

Abstract
Although overall cancer incidence rates are decreasing, melanoma incidence rates continue to increase about 3% annually. Melanoma is a significant public health problem that exacts a substantial financial burden. Years of potential life lost from melanoma deaths contribute to the social, economic and human toll of this disease. However, most cases are potentially preventable. Research has clearly established that exposure to ultraviolet (UV) radiation increases melanoma risk. Unprecedented anti-tumor activity and evolving survival benefit from novel targeted therapies and immunotherapies are now available for patients with unresectable and/or metastatic melanoma. Still, prevention (minimizing sun exposure that may result in tanned or sunburned skin and avoiding indoor tanning) and early detection (identifying lesions before they become invasive, or at an earlier stage) have significant potential to reduce melanoma incidence and melanoma-associated deaths. This paper reviews the state of the science on prevention and early detection of melanoma, and current areas of scientific uncertainty and ongoing debate. The US Surgeon General’s Call to Action to Prevent Skin Cancer and US Preventive Services Task Force reviews on skin cancer have propelled a national discussion on melanoma prevention and screening that makes this an extraordinary and exciting time for diverse disciplines in multiple sectors – health care, government, education, business, advocacy and community – to coordinate efforts and leverage existing knowledge to make major strides in reducing the public health burden of melanoma in the US.
Keywords: Melanoma, Skin cancer, Melanoma/prevention & control*, Melanoma/epidemiology, Sunbathing, Suntan, Ultraviolet rays/adverse effects*, Indoor tanning, Legislation as Topic, Early Detection of Cancer, United States Food and Drug Administration, United States Preventive Services Task Force, Public health
INTRODUCTION
The incidence of melanoma has been increasing for more than forty years in the US, since population-based cancer statistics have been collected.1 Although the incidence rate for all cancer sites combined is decreasing, the melanoma incidence rate has continued to increase.2 Melanoma is the only cancer which is not projected to meet federal objectives for reductions in death rates.3 Melanoma is a significant public health problem that exacts a substantial financial and social burden; however, most cases are potentially preventable.1 Research has clearly established that exposure to ultraviolet (UV) radiation increases melanoma risk.4, 5
Melanoma prevention recommendations include minimizing overexposurea to the sun and avoiding indoor tanning, yet studies show that US adults, adolescents and children are not adequately protected from the sun, and indoor tanning remains prevalent in older adolescents and young adults.6–9 These alarming data, along with the availability of best practices and evidence-based interventions to reduce UV exposure, inspired the US Surgeon General to publish a “Call to Action to Prevent Skin Cancer” in 2014.1 Key goals of this effort are to increase opportunities for sun protection in outdoor settings, provide individuals with information to make informed, healthy choices about UV exposure, promote policies that advance the national goal of preventing skin cancer, reduce harms from indoor tanning, and strengthen research, surveillance, monitoring, and evaluation related to skin cancer prevention. Along with this Call to Action, recent state legislation to support sun protection in schools and restrict minors’ access to indoor tanning, and actions by the US Food and Drug Administration (FDA) to reclassify tanning devices10 and propose a new federal rule restricting minors’ access to tanning beds,11 have heralded a national focus on melanoma prevention that is unparalleled in US history. Together these changes present a significant opportunity for the US to change norms and policies to increase sun protection and reduce tanning behaviors.
Unprecedented anti-tumor activity and evolving survival benefit from novel targeted therapies and immunotherapies that are now available have ushered in a new era for patients with unresectable and/or metastatic melanoma.12–18 Still, prevention (through minimizing overexposure to the sun and avoiding indoor tanning) and early detection (identifying lesions at earlier stages of development) have significant potential to reduce melanoma incidence and melanoma-associated deaths. Earlier detection of thinner melanomas is linked to higher survival rates, although no randomized, controlled trials have been conducted to assess the impact of clinician screening on melanoma mortality. The lack of clear evidence regarding effectiveness of population-based screening to reduce melanoma mortality resulted in a US Preventive Services Task Force (USPSTF) recommendation in 2009, and an updated draft recommendation statement proposed in 2015, that current evidence for skin screening of the general population is, “insufficient to reliably conclude that early detection of skin cancer through visual examination by a clinician reduces morbidity or mortality.”19, 20 The USPSTF’s 2015 draft recommendation statement highlights research needs and gaps, and this critical guidance can be utilized to further develop the scientific evidence base for screening.
The national discussion on melanoma prevention and screening makes this an extraordinary and exciting time for clinicians and researchers to impact melanoma incidence and mortality. The time is now for diverse disciplines in multiple sectors – health care, government, education, business, advocacy and community – to coordinate efforts and leverage existing knowledge to make major strides in reducing the public health burden of melanoma in the US. Examples of how clinicians and researchers are collaborating to embrace approaches with broad reach and maximal impact include The University of Texas MD Anderson Cancer Center’s Melanoma Moon Shot, which as a component of this broad effort emphasizes a program of innovative behavioral research and dissemination of evidence-based prevention strategies and public policy initiatives alongside a research focus on personalized melanoma treatment strategies (http://www.cancermoonshots.org/cancer-types/melanoma),21–23 and Oregon Health and Science University’s War on Melanoma, which prioritizes research, public education and early detection (https://www.ohsu.edu/xd/health/services/dermatology/war-on-melanoma/).
Epidemiology of melanoma and nonmelanoma skin cancer
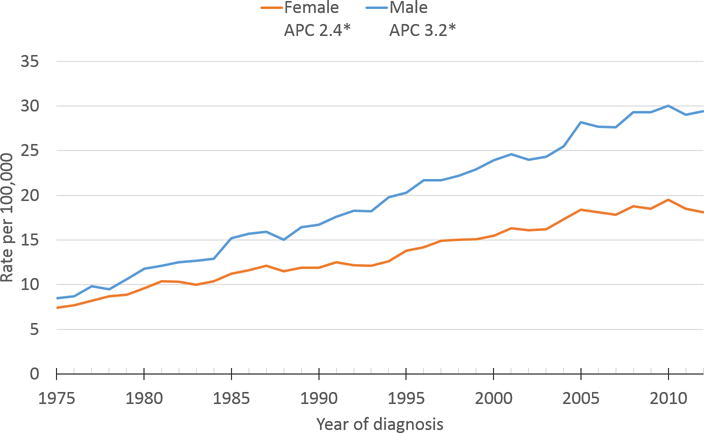
Nearly 5 million patients receive treatment for melanoma or nonmelanoma skin cancer (NMSC) in the US each year.24 These cases are primarily keratinocyte carcinomas (i.e., basal cell [BCC] and squamous cell carcinomas [SCC]), which are the most common cancers in the US but are not tracked in central cancer registry systems. Although melanoma is less common, it causes nearly 75% of skin cancer deaths.25 Melanoma is the fifth and sixth most common cancer in males and females, respectively,25 and is one of the most common cancers among adolescents and young adults.26 In 2012, the most recent year for which national data are available, 67,753 people in the US were diagnosed with invasive melanomas of the skin,25 and the American Cancer Society estimates that 76,380 cases of invasive melanoma and 68,480 cases of melanoma in situ will be diagnosed in 2016.27 From 1975 to 2012, incidence increased steadily at an annual average rate of 3.2% in males and 2.4% in females (Figure 1).28 Unlike most other cancers for which the incidence rate is either stable or decreasing,2 the incidence rate for melanoma is expected to continue to rise. Indeed, a recent estimate projected that 112,000 new invasive melanomas (i.e., exclusive of melanoma in situ) will be diagnosed in the US in 2030 in the absence of new public health interventions.29
Figure 1.
Melanoma incidence is more common overall among some groups: non-Hispanic whites, males, and older individuals (Tables 1 and 2). However, among individuals younger than age 50, melanoma is more common among females than males.25 Some have attributed higher rates and recent increases among young females to intentional tanning behaviors, especially indoor tanning.30 After age 50, melanoma incidence rates stabilize for females while increasing steeply among males.25 These patterns by age and gender likely reflect different sun protection and exposure patterns over a lifetime among women compared to men.9
Table 1.
Melanoma Incidence and Mortality Rates by Age and Sex, United States, 2008–2012
| Sex | Age (years) | Rate per 100,000 | 95% CI | Average annual count |
|---|---|---|---|---|
| Incidence | ||||
|
| ||||
| Male | 0–19 | 0.3 | (0.3–0.4) | 143 |
| 20–49 | 9.9 | (9.8–10.0) | 6087 | |
| 50–64 | 41.4 | (41.0–41.7) | 12011 | |
| 65+ | 117.4 | (116.7–118.1) | 19872 | |
|
| ||||
| Female | 0–19 | 0.5 | (0.5–0.5) | 213 |
| 20–49 | 13.9 | (13.8–14.1) | 8650 | |
| 50–64 | 27.6 | (27.3–27.8) | 8379 | |
| 65+ | 44.2 | (43.8–44.6) | 10223 | |
|
| ||||
| Mortality | ||||
|
| ||||
| Male | 0–19 | 0.0 | (0.0, 0.0) | 3 |
| 20–49 | 1.1 | (1.0, 1.1) | 658 | |
| 50–64 | 5.7 | (5.6, 5.8) | 1661 | |
| 65+ | 21.7 | (21.4, 22.1) | 3613 | |
|
| ||||
| Female | 0–19 | 0.0 | (0.0, 0.0) | 4 |
| 20–49 | 0.7 | (0.7, 0.7) | 439 | |
| 50–64 | 2.7 | (2.6, 2.8) | 840 | |
| 65+ | 7.7 | (7.6, 7.9) | 1852 | |
Source for 2008–2012 incidence rates:
United States Cancer Statistics: 1999 – 2012 Incidence, WONDER Online Database. United States Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2015. Data are from population areas that meet United States Cancer Statistics publication criteria (www.cdc.gov/cancer/npcr/uscs/technical_notes/critera.htm) for 2008–2012 and were reported to the National Program of Cancer Registries (CDC) and the Surveillance, Epidemiology and End Results (SEER) program (NCI). They cover about 99.1% of the U.S. population.
Source for 2008–2012 mortality data: Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Mortality – All COD, Aggregated With State, Total U.S. (1969–2012) <Katrina/Rita Population Adjustment>, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2015. Underlying mortality data provided by NCHS (www.cdc.gov/nchs).
Table 2.
Melanoma Incidence and Mortality Rates by Sex and Race/Ethnicity, United States, 2008–2012
| Both Sexes | Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Rate per 100,000 |
95% CI | Average annual count |
Rate per 100,000 |
95% CI | Average annual count |
Rate per 100,000 |
95% CI | Average annual count |
|
| Incidence | |||||||||
| All races | 19.9 | (19.9–20.0) | 65,557 | 25.5 | (25.3–25.6) | 38,112 | 15.0 | (15.9–16.0) | 27,465 |
| White | 22.6 | (22.5–22.6) | 62,009 | 28.4 | (28.3–28.5) | 36,256 | 18.3 | (18.2–18.4) | 25,753 |
| White, Hispanic | 4.3 | (4.2–4.4) | 1,264 | 4.8 | (4.6–5.0) | 577 | 4.2 | (4.0–4.3) | 687 |
| White, non-Hispanic | 25.1 | (25.0–25.2) | 60,744 | 31.2 | (31.0–31.3) | 35,678 | 20.7 | (20.5–20.8) | 25,066 |
| Black | 1.0 | (1.0–1.1) | 342 | 1.1 | (1.0–1.2) | 156 | 1.0 | (0.9–1.0) | 186 |
| American Indian/Alaska Native | 4.6 | (4.3–5.0) | 135 | 5.8 | (5.1–6.5) | 71 | 3.9 | (3.5–4.4) | 64 |
| Asian/Pacific Islander | 1.3 | (1.2–1.4) | 191 | 1.5 | (1.4–1.7) | 94 | 1.2 | (1.1–1.3) | 97 |
| Hispanic* | 4.2 | (4.1–4.4) | 1,354 | 4.7 | (4.5–4.9) | 618 | 4.1 | (3.9–4.2) | 736 |
| Mortality | |||||||||
| All races | 2.7 | (2.7, 2.7) | 9,071 | 4.1 | (4, 4.1) | 5,936 | 1.7 | (1.7, 1.7) | 3,135 |
| White | 3.1 | (3.1, 3.2) | 8,872 | 4.6 | (4.6, 4.7) | 5,838 | 2 | (1.9, 2) | 3,033 |
| White, Hispanic | 0.8 | (0.8, 0.9) | 210 | 1.1 | (1, 1.2) | 123 | 0.6 | (0.6, 0.7) | 87 |
| White, non-Hispanic | 3.4 | (3.4, 3.4) | 8,651 | 5 | (4.9, 5.1) | 5,709 | 2.1 | (2.1, 2.2) | 2,942 |
| Black | 0.4 | (0.4, 0.4) | 132 | 0.5 | (0.4, 0.5) | 63 | 0.4 | (0.3, 0.4) | 70 |
| American Indian/Alaska Native | 0.7 | (0.6, 0.9) | 19 | 1 | (0.7, 1.3) | 11 | 0.6 | (0.4, 0.8) | 8 |
| Asian/Pacific Islander | 0.4 | (0.3, 0.4) | 48 | 0.4 | (0.3, 0.5) | 24 | 0.3 | (0.3, 0.4) | 24 |
| Hispanic* | 0.8 | (0.7, 0.8) | 214 | 1 | (1, 1.1) | 125 | 0.6 | (0.5, 0.6) | 88 |
Hispanic ethnicity includes persons of all races.
Source for 2008–2012 incidence rates: United States Cancer Statistics: 1999 – 2012 Incidence, WONDER Online Database. United States Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2015. Data are from population areas that meet United States Cancer Statistics publication criteria (www.cdc.gov/cancer/npcr/uscs/technical_notes/critera.htm) for 2008–2012 and were reported to the National Program of Cancer Registries (CDC) and the Surveillance, Epidemiology and End Results (SEER) program (NCI). They cover about 99.1% of the U.S. population.
Source for 2008–2012 mortality data: Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Mortality – All COD, Aggregated With State, Total U.S. (1969–2012) <Katrina/Rita Population Adjustment>, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2015. Underlying mortality data provided by NCHS (www.cdc.gov/nchs).
The scientific community has debated the reasons for trends in melanoma incidence over time.31 Mortality has remained relatively stable, and early-stage melanomas make up much of the increase in incidence, leading some to suggest that increased incidence may be due solely to screening and overdiagnosis of potentially indolent lesions.32, 33 Screening for skin cancer has become increasingly common.34 However, recent analyses have described incidence increases among melanomas of all thicknesses,35, 36 and melanoma mortality among males has been gradually increasing about 1% a year (Figure 2). Increasing melanoma incidence also has been observed across all socioeconomic status (SES) groups in the California subset of the Surveillance, Epidemiology, and End Results (SEER) Program.37 Among the lowest SES group, who may have limited access to screening, the highest increases were observed for 2.01 to 4.00 mm and ≥ 4.01 mm tumors. Overall, findings suggest that melanoma incidence increases are not solely a result of increased screening.
Figure 2.

In 2012, 9,251 persons died from melanoma in the US: 6,013 males and 3,238 females (rate of 4.0 and 1.7 per 100,000, respectively),38 with an estimated 10,130 deaths expected to occur in 2016.27 Deaths due to melanoma are most common among those with the highest incidence: non-Hispanic whites, males and individuals over age 50.38 Melanoma survival is strongly associated with stage at diagnosis;39 individuals diagnosed at a later stage have poorer survival.35, 40 Five-year survival has been higher in females than males, even when stratified by stage at diagnosis.40 Although black and Hispanic patients are generally diagnosed with melanoma at later stages and have poorer survival compared to non-Hispanic whites, differences were not statistically significant when controlled for stage at diagnosis.40 Overall, melanoma survival has been improving over the past two decades, with 92% of people diagnosed during 2001–2003 surviving 5 years after diagnosis compared to 88% of those diagnosed during 1989–1991.35 Based on a SEER Cancer Statistics Review, the overall 5-year relative survival rate for those diagnosed 2005–2011 was 92%.41 Ninety-eight percent of patients diagnosed with local disease survived for five years, compared to 63% diagnosed with regional nodal disease and only 17% diagnosed with distant metastasis. These wide variations highlight not only the tremendous heterogeneity of prognosis across all stages of disease, but also the significant opportunity to reduce the public health burden of melanoma with successful prevention and early detection efforts in the US. Remarkably, only since 2011 have new treatment options become available – including both checkpoint inhibitor-based immunotherapy and targeted therapy for patients with BRAF mutations – that together are beginning to provide great promise for patients with advanced melanoma.12–18
Financial and Social Costs
The average annual cost of melanoma treatment increased by 288%, compared to 25% for all other cancers combined, between 2002–2006 and 2007–2011.24 Overall, skin cancer treatment costs $8.1 billion in the US each year, with $3.3 billion attributable to melanoma.24 Indirect costs such as lost productivity attributable to melanoma are estimated to be $39.2 million for morbidity and $3.3 billion for mortality each year.42 Beyond treatment, each potentially preventable melanoma death causes about 15 additional years of potential life lost, which contribute to the social, economic, and human toll of this disease. Prevention interventions aimed at reducing melanoma incidence have the potential to substantially decrease melanoma-related costs by an estimated $250 million per year (Figure 3).29
Figure 3.

MELANOMA PREVENTION AND EARLY DETECTION
The following sections elaborate on the state of the science pertaining to prevention strategies (sun protection and avoidance of indoor tanning) and evidence-based interventions and best practices for early detection and screening. USPSTF recommendations concerning skin cancer counseling and screening are discussed along with current areas of ongoing debate.
Melanoma Prevention: Reducing UV Exposure
The vast majority of skin cancers are caused by UV exposure from the sun and/or indoor tanning devices.4, 43 Melanoma prevention strategies include sun protection (i.e., using sunscreen regularly; wearing protective clothing, wide-brimmed hats and sunglasses; seeking shade and limiting time outdoors during midday hours when UV radiation from the sun is most intense) and avoidance of indoor tanning.27, 44 Although it is clear that UV exposure plays a key role in the development of most skin cancers, the importance of age at overexposure is unclear, with some research showing that sunburns in childhood are particularly harmful and other studies showing that sunburn during any life period raises risk.45, 46 Scientific evidence links indoor tanning to an increased risk of developing melanoma, BCC and SCC.47–50 Moreover, genetic sequencing data support the role of UV exposure in increasing risk for melanoma; recent studies, including the melanoma effort of The Cancer Genome Atlas Program, demonstrated that melanoma has the highest mutation rate among all solid tumors studied and that the majority of somatic mutations in melanomas are associated with a “UV signature.”51–53
Occupational exposure to UV may play a role in the development of melanoma. Some ecological studies have shown that outdoor workers were at increased risk of SCC and BCC, but not melanoma.54, 55 However, studies on the relationship between occupational UV exposure and melanoma are often limited by lack of information on other related factors.56, 57 A large meta-analysis stratifying studies by latitude found that workers in UV-intense areas were at increased risk of melanoma.58 An Australian analysis of melanoma by body site found that occupational exposure was associated with melanomas of the head and neck, whereas recreational exposures were associated with melanomas of the trunk.59
Sun Protection
Prevalence of Sunburn and Sun Protection Behavior
In 2010, 38% of US adults reported being sunburned in the past year.9 Although most (70%) US adults reported usually or always protecting their skin from the sun when outdoors for more than an hour on a sunny day,9 individual methods of protection were less common. For example, only 31% of adults (21% of men and 41% of women) reported use of sunscreen with a sun protection factor (SPF) of 15 or higher on exposed skin. Non-Hispanic whites had the highest prevalence of sunscreen use (37%), followed by Hispanics (22%) and non-Hispanic blacks (10%). Sunscreen use was less common in younger adults ages 18 to 24 (23%) compared to individuals 25 or older (32%). More males (46%) than females (34%) wore protective clothing, while more females (44%) than males (31%) sought shade; adults 25 and older were more likely to use protective clothing and shade.9 Research shows that some melanoma survivors sunbathe, experience sunburns or do not use adequate protection despite their diagnosis.60
A 2004 population-based survey of adolescents ages 11 to 18 showed that 69% reported at least one sunburn during the previous summer; 5% routinely wore wide-brimmed hats, 23% wore protective clothing and 22% sought shade.61 According to the 2013 Youth Risk Behavior Survey (YRBS), a nationally representative sample of high school students in grades 9 through 12, only 10% of high school students (13% of females and 7% of males) reported using sunscreen with SPF 15 or higher always or most of the time when outside for more than one hour on a sunny day.8 Sunscreen use was highest in Asian students (16%; 24% of females and 8% of males) followed by non-Hispanic white students (12%; 15% of females and 8% of males). US population-based estimates of parent sun protection practices for children are lacking. In a population-based study of fifth-grade children from Framingham, Massachusetts, 55% of children reported experiencing one or more sunburns during the previous summer, and only 25% reported routinely using sunscreen.62
Evidence on Effectiveness of Community-wide Programs
The Community Preventive Services Task Force conducted systematic reviews on the effectiveness of community-based interventions to prevent skin cancer. Recommendations based on these reviews are published in The Guide to Community Preventive Services (aka The Community Guide). Currently, The Community Guide states that there is sufficient evidence to recommend education and policy approaches to increase preventive behaviors in the following settings: child care centers, primary and middle schools, outdoor recreational and tourism areas, and occupational settings.63
The Community Guide also states that multicomponent community-wide interventions are effective at increasing preventive behaviors. These interventions are defined as having at least two distinct components (such as strategies directed toward individuals, mass media campaigns or environmental and policy changes) implemented in multiple settings or the entire community in a defined geographic area.63 Although mass media campaigns, specifically, were found to be effective when used as one component in a multicomponent community-wide intervention, the small number of studies regarding mass media campaigns in the absence of other initiatives, as well as methodological issues, led to a finding of insufficient evidence for mass media campaigns alone.
Much of The Community Guide’s review of multicomponent community-wide interventions was based on research conducted in Australia,63 which has one of the highest skin cancer incidence rates in the world.64 In 1988, a sun protection program called SunSmart began in the state of Victoria, and has since been implemented in all Australian states and territories.65 After decades of prevention efforts in Australia, skin cancer incidence rates are beginning to stabilize or decline among adolescents and young adults.66, 67 A recent study estimated that regular sunscreen use in Australia has likely reduced skin cancer incidence by 10–15%, potentially preventing 14,190 people from developing SCCs and 1,730 people from developing melanomas.68 An economic evaluation of Australia’s SunSmart program demonstrated that the program saved an estimated $AU2.30 in health care costs for each $AU1 invested in the program.69
Policies and Environmental Interventions to Support Sun Protection in Schools, Occupational, and Recreational Settings
In 2002, the CDC published guidelines for school programs to prevent skin cancer.70 This document underscores the importance of policies in schools to support skin cancer prevention through strategies such as allowing or encouraging students to wear hats and protective clothing, and to carry and apply sunscreen in schools. Addressing the physical environment is also a priority of the school guidelines, especially by increasing shade in outdoor areas. As a follow-up to the publication of the guidelines, the CDC produced a document, “Shade Planning for America’s Schools,” to provide specific guidance on how to evaluate and increase the availability of shade on school grounds.71
According to the 2012 School Health Policies and Practices Study (SHPPS), which examined state and school district policies, 31% of states reported developing, revising or assisting in developing model policies related to sun safety for schools or districts, and 32% reported distributing such policies to districts or schools.72 Less than 2% of school districts required that schools allow students to apply sunscreen while at school, and most districts had no policy either requiring or recommending that schools allow students to apply sunscreen. School district guidance regarding other sun protection strategies, such as avoiding outdoor activities during peak hours of UV exposure intensity or encouraging students to wear sun protective clothing and hats, was not required or recommended in over 50% of school districts.72
The 2014 SHPPS, which examined individual school policies, reported that 15% of schools surveyed reported scheduling outdoor activities to avoid times when the sun was at peak UV intensity, 48% of schools reported that teachers allowed time for students to apply sunscreen at school and 28% stated that teachers reminded students to apply sunscreen before going outside.73 Additionally, 30% of schools reported encouraging students to wear protective clothing, while 8% prohibited students from wearing hats or visors when in the sun during the school day. SHPPS did not directly report on schools allowing or prohibiting use of sunscreen while on school grounds. California, Oregon and Texas have passed state laws allowing children to carry and apply sunscreen while on school property.74–76
Municipal and recreational policies and environmental interventions are also critical to support sun protection. The city of Phoenix, Arizona, adopted a Master Shade Plan, led by the city’s Parks and Recreation department, to increase shade and tree cover in the city.77 The city of Toronto, Canada, also has implemented a municipal shade policy since 2010, intended to increase shade in that city.78 Several municipalities and organizations have increased availability of sunscreen for the public. The city of Miami Beach has partnered with Mount Sinai Medical Center and a sunscreen manufacturer to offer sunscreen at 50 dispensers in public pools, parks and beaches.79 The city of Boston has distributed 30 sunscreen dispensers in city parks, in partnership with the Melanoma Foundation of New England and Make Big Change.80 Additionally, some sports venues have made free sunscreen available.81–84 Likewise, colleges and universities can support skin cancer prevention by making sunscreen available in outdoor recreation and sports venues and implementing policies to promote sun protection and the avoidance of indoor tanning.85 Although these particular efforts have not been evaluated, The Community Guide recommends environmental approaches to sun protection in outdoor and tourism settings.63
Sun protection interventions in outdoor occupational settings are also recommended by The Community Guide.63 Educational, environmental and policy approaches increased uptake of sun protection among outdoor workers. Policy approaches, such as requiring or providing sun protective clothing or rotating workers out of UV-intense tasks, may be particularly important for outdoor workers because they may have little individual control over their environment and UV exposure levels while at work.
Indoor Tanning
Indoor tanning is the practice of using tanning beds (also called “sunbeds”), booths or lamps to tan the skin for cosmetic purposes. Most tanning devices emit primarily UVA radiation and small amounts of UVB, though amounts vary widely.86, 87 Although UVB radiation is much more potent than UVA radiation in causing sunburn, high doses of UVA can lead to erythema, burning and tanning; both UVA and UVB radiation have been shown to cause skin cancer.88, 89 Almost 2,000 indoor tanning-related injuries were treated in emergency departments in 2012; most of these injuries were skin burns.90 Studies show that, depending on the type of tanning device used, the amount of UVA exposure may be 4 to 13 times the amount typically received from summer noontime sun in the District of Columbia.86, 87 Frequent indoor tanners may receive 1.2 to 4.7 times the yearly dose of UVA they receive from sunlight, in addition to doses received by sun exposure.87
Carcinogenicity of indoor tanning
The first expert review of tanning bed use and skin cancer was published in 2006 by the World Health Organization’s (WHO) International Agency for Research on Cancer (IARC).91 In that review, IARC released results of its meta-analysis of 19 studies of associations between tanning bed use and skin cancer risk. The IARC meta-analysis showed a 15% increase in melanoma risk (summary relative risk [RR], 1.15; 95% confidence interval [CI], 1.00, 1.31) for those who had ever used a sunbed compared to those who never had. Based on those data, in 2009 IARC added UV-emitting tanning devices to its list of group 1 carcinogens – meaning that tanning lamps are “carcinogenic to humans.”5 Recent evidence shows that the tanning response is mediated in large part by signals emanating directly from damage to DNA and that tanning does not occur without DNA damage.92
Early life exposure and melanoma risk
The IARC meta-analysis showed that melanoma risk was greater with first exposure to an indoor tanning device before age 35 (summary RR, 1.75; 95% CI, 1.35, 2.26).91 Although some challenged these findings because the association was weak, a dose-response relationship could not be confirmed, and studies did not examine exposures to specific tanning devices, more recent research has strengthened the evidence of an association between tanning bed exposure and melanoma risk. A Minnesota case-control study of indoor tanning and melanoma risk revealed that risk increased with the number of years, hours, and sessions of indoor tanning, and risk increased independent of outdoor exposure.93 An Australian population-based case-control study of early onset melanoma showed that ever using a sunbed (i.e., indoor tanning device), compared to never using one, was associated with a greater risk of developing melanoma (odds ratio [OR], 1.41; 95% CI, 1.01, 1.96).94 This association was stronger for earlier age at first use (ptrend = 0.02). There was a doubling of risk for > 10 lifetime sunbed sessions (OR, 2.01; 95% CI, 1.22, 3.31). This association was stronger for melanoma diagnosed between ages 18 and 29 (OR for > 10 lifetime sessions, 6.57; 95% CI, 1.41–30.49) than for melanoma diagnosed between ages 30 and 39 (OR, 1.60; 95% CI, 0.92–2.77; pinteraction = .01). Among those who ever used a sunbed and were diagnosed with melanoma between ages 18 and 29, 76% of melanomas were estimated to be attributable to sunbed use.94 A recent case-control study from Minnesota found that 97% of women in the study who were diagnosed with melanoma younger than age 30, and 94% of women who were diagnosed from age 30 to 39, had engaged in indoor tanning; the median age of initiation of indoor tanning was 16 years, and the median number of sessions was over 100, in both age groups.95 In a study in Norway and Sweden, authors concluded that the risk of melanoma appeared to increase with accumulating solarium exposure during early adulthood.96 More recent meta-analyses have continued to document increased risk of melanoma for indoor tanners, especially those who start at younger ages or tan more frequently.48, 49, 97 It is estimated that for each additional session of tanning bed use per year, there is a 1.8% increase in melanoma risk.48, 49
Prevalence of Use
Indoor tanning’s popularity surged in the US in the 1980s.98 Approximately 18,000 to 19,000 indoor tanning salons and 15,000 to 20,000 other commercial facilities (e.g., health clubs, gyms and spas) offer tanning services in the US.11 A report of data from 116 US cities showed that the average number of tanning salons exceeded the average number of Starbucks or McDonald’s in those cities.99 Tanning services are sometimes offered as amenities in gyms and residential settings such as apartment buildings.100 In an observational study of 125 US colleges and universities, researchers found that indoor tanning was available on campus in 12% of colleges and in off-campus housing in 42% of colleges. More than 14% of colleges allowed campus cash cards to be used to pay for indoor tanning at off-campus facilities.101
An estimated 1 million people visit a US tanning facility each day,102 and 11.3 million people engage in indoor tanning each year.6, 7 According to the 2013 National Health Interview Survey, a representative sample of the US civilian noninstitutionalized population age 18 or older, 4.2% of all adults (6.5% of females and 1.7% of males) reported using an indoor tanning device in the past 12 months.7 Use was most common among young adults ages 18 to 29 (11%; 19% of females and 4% of males). Although all percentages represent significant reductions in prevalence compared to 2010,7 these data suggest that about 7.8 million US adult females and 1.9 million males engaged in indoor tanning in 2013. Research shows that about 25% of female indoor tanners ages 18 to 25 practiced indoor tanning in locations other than tanning salons, mostly in gyms, private homes or apartments, and year-round tanning was more common in this group.100 Adult males who self-reported as gay, homosexual or bisexual (sexual minority males) were more likely to report engaging in indoor tanning than males who self-reported as heterosexual. Sexual minority females were less likely to report indoor tanning than heterosexual females.103 Remarkably, some melanoma survivors continue to engage in indoor tanning despite known risks.60
According to the 2013 YRBS, 5% of US high school student males and 20% of females reported using an indoor tanning device one or more times during the 12 months before the survey (not including spray tanning).6 Indoor tanning was most common among non-Hispanic white females in higher grades: 35% of 11th graders and 40% of 12th graders.8 Among students who reported using devices within the past year, more than one-half (51%) were “frequent tanners,” doing so ≥ 10 times within the past year. Among non-Hispanic white female high school students, 31% reported using a tanning device in 2013, representing a decrease from 37% in 2009.6 Despite reductions in indoor tanning prevalence, about 1.5 million female and 400,000 male students are still estimated to use indoor tanning devices; most (1.6 million) of these students are younger than 18.
Association with other Risk Behaviors
Frequent tanning bed use was associated with smoking cigarettes, binge-drinking, having high concern about weight and other risk behaviors in female teens.104 According to the 2009 YRBS, male high school students who tanned indoors were more likely to have ever taken steroids without a doctor’s prescription, used unhealthy weight control practices, engaged in binge drinking and attempted suicide.105 In a survey of Colorado high school students, use of steroids, alcohol, marijuana and illicit drugs was positively associated with indoor tanning.106 In young women, indoor tanning was associated with substance and alcohol use.107, 108
Motivations for Tanning
Some people continue to intentionally tan even if they are aware that UV exposure raises skin cancer risk,109 often believing that having a tan is attractive and appears healthy.61 Some have promoted sunless tanning (such as “spray tanning”) as an alternative to indoor tanning.110 However, a significant majority of tan seekers continue to sunbathe or indoor tan despite also using sunless tanning products.111, 112 Sunless tanning has preceded initiation of indoor tanning in teens.113 Exposure to chemicals through inhalation is another concern with sunless tanning.114
About 5 to 10% of indoor tanners have met criteria for tanning dependence,115–117 similar to prevalence rates for substance dependence. Assessments of tanning dependence have been adapted from Diagnostic and Statistical Manual of Mental Disorders criteria118, 119 or the CAGE, a brief screening instrument for problematic alcohol use.120 Other studies in humans and mice add evidence to the possibility of tanning addiction.121–124 Exposure to UV light triggers damage to DNA in the nucleus of keratinocytes, resulting in activation of the p53 tumor suppressor gene. This then transcriptionally up-regulates the expression of the gene encoding proopiomelanocortin (POMC) that is processed to melanocyte-stimulating hormone, inducing tanning. At the same time, another POMC-derived peptide, β-endorphin, is synthesized in skin, elevating plasma levels.92 Endogenous β-endorphin has analgesic effects and promotes relaxation and feelings of well-being in humans, similar to opiates.
Recommendations of Organizations
In addition to individual statements from numerous professional and other organizations (WHO, American Academy of Pediatrics [AAP], American Academy of Dermatology, American Medical Association, Canadian Pediatric Society, National Council on Skin Cancer Prevention and Society for Behavioral Medicine), leading cancer-focused and other concerned organizations signed a “Joint Position Statement on Indoor Tanning” in July 2015, citing high usage of tanning beds by teens and young women and the carcinogenicity of this exposure. The statement strongly supported state and federal legislation to prohibit the use of indoor tanning by minors under 18, educational efforts to effectively communicate risks of indoor tanning to teens and their parents, and counter-advertising to de-normalize the perceived beauty of tanned skin.125 To date, 22 organizations have endorsed this joint position statement on indoor tanning.
Regulation of Tanning Devices
Federal Regulation
The FDA is responsible for regulating UV tanning devices. Until 2014, the FDA categorized tanning devices as Class 1 medical devices, in the same category as tongue depressors and Band-Aids®. On March 25, 2010, the General and Plastic Surgery Devices Panel of the FDA Center for Devices and Radiologic Health Medical Devices Advisory Committee convened a public meeting to discuss tanning devices whereby experts discussed evidence that tanning bed exposure increases skin cancer risk; counter-arguments were provided by representatives of the indoor tanning industry.126 On May 27, 2014, the FDA issued a final order announcing the reclassification of UV sunlamp products from ‘low-risk’ Class I devices to ‘moderate-risk’ Class II devices that require stricter controls for design and safety and carry a visible boxed warning: “Attention: This sunlamp product should not be used on persons under the age of 18 years.”10
On December 18, 2015, the FDA announced a proposed rule to restrict the use of sunlamp products to people ages 18 and older.11 If finalized, this rule will become law in the US, superseding state laws. The rule also will require users over age 18 to sign a risk acknowledgement certification before use, and then every 6 months, stating that they have been informed about health risks.
The Tanning Accountability and Notification (“TAN Act”) (HR 945) of 2007 requires the FDA to conduct consumer testing to determine if warning labels on commercial tanning beds are positioned correctly and provide sufficient information pertaining to skin cancer risk.127 The Affordable Care Act (ACA) mandated in 2010 that indoor tanning services be levied with a 10% excise tax (the “tanning tax” or “tan tax”) to provide revenue for the ACA.128, 129 Tanning salons must receive a payment for indoor UV tanning services, report the tax each quarter and remit the tax to the Internal Revenue Service. The tan tax was expected to raise 2.7 billion dollars over 10 years, but initially the number of taxpayers filing tanning services excise tax returns was lower than expected.130 Research suggests that most salons are collecting the tax from clients, and that younger clients do not appear to mind paying the tax.131
State and Local Regulations
In 2009, Howard County, MD, became the first US jurisdiction to ban tanning for children under age 18. In October 2011, Governor Brown of California signed the first state law banning under-18 salon tanning, effective January 2012. As of April 2016, 13 other states (Delaware, Hawaii, Illinois, Louisiana, Massachusetts, Minnesota, Nevada, New Hampshire, North Carolina, Oregon, Texas, Vermont and Washington), the District of Columbia and other jurisdictions have passed under-18 bans. Now 42 states have at least some kind of legislation regarding minors’ use of indoor tanning.132, 133
Are State Indoor Tanning Laws Effective?
Studies examining parental permission laws found that tanning facilities had poor compliance with these laws,134–136 and these laws were not effective in reducing indoor tanning among teens.137, 138 More recently, researchers have evaluated tanning bed laws including age restrictions using data from the YRBS.139 Tanning laws were classified into “systems access” (e.g., requirements for indoor tanning device operators to obtain signed statements from patrons and post a warning sign); and “youth access” (parental permission [laws prohibiting minors under a certain age from using indoor tanning devices without parental consent or parental accompaniment] and age restrictions [laws prohibiting minors under a certain age from using indoor tanning devices]). The presence of any law was associated with a significant reduction in indoor tanning by 30% among female students. Systems access, parental permission and age restriction laws were associated with a larger reduction, 42%, in indoor tanning by female students. Of all forms of legislation, age restrictions appeared to be most effective at reducing rates of indoor tanning.139 Given the small number of states with these laws, states were not categorized by type of age restriction law and thus the study was unable to assess effects of different age restrictions on tanning rates. Associations between indoor tanning laws and reported indoor tanning among male students were not statistically significant, possibly due to their lower prevalence of indoor tanning and older age of tanning initiation.139
Enforcement provisions for tanning legislation vary across states, and there is a need for future research to examine the enforcement of stated provisions and the impact on indoor tanning behavior and skin cancer incidence.140 To realize the public health benefits intended by legislation to restrict minors’ access to tanning beds, facilities must comply. Research on California’s age restriction law showed that 77% of facilities were compliant.141 Data were collected by telephone by an individual posing as a 17 year-old, which is a common methodology in studies that evaluate large numbers of tanning facilities where it may be resource-prohibitive to conduct in-person visits to collect compliance data. Research suggests that telephone assessment of compliance with tanning laws is comparable to face-to-face assessment,142 but additional study of intermethod reliability would advance this research. While a majority of California facilities appeared compliant with the under-18 ban, statewide education or other interventions may be indicated to enhance compliance, especially considering that most facilities in this study denied that UV tanning posed any dangers and made specific unlawful claims about health benefits. Direct sales to the public can present problems for enforcement; WHO recommends prohibiting direct sales and unsupervised use of tanning equipment as a complement to age restrictions.143
Tanning Restrictions in other Nations
Austria, Belgium, Finland, France, Germany, Iceland, Italy, Norway, Portugal, Spain, the United Kingdom and several Canadian provinces ban tanning salon access for minors under age 18 years. Brazil and all states and territories in Australia have banned indoor tanning beds for everyone, regardless of age.144–146
Targeting the Tanning Industry’s False and Deceptive Practices
The US Federal Trade Commission (FTC) issued a complaint against the Indoor Tanning Association (ITA) alleging that its 2008 advertising campaign included false statements portraying indoor tanning as safe and beneficial and sanctioned by the government (thus misrepresenting the nature of FDA approval). In January 2010, a settlement was reached barring the ITA and related entities from making the misrepresentations or providing deceptive advertisements.147 In 2016, the FTC reached a settlement with Mercola indoor tanning systems; the company will pay refunds to consumers and will be permanently banned from marketing or selling indoor tanning systems.148
In 2012, a minority investigative report commissioned by representatives of the US House of Representatives Committee on Energy and Commerce revealed findings of false and misleading health information given to adolescents by the vast majority of tanning salons contacted by investigators.149 Salons minimized the dangerous effects of indoor tanning; 51% of salons specifically denied that indoor tanning would increase skin cancer risk.
Two state attorneys general have filed suits against several tanning chains or franchises in their states; suits were related to false health claims, unlawful concealment of indoor tanning risks and the offer of unlimited tanning by salons. These suits have generally been resolved through the payment of fines or agreements resulting in salons changing their messaging, including ceasing to make claims regarding the health or safety of indoor tanning.150–153
Melanoma Prevention Recommendations for Clinicians
Clinicians have an important role to play in addressing prevention of skin cancer, yet studies show that only about one-third of primary care physicians counsel patients on sun protection and one-half counsel on the avoidance of indoor tanning.154 In a population-based survey of adolescents and their parents, 44% reported receiving sun protection counseling from a physician.155 Counseling rates may be higher in pediatricians156, 157 or for patients who are at higher risk of skin cancer.154
A review of clinical preventive services conducted by the USPSTF in 2012 recommended that health care providers counsel fair-complexioned children, adolescents and young adults ages 10 to 24 to minimize UV exposure to reduce skin cancer risk, assigning this service a “B”grade.158, 159 The implications of the rating are significant, as an “A” or “B” grade means that the USPSTF recommends that providers offer or provide the service. The USPSTF ratings mean that there is high certainty that the net benefit is substantial (“A” grade) or moderate, or there is moderate certainty that the net benefit is moderate to substantial (“B” grade). Effective counseling used cancer prevention or appearance-focused messages to promote the use of broad-spectrum sunscreen with a minimum SPF of 15, protective clothing including hats, shade, avoidance of the outdoors during midday hours and avoidance of indoor tanning. The USPSTF identified effective low-intensity counseling strategies that could be conducted during the primary care session, including self-guided booklets, a video, peer counseling, clinician counseling with computer-assisted feedback and UV photography which shows the patient the extent of UV-induced facial skin damage.160–164 Through the Affordable Care Act, recommended preventive services with an A or B rating from the USPSTF are reimbursable to providers under most insurance plans, and must be provided with no cost sharing to patients. However, specific details regarding coverage vary by insurers, and providers and patients may be unaware of requirements.165 There is no specific billing code for skin cancer prevention counseling (though there is an existing code for “other specified counseling”).
The AAP recognizes that skin cancer prevention is a life-long effort. Beginning in infancy, pediatricians are advised to incorporate skin cancer prevention advice into at least one well child visit per year, and during “teachable moments” as when a child or teen presents with a sunburn. AAP also advises pediatricians to encourage children and teens to engage in outdoor physical activities, but to do so in a sun-safe manner.166 As pediatricians often have relationships with families over years and decades, they are well positioned to discuss with pre-teens, teens and their families the importance of avoiding indoor tanning.167 Discussions about indoor tanning could be included in the confidential part of the teen interview that requests information such as the teen’s tobacco and electronic cigarette use, alcohol and substance use, and sexual activity.
Early Detection: Skin Examination and Screening
Early detection of melanomas is important, as those diagnosed at later stages are associated with a greater risk of death from melanoma and are overall less treatable. However, the evidence on the best way to reduce melanoma mortality through early detection is currently a subject of ongoing debate. The following sections present information about three approaches that could potentially detect melanomas earlier: skin self-examination, clinician skin examination, and population-based screening.
Skin Self-Examination (SSE)
In a population-based, case-control study of 1,199 Connecticut residents, Berwick et al.168 reported a 63% reduction in fatal or advanced melanoma associated with SSE. While only 13% of patients performed SSE, the mean thickness of melanomas on the back was significantly lower in those who performed SSE (1.09 mm) compared to those who did not (1.65 mm) (p = 0.014). Subsequent analysis of the data at a median of 5.4 years demonstrated a lower risk of death from melanoma in patients with increased skin awareness; SSE was not associated with reduced melanoma mortality.169, 170 A 2003 study found that regular SSE performance was significantly associated with a reduced likelihood of being diagnosed with a melanoma > 1 mm (OR, 0.65; 95% CI, 0.45–0.93), although details regarding the thoroughness and frequency of SSE were not reported.171 Swetter et al. assessed SSE in 566 newly-diagnosed melanoma patients, and routine SSE of some/all of the body compared with none was associated with nearly twice the likelihood of a ≤ 1 mm melanoma at diagnosis (OR, 1.98; 95% CI, 1.24–3.18), with the greatest benefits observed in individuals older than 60 years and in men who used a melanoma picture to aid in SSE.172 Thoroughness of SSE, as measured by the number of body sites examined and use of a picture aid illustrating a melanoma, has been shown to be the best predictor of reduced melanoma thickness.172, 173 However, variable study definitions of SSE, including the number or percent of body sites examined, frequency and method of examination,174, 175 and the small number of studies examining supplemental techniques such as the use of photographs,176 impede the understanding of the potential effect of SSE on melanoma thickness at diagnosis.
The USPSTF evaluated SSE in their 2009 statement, which designated the evidence as insufficient to recommend SSE for the general population.19 Despite the potential benefit of SSE for early melanoma detection, SSE prevalence in the general population is low, with less than 20% of individuals in the US estimated to practice regular, thorough SSE.174, 177 Rates of SSE in middle-aged and older men also appear to be low. In a population-based telephone survey in Queensland, Australia, 20% of men 50 years or older reported conducting whole-body SSE one or more times in the past year.178 Various educational and interventional programs, including dual patient and partner skin examination training, workbooks, videos and postcard reminders, and mole-mapping diagrams,179–182 have successfully increased SSE performance in higher risk populations.
Clinician Skin Examination
Melanomas detected by clinicians through directed skin examinations or during the course of routine physical examinations (i.e., “opportunistic screening”) are thinner than those found by patients or their significant others.172, 183–187 In an analysis of 3 international studies of more than 2,400 patients, tumor thickness was reduced by a mean of 0.55 mm when comparing melanomas initially detected by physicians versus by patients or family members.188 A population-based, case-control study was conducted by Aitken et al.184 of more than 3,700 Queensland residents with histologically-confirmed first primary invasive melanoma diagnosed between January 2000 and December 2003, and a similar number of eligible controls. Whole-body physician skin examination (PSE) in cases in the three years before diagnosis was inversely associated with melanoma thickness (χ2 test for trend, 44.37; p < .001), ranging from a 14% lower risk of being diagnosed with a melanoma > 0.75 mm (OR, 0.86; 95% CI, 0.75–0.98) to a 40% lower risk for melanomas ≥ 3 mm (OR, 0.60; 95% CI, 0.43–0.83). Skin screening was associated with a 38% increased likelihood of being diagnosed with melanoma ≤0.75 mm and a 32% higher likelihood of melanoma ≤ 1 mm (OR, 1.32; 95% CI, 1.18–1.47), resulting in a projected (though not proven) 26% fewer melanoma deaths in screened cases versus unscreened cases within 5 years.
Similar benefit of PSE within the year prior to diagnosis was noted in an observational cohort study of 566 newly-diagnosed adults with cutaneous melanoma referred to 2 geographically-distinct US academic institutions.172 Tumors (≤1mm) were significantly associated with physician discovery (p ≤ .0001), which was reported by only 19% of patients. However, patients who had a whole-body skin examination by a physician in the year prior to diagnosis were more than twice as likely to have a ≤ 1 mm tumor (OR, 2.51; 95% CI, 1.62–3.87), largely due to the effect of physician skin examination in men > 60 years, who had over 4 times the odds of a ≤ 1 mm melanoma (OR, 4.09; 95% CI, 1.88–8.89) and thus, appeared to benefit most from PSE.
Worldwide Data on Melanoma Population-Based Screening, Incidence, and Mortality
Population-based melanoma screening studies include a community-based clinical trial in Queensland, Australia,189 a screening program conducted at Lawrence Livermore National Laboratory (LLNL),190 and a pilot study of general population screening in the German state of Schleswig-Holstein beginning in 2003,191, 192 which was followed by a nationwide screening program initiated in Germany in 2008.193, 194
Queensland, Australia
Forty-four eligible Queensland communities (estimated population of 560,000 adults who were 30 years or older) were randomized into intervention or control groups to compare the effects of a three-year community-based melanoma screening intervention and usual medical care.189 The Queensland trial was designed to detect a 20% reduction in mortality from melanoma during the 15 years following the start of the screening intervention. Due to financial constraints, the trial was not completed, although some observations were made from 18 communities enrolled and randomized in the study.195 Within intervention communities, the overall rate of skin cancer detected per patient screened increased, and men and attendees 50 years or older were more frequently referred and diagnosed with melanoma,196 again supporting the value of targeted screening to older individuals, and men in particular.197 Melanomas detected by the screening intervention tended to be less advanced than melanomas detected in the general population of Queensland: 39% were in situ lesions, 55% were < 1 mm, and 6% were ≥ 1 mm,196 in contrast to the general population of Queensland from 1999 through 2002, in which 36% were in situ lesions, 48% were < 1 mm, and 16% were ≥ 1 mm.198 Furthermore, the specificity (86%) for detection of melanoma through whole-body skin examination was deemed comparable to that of other screening tests, including mammography for breast cancer.196
Lawrence Livermore National Laboratory (LLNL)
A long term employee program conducted at the LLNL included melanoma education, SSE, and the opportunity for skin screening by a physician.190 The incidence of melanomas > 0.75 mm was reduced by 69% in the screening program period (1984 to 1996) compared to the preceding early awareness period (1976 to 1984, during which time employees learned about their melanoma risk). This program also showed a crude reduction in melanoma mortality in the LLNL workforce compared with California during this timeframe, based on observed mortality in five San Francisco-Oakland-Bay Area counties as reported to the SEER program from 1984 to 1996: 0 deaths at LLNL compared to an expected number of 3.39 deaths (p = .034).190
Schleswig-Holstein, Germany
The most compelling population-based data regarding potential screening effectiveness were collected from the “Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany” (SCREEN) pilot project conducted in the northern state of Schleswig-Holstein, Germany.191, 192 General practitioners and dermatologists completed an 8-hour skin cancer training program. Sixty-four percent (1,673) of Schleswig-Holstein’s general practitioners participated in the screening, along with 98% (116) of dermatologists. Whole-body skin examination by a general practitioner was followed by referral to a dermatologist for further evaluation of suspicious skin findings and biopsy if necessary. It was possible for patients to initially visit a dermatologist based on skin cancer risk factors alone, but most patients opted to visit a general practitioner first.
Following a two-year pre-screening period of intensive public education regarding melanoma clinical warning signs and the screening initiative, almost 20% of the adult population aged 20 years or older (360,288 participants with a mean age of 49.7 [SD = 16.2] years192) was screened over a one-year period from 2003 to 2004. The majority of initial screening examinations (77%) were performed by general practitioners; dermatologists performed 23% of the initial examinations.191, 192 Although 73,710 individuals (26%) were referred to dermatologists following initial general practitioner screening, nearly 37% of those referred did not undergo consult by a dermatologist and were lost to follow-up.192 In 2009 (5 years after the screening program), age- and sex-adjusted melanoma mortality rates declined by 48% (a 47% decline in men and 49% decline in women), compared to historical mortality rates in Schleswig-Holstein and prior and 2009 mortality rates in surrounding states and Denmark, where no screening intervention took place.191
To what degree extensive pre-SCREEN public awareness campaigns themselves contributed to the mortality reduction remains unclear, as it is difficult to separate the potential mortality benefit of this education on early detection from the visual skin inspections by clinicians during the one-year screening period. Additionally, the demonstration of improved survival is insufficient evidence of the benefit of screening, as this may simply reflect lead-time, length bias, or overdiagnosis. Some have hypothesized that differences in coding of death data could have been responsible for temporal declines in melanoma mortality.194, 199
An increased incidence of melanoma and NMSC occurred during the screening intervention and early follow-up period; an initial increase was expected given the detection of existing skin cancer in the population.192 The proportion of individuals diagnosed with early stage tumors increased from 52% in the pre-SCREEN period (2001 to 2003) to 64% in the one-year screening period (2003 to 2004).192 In July 2008, the German Federal Joint Committee included skin cancer screening as part of nationwide services provided by the Health Insurance Funds.192, 193, 200 Whole-body screenings have been offered free of charge once every 2 years for an estimated 45 million German residents who are 35 years of age or older, with the 8-hour physician training course and dual screening process used in the pilot study in Schleswig-Holstein.192, 193, 200
The first analyses of this nationwide effort showed that melanoma mortality in Schleswig-Holstein increased to its pre-SCREEN rate for both sexes and all ages, thus demonstrating only a transient decline in mortality in Schleswig-Holstein five years after the SCREEN pilot project.193, 194 No decrease in mortality has been observed five years after screening began in Germany overall; a slight increase was actually noted, likely due to population changes per census data in men and individuals 64 years of age or older.193, 194 Potential reasons for the lack of a measurable reduction in mortality rates in Germany or Schleswig-Holstein after the nationwide screening effort include: less intensive or thorough screening (e.g., poorer quality, less consistently performed skin exams and suboptimal referral patterns from primary care providers [PCP] to dermatologists); higher age of eligibility for the nationwide screening program (≥ 35 years of age) compared to the pilot SCREEN program (≥ 20 years of age); inability to accurately track participation rates by physicians or patients; nonreferral of individuals by general practitioners to dermatologists based on melanoma risk factors alone (as was permissible in the Schleswig-Holstein pilot); and lack of intensive nationwide mass-media publicity as was used in SCREEN.193, 194 It is possible that reduced mortality will be observed with longer follow-up, although no such trend has yet been observed in preliminary analyses. The economic impact of this ambitious nationwide skin cancer screening endeavor, and how the German health care system has managed the various screening-related outcomes, have not been reported.
USPSTF Recommendations for Screening by Primary Care Providers (PCP)
Given the lack of a prospective, randomized controlled trial assessing the impact of screening on melanoma mortality, the USPSTF in 2009 recommended neither for nor against routine skin cancer screening of the general population by PCPs, assigning a rating of “I” for “insufficient” evidence to support this practice.19 The USPSTF further noted that the potential harms of screening had not been adequately addressed, including both physical and psychological effects related to misdiagnosis and unnecessary biopsies.
In preparing the 2015 draft recommendation, the USPSTF evaluated an AHRQ evidence-based systematic review of literature published from January 1, 1995 through June 1, 2015, which yielded 13 relevant studies. Studies focused primarily on the SCREEN program, which was assessed to be of “fair-quality.”191 However, the recent analyses of melanoma incidence and mortality in Schleswig-Holstein and Germany following the nationwide screening initiated in 2008193, 194 were not included in the systematic review, given the date of publication. The updated 2015 Task Force review differed from that which led to the 2009 recommendation in that NMSC was excluded as an outcome of interest due to its low mortality rates and lack of “substantial morbidity.” The USPSTF Draft Recommendation Statement was released on November 30, 2015, followed by a four-week period for public comment (closed December 28, 2015) before the final statement will be issued.20 The USPSTF concluded that, “current evidence is insufficient to assess the balance of benefits and harms of visual skin cancer screening in adults,” and has once again tentatively assigned this practice an “I” grade, pending a final recommendation.
The USPSTF noted limitations of the SCREEN pilot, including the high proportion of “lower-risk” women screened compared to higher-risk men, the 37% of general practitioner-referred patients who did not follow up with dermatologists for their suspicious skin lesions, and the inability to assess the impact of the pre-SCREEN public education program apart from the visual skin cancer screening. Furthermore, the population-based changes in mortality in the SCREEN program could not be interpreted as causal because individual-level data on outcomes for screened individuals were not available. The USPSTF Evidence Synthesis concluded that the absolute mortality reduction of 0.8 deaths per 100,000 individuals screened suggested a modest benefit overall.201 Additional analyses have raised concerns about the design of the SCREEN study, including potential underreporting of melanoma deaths by physicians and self-referral of high-risk participants, and thus the data that demonstrated the initial reductions are a subject of ongoing debate.194, 199 The lack of available data regarding thickness-specific incidence or potential benefit of screening in certain subgroups (e.g., older men) makes firm conclusions regarding the German nationwide screening effort premature. Nonetheless, Germany’s national screening program provides a valuable opportunity to collect effectiveness data on population-based screening.
Importantly, the USPSTF noted that their latest screening recommendation does not apply to patients with a history of premalignant skin lesions or skin cancer, who present with a suspicious skin lesion, or are already followed for increased risk of skin cancer based on abnormal mole phenotype or family history of melanoma. Potential harms of screening related to overdiagnosis and overtreatment were noted, though precise assessment of these harms was not possible from data included in the Evidence Synthesis.201 Further research regarding screening high risk groups, and case-control studies of screened versus unscreened individuals – without potential confounding from an educational campaign or other intervention – was deemed necessary to fully evaluate the benefit of skin screening.
Potential Impact of Screening on NMSC Morbidity and Cost
Detection of (highly curable) NMSC was not a directive of the latest USPSTF review and in fact, was considered a potential harm of screening for “lesions that may have little potential for malignant spread and mortality.”19 Concern for overtreatment of both indolent pigmented lesions mimicking melanoma (i.e., “false-positives” detected through screening) as well as nonfatal NMSCs was raised in the 2009 USPSTF recommendation statement. However, SCC results in the second highest rate of skin cancer-associated mortality after melanoma; up to 5.2% of patients with cutaneous SCC will develop nodal metastasis and up to 2.1% will die from distant disease.202 The economic burden of treating NMSC cannot be ignored, in addition to patient-related factors including optimizing surgical and cosmetic outcome and reducing lost work-time. The annual cost of treating NMSC in the U.S. has been estimated at $4.8 billion.24 Earlier detection of NMSC is likely to result in fewer surgeries with more rapid patient recovery, improved cosmetic outcome for these UV-related tumors on the head and neck, and lower cost of treatment.
Feasibility of Skin Cancer Screening Implementation in the US
Recent evidence from the screening studies in Germany and the latest USPSTF recommendation raise questions regarding where screening is headed for PCPs in the US. A nationwide screening program as was conducted in Germany is not likely to be feasible, and findings of population-based skin screening studies in other countries may not generalize to the US depending on the comparability of skin cancer risk factor distributions across populations. PCPs may not be adequately trained to identify early skin cancer.203, 204 A survey of more than 1,600 randomly-selected physicians found that time constraints, competing comorbidities, and patient embarrassment were the top three barriers to performing whole-body skin examinations.205 Factors that facilitated examination by physicians included having more patients at high risk for skin cancer, patient demand for a complete examination or mole check, and appropriate training.
It is unclear what implementation techniques will overcome these barriers in clinical practice, though various training strategies are being tested. A 1.5 hour, web-based curriculum entitled INFORMED (INternet-based program FOR Melanoma Early Detection, available at www.skinsight.com/info/for_professionals/skin-cancer-detection-informed/skin-cancer-education) was designed to provide clinical guidance for early detection of melanoma (as well as other common skin cancers) by PCPs.206 A study evaluating the effect of INFORMED on 54 PCPs in two integrated health care delivery systems suggested that it decreased dermatology referrals, particularly for benign skin lesion assessment.207 The INFORMED training improved appropriate PCP diagnosis and management from 36% pre-training to 47% post-training, and dermatology utilization decreased without any change in biopsies performed or skin cancers diagnosed.
A population-based study in France evaluated the effect of a PCP awareness and training campaign on stage-specific melanoma incidence.208 All (1,241) general practitioners in the region of Champagne-Ardenne received repeated postal mailings to raise melanoma awareness, and 398 (32%) attended a 2.5-hour, dermatologist-led, skin cancer training session. From pre- (2005–2007) to post-intervention (2009–2011), Champagne-Ardenne showed a 34% reduction in the incidence of melanomas ≥ 3 mm in tumor thickness, from 1.07 to 0.71/100,000 habitants per year (standardized for age) (p = .01). This reduction was most pronounced in men compared with women (44% vs 11 %, respectively). Likewise, the proportion of in situ and < 1 mm melanomas increased from 20 to 28% (p = .001) and from 51% to 57% (p = .05), respectively. There were no significant changes in incidence in the control area that comprised regions without the PCP educational campaign.
Since Americans make an average of 1.7 visits to PCPs each year,209 PCPs can serve as an important source of skin cancer diagnosis and triage. Although the USPSTF did not recommend skin cancer screening, they advised clinicians that biopsy of suspicious skin lesions noted during physical examinations is warranted.159 Implementation of skin screening requires a paradigm shift in the way primary care is delivered, necessitating evaluation of feasibility including adequate time to conduct the exam, and possible harms, such as cost and utilization of scarce resources, along with further study of the potential benefits of early melanoma detection.
SUMMARY AND CONCLUSIONS
US adults, adolescents and children are not adequately protected from excessive UV exposure, despite expert guidance and the existence of evidence-based, melanoma prevention interventions recommended by The Community Guide and USPSTF. The Surgeon General’s Call to Action highlights youth as a critical population to reach with intervention to promote sun protection and discourage indoor tanning, and invites multiple sectors across the US to coordinate efforts and leverage existing knowledge to reduce the nation’s skin cancer burden.
There is a lack of national, population-based data or estimates of parent sun protection practices for children in the US, and estimates of behaviors other than indoor tanning and sunscreen use across age groups. Furthermore, physician counseling for sun protection and assessments of provider knowledge of skin cancer prevention are understudied areas. These gaps in research minimize our ability to spot trends, target interventions and evaluate progress.
As increasing numbers of states prohibit indoor tanning among minors, researchers will need to evaluate compliance with and enforcement of such laws. The proposed FDA rule to ban minors’ access to tanning is significant, but finalization of this age restriction rule may not occur for months or years after the public comment period. Despite the expansive effects of legislation and FDA regulations, it is necessary to continue to develop and disseminate evidence-based interventions to reduce positive tanning attitudes and tanning behaviors, starting in childhood, given the current availability of indoor tanning devices at home through direct purchase as well as the alternative to sunbathe for individuals seeking a tan.
While multiple studies support the value of early detection of melanoma through clinician skin examination,188 evidence that this translates into reduced population-based melanoma mortality has been insufficient, in both 2009 and 2015, for the USPSTF to recommend skin screening as part of primary care practice.19, 20 An observational study of a population-based screening program in one state in Germany showed promising results, with large reductions in mortality rates not observed in surrounding states without screening programs.191 Based on these early results, the screening program was expanded to the rest of the country, but mortality rates have remained stable nationally and mortality reductions in the state initially piloting the screening program were not sustained.193 There is a critical need to augment evidence regarding the potential benefits of skin screening; PCP and other providers’ education regarding skin cancer awareness, SSE and screening; and appropriate triage to dermatologists, as PCPs account for the majority of physician-detected melanoma. The proliferation of new technologies may hold promise for future prevention and early detection of melanoma. For example, smart phone applications (or “apps”) are available to give users real-time information regarding their UV exposure based on their location, methods of protection, and skin type, and may be effective at improving sun protection.210 The growing popularity of wearable health monitoring devices has incorporated sun protection, and some devices include wearable UV sensors.211 Mole mapping apps can assist high-risk patients with many nevi keep track of any changes, and tele-dermatology may expand access for some who have questionable lesions but do not live close to a dermatologist.212, 213 Though these new approaches are exciting, evaluation of their effectiveness in the real world will be important; one study from 2008 found that users of personal UV sensors were likely to use less sun protection when wearing the sensor.214
Increased attention to the problems of melanoma resulting in high-level government support such as the Surgeon General’s Call to Action and continuing FDA actions to address the harms of indoor tanning have the potential to reduce their future health burden if implemented and supported. New tools for early detection may result in earlier diagnoses. Moreover, improved understanding of the molecular and immunological underpinnings of melanoma have ushered in a new era of transformative treatment options for patients with advanced melanoma over the past five years that have already begun to improve survival outcomes. In conclusion, we are at a uniquely exciting time in the area of melanoma prevention and treatment – the time to act is now to continue to reduce the burden of melanoma in the US and beyond.
Acknowledgments
Authors would like to thank Alan C. Geller, MPH, RN, Senior Lecturer of Social and Behavioral Sciences, Harvard T.H. Chan School Of Public Health and Director, Melanoma Epidemiology, Massachusetts General Hospital, Boston MA for his insights into the conceptualization of this review article.
Funding source: Support provided, in part, by the generous philanthropic contributions to The University of Texas MD Anderson Cancer Center Melanoma Moon Shots Program, the Cancer Center Support Grant (CA16672, PI: R. DePinho, MD Anderson Cancer Center), from the National Cancer Institute, National Institutes of Health, and the Michael and Patricia Booker Melanoma Research Endowment. Dr. Gershenwald has participated on an advisory board for Merck since June 2014, and this advisory role is not related to the content of this review article. Dr. Tripp reported stock ownership in Merck, Abbott Laboratories and AbbVie, and these financial relationships are not related to the content of this review article. The remaining authors have no financial disclosures to report.
Footnotes
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Contributions: Mary K. Tripp: Conceptualization, investigation, writing – original draft, and writing – review and editing. Meg Watson: Conceptualization, methodology, formal analysis, writing – original draft, and writing – review and editing. Sophie J. Balk: Conceptualization, writing – original draft, and writing – review and editing. Susan M. Swetter: Conceptualization, investigation, writing – original draft, and writing – review and editing. Jeffrey E. Gershenwald: Conceptualization, methodology, investigation, resources, writing – original draft, writing – review and editing, visualization, supervision, project administration, and funding acquisition.
For the purposes of this document, overexposure is defined as sun exposure that may result in tanned or sunburned skin, or that may increase a person’s risk of skin cancer.1
Contributor Information
Mary K. Tripp, Department of Behavioral Science, The University of Texas MD Anderson Cancer Center, Houston, Texas.
Meg Watson, Division of Cancer Prevention and Control, Centers for Disease Control and Prevention, Atlanta, Georgia.
Sophie J. Balk, Children’s Hospital at Montefiore, Albert Einstein College of Medicine, Bronx, NY.
Susan M. Swetter, Department of Dermatology, Pigmented Lesion and Melanoma Program, Stanford University Medical Center and Cancer Institute Stanford, California; Dermatology Service, Veterans Affairs Palo Alto Health Care System, Palo Alto, California.
Jeffrey E. Gershenwald, Department of Surgical Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas.
References
- 1.U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent Skin Cancer. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2014. www.surgeongeneral.gov/library/calls/prevent-skin-cancer/call-to-action-prevent-skin-cancer.pdf. [PubMed] [Google Scholar]
- 2.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. doi: 10.3322/caac.21332. [DOI] [PubMed] [Google Scholar]
- 3.Weir HK, Thompson TD, Soman A, Moller B, Leadbetter S, White MC. Meeting the Healthy People 2020 objectives to reduce cancer mortality. Prev Chronic Dis. 2015;12:E104. doi: 10.5888/pcd12.140482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Armstrong BK, Kricker A. How much melanoma is caused by sun exposure? Melanoma Res. 1993;3:395–401. doi: 10.1097/00008390-199311000-00002. [DOI] [PubMed] [Google Scholar]
- 5.El Ghissassi F, Baan R, Straif K, et al. A review of human carcinogens–part D: radiation. Lancet Oncol. 2009;10:751–752. doi: 10.1016/s1470-2045(09)70213-x. [DOI] [PubMed] [Google Scholar]
- 6.Guy GP, Jr, Berkowitz Z, Everett Jones S, Holman DM, Garnett E, Watson M. Trends in indoor tanning among US high school students, 2009–2013. JAMA Dermatol. 2015;151:448–50. doi: 10.1001/jamadermatol.2014.4677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Guy GP, Jr, Berkowitz Z, Holman DM, Hartman AM. Recent changes in the prevalence of and factors associated with frequency of indoor tanning among US adults. JAMA Dermatol. 2015;151:1256–9. doi: 10.1001/jamadermatol.2015.1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Centers for Disease Control and Prevention. 1991–2013 High School Youth Risk Behavior Survey Data. https://nccd.cdc.gov/youthonline/. Accessed December 16, 2015.
- 9.Centers for Disease Control and Prevention National Center for Health Statistics. UV Exposure and Sun Protective Practices. National Health Interview Survey NCI and CDC co-sponsored Cancer Control Supplement, 1992–2010, 2005–2010. http://www.progressreport.cancer.gov/prevention/sun_protection. Accessed December 16, 2015.
- 10.Federal Register. General and Plastic Surgery Devices: Reclassification of Ultraviolet Lamps for Tanning, Henceforth To Be Known as Sunlamp Products and Ultraviolet Lamps Intended for Use in Sunlamp Products. https://www.federalregister.gov/articles/2014/06/02/2014-12546/general-and-plastic-surgery-devicesreclassification-of-ultraviolet-lamps-for-tanning-henceforth-to. Accessed November 4, 2015. [PubMed]
- 11.U.S. Food and Drug Administration. General and Plastic Surgery Devices: Restricted Sale, Distribution, and Use of Sunlamp Products. Date posted: Dec 22, 2015. 21 CFR Part 878 Federal Register Number:2015-32024. [Google Scholar]
- 12.Larkin J, Ascierto PA, Dreno B, et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N Engl J Med. 2014;371:1867–76. doi: 10.1056/NEJMoa1408868. [DOI] [PubMed] [Google Scholar]
- 13.Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373:23–34. doi: 10.1056/NEJMoa1504030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Long GV, Stroyakovskiy D, Gogas H, et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N Engl J Med. 2014;371:1877–88. doi: 10.1056/NEJMoa1406037. [DOI] [PubMed] [Google Scholar]
- 15.Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–23. doi: 10.1056/NEJMoa1003466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med. 2012;367:1694–703. doi: 10.1056/NEJMoa1210093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372:30–9. doi: 10.1056/NEJMoa1412690. [DOI] [PubMed] [Google Scholar]
- 18.Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364:2517–26. doi: 10.1056/NEJMoa1104621. [DOI] [PubMed] [Google Scholar]
- 19.U.S. Preventive Services Task Force. Screening for skin cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;150:188–93. doi: 10.7326/0003-4819-150-3-200902030-00008. [DOI] [PubMed] [Google Scholar]
- 20.U.S. Preventive Services Task Force. Draft recommendation statement: skin cancer: screening. 2015 http://www.uspreventiveservicestaskforce.org/Page/Document/draft-recommendation-statement168/skin-cancer-screening2. Accessed January 20, 2016.
- 21.Watson M, Thomas CC, Massetti GM, et al. CDC Grand Rounds: Prevention and Control of Skin Cancer. MMWR Morb Mortal Wkly Rep. 2015;64:1312–4. doi: 10.15585/mmwr.mm6447a2. [DOI] [PubMed] [Google Scholar]
- 22.Centers for Disease Control and Prevention. Public Health Grand Rounds: Prevention and Control of Skin Cancer. 2015 Apr 21; http://www.cdc.gov/cdcgrandrounds/archives/2015/april2015.htm. Accessed January 26, 2016.
- 23.Gershenwald JE, Guy GP., Jr Stemming the rising incidence of melanoma: Calling prevention to action. J Natl Cancer Inst. 2016 doi: 10.1093/jnci/djv381. 108.djv381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Guy GP, Jr, Machlin SR, Ekwueme DU, Yabroff KR. Prevalence and costs of skin cancer treatment in the U.S., 2002–2006 and 2007–2011. Am J Prev Med. 2015;48:183–7. doi: 10.1016/j.amepre.2014.08.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2012 Incidence and Mortality Web-based Report. 2015 www.cdc.gov/uscs. Accessed December 15, 2015.
- 26.Weir HK, Marrett LD, Cokkinides V, et al. Melanoma in adolescents and young adults (ages 15–39 years): United States, 1999–2006. J Am Acad Dermatol. 2011;65:S38–49. doi: 10.1016/j.jaad.2011.04.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.American Cancer Society. Cancer Facts & Figures 2016. Atlanta, GA: American Cancer Society; 2016. [Google Scholar]
- 28.Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence – SEER 9 Regs Research Data, Nov 2014 Sub (1973–2012) <Katrina/Rita Population Adjustment> – Linked To County Attributes – Total U.S., 1969–2013 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2015 based on the November 2014 submission.
- 29.Guy GP, Jr, Thomas CC, Thompson T, Watson M, Massetti GM, Richardson LC. Vital signs: melanoma incidence and mortality trends and projections – United States, 1982–2030. MMWR Morb Mortal Wkly Rep. 2015;64:591–6. [PMC free article] [PubMed] [Google Scholar]
- 30.Bradford PT, Anderson WF, Purdue MP, Goldstein AM, Tucker MA. Rising melanoma incidence rates of the trunk among younger women in the United States. Cancer Epidemiol Biomarkers Prev. 2010;19:2401–6. doi: 10.1158/1055-9965.EPI-10-0503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer Inst. 2010;102:605–13. doi: 10.1093/jnci/djq099. [DOI] [PubMed] [Google Scholar]
- 32.Swerlick RA, Chen S. The melanoma epidemic: more apparent than real? Mayo Clin Proc. 1997;72:559–64. doi: 10.4065/72.6.559. [DOI] [PubMed] [Google Scholar]
- 33.Glusac EJ. The melanoma ‘epidemic’: lessons from prostate cancer. J Cutan Pathol. 2012;39:17–20. doi: 10.1111/j.1600-0560.2011.01848.x. [DOI] [PubMed] [Google Scholar]
- 34.Lakhani NA, Saraiya M, Thompson TD, King SC, Guy GP., Jr Total body skin examination for skin cancer screening among U.S. adults from 2000 to 2010. Prev Med. 2014;61:75–80. doi: 10.1016/j.ypmed.2014.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Shaikh WR, Dusza SW, Weinstock MA, Oliveria SA, Geller AC, Halpern AC. Melanoma thickness and survival trends in the United States, 1989 to 2009. J Natl Cancer Inst. 2016;108:djv294. doi: 10.1093/jnci/djv294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jemal A, Saraiya M, Patel P, et al. Recent trends in cutaneous melanoma incidence and death rates in the United States, 1992–2006. J Am Acad Dermatol. 2011;65:S17–25.e1-3. doi: 10.1016/j.jaad.2011.04.032. [DOI] [PubMed] [Google Scholar]
- 37.Linos E, Swetter SM, Cockburn MG, Colditz GA, Clarke CA. Increasing burden of melanoma in the United States. J Invest Dermatol. 2009;129:1666–74. doi: 10.1038/jid.2008.423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.U.S. Department of Health and Human Services. United States cancer statistics: 1999–2012 mortality. 2015 http://wonder.cdc.gov/CancerMort-v2012.html Accessed December 20, 2015.
- 39.Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27:6199–206. doi: 10.1200/JCO.2009.23.4799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pollack LA, Li J, Berkowitz Z, et al. Melanoma survival in the United States, 1992 to 2005. J Am Acad Dermatol. 2011;65:S78–86. doi: 10.1016/j.jaad.2011.05.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Howlader N, Noone AM, Krapcho M, et al., editors. SEER Cancer Statistics Review. National Cancer Institute; Bethesda, MD: 1975–2012. http://seer.cancer.gov/csr/1975_2012/, based on November 2014 SEER data submission, posted to the SEER website April 2015. [Google Scholar]
- 42.Guy GP, Ekwueme DU. Years of potential life lost and indirect costs of melanoma and non-melanoma skin cancer: a systematic review of the literature. Pharmacoeconomics. 2011;29:863–74. doi: 10.2165/11589300-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 43.Lucas RM, McMichael AJ, Armstrong BK, Smith WT. Estimating the global disease burden due to ultraviolet radiation exposure. Int J Epidemiol. 2008;37:654–667. doi: 10.1093/ije/dyn017. [DOI] [PubMed] [Google Scholar]
- 44.Green AC, Williams GM, Logan V, Strutton GM. Reduced melanoma after regular sunscreen use: randomized trial follow-up. J Clin Oncol. 2011;29:257–263. doi: 10.1200/JCO.2010.28.7078. [DOI] [PubMed] [Google Scholar]
- 45.Dennis LK, Vanbeek MJ, Beane Freeman LE, Smith BJ, Dawson DV, Coughlin JA. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Ann Epidemiol. 2008;18:614–627. doi: 10.1016/j.annepidem.2008.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomarkers Prev. 2014;23:1080–9. doi: 10.1158/1055-9965.EPI-13-0821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wehner MR, Shive ML, Chren MM, Han J, Qureshi AA, Linos E. Indoor tanning and non-melanoma skin cancer: systematic review and meta-analysis. BMJ. 2012;345:e5909. doi: 10.1136/bmj.e5909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Boniol M, Autier P, Boyle P, Gandini S. Cutaneous melanoma attributable to sunbed use: systematic review and meta-analysis. BMJ. 2012;345:e4757. doi: 10.1136/bmj.e4757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Boniol M, Autier P, Boyle P, Gandini S. Correction: cutaneous melanoma attributable to sunbed use: systematic review and meta-analysis. BMJ. 2012;345:e8503. doi: 10.1136/bmj.e8503.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ferrucci LM, Cartmel B, Molinaro AM, Leffell DJ, Bale AE, Mayne ST. Indoor tanning and risk of early-onset basal cell carcinoma. J Am Acad Dermatol. 2012;67:552–562. doi: 10.1016/j.jaad.2011.11.940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hodis E, Watson IR, Kryukov GV, et al. A landscape of driver mutations in melanoma. Cell. 2012;150:251–63. doi: 10.1016/j.cell.2012.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Lawrence MS, Stojanov P, Polak P, et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature. 2013;499:214–8. doi: 10.1038/nature12213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.The Cancer Genome Atlas Network. Genomic Classification of Cutaneous Melanoma. Cell. 2015;161:1681–96. doi: 10.1016/j.cell.2015.05.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gallagher RP, Elwood JM, Yang CP. Is chronic sunlight exposure important in accounting for increases in melanoma incidence? Int J Cancer. 1989;44:813–5. doi: 10.1002/ijc.2910440511. [DOI] [PubMed] [Google Scholar]
- 55.Pukkala E, Martinsen JI, Lynge E, et al. Occupation and cancer – follow-up of 15 million people in five Nordic countries. Acta Oncol. 2009;48:646–790. doi: 10.1080/02841860902913546. [DOI] [PubMed] [Google Scholar]
- 56.Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol. 2002;146(Suppl 61):1–6. doi: 10.1046/j.1365-2133.146.s61.2.x. [DOI] [PubMed] [Google Scholar]
- 57.Leiter U, Garbe C. Epidemiology of melanoma and non-melanoma skin cancer—the role of sunlight. In: Reichrath J, editor. Sunlight, Vitamin D and Skin Cancer. Vol. 624. New York, NY: Springer; 2008. pp. 89–103. [DOI] [PubMed] [Google Scholar]
- 58.Chang YM, Barrett JH, Bishop DT, et al. Sun exposure and melanoma risk at different latitudes: a pooled analysis of 5700 cases and 7216 controls. Int J Epidemiol. 2009;38:814–30. doi: 10.1093/ije/dyp166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Whiteman DC, Stickley M, Watt P, Hughes MC, Davis MB, Green AC. Anatomic site, sun exposure, and risk of cutaneous melanoma. J Clin Oncol. 2006;24:3172–7. doi: 10.1200/JCO.2006.06.1325. [DOI] [PubMed] [Google Scholar]
- 60.Nahar VK, Allison Ford M, Brodell RT, et al. Skin cancer prevention practices among malignant melanoma survivors: a systematic review [Epub ahead of print Epub ahead of print December 7, 2015] J Cancer Res Clin Oncol. 2015 doi: 10.1007/s00432-015-2086-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Cokkinides V, Weinstock M, Glanz K, Albano J, Ward E, Thun M. Trends in sunburns, sun protection practices, and attitudes toward sun exposure protection and tanning among US adolescents, 1998–2004. Pediatrics. 2006;118:853–64. doi: 10.1542/peds.2005-3109. [DOI] [PubMed] [Google Scholar]
- 62.Dusza SW, Halpern AC, Satagopan JM, et al. Prospective study of sunburn and sun behavior patterns during adolescence. Pediatrics. 2012;129:309–17. doi: 10.1542/peds.2011-0104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Guide to Community Preventive Services. Preventing skin cancer: education and policy approaches. www.thecommunityguide.org/cancer/skin/education-policy/index.html. Last updated: May 22, 2014.
- 64.Australian Institute of Health and Welfare. Cancer in Australia: an overview. Canberra: AIHW; 2014. (Cancer series no. 78. Cat. no. CAN 75). [Google Scholar]
- 65.SunSmart Victoria. History. 2015 http://www.sunsmart.com.au/about/history. Accessed December 20, 2015.
- 66.Olsen CM, Williams PF, Whiteman DC. Turning the tide? Changes in treatment rates for keratinocyte cancers in Australia 2000 through 2011. J Am Acad Dermatol. 2014;71:21–6.e1. doi: 10.1016/j.jaad.2014.02.011. [DOI] [PubMed] [Google Scholar]
- 67.Iannacone MR, Youlden DR, Baade PD, Aitken JF, Green AC. Melanoma incidence trends and survival in adolescents and young adults in Queensland, Australia. Int J Cancer. 2015;136:603–9. doi: 10.1002/ijc.28956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Olsen CM, Wilson LF, Green AC, et al. Cancers in Australia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471–476. doi: 10.1111/1753-6405.12470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Shih ST, Carter R, Sinclair C, Mihalopoulos C, Vos T. Economic evaluation of skin cancer prevention in Australia. Prev Med. 2009;49:449–53. doi: 10.1016/j.ypmed.2009.09.008. [DOI] [PubMed] [Google Scholar]
- 70.Glanz K, Saraiya M, Wechsler H, Centers for Disease Control and Prevention Guidelines for school programs to prevent skin cancer. MMWR Recomm Rep. 2002;51(RR-4):1–18. [PubMed] [Google Scholar]
- 71.Centers for Disease Control and Prevention. Shade Planning for America’s Schools. 2008 www.cdc.gov/cancer/skin/pdf/shade_planning.pdf Accessed June 15, 2015.
- 72.Everett Jones S, Barrios L, Feldman M, Hall-Jordan L. Results from the School Health Policies and Practices Study 2012. U.S. Department of Health and Human Services Centers for Disease Control and Prevention; 2013. Safe and healthy school environment: results from the School Health Policies and Practices Study 2012; pp. 91–109. editor. [Google Scholar]
- 73.U.S. Department of Health and Human Services Centers for Disease Control and Prevention. Results from the School Health Policies and Practices Study 2014. 2015:91–109. http://www.cdc.gov/healthyyouth/data/shpps/pdf/shpps-508-final_101315.pdf.
- 74.Act of June 1, 2015, 84th Leg., R.S., ch. 1139, §1, 2015 Tex. Gen. Laws 3849 – 3850 (codified at Tex. Education Code §38.021).
- 75.California Senate Bill 1632. http://www.leginfo.ca.gov/pub/01-02/bill/sen/sb_1601-1650/sb_1632_bill_20020826_chaptered.html. Accessed December 20, 2015.
- 76.78th Oregon Legislative Assembly. Enrolled House Bill 3041 (HB 3041-A) https://olis.leg.state.or.us/liz/2015R1/Downloads/MeasureDocument/HB3041. Accessed December 20, 2015.
- 77.City of Phoenix Parks and Recreation. Tree & Shade. 2015 https://www.phoenix.gov/parks/parks/urban-forest/tree-and-shade. Accessed December 20, 2015.
- 78.Toronto Cancer Prevention Coalition. Shade Guidelines. 2010 https://www1.toronto.ca/city_of_toronto/toronto_public_health/healthy_public_policy/tcpc/files/pdf/shade_guidelines.pdf. Accessed December 20, 2015.
- 79.Flechas J. Miami Beach unveils free sunscreen dispensers on sand. 2015 http://www.miamiherald.com/news/local/community/miami-dade/miami-beach/article14060885.html. Accessed December 20, 2015.
- 80.Ducharme J. Boston parks now have free sunscreen dispensers to combat skin cancer. 2015 http://www.bostonmagazine.com/health/blog/2015/06/30/boston-parks-sunscreen-dispensers/. Accessed December 20, 2015.
- 81.Florida Gators Football. Gator football game day initiatives. 2015 http://floridagators.com/news/2015/9/2/31084.aspx. Accessed December 20, 2015.
- 82.Beauchamp J. Stadium Village fan zone offers relief from heat & freebies. 2015 http://www.news4jax.com/sports/stadium-village-fan-zone-offers-relief-from-heat-freebies. Accessed December 20, 2015.
- 83.Cordova R, Hwang K. Cactus League preview: Salt River Fields stadium guide. 2015 http://www.azcentral.com/story/entertainment/events/2015/02/25/cactus-league-stadium-guide-salt-river-fields-at-talking-stick/24009267/?from=global&sessionKey=&autologin=. Accessed December 20, 2015.
- 84.State of Rhode Island Department of Health. About skin cancer. http://www.health.ri.gov/cancer/skin/. Accessed December 20, 2015.
- 85.The University of Texas MD Anderson Cancer Center. Skin Cancer Prevention Toolkit for Institutions of Higher Education. The University of Texas MD Anderson Cancer Center. 2015 http://www.texascancer.info/pdfs/skin_cancer_prevention_toolkit.pdf. Accessed January 15, 2016.
- 86.Hornung RL, Magee KH, Lee WJ, Hansen LA, Hsieh YC. Tanning facility use: are we exceeding Food and Drug Administration limits? J Am Acad Dermatol. 2003;49:655–61. doi: 10.1067/s0190-9622(03)01586-x. [DOI] [PubMed] [Google Scholar]
- 87.Miller SA, Hamilton SL, Wester UG, Cyr WH. An analysis of UVA emissions from sunlamps and the potential importance for melanoma. Photochem Photobiol. 1998;68:63–70. [PubMed] [Google Scholar]
- 88.National Toxicology Program. Ultraviolet radiation related exposures: solar radiation, exposure to sunlamps or sunbeds, broad-spectrum UVR, UVA, UVB, UVC. Rep Carcinog. 2011;12:429–33. [PubMed] [Google Scholar]
- 89.World Health Organization. Ultraviolet radiation and health. http://www.who.int/uv/uv_and_health/en/index.html. Accessed January 26, 2016.
- 90.Guy GP, Jr, Watson M, Haileyesus T, Annest JL. Indoor tanning-related injuries treated in a national sample of U.S. hospital emergency departments. JAMA Intern Med. 2015;175:309–311. doi: 10.1001/jamainternmed.2014.6697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.International Agency for Research on Cancer Working Group on Artificial Ultraviolet (UV) Light and Skin Cancer. The association of use of sunbeds with cutaneous malignant melanoma and other skin cancers: A systematic review. Int J Cancer. 2006;120:1116–22. doi: 10.1002/ijc.22453. [DOI] [PubMed] [Google Scholar]
- 92.Fisher DE, James WD. Indoor tanning–science, behavior, and policy. N Engl J Med. 2010;363:901–3. doi: 10.1056/NEJMp1005999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Lazovich D, Vogel RI, Berwick M, Weinstock MA, Anderson KE, Warshaw EM. Indoor tanning and risk of melanoma: a case-control study in a highly exposed population. Cancer Epidemiol Biomarkers Prev. 2010;19:1557–1568. doi: 10.1158/1055-9965.EPI-09-1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Cust AE, Armstrong BK, Goumas C, et al. Sunbed use during adolescence and early adulthood is associated with increased risk of early-onset melanoma. Int J Cancer. 2011;128:2425–2435. doi: 10.1002/ijc.25576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Lazovich D, Isaksson Vogel R, Weinstock MA, Nelson HH, Ahmed RL, Berwick M. Association between indoor tanning and melanoma in younger men and women [Epub ahead of print January 27, 2016] JAMA Dermatol. 2016 doi: 10.1001/jamadermatol.2015.2938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Veierod MB, Adami HO, Lund E, Armstrong BK, Weiderpass E. Sun and solarium exposure and melanoma risk: effects of age, pigmentary characteristics, and nevi. Cancer Epidemiol Biomarkers Prev. 2010;19:111–20. doi: 10.1158/1055-9965.EPI-09-0567. [DOI] [PubMed] [Google Scholar]
- 97.Colantonio S, Bracken MB, Beecker J. The association of indoor tanning and melanoma in adults: systematic review and meta-analysis. J Am Acad Dermatol. 2014;70:847–857 e01-18. doi: 10.1016/j.jaad.2013.11.050. [DOI] [PubMed] [Google Scholar]
- 98.Edwards J. Tanning salons in the U.S. IBISWorld Industry Report 81219c. 2013 Aug; [Google Scholar]
- 99.Hoerster KD, Garrow RL, Mayer JA, et al. Density of indoor tanning facilities in 116 large U.S. cities. Am J Prev Med. 2009;36:243–246. doi: 10.1016/j.amepre.2008.10.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Hillhouse J, Stapleton JL, Florence LC, Pagoto S. Prevalence and correlates of indoor tanning in nonsalon locations among a national sample of young women. JAMA Dermatol. 2015;151:1134–6. doi: 10.1001/jamadermatol.2015.1323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Pagoto SL, Lemon SC, Oleski JL, et al. Availability of tanning beds on U.S. college campuses. JAMA Dermatol. 2015;151:59–63. doi: 10.1001/jamadermatol.2014.3590. [DOI] [PubMed] [Google Scholar]
- 102.Levine JA, Sorace M, Spencer J, Siegel DM. The indoor UV tanning industry: a review of skin cancer risk, health benefit claims, and regulation. J Am Acad Dermatol. 2005;53:1038–1044. doi: 10.1016/j.jaad.2005.07.066. [DOI] [PubMed] [Google Scholar]
- 103.Mansh M, Katz KA, Linos E, Chren MM, Arron S. Association of skin cancer and indoor tanning in sexual minority men and women. JAMA Dermatol. 2015;151:1308–1316. doi: 10.1001/jamadermatol.2015.3126. [DOI] [PubMed] [Google Scholar]
- 104.O’Riordan DL, Field AE, Geller AC, et al. Frequent tanning bed use, weight concerns, and other health risk behaviors in adolescent females (United States) Cancer Causes Control. 2006;17:679–86. doi: 10.1007/s10552-005-0453-9. [DOI] [PubMed] [Google Scholar]
- 105.Miyamoto J, Berkowitz Z, Jones SE, Saraiya M. Indoor tanning device use among male high school students in the United States. J Adolesc Health. 2012;50:308–10. doi: 10.1016/j.jadohealth.2011.08.007. [DOI] [PubMed] [Google Scholar]
- 106.Sendelweck MA, Bell E, Anderson AM, et al. Associations between indoor tanning and substance use among Colorado high school students [Epub ahead of print January 20, 2016] JAMA Dermatol. 2016 doi: 10.1001/jamadermatol.2015.5663. [DOI] [PubMed] [Google Scholar]
- 107.Heckman CJ, Cohen-Filipic J, Darlow S, Kloss JD, Manne SL, Munshi T. Psychiatric and addictive symptoms of young adult female indoor tanners. Am J Health Promot. 2014;28:168–74. doi: 10.4278/ajhp.120912-QUAN-442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Mosher CE, Danoff-Burg S. Indoor tanning, mental health, and substance use among college students: the significance of gender. J Health Psychol. 2010;15:819–27. doi: 10.1177/1359105309357091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Monfrecola G, Fabbrocini G, Posteraro G, Pini D. What do young people think about the dangers of sunbathing, skin cancer and sunbeds? A questionnaire survey among Italians. Photodermatol Photoimmunol Photomed. 2000;16:15–8. doi: 10.1034/j.1600-0781.2000.160105.x. [DOI] [PubMed] [Google Scholar]
- 110.Holman DM, Fox KA, Glenn JD, et al. Strategies to reduce indoor tanning: current research gaps and future opportunities for prevention. Am J Prev Med. 2013;44:672–81. doi: 10.1016/j.amepre.2013.02.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Mahoney A, Swetter SM, Biello KB, Resnick EA, Feuerstein I, Geller AC. Attitudes toward indoor tanning among users of sunless tanning products. Arch Dermatol. 2012;148:124–6. doi: 10.1001/archderm.148.1.123. [DOI] [PubMed] [Google Scholar]
- 112.Brooks K, Brooks D, Dajani Z, et al. Use of artificial tanning products among young adults. J Am Acad Dermatol. 2006;54:1060–6. doi: 10.1016/j.jaad.2006.01.014. [DOI] [PubMed] [Google Scholar]
- 113.Quinn M, Alamian A, Hillhouse J, Scott C, Turrisi R, Baker K. Prevalence and correlates of indoor tanning and sunless tanning product use among female teens in the United States. Prev Med Rep. 2015;2:40–43. doi: 10.1016/j.pmedr.2014.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.U.S. Food and Drug Administration. Tanning Products. http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/Tanning/ucm116434.htm. Accessed December 20, 2015.
- 115.Hillhouse JJ, Baker MK, Turrisi R, et al. Evaluating a measure of tanning abuse and dependence. Arch Dermatol. 2012;148:815–9. doi: 10.1001/archdermatol.2011.2929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Stapleton JL, Hillhouse JJ, Turrisi R, Baker K, Manne SL, Coups EJ. The Behavioral Addiction Indoor Tanning Screener (BAITS): an evaluation of a brief measure of behavioral addictive symptoms. Acta Derm Venereol. 2015 doi: 10.2340/00015555-2290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Heckman CJ, Darlow S, Kloss JD, et al. Measurement of tanning dependence. J Eur Acad Dermatol Venereol. 2014;28:1179–1185. doi: 10.1111/jdv.12243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders: DSM 5. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- 119.First M, Spitzer R, Gibbon M, Williams J. Structured Clinical Interview for DSM-IV Axis I Disorders (SCID) New York, NY: New York State Psychiatric Institute Biometrics Research Department; 1995. [Google Scholar]
- 120.Mayfield D, McLeod G, Hall P. The CAGE questionnaire: validation of a new alcoholism screening instrument. Am J Psychiatry. 1974;131:1121–3. doi: 10.1176/ajp.131.10.1121. [DOI] [PubMed] [Google Scholar]
- 121.Harrington CR, Beswick TC, Graves M, et al. Activation of the mesostriatal reward pathway with exposure to ultraviolet radiation (UVR) vs. sham UVR in frequent tanners: a pilot study. Addict Biol. 2012;17:680–6. doi: 10.1111/j.1369-1600.2010.00312.x. [DOI] [PubMed] [Google Scholar]
- 122.Feldman SR, Liguori A, Kucenic M, et al. Ultraviolet exposure is a reinforcing stimulus in frequent indoor tanners. J Am Acad Dermatol. 2004;51:45–51. doi: 10.1016/j.jaad.2004.01.053. [DOI] [PubMed] [Google Scholar]
- 123.Kaur M, Liguori A, Lang W, Rapp SR, Fleischer AB, Jr, Feldman SR. Induction of withdrawal-like symptoms in a small randomized, controlled trial of opioid blockade in frequent tanners. J Am Acad Dermatol. 2006;54:709–11. doi: 10.1016/j.jaad.2005.11.1059. [DOI] [PubMed] [Google Scholar]
- 124.Fell GL, Robinson KC, Mao J, Woolf CJ, Fisher DE. Skin beta-endorphin mediates addiction to UV light. Cell. 2014;157:1527–34. doi: 10.1016/j.cell.2014.04.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Association of American Cancer Institutes. AACI CancerBlog. UV Safety Month Fuels Efforts to Ban Indoor Tanning. 2015 Jul 15; Posted on. http://www.aaci-cancer.org/pdf/JointPositionStatementonIndoorTanning07. Accessed January 26, 2016.
- 126.U.S. Food and Drug Administration. Center for Devices and Radiological Health, Medical Devices Advisory Committee. General and plastic surgery devices panel: transcript. 2010 http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/GeneralandPlasticSurgeryDevicesPanel/UCM210232.pdf. Accessed December 20, 2015.
- 127.Congress Mandates Better Skin Cancer Warnings on Tanning Beds. https://maloney.house.gov/media-center/press-releases/congress-mandates-better-skin-cancer-warnings-tanning-beds. Accessed January 17, 2016.
- 128.U.S. Patient Protection and Affordable Care Act. https://www.gpo.gov/fdsys/pkg/PLAW-111publ148/html/PLAW-111publ148.htm. Accessed March 5, 2016.
- 129.U.S. Internal Revenue Service. Indoor Tanning Services; Excise Taxes. Filed by the Office of the Federal Register on June 10, 2013 and published in the issue of the Federal Register for June 11, 2013, 78 FR 34874. https://www.irs.gov/irb/2013-28_IRB/ar06.html. Accessed March 5, 2016.
- 130.Treasury Inspector General for Tax Administration. Affordable Care Act: The number of taxpayers filing tanning excise tax returns is lower than expected. 2011 Sep 22; Reference Number: 2011-40-115. https://www.treasury.gov/tigta/auditreports/2011reports/201140115fr.pdf.
- 131.Jain N, Rademaker A, Robinson JK. Implementation of the federal excise tax on indoor tanning services in Illinois. Arch Dermatol. 2012;148:122–4. doi: 10.1001/archderm.148.1.122. [DOI] [PubMed] [Google Scholar]
- 132.National Conference of State Legislatures. Indoor tanning restrictions for minors – a state-by-state comparison. http://www.ncsl.org/research/health/indoor-tanning-restrictions.aspx. Accessed December 29, 2015.
- 133.AIM at Melanoma Foundation. Global Advocacy and Engagement. Melanoma Legislation. https://www.aimatmelanoma.org/global-advocacy-and-engagement/melanoma-legislation/. Accessed January 26, 2016.
- 134.Culley CA, Mayer JA, Eckhardt L, et al. Compliance with federal and state legislation by indoor tanning facilities in San Diego. J Am Acad Dermatol. 2001;44:53–60. doi: 10.1067/mjd.2001.110063. [DOI] [PubMed] [Google Scholar]
- 135.Fleischer AB, Jr, Lee WJ, Adams DP, Zanolli MD. Tanning facility compliance with state and federal regulations in North Carolina: a poor performance. J Am Acad Dermatol. 1993;28:212–217. doi: 10.1016/0190-9622(93)70029-s. [DOI] [PubMed] [Google Scholar]
- 136.Forster JL, Lazovich D, Hickle A, Sorensen G, Demierre MF. Compliance with restrictions on sale of indoor tanning sessions to youth in Minnesota and Massachusetts. J Am Acad Dermatol. 2006;55:962–967. doi: 10.1016/j.jaad.2006.06.036. [DOI] [PubMed] [Google Scholar]
- 137.Cokkinides V, Weinstock M, Lazovich D, Ward E, Thun M. Indoor tanning use among adolescents in the US, 1998 to 2004. Cancer. 2009;115:190–8. doi: 10.1002/cncr.24010. [DOI] [PubMed] [Google Scholar]
- 138.Mayer JA, Woodruff SI, Slymen DJ, et al. Adolescents’ use of indoor tanning: a large-scale evaluation of psychosocial, environmental, and policy-level correlates. Am J Public Health. 2011;101:930–938. doi: 10.2105/AJPH.2010.300079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Guy GP, Jr, Berkowitz Z, Jones SE, et al. State indoor tanning laws and adolescent indoor tanning. Am J Public Health. 2014;104:e69–e74. doi: 10.2105/AJPH.2013.301850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Bulger AL, Mayer JE, Gershenwald JE, Guild SR, Gottlieb MA, Geller AC. Enforcement provisions of indoor tanning bans for minors: an analysis of the first 6 U.S. States. Am J Public Health. 2015;105:e10–e12. doi: 10.2105/AJPH.2015.302684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Grewal SK, Haas AF, Pletcher MJ, Resneck JS., Jr Compliance by California tanning facilities with the nation’s first statewide ban on use before the age of 18 years. J Am Acad Dermatol. 2013;69:883–889 e4. doi: 10.1016/j.jaad.2013.09.016. [DOI] [PubMed] [Google Scholar]
- 142.Hurd AL, Mayer JA, Woodruff SI, Belch GE, Patel MR. Comparing two methods of measuring legislation compliance among indoor tanning facilities. Journal of the American Academy of Dermatology. 2006;54:433–439. doi: 10.1016/j.jaad.2005.11.1078. [DOI] [PubMed] [Google Scholar]
- 143.World Health Organization. Artificial Tanning Sunbeds Risks and Guidance. 2003 http://www.who.int/uv/publications/en/sunbeds.pdf. Accessed December 20, 2015.
- 144.Cancer Council Australia. National Cancer Control Policy. http://wiki.cancer.org.au/policy/Position_statement_-_Solariums. Accessed January 14, 2016.
- 145.Centers for Disease Control and Prevention. Skin Cancer: http://www.cdc.gov/cancer/skin/basic_info/indoor_tanning.htm. Accessed January 21, 2016. [Google Scholar]
- 146.Pawlak MT, Bui M, Amir M, Burkhardt DL, Chen AK, Dellavalle RP. Legislation restricting access to indoor tanning throughout the world. Arch Dermatol. 2012;148:1006–1012. doi: 10.1001/archdermatol.2012.2080. [DOI] [PubMed] [Google Scholar]
- 147.U.S. Federal Trade Commission. Indoor Tanning Association Settles FTC Charges That It Deceived Consumers About Skin Cancer Risks From Tanning. https://www.ftc.gov/news-events/press-releases/2010/01/indoor-tanning-association-settles-ftc-charges-it-deceived. Accessed January 1, 2016.
- 148.Marketers of Indoor Tanning Systems to Pay Refunds to Consumers. https://www.ftc.gov/news-events/press-releases/2016/04/marketers-indoor-tanning-systems-pay-refunds-consumers. Accessed April 20, 2016.
- 149.U.S. House of Representatives Committee on Energy and Commerce—Minority Staff. False and Misleading Health Information Provided to Teens by the Indoor Tanning Industry: Investigative Report. https://democrats-energycommerce.house.gov/sites/democrats.energycommerce.house.gov/files/False-Health-Info-by-Indoor-Tanning-Industry-2012-2-1.pdf Accessed January 1, 2016.
- 150.Clique 2 Houston. Darque Tan, Texas settle lawsuit over tanning bed claims. http://www.click2houston.com/news/darque-tan-texas-settle-lawsuit-over-tanning-bed-claims_20151124031337839. Accessed January 1, 2016.
- 151.Office of the New York State Attorney General. A.G. Schneiderman Announces Agreements Barring National Tanning Salon Chain Hollywood Tans And Manhattan Franchise From Making Health Claims. http://www.ag.ny.gov/press-release/ag-schneiderman-announces-agreements-barring-national-tanning-salon-chain-hollywood. Accessed December 31, 2015.
- 152.Office of the New York State Attorney General. A.G. Schneiderman Announces Lawsuits Accusing Two NYC & Upstate Tanning Salon Companies Of Unlawfully Concealing Indoor Tanning Risks. http://www.ag.ny.gov/press-release/ag-schneiderman-announces-lawsuits-accusing-two-nyc-upstate-tanning-salon-companies Accessed January 1, 2016.
- 153.Office of the New York State Attorney General. A.G. Schneiderman Announces Agreement With Planet Fitness To Cease Advertising Practices That Encourage Frequent Indoor Tanning. http://www.ag.ny.gov/press-release/ag-schneiderman-announces-agreement-planet-fitness-cease-advertising-practices. Accessed January 1, 2016.
- 154.Geller AC, O’Riordan DL, Oliveria SA, Valvo S, Teich M, Halpern AC. Overcoming obstacles to skin cancer examinations and prevention counseling for high-risk patients: results of a national survey of primary care physicians. J Am Board Fam Pract. 2004;17:416–23. doi: 10.3122/jabfm.17.6.416. [DOI] [PubMed] [Google Scholar]
- 155.Bandi P, Cokkinides VE, Weinstock MA, Ward EM. Physician sun protection counseling: prevalence, correlates, and association with sun protection practices among US adolescents and their parents, 2004. Prev Med. 2010;51:172–7. doi: 10.1016/j.ypmed.2010.05.003. [DOI] [PubMed] [Google Scholar]
- 156.Dietrich AJ, Olson AL, Sox CH, Winchell CW, Grant-Petersson J, Collison DW. Sun protection counseling for children: primary care practice patterns and effect of an intervention on clinicians. Arch Fam Med. 2000;9:155–9. doi: 10.1001/archfami.9.2.155. [DOI] [PubMed] [Google Scholar]
- 157.Balk SJ, O’Connor KG, Saraiya M. Counseling parents and children on sun protection: a national survey of pediatricians. Pediatrics. 2004;114:1056–64. doi: 10.1542/peds.2004-1305. [DOI] [PubMed] [Google Scholar]
- 158.U.S. Preventive Services Task Force. Final Update Summary: Skin Cancer: Counseling. 2012 http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/skin-cancer-counseling. Accessed December 20, 2015.
- 159.Moyer VA, on behalf of the U.S. Preventive Services Task Force Behavioral counseling to prevent skin cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:59–65. doi: 10.7326/0003-4819-157-1-201207030-00442. [DOI] [PubMed] [Google Scholar]
- 160.Hillhouse J, Turrisi R, Stapleton J, Robinson J. A randomized controlled trial of an appearance-focused intervention to prevent skin cancer. Cancer. 2008;113:3257–66. doi: 10.1002/cncr.23922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Stapleton J, Turrisi R, Hillhouse J, Robinson JK, Abar B. A comparison of the efficacy of an appearance-focused skin cancer intervention within indoor tanner subgroups identified by latent profile analysis. J Behav Med. 2010;33:181–90. doi: 10.1007/s10865-009-9246-z. [DOI] [PubMed] [Google Scholar]
- 162.Turrisi R, Mastroleo NR, Stapleton J, Mallett K. A comparison of 2 brief intervention approaches to reduce indoor tanning behavior in young women who indoor tan very frequently. Arch Dermatol. 2008;144:1521–4. doi: 10.1001/archderm.144.11.1521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Norman GJ, Adams MA, Calfas KJ, et al. A randomized trial of a multicomponent intervention for adolescent sun protection behaviors. Arch Pediatr Adolesc Med. 2007;161:146–52. doi: 10.1001/archpedi.161.2.146. [DOI] [PubMed] [Google Scholar]
- 164.Mahler HI, Kulik JA, Gerrard M, Gibbons FX. Long-term effects of appearance-based interventions on sun protection behaviors. Health Psychol. 2007;26:350–60. doi: 10.1037/0278-6133.26.3.350. [DOI] [PubMed] [Google Scholar]
- 165.Fox JB, Shaw FE. Clinical preventive services coverage and the Affordable Care Act. Am J Public Health. 2015;105:e7–e10. doi: 10.2105/AJPH.2014.302289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Balk SJ, Council on Environmental Health Section on Dermatology Ultraviolet radiation: a hazard to children and adolescents. Pediatrics. 2011;127:e791–817. doi: 10.1542/peds.2010-3502. [DOI] [PubMed] [Google Scholar]
- 167.Balk SJ, Fisher DE, Geller AC. Teens and indoor tanning: a cancer prevention opportunity for pediatricians. Pediatrics. 2013;131:772–85. doi: 10.1542/peds.2012-2404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Berwick M, Begg CB, Fine JA, Roush GC, Barnhill RL. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst. 1996;88:17–23. doi: 10.1093/jnci/88.1.17. [DOI] [PubMed] [Google Scholar]
- 169.Berwick M, Armstrong BK, Ben-Porat L, et al. Sun exposure and mortality from melanoma. J Natl Cancer Inst. 2005;97:195–9. doi: 10.1093/jnci/dji019. [DOI] [PubMed] [Google Scholar]
- 170.Leachman SA, Cassidy PB, Chen SC, et al. Methods of melanoma detection. Cancer Treat Res. 2016;167:51–105. doi: 10.1007/978-3-319-22539-5_3. [DOI] [PubMed] [Google Scholar]
- 171.Carli P, De Giorgi V, Palli D, et al. Dermatologist detection and skin self-examination are associated with thinner melanomas: results from a survey of the Italian Multidisciplinary Group on Melanoma. Arch Dermatol. 2003;139:607–12. doi: 10.1001/archderm.139.5.607. [DOI] [PubMed] [Google Scholar]
- 172.Swetter SM, Pollitt RA, Johnson TM, Brooks DR, Geller AC. Behavioral determinants of successful early melanoma detection: role of self and physician skin examination. Cancer. 2012;118:3725–34. doi: 10.1002/cncr.26707. [DOI] [PubMed] [Google Scholar]
- 173.Pollitt RA, Geller AC, Brooks DR, Johnson TM, Park ER, Swetter SM. Efficacy of skin self-examination practices for early melanoma detection. Cancer Epidemiol Biomarkers Prev. 2009;18:3018–23. doi: 10.1158/1055-9965.EPI-09-0310. [DOI] [PubMed] [Google Scholar]
- 174.Weinstock MA, Martin RA, Risica PM, et al. Thorough skin examination for the early detection of melanoma. Am J Prev Med. 1999;17:169–75. doi: 10.1016/s0749-3797(99)00077-x. [DOI] [PubMed] [Google Scholar]
- 175.Oliveria SA, Christos PJ, Halpern AC, Fine JA, Barnhill RL, Berwick M. Evaluation of factors associated with skin self-examination. Cancer Epidemiol Biomarkers Prev. 1999;8:971–8. [PubMed] [Google Scholar]
- 176.Oliveria SA, Dusza SW, Phelan DL, Ostroff JS, Berwick M, Halpern AC. Patient adherence to skin self-examination. effect of nurse intervention with photographs. Am J Prev Med. 2004;26:152–5. doi: 10.1016/j.amepre.2003.10.006. [DOI] [PubMed] [Google Scholar]
- 177.Weinstock MA, Risica PM, Martin RA, et al. Reliability of assessment and circumstances of performance of thorough skin self-examination for the early detection of melanoma in the Check-It-Out Project. Prev Med. 2004;38:761–5. doi: 10.1016/j.ypmed.2004.01.020. [DOI] [PubMed] [Google Scholar]
- 178.Aitken JF, Janda M, Lowe JB, et al. Prevalence of whole-body skin self-examination in a population at high risk for skin cancer (Australia) Cancer Causes Control. 2004;15:453–63. doi: 10.1023/B:CACO.0000036451.39128.f6. [DOI] [PubMed] [Google Scholar]
- 179.Robinson JK, Turrisi R, Stapleton J. Efficacy of a partner assistance intervention designed to increase skin self-examination performance. Arch Dermatol. 2007;143:37–41. doi: 10.1001/archderm.143.1.37. [DOI] [PubMed] [Google Scholar]
- 180.Robinson JK, Turrisi R, Mallett K, Stapleton J, Pion M. Comparing the efficacy of an in-person intervention with a skin self-examination workbook. Arch Dermatol. 2010;146:91–4. doi: 10.1001/archdermatol.2009.350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Janda M, Neale RE, Youl P, Whiteman DC, Gordon L, Baade PD. Impact of a video-based intervention to improve the prevalence of skin self-examination in men 50 years or older: the randomized skin awareness trial. Arch Dermatol. 2011;147:799–806. doi: 10.1001/archdermatol.2011.48. [DOI] [PubMed] [Google Scholar]
- 182.Chiu V, Won E, Malik M, Weinstock MA. The use of mole-mapping diagrams to increase skin self-examination accuracy. J Am Acad Dermatol. 2006;55:245–50. doi: 10.1016/j.jaad.2006.02.026. [DOI] [PubMed] [Google Scholar]
- 183.Epstein DS, Lange JR, Gruber SB, Mofid M, Koch SE. Is physician detection associated with thinner melanomas? JAMA. 1999;281:640–3. doi: 10.1001/jama.281.7.640. [DOI] [PubMed] [Google Scholar]
- 184.Aitken JF, Elwood M, Baade PD, Youl P, English D. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010;126:450–8. doi: 10.1002/ijc.24747. [DOI] [PubMed] [Google Scholar]
- 185.Kantor J, Kantor DE. Routine dermatologist-performed full-body skin examination and early melanoma detection. Arch Dermatol. 2009;145:873–6. doi: 10.1001/archdermatol.2009.137. [DOI] [PubMed] [Google Scholar]
- 186.Kovalyshyn I, Dusza SW, Siamas K, Halpern AC, Argenziano G, Marghoob AA. The impact of physician screening on melanoma detection. Arch Dermatol. 2011;147:1269–75. doi: 10.1001/archdermatol.2011.181. [DOI] [PubMed] [Google Scholar]
- 187.Swetter SM, Johnson TM, Miller DR, Layton CJ, Brooks KR, Geller AC. Melanoma in middle-aged and older men: a multi-institutional survey study of factors related to tumor thickness. Arch Dermatol. 2009;145:397–404. doi: 10.1001/archdermatol.2008.603. [DOI] [PubMed] [Google Scholar]
- 188.Terushkin V, Halpern AC. Melanoma early detection. Hematol Oncol Clin North Am. 2009;23:481–500. doi: 10.1016/j.hoc.2009.03.001. [DOI] [PubMed] [Google Scholar]
- 189.Aitken JF, Elwood JM, Lowe JB, Firman DW, Balanda KP, Ring IT. A randomised trial of population screening for melanoma. J Med Screen. 2002;9:33–7. doi: 10.1136/jms.9.1.33. [DOI] [PubMed] [Google Scholar]
- 190.Schneider JS, Moore DH, 2nd, Mendelsohn ML. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741–9. doi: 10.1016/j.jaad.2007.10.648. [DOI] [PubMed] [Google Scholar]
- 191.Katalinic A, Waldmann A, Weinstock MA, et al. Does skin cancer screening save lives?: an observational study comparing trends in melanoma mortality in regions with and without screening. Cancer. 2012;118:5395–402. doi: 10.1002/cncr.27566. [DOI] [PubMed] [Google Scholar]
- 192.Breitbart EW, Waldmann A, Nolte S, et al. Systematic skin cancer screening in Northern Germany. J Am Acad Dermatol. 2012;66:201–11. doi: 10.1016/j.jaad.2010.11.016. [DOI] [PubMed] [Google Scholar]
- 193.Katalinic A, Eisemann N, Waldmann A. Skin cancer screening in Germany. Dtsch Arztebl Int. 2015;112:629–634. doi: 10.3238/arztebl.2015.0629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Boniol M, Autier P, Gandini S. Melanoma mortality following skin cancer screening in Germany. BMJ Open. 2015;5:e008158. doi: 10.1136/bmjopen-2015-008158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195.Aitken JF, Youl PH, Janda M, Lowe JB, Ring IT, Elwood M. Increase in skin cancer screening during a community-based randomized intervention trial. Int J Cancer. 2006;118:1010–6. doi: 10.1002/ijc.21455. [DOI] [PubMed] [Google Scholar]
- 196.Aitken JF, Janda M, Elwood M, Youl PH, Ring IT, Lowe JB. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006;54:105–14. doi: 10.1016/j.jaad.2005.08.072. [DOI] [PubMed] [Google Scholar]
- 197.Curiel-Lewandrowski C, Chen SC, Swetter SM, on behalf of the Melanoma Prevention Working Group-Pigmented Skin Lesion Sub-Committee Screening and prevention measures for melanoma: is there a survival advantage? Curr Oncol Rep. 2012;14:458–67. doi: 10.1007/s11912-012-0256-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Coory M, Baade P, Aitken J, Smithers M, McLeod GR, Ring I. Trends for in situ and invasive melanoma in Queensland, Australia, 1982–2002. Cancer Causes Control. 2006;17:21–7. doi: 10.1007/s10552-005-3637-4. [DOI] [PubMed] [Google Scholar]
- 199.Stang A, Jockel KH. Does skin cancer screening save lives? A detailed analysis of mortality time trends in Schleswig-Holstein and Germany. Cancer. 2016;122:432–7. doi: 10.1002/cncr.29755. [DOI] [PubMed] [Google Scholar]
- 200.Geller AC, Greinert R, Sinclair C, et al. A nationwide population-based skin cancer screening in Germany: proceedings of the first meeting of the International Task Force on Skin Cancer Screening and Prevention (September 24 and 25, 2009) Cancer Epidemiol. 2010;34:355–8. doi: 10.1016/j.canep.2010.03.006. [DOI] [PubMed] [Google Scholar]
- 201.Screening for Skin Cancer in Adults: An Updated Systematic Evidence Review for the U.S. Preventive Services Task Force. Dec, 2015. Evidence Synthesis Number 137. (AJRQ Publication no. 14-05210-EF-1). (Prepared by Kaiser Permanente Research Affiliates Evidence-based Practice Center Group Health Research Institute – Seattle, WA: and Kaiser Permanante Center for Health Research – Portland, OR) [Google Scholar]
- 202.Karia PS, Jambusaria-Pahlajani A, Harrington DP, Murphy GF, Qureshi AA, Schmults CD. Evaluation of American Joint Committee on Cancer, International Union Against Cancer, and Brigham and Women’s Hospital tumor staging for cutaneous squamous cell carcinoma. J Clin Oncol. 2014;32:327–34. doi: 10.1200/JCO.2012.48.5326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 203.Moore MM, Geller AC, Zhang Z, et al. Skin cancer examination teaching in US medical education. Arch Dermatol. 2006;142:439–44. doi: 10.1001/archderm.142.4.439. [DOI] [PubMed] [Google Scholar]
- 204.Geller AC, Venna S, Prout M, et al. Should the skin cancer examination be taught in medical school? Arch Dermatol. 2002;138:1201–3. doi: 10.1001/archderm.138.9.1201. [DOI] [PubMed] [Google Scholar]
- 205.Oliveria SA, Heneghan MK, Cushman LF, Ughetta EA, Halpern AC. Skin cancer screening by dermatologists, family practitioners, and internists: barriers and facilitating factors. Arch Dermatol. 2011;147:39–44. doi: 10.1001/archdermatol.2010.414. [DOI] [PubMed] [Google Scholar]
- 206.Shaikh WR, Geller A, Alexander G, et al. Developing an interactive web-based learning program on skin cancer: the learning experiences of clinical educators. J Cancer Educ. 2012;27:709–16. doi: 10.1007/s13187-012-0378-4. [DOI] [PubMed] [Google Scholar]
- 207.Eide MJ, Asgari MM, Fletcher SW, et al. Effects on skills and practice from a web-based skin cancer course for primary care providers. J Am Board Fam Med. 2013;26:648–57. doi: 10.3122/jabfm.2013.06.130108. [DOI] [PubMed] [Google Scholar]
- 208.Grange F, Woronoff AS, Bera R, et al. Efficacy of a general practitioner training campaign for early detection of melanoma in France. Br J Dermatol. 2014;170:123–9. doi: 10.1111/bjd.12585. [DOI] [PubMed] [Google Scholar]
- 209.Weinstock MA. Early detection of melanoma. JAMA. 2000;284:886–9. doi: 10.1001/jama.284.7.886. [DOI] [PubMed] [Google Scholar]
- 210.Buller DB, Berwick M, Lantz K, et al. Evaluation of immediate and 12-week effects of a smartphone sun-safety mobile application: a randomized clinical trial. JAMA Dermatol. 2015;151:505–12. doi: 10.1001/jamadermatol.2014.3894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211.Jolly J. Wearable devices to prevent sunburn. 2015 http://well.blogs.nytimes.com/2015/06/16/wearable-devices-to-prevent-sunburn/. Accessed December 20, 2015.
- 212.Landow SM, Mateus A, Korgavkar K, Nightingale D, Weinstock MA. Teledermatology: key factors associated with reducing face-to-face dermatology visits. J Am Acad Dermatol. 2014;71:570–6. doi: 10.1016/j.jaad.2014.02.021. [DOI] [PubMed] [Google Scholar]
- 213.Landow SM, Oh DH, Weinstock MA. Teledermatology Within the Veterans Health Administration, 2002–2014. Telemed J E Health. 2015;21:769–73. doi: 10.1089/tmj.2014.0225. [DOI] [PubMed] [Google Scholar]
- 214.Carli P, Crocetti E, Chiarugi A, et al. The use of commercially available personal UV-meters does cause less safe tanning habits: a randomized-controlled trial. Photochem Photobiol. 2008;84:758–63. doi: 10.1111/j.1751-1097.2007.00256.x. [DOI] [PubMed] [Google Scholar]