

Abstract
Background:
Use of syndesmotic suture button fixation has gained in popularity for treating an injury to the tibiofibular syndesmosis. This biomechanical study used a cadaveric model to simulate in vivo loading conditions to assess the impact of the placement of a syndesmotic stabilization construct using a suture button device.
Methods:
Biomechanical fixation stability with suture button device (TightRope; Arthrex, Naples, FL) placed at 4 distances from the tibiotalar joint line (0.5, 1.5, 2.5, and 3.5 cm) and 3 trajectories (anterior, medial, and posterior) were studied using cadaveric lower extremities with created syndesmotic injuries. Nondestructive testing was conducted on a biaxial servo-hydraulic load frame. The load application consisted of 2 portions: (1) axial compression simulating weightbearing and (2) external rotation of the ankle (up to 12 degrees and under 7.5 Nm) around the long axis of the tibia combined with weightbearing. Fibular motion and syndesmotic widening were tracked using motion analysis to quantify stability.
Results:
Fixation placed at 0.5 or 1.5 cm from the joint line in medial or posterior trajectories resulted in the lowest increases in fibular rotation under loading. More proximal or anterior placements led to increased fibular motion and decreased rotational stability. Ankle width changes were minimal in most groups, although slightly increased widening occurred at proximal and anterior placements.
Conclusion:
Placement of the syndesmotic suture button fixation 0.5-1.5 cm of the joint line in medial or posterior orientations provides the most rotationally stable fixation in a cadaveric model. These findings support flexibility in syndesmotic suture button fixation positioning when hardware constraints limit ideal placement.
Keywords: ankle fracture, syndesmosis, suture button, biomechanical
Introduction
Distal fibula fractures are common and often involve injury to the tibiofibular syndesmosis, requiring stabilization in 15% to 35% of operative ankle fractures.1,5,9,16,21 Recently, suture button constructs for syndesmosis stabilization are gaining favor because of their more dynamic stabilization, reduction of complications associated with rigid fixation, and need for hardware removal. Multiple studies have shown suture button fixation provides comparable outcomes to screw fixation.3,18,25,26 Even at midterm follow-up, suture button fixation has resulted in excellent clinical outcomes. 6
A significant amount of research has been performed on syndesmotic fixation. Previous studies have looked at the biomechanical properties of single–suture button fixation when compared to an all-suture construct, 2–suture button construct, or some form of combination of suture button and suture construct.1,12,14,17,24 Other studies have compared suture button fixation vs screw fixation or hybrid fixation.3,15,19,25 Additionally, studies have retrospectively looked at the anterior to posterior orientation of the fixation construct. 11 The appropriate amount of tensioning during implementation of suture button construct has also been researched. 10 Although great progress has been made regarding the use of suture buttons for syndesmosis injuries, a recent systematic review comparing the biomechanical properties of different suture button configurations in cadaveric studies demonstrated the need for further biomechanical research in this field. 23
In the absence of standardized guidelines, surgeons often rely on judgment or prior studies to determine suture button placement, underscoring the need for biomechanical evidence to guide optimal positioning. Fracture morphology influences plate orientation and available holes for suture button fixation, underscoring the need to identify positions and trajectories that provide adequate syndesmotic stability. To the knowledge of the authors, the optimal position of a suture button such as the Arthrex Tightrope Fixation device for ankle syndesmosis stabilization has not been ascertained. Multiple studies have evaluated the optimal screw positioning for syndesmosis repair,8,20 but no study has systematically evaluated optimal positioning for a suture button device, leaving a key gap in clinical guidance. Our study aims to better understand the optimal position of a syndesmotic stabilization construct using an Arthrex Syndesmosis Fixation device in a cadaveric syndesmosis injury model. We hypothesize that the placement (position and trajectory) of the suture button fixation device is a significant factor that can cause differences in fixation strengths (diastasis) and deviations of the relative tibiofibular motion from the intact ankle.
Materials and Methods
Institutional review board approval was obtained prior to the initiation of this study.
Specimen Preparation
Eight fresh frozen human cadaveric lower extremities were procured for this study (donors mean age: 59.0 years, range: 52-68 years, 3 males and 5 females). The inclusion criteria consisted of male or female donors aged 18-70 years who maintained an active or ambulatory lifestyle. Donors were excluded if they had cancer that had metastasized to the lower limb, or if they had documented injuries or surgeries involving the foot and ankle. Sample size was determined through a priori power analysis, using fibular rotation findings from a prior study on suture button fixation. 3 A sample size of 8 will yield more than 80% power at 5% significance level for detecting differences of 30%. The specimens included the lower leg (disarticulated at the knee) with intact ankle and foot. The specimens were stored at −20°C freezer and thawed overnight at room temperature before the day of testing. Four fixation distances of 0.5, 1.5, 2.5, and 3.5 cm from the joint line were studied. At each of the 3 lower distances (0.5, 1.5, and 2.5 cm), 3 trajectories were tested: directly along the malleolar axis, 1 cm anterior to the malleolar axis, and 1 cm posterior to the malleolar axis. At the most proximal distance of 3.5 cm, 1 trajectory along the malleolar axis was studied (Figure 1). This makes a total of 10 repeated study groups. A custom-made drilling jig was used to prepare these 10 trajectories on each specimen. The soft tissues that surround the proximal section of the limb were carefully dissected to facilitate potting, as were those around the syndesmosis. Saline solution was periodically sprayed onto the exposed ankle to maintain the moisture in the specimen. Before creating syndesmotic injuries, a baseline control with intact syndesmosis and all 10 trajectories predrilled was tested first. Pilot tests were conducted with an incremental set of 3 bone tunnels predrilled. The findings indicated that the reductions in construct stiffness compared with the intact were 6.8%, 7.5%, 8.9%, and 12.0% for the 3-, 6-, 9-, and 12-tunnel configurations, respectively. Consequently, with 10 predrilled tunnels, the anticipated reduction in stiffness would be approximately 10% compared to the intact state (Supplementary Table S1).
Figure 1.

Illustration showing the exiting point on the distal tibia for the drilling trajectories used in the 10 study groups.
Syndesmotic Injury Model and Repair
Syndesmotic injury was created by sectioning the anterior-inferior and posterior-inferior tibiofibular ligaments, the posterior deep deltoid ligament, and 10 cm of the interosseous membrane with a scalpel. Surgical repair using a suture button implant at each of the 10 predrilled trajectories was performed following manufacturer guidelines at a random order preselected before the start of testing. Following each testing trial, the implant was carefully removed and inspected for any damage before manually restoring it to the original configuration. A total of 20 implants were used for the 80 repairs, with each implant used fewer than 5 repeated trials.
Biomechanical Testing
After preparation, each lower limb specimen was mounted onto a biaxial servo-hydraulic load frame (Bionix Landmark 370, MTS Systems, Eden Prairie, MN) for nondestructive testing (Figure 2). The long axis of the tibia was aligned with the actuator. A 3/8-inch threaded rod was inserted through the proximal tibia in the anteroposterior direction and coupled with a pair of I-bolts mounted on the actuator to facilitate the application of axial compression and external rotation loads. The foot was placed in the neutral position on a 1-inch-thick 1-foot by 1-foot plexiglass block secured to the base of the load frame. The surface of the block that was in contact with the foot was lined with 60-grit self-adhesive coarse sandpaper to prevent any slipping of the foot. The foot position was visually monitored for any slippage throughout the loading period. This setup aimed to impose as little physical constraint as possible on the foot to best mimic physiologic loading conditions.
Figure 2.

Experimental setup for application of combined axial and torsional loads to the ankle joint.
The loading protocols consisted of 2 phases: the first was axial compression simulated weightbearing, and the second was combined weightbearing with external rotation at the ankle. The quasi-static axial force of up to 1 body weight was applied through the proximal tibia at a rate of 0.5 mm/s. Once the peak compression was achieved, the tibia was internally rotated (equivalent to external rotation of the foot) up to a physiologic range of 12 degrees and under 7.5 Nm, a threshold that has been used by several previous studies on syndesmotic injury repair for weightbearing simulation.3,4,7,13 Three cycles of loading and unloading were used to precondition the specimens before data collection.
At the ankle, the relative motions between the fibula, the tibia, and the talus in response to loading were tracked using a motion analysis system (Optotrak Certus, Northern Digital Inc, Waterloo, Ontario, Canada) and synchronized with the collection of the MTS loading data. The marker triads were placed on the posterior side of the tibia, the fibula, and on the posterior talus. Two single markers were placed on the malleoli to measure the distance changes at the ankle width. All data was collected at the rate of 60 Hz.
Data Analysis
The relative range of motion (ROM) between the fibula and tibia and changes in ankle width in response to axial compression loading and the combined compression and torsional loading were the primary outcomes. Differences in these variables between the 10 fixation trajectories were compared against the intact control at the common peak load for each set of repeated trials. The fixation stiffness of the 10 trajectory groups was also evaluated. Mixed effect analysis and post hoc multiple comparisons were performed. The effects of distance to the joint line and trajectory were evaluated using the same test. The level of statistical significance was set at .05.
Results
Results of tibiofibular rotations in response to axial loading alone and to a combination of axial loading with external rotation are presented in Table 1 (or Figure 3). Under axial loading, the mean tibiofibular ROM increased in all 10 repaired groups over Intact, by 54% to 102%. The increases from 6 of the 10 groups reached statistical significance (P < .05). The addition of external rotational loading generated greater tibiofibular ROM for all groups. Statistical significance over the intact group was reached in the 3 anterior trajectory repairs (0.5 cm anterior, 1.5 cm anterior, 2.5 cm anterior) and at all trajectories of the 2 most proximal level repairs (2.5 and 3.5 cm). The differences between repairs were not remarkable.
Table 1.
The Tibiofibular ROM in Axial Loading Alone and With External Rotation. a
| Axial Load Alone, degrees, Mean (SD) |
With External Rotation, degrees, Mean (SD) |
|
|---|---|---|
| Intact | 0.48 (0.56) | 0.69 (0.69) |
| 0.5 cm anterior | 0.74 (0.58)* | 1.33 (1.03)*** |
| 0.5 cm medial | 0.77 (0.88) | 1.05 (0.93) |
| 0.5 cm posterior | 0.87 (0.72)* | 1.04 (0.96) |
| 1.5 cm anterior | 0.84 (0.45) | 1.21 (0.95)** |
| 1.5 cm medial | 0.96 (0.70)* | 0.99 (0.70) |
| 1.5 cm posterior | 0.83 (0.41)* | 0.99 (0.83) |
| 2.5 cm anterior | 0.75 (0.44) | 1.22 (0.77)** |
| 2.5 cm medial | 0.93 (0.68)* | 1.08 (0.93)* |
| 2.5 cm posterior | 0.89 (0.76)* | 1.12 (1.07)* |
| 3.5 cm medial | 0.87 (0.59) | 1.18 (0.73) * |
Difference over Intact: *P < .05, **P < .01, ***P < .001.
Figure 3.
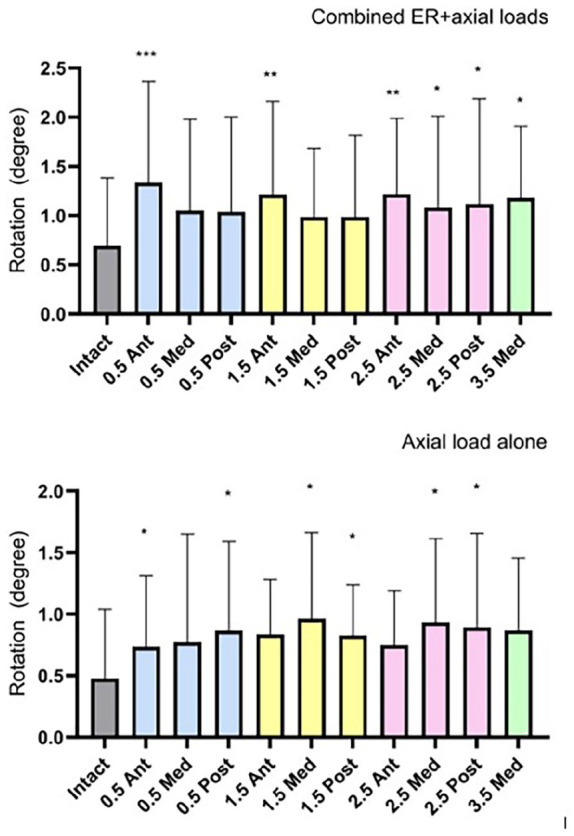
The mean (SD) tibiofibular range of motion under combined axial loading and external rotation (top) and axial loading only (bottom). Asterisks denote statistically significant differences over Intact: *P ≤ .05, **P ≤ .01, ***P ≤ .001.
Changes in ankle width were also greater in repaired groups and increased with combined loading (Table 2 and Figure 4). However, the differences between the repaired and the intact were only significant in 2 repair groups (2.5 cm medial and 2.5 cm posterior in axial loading alone). The differences between repairs were also not remarkable. A moderate to strong correlation was observed between tibiofibular rotation and ankle width change, with Pearson R values ranging from 0.52 to 0.8. This correlation was present in both intact and most repaired groups, achieving statistical significance or marginal significance. However, 2 exceptions were noted in 0.5-cm medial and 3.5-cm medial groups ( Supplementary Table S2).
Table 2.
Changes in Ankle Width in Axial Loading Alone and With External Rotation.
| Axial Load Alone, mm, Mean (SD) |
With External Rotation, mm, Mean (SD) |
|
|---|---|---|
| Intact | 0.37 (0.19) | 0.43 (0.26) |
| 0.5 cm anterior | 0.39 (0.27) | 0.48 (0.27) |
| 0.5 cm medial | 0.43 (0.45) | 0.58 (0.45) |
| 0.5 cm posterior | 0.45 (0.25) | 0.38 (0.33) |
| 1.5 cm anterior | 0.57 (0.34) | 0.62 (0.43) |
| 1.5 cm medial | 0.51 (0.25) | 0.46 (0.29) |
| 1.5 cm posterior | 0.54 (0.34) | 0.42 (0.29) |
| 2.5 cm anterior | 0.50 (0.31) | 0.58 (0.23) |
| 2.5 cm medial | 0.56 (0.26)* | 0.54 (0.32) |
| 2.5 cm posterior | 0.57 (0.31)* | 0.41 (0.30) |
| 3.5 cm medial | 0.56 (0.28) | 0.71 (0.41) |
Significant difference over Intact.
Figure 4.

The mean (SD) changes in joint width under combined axial loading and external rotation (top) and axial loading only (bottom). The asterisk denotes a statistically significant difference over Intact at P ≤ .05.
Globally, the mean ankle stiffness of the intact control was 190 (83) N/mm in axial loading and 271 (97) Nm/degree in external rotation. Both stiffnesses were reduced in all repair groups by 9% to 19% in axial loading and by 6% to 25% in external rotation. No statistical differences were observed.
Discussion
This study is the first to systematically assess the impact of both distance from the joint line and anterior-to-posterior trajectory on the biomechanical stability of syndesmotic suture button fixation. Although screw fixation guidance exists, suture button positioning lacks similar evidence. Our findings show that placement closer to the joint line—specifically 0.5 cm or 1.5 cm—and oriented medially or posteriorly yields superior control of fibular rotation under axial and combined loading. These results provide valuable intraoperative guidance, especially in the presence of fracture hardware that limits available placement options.
Several studies have investigated the optimal distance of syndesmotic screw fixation; however, to the authors’ knowledge, no research has evaluated the optimal distance for syndesmotic suture button device fixation. For screw fixation, the Arbeitsgemeinschaft fur Osteosynthesefragen (AO) internation fixation manual suggests screws be inserted 2-3 cm above the articular surface. 22 Yüce et al 27 found that the syndesmotic malreduction rate increases with the distance from the articular surface. Whereas Li et al 8 evaluated the ideal position for syndesmotic screw fixation and found that the clinical outcomes were similar regardless of whether the screw was placed less than 2 cm, between 2 and 3 cm, or more than 3 cm from the joint line. This study aimed to further investigate the biomechanical impact of placement of a syndesmotic suture button device, focusing on both the distance from the tibial talar joint line, and the orientation in the anterior to posterior trajectory.
Syndesmotic ankle injuries are often associated with distal fibular fractures requiring open reduction and internal fixation.1,5,9,16 A vast majority of distal fibular fractures are reduced and stabilized using a plating technique. Especially in the setting of osteoporotic bone, most suture button constructs are placed through the fibular plate to increase the surface area and decrease the chance of the implant pulling through the bone. Given the variability of fracture patterns and limitation in the number of screw holes available within a plate, it can sometimes be difficult to have an open, available screw hole for a syndesmotic suture button device. This may restrict the surgeon’s option to position the suture button at a specific distance from the tibial talar joint without compromising the fracture stabilization. Additionally, there may be a need for a second syndesmotic suture button device. Schermann et al 17 reported that using a single suture button along with suture tape reconstruction provides sufficient stabilization of the syndesmosis. However, incorporating a second suture button enhances the stability further. Conversely, Parker et al 15 found no benefit to using a second suture button when comparing single, parallel double, or divergent double suture button configurations. In their meta-analysis, Wixted et al 23 identified a few differences between single– and double–suture button configurations in the existing literature. Furthermore, a study by Schon et al 18 showed that a 2–suture button construct could result in an excessive compression of the syndesmosis. Therefore, the necessity for a second syndesmotic suture button device warrants further study. Nonetheless, having multiple options regarding the distance from the tibiotalar joint line and the orientation of the syndesmotic suture button device, which could still result in syndesmotic stability, could be advantageous.
Data from the current study showed an increased fibular rotation of all repair groups compared to the preinjury state, either under axial weightbearing load or when combining weightbearing with external rotation. Several previous studies have reiterated these findings,1,3,15 indicating that syndesmotic injuries repaired with a single suture button do not restore ankle stability to its preinjury level in the immediate postoperative period. The increases varied significantly among the 10 repair groups, ranging from 42% of the intact to as high as 93% of the intact when subjected to combined loading. (In comparison, Baker et al 1 reported an increase from 1.25 to 5.22 degrees or more than 300% of increase under similar loading conditions.) The medial and posterior trajectories of the 2 distal sets (0.5 and 1.5 cm) exhibited smaller increases ranging from 42% to 52% of the intact values. The other 5 groups, which included all anterior trajectories and 2 proximal sets (2.5 and 3.5 cm), displayed significantly greater increases compared to the intact. This suggests that positioning the suture button device either 0.5 or 1.5 cm away from the joint line, whether medially or posteriorly, yields more stability than positioning it anteriorly or at a greater distance from the joint line. The most pronounced increase observed among the 10 repairs occurred with the anterior positioning at 0.5 cm from the joint line, leading to a 93% increase. Inferior outcomes with anterior trajectories may stem from fibular positioning after reduction. Anterior fixation tends to cause anterior fibular translation, whereas posterior fixation leads to posterior translation. 11 When an external torque causes the fibula to externally rotate, a posteriorly translated fibula may be resisted by the ascending tibial incisura, whereas an anteriorly positioned fibula can rotate more freely along the descending portion of the incisura without additional resistance.
Our findings on fibular rotation did not correspond to comparable levels of changes in syndesmotic widening, as measured by changes in ankle width, despite some correlations between the two. These findings align with the results discovered by Burssens et al, 2 who found that higher displacements occurred in axial rotation and posterior translation of the fibula rather than syndesmotic widening when a torque is applied. Only a suture button device placed at 2.5 cm in a medial or posterior trajectory showed a statistically significant increase compared to the intact state under axial loading. When both axial and external rotation loading were applied, no significant changes were noted. Table 2 suggests a potential trend that at proximal distances from the joint line, an anterior trajectory leads to increased ankle width when an axial and external rotation loading are applied. Moreover, there appears to be a trend suggesting that greater distance from the joint line may result in an increase in ankle width under axial force alone is applied. These findings are consistent with biomechanical principles, as a fixation point situated further from the joint line results in a longer lever arm, which enable contact forces to generate increased movement or instability.
Based on the findings of this study, it can be concluded that to achieve optimal rotational stability of the fibula minimizing syndesmotic widening under axial or axial combined external rotational loading, a suture button device positioned at 0.5 and 1.5 cm from the joint line in a medial or posterior direction provides the best stability. However, placement of a syndesmotic TightRope at 2.5 and 3.5 cm from the joint line can still result in adequate stability to syndesmotic widening when an axial plus external rotational force is applied. These findings can guide intraoperative decisions, when hardware or fracture morphology limits suture button device placement. Understanding which trajectories offer sufficient stability gives flexibility to adapt fixation without compromising biomechanical outcomes. When optimal positioning conflicts with fracture fixation or soft tissue management, a more proximal, or anterior or posteriorly directed, syndesmotic suture button device placement can be used to preserve fracture stability, with the understanding that this may come at the expense of some rotational stability.
This study did not evaluate the quality of the reduction of each suture button fixation directly, which presents a good area for future investigations. Although their study assessed both screw fixation and suture button fixation, Nimick et al 11 found that anterior-directed syndesmotic fixation led to anterior malreduction of the fibula, whereas posterior-directed fixation resulted in posterior malreduction of the fibula. Based on their findings, a medial (transmalleolar) trajectory would be preferred to a posterior trajectory, even though stability was similar at multiple distances from the joint line.
The present study has limitations commonly associated with cadaveric research, including variability in bone quality and a limited number of available specimens. All cadaveric models used complete syndesmotic disruptions, not fully representing the variety in degree of injury seen in clinical settings. Although individual suture button device systems were used multiple times, which could have affected their integrity, each one was thoroughly assessed for strength and integrity prior to reuse. Importantly, no suture button device was used greater than 5 times, and the order of testing distances and trajectories was intentionally varied to ensure that each repair group received consistent evaluation, from the first to the fifth use of a suture button device. The evaluation of fixation performance under cyclic loading was not conducted in this study because of the limited availability of TightRope devices and the extended duration required for testing.
Future studies could evaluate if the differences in rotational stability at the different positions has an impact on rehabilitation and need for longer immobilization. Additionally, they can evaluate the effect of using double–suture button device constructs.
Conclusion
This biomechanical study demonstrated that a syndesmotic suture button placed at 0.5or 1.5 cm from the joint line in a medial or posterior trajectory offers optimal rotational stability and limits syndesmotic widening under simulated physiologic loading. Although proximal or anterior placements may still prevent excessive widening, they allow greater fibular rotation. When optimal placement is not feasible because of fracture morphology or implant constraints, the study findings support informed compromises by identifying which placements are most likely to maintain syndesmotic stability.
Supplemental Material
Supplemental material, sj-pdf-1-fao-10.1177_24730114251342243 for Optimal Tightrope Positioning for Adequate Syndesmotic Stabilization in Simulated Syndesmotic Injuries by Mark A. Goss, Alex T. Burton, Jonathan C. Kraus, Linda M. McGrady and Mei Wang in Foot & Ankle Orthopaedics
Acknowledgments
Implants used in this study were provided in kind by Arthrex.
Supplementary Table S1.
Axial Stiffness and Its Reduction After Drilling of Tunnels Compared to the Intact Condition.
| Condition | Intact | 3 Tunnels | 6 Tunnels | 9 Tunnels | 12 Tunnels |
|---|---|---|---|---|---|
| Stiffness, kN/mm | 4.72 | 4.40 | 4.37 | 4.31 | 4.16 |
| % reduction | – | 6.8 | 7.5 | 8.9 | 12.0 |
Supplementary Table S2.
Results of Pearson Correlation Between Fibular Rotation and Ankle Width Changes.
| Conditions | 0.5 cm Anterior | 0.5 cm Medial | 0.5 cm Posterior | 1.5 cm Anterior | 1.5 cm Medial | |
|---|---|---|---|---|---|---|
| R value | 0.74 | 0.29 | 0.52 | 0.56 | 0.59 | |
| P value | 0.02 | 0.24 | 0.09 | 0.07 | 0.06 | |
| Conditions | 1.5 cm Posterior | 2.5 cm Anterior | 2.5 cm Medial | 2.5 cm Posterior | 3.5 cm Medial | Intact |
| R value | 0.58 | 0.69 | 0.74 | 0.29 | 0.52 | 0.69 |
| P value | 0.07 | 0.03 | 0.02 | 0.24 | 0.09 | 0.03 |
Footnotes
Ethical Approval: Institutional review board approval was obtained prior to the initiation of this cadaveric study.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alex T. Burton, MD, received a grant from Arthrex (IRR-01718) to supply the tightropes necessary for the study. Disclosure forms for all authors are available online.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an intramural grant. Implants were donated by Arthrex through a research grant (IRR-01718).
ORCID iD: Mark A. Goss, MD,  https://orcid.org/0000-0001-8626-3159
https://orcid.org/0000-0001-8626-3159
Data availability: The data generated in this study are available from the corresponding author by request.
References
- 1. Baker HP, Muriuki MG, Straszewski AJ, et al. Comparison of a novel modified all-suture construct versus suspensory suture-button fixation in a syndesmotic injury model. J Orthop Trauma. 2023;37(3):E104-E110. doi: 10.1097/BOT.0000000000002503 [DOI] [PubMed] [Google Scholar]
- 2. Burssens A, Krähenbühl N, Weinberg MM, Lenz AL, Saltzman CL, Barg A. Comparison of external torque to axial loading in detecting 3-dimensional displacement of syndesmotic ankle injuries. Foot Ankle Int. 2020;41(10):1256-1268. doi: 10.1177/1071100720936596 [DOI] [PubMed] [Google Scholar]
- 3. Clanton TO, Whitlow SR, Williams BT, et al. Biomechanical comparison of 3 current ankle syndesmosis repair techniques. Foot Ankle Int. 2017;38(2):200-207. doi: 10.1177/1071100716666278 [DOI] [PubMed] [Google Scholar]
- 4. Ebramzadeh E, Knutsen AR, Sangiorgio SN, Brambila M, Harris TG. Biomechanical comparison of syndesmotic injury fixation methods using a cadaveric model. Foot Ankle Int. 2013;34(12):1710-1717. doi: 10.1177/1071100713503816 [DOI] [PubMed] [Google Scholar]
- 5. Egol KA, Pahk B, Walsh M, Tejwani NC, Davidovitch RI, Koval KJ. Outcome after unstable ankle fracture: effect of syndesmotic stabilization. J Orthop Trauma. 2010;24(1):7-11. doi: 10.1097/BOT.0b013e3181b1542c [DOI] [PubMed] [Google Scholar]
- 6. Forsythe K, Freedman KB, Stover MD, Patwardhan AG. Comparison of a novel FiberWire-button construct versus metallic screw fixation in a syndesmotic injury model. Foot Ankle Int. 2008;29(1):49-54. doi: 10.3113/FAI.2008.0049 [DOI] [PubMed] [Google Scholar]
- 7. Lamothe JM, Baxter JR, Murphy C, Gilbert S, Desandis B, Drakos MC. Three-dimensional analysis of fibular motion after fixation of syndesmotic injuries with a screw or suture-button construct. Foot Ankle Int. 2016;37(12):1350-1356. doi: 10.1177/1071100716666865 [DOI] [PubMed] [Google Scholar]
- 8. Li JK, Yu Y, Wu YH, Wang J, Zeng XT, Zhao JG. Does the level of syndesmotic screw insertion affect clinical outcome after ankle fractures with syndesmotic instability? Orthop Surg. 2023;15(1):247-255. doi: 10.1111/os.13569 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Litrenta J, Saper D, Tornetta P, et al. Does syndesmotic injury have a negative effect on functional outcome? A multicenter prospective evaluation. J Orthop Trauma. 2015;29(9):410-413. doi: 10.1097/BOT.0000000000000295 [DOI] [PubMed] [Google Scholar]
- 10. Morellato J, Louati H, Bodrogi A, et al. The effect of varying tension of a suture button construct in fixation of the tibiofibular syndesmosis - evaluation using stress computed tomography. J Orthop Trauma. 2017;31(2):103-110. doi: 10.1097/BOT.0000000000000737 [DOI] [PubMed] [Google Scholar]
- 11. Nimick CJ, Collman DR, Lagaay P. Fixation orientation in ankle fractures with syndesmosis injury. J Foot Ankle Surg. 2013;52(3):315-318. doi: 10.1053/j.jfas.2013.02.005 [DOI] [PubMed] [Google Scholar]
- 12. O’Daly AE, Kreulen RT, Thamyongkit S, et al. Biomechanical evaluation of a new suture button technique for reduction and stabilization of the distal tibiofibular syndesmosis. Foot Ankle Orthop. 2020;5(4):1-7. doi: 10.1177/2473011420969140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pang EQ, Bedigrew K, Palanca A, Behn AW, Hunt KJ, Chou L. Ankle joint contact loads and displacement in syndesmosis injuries repaired with Tightropes compared to screw fixation in a static model. Injury. 2019;50(11):1901-1907. doi: 10.1016/j.injury.2019.09.012 [DOI] [PubMed] [Google Scholar]
- 14. Parker AS, Beason DP, Slowik JS, Sabatini JB, Waldrop NE. Biomechanical comparison of 3 syndesmosis repair techniques with suture button implants. Orthop J Sport Med. 2018;6(10):1-6. doi: 10.1177/2325967118804204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Patel NK, Chan C, Murphy CI, Debski RE, Musahl V, Hogan MV. Hybrid fixation restores tibiofibular kinematics for early weightbearing after syndesmotic injury. Orthop J Sport Med. 2020;8(9):1-7. doi: 10.1177/2325967120946744 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Sagi HC, Shah AR, Sanders RW. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J Orthop Trauma. 2012;26(7):439-443. doi: 10.1097/BOT.0b013e31822a526a [DOI] [PubMed] [Google Scholar]
- 17. Schermann H, Ogawa T, Lubberts B, et al. Comparison of several combinations of suture tape reinforcement and suture button constructs for fixation of unstable syndesmosis. J Am Acad Orthop Surg. 2022;30(10):E769-E778. doi: 10.5435/JAAOS-D-21-00508 [DOI] [PubMed] [Google Scholar]
- 18. Schon JM, Williams BT, Venderley MB, et al. A 3-D CT analysis of screw and suture-button fixation of the syndesmosis. Foot Ankle Int. 2017;38(2):208-214. doi: 10.1177/1071100716673590 [DOI] [PubMed] [Google Scholar]
- 19. Teramoto A, Suzuki D, Kamiya T, Chikenji T, Watanabe K, Yamashita T. Comparison of different fixation methods of the suture-button implant for tibiofibular syndesmosis injuries. Am J Sports Med. 2011;39(10):2226-2232. doi: 10.1177/0363546511413455 [DOI] [PubMed] [Google Scholar]
- 20. Verim O, Serhan Er M, Altinel L, Tasgetiren S. Biomechanical evaluation of syndesmotic screw position: a finite-element analysis. J Orthop Trauma. 2014;28(4):210-215. doi: 10.1097/BOT.0b013e3182a6df0a [DOI] [PubMed] [Google Scholar]
- 21. Weening B, Bhandari M. Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma. 2005;19(2):102-108. doi: 10.1097/00005131-200502000-00006 [DOI] [PubMed] [Google Scholar]
- 22. Willenegger H, Weber B. G., Malleolar Fractures. In: Müller ME, Allgöwer M, Willenegger H, eds Technique of Internal Fixation of Fractures. Springer Berlin Heidelberg; 1965;112-145. doi:10.1007/978-3-642-88356-9 [Google Scholar]
- 23. Wixted CM, Luo EJ, Stauffer TP, Wu KA, Adams SB, Anastasio AT. Biomechanical profile of varying suture button constructs in cadaveric specimens: a systematic review and meta-analysis. Ann Transl Med. 2023;11(10):344-344. doi: 10.21037/atm-23-1527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Wood AR, Arshad SA, Kim H, Stewart D. Kinematic analysis of combined suture-button and suture anchor augment constructs for ankle syndesmosis injuries. Foot Ankle Int. 2020;41(4):463-472. doi: 10.1177/1071100719898181 [DOI] [PubMed] [Google Scholar]
- 25. Xu K, Zhang J, Zhang P, et al. Comparison of suture-button versus syndesmotic screw in the treatment of distal tibiofibular syndesmosis injury: a meta-analysis. J Foot Ankle Surg. 2021;60(3):555-566. doi: 10.1053/j.jfas.2020.08.005 [DOI] [PubMed] [Google Scholar]
- 26. Xu Y, Kang R, Li M, et al. The clinical efficacy of suture-button fixation and trans-syndesmotic screw fixation in the treatment of ankle fracture combined with distal tibiofibular syndesmosis injury: a retrospective study. J Foot Ankle Surg. 2022;61(1):143-148. doi: 10.1053/j.jfas.2021.07.009 [DOI] [PubMed] [Google Scholar]
- 27. Yüce A, Mısır A, Yerli M, et al. The effect of syndesmotic screw level on postoperative syndesmosis malreduction. J Foot Ankle Surg. 2022;61:482-485. doi: 10.1053/j.jfas.2021.09.022 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-pdf-1-fao-10.1177_24730114251342243 for Optimal Tightrope Positioning for Adequate Syndesmotic Stabilization in Simulated Syndesmotic Injuries by Mark A. Goss, Alex T. Burton, Jonathan C. Kraus, Linda M. McGrady and Mei Wang in Foot & Ankle Orthopaedics