

Abstract
Aim: This study examines the association between burnout, nurse safety behaviors, and patient safety competency among nurses working in cancer hospitals using person-centered and variable-centered methodologies.
Background: Burnout is prevalent among nurses worldwide, with cancer hospital nurses exhibiting high levels of burnout. Burnout correlates with a higher incidence of adverse events and diminished patient safety. Nurse safety behaviors and patient safety competency play protective roles in ensuring patient safety.
Methods: This study used a cross-sectional online survey and included 2092 eligible nurses, with 95.0% being female. We invited nurses from cancer hospitals in 12 provinces in China to complete an online survey from April to June 2023. Through the online Questionnaire Star platform, invited nurses provided demographic information and completed the Maslach Burnout Inventory, the Nurse Safety Behaviors Scale, and the Patient Safety Competency Scale. Latent profile analysis was used to identify heterogeneous characteristics of nurse burnout.
Results: From a person-centered perspective, nurse burnout was categorized into three latent profiles: “high achievement stable type” (70.3%), “high-efficiency contradictory type” (6.6%), and “high-pressure adaptive type” (23.1%). From a variable-centered perspective, patient safety competency partially mediated the relationship between burnout profiles and nurse safety behaviors.
Conclusion: This study identified three heterogeneous latent profiles of burnout among cancer hospital nurses and highlighted the significant impact of excessive working hours and lack of safety training on burnout across different job titles and income levels. Additionally, it verified the mediation effect of patient safety competency between burnout profiles and nurse safety behaviors. Future treatments should focus on high-risk populations by offering improved safety training and suitable work schedules to reduce burnout. Furthermore, personalized measures to enhance nurses' safety competencies should be adopted to improve burnout and safety behaviors. This study integrates person-centered and variable-centered methods, offering new insights and underscoring the critical role of safety in mitigating burnout.
Keywords: burnout, cancer hospitals, latent profile, nurses, nurse safety behaviors, patient safety competency
1. Introduction
Health problems are increasingly becoming a major public health concern due to the rapid socioeconomic growth worldwide [1] . Given their vital role in safeguarding public health, government agencies and society must place greater emphasis on the occupational health of nurses. Burnout is a serious problem that affects nurses worldwide.
The psychological illness known as burnout is caused by extended exposure to work-related stress without adequate management. It poses a serious risk to the occupational health of nurses because it can result in emotional exhaustion, depersonalization, and a lack of personal accomplishment [2–4]. China now suffers from an imbalance in the allocation of nursing personnel throughout provinces and cities, which increases workloads, lowers productivity, and raises burnout rates among nurses [5].
Burnout presents a severe challenge to the healthcare sector, impacting not only nurses' mental health and job satisfaction but also potentially leading to decreased job performance and high turnover rates. This, in turn, affects the stability of medical teams and the quality of patient care. High levels of burnout increase the incidence of adverse events, reducing patient safety [2, 6, 7]. Patient safety is a critical public health issue, and ensuring safety and quality in cancer care is paramount [8]. With the rising incidence of cancer, nurses in cancer hospitals face immense work pressure. Additionally, when dealing with the grief, fear, and death of cancer patients, nurses may experience compassion fatigue and moral distress, exacerbating burnout [9–11]. Therefore, exploring burnout and its related factors, particularly from a safety perspective, among cancer hospital nurses is of significant importance.
Currently, while the issue of burnout among cancer hospital nurses has received clinical attention, there has been a lack of in-depth analysis from the perspective of nurse-centered safety, focusing on the heterogeneous profiles of burnout and their influencing factors. Latent profile analysis (LPA) is an exploratory, person-centered research method that can identify heterogeneous groups of nurse burnout and the differences between these groups. It also employs objective statistical indicators to measure the accuracy and validity of different profiles, ultimately determining the subgroups of burnout [12, 13].
In this study, we aim to reveal the latent profiles of burnout among cancer hospital nurses and explore its antecedents. Additionally, we seek to investigate the relationships between burnout, nurse safety behaviors, and patient safety competency.
1.1. Theoretical Framework and Hypothesis Development
1.1.1. Burnout and Nurse Safety Behaviors
Nurse safety behaviors refer to the conduct exhibited by nursing staff while providing comprehensive care services to patients, including psychological, physiological, and social activities. This encompasses adherence to nursing guidelines and core institutional protocols, as well as the implementation of safety measures [14]. Nurse safety behaviors enhance the quality of care and ensure patient safety. According to Bandura's Social Cognitive Theory (SCT), individual, behavioral, and environmental factors interact and mutually influence one another [15]. Nurses' burnout is an emotional response exhibited by individuals, while safety behaviors are the behavioral state adopted by nurses under the influence of personal and environmental factors. The literature indicates that burnout may reduce nurses' self-efficacy regarding safety behaviors, thereby decreasing its actual execution. In such situations, nurses may neglect their work tasks and overlook critical safety procedures, posing potential threats to patient safety [16, 17]. Furthermore, some studies have found that burnout affects nurses' expectations of work outcomes, reducing their motivation to engage in safety behaviors [18].
1.1.2. Burnout and Patient Safety Competency
Patient safety competency refers to the ability of healthcare professionals to minimize unnecessary harm related to medical care to an acceptable minimum level during the risk control process. It encompasses six aspects: patient-centered care, clinical practice, continuous quality improvement, evidence-based practice, patient safety culture, and safety risk management [19]. Studies showed that patient safety competency can improve the quality of care, reduce the occurrence of nursing errors, and effectively ensure patient safety [20]. Further research indicates that burnout affects nurses' competency in patient safety, potentially leading to decreased cognitive abilities and reduced sensitivity to patient conditions, thereby impacting their ability to respond in complex situations [21]. Emotional exhaustion and work fatigue may impair nurses' ability to recognize and respond quickly to patient conditions, consequently reducing their performance in patient safety [22].
1.1.3. Mediating Role of Patient Safety Competency
From the perspective of SCT, we hypothesized that nurses' patient safety competency may mediate the relationship between burnout and nurse safety behaviors. Specifically, burnout may weaken nurses' self-efficacy and alter their expectations of safety behavior outcomes, which can further affect their patient safety competency [23]. A decline in patient safety competency directly impacts nurses' performance at work, indirectly affecting their patient safety performance by weakening their ability to recognize and handle nurse safety behaviors [24]. Therefore, we hypothesized that nurses' patient safety competency mediates the relationship between burnout and nurse safety behaviors.
H1: Nurses' patient safety competency mediates the relationship between burnout and nurse safety behaviors.
In summary, this study aims to apply LPA to explore the heterogeneous latent profile characteristics and predictors of burnout among cancer hospital nurses. From the perspective of nursing safety, we aim to use SCT to explore the mediating role of nurses' patient safety competency in the relationship between latent profiles of burnout and nurse safety behaviors.
2. Methods
2.1. Study Design
A cross-sectional design was used.
2.2. Participants and Settings
From April to June 2023, 2092 nurses from tertiary cancer hospitals in 12 provinces of China were selected to participate in this research study using the convenience sampling method. The inclusion criteria were as follows: (i) nurses aged ≥ 18 years and (ii) clinical nurses who had obtained the certificate of a registered nurse. The exclusion criteria were as follows: (i) nurses on maternity or sick leave and (ii) nurses visiting for study and clinical practice.
2.3. Procedure
Prior to data collection, the researcher contacted the nursing management teams of cancer hospitals across 12 provinces and cities, securing their agreement to conduct the study. The questionnaire was distributed and collected via the online platform Questionnaire Star. The introductory page provided participants with detailed information on the study's purpose, methodology, and instructions for completion. Participants were informed that their participation was voluntary and anonymous, with the right to withdraw at any time without consequences.
To ensure data integrity, each IP address was restricted to a single submission, and the survey was presented in a sequential, page-turning format, requiring approximately 10 to 15 min to complete. Participants were required to complete all questions before submission, minimizing missing data. The researcher collaborated with department heads to distribute the survey links via departmental WeChat groups, setting a 5-day submission deadline. At the end of the data collection period, two researchers reviewed the submissions, excluding invalid responses. Of the 2240 questionnaires distributed, 2149 were returned. After removing 57 invalid responses, the final sample comprised 2092 valid questionnaires, yielding an effective response rate of 93.4%.
2.4. Variables and Instruments
General demographic information was designed by reviewing the literature of previous studies and included gender, age, education level, job position, title, employment form, years of service, monthly income, marital status, weekly working hours, the total number of adverse events experienced in a career, and safety training courses.
2.4.1. Burnout
We utilized the Maslach Burnout Inventory–Human Services Survey (MBI-HSS) to assess burnout among nurses in cancer hospitals. Developed by Maslach and Jackson [25], the MBI-HSS has been validated for reliability and accuracy within the Chinese nursing population by scholars such as Feng et al. [26]. This scale comprises 22 items, divided into three dimensions: emotional exhaustion, depersonalization, and personal accomplishment. Each item is rated on a 7-point Likert scale, ranging from “never” to “every day,” with scores from 0 to 6. Emotional exhaustion, the core component, represents the dimension of individual stress. Depersonalization reflects the interpersonal relationship dimension, while personal accomplishment pertains to the self-evaluation dimension [27]. Cronbach's alpha coefficient for the entire scale was 0.934, and Cronbach's alpha coefficient for each dimension ranged from 0.865 to 0.934.
2.4.2. Patient Safety Competence
The Patient Safety Competency Self-Rating Scale of Nurses (PSC-SSN) was employed to allow nurses to self-assess their safety competency [28]. The PSC-SSN comprises 29 items distributed across four dimensions: knowledge factors (10 items), system factors (eight items), attitude factors (five items), and skills factors (six items). Each item is rated on a 5-point Likert scale, with “1” representing “very unclear” and “5” representing “very clear,” resulting in total scores ranging from 29 to 145. Higher scores indicate stronger safety competency. In this study, the PSC-SSN demonstrated excellent reliability, with an overall Cronbach's alpha coefficient of 0.970. Cronbach's alpha coefficients for each dimension ranged from 0.812 to 0.934, indicating robust internal consistency.
2.4.3. Nurse Safety Behaviors
The Nurse Safety Behavior Questionnaire (NSBQ) is designed to measure nurses' behaviors that prevent patient harm and promote patient safety at work [29]. This one-dimensional scale consists of 12 items, each rated on a 5-point Likert scale, with “1” indicating “never” and “5” indicating “always.” Total scores range from 12 to 60, with higher scores indicating better performance in nurse safety behaviors. In this study, the NSBQ demonstrated excellent reliability, with Cronbach's alpha coefficient of 0.910.
2.5. Statistical Analysis
The double data entry was conducted using Epidata 3.1 software, while data analysis was performed using Mplus 8.3 and SPSS 24.0. The MBI-HSS utilized a 7-point Likert scale, and LPA was conducted on the mean scores of its three dimensions. The LPA was executed with Mplus software, employing model fit indices such as the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and sample-size adjusted BIC (aBIC) to assess the profiles' accuracy. Lower values of AIC, BIC, and aBIC indicate superior model fit [30]. Entropy values closer to one suggest more precise classification, with values of 0.80 or higher signifying a classification accuracy of 90% or more [31]. The Lo-Mendell–Rubin adjusted likelihood ratio test (LMRT) and bootstrapped likelihood ratio test (BLRT) were utilized to compare models with different class numbers. These tests assess M-class models against M + 1-class models, where a significant p value denotes a better fit for the M + 1 class model [32]. A thorough evaluation of all indices is essential to determine the most optimal model [33].
We used the R3STEP approach to investigate the antecedents of latent burnout profiles. We employed the R3STEP function in Mplus [34, 35], which performs a sequence of multinomial logistic regressions. This approach evaluates whether an increase in covariates would lead to a higher probability of an individual belonging to one class over another. The bootstrap method was employed to assess the mediating effect of nurses' patient safety competency on the relationship between burnout profiles and safety behaviors. Bootstrap samples were drawn 5000 times from the original dataset, and 95% confidence intervals were calculated. If the 95% confidence interval for the standardized path coefficient does not include 0, the mediating effect is deemed significant.
2.6. Ethical Consideration
According to Chinese national ethical regulations and institutional guidelines, this study did not require prior ethical review. Specifically, the Measures for the Ethical Review of Life Sciences and Medical Research Involving Humans (2023), issued by the Chinese government, states that noninterventional studies that do not involve medical interventions, biological samples, or personally identifiable sensitive information are exempted from prior ethical review (Article 35). This study strictly adhered to the institutional ethical standards. Participants were informed of the study's purpose and data usage at the time of participation, and written informed consent was obtained. Participation was entirely voluntary. Additionally, this study was conducted anonymously, did not involve any unethical behavior or clinical interventions, and posed no physical or psychological risks to the participants.
3. Results
3.1. Demographic Information on Survey Respondents
A total of 2092 nurses from cancer hospitals participated in the study, as detailed in Table 1. The majority of participants were female (95.0%), with an average age of 31.89 years (M = 31.89, SD = 7.73), and 60.4% were married. Of the respondents, 69.8% held a bachelor's degree in nursing, and 41.2% had between 4 and 9 years of work experience. Most were employed on a contractual basis (73.4%) and earned a monthly income between 6000 and 9000 RMB (57.8%). Additionally, 87.0% were staff nurses, and 71.1% held the title of senior nurse. The majority worked less than 40 h per week (76.7%), had not experienced adverse events in their careers (55.9%), and had received safety training (94.5%).
Table 1.
Demographic information on survey respondents (mean SD or n [%]).
| Variable | Number | Class 1 | Class 2 | Class 3 |
|---|---|---|---|---|
| n = 1475 | n = 137 | n = 480 | ||
| Age (year) | 31.89 ± 7.73 | 32.06 ± 8.09 | 30.66 ± 7.70 | 31.75 ± 6.50 |
|
| ||||
| Gender | ||||
| Male | 104 (5.0) | 51 (3.5) | 18 (13.1) | 35 (7.3) |
| Female | 1988 (95.0) | 1424 (96.5) | 119 (86.9) | 445 (92.7) |
|
| ||||
| Education level | ||||
| Junior college | 357 (17.1) | 273 (18.5) | 16 (11.7) | 68 (14.2) |
| Faulty-to-undergraduate | 246 (11.8) | 175 (11.9) | 17 (12.4) | 54 (11.3) |
| Undergraduate | 1461 (69.8) | 1010 (68.5) | 102 (74.5) | 349 (72.7) |
| ≥ Postgraduate | 28 (1.3) | 17 (1.2) | 2 (1.5) | 9 (1.9) |
|
| ||||
| Job position | ||||
| None | 1821 (87.0) | 1292 (87.6) | 120 (87.6) | 409 (85.2) |
| Tutor | 164 (7.8) | 102 (6.9) | 16 (11.7) | 46 (9.6) |
| Head nurse | 107 (5.1) | 81 (5.5) | 1 (0.7) | 25 (5.2) |
|
| ||||
| Title | ||||
| Nurse | 536 (25.6) | 426 (28.9) | 26 (19.0) | 84 (17.5) |
| Nurse practitioner | 833 (39.8) | 547 (37.1) | 71 (51.8) | 215 (44.8) |
| Senior nurse or head nurse and above | 723 (34.6) | 502 (34.0) | 40 (29.2) | 181 (37.7) |
|
| ||||
| Years of service | ||||
| < 4 | 503 (24.0) | 388 (26.3) | 31 (22.6) | 84 (17.5) |
| 4∼ | 862 (41.2) | 546 (37.0) | 72 (52.6) | 244 (50.8) |
| 10∼ | 500 (23.9) | 350 (23.7) | 31 (22.6) | 119 (24.8) |
| 20∼ | 227 (10.9) | 191 (12.9) | 3 (2.2) | 33 (6.9) |
|
| ||||
| Employment form | ||||
| Formal incorporation | 350 (16.7) | 272 (18.4) | 14 (10.2) | 64 (13.3) |
| Contract employment | 1536 (73.4) | 1050 (71.2) | 111 (81.0) | 375 (78.1) |
| Personnel agency | 206 (9.8) | 153 (10.4) | 12 (8.8) | 41 (8.5) |
|
| ||||
| Monthly income (RMB) | ||||
| 1000∼ | 320 (15.3) | 214 (14.5) | 30 (21.9) | 76 (15.8) |
| 6000∼ | 1209 (57.8) | 806 (54.6) | 89 (65.0) | 314 (65.4) |
| 10,000∼ | 563 (26.9) | 455 (30.8) | 18 (13.1) | 90 (18.8) |
|
| ||||
| Marital status | ||||
| Married | 1263 (60.4) | 882 (59.8) | 80 (58.4) | 301 (62.7) |
| Single | 829 (39.6) | 593 (40.2) | 57 (41.6) | 179 (37.3) |
|
| ||||
| Weekly working hours | ||||
| ≤ 40 | 1604 (76.7) | 1224 (83.0) | 74 (54.0) | 306 (63.8) |
| > 40 | 488 (23.3) | 251 (17.0) | 63 (46.0) | 174 (36.3) |
|
| ||||
| Adverse incident experience | ||||
| None | 1169 (55.9) | 921 (62.4) | 51 (37.2) | 197 (41.0) |
| Yes | 923 (44.1) | 554 (37.6) | 86 (62.8) | 283 (59.0) |
|
| ||||
| Safety training courses | ||||
| Attended | 1976 (94.5) | 1412 (95.7) | 122 (89.1) | 442 (92.1) |
| Not-attended | 116 (5.5) | 63 (4.3) | 15 (10.9) | 38 (7.9) |
Note: Class 1 = high achievement Stable Type; Class 2 = high-efficiency contradictory type; Class 3 = high-pressure adaptive type.
3.2. Model Selection
To analyze burnout among the 2092 nurses from cancer hospitals, we sequentially established latent profile models ranging from 1 to 5 profiles. Based on a thorough evaluation of the latent profile indicators, the three-profile model was identified as the optimal solution, as shown in Table 2. The justification for this selection is as follows: (1) The AIC, BIC, and aBIC values decreased as the number of profiles increased and began to plateau at the two-profile model, (2) an entropy value greater than 0.80 indicated a classification accuracy of 90% for this model, and (3) the LMR and BLRT values were statistically significant (p < 0.05). Considering all fit indices and the clinical practical significance, the three-profile model was deemed the most appropriate.
Table 2.
Burnout latent profile model fit metrics.
| Model | LL | AIC | BIC | aBIC | Entropy | LMR p value | BLRT p value | Class (%) |
|---|---|---|---|---|---|---|---|---|
| Class 1 | −10741.637 | 21495.274 | 21529.150 | 21510.087 | NA | NA | NA | 1 |
| Class 2 | −9633.623 | 19287.247 | 19343.706 | 19311.935 | 0.914 | < 0.0001 | < 0.0001 | 76.3/23.7 |
| Class 3 | −9204.753 | 18437.505 | 18516.548 | 18472.068 | 0.922 | < 0.0001 | < 0.0001 | 70.3/6.6/23.1 |
| Class 4 | −8948.567 | 17933.133 | 18034.759 | 17977.571 | 0.927 | 0.0008 | < 0.0001 | 23.9/6.6/66.1/3.4 |
| Class 5 | −8637.085 | 17318.170 | 17442.379 | 17372.483 | 0.871 | 0.1079 | < 0.0001 | 3.0/46.9/28.1/17.6/4.4 |
Note: aBIC = sample-size-adjusted BIC.
Abbreviations: AIC = Akaike Information Criteria; BIC = Bayesian Information Criteria; BLRT = bootstrapped likelihood ratio tests; LL = log-likelihood; LMR = LoMendell–Rubin.
To verify the reliability of the above LPA results, we calculated the average membership probabilities for each profile within the three-profile model. The results showed that the average membership probability for Class 1 was 0.979, for Class 2 was 0.942, and for Class 3 was 0.928, indicating that the model fit with three profiles is reliable [36].
3.3. Characteristics and Naming of Latent Profiles of Burnout
As shown in Figure 1, the three latent profiles of cancer hospital nurses exhibit high response probabilities in the three dimensions of burnout. The profiles were named based on their characteristics. Class 1: Named “high achievement stable type,” this profile includes 1475 nurses (70.3%), the largest proportion. Nurses in this group score low on emotional exhaustion and depersonalization, and high on personal accomplishment. This indicates that they experience less emotional stress and detachment at work while feeling satisfied with their accomplishments. These nurses exhibit the lowest levels of burnout and the highest sense of achievement.
Figure 1.
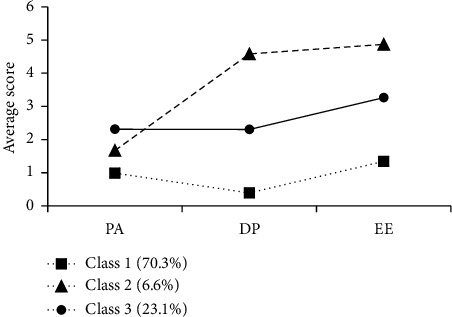
Graphical representation of latent profiles of nurse burnout. Note: EE = emotional exhaustion; DP = depersonalization; PA = personal performance; Class 1 = high achievement stable type; Class 2 = high-efficiency contradictory type; Class 3 = high-pressure adaptive type.
Class 2: Named “high-efficiency contradictory type,” this profile comprises 137 nurses (6.6%). These nurses score the highest on emotional exhaustion and depersonalization but have moderate scores on personal accomplishment. This indicates that they experience high levels of emotional stress and detachment at work, but their sense of accomplishment is not particularly low. These nurses face internal contradictions, despite experiencing significant emotional stress and detachment, they maintain high work efficiency and a moderate level of achievement.
Class 3: Named “high-pressure adaptive type,” this profile includes 480 nurses (23.1%). These nurses score the lowest on personal accomplishment, indicating the highest sense of accomplishment deficit, while scoring moderately on emotional exhaustion and depersonalization. This suggests that they experience a significant lack of accomplishment and moderate levels of emotional stress and detachment at work. These nurses have a poorer ability to adapt to high-pressure environments, exhibiting moderate levels of burnout and the lowest sense of achievement.
3.4. Analysis of Antecedents of Latent Profiles of Burnout
Using the R3STEP method, multinomial logistic regression was conducted to examine the relationships between various factors and the latent profiles of occupational burnout. As shown in Table 3, male nurses were more likely to fall into the “high-efficiency contradictory type” and “high-pressure adaptive type” categories compared to the “high achievement stable type.” Nurses in the “high-efficiency contradictory type” typically held lower positions, had lower incomes, worked more than 40 h per week, experienced adverse events, and did not receive safety training. Nurses in the “high-pressure adaptive type” generally held higher professional titles but had lower incomes, worked more than 40 h per week, experienced adverse events, and did not receive safety training.
Table 3.
Adjusted logit differences from multinomial logistic regression analysis (R3STEP).
| Profile comparison | Class 2 vs. Class 1 | Class 3 vs. Class 1 | Class 3 vs. Class 2 | |
|---|---|---|---|---|
| Age (year) | 0.015 | 0.005 | −0.011 | |
|
| ||||
| Gender | Male (ref.) | |||
| Female | −1.140∗ | −0.624∗ | 0.517 | |
|
| ||||
| Education level | Junior college (ref.) | |||
| Faulty-to-undergraduate | 0.238 | −0.171 | −0.409 | |
| Undergraduate | 0.077 | −0.180 | −0.257 | |
| ≥ Postgraduate | 0.835 | 0.376 | −0.459 | |
|
| ||||
| Job position | None (ref.) | |||
| Tutor | 0.396 | 0.187 | −0.209 | |
| Head nurse | −17.430∗∗ | −0.043 | 17.387 | |
|
| ||||
| Title | Nurse (ref.) | |||
| Nurse practitioner | 0.562 | 0.469 | −0.093 | |
| Senior nurse or head nurse and above | 0.393 | 0.643∗ | 0.249 | |
|
| ||||
| Years of service | < 4 (ref.) | |||
| 4∼ | −0.162 | 0.333 | 0.495 | |
| 10∼ | −0.379 | 0.068 | 0.446 | |
| 20∼ | −2.728 | −0.489 | 2.240 | |
|
| ||||
| Employment form | Formal incorporation (ref.) | |||
| Contract employment | −0.635 | 0.043 | 0.678 | |
| Personnel agency | −0.523 | 0.031 | 0.554 | |
|
| ||||
| Monthly income (RMB) | 1000 (ref.) | |||
| 6000 | −0.450 | −0.233 | 0.218 | |
| 10,000 | −0.976∗ | −0.563∗ | 0.413 | |
|
| ||||
| Marital status | Married (ref.) | |||
| Single | 0.202 | 0.234 | 0.033 | |
|
| ||||
| Weekly working hours | ≤ 40 (ref.) | |||
| > 40 | 1.132∗∗ | 0.838∗∗ | −0.294 | |
|
| ||||
| Adverse incident experience | None (ref.) | |||
| Yes | 0.948∗∗ | 0.676∗∗ | −0.272 | |
|
| ||||
| Safety training courses | Attended (ref.) | |||
| Not-attended | 0.982∗ | 0.665∗ | −0.317 | |
Note: The values represent adjusted logit differences between latent profiles (e.g., Class 2 vs. Class 1) derived using the R3STEP method, which corrects for classification errors in latent profile analysis. Positive values indicate that the logit value for the comparison group (e.g., Class 2) is higher than the reference group (e.g., Class 1), while negative values indicate the opposite. Class 1 = high achievement stable type; Class 2 = high-efficiency contradictory type; Class 3 = high-pressure adaptive type.
∗p < 0.05.
∗∗p < 0.001.
3.5. Mediation Effect Analysis
Before testing for mediation effects, we verified key assumptions to ensure the robustness of the analysis. The Durbin–Watson statistic was approximately two, indicating no autocorrelation among residuals. The variance inflation factor (VIF) values were all below 10, confirming the absence of multicollinearity. To control for potential confounders, we adjusted for gender, age, education level, job position, professional title, employment form, years of service, monthly income, marital status, weekly working hours, the total number of adverse events experienced during a career, and participation in safety training courses. In the mediation effect analysis, the latent profiles of burnout were encoded as dummy variables, while patient safety competency (the mediating variable) and safety behaviors (the dependent variable) were treated as continuous variables. The model demonstrated a good fit, with indices as follows: CFI = 0.957, TLI = 0.895, RMSEA = 0.048, and SRMR = 0.043.
As shown in Table 4 and Figure 2, the results of the mediation analysis indicate that in Path 1, when “high achievement stable type” is used as the reference group, the mediation effect of the “high-efficiency contradictory type” on safety behaviors through patient safety competency is −1.992. The 95% bootstrap confidence interval for this effect is [−2.613, −1.458], which does not include “0,” suggesting a significant partial mediation effect, accounting for 46.3% of the total effect. Furthermore, after incorporating patient safety competency as a mediating variable, the direct effect of the “high-efficiency contradictory type” on safety behaviors is −2.314, with a 95% bootstrap confidence interval of [−3.348, −1.330], again not including “0,” indicating a significant direct effect.
Table 4.
Analysis of mediating effects of patient safety competency (unstandardized).
| Class 1 (ref.) | Impact | 95% CI | |
|---|---|---|---|
| LLCI | ULCI | ||
| Class 2 ⟶ M ⟶ Y | −1.992a | −2.613 | −1.458 |
| Class 2 ⟶ Y | −2.314a | −3.348 | −1.330 |
| Class 3 ⟶ M ⟶ Y | −2.013a | −2.457 | −1.634 |
| Class 3 ⟶ Y | −1.318a | −1.852 | −0.837 |
Note: Class 1 = high achievement stable type; Class 2 = high-efficiency contradictory type; Class 3 = high-pressure adaptive type; M = patient safety competency; Y = nurse safety behaviors.
aSignificant mediation effect.
Figure 2.
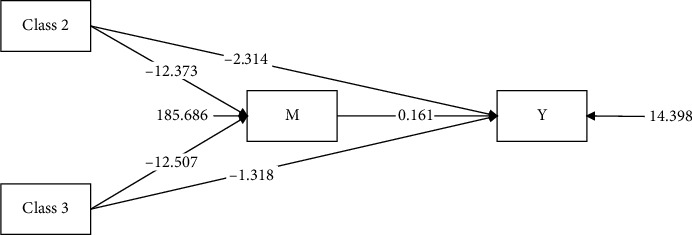
Diagrammatic representation of the mediating effect. Note: Class 2 = high-efficiency contradictory type; Class 3 = high-pressure adaptive type; M = patient safety competency; Y = nurse safety behaviors.
In Path 2, the mediation effect of the “high-pressure adaptive type” on safety behaviors through patient safety competency is −2.013, with a 95% bootstrap confidence interval of [−2.457, −1.634], which does not include “0,” indicating a significant partial mediation effect, accounting for 60.4% of the total effect. This mediation effect is larger than that observed in Path 1. Additionally, after incorporating patient safety competency as a mediating variable, the direct effect of the “high-pressure adaptive type” on safety behaviors is −1.318, with a 95% bootstrap confidence interval of [−1.852, −0.837], again not including “0,” suggesting a significant direct effect.
4. Discussion
This multicenter study investigates the latent profiles of burnout among nurses in Chinese cancer hospitals. Our findings identified three distinct latent profile characteristics of burnout: “high achievement stable type,” “high-efficiency contradictory type,” and “high-pressure adaptive type.” We observed variations in the antecedents of these burnout profiles among the nurses. Furthermore, the study confirmed our initial hypothesis that patient safety competency mediates the relationship between latent burnout profiles and safety behavior.
4.1. Person-Centered Analysis
4.1.1. Latent Profile Characteristics of Burnout
This study identified three burnout profiles among cancer hospital nurses, providing a nuanced understanding of their occupational stress and highlighting the unique emotional and physical challenges of long-term cancer care. A meta-analysis over the past decade found that burnout among nurses is moderate to high, with a global prevalence of 30%, and this rate is expected to rise [37]. Studies also show a negative association between nurse burnout and patient safety [38]. Factors such as poor working conditions, insufficient time for nursing activities, and excessive workloads contribute to burnout, particularly the emotional exhaustion and depersonalization dimensions, which are most closely linked to patient safety. This relationship has persisted over time, with increasing correlations to the quality of care over the last 30 years [39]. Burnout not only affects nurses' physical and mental health but also compromises care quality, increases medication errors, and threatens patient safety [40].
“High achievement stable type” nurses exhibited low levels of emotional exhaustion and depersonalization, alongside relatively high personal accomplishment. This suggests that they can maintain low emotional stress while deriving a sense of achievement from their work. These nurses likely benefit from strong personal resources and adequate professional support, demonstrating high psychological resilience [41]. Importantly, their resilience and engagement may contribute to consistent patient safety behaviors, as they are more likely to approach tasks with focus and motivation.
“High-efficiency contradictory type” nurses exhibited higher levels of depersonalization, suggesting that while they effectively regulate their emotions and adopt positive coping strategies, they may also detach from their work environment and the recipients of their services. This finding aligns with research on European oncologists, highlighting the significant role of depersonalization in burnout [42, 43]. Cancer nurses face ongoing exposure to the sadness and fear of their patients, as well as negative events such as death, which can lead them to adopt avoidance and relational distancing strategies to manage compassion fatigue and moral distress [9, 10, 17, 44]. Such detachment, while protective against emotional overload, may undermine patient safety by reducing attentiveness, empathy, and engagement in care tasks, potentially leading to errors or missed opportunities for intervention.
“High-pressure adaptive type” nurses reported significantly higher levels of emotional exhaustion and lower scores for personal accomplishment. This indicates that they experience considerable emotional stress in their work. Potential contributing factors include understaffing, insufficient organizational support, heavy workloads, frequent exposure to adverse events, and the generally low cure rates in oncology care. These stressors may trigger negative emotions such as depression and distress, further exacerbating self-doubt and feelings of professional inefficacy [45, 46]. As emotional exhaustion intensifies, these nurses may struggle to maintain the cognitive and emotional resources necessary for delivering safe and effective patient care, increasing the risk of errors and declining quality of care.
These profiles show that burnout is multifaceted, requiring tailored interventions to address its behavioral implications for patient safety competence. For “high achievement stable type” nurses, reinforcing existing support can sustain their positive behaviors and high engagement. For “high-efficiency contradictory type” nurses, psychological support and emotional management interventions can reduce detachment and enhance their connection with patients. For “high-pressure adaptive type” nurses, reducing workload and strengthening support systems can mitigate emotional exhaustion and improve their capacity to focus on patient safety. By addressing the specific characteristics of each burnout profile, these targeted interventions can alleviate burnout, enhance nurse performance, and ultimately improve patient care quality.
4.1.2. Antecedent Factors of Latent Profiles of Burnout
The results of this study indicate that, compared to the “high achievement stable type” reference group, male nurses are more likely to be classified into the “high-efficiency contradictory type” and “high-pressure adaptive type.” Nurses categorized as “high efficiency contradictory type” typically hold lower positions and incomes, work more than 40 h per week, have experienced adverse events, and have not received safety training. Similarly, nurses classified as “high-pressure adaptive type” typically hold higher professional titles but lower incomes and exhibit similar patterns of work hours and experiences.
These findings are consistent with the previous research, highlighting the significant impact of work environment and career development on burnout [47]. Long hours and frequent shifts are known to exacerbate work-family conflicts, increasing burnout risk [48–50]. In China, nurses with higher professional titles often shoulder heavier responsibilities, such as critical care, emergency management, and quality control, leading to significant mental and physical strain [51]. Moreover, frequent exposure to adverse events, insufficient safety training, and lack of organizational support further aggravate burnout levels.
Cancer hospital nurses, in particular, face additional risks such as radiation and exposure to antitumor drugs, which intensify psychological stress and negative emotions [52, 53]. Income disparities, especially in remote regions of China, exacerbate effort-reward imbalances and contribute to burnout. Evidence suggests that implementing high-performance work systems can mitigate nurses' anxiety and depression, enhance job satisfaction, and reduce burnout [54].
To address these challenges, health authorities should allocate human resources more effectively and increase income levels in remote areas. Clinical managers should optimize work schedules, balance workloads with adequate rest, establish safe working environments, and minimize exposure risks. These measures are essential to reduce burnout and promote nurse well-being.
4.2. Variable-Centered Analysis
Based on the SCT, this study, with the “high achievement stability type” of nurse burnout as a reference, indicates that patient safety competency partial mediates the effect of nurse burnout latent profiles on their safety behaviors. This underscores the crucial role of enhancing nurses' patient safety competency as a strategy to address nurse burnout.
Nurse safety behaviors and patient safety competency are critical aspects of ensuring safety. Previous studies have showed that burnout can reduce nurse safety behaviors, increase the incidence of adverse events, and lower the quality of care, posing a threat to patient safety [16, 55]. Furthermore, nurses' patient safety competency, including their knowledge, skills, and attitudes toward safety practices, is an essential factor in ensuring patient safety. The research has indicated that systems thinking, psychological safety, teamwork, and professionalism can enhance patient safety competency [56, 57]. The negative impact of nurse burnout on patient safety competency implies that enhancing nurses' patient safety competency can directly improve their safety behaviors and play a crucial role in addressing nurse burnout. For example, through systematic safety training and professional development support, nurses' self-efficacy and professional skills can be enhanced, thereby reducing the impact of burnout.
Healthcare institutions should address nurses' burnout issues by indirectly improving their safety behaviors by enhancing their patient safety competency. This not only helps reduce the incidence of burnout but also enhances overall nursing quality and patient safety levels.
5. Conclusion
In summary, the results of this study not only reveal the various manifestations and causes of nurse burnout but also provide theoretical support through variable-centered analysis, indicating the significant role of patient safety competency in the relationship between burnout latent profiles and nurse safety behaviors. Nursing managers should adopt personalized interventions for different types of burnout, focusing on enhancing nurses' patient safety competency to improve their burnout status and increase nurse safety behaviors.
5.1. Implications for Nursing Management
Nursing managers should develop targeted interventions based on the three identified burnout profiles (“high achievement stable type,” “high-efficiency contradictory type,” and “high-pressure adaptive type”) and provide personalized support to address specific needs and vulnerabilities. This study highlights the crucial role of patient safety competency in mediating the relationship between burnout and safety behaviors, emphasizing the importance of comprehensive safety training programs. Nursing managers should prioritize ongoing education and training initiatives, optimize work schedules to prevent burnout, and ensure adequate staffing levels. Additionally, providing extra support for high-risk groups, fostering a positive work environment, and promoting work-life balance are essential strategies.
The significance of this research lies in its integration of person-centered and variable-centered approaches, offering new insights into the multifaceted nature of burnout and its impact on nurse safety behaviors. By implementing these measures, nursing management can significantly enhance nurse well-being and job satisfaction, ultimately improving patient care quality in cancer hospitals.
5.2. Limitations
Although the findings of this study offer practical insights into cancer nurses' burnout, several limitations should be noted. First, data were based on self-reported questionnaires, which may be prone to social desirability and recall biases. Future studies could incorporate objective data (e.g., job performance assessments) to validate the results. Second, the cross-sectional design prevents the determination of causal relationships. Longitudinal designs are needed to better understand the dynamics between burnout, patient safety competency, and safety behaviors. Additionally, the sample was limited to a specific region, which affects the external validity of the findings. Expanding the sample in future research would improve generalizability. Finally, path analysis models assume reliable and valid measurements, but measurement errors may impact the model's accuracy. Future studies should address measurement error in latent variable modeling or use multiple measures to reduce its impact, thereby enhancing the model's reliability.
5.3. Future Directions
Future research should further explore the following aspects. Firstly, an in-depth investigation of the formation mechanisms of different types of burnout and their long-term impacts on nurses' professional development to develop more effective intervention strategies. Secondly, exploration of specific measures to enhance nurses' patient safety competency, such as safety training and psychological support, to mitigate the negative effects of burnout. Lastly, it is recommended to adopt longitudinal research designs to dynamically track changes in nurse burnout, patient safety competency, and safety behaviors to further validate their causal relationships.
Acknowledgments
The authors would like to thank Ms. Lu Liu for data entry and collection. They also acknowledge the contribution of all the nursing staff of the various hospitals that participated in the research study. The authors used AI-assisted language polishing tools, specifically DeepSeek, to improve the clarity and readability of the manuscript. The AI software was only employed for language refinement and did not contribute to the conceptualization, data analysis, or interpretation of results. After using this tool, the authors carefully reviewed and edited the content as needed and take full responsibility for the final version of the manuscript.
Contributor Information
Yan Liu, Email: liuyan@cicams.ac.cn.
Fan Zhang, Email: timzhang8702@163.com.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Disclosure
The funding sources had no role in the design of the study, data collection, analysis, interpretation, or the decision to submit the manuscript for publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Fengyan Ma: conceptualization, methodology, formal analysis, writing – original draft, and project management.
Yajing Zhu: conceptualization and survey.
Lu Liu: conceptualization and survey.
Helin Chen: investigation and data organization.
Yan Liu: writing – review and supervision.
Fan Zhang: resources, writing – review, and supervision.
Funding
This study was funded by the CAMS Innovation Fund for Medical Sciences (CIFMS) (Grant No. 2024-I2M-C&T-B-053), the Research Project of Bureau of Health Care for Senior Officials (Grant No. 2022ZD17), and the National Key R&D Program of China (Grant No. 2021YFC2500900).
References
- 1.Rantanen J., Lehtinen S., Iavicoli S. Occupational Health Services in Selected International Commission on Occupational Health (ICOH) Member Countries. Scandinavian Journal of Work, Environment & Health . 2013;39(2):212–216. doi: 10.5271/sjweh.3317. [DOI] [PubMed] [Google Scholar]
- 2.Bruyneel A., Bouckaert N., Maertens de Noordhout C., et al. Association of Burnout and Intention-To-Leave the Profession With Work Environment: A Nationwide Cross-Sectional Study Among Belgian Intensive Care Nurses after Two Years of Pandemic. International Journal of Nursing Studies . 2023;137:p. 104385. doi: 10.1016/j.ijnurstu.2022.104385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Atroszko P. A., Demetrovics Z., Griffiths M. D. Work Addiction, Obsessive-Compulsive Personality Disorder, Burn-Out, and Global Burden of Disease: Implications from the ICD-11. International Journal of Environmental Research and Public Health . 2020;17(2):p. 660. doi: 10.3390/ijerph17020660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stufano A., Awoonor-Williams J. K., Vimercati L. Editorial: Factors and Health Outcomes of Job Burnout. Frontiers in Public Health . 2022;10:p. 1023462. doi: 10.3389/fpubh.2022.1023462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cheng J., Kuang X., Zeng L. The Impact of Human Resources for Health on the Health Outcomes of Chinese People. BMC Health Services Research . 2022;22(1):p. 1213. doi: 10.1186/s12913-022-08540-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Al Sabei S. D., Labrague L. J., Miner Ross A., et al. Nursing Work Environment, Turnover Intention, Job Burnout, and Quality of Care: The Moderating Role of Job Satisfaction. Journal of Nursing Scholarship . 2020;52(1):95–104. doi: 10.1111/jnu.12528. [DOI] [PubMed] [Google Scholar]
- 7.Shah M. K., Gandrakota N., Cimiotti J. P., Ghose N., Moore M., Ali M. K. Prevalence of and Factors Associated With Nurse Burnout in the US. JAMA Network Open . 2021;4(2):p. e2036469. doi: 10.1001/jamanetworkopen.2020.36469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Winckworth-Prejsnar K., Nardi E. A., McCanney J., et al. Ensuring Patient Safety and Access in Cancer Care. Journal of the National Comprehensive Cancer Network . 2017;15(12):1460–1464. doi: 10.6004/jnccn.2017.7049. [DOI] [PubMed] [Google Scholar]
- 9.Granek L., Krzyzanowska M. K., Nakash O., et al. Gender Differences in the Effect of Grief Reactions and Burnout on Emotional Distress Among Clinical Oncologists. Cancer . 2016;122(23):3705–3714. doi: 10.1002/cncr.30236. [DOI] [PubMed] [Google Scholar]
- 10.Kaiyu T., Xia L. Influence of Moral Dilemma on Job Burnout of Nurses in Oncology Department. Chinese Nursing Research . 2017;31(34):4344–4348. [Google Scholar]
- 11.Eelen S., Bauwens S., Baillon C., Distelmans W., Jacobs E., Verzelen A. The Prevalence of Burnout Among Oncology Professionals: Oncologists Are at Risk of Developing Burnout. Psycho-Oncology . 2014;23(12):1415–1422. doi: 10.1002/pon.3579. [DOI] [PubMed] [Google Scholar]
- 12.Kenntemich L., von Hülsen L., Schäfer I., Böttche M., Lotzin A. Profiles of Risk Factors for Depressive and Anxiety Symptoms during the COVID-19 Pandemic: A Latent Class Analysis. Psychiatry Research . 2023;323:p. 115150. doi: 10.1016/j.psychres.2023.115150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.MacLean E., Dendukuri N. Latent Class Analysis and the Need for Clear Reporting of Methods. Clinical Infectious Diseases . 2021;73(7):e2285–e2286. doi: 10.1093/cid/ciaa1131. [DOI] [PubMed] [Google Scholar]
- 14.Ma F., Zhu Y., Liu L., Chen H., Liu Y. Work Engagement and Safety Behavior of Nurses in Specialized Cancer Hospitals: The Mediating Role of Self-Efficacy. Journal of Nursing Management . 2023;2023:1–9. doi: 10.1155/2023/9034073. [DOI] [Google Scholar]
- 15.Bandura A. Social Cognitive Theory: An Agentic Perspective. Asian Journal of Social Psychology . 1999;2(1):21–41. doi: 10.1111/1467-839x.00024. [DOI] [PubMed] [Google Scholar]
- 16.Aihua Z., Xianqiong F., Lei Y., Tao L. Mediating Effect of Perceived Patient Safety Culture on Job Burnout and Safety Behavior of Nurses in Emergency Department of Class III Hospitals. Chinese Journal of Modern Nursing . 2022;28(30):4180–4185. [Google Scholar]
- 17.Van Bogaert P., Timmermans O., Weeks S. M., van Heusden D., Wouters K., Franck E. Nursing Unit Teams Matter: Impact of Unit-Level Nurse Practice Environment, Nurse Work Characteristics, and Burnout on Nurse Reported Job Outcomes, and Quality of Care, and Patient Adverse Events--A Cross-Sectional Survey. International Journal of Nursing Studies . 2014;51(8):1123–1134. doi: 10.1016/j.ijnurstu.2013.12.009. [DOI] [PubMed] [Google Scholar]
- 18.Phillips C. Relationships between Workload Perception, Burnout, and Intent to Leave Among Medical–Surgical Nurses. International Journal of Evidence-Based Healthcare . 2020;18(2):265–273. doi: 10.1097/xeb.0000000000000220. [DOI] [PubMed] [Google Scholar]
- 19.Fu M., Wang T., Hu S., et al. Patient Safety Value, Safety Attitude and Safety Competency Among Emergency Nurses in China: A Structural Equation Model Analysis. Journal of Nursing Management . 2022;30(8):4452–4460. doi: 10.1111/jonm.13876. [DOI] [PubMed] [Google Scholar]
- 20.Hafezi A., Babaii A., Aghaie B., Abbasinia M. The Relationship Between Patient Safety Culture and Patient Safety Competency With Adverse Events: A Multicenter Cross-Sectional Study. BMC Nursing . 2022;21(1):p. 292. doi: 10.1186/s12912-022-01076-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.West C. P., Dyrbye L. N., Erwin P. J., Shanafelt T. D. Interventions to Prevent and Reduce Physician Burnout: A Systematic Review and Meta-Analysis. The Lancet . 2016;388(10057):2272–2281. doi: 10.1016/s0140-6736(16)31279-x. [DOI] [PubMed] [Google Scholar]
- 22.Johnson J., Louch G., Dunning A., et al. Burnout Mediates the Association Between Depression and Patient Safety Perceptions: A Cross‐Sectional Study in Hospital Nurses. Journal of Advanced Nursing . 2017;73(7):1667–1680. doi: 10.1111/jan.13251. [DOI] [PubMed] [Google Scholar]
- 23.Dall’Ora C., Ball J., Reinius M., Griffiths P. Burnout in Nursing: A Theoretical Review. Human Resources for Health . 2020;18(1):p. 41. doi: 10.1186/s12960-020-00469-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Abdi F., Jahangiri M., Kamalinia M., Cousins R., Mokarami H. Developing a Model for Predicting Safety Performance of Nurses Based on Psychosocial Safety Climate and Role of Job Demands and Resources, Job Satisfaction, and Emotional Exhaustion as Mediators. BMC Psychology . 2023;11(1):p. 187. doi: 10.1186/s40359-023-01223-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Maslach C., Jackson S., Leiter M. The Maslach Burnout Inventory Manual . 1997. [Google Scholar]
- 26.Feng Y., Luo H., Ye Z. Job Burnout of Nurses. Chinese Mental Health Journal . 2004;18(7):477–479. [Google Scholar]
- 27.Maslach C., Schaufeli W. B., Leiter M. P. Job Burnout. Annual Review of Psychology . 2001;52(1):397–422. doi: 10.1146/annurev.psych.52.1.397. [DOI] [PubMed] [Google Scholar]
- 28.Wei B., Yan W., Mingfang Z., Yan J. Development and Evaluation of a Rating Scale of Patient Safety Competency for Nurses. Journal of Army Medical University . 2016;38(7):776–780. [Google Scholar]
- 29.Shih C. P., Chang L. Y., Chen J. C., Ng C. J., Reinfeld W., Hsu K. H. The Factors Influencing Safety Behavior of Medical Staffs in Emergency Room of a Medical Center in Taiwan. Journal of Management . 2008;25(4):p. 15. [Google Scholar]
- 30.Tofighi D., Enders C. K. Identifying the Correct Number of Classes in Growth Mixture Models. 2007.
- 31.Celeux G., Soromenho G. An Entropy Criterion for Assessing the Number of Clusters in a Mixture Model. Journal of Classification . 1996;13(2):195–212. doi: 10.1007/bf01246098. [DOI] [Google Scholar]
- 32.Lo Y., Mendell N. R., Rubin D. B. Testing the Number of Components in a Normal Mixture. Biometrika . 2001;88(3):767–778. doi: 10.1093/biomet/88.3.767. [DOI] [Google Scholar]
- 33.McLachlan G. J., Bean R. W., Peel D. A Mixture Model-Based Approach to the Clustering of Microarray Expression Data. Bioinformatics . 2002;18(3):413–422. doi: 10.1093/bioinformatics/18.3.413. [DOI] [PubMed] [Google Scholar]
- 34.Asparouhov T., Muthén B. Auxiliary Variables in Mixture Modeling: Three-step Approaches Using M Plus. Structural Equation Modeling: A Multidisciplinary Journal . 2014;21(3):329–341. doi: 10.1080/10705511.2014.915181. [DOI] [Google Scholar]
- 35.Vermunt J. K. Latent Class Modeling with Covariates: Two Improved Three-Step Approaches. Political Analysis . 2010;18(4):450–469. doi: 10.1093/pan/mpq025. [DOI] [Google Scholar]
- 36.Weller B. E., Bowen N. K., Faubert S. J. Latent Class Analysis: A Guide to Best Practice. Journal of Black Psychology . 2020;46(4):287–311. doi: 10.1177/0095798420930932. [DOI] [Google Scholar]
- 37.Ge M. W., Hu F. H., Jia Y. J., Tang W., Zhang W. Q., Chen H. L. Global Prevalence of Nursing Burnout Syndrome and Temporal Trends for the Last 10 years: A Meta-Analysis of 94 Studies Covering over 30 Countries. Journal of Clinical Nursing . 2023;32(17-18):5836–5854. doi: 10.1111/jocn.16708. [DOI] [PubMed] [Google Scholar]
- 38.Jun J., Ojemeni M. M., Kalamani R., Tong J., Crecelius M. L. Relationship between Nurse Burnout, Patient and Organizational Outcomes: Systematic Review. International Journal of Nursing Studies . 2021;119:p. 103933. doi: 10.1016/j.ijnurstu.2021.103933. [DOI] [PubMed] [Google Scholar]
- 39.Li L. Z., Yang P., Singer S. J., Pfeffer J., Mathur M. B., Shanafelt T. Nurse Burnout and Patient Safety, Satisfaction, and Quality of Care: A Systematic Review and Meta-Analysis. JAMA Network Open . 2024;7(11):p. e2443059. doi: 10.1001/jamanetworkopen.2024.43059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Giusti E. M., Ferrario M. M., Veronesi G., D’Amato A., Gianfagna F., Iacoviello L. Perceived Work Stressors and the Transition to Burnout Among Nurses in Response to the Pandemic: Implications for Healthcare Organizations. Scandinavian Journal of Work, Environment & Health . 2024;50(3):158–167. doi: 10.5271/sjweh.4148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Castillo-González A., Velando-Soriano A., De La Fuente-Solana E. I., Martos-Cabrera B. M., Membrive-Jiménez M. J., Lucía R. B. Cañadas-De La Fuente GA: Relation and Effect of Resilience on Burnout in Nurses: A Literature Review and Meta-Analysis. International Nursing Review . 2024;71(1):160–167. doi: 10.1111/inr.12838. [DOI] [PubMed] [Google Scholar]
- 42.Banerjee S., Califano R., Corral J., et al. Professional Burnout in European Young Oncologists: Results of the European Society for Medical Oncology (ESMO) Young Oncologists Committee Burnout Survey. Annals of Oncology . 2017;28(7):1590–1596. doi: 10.1093/annonc/mdx196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kust D., Murgic J., Vukovic P., et al. Oncologist Burnout Syndrome in Eastern Europe: Results of the Multinational Survey. JCO Oncology Practice . 2020;16(4):e366–e376. doi: 10.1200/jop.19.00470. [DOI] [PubMed] [Google Scholar]
- 44.Eche I. J., Phillips C. S., Alcindor N., Mazzola E. A Systematic Review and Meta-Analytic Evaluation of Moral Distress in Oncology Nursing. Cancer Nursing . 2023;46(2):128–142. doi: 10.1097/ncc.0000000000001075. [DOI] [PubMed] [Google Scholar]
- 45.Guastello A. D., Brunson J. C., Sambuco N., et al. Predictors of Professional Burnout and Fulfilment in a Longitudinal Analysis on Nurses and Healthcare Workers in the COVID-19 Pandemic. Journal of Clinical Nursing . 2022;33(1):288–303. doi: 10.1111/jocn.16463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Shahrour G., Dardas L. A. Acute Stress Disorder, Coping Self‐Efficacy and Subsequent Psychological Distress Among Nurses Amid COVID‐19. Journal of Nursing Management . 2020;28(7):1686–1695. doi: 10.1111/jonm.13124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Soto-Rubio A., Giménez-Espert M. d C., Prado-Gascó V. Effect of Emotional Intelligence and Psychosocial Risks on Burnout, Job Satisfaction, and Nurses’ Health during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health . 2020;17(21):p. 7998. doi: 10.3390/ijerph17217998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Cañadas‐De la Fuente G. A., Gómez‐Urquiza J. L., Ortega‐Campos E. M., Cañadas G. R., Albendín‐García L., De la Fuente‐Solana E. I. Prevalence of Burnout Syndrome in Oncology Nursing: A Meta-Analytic Study. Psycho-Oncology . 2018;27(5):1426–1433. doi: 10.1002/pon.4632. [DOI] [PubMed] [Google Scholar]
- 49.HaGani N., Yagil D., Cohen M. Burnout Among Oncologists and Oncology Nurses: A Systematic Review and Meta-Analysis. Health Psychology . 2022;41(1):53–64. doi: 10.1037/hea0001155. [DOI] [PubMed] [Google Scholar]
- 50.Pang Y., He Y., Chen Z., Han X., Leng J., Tang L. The Perceptions of Burnout and Related Influencing Factors in Chinese Physicians and Nurses Working in a Cancer Hospital. Psycho-Oncology . 2021;30(9):1525–1534. doi: 10.1002/pon.5709. [DOI] [PubMed] [Google Scholar]
- 51.Kanthak M. K., Stalder T., Hill L. K., Thayer J. F., Penz M., Kirschbaum C. Autonomic Dysregulation in Burnout and Depression: Evidence for the Central Role of Exhaustion. Scandinavian Journal of Work, Environment & Health . 2017;43(5):475–484. doi: 10.5271/sjweh.3647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Xu W., Pan Z., Li Z., Lu S., Zhang L. Job Burnout Among Primary Healthcare Workers in Rural China: A Multilevel Analysis. International Journal of Environmental Research and Public Health . 2020;17(3):p. 727. doi: 10.3390/ijerph17030727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Li S., Ten Berge J., Kristiansen M. H. Burnout and Its Antecedents: Considering Both Work and Household Time Claims, and Flexibility in Relation to Burnout. Frontiers in Public Health . 2022;10:p. 863348. doi: 10.3389/fpubh.2022.863348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bernales-Turpo D., Quispe-Velasquez R., Flores-Ticona D., et al. Burnout, Professional Self-Efficacy, and Life Satisfaction as Predictors of Job Performance in Health Care Workers: The Mediating Role of Work Engagement. J Prim Care Community Health . 2022;13:p. 21501319221101845. doi: 10.1177/21501319221101845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Labrague L. J., Al Sabei S. D., AbuAlRub R. F., Burney I. A., Al Rawajfah O. Authentic Leadership, Nurse-Assessed Adverse Patient Events and Quality of Care: The Mediating Role of Nurses’ Safety Actions. Journal of Nursing Management . 2021;29(7):2152–2162. doi: 10.1111/jonm.13356. [DOI] [PubMed] [Google Scholar]
- 56.Habibi Soola A., Ajri-Khameslou M., Mirzaei A., Bahari Z. Predictors of Patient Safety Competency Among Emergency Nurses in Iran: A Cross-Sectional Correlational Study. BMC Health Services Research . 2022;22(1):p. 547. doi: 10.1186/s12913-022-07962-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Kakemam E., Ghafari M., Rouzbahani M., Zahedi H., Roh Y. S. The Association of Professionalism and Systems Thinking on Patient Safety Competency: A Structural Equation Model. Journal of Nursing Management . 2022;30(3):817–826. doi: 10.1111/jonm.13536. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.