

Abstract
Purpose
Optimizing muscle activation through exercise variation is critical for enhancing performance and reducing injury risk. This cross-sectional study examined how trunk position (neutral vs. flexion) and surface stability (ground-based vs. suspension-based) influence lower extremity and trunk muscle activation during the Bulgarian Split Squat (BSS).
Methods
Twenty-one trained female athletes (mean ± SD: age 20.3 ± 2.5 years; height 165.9 ± 5.8 cm; body weight 58.5 ± 5.7 kg) participated in the study. Surface electromyography was used to assess activation of eight lower extremity and trunk muscles: gluteus medius (GMed), gluteus maximus (GMax), vastus lateralis (VL), rectus femoris (RF), vastus medialis (VM), semitendinosus (ST), biceps femoris (BF), and erector spinae (ES) during four BSS variations.
Results
Suspension-based BSS resulted in significantly greater activation of the ES (p = 0.046), while trunk flexion increased activation in the GMax, BF, and RF muscles (p < 0.05).
Conclusion
Suspension-based BSS is particularly effective for targeting trunk stabilizers like the ES, while trunk flexion enhances posterior chain muscle activation, especially GMax and BF. These variations can be strategically applied in strength training and rehabilitation to meet specific neuromuscular goals. In practice, the findings may guide individualized programming for enhancing performance or preventing injuries in female athletes.
Trial registration
ClinicalTrials.gov identifier NCT06112015, registered on 01/11/2023.
Keywords: Electromyography, Strength training, Suspension training, Posterior chain
Introduction
Individualized strength training is a cornerstone of injury prevention and rehabilitation. However, traditional exercise programs that emphasize isolated muscle strengthening may not sufficiently address the neuromuscular demands of dynamic and sport-specific tasks [1]. In contrast, functional training programs, which incorporate multi-joint and multiplanar movements, promote enhanced motor control, postural stability, and neuromuscular coordination through increased central nervous system activation [2, 3].
Among the tools used in functional training, suspension-based exercise systems have gained popularity for their ability to elicit greater muscle activation by creating instability and requiring enhanced core engagement to maintain postural alignment [4]. They enhance joint safety through closed kinetic chain mechanics and closely simulate athletic movement patterns [5]. These systems also offer advantages such as portability, cost-efficiency, and adaptability across training settings [6].
A critical component in functional biomechanics is the lumbopelvic-hip complex (LPHC), which serves as a biomechanical hub during load transfer and force generation in sport-spesific movements. Deficits in LPHC strength and control have been associated with altered lower limb kinematics and increased injury risk, particularly among female athletes [7, 8]. Consequently, enhancing activation of LPHC muscles is a strategic focus in both performance enhancement and injury prevention.
Recent studies have shown that minor modifications in exercise technique, such as trunk positioning, can meaningfully influence muscle recruitment [9, 10]. Specifically, increasing trunk flexion during unilateral lower-limb tasks shifts the center of mass posteriorly, enhancing posterior chain engagement and reducing anterior knee loading. A forward lean of approximately 40° has additionally been shown to reduce anterior cruciate ligament (ACL) forces and strains by increasing hip flexion and promoting hamstring–quadriceps co-contraction, which is clinically relevant in both rehabilitation and injury prevention settings [10].
The Bulgarian Split Squat (BSS) is a widely utilized exercise in strength and conditioning programs to improve single-leg strength, balance, and functional performance [11]. However, limited research has examined how trunk positioning and suspension-based modifications affect neuromuscular activation during the BSS particularly in female athletes, who demonstrate sex-specific movement patterns and are at elevated risk for lower extremity injuries [7].
Therefore, the aim of this study was to examine how trunk position (neutral vs. flexion) and support surface (ground-based vs. suspension-based) affect muscle activation patterns during BSS in trained female athletes.
We hypothesized that:
Suspension-based BSS would increase muscle activation, particularly in stabilizing muscles such as the erector spinae.
Trunk flexion would enhance activation of posterior chain muscles, including the gluteus maximus, biceps femoris, and semitendinosus.
Understanding these neuromuscular responses can guide clinicians and performance professionals in selecting exercise variations that align with specific training and rehabilitation objectives in female athletic populations.
Materials and methods
Participants
Twenty-one trained female athletes (mean ± SD: age 20.3 ± 2.5 years; height 165.9 ± 5.8 cm; body weight 58.5 ± 5.7 kg) from various sports disciplines volunteered for this study. The distribution of participants by sport was as follows: football (n = 9), flag football (n = 6), badminton (n = 2), boxing (n = 1), kickboxing (n = 1), table tennis (n = 1), and taekwondo (n = 1). All participants had at least two years of competitive experience and were actively registered with their respective sport federations.
To minimize variability associated with sex-specific biomechanical and hormonal factors, and to address the underrepresentation of female athletes in the literature [7], inclusion was limited to females. The study specifically targeted trained female athletes to evaluate neuromuscular responses under sport-relevant exercise conditions. As the primary focus was on performance-related outcomes, the inclusion of untrained controls was beyond the scope of this investigation.
Exclusion criteria included any musculoskeletal injury within the past year, current pain during trunk or lower limb movement, or the presence of systemic, neurological, or cognitive disorders.
All participants were informed of the study procedures and signed consent forms prior to participation. Ethical approval was obtained from the Gazi University Ethics Committee (2021 − 1133, dated 07/12/2021), and the trial was registered at ClinicalTrials.gov (NCT06112015).
Experimental design
A within-subject, repeated-measures framework was adopted to compare muscle activation across four BSS exercise variations. These included:
G-BSS-N: Ground-Based BSS with Neutral Trunk Position.
G-BSS-F: Ground-Based BSS with Trunk Flexion (40°).
S-BSS-N: Suspension-Based BSS with Neutral Trunk Position.
S-BSS-F: Suspension-Based BSS with Trunk Flexion (40°).
Participants attended two laboratory sessions. The first session included familiarization and instruction. The second session comprised maximal voluntary isometric contraction (MVIC) testing and surface electromyography (EMG) data collection. All participants were tested at approximately the same time of day (late morning to early afternoon) to reduce diurnal variation in neuromuscular performance. The order of the four exercise conditions was randomized using a shuffled-card method. Each condition was performed for three repetitions, and EMG data were recorded during the eccentric (descent) phase of each repetition. A 30-second rest was provided between repetitions and a 10-minute rest between conditions to minimize fatigue. Movement tempo was standardized using a metronome. Perceived exertion was monitored using the Borg scale, and trials were only conducted when ratings were ≤ 1, ensuring adequate neuromuscular recovery and fatigue control. The flow of participants through the study is presented in Fig. 1.
Fig. 1.

Flow diagram of participant recruitment, eligibility screening, exclusions, and progression through testing sessions. MVIC: maximal voluntary isometric contraction; EMG: electromyography
Surface electromyography (EMG)
Muscle activation was measured using a Noraxon MiniDTS surface EMG system. Disposable Ag/AgCl bipolar electrodes (Noraxon Dual EMG) were placed on the dominant leg, in accordance with SENIAM guidelines, with a 20 mm inter-electrode distance. Prior to electrode placement, the skin was shaved if necessary, lightly abraded, and cleaned with alcohol to reduce impedance and ensure signal quality, in accordance with SENIAM recommendations. The following muscles were assessed: gluteus medius (GMed), gluteus maximus (GMax), vastus lateralis (VL), rectus femoris (RF), vastus medialis (VM), semitendinosus (ST), biceps femoris (BF), and erector spinae (ES).
EMG signals were sampled at 1500–3000 Hz and band-pass filtered (20–450 Hz). The root mean square (RMS) of each signal was computed using a 100 ms moving window during the eccentric phase of movement.
MVIC normalization
To normalize EMG data, MVIC were recorded for each muscle in accordance with standard manual muscle testing positions [12]. Each MVIC trial was held for 5 s and repeated three times, with a 60-second rest between trials. The highest RMS value from the three trials was used for normalization. Prior to testing, participants performed light treadmill walking as a warm-up, and verbal encouragement was provided to ensure maximal effort.
Exercise description
Ground-based Bulgarian split squat (G-BSS)
Participants began in a split-stance position with the dominant foot forward and the non-dominant foot placed behind on a bench, with toes resting on top. Hands were crossed over the chest, and trunk posture was maintained as instructed [13]. The step distance was standardized to 75% of the distance between the anterior superior iliac spines (ASIS), and bench height was determined by the participant’s tibial length (measured from the medial joint line to the medial malleolus) [14, 15].
In the G-BSS-N, participants maintained an upright trunk throughout the movement. The back knee was lowered until it touched the floor (~ 100–110° knee flexion), and then the front leg was extended to return to the starting position (Fig. 2a).
Fig. 2.
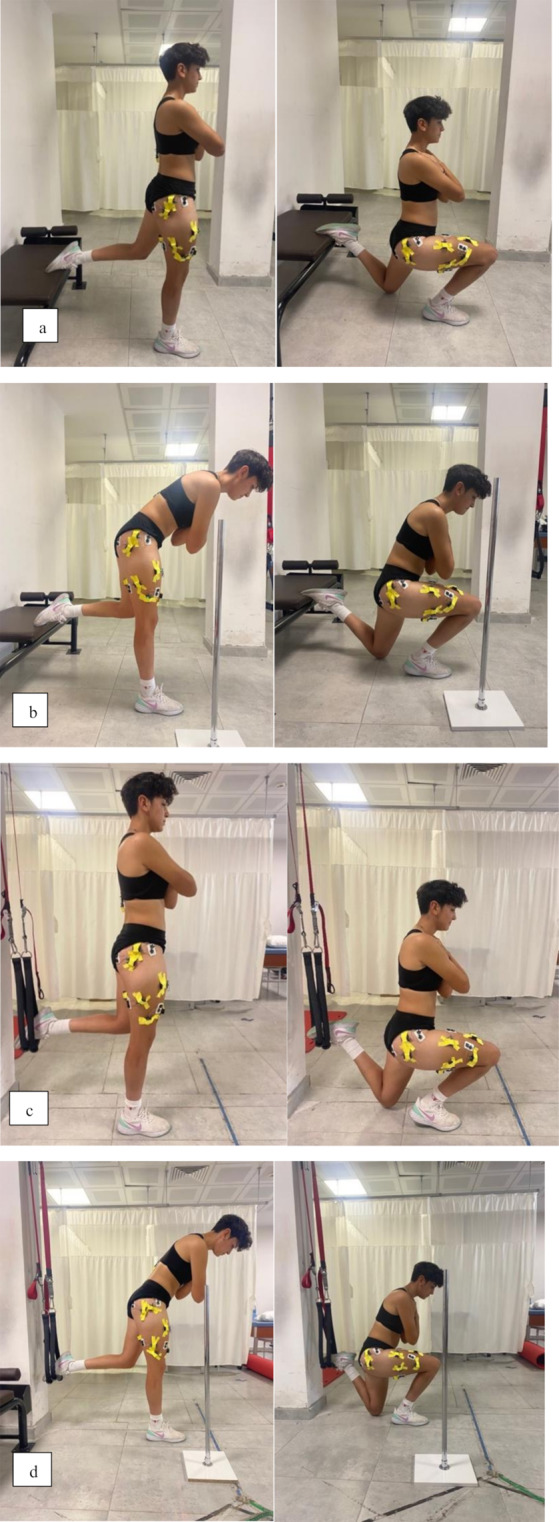
Exercise variations of the Bulgarian split squat (BSS): (a) G-BSS-N, (b) G-BSS-F, (c) S-BSS-N, and (d) S-BSS-F. G-BSS-F: ground-based Bulgarian split squat with trunk flexion; G-BSS-N: ground-based Bulgarian split squat with neutral trunk position; S-BSS-F: suspension-based Bulgarian split squat with trunk flexion; S-BSS-N: suspension-based Bulgarian split squat with neutral trunk position
In the G-BSS-F, participants flexed the trunk forward to a 40° angle, measured using a goniometer. A vertical bar placed at shoulder level served as a visual guide to maintain trunk flexion without forward translation [16]. The same movement sequence was performed while holding this posture (Fig. 2b).
Suspension-based Bulgarian split squat (S-BSS)
The setup was identical to G-BSS, except the non-dominant foot was suspended in a rope loop instead of being placed on a bench. The loop height was matched to the bench height used in G-BSS (tibial length). Step length and foot placement were standardized using the same ASIS and leg-length measurements [14].
In the S-BSS-N, participants maintained an upright trunk position while lowering the back knee to ~ 100–110° flexion, then returning to the start by extending the front leg (Fig. 2c).
In the S-BSS-F, participants flexed the trunk forward to 40°, with alignment monitored using a vertical reference placed at shoulder height. The movement was executed as in other conditions while maintaining this flexed posture (Fig. 2d).
Statistical analysis
All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). o examine the effects of the four exercise conditions on the normalized EMG activation levels of each muscle, generalized estimating equations (GEE) were used. This method accounts for the correlated structure of repeated measures and provides robust estimates even when assumptions such as sphericity or normality are not met.
Separate linear GEE models were fitted for each muscle, with condition (G-BSS-F, G-BSS-N, S-BSS-F, S-BSS-N) as the within-subject factor. An exchangeable working correlation matrix and robust standard errors were applied. When a significant main effect was detected, pairwise comparisons of estimated marginal means were conducted using Bonferroni correction to adjust for multiple testing. Statistical significance was set at p < 0.05.
A post hoc power analysis was conducted using G*Power (version 3.1) based on a repeated-measures design with four conditions, an alpha level of 0.05, and a moderate effect size (f = 0.30). This effect size assumption was based on prior EMG research comparing muscle activation during suspension-based and traditional split squat exercises, which reported small-to-moderate effects (e.g., d ≈ 0.56 for GMax activity) [17]. Given the sample size (n = 21), the achieved statistical power (1 − β) was calculated as 0.89.
Results
The demographic characteristics of the participants are presented in Table 1.
Table 1.
Demographic characteristics of the participants (n = 21)
| Variable | Mean ± SD | Min | Max |
|---|---|---|---|
| Age (years) | 20.3 ± 2.5 | 18.0 | 25.0 |
| Height (cm) | 165.9 ± 5.8 | 153.0 | 175.0 |
| Body weight (kg) | 58.5 ± 5.7 | 51.0 | 70.0 |
| Body Mass Index (BMI, kg/m²) | 21.2 ± 2.0 | 18.2 | 25.2 |
| Sports experience (years) | 5.9 ± 2.4 | 3.0 | 10.0 |
BMI: body mass index
Table 2 displays the normalized EMG activation levels, expressed as %MVIC, for the muscles that showed statistically significant differences across the four BSS exercise conditions: G-BSS-N, G-BSS-F, S-BSS-N, and S-BSS-F.
Table 2.
Normalized EMG activation levels (%MVIC) across four Bulgarian split squat conditions for each muscle
| Muscle | G-BSS-F (Mean ± SD, 95% CI) |
G-BSS-N (Mean ± SD, 95% CI) |
S-BSS-F (Mean ± SD, 95% CI) |
S-BSS-N (Mean ± SD, 95% CI) |
Significant Differences (p < 0.05) |
|---|---|---|---|---|---|
| ES |
35.14±2.78 (29.69–40.59) |
29.95±2.78 (24.50–35.40) |
36.45±2.78 (31.00–41.90) |
37.81±2.78 (32.36–43.26) |
S-BSS-N > G-BSS-N (p = 0.046) |
| GMax |
21.32±1.58 (18.22–24.43) |
16.25 ±1.58 (13.14–19.36) |
21.07±1.58 (17.96–24.17) |
16.23±1.58 (13.13–19.34) |
G-BSS-F > G-BSS-N (p = 0.024) S-BSS-F > S-BSS-N (p = 0.031) |
| BF |
20.98±1.89 (17.27–24.69) |
14.46±1.89 (10.75–18.18) |
23.09±1.89 (19.38–26.80) |
15.96±1.89 (12.25–19.68) |
G-BSS-F > G-BSS-N (p = 0.015) S-BSS-F > S-BSS-N (p = 0.008) |
| RF |
75.91±7.35 (61.49–90.33) |
52.22±7.35 (37.80–66.64) |
51.00±7.35 (36.58–65.42) |
68.02±7.35 (53.60–82.44) |
G-BSS-F > G-BSS-N (p = 0.023) |
| ST | 31.35±3.68 (24.13–38.58) |
41.00±3.68 (33.78–48.22) |
26.86±3.68 (19.64–34.08) |
33.66±3.68 (26.44–40.88) |
ns |
| VM | 187.28±33.68 (121.26–253.30) |
176.30±33.68 (110.28–242.32) |
207.54±33.68 (141.52–273.56) |
188.85±33.68 (122.83–254.87) |
ns |
| VL | 78.90±10.13 (59.03–98.76) |
104.71±10.13 (84.84–124.58) |
75.17±10.13 (55.30–95.03) |
88.81±10.13 (68.94–108.679 | ns |
| GMed | 27.26±5.75 (15.98–38.54) |
31.08±5.75 (19.80–42.36) |
26.49±5.75 (15.21–37.77) |
29.96±5.75 (18.68–41.24) |
ns |
G-BSS-F: ground-based Bulgarian split squat with trunk flexion; G-BSS-N: ground-based Bulgarian split squat with neutral trunk position; S-BSS-F: suspension-based Bulgarian split squat with trunk flexion; S-BSS-N: suspension-based Bulgarian split squat with neutral trunk position; ES: erector spinae; GMax: gluteus maximus; BF: biceps femoris; RF: rectus femoris; ST: semitendinosus; VM: vastus medialis; VL: vastus lateralis; GMed: gluteus medius; ns: non-significant differences (p > 0.05). P-values are based on pairwise comparisons derived from generalized estimating equations (GEE) with Bonferroni correction
GEE with Bonferroni-adjusted pairwise comparisons revealed the following statistically significant differences:
ES: Activation was significantly greater in S-BSS-N compared to G-BSS-N (p = 0.046).
GMax: Significantly higher activation was observed in G-BSS-F compared to G-BSS-N (p = 0.024) and in S-BSS-F compared to S-BSS-N (p = 0.031).
BF: Activation was significantly greater in G-BSS-F compared to G-BSS-N (p = 0.015) and in S-BSS-F compared to S-BSS-N (p = 0.008).
RF: Activation was significantly greater in G-BSS-F compared to G-BSS-N (p = 0.023).
No significant differences were observed in GMed, ST, VL, or VM across conditions (p > 0.05 for all). Fig. 3 provides a visual comparison of muscle activation levels across conditions, including 95% confidence intervals.
Fig. 3.

Normalized electromyographic (EMG) activation levels across Bulgarian split squat conditions. Activation levels are expressed as a percentage of maximal voluntary isometric contraction (%MVIC). Error bars indicate 95% confidence intervals (CI) of estimated marginal means from generalized estimating equations (GEE). ES: erector spinae; GMax: gluteus maximus; BF: biceps femoris; RF: rectus femoris; ST: semitendinosus; VM: vastus medialis; VL: vastus lateralis; GMed: gluteus medius. G-BSS-F: ground-based Bulgarian split squat with trunk flexion; G-BSS-N: ground-based Bulgarian split squat with neutral trunk position; S-BSS-F: suspension-based Bulgarian split squat with trunk flexion; S-BSS-N: suspension-based Bulgarian split squat with neutral trunk position
Discussion
The hypothesis that S-BSS would produce greater neuromuscular activation was only partially supported. While ES activity significantly increased only in S-BSS-N, no significant differences were observed in lower limb muscle activation. This finding suggests that postural instability, rather than trunk flexion, was the primary factor contributing to increased trunk stabilizer recruitment in trained female athletes. This interpretation aligns with biomechanical evidence indicating that exercises performed on unstable surfaces elicit greater activation of spinal stabilizing muscles, including the ES, compared to stable conditions [18].
The second hypothesis was more consistently supported: trunk flexion led to increased activation in posterior chain muscles, particularly the GMax and BF, across both G-BSS and S-BSS exercise conditions. GMax activation significantly increased under trunk-flexed conditions in both ground- and suspension-based exercises. This supports the biomechanical rationale that forward trunk inclination shifts the center of mass posteriorly, increases hip flexion angle, and enhances GMax recruitment—consistent with previous findings on trunk-flexed lunge and squat variations [9, 19].
BF activation followed a similar pattern, with significantly higher values observed during trunk-flexed conditions regardless of surface stability. As a biarticular muscle contributing to both hip extension and knee flexion, BF may become more active under increased posterior chain demand. The elevated activation likely reflects the need for greater hip extensor torque and pelvic stabilization during forward trunk inclination, corroborating earlier reports [9, 20].
Interestingly, RF activation increased only during ground-based exercises. The stable rear-foot support in G-BSS may have enabled more efficient anterior load transmission, promoting consistent quadriceps engagement In contrast, no significant activation changes were observed in VM, VL, GMed, or ST, suggesting that these muscles—likely playing stabilizing roles—were less responsive to sagittal-plane trunk or surface modifications. GMed’s role in frontal plane control, for example, may not be sufficiently challenged during the BSS.
With the increasing popularity of suspension exercises (SE), their neuromuscular demands continue to be explored. Previous studies have reported mixed results, with some showing increased muscle activation in SE and others observing no significant change in specific muscles [13, 20–22]. In the current study, only ES activation significantly increased under suspension-based conditions, aligning with research suggesting that core stabilizers are more responsive to unstable environments. This may also reflect the athletic profile of our participants, as trained individuals generally exhibit higher baseline neuromuscular control—especially in trunk stability [23]. Consequently, potential activation gains during instability-based training may be attenuated. Supporting this, Krause and Hollman [20] reported increased activation in various hip and thigh muscles in non-athletic populations during suspended lunges—effects not mirrored in our athletic sample. Similarly, Atkins et al. [21] noted only rectus abdominis activation increased in elite swimmers during suspended plank variations. Our results are further supported by Aguilera-Castells et al. [13], who found no significant activation differences in the lower extremities during traditional versus S-BSS. The elevated ES activation observed in our study may reflect increased postural control and balance demands that selectively engage deep trunk stabilizers under unstable conditions.
Trunk flexion during BSS significantly increased activation in GMax, BF, and RF but did not affect ES, ST, VL, VM, or GMed. Literature highlights the biomechanical influence of trunk angle on knee and hip loading. Increased trunk flexion enhances hamstring engagement and reduces anterior cruciate ligament ACL tension, potentially lowering injury risk [24, 25]. Kulas et al. [10] demonstrated that moderate trunk flexion (~ 40°) during single-leg squats reduced ACL loading, likely due to the shift in muscular demand from the quadriceps to the hamstrings.
Similar findings are reported in other functional exercises. Farrokhi et al. [9] showed greater GMax and BF activation during forward lunges with trunk flexion. Bezerra et al. [19] observed increased ES and GMax activity during dynamic lunges with trunk lean, while thigh muscle activation remained unchanged. In contrast, Krause et al. [20] reported increased BF activity but no changes in GMax, GMed, RF, or adductor longus in similar settings, suggesting exercise technique and population characteristics may influence outcomes.
This study had several limitations. First, the heterogeneous sport backgrounds of participants—including football, badminton, boxing, flag football, kickboxing, table tennis, and taekwondo—could have influenced EMG responses. Although these sports share core physical qualities such as anaerobic endurance and lower-limb strength, sport-specific neuromuscular adaptations may differ. Athletes engaged in unilateral or explosive movements (e.g., boxing, taekwondo) may display different recruitment strategies compared to those with repetitive loading patterns (e.g., football). Therefore, while the findings are informative for trained female athletes, they should not be overgeneralized across all sports disciplines. Future research should consider more homogeneous athletic populations to better elucidate sport-specific activation patterns.
Second, the absence of a non-athletic control group limits the generalizability of the results to untrained individuals. The study was specifically designed to explore neuromuscular responses in trained female athletes; however, including untrained individuals in future research may help distinguish training-related adaptations from baseline neuromuscular patterns. Third, the menstrual cycle phase of participants was not recorded. Hormonal fluctuations can affect neuromuscular control, joint laxity, and muscle stiffness, potentially influencing EMG amplitude and force output [26, 27]. Incorporating menstrual cycle tracking in future studies could improve the interpretation of muscle activation patterns in female athletes.
In summary, this study demonstrates that trunk position and surface stability elicit muscle-specific activation patterns during BSS. While suspension-based conditions enhance trunk muscle engagement, trunk flexion is more effective for activating posterior chain muscles. These findings may support coaches, physiotherapists, and exercise professionals in developing more targeted lower limb training strategies—particularly for female athletes. This is especially relevant given the increased susceptibility of women to ACL injuries, often linked to neuromuscular factors such as greater knee valgus angles and reduced hamstring–quadriceps co-activation. Exercises that emphasize trunk and posterior chain control—like those employed in the present study—may help improve neuromuscular control and potentially reduce injury risk in this population [28]. Moreover, the current findings could contribute to the design of clinical rehabilitation protocols and sport-specific strength programs aimed at enhancing trunk and posterior chain engagement to mitigate biomechanical risk. Nonetheless, due to the heterogeneity of the sample and the absence of a non-athletic control group, interpretations should remain cautious and specific to the studied context. Future studies are warranted to determine whether these acute EMG responses translate into long-term performance gains, reduced injury incidence, or sport-specific functional adaptations.
Acknowledgements
This study was presented as an e-poster at the 21st Congress of the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA), held in Milan, Italy, on May 8–10, 2024.
Author contributions
E.A.P. wrote the original draft and was responsible for conceptualization, methodology, investigation, data curation, and visualization. N.A.G. and N.K. contributed to conceptualization, methodology, supervision, investigation, and manuscript review. S.G. participated in methodology, investigation, and data curation. Y.P. contributed to methodology, data curation, visualization, and manuscript review. All authors reviewed and approved the final manuscript.
Funding
The authors reported there is no funding associated with the work featured in this article.
Data availability
The raw data underlying the findings of this study may be provided by the authors upon reasonably justified request.
Declarations
Ethics approval and consent to participate
All participants were informed of the study procedures and signed consent forms prior to participation. Ethical approval was obtained from the Gazi University Ethics Committee (approval number: 2021 − 1133, dated 07/12/2021). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for publication
Written informed consent for publication of personal and clinical details as well as identifying images was obtained from all participants.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.DiStefano LJ, et al. Comparison of integrated and isolated training on performance measures and neuromuscular control. J Strength Conditioning Res. 2013;27(4):1083–90. [DOI] [PubMed] [Google Scholar]
- 2.Jordan SL, et al. Core musculature co-contraction during suspension training exercises. J Bodyw Mov Ther. 2022;30:82–8. [DOI] [PubMed] [Google Scholar]
- 3.Pastucha D, et al. Clinical anatomy aspects of functional 3D training–case study. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012;156(1):63–9. [DOI] [PubMed] [Google Scholar]
- 4.Soligon SD, et al. Suspension training vs. traditional resistance training: effects on muscle mass, strength and functional performance in older adults. Eur J Appl Physiol. 2020;120:2223–32. [DOI] [PubMed] [Google Scholar]
- 5.Nowak A, et al. Effectiveness of resistance training with the use of a suspension system in patients after myocardial infarction. Int J Environ Res Public Health. 2020;17(15):5419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mok NW, et al. Core muscle activity during suspension exercises. J Sci Med Sport. 2015;18(2):189–94. [DOI] [PubMed] [Google Scholar]
- 7.Myer GD, Ford KR, Hewett TE. Rationale and clinical techniques for anterior cruciate ligament injury prevention among female athletes. J Athl Train. 2004;39(4):352. [PMC free article] [PubMed] [Google Scholar]
- 8.Zambarano E. Relationship between Lumbo-pelvic-hip complex muscle activation and lower limb biomechanics during functional tasks before and after fatigue. The University of Toledo; 2019.
- 9.Farrokhi S, et al. Trunk position influences the kinematics, kinetics, and muscle activity of the lead lower extremity during the forward lunge exercise. J Orthop Sports Phys Therapy. 2008;38(7):403–9. [DOI] [PubMed] [Google Scholar]
- 10.Kulas AS, Hortobágyi T, DeVita P. Trunk position modulates anterior cruciate ligament forces and strains during a single-leg squat. Clin Biomech Elsevier Ltd. 2012;27(1):16–21. [DOI] [PubMed] [Google Scholar]
- 11.Appleby BB, Cormack SJ, Newton RU. Specificity and transfer of lower-body strength: influence of bilateral or unilateral lower-body resistance training. J Strength Conditioning Res. 2019;33(2):318–26. [DOI] [PubMed] [Google Scholar]
- 12.Coratella G, et al. The activation of gluteal, thigh, and lower back muscles in different squat variations performed by competitive bodybuilders: implications for resistance training. Int J Environ Res Public Health. 2021;18(2):772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aguilera-Castells J, et al. Muscle activity of Bulgarian squat. Effects of additional vibration, suspension and unstable surface. PLoS ONE. 2019;14(8):e0221710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Boudreau SN, et al. Hip-muscle activation during the lunge, single-leg squat, and step-up-and-over exercises. J Sport Rehabilitation. 2009;18(1):91–103. [DOI] [PubMed] [Google Scholar]
- 15.Mausehund L, Skard AE, Krosshaug T. Muscle activation in unilateral barbell exercises: implications for strength training and rehabilitation. J Strength Conditioning Res. 2019;33:S85–94. [DOI] [PubMed] [Google Scholar]
- 16.Knoll MG, et al. Comparisons of single leg squat variations on lower limb muscle activation and center of pressure alterations. Int J Exerc Sci. 2019;12(1):950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Miller WM, et al. Comparison of myoelectric activity during a suspension-based and traditional split squat. J Strength Conditioning Res. 2019;33(12):3236–41. [DOI] [PubMed] [Google Scholar]
- 18.Imai A, et al. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J Orthop Sports Phys Therapy. 2010;40(6):369–75. [DOI] [PubMed] [Google Scholar]
- 19.Bezerra EDS, et al. Influence of trunk position during three lunge exercises on muscular activation in trained women. Int J Exerc Sci. 2021;14(1):202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Krause DA, Hollman JH. Electromyographic analysis of hip muscle activation during a single limb squat lateral slide exercise. Int J Sports Phys Therapy. 2020;15(5):755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Atkins SJ, et al. Electromyographic response of global abdominal stabilizers in response to stable-and unstable-base isometric exercise. J Strength Conditioning Res. 2015;29(6):1609–15. [DOI] [PubMed] [Google Scholar]
- 22.Byrne JM, et al. Effect of using a suspension training system on muscle activation during the performance of a front plank exercise. J Strength Conditioning Res. 2014;28(11):3049–55. [DOI] [PubMed] [Google Scholar]
- 23.Malm C, Jakobsson J, Isaksson A. Physical activity and sports—real health benefits: a review with insight into the public health of Sweden. Sports. 2019;7(5):127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li G, et al. The importance of quadriceps and hamstring muscle loading on knee kinematics and in-situ forces in the ACL. J Biomech. 1999;32(4):395–400. [DOI] [PubMed] [Google Scholar]
- 25.Ohkoshi Y, et al. Biomechanical analysis of rehabilitation in the standing position. Am J Sports Med. 1991;19(6):605–11. [DOI] [PubMed] [Google Scholar]
- 26.Martínez-Fortuny N, et al. Menstrual cycle and sport injuries: a systematic review. Int J Environ Res Public Health. 2023;20(4):3264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Soedirdjo SD, et al. Sex hormone-mediated change on muscle activation deactivation dynamics in young eumenorrheic women. Front Physiol. 2023;14:1104578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ramezani F, Saki F, Tahayori B. Neuromuscular training improves muscle co-activation and knee kinematics in female athletes with high risk of anterior cruciate ligament injury. Eur J Sport Sci. 2024;24(1):56–65. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The raw data underlying the findings of this study may be provided by the authors upon reasonably justified request.