar]
- 95.Lucia F, Key S, Dissaux G, Goasduff G, Lucia A-S, Ollivier L, et al. Inhomogeneous tumor dose distribution provides better local control than homogeneous distribution in stereotactic radiotherapy for brain metastases. Radiother Oncol. 2019;130:132–8. doi: 10.1016/j.radonc.2018.06.039. [DOI] [PubMed] [Google Scholar]
- 96.Rades D, Hornung D, Blanck O, Martens K, Khoa MT, Trang NT, et al. Stereotactic radiosurgery for newly diagnosed brain metastases. Strahlenther Onkol. 2014;190:786–91. doi: 10.1007/s00066-014-0625-1. [DOI] [PubMed] [Google Scholar]
- 97.Sayan M, Zoto Mustafayev T, Sahin B, Kefelioglu ESS, Wang S-J, Kurup V, et al. Evaluation of response to stereotactic radiosurgery in patients with radioresistant brain metastases. Radiat Oncol J. 2019;37:265–70. doi: 10.3857/roj.2019.00409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Trifiletti DM, Lee C-C, Kano H, Cohen J, Janopaul-Naylor J, Alonso-Basanta M, et al. Stereotactic radiosurgery for brainstem metastases: an international cooperative study to define response and toxicity. Int J Radiat Oncol*Biol*Physics. 2016;96:280–8. doi: 10.1016/j.ijrobp.2016.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Zhang L, Hu Y, Chen W, Tian Y, Xie Y, Chen J. Pre-stereotactic radiosurgery neutrophil-to-lymphocyte ratio is a predictor of the prognosis for brain metastases. J Neurooncol. 2020;147:691–700. doi: 10.1007/s11060-020-03477-w. [DOI] [PubMed] [Google Scholar]
- 100.Blamek S, Stankiewicz M, Maciejewski B. Clinical and volumetric predictors of local control after robotic stereotactic radiosurgery for cerebral metastases: active systemic disease may affect local control in the brain. Radiol Oncol. 2020;55:82–7. doi: 10.2478/raon-2020-0065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Huang J, Milchenko M, Rao YJ, LaMontagne P, Abraham C, Robinson CG, et al. A feasibility study to evaluate early treatment response of brain metastases one week after stereotactic radiosurgery using perfusion weighted imaging. PLoS ONE. 2020;15:e0241835. doi: 10.1371/journal.pone.0241835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Prabhu RS, Dhabaan A, Hall WA, Ogunleye T, Crocker I, Curran WJ, et al. Clinical outcomes for a novel 6 degrees of freedom image guided localization method for frameless radiosurgery for intracranial brain metastases. J Neurooncol. 2013;113:93–9. doi: 10.1007/s11060-013-1093-7. [DOI] [PubMed] [Google Scholar]
- 103.Luther N, Kondziolka D, Kano H, Mousavi SH, Engh JA, Niranjan A, et al. Predicting tumor control after resection bed radiosurgery of brain metastases. Neurosurgery. 2013;73:1001–6. doi: 10.1227/NEU.0000000000000148. [DOI] [PubMed] [Google Scholar]
- 104.Lee SR, Oh JY, Kim S-H. Gamma Knife radiosurgery for cystic brain metastases. Br J Neurosurg. 2015;30:43–8. doi: 10.3109/02688697.2015.1039489. [DOI] [PubMed] [Google Scholar]
- 105.Matsunaga S, Shuto T, Kawahara N, Suenaga J, Inomori S, Fujino H. Gamma Knife surgery for brain metastases from colorectal cancer. J Neurosurg. 2011;114:782–9. doi: 10.3171/2010.9.JNS10354. [DOI] [PubMed] [Google Scholar]
- 106.Matsunaga S, Shuto T, Kobayashi N. Gamma Knife Radiosurgery for metastatic brain tumors from cancer of unknown primary. World Neurosurg. 2019;122:e1465–71. doi: 10.1016/j.wneu.2018.11.086. [DOI] [PubMed] [Google Scholar]
- 107.Matsunaga S, Shuto T, Sato M. Gamma Knife surgery for metastatic brain tumors from gynecologic cancer. World Neurosurg. 2016;89:455–63. doi: 10.1016/j.wneu.2016.01.062. [DOI] [PubMed] [Google Scholar]
- 108.Romano KD, Trifiletti DM, Garda A, Xu Z, Schlesinger D, Watkins WT, et al. Choosing a prescription isodose in stereotactic radiosurgery for brain metastases: implications for local control. World Neurosurg. 2017;98:761–e7671. doi: 10.1016/j.wneu.2016.11.038. [DOI] [PubMed] [Google Scholar]
- 109.Kim I-Y, Jung S, Jung T-Y, Moon K-S, Jang W-Y, Park J-Y, et al. Repeat stereotactic radiosurgery for recurred metastatic brain tumors. J Korean Neurosurg Soc. 2018;61:633–9. doi: 10.3340/jkns.2017.0238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Paudel N, Helenowski I, Kane L, Sachdev S, Bloch O, Tate M, et al. Stereotactic radiosurgery for the treatment of brain metastasis from gastrointestinal primary cancers. J Radiosurgery SBRT. 2019;6:27–34. [PMC free article] [PubMed] [Google Scholar]
- 111.Wolf A, Kvint S, Chachoua A, Pavlick A, Wilson M, Donahue B, et al. Toward the complete control of brain metastases using surveillance screening and stereotactic radiosurgery. J Neurosurg. 2018;128:23–31. doi: 10.3171/2016.10.JNS161036. [DOI] [PubMed] [Google Scholar]
- 112.Amsbaugh MJ, Yusuf MB, Gaskins J, Dragun AE, Dunlap N, Guan T, et al. A dose–volume response model for brain metastases treated with frameless single-fraction robotic radiosurgery: seeking to better predict response to treatment. Technol Cancer Res Treat. 2016;16:344–51. doi: 10.1177/1533034616685025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Mohammadi AM, Schroeder JL, Angelov L, Chao ST, Murphy ES, Yu JS, et al. Impact of the radiosurgery prescription dose on the local control of small (2 cm or smaller) brain metastases. J Neurosurg. 2017;126:735–43. doi: 10.3171/2016.3.JNS153014. [DOI] [PubMed] [Google Scholar]
- 114.Trifiletti DM, Hill C, Cohen-Inbar O, Xu Z, Sheehan JP. Stereotactic radiosurgery for small brain metastases and implications regarding management with systemic therapy alone. J Neurooncol. 2017;134:289–96. doi: 10.1007/s11060-017-2519-4. [DOI] [PubMed] [Google Scholar]
- 115.Han JH, Kim DG, Chung H-T, Paek SH, Park C-K, Kim C-Y, et al. Stereotactic radiosurgery for brain metastases from hepatocellular carcinoma. J Neurooncol. 2013;115:45–51. doi: 10.1007/s11060-013-1192-5. [DOI] [PubMed] [Google Scholar]
- 116.Amsbaugh M, Pan J, Yusuf MB, Dragun A, Dunlap N, Guan T et al. Dose-volume response relationship for Brain metastases treated with Frameless single-fraction Linear Accelerator-based stereotactic radiosurgery. Cureus. 2016;8(4). [DOI] [PMC free article] [PubMed]
- 117.de Azevedo Santos TR, Tundisi CF, Ramos H, Maia MAC, Pellizzon ACA, Silva MLG et al. Local control after radiosurgery for brain metastases: predictive factors and implications for clinical decision. Radiat Oncol. 2015;10. [DOI] [PMC free article] [PubMed]
- 118.Klausner G, Troussier I, Biau J, Jacob J, Schernberg A, Canova C-H, et al. Stereotactic radiation therapy for renal cell carcinoma brain metastases in the tyrosine kinase inhibitors era: outcomes of 120 patients. Clin Genitourin Cancer. 2019;17:191–200. doi: 10.1016/j.clgc.2019.02.007. [DOI] [PubMed] [Google Scholar]
- 119.Baschnagel AM, Meyer KD, Chen PY, Krauss DJ, Olson RE, Pieper DR, et al. Tumor volume as a predictor of survival and local control in patients with brain metastases treated with Gamma Knife surgery. J Neurosurg. 2013;119:1139–44. doi: 10.3171/2013.7.JNS13431. [DOI] [PubMed] [Google Scholar]
- 120.Minniti G, Scaringi C, Paolini S, Clarke E, Cicone F, Esposito V, et al. Repeated stereotactic radiosurgery for patients with progressive brain metastases. J Neurooncol. 2015;126:91–7. doi: 10.1007/s11060-015-1937-4. [DOI] [PubMed] [Google Scholar]
- 121.Sia J, Paul E, Dally M, Ruben J. Stereotactic radiosurgery for 318 brain metastases in a single Australian centre: the impact of histology and other factors. J Clin Neurosci. 2015;22:303–7. doi: 10.1016/j.jocn.2014.07.019. [DOI] [PubMed] [Google Scholar]
- 122.Seastone DJ, Elson P, Garcia JA, Chao ST, Suh JH, Angelov L, et al. Clinical outcome of stereotactic radiosurgery for central nervous system metastases from renal cell carcinoma. Clin Genitourin Cancer. 2014;12:111–6. doi: 10.1016/j.clgc.2013.10.001. [DOI] [PubMed] [Google Scholar]
- 123.Leeman JE, Flickinger JC, Clump DA, Wegner RE, Heron DE, Burton SA, et al. Detection and treatment of small brain metastases resulting from renal cell carcinoma predict improved survival after stereotactic radiosurgery. J Radiation Oncol. 2012;1:381–7. doi: 10.1007/s13566-012-0060-9. [DOI] [Google Scholar]
- 124.Roh TH, Choi MS, You N, Jeong D, Jang AH, Seo MR, et al. Identifying candidates for gamma knife radiosurgery among elderly patients with brain metastases. J Neurooncol. 2018;137:559–65. doi: 10.1007/s11060-018-2745-4. [DOI] [PubMed] [Google Scholar]
- 125.Follwell MJ, Khu KJ, Cheng L, Xu W, Mikulis DJ, Millar B-A, et al. Volume specific response criteria for brain metastases following salvage stereotactic radiosurgery and associated predictors of response. Acta Oncol. 2012;51:629–35. doi: 10.3109/0284186X.2012.681066. [DOI] [PubMed] [Google Scholar]
- 126.Lwu S, Goetz P, Monsalves E, Aryaee M, Ebinu J, Laperriere N, et al. Stereotactic radiosurgery for the treatment of melanoma and renal cell carcinoma brain metastases. Oncol Rep. 2012;29:407–12. doi: 10.3892/or.2012.2139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Acker G, Hashemi S-M, Fuellhase J, Kluge A, Conti A, Kufeld M et al. Efficacy and safety of CyberKnife radiosurgery in elderly patients with brain metastases: a retrospective clinical evaluation. Radiat Oncol. 2020;15. [DOI] [PMC free article] [PubMed]
- 128.Kawabe T, Yamamoto M, Sato Y, Barfod BE, Urakawa Y, Kasuya H, et al. Gamma Knife surgery for patients with brainstem metastases. J Neurosurg. 2012;117(Special_Suppl):23–30. doi: 10.3171/2012.7.GKS12977. [DOI] [PubMed] [Google Scholar]
- 129.Voong KR, Farnia B, Wang Q, Luo D, McAleer MF, Rao G, et al. Gamma knife stereotactic radiosurgery in the treatment of brainstem metastases: the MD Anderson experience. Neuro-Oncol Pract. 2015;2:40–7. doi: 10.1093/nop/npu032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Wardak Z, Christie A, Bowman A, Stojadinovic S, Nedzi L, Barnett S, et al. Stereotactic radiosurgery for multiple brain metastases from renal-cell carcinoma. Clin Genitourin Cancer. 2019;17:e273–80. doi: 10.1016/j.clgc.2018.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Yomo S, Hayashi M. Is upfront stereotactic radiosurgery a rational treatment option for very elderly patients with brain metastases? A retrospective analysis of 106 consecutive patients age 80 years and older. BMC Cancer. 2016;16. [DOI] [PMC free article] [PubMed]
- 132.Likhacheva A, Pinnix C, Parikh N, Allen P. Predictors of survival in contemporary practice after initial radiosurgery for brain metastases. Int J Radiat Oncol*Biol*Physics. 2013;85:656–61. doi: 10.1016/j.ijrobp.2012.05.047. [DOI] [PubMed] [Google Scholar]
- 133.Bilger A, Frenzel F, Oehlke O, Wiehle R, Milanovic D, Prokic V, et al. Local control and overall survival after frameless radiosurgery: a single center experience. Clin Transl Radiat Oncol. 2017;7:55–61. doi: 10.1016/j.ctro.2017.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Koffer P, Chan J, Rava P, Gorovets D, Ebner D, Savir G, et al. Repeat stereotactic radiosurgery for locally recurrent brain metastases. World Neurosurg. 2017;104:589–93. doi: 10.1016/j.wneu.2017.04.103. [DOI] [PubMed] [Google Scholar]
- 135.Juloori A, Miller JA, Parsai S, Kotecha R, Ahluwalia MS, Mohammadi AM, et al. Overall survival and response to radiation and targeted therapies among patients with renal cell carcinoma brain metastases. J Neurosurg. 2020;132:188–96. doi: 10.3171/2018.8.JNS182100. [DOI] [PubMed] [Google Scholar]
- 136.Almeida-Freitas DB, Pinho MC, Otaduy MCG, Braga HF, Meira-Freitas D, da Costa Leite C. Assessment of irradiated brain metastases using dynamic contrast-enhanced magnetic resonance imaging. Neuroradiology. 2014;56(6):437–43. doi: 10.1007/s00234-014-1344-0. [DOI] [PubMed] [Google Scholar]
- 137.Brigell RH, Cagney DN, Martin AM, Besse LA, Catalano PJ, Lee EQ, et al. Local control after brain-directed radiation in patients with cystic versus solid brain metastases. J Neurooncol. 2019;142:355–63. doi: 10.1007/s11060-019-03106-1. [DOI] [PubMed] [Google Scholar]
- 138.Rahman M, Cox JB, Chi Y-Y, Carter JH, Friedman WA. Radiographic response of brain metastasis after linear accelerator radiosurgery. Stereotact Funct Neurosurg. 2012;90:69–78. doi: 10.1159/000334669. [DOI] [PubMed] [Google Scholar]
- 139.Aiyama H, Yamamoto M, Kawabe T, Watanabe S, Koiso T, Sato Y, et al. Clinical significance of conformity index and gradient index in patients undergoing stereotactic radiosurgery for a single metastatic tumor. J Neurosurg. 2018;129:103–10. doi: 10.3171/2018.6.GKS181314. [DOI] [PubMed] [Google Scholar]
- 140.Dupic G, Brun L, Molnar I, Leyrat B, Chassin V, Moreau J, et al. Significant correlation between gross tumor volume (GTV) D98% and local control in multifraction stereotactic radiotherapy (MF-SRT) for unresected brain metastases. Radiother Oncol. 2021;154:260–8. doi: 10.1016/j.radonc.2020.11.021. [DOI] [PubMed] [Google Scholar]
- 141.Kim KH, Kong D-S, Cho KR, Lee MH, Choi J-W, Seol HJ, et al. Outcome evaluation of patients treated with fractionated Gamma Knife radiosurgery for large (> 3 cm) brain metastases: a dose-escalation study. J Neurosurg. 2020;133:675–84. doi: 10.3171/2019.5.JNS19222. [DOI] [PubMed] [Google Scholar]
- 142.Baliga S, Garg MK, Fox J, Kalnicki S, Lasala PA, Welch MR, et al. Fractionated stereotactic radiation therapy for brain metastases: a systematic review with tumour control probability modelling. Br J Radiol. 2017;90:20160666. doi: 10.1259/bjr.20160666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Mengue L, Bertaut A, Ngo Mbus L, Doré M, Ayadi M, Clément-Colmou K et al. Brain metastases treated with hypofractionated stereotactic radiotherapy: 8 years experience after Cyberknife installation. Radiat Oncol. 2020;15. [DOI] [PMC free article] [PubMed]
- 144.Angelov L, Mohammadi AM, Bennett EE, Abbassy M, Elson P, Chao ST, et al. Impact of 2-staged stereotactic radiosurgery for treatment of brain metastases ≥ 2 cm. J Neurosurg. 2018;129:366–82. doi: 10.3171/2017.3.JNS162532. [DOI] [PubMed] [Google Scholar]
- 145.Lockney NA, Wang DG, Gutin PH, Brennan C, Tabar V, Ballangrud A, et al. Clinical outcomes of patients with limited brain metastases treated with hypofractionated (5 × 6 gy) conformal radiotherapy. Radiother Oncol. 2017;123:203–8. doi: 10.1016/j.radonc.2017.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Minniti G, D’Angelillo RM, Scaringi C, Trodella LE, Clarke E, Matteucci P, et al. Fractionated stereotactic radiosurgery for patients with brain metastases. J Neurooncol. 2014;117:295–301. doi: 10.1007/s11060-014-1388-3. [DOI] [PubMed] [Google Scholar]
- 147.Minniti G, Scaringi C, Paolini S, Lanzetta G, Romano A, Cicone F, et al. Single-fraction versus Multifraction (3 × 9 Gy) stereotactic radiosurgery for Large (> 2 cm) brain metastases: a comparative analysis of local control and risk of radiation-induced brain necrosis. Int J Radiat Oncol*Biol*Physics. 2016;95:1142–8. doi: 10.1016/j.ijrobp.2016.03.013. [DOI] [PubMed] [Google Scholar]
- 148.Traylor JI, Habib A, Patel R, Muir M, Gadot R, Briere T, et al. Fractionated stereotactic radiotherapy for local control of resected brain metastases. J Neurooncol. 2019;144:343–50. doi: 10.1007/s11060-019-03233-9. [DOI] [PubMed] [Google Scholar]
- 149.Kumar AMS, Miller J, Hoffer SA, Mansur DB, Coffey M, Lo SS, et al. Postoperative hypofractionated stereotactic brain radiation (HSRT) for resected brain metastases: improved local control with higher BED10. J Neurooncol. 2018;139:449–54. doi: 10.1007/s11060-018-2885-6. [DOI] [PubMed] [Google Scholar]
- 150.Bachmann N, Leiser D, Ermis E, Vulcu S, Schucht P, Raabe A et al. Impact of regular magnetic resonance imaging follow-up after stereotactic radiotherapy to the surgical cavity in patients with one to three brain metastases. Radiat Oncol. 2019;14. [DOI] [PMC free article] [PubMed]
- 151.Mahajan A, Ahmed S, McAleer MF, Weinberg JS, Li J, Brown P, et al. Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: a single-centre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017;18:1040–8. doi: 10.1016/S1470-2045(17)30414-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Brennan C, Yang TJ, Hilden P, Zhang Z, Chan K, Yamada Y, et al. A phase 2 trial of stereotactic radiosurgery boost after surgical resection for brain metastases. Int J Radiat Oncol*Biol*Physics. 2014;88:130–6. doi: 10.1016/j.ijrobp.2013.09.051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Cleary RK, Meshman J, Dewan M, Du L, Cmelak AJ, Luo G et al. Postoperative fractionated stereotactic radiosurgery to the Tumor Bed for surgically resected brain metastases. Cureus. 2017;9(5). [DOI] [PMC free article] [PubMed]
- 154.Soliman H, Myrehaug S, Tseng C-L, Ruschin M, Hashmi A, Mainprize T, et al. Image-guided, linac-based, surgical cavity-hypofractionated stereotactic radiotherapy in 5 daily fractions for brain metastases. Neurosurgery. 2019;85:E860–9. doi: 10.1093/neuros/nyz162. [DOI] [PubMed] [Google Scholar]
- 155.Keller A, Doré M, Cebula H, Thillays F, Proust F, Darié I, et al. Hypofractionated stereotactic radiation therapy to the resection bed for intracranial metastases. Int J Radiat Oncol*Biol*Physics. 2017;99:1179–89. doi: 10.1016/j.ijrobp.2017.08.014. [DOI] [PubMed] [Google Scholar]
- 156.Doré M, Martin S, Delpon G, Clément K, Campion L, Thillays F. Stereotactic radiotherapy following surgery for brain metastasis: predictive factors for local control and radionecrosis. Cancer/Radiothérapie. 2017;21:4–9. doi: 10.1016/j.canrad.2016.06.010. [DOI] [PubMed] [Google Scholar]
- 157.Mousli A, Bihin B, Gustin T, Koerts G, Mouchamps M, Daisne JF. Surgical bed stereotactic radiotherapy of brain metastases: clinical outcome and predictors of local and distant brain failure. Cancer/Radiothérapie. 2020;24:298–305. doi: 10.1016/j.canrad.2019.12.002. [DOI] [PubMed] [Google Scholar]
- 158.Eaton BR, Gebhardt B, Prabhu R, Shu H-K, Curran WJ, Crocker I. Hypofractionated radiosurgery for intact or resected brain metastases: defining the optimal dose and fractionation. Radiat Oncol. 2013;8. [DOI] [PMC free article] [PubMed]
- 159.El Shafie RA, Dresel T, Weber D, Schmitt D, Lang K, König L et al. Stereotactic cavity irradiation or whole-brain Radiotherapy following brain metastases Resection—Outcome, prognostic factors, and recurrence patterns. Front Oncol. 2020;10. [DOI] [PMC free article] [PubMed]
- 160.Gui C, Grimm J, Kleinberg LR, Zaki P, Spoleti N, Mukherjee D, et al. A dose-response model of local tumor control probability after stereotactic radiosurgery for brain metastases resection cavities. Adv Radiat Oncol. 2020;5:840–9. doi: 10.1016/j.adro.2020.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Ahmed KA, Freilich JM, Abuodeh Y, Figura N, Patel N, Sarangkasiri S, et al. Fractionated stereotactic radiotherapy to the post-operative cavity for radioresistant and radiosensitive brain metastases. J Neurooncol. 2014;118:179–86. doi: 10.1007/s11060-014-1417-2. [DOI] [PubMed] [Google Scholar]
- 162.Jhaveri J, Chowdhary M, Zhang X, Press RH, Switchenko JM, Ferris MJ, et al. Does size matter? Investigating the optimal planning target volume margin for postoperative stereotactic radiosurgery to resected brain metastases. J Neurosurg. 2019;130:797–803. doi: 10.3171/2017.9.JNS171735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Yusuf MB, Amsbaugh MJ, Burton E, Nelson M, Williams B, Koutourousiou M, et al. Increasing time to postoperative stereotactic radiation therapy for patients with resected brain metastases: investigating clinical outcomes and identifying predictors associated with time to initiation. J Neurooncol. 2017;136:545–53. doi: 10.1007/s11060-017-2679-2. [DOI] [PubMed] [Google Scholar]
- 164.Foreman PM, Jackson BE, Singh KP, Romeo AK, Guthrie BL, Fisher WS, et al. Postoperative radiosurgery for the treatment of metastatic brain tumor: evaluation of local failure and leptomeningeal disease. J Clin Neurosci. 2018;49:48–55. doi: 10.1016/j.jocn.2017.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Ojerholm E, Lee JYK, Thawani JP, Miller D, O’Rourke DM, Dorsey JF, et al. Stereotactic radiosurgery to the resection bed for intracranial metastases and risk of leptomeningeal carcinomatosis. J Neurosurg. 2014;121:75–83. doi: 10.3171/2014.6.GKS14708. [DOI] [PubMed] [Google Scholar]
- 166.Lee C-C, Yen C-P, Xu Z, Schlesinger D, Sheehan J. Large intracranial metastatic tumors treated by Gamma Knife surgery: outcomes and prognostic factors. J Neurosurg. 2014;120:52–9. doi: 10.3171/2013.9.JNS131163. [DOI] [PubMed] [Google Scholar]
- 167.Pontoriero A, Conti A, Iatì G, Mondello S, Aiello D, Rifatto C, et al. Prognostic factors in patients treated with stereotactic image-guided robotic radiosurgery for brain metastases: a single-center retrospective analysis of 223 patients. Neurosurg Rev. 2016;39:495–504. doi: 10.1007/s10143-016-0718-7. [DOI] [PubMed] [Google Scholar]
- 168.Kilburn JM, Ellis TL, Lovato JF, Urbanic JJ, Daniel Bourland J, Munley MT, et al. Local control and toxicity outcomes in brainstem metastases treated with single fraction radiosurgery: is there a volume threshold for toxicity? J Neurooncol. 2014;117:167–74. doi: 10.1007/s11060-014-1373-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Lee C-K, Lee SR, Cho JM, Yang KA, Kim S-H. Therapeutic effect of Gamma Knife Radiosurgery for multiple brain metastases. J Korean Neurosurg Soc. 2011;50:179–84. doi: 10.3340/jkns.2011.50.3.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Ebinu JO, Lwu S, Monsalves E, Arayee M, Chung C, Laperriere NJ, et al. Gamma Knife Radiosurgery for the treatment of cystic cerebral metastases. Int J Radiat Oncol*Biol*Physics. 2013;85:667–71. doi: 10.1016/j.ijrobp.2012.06.043. [DOI] [PubMed] [Google Scholar]
- 171.Lockney NA, Wang DG, Pei X, Goldman DA, Zhang Z, Lin A, et al. Phosphatidylinositol-3-kinase mutations are associated with increased local failure in brain metastases treated with radiation. Int J Radiat Oncol*Biol*Physics. 2018;101:833–44. doi: 10.1016/j.ijrobp.2018.03.032. [DOI] [PubMed] [Google Scholar]
- 172.Ahmed KA, Sarangkasiri S, Chinnaiyan P, Sahebjam S, Yu H-HM, Etame AB, et al. Outcomes following hypofractionated stereotactic radiotherapy in the management of brain metastases. Am J Clin Oncol. 2016;39:379–83. doi: 10.1097/COC.0000000000000076. [DOI] [PubMed] [Google Scholar]
- 173.Choi CYH, Chang SD, Gibbs IC, Adler JR, Harsh GR, Lieberson RE, et al. Stereotactic radiosurgery of the postoperative resection cavity for brain metastases: prospective evaluation of target margin on tumor control. Int J Radiat Oncol*Biol*Physics. 2012;84:336–42. doi: 10.1016/j.ijrobp.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 174.Rades D, Evers JN, Veninga T, Stalpers LJA, Lohynska R, Schild SE. Shorter-course whole-brain radiotherapy for brain metastases in elderly patients. Int J Radiat Oncol*Biol*Physics. 2011;81:e469–73. doi: 10.1016/j.ijrobp.2011.01.058. [DOI] [PubMed] [Google Scholar]
- 175.Lee DS, Kim YS, Lee CG, Lim JH, Suh C-O, Kim HJ, et al. Early volumetric change and treatment outcome of metastatic brain tumors after external beam radiotherapy: differential radiotherapy for brain metastasis. Clin Transl Oncol. 2013;15:889–96. doi: 10.1007/s12094-013-1016-2. [DOI] [PubMed] [Google Scholar]
- 176.Heisterkamp C, Haatanen T, Schild SE, Rades D. Dose escalation in patients receiving whole-brain radiotherapy for brain metastases from colorectal cancer. Strahlenther Onkol. 2010;186:70–5. doi: 10.1007/s00066-010-2067-8. [DOI] [PubMed] [Google Scholar]
- 177.Rades D, Panzner A, Dziggel L, Haatanen T, Lohynska R, Schild SE. Dose-escalation of whole-brain radiotherapy for brain metastasis in patients with a favorable survival prognosis. Cancer. 2011;118:3852–9. doi: 10.1002/cncr.26680. [DOI] [PubMed] [Google Scholar]
- 178.Rades D, Meyners T, Veninga T, Stalpers LJA, Schild SE. Hypofractionated whole-brain radiotherapy for multiple brain metastases from transitional cell carcinoma of the bladder. Int J Radiat Oncol*Biol*Physics. 2010;78:404–8. doi: 10.1016/j.ijrobp.2009.07.1717. [DOI] [PubMed] [Google Scholar]
- 179.Meyners T, Heisterkamp C, Kueter J-D, Veninga T, Stalpers LJ, Schild SE et al. Prognostic factors for outcomes after whole-brain irradiation of brain metastases from relatively radioresistant tumors: a retrospective analysis. BMC Cancer. 2010;10. [DOI] [PMC free article] [PubMed]
- 180.Rades D, Heisterkamp C, Schild SE. Do patients receiving whole-brain radiotherapy for brain metastases from renal cell carcinoma benefit from escalation of the radiation dose? Int J Radiat Oncol*Biol*Physics. 2010;78:398–403. doi: 10.1016/j.ijrobp.2009.08.022. [DOI] [PubMed] [Google Scholar]
- 181.Antoni. Outcome improvement in RPA I or II patients with 1 or 2 brain metastases by combined surgery and Radiotherapy. World J Oncol. 2013;4(1):37–45. [DOI] [PMC free article] [PubMed]
- 182.Buglione M, Pedretti S, Gipponi S, Buttolo L, Panciani P, Poliani PL, et al. The treatment of patients with 1–3 brain metastases: is there a place for whole brain radiotherapy alone, yet? A retrospective analysis. Radiol Med. 2015;120:1146–52. doi: 10.1007/s11547-015-0542-0. [DOI] [PubMed] [Google Scholar]
- 183.Rades D, Kueter JD, Gliemroth J, Veninga T, Pluemer A, Schild SE. Resection plus whole-brain irradiation versus resection plus whole-brain irradiation plus boost for the treatment of single brain metastasis. Strahlenther Onkol. 2012;188:143–7. doi: 10.1007/s00066-011-0024-9. [DOI] [PubMed] [Google Scholar]
- 184.Hughes RT, Black PJ, Page BR, Lucas JT, Qasem SA, Watabe K, et al. Local control of brain metastases after stereotactic radiosurgery: the impact of whole brain radiotherapy and treatment paradigm. J Radiosurg SBRT. 2016;4:89–96. [PMC free article] [PubMed] [Google Scholar]
- 185.Dziggel L, Schild SE, Veninga T, Bajrovic A. Clinical factors asssociated with treatment outcomes following whole-brain irradiation in patients with prostate cancer. Vivo. 2017;31:35–8. doi: 10.21873/invivo.11021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 186.Shiau C-Y, Sneed PK, Shu H-KG, Lamborn KR, McDermott MW, Chang S, et al. Radiosurgery for brain metastases: relationship of dose and pattern of enhancement to local control. Int J Radiat Oncol*Biol*Physics. 1997;37:375–83. doi: 10.1016/S0360-3016(96)00497-X. [DOI] [PubMed] [Google Scholar]
- 187.Jalalifar SA, Soliman H, Sahgal A, Sadeghi-Naini A. Predicting the outcome of radiotherapy in brain metastasis by integrating the clinical and MRI-based deep learning features. Med Phys. 2022;49(11):7167–78. doi: 10.1002/mp.15814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.The Royal College of Radiologists. Radiotherapy dose fractionation, Fourth edition | The Royal College of Radiologists. www.rcr.ac.uk. Published 2024. https://www.rcr.ac.uk/our-services/all-our-publications/clinical-oncology-publications/radiotherapy-dose-fractionation-fourth-edition/.
- 189.Gondi V, Bauman G, Bradfield L, et al. Radiation therapy for brain metastases: an ASTRO clinical practice guideline. Practical Radiation Oncol. 2022;12(4):265–82. doi: 10.1016/j.prro.2022.02.003. [DOI] [PubMed] [Google Scholar]
- 190.Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(71). https://www.bmj.com/content/372/bmj.n71. [DOI] [PMC free article] [PubMed]
- 191.Le Rhun E, Guckenberger M, Smits M, et al. EANO–ESMO clinical practice guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann Oncol. 2021;32(11):1332–47. doi: 10.1016/j.annonc.2021.07.016. [DOI] [PubMed] [Google Scholar]
- 192.Brown PD, Ballman KV, Cerhan JH, et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017;18(8):1049–60. doi: 10.1016/s1470-2045(17)30441-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193.Beslissing tot behandeling met radiotherapie bij hersenmetastasen - Richtlijn - Richtlijnendatabase. (n.d.). Richtlijnendatabase.nl. Retrieved May 23. 2024, from https://richtlijnendatabase.nl/richtlijn/hersenmetastasen/behandeling_-_hersenmetastasen/beslissing_tot_behandeling_met_radiotherapie_bij_hersenmetastasen.html.
- 194.Chao ST, De Salles A, Hayashi M, Levivier M, Ma L, Martinez R, Paddick I, Régis J, Ryu S, Slotman BJ, Sahgal A. Stereotactic radiosurgery in the management of Limited (1–4) brain metasteses: systematic review and International Stereotactic Radiosurgery Society Practice Guideline. Neurosurgery. 2017;83(3):345–53. doi: 10.1093/neuros/nyx522. [DOI] [PubMed] [Google Scholar]
- 195.Zimmerman AL, Murphy ES, Suh JH, Vogelbaum MA, Barnett GH, Angelov L, Ahluwalia M, Reddy CA, Chao ST. Treatment of large brain metastases with stereotactic radiosurgery. Technol Cancer Res Treat. 2015;15(1):186–95. doi: 10.1177/1533034614568097. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data used for this study is available at ETZ and is accessible after approval from the ETZ Science office.