

Abstract
Left unaddressed, NAFLD will continue to have substantial health, economic and social implications. To address the challenge, a paradigm shift is needed in the way NAFLD is conceptualised. Concerted, collaborative action across medical specialities, industry sectors and governments will be vital to tackling this public health threat. To drive this change, in this review, we present current global healthcare and socioeconomic costs for NAFLD and highlight priority actions to take. The estimated healthcare costs of patients with NAFLD are nearly twice as high as their age-matched counterparts without the disease and are highest in advanced fibrosis and end-stage liver disease. NAFLD is accountable for the highest increase in disability-adjusted life years (DALYs) among all liver diseases globally. NAFLD and NASH-specific drug therapies are not available and there is considerable uncertainty regarding the cost, optimal length of treatment, impact on liver-related outcome and mortality. Among the currently available bariatric procedures, sleeve gastrectomy is reported to be the most cost-effective for NASH resolution. Gastric bypass remains very expensive, while data on bariatric endoscopy are limited. Lastly, we propose a global NAFLD/NASH investment framework to guide the development of achievable yet ambitious country-specific targets and strategic actions to optimise resource allocation and reduce the prevalence of NAFLD and NASH. Its focus on high-level inputs will be critical to enabling a political and financial environment that supports clinical-level implementation of NAFLD prevention, treatment and care efforts, across all settings.
Keywords: NAFLD, Healthcare costs, Socioeconomic costs
Introduction
Non-alcoholic fatty liver disease (NAFLD), which is characterised by excess fat in the liver, is an increasingly prevalent chronic liver disease, often as a result of obesity1. Non-alcoholic steatohepatitis (NASH) is the histologic phenotype of NAFLD characterised by liver injury (inflammation and ballooning) in addition to steatosis. In contrast to simple steatosis, NASH is more rapidly progressive to cirrhosis and complications2. NASH is the second most common indication for liver transplantation in the United Kingdom and the USA3, 4 and an important cause of liver cancer5. A multisystem disease, NAFLD is an independent risk factor for several comorbidities, such as type 2 diabetes (T2D)6, hypertension and dyslipidemia7, 8. In the USA, the life expectancy of people with NAFLD is four years lower than their age-matched counterparts8, 9. The most common causes of death include cardiovascular events, extrahepatic cancers and cirrhosis-related complications10, 11.
Consequent to increasing prevalence and associated diseases, the healthcare and economic burden of NAFLD is substantial12. The cost of care for NAFLD patients is nearly twice as high as those without the disease, likely due to multiple factors including testing, monitoring and hospitalisation13. Additionally, there is an indirect societal impact subsequent to early mortality, absenteeism, caregiver burden, as well as reduced health-related quality of life14. The lack of effective and sustainable therapeutic interventions to halt disease progression, reduce comorbidities and mortality make this a major healthcare problem worldwide.
While NAFLD is closely related to obesity, diabetes and cardiovascular disease, the public health and health systems responses to the issue have been weak and fragmented. In this review, we summarise the healthcare and economic burden of NAFLD and discuss the challenges posed by the increasing prevalence worldwide. We highlight the gaps in research, uncertainties related to the future management and treatment, and the need for a global framework and national action plans in tackling this condition to decrease the global burden of disease on health systems and the economy.
Healthcare Costs of NAFLD
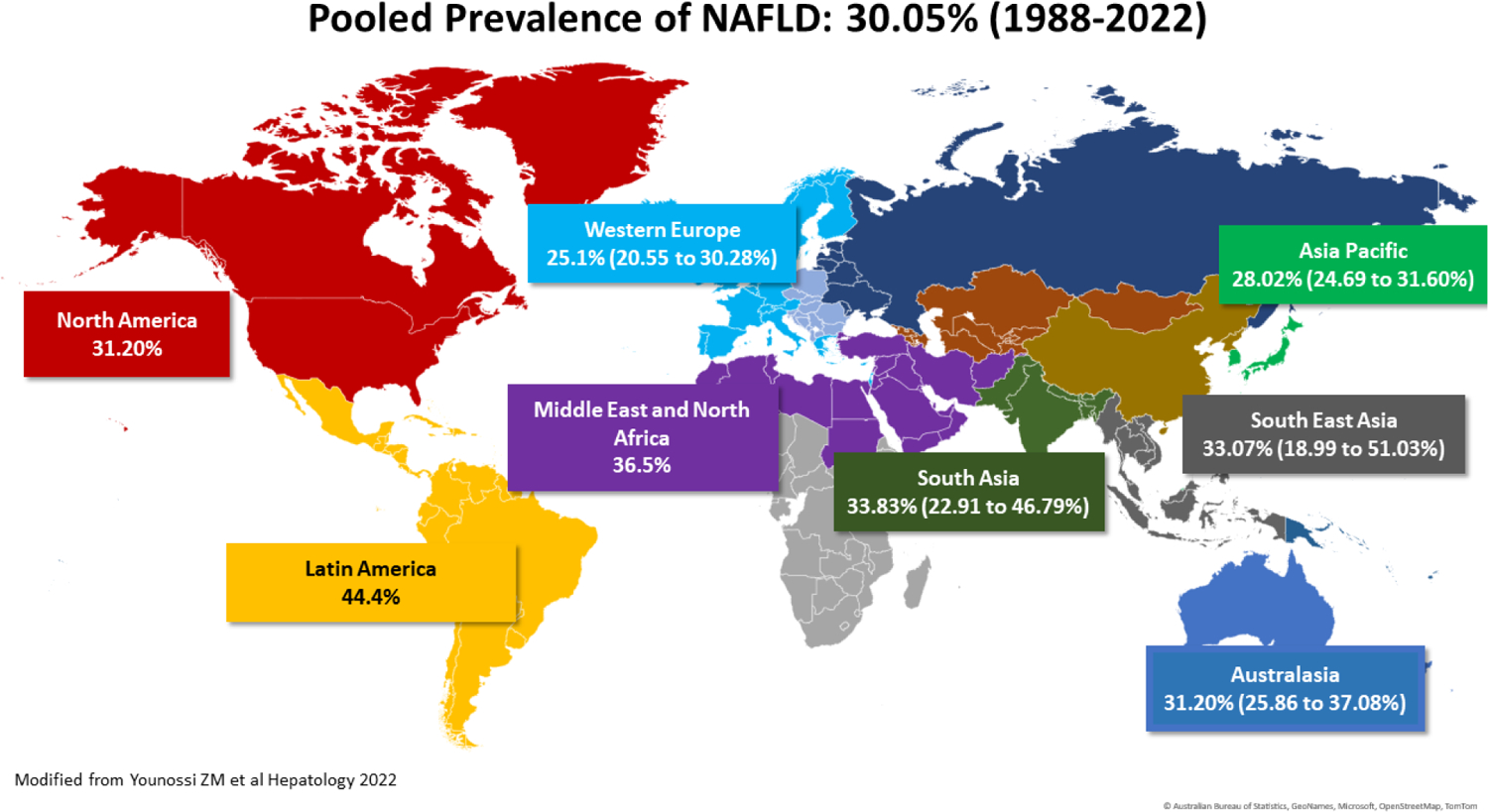
The global NAFLD prevalence over the last 4 decades is estimated to be 30%, with rates between 44% in Latin America and 28% in Asia Pacific (Figure 1). The prevalence has increased from 24% in 1991–2006 to 38% in 2021 and is projected to continue to rise15–22(Figure 2). Type 2 diabetes and obesity are closely associated with a higher risk of NAFLD. Globally, it is estimated that 55–70% of people with T2D have NAFLD, 30–60% have NASH and 12–20% have clinically significant fibrosis (stage ≥2)16, 23. Likewise, approximately 75–80% of patients undergoing bariatric surgery for weight loss have NAFLD proven by imaging and liver biopsy24, 25. Healthcare cost estimates available in literature differ by region, country, disease phenotype (NAFLD vs NASH), database and methodology, but they are uniformly high when compared to individuals without the disease or with T2DM and unclear NAFLD status. In the US, the lifetime cost of care for all patients with NASH was estimated around US $222 billion in 201714.
Figure 1.

Global NAFLD prevalence (1998–2022)
Figure 2.
Increasing NAFLD prevalence over time
A recent model developed by Younossi et al, investigated the economic costs of NASH in the U.S. by obesity status26. Using a discrete-time Markov model which involved patients with NASH who were allowed to move through 9 health states and 3 absorbing death states (liver, cardiac, and other deaths) with 1-year cycles and 20-year horizon in which the transition probabilities were estimated from literature and population-based data, the investigators found that for the U.S, NASH cases were forecasted to increase by 82.6%, from 11.61 million (2020) to 19.53 million (2039). During the same period, they also found that cases of advanced liver disease will increase by 77.9%, from 1.51 million to 2.67 million. However, overall, the proportion of NASH cases within the NAFLD population will remain approximately the same at 13% indicating that the rate of NASH is not accelerating over time but growing in proportion to NAFLD cases. The projected cumulative estimated direct healthcare costs were reported as 1,208.47 billion USD for those patients who were obese and had NASH while for those with NASH but who were not obese, the costs were reported to be 453.88 billion USD. By 2039, the projected NASH attributable healthcare cost per patient was reported to increase from 3,636 USD to 6,968 USD, with the increase most likely driven by the growing number of patients with NASH and advanced fibrosis.
In Europe the total NASH-related costs ranged between €8548-19 546M in 201827. Of these, health system costs were €619–1292M, while wellbeing costs (which measure costs associated with DALYs) were €41 536–90 379M. Other studies estimate an annual cost of about €35 billion (from €354 to €1,163 per patient) in Europe and $103 billion ($1,613 per patient) in the US12. In a more recent study from Europe and US from 2018, the mean total annual per patient cost of NASH was €2,763, €4,917, and €5,509 for direct medical, direct non-medical, and indirect costs, respectively28. Per patient cost was estimated to be the highest in the US and the lowest in France.
Another modeling study assessing cost of NASH was conducted in Hong Kong29. This study suggested the total costs of NASH to be $1.32 billion (USD) with an average per person cost of $257. In addition, the study suggested that the costs of NASH in 2017–2018 accounted for 0.41% of Hong Kong’s total health expenditures.
In an analysis of a large US-based insurance claims database, the annual cost of longitudinal care per NAFLD patient is significantly higher than controls matched by age, sex, presence of diabetes, hypertension, dyslipidemia, cardiovascular disease and length of follow-up ($3,789 versus $2,298)13. Importantly, the cost is even higher around first NAFLD diagnosis ($7,804). The largest increases in healthcare utilisation which may account for the increased costs were represented by imaging, hospitalisations, liver biopsies, laboratory tests and outpatient office visits. Hospitalisations of patients with NAFLD have tripled in the US between 2007–201430, especially among men, Hispanics and government insured patients. Similarly, healthcare costs were nearly twice as high in patients with NAFLD than matched controls in cohorts from Sweden31, Italy32, Germany33, France34 and Spain35. It is important to note that the independent impact of NAFLD on healthcare costs was not consistently analysed in all studies and the contribution of metabolic comorbidities could contribute to an overestimation of the economic burden of the disease. This potential confounding is an important limitation to be considered in the design of future studies.
Moreover, there are substantial discrepancies between the cost estimates in the European versus US studies. Whereas some regional variations are expected, the large inconsistencies are more likely a result of differences in assumptions used in the models. We call for standardisation of transition rates between disease stages, utility scores, resource utilisation estimates, and their consistent use in different models to eliminate uncertainty.
A common finding of all studies is that the care is more expensive in advanced stages, likely due to the evaluation and management of complications related to end-stage-liver disease, including hospitalisations. Early detection is crucial for timely intervention to prevent disease progression and could ultimately have an impact on decreasing socioeconomic costs. Therefore, rational utilisation of healthcare resources to detect the small proportion of those who are at risk for fibrosis in the general population is critical, and this will require the implementation of clinical care pathways that are not only feasible, efficient and accessible but also cost-effective. Several strategies for proactive case finding have been recommended, most of which include sequential testing with blood-based biomarkers followed by elastography36,37. However, there is considerable heterogeneity in these approaches between regions, countries and even practice settings38. Several models have demonstrated that a sequential approach using FIB-4 or the NAFLD fibrosis score, followed by elastography (vibration-controlled transient elastography or magnetic resonance elastography), are cost-effective, especially when used in high-risk populations such as those with T2DM or obesity, and could avert a significant number of liver biopsies, resulting in systemic cost-savings and QALYs gain39–45. The development of optimal screening strategies for NAFLD with fibrosis in primary care and community settings remains a critical research focus48, 49. In the absence of effective medications leading to NASH resolution or fibrosis improvement, early detection strategies for NASH fibrosis will have to evidence that they improve long term outcomes through the facilitation early weight loss intervention and the management of metabolic risk factors. Nevertheless, given the high disease prevalence, it is becoming increasingly clear that NAFLD identification and management requires multidisciplinary efforts and implementation of models of care that combine primary care physicians, hepatologists, endocrinologists, weight management specialists, dieticians and others.
Socioeconomic costs indirectly associated with NAFLD
In addition to the direct health care costs, the total economic costs include the indirect effect of premature mortality and disability resulting from NAFLD and related complications, commonly assessed through disability-adjusted life years (DALYs). In an analysis of the Global Burden of Disease data from 2007–2017, NAFLD was the most rapidly growing contributor to liver mortality and morbidity1. NAFLD was responsible for 6–17% of liver-cancer related death globally (with a 26% increase), 9% of the global cases of cirrhosis (with a 15% increase) and the highest increase in DALYs. Among the world regions, Asia accounted for 48% of the global incidence in liver-related complications from NAFLD and 46% of NAFLD-related death, with a 2% annual percent change increase in DALYs48. Similar trends were seen in the United States, where the highest increase in death rates and years of life lost from cirrhosis and HCC were due to alcohol-related liver disease, followed by NAFLD9. It remains unclear whether the impact on DALYs is solely attributable to NAFLD, especially in early stages, as most studies which have not focused on cirrhosis and HCC have not adjusted for all possible associated confounders beyond age. It is likely that metabolic comorbidities can contribute to the disability estimation, and these should be considered in future study designs.
In addition, patients with NASH experience worse health-related quality of life (HRQL), lower productivity and increased healthcare utilization when compared to the general population and individuals with T2DM after matching for confounders49. The indirect economic impact of NAFLD related to impairment of HRQL and work productivity can add to the direct economic burden of NAFLD, leading to substantial societal costs.
Socioeconomic inequalities and NAFLD
Globally, low socioeconomic status (SES) is associated with greater mortality50–52. An individual’s sociocultural and economic context directly influences their lifestyle, environment and access to health systems, which in turn impact the risk of morbidity, which in turn negatively affects the socioeconomic system at the individual and population levels53.
Studies of SES in NAFLD are scarce but the topic has received increasing attention in recent years. Socially disadvantaged populations have a higher risk of NAFLD and related complications54–57. In a recent analysis of US the National Health and Nutrition Examination Survey (NHANES) database in 2017–2018, high-quality diet, increased physical activity and college education were associated with a lower risk of hepatic steatosis by VCTE54. Food insecurity may be an independent predictor of NAFLD and advanced fibrosis among low-income adults58–60. Processed meat consumption61 and inadequate physical activity62 are independent predictors of NAFLD. In children, community socioeconomic deprivation was associated with younger age at NALFD diagnosis, but not with NAFLD severity63. Children in low SES have a higher prevalence of obesity, higher added sugar intake, such as sweets and soft drinks, and lower fruit and vegetable intake64. In the US, lack of health insurance is associated with higher risk of death in those hospitalised with NAFLD30.
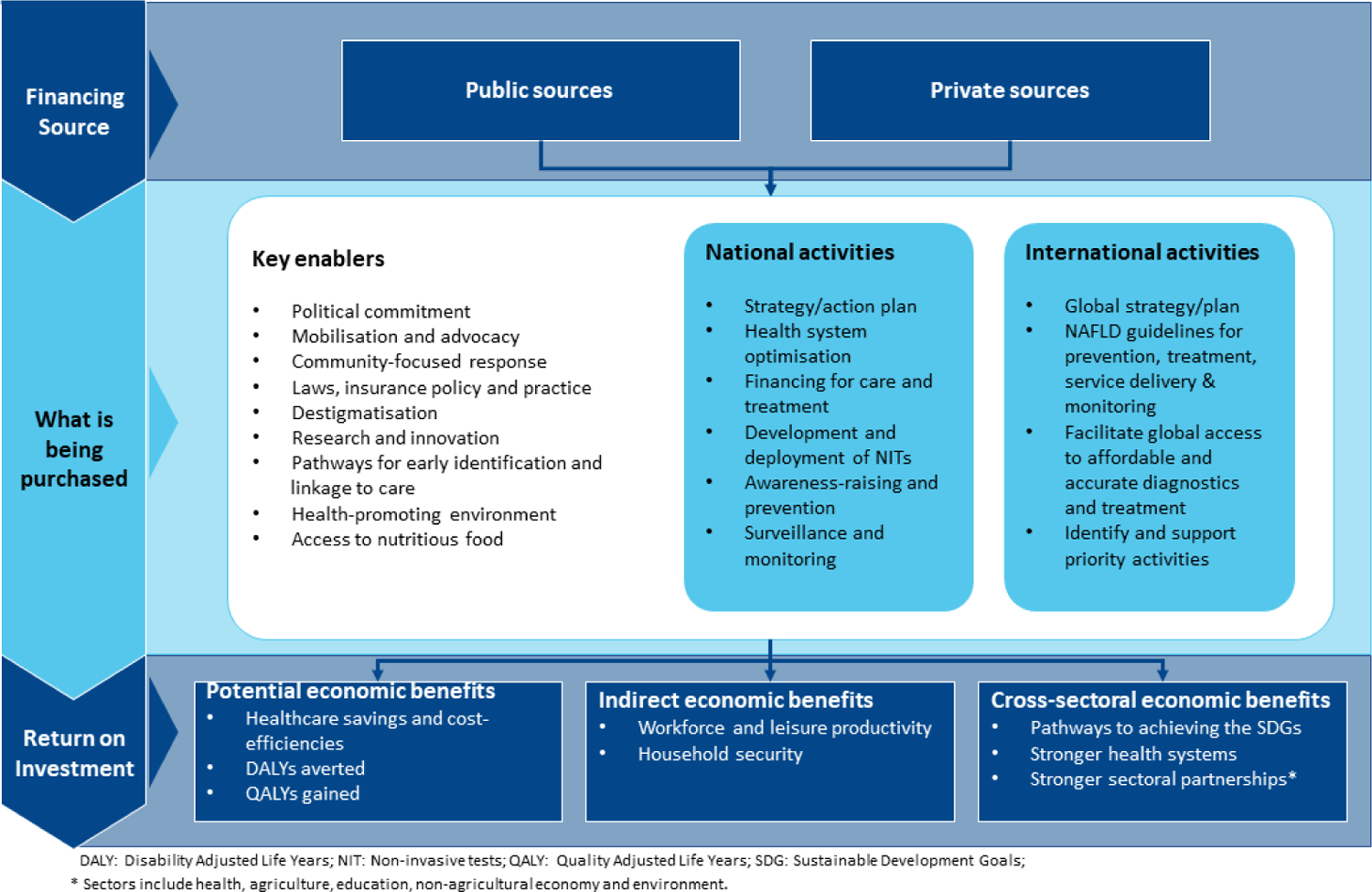
Elements of SES are intertwined, and the distinction between their level of contribution can be difficult. For example, higher income allows for a healthier diet, more physical activity, increased self-care, and access to high-quality healthcare. Given this relationship between SES and health, health strategies to decrease NAFLD burden should target these inequalities65. Current international efforts such as the Sustainable Development Goals (SDGs) and the WHO European Action Plan 25×25 health plan (25% decrease in mortality from major noncommunicable diseases (NCDs) by 2025)66 promote these components at the population level, such as universal access to a nutritious diet, education, walkable environments, and high quality healthcare. As NAFLD is not included in the aforementioned initiatives, a NAFLD-specific framework, using 16 SDG targets and 7 indicators, has been developed to place NAFLD in the global, multisectoral context, similar to other NCDs67. These include health, agriculture, education, the economy and the environment (Figure 3). This framework can be used to prioritise strategies and identify context-specific policies and intervention to decrease healthcare and socioeconomic costs.
Figure 3.
Proposal for a global NAFLD/NASH investment framework
Treatment costs
Treatment of NAFLD remains a major challenge in the absence of approved therapies to date. Current methods vary in effectiveness, invasiveness and cost. Life-style changes in dietary choices and physical activity are effective interventions for NASH resolution, fibrosis regression68, portal hypertension69 and the likelihood of needing a liver transplant70, which can likely be adopted at lower cost than invasive interventions. However, they are unlikely to have a large impact on the burden of NAFLD, because less than 10% of individuals achieve and maintain sufficient weight loss68. The most effective intervention to date is bariatric surgery, which is more expensive, but can lead to sustainable NASH resolution in 84%, and fibrosis regression in 70% of patients at five years71, 72 and reduce liver-related and major cardiovascular events73. An economic evaluation using a Markov-based state-transition model to simulate the impact of sleeve gastrectomy, Roux-en-Y gastric bypass, and intensive lifestyle intervention in patients with NASH and compensated cirrhosis suggests that bariatric surgery could be highly cost-effective compared to usual care. While sleeve gastrectomy is cost-effective across all classes of obesity, with an incremental cost-effectiveness ratio (ICER) raging between $18716 (for mild obesity) and $6563 (for severe obesity) per quality-adjusted life year (QALY). However, the cost of gastric bypass would have to decrease by $2289 (for mild obesity) to $4489 (for severe obesity) to meet the cost-effectiveness threshold of $100 000 per QALY74. Both gastric bypass and sleeve gastrectomy can lead to an increase in QALYs in patients with NASH and cirrhosis when compared to standard of care74. It is important to note that in patients with cirrhosis the choice for surgical weight loss approaches should be made after careful evaluation of risks based on hepatic function and presence of portal hypertension, irrespective of BMI.
Endoscopic interventions for weight loss, such as endoscopic sleeve gastroplasty, are safe and effective novel interventions that can complement lifestyle modifications for management of class 1 and 2 obesity, but their role in NASH treatment remains to be demonstrated75. Other methods, such as intragastric balloon placement show promising results for NASH resolution and fibrosis improvement in 50% of patients76. Cost-effectiveness studies with long-term follow-up to assess for sustainability of results are needed to determine the role of these interventions in NASH management.
There are several investigational drugs under evaluation for safety and efficacy in NASH, a few of which have reached phase 377. Some of these agents, such as the glucagon-like peptide-1 (GLP-1) receptor agonist semaglutide, and the dual glucose-dependent insulinotropic polypeptide and GLP-1 receptor agonist tirzepatide have been approved as weight loss and type 2 DM therapies, and their cost-effectiveness in NASH remains to be determined. The current investigational efficacy endpoints for accelerated approval in NASH are based on histological improvement of fibrosis and resolution of NASH. However, it remains unclear whether these surrogate endpoints will translate to a decreased risk of cirrhosis and related complications, fewer comorbidities and better quality of life. More importantly, the appropriate length of treatment beyond the trial period remains uncertain. Whether treatment will be applied for a finite time until NASH resolution is achieved or given as lifelong maintenance, akin to diabetes or hypertension, will have huge implications on lifetime costs. For example, a 2-year treatment with a drug that results in NASH resolution followed by long-term maintenance of this histologic endpoint might be superior to a short-term treatment that reduces fibrosis but may not eliminate the risk of future disease progression after discontinuation78. Furthermore, metabolic drugs that favorably impact the cardiovascular risk by reducing insulin resistance and weight might have a greater impact on mortality and morbidity than those with antifibrotic or antiinflammatory mechanism of action.
In another simulation of a cohort with 21-year life expectancy, for a pharmaceutical intervention to be considered cost-effective in reducing fibrosis and mortality, annual drug cost should not exceed $12,000. For an annual cost of $36,000 for example, the ICER would be $2,517,676/QALY gained, which exceeds an economically justifiable price79.
Gaps in NAFLD global cost estimates
Most of the data reporting the healthcare and economic costs associated with NAFLD come from Europe, Hong Kong and USA, leaving a large gap in estimation of the global situation. Existing data cannot be extrapolated due to substantial heterogeneity in populations, health systems, costs, practice patterns, access to quality testing and care between and within countries, especially between low- and high-income settings. Therefore, data generation from all regions of the world is critical, as action plans to reduce the care costs and prevalence need to be developed and prioritised based on country and sub-national-specific evidence. This heterogeneity has been found in other key comorbid conditions such as T2DM80 and cardiovascular disease81.
Some of the strongest evidence is from the Organisation for Economic Co-operation and Development (OECD), which has developed models that show positive effects of heath policies on economic metrics in liver diseases of all causes in the 27 European Union member states plus Iceland, Norway, Russia, Switzerland and the United Kingdom, for the period 2020–2050. Policy interventions such as food reformulation, alcohol pricing and taxation are among the most effective in improving health expenditure, years of life lost, DALYs and workforce productivity, with an estimated €31 billion in potential economic gains82. Similar investment studies that systematically estimate the potential impact of policy interventions in lowering costs should be developed for NAFLD, to identify which actions are cost-effective and their returns on investment, in order to develop policies with net benefit.
A call for a NAFLD/NASH investment framework
Assessing the socioeconomic and healthcare burden of NAFLD is a necessary first step in understanding and subsequently reducing the magnitude of the problem. Almost no country globally has a written strategy for addressing the disease83, while it is absent from key global policies, including the World Health Organization’s Global Action Plan for the Prevention and Control of Non-Communicable Diseases (NCDs). To address the challenge of growing prevalence and further increasing costs, a first step is to develop a NAFLD/NASH investment framework, consisting of policies and other actions to guide an efficient policy response. Such a framework should focus on the high-level inputs that are critical to enabling a political and financial environment that support country-level implementation of NAFLD/NASH strategies, across all settings. Similar disease-specific investment cases, using real world case studies and modelling, have already been developed for HIV84, obesity85, diabetes86, viral hepatitis B87, C88–90 and other conditions. We believe that a NAFLD-specific investment framework is essential in addressing liver-related goals as they are not included in those developed for obesity or diabetes. This should incorporate activities such as increasing awareness of liver disease in those with risk factors, the use of NITs to identify those at high risk for fibrosis, optimisation of clinical care pathways which include efficient diagnosis, referral strategies and longitudinal monitoring, in addition to aspects of NASH-related therapeutics that are expected to be approved in the near future. These issues are not currently addressed in investment frameworks of other diseases and essential in NAFLD management and the ultimate goal of decreasing the burden of liver disease and related complications. A NAFLD/NASH-specific investment framework can identify key synergies between prevention and treatment strategies and opportunities to progress towards the Sustainable Development Goals (SDGs) and achieve universal health coverage, which is central to the SDGs and in line with global health priorities set by WHO.
Conclusions
The chronic and long-term nature of NAFLD, the multiple associated comorbidities and costs, and the lack of effective therapies to stop fatty liver disease progression or improve outcomes present particular healthcare and socioeconomic challenges. It is imperative to mobilise efforts to place fatty liver disease on the global health and development agenda, create action plans to implement cost-effective patient care pathways for disease identification at an early stage, and to address social, economic and environmental determinants of health. Given the high and increasing prevalence of NAFLD and the lack of national and global strategies, coordinated, transformative efforts are needed on how to mitigate non-sustainable escalating costs and expected disparities between and within countries. We propose developing a global fatty liver disease investment framework that sets out achievable yet ambitious country-specific targets and strategic actions to optimise resource allocation and embed these within the United Nations’ Sustainable Development Goals. Such solutions to the global NAFLD burden should be framed as a matter of whole-of-society responsibility and not solely that of a provider or patient.
Key points.
The estimated healthcare costs associated with NAFLD and NASH are high and estimated to increase in the regions where modeling has been applied: United States, Europe and Hong Kong, whereas there is a gap in assessment in the other regions.
The costs, mostly arising from testing and hospitalisations, are highest in advanced fibrosis and end-stage liver disease.
Very few studies have analysed the impact of NAFLD/NASH on healthcare costs independent of metabolic comorbidities, which can contribute to an overestimation.
Globally, among all causes of liver disease, NAFLD is accountable for the highest increase in disability-adjusted life years (DALYs).
Socioeconomic disadvantage is associated with higher risk of NAFLD and disease progression, which in turn exacerbate the economic burden.
Cost-effectiveness estimates of drug therapies remain uncertain in the absence of approved treatments with impact on liver events and mortality.
Modeling in patients with NASH cirrhosis estimate sleeve gastrectomy to be the most cost-effective among bariatric surgery procedures when compared to intensive life-style interventions.
To address the challenge of increasing prevalence and healthcare costs, we call for an investment framework to raise the profile of NAFLD/NASH and yield significant cost-efficiencies by guiding decision-makers on which actions should be implemented.
Conflict of Interest:
AMA received funding to her institution from Pfizer, Novo Nordisk, and Target Pharma and serves on an advisory board and as a consultant for Novo Nordisk. JVL reports grants to his institution from AbbVie, Gilead Sciences, MSD and Roche and personal fees from AbbVie, CEPHEID, Gilead Sciences, GSK, Genfit, Intercept, Janssen, MSD, Novo Nordisk, Novavax and ViiV, all outside of the submitted work. ZMY: Abbott, Astra Zeneca, Bristol-Myers Squibb, Gilead Sciences, Intercept, Madrigal, Merck, NovoNordisk, and Siemens Healthineers.
Financial support statement:
AMA is supported by the following National Institute of Health Grants: DK115594 and DK128127
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- 1.Paik JM, Golabi P, Younossi Y, Mishra A Younossi ZM Changes in the Global Burden of Chronic Liver Diseases From 2012 to 2017: The Growing Impact of NAFLD. Hepatology 2020;72:1605–1616. [DOI] [PubMed] [Google Scholar]
- 2.Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015;13:643–54.e1–9; quiz e39–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Noureddin M, Vipani A, Bresee C, Todo T, Kim IK, Alkhouri N et al. NASH Leading Cause of Liver Transplant in Women: Updated Analysis of Indications For Liver Transplant and Ethnic and Gender Variances. Am J Gastroenterol 2018;113:1649–1659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Younossi ZM, Stepanova M, Ong J, Trimble G, AlQhatani S, Younossi I et al. Nonalcoholic Steatohepatitis Is the Most Rapidly Increasing Indication for Liver Transplantation in the United States. Clin Gastroenterol Hepatol 2021;19:580–589.e5. [DOI] [PubMed] [Google Scholar]
- 5.Fitzmaurice C, Abate D, Abbasi N, Abbastabar H, Abd-Allah F, Abdel_Rahman O et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol 2019;5:1749–1768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mantovani A, Petracca G, Beatrice G, Tilg H, Byrne CD, Targher G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: an updated meta-analysis of 501 022 adult individuals. Gut 2021;70:962–969. [DOI] [PubMed] [Google Scholar]
- 7.Lonardo A, Nascimbeni F, Mantovani A, Targher G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J Hepatol 2018;68:335–352. [DOI] [PubMed] [Google Scholar]
- 8.Allen AM, Therneau TM, Larson JJ, Coward A, Somers VK, Kamath PS. Nonalcoholic fatty liver disease incidence and impact on metabolic burden and death: A 20 year-community study. Hepatology 2018;67:1726–1736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Paik JM, Golabi P, Biswas R, Alqatani S, Venkatesan C, Younossi ZM. Nonalcoholic Fatty Liver Disease and Alcoholic Liver Disease are Major Drivers of Liver Mortality in the United States. Hepatol Commun 2020;4:890–903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kim D, Kim WR, Kim HJ, Therneau TM. Association between noninvasive fibrosis markers and mortality among adults with nonalcoholic fatty liver disease in the United States. Hepatology 2013;57:1357–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mantovani A, Petracca G, Beatrice G, Csermely A, Tilg H, Byrne CD et al. Non-alcoholic fatty liver disease and increased risk of incident extrahepatic cancers: a meta-analysis of observational cohort studies. Gut 2022;71:778–788. [DOI] [PubMed] [Google Scholar]
- 12.Younossi ZM, Blissett D, Blissett R, Henry L, Stepanova M, Younossi Y et al. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology 2016;64:1577–1586. [DOI] [PubMed] [Google Scholar]
- 13.Allen AM, Van Houten HK, Sangaralingham LR, Talwalkar JA, McCoy RG. Healthcare Cost and Utilization in Nonalcoholic Fatty Liver Disease: Real-World Data From a Large U.S. Claims Database. Hepatology 2018;68:2230–2238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Younossi ZM, Tampi R, Priyadarshini M, Nader F, Younossi IM, Racila A Burden of Illness and Economic Model for Patients With Nonalcoholic Steatohepatitis in the United States. Hepatology 2019;69:564–572. [DOI] [PubMed] [Google Scholar]
- 15.Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73–84. [DOI] [PubMed] [Google Scholar]
- 16.Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol 2019;71:793–801. [DOI] [PubMed] [Google Scholar]
- 17.Younossi Z, Tacke F, Arrese M, Chander Sharma B, Mostafa I, Bugianesi E et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019;69:2672–2682. [DOI] [PubMed] [Google Scholar]
- 18.Riazi K, Azhari H, Charette JH, Underwood FE, King JA, Afshar EE et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2022;7:851–861. [DOI] [PubMed] [Google Scholar]
- 19.Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol 2018;69:896–904. [DOI] [PubMed] [Google Scholar]
- 20.Estes C, Razavi H, Loomba R, Younossi ZM, Sanyal AJ. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018;67:123–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Adams LA, Roberts SK, Strasser SI, Mahady SE, Powell E, Estes C et al. Nonalcoholic fatty liver disease burden: Australia, 2019–2030. J Gastroenterol Hepatol 2020;35:1628–1635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Estes C, Chan HLY, Chien RN, Chuang WL, Fung J, Goh GB et al. Modelling NAFLD disease burden in four Asian regions-2019–2030. Aliment Pharmacol Ther 2020;51:801–811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stefan N, Cusi K. A global view of the interplay between non-alcoholic fatty liver disease and diabetes. Lancet Diabetes Endocrinol 2022;10:284–296. [DOI] [PubMed] [Google Scholar]
- 24.Allen AM, Shah VH, Therneau TM, Venkatesh SK, Mounajjed T, Larson JJ et al. The Role of Three-Dimensional Magnetic Resonance Elastography in the Diagnosis of Nonalcoholic Steatohepatitis in Obese Patients Undergoing Bariatric Surgery. Hepatology 2020;71:510–521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Soresi M, Cabibi D, Giglio RV, Martorana S, Guercio G, Porcasi R et al. The Prevalence of NAFLD and Fibrosis in Bariatric Surgery Patients and the Reliability of Noninvasive Diagnostic Methods. Biomed Res Int 2020;2020:5023157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Younossi ZM, Paik JM, Henry L, Yang J, Fernandes G, Stepanova M et al. The Growing Economic and Clinical Burden of Nonalcoholic Steatohepatitis (NASH) in the United States (U.S.). Journal of Clinical and Experimental Hepatology 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schattenberg JM, Lazarus JV, Newsome PN, Serfaty L, Aghemo A, Augustin S et al. Disease burden and economic impact of diagnosed non-alcoholic steatohepatitis in five European countries in 2018: A cost-of-illness analysis. Liver Int 2021;41:1227–1242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.O’Hara J, Finnegan A, Dhillon H, Ruiz-Casas L, Pedra G, Franks B et al. Cost of non-alcoholic steatohepatitis in Europe and the USA: The GAIN study. JHEP Rep 2020;2:100142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tampi RP, Wong VW, Wong GL, Shu SS, Chan HL, Fung J et al. Modelling the economic and clinical burden of non-alcoholic steatohepatitis in East Asia: Data from Hong Kong. Hepatol Res 2020;50:1024–1031. [DOI] [PubMed] [Google Scholar]
- 30.Adejumo AC, Samuel GO, Adegbala OM, Adejumo KL, Ojelabi O, Akanbi O et al. Prevalence, trends, outcomes, and disparities in hospitalizations for nonalcoholic fatty liver disease in the United States. Ann Gastroenterol 2019;32:504–513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hagström H, Nasr P, Ekstedt M, Hammar U, Widman L, Stål P et al. Health Care Costs of Patients With Biopsy-Confirmed Nonalcoholic Fatty Liver Disease Are Nearly Twice Those of Matched Controls. Clin Gastroenterol Hepatol 2020;18:1592–1599.e8. [DOI] [PubMed] [Google Scholar]
- 32.Petta S, Ting J, Saragoni S, Degli Esposti L, Shreay S, Petroni ML et al. Healthcare resource utilization and costs of nonalcoholic steatohepatitis patients with advanced liver disease in Italy. Nutr Metab Cardiovasc Dis 2020;30:1014–1022. [DOI] [PubMed] [Google Scholar]
- 33.Canbay A, Kachru N, Haas JS, Meise D, Ozbay AB, Sowa JP. Healthcare resource utilization and costs among nonalcoholic fatty liver disease patients in Germany. Ann Transl Med 2021;9:615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Boursier J, Shreay S, Fabron C, Torreton E, Fraysse J. Hospitalization costs and risk of mortality in adults with nonalcoholic steatohepatitis: Analysis of a French national hospital database. EClinicalMedicine 2020;25:100445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Romero-Gomez M, Kachru N, Zamorano MA, Darba J, Shreay S. Disease severity predicts higher healthcare costs among hospitalized nonalcoholic fatty liver disease/nonalcoholic steatohepatitis (NAFLD/NASH) patients in Spain. Medicine (Baltimore) 2020;99:e23506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Srivastava A, Gailer R, Tanwar S, Trembling P, Parkes J, Rodger A et al. Prospective evaluation of a primary care referral pathway for patients with non-alcoholic fatty liver disease. J Hepatol 2019;71:371–378. [DOI] [PubMed] [Google Scholar]
- 37.Abeysekera KWM, Macpherson I, Glyn-Owen K, McPherson S, Parker R, Harris R et al. Community pathways for the early detection and risk stratification of chronic liver disease: a narrative systematic review. Lancet Gastroenterol Hepatol 2022;7:770–780. [DOI] [PubMed] [Google Scholar]
- 38.Lazarus JV, Castera L, Mark HE, Allen AM, Adams LA, Anstee QM et al. Real-world evidence on non-invasive tests and associated cut-offs used to assess fibrosis in routine clinical practice. JHEP reports 2022;in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zhang E, Wartelle-Bladou C, Lepanto L, Lachaine J, Cloutier G, Tang A. Cost-utility analysis of nonalcoholic steatohepatitis screening. Eur Radiol 2015;25:3282–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Tanajewski L, Harris R, Harman DJ, Aithal GP, Card TR, Gkountouras G et al. Economic evaluation of a community-based diagnostic pathway to stratify adults for non-alcoholic fatty liver disease: a Markov model informed by a feasibility study. BMJ Open 2017;7:e015659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Serra-Burriel M, Graupera I, Torán P, Thiele M, Roulot D, Wai-Sun Wong V et al. Transient elastography for screening of liver fibrosis: Cost-effectiveness analysis from six prospective cohorts in Europe and Asia. J Hepatol 2019;71:1141–1151. [DOI] [PubMed] [Google Scholar]
- 42.Srivastava A, Jong S, Gola A, Gailer R, Morgan S, Sennett K et al. Cost-comparison analysis of FIB-4, ELF and fibroscan in community pathways for non-alcoholic fatty liver disease. BMC Gastroenterol 2019;19:122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Noureddin M, Jones C, Alkhouri N, Gomez EV, Dieterich DT, Rinella ME. Screening for Nonalcoholic Fatty Liver Disease in Persons with Type 2 Diabetes in the United States Is Cost-effective: A Comprehensive Cost-Utility Analysis. Gastroenterology 2020;159:1985–1987.e4. [DOI] [PubMed] [Google Scholar]
- 44.Vilar-Gomez E, Lou Z, Kong N, Vuppalanchi R, Imperiale TF, Chalasani N. Cost Effectiveness of Different Strategies for Detecting Cirrhosis in Patients With Nonalcoholic Fatty Liver Disease Based on United States Health Care System. Clin Gastroenterol Hepatol 2020;18:2305–2314.e12. [DOI] [PubMed] [Google Scholar]
- 45.Kalutkiewicz MK ER, Pepin K, Allen AM, Loomba R. Cost-effectiveness of magnetic resonance elastography for nonalcoholic steatohepatitis fibrosis in the United Kingdom. EASL NASH Summit 2022. [Google Scholar]
- 46.Lazarus JV, Anstee QM, Hagström H, Cusi K, Cortez-Pinto H, Mark HE et al. Defining comprehensive models of care for NAFLD. Nat Rev Gastroenterol Hepatol 2021;18:717–729. [DOI] [PubMed] [Google Scholar]
- 47.Wong VW, Zelber-Sagi S, Cusi K, Carrieri P, Wright E, Crespo J et al. Review article Management of NAFLD in primary care settings. Liver Int 2022. [DOI] [PubMed] [Google Scholar]
- 48.Golabi P, Paik JM, AlQahtani S, Younossi Y, Tuncer G, Younossi ZM. Burden of non-alcoholic fatty liver disease in Asia, the Middle East and North Africa: Data from Global Burden of Disease 2009–2019. J Hepatol 2021;75:795–809. [DOI] [PubMed] [Google Scholar]
- 49.Balp MM, Krieger N, Przybysz R, Way N, Cai J, Zappe D et al. The burden of non-alcoholic steatohepatitis (NASH) among patients from Europe: A real-world patient-reported outcomes study. JHEP Rep 2019;1:154–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet 2017;389:1229–1237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Chetty R, Stepner M, Abraham S, Lin S, Scuderi B, Turner N et al. The Association Between Income and Life Expectancy in the United States, 2001–2014. Jama 2016;315:1750–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Stringhini S, Dugravot A, Shipley M, Goldberg M, Zins M, Kivimäki M et al. Health behaviours, socioeconomic status, and mortality: further analyses of the British Whitehall II and the French GAZEL prospective cohorts. PLoS Med 2011;8:e1000419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Lazarus JV, Colombo M, Cortez-Pinto H, Huang TT, Miller V, Ninburg M et al. NAFLD - sounding the alarm on a silent epidemic. Nat Rev Gastroenterol Hepatol 2020;17:377–379. [DOI] [PubMed] [Google Scholar]
- 54.Vilar-Gomez E, Nephew LD, Vuppalanchi R, Gawrieh S, Mladenovic A, Pike F et al. High-quality diet, physical activity, and college education are associated with low risk of NAFLD among the US population. Hepatology 2022;75:1491–1506. [DOI] [PubMed] [Google Scholar]
- 55.Cho J, Lee I, Park DH, Kwak HB, Min K. Relationships between Socioeconomic Status, Handgrip Strength, and Non-Alcoholic Fatty Liver Disease in Middle-Aged Adults. Int J Environ Res Public Health 2021;18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Giammarino AM, Qiu H, Bulsara K, et al. Community Socioeconomic Deprivation Predicts Nonalcoholic Steatohepatitis. Hepatol Commun 2022;6:550–560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Talens M, Tumas N, Lazarus JV, Benach J, Pericas JM. What Do We Know about Inequalities in NAFLD Distribution and Outcomes? A Scoping Review. J Clin Med 2021;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Golovaty I, Tien PC, Price JC, Sheira L, Seligman H, Weiser SD. Food Insecurity May Be an Independent Risk Factor Associated with Nonalcoholic Fatty Liver Disease among Low-Income Adults in the United States. J Nutr 2020;150:91–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Tutunchi H, Saghafi-Asl M, Ebrahimi-Mameghani M, Ostadrahimi A. Food Insecurity and Lipid Profile Abnormalities Are Associated with an Increased Risk of Nonalcoholic Fatty Liver Disease (NAFLD): A Case-Control Study. Ecol Food Nutr 2021;60:508–524. [DOI] [PubMed] [Google Scholar]
- 60.Tamargo JA, Sherman KE, Campa A, Martinez SS, Li T, Hernandez J et al. Food insecurity is associated with magnetic resonance-determined nonalcoholic fatty liver and liver fibrosis in low-income, middle-aged adults with and without HIV. Am J Clin Nutr 2021;113:593–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Zelber-Sagi S, Ivancovsky-Wajcman D, Fliss Isakov N, Webb M, Orenstein D, Shibolet et al. High red and processed meat consumption is associated with non-alcoholic fatty liver disease and insulin resistance. J Hepatol 2018;68:1239–1246. [DOI] [PubMed] [Google Scholar]
- 62.Kim D, Vazquez-Montesino LM, Li AA, Cholankeril G, Ahmed A. Inadequate Physical Activity and Sedentary Behavior Are Independent Predictors of Nonalcoholic Fatty Liver Disease. Hepatology 2020;72:1556–1568. [DOI] [PubMed] [Google Scholar]
- 63.Orkin S, Brokamp C, Yodoshi T, Trout AT, Liu C, Meryum S et al. Community Socioeconomic Deprivation and Nonalcoholic Fatty Liver Disease Severity. J Pediatr Gastroenterol Nutr 2020;70:364–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Williams J, Buoncristiano M, Nardone P, Rito AI, Spinelli A, Hejgaard T et al. A Snapshot of European Children’s Eating Habits: Results from the Fourth Round of the WHO European Childhood Obesity Surveillance Initiative (COSI). Nutrients 2020;12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ventura-Cots M, Bataller R, Lazarus JV, Benach J, Pericàs JM. Applying an equity lens to liver health and research in Europe. J Hepatol 2022. [DOI] [PubMed] [Google Scholar]
- 66.Global Burden of Disease (GBD).
- 67.Lazarus JV, Mark HE, Colombo M, Demaio S, Dillon JF, George J et al. A sustainable development goal framework to guide multisectoral action on NAFLD through a societal approach. Aliment Pharmacol Ther 2022;55:234–243. [DOI] [PubMed] [Google Scholar]
- 68.Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015;149:367–78.e5; quiz e14–5. [DOI] [PubMed] [Google Scholar]
- 69.Berzigotti A, Albillos A, Villanueva C, Genescá J, Ardevol A, Augustín S et al. Effects of an intensive lifestyle intervention program on portal hypertension in patients with cirrhosis and obesity: The SportDiet study. Hepatology 2017;65:1293–1305. [DOI] [PubMed] [Google Scholar]
- 70.Segev DL, Thompson RE, Locke JE, Simpkins CE, Thuluvath PJ, Montgomery RA et al. Prolonged waiting times for liver transplantation in obese patients. Ann Surg 2008;248:863–70. [DOI] [PubMed] [Google Scholar]
- 71.Lassailly G, Caiazzo R, Ntandja-Wandji LC, Gnemmi V, Baud G, Verkindt H et al. Bariatric Surgery Provides Long-term Resolution of Nonalcoholic Steatohepatitis and Regression of Fibrosis. Gastroenterology 2020;159:1290–1301.e5. [DOI] [PubMed] [Google Scholar]
- 72.Jan A, Narwaria M, Mahawar KK. A Systematic Review of Bariatric Surgery in Patients with Liver Cirrhosis. Obes Surg 2015;25:1518–26. [DOI] [PubMed] [Google Scholar]
- 73.Aminian A, Al-Kurd A, Wilson R, Bena J, Fayazzadeh H, Singh T et al. Association of Bariatric Surgery With Major Adverse Liver and Cardiovascular Outcomes in Patients With Biopsy-Proven Nonalcoholic Steatohepatitis. Jama 2021;326:2031–2042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Klebanoff MJ, Corey KE, Samur S, Choi JG, Kaplan LM, Chhatwal J et al. Cost-effectiveness Analysis of Bariatric Surgery for Patients With Nonalcoholic Steatohepatitis Cirrhosis. JAMA Netw Open 2019;2:e190047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Abu Dayyeh BK, Bazerbachi F, Vargas EJ, Sharaiha RZ, Thompson CC, Thaemert BC et al. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity (MERIT): a prospective, multicentre, randomised trial. Lancet 2022;400:441–451. [DOI] [PubMed] [Google Scholar]
- 76.Bazerbachi F, Vargas EJ, Rizk M, Maselli DB, Mounajjed T, Venkatesh SK et al. Intragastric Balloon Placement Induces Significant Metabolic and Histologic Improvement in Patients With Nonalcoholic Steatohepatitis. Clin Gastroenterol Hepatol 2021;19:146–154.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Vuppalanchi R, Noureddin M, Alkhouri N, Sanyal AJ. Therapeutic pipeline in nonalcoholic steatohepatitis. Nat Rev Gastroenterol Hepatol 2021;18:373–392. [DOI] [PubMed] [Google Scholar]
- 78.Younossi ZM, Tampi RP, Nader F, Younossi IM, Cable R, Srishord M et al. Hypothetical treatment of patients with non-alcoholic steatohepatitis: Potential impact on important clinical outcomes. Liver Int 2020;40:308–318. [DOI] [PubMed] [Google Scholar]
- 79.Rustgi VK, Duff SB, Elsaid MI. Cost-effectiveness and potential value of pharmaceutical treatment of nonalcoholic fatty liver disease. J Med Econ 2022;25:347–355. [DOI] [PubMed] [Google Scholar]
- 80.Peter P, Lipska K. The rising cost of diabetes care in the USA. Lancet Diabetes Endocrinol 2016;4:479–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 2011;123:933–44. [DOI] [PubMed] [Google Scholar]
- 82.Karlsen TH, Sheron N, Zelber-Sagi S, Carrieri P, Dusheiko G, Bugianesi E et al. The EASL-Lancet Liver Commission: protecting the next generation of Europeans against liver disease complications and premature mortality. Lancet 2022;399:61–116. [DOI] [PubMed] [Google Scholar]
- 83.Lazarus JV, Mark HE, Villota-Rivas M, Palayew A, Carrieri P, Colombo M et al. The global NAFLD policy review and preparedness index: Are countries ready to address this silent public health challenge? J Hepatol 2022;76:771–780. [DOI] [PubMed] [Google Scholar]
- 84.Schwartländer B, Stover J, Hallett T, Atun R, Avila C, Gouws E et al. Towards an improved investment approach for an effective response to HIV/AIDS. Lancet 2011;377:2031–41. [DOI] [PubMed] [Google Scholar]
- 85.Milliken OV, Ellis VL. Development of an investment case for obesity prevention and control: perspectives on methodological advancement and evidence. Rev Panam Salud Publica 2018;42:e62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Alva ML. A Review of the Impacts of Different Approaches for Diabetes Prevention and a Framework for Making Investment Decisions. Int J Environ Res Public Health 2018;15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Howell J, Pedrana A, Schroeder SE, Scott N, Aufegger L, Atun R et al. A global investment framework for the elimination of hepatitis B. J Hepatol 2021;74:535–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Pedrana AHJ, Schröder S, Scott N, Wilson D, Kuschel C, Aufegger L, Hellard M. Eliminating Viral Hepatitis: The Investment Case. Doha, Qatar: World Innovation Summit for Health, 2018. [Google Scholar]
- 89.Pedrana A, Howell J, Scott N, Schroeder S, Kuschel C, Lazarus JV et al. Global hepatitis C elimination: an investment framework. Lancet Gastroenterol Hepatol 2020;5:927–939. [DOI] [PubMed] [Google Scholar]
- 90.Scott N, Kuschel C, Pedrana A, Schroeder S, Howell J, Thompson A et al. A model of the economic benefits of global hepatitis C elimination: an investment case. Lancet Gastroenterol Hepatol 2020;5:940–947. [DOI] [PubMed] [Google Scholar]