

Abstract
This review provides an updated summary of the state of our knowledge of the genetic contributions to the pathogenesis of congenital heart disease. Since 2007, when the initial American Heart Association scientifi statement on the genetic basis of congenital heart disease was published, new genomic techniques have become widely available that have dramatically changed our understanding of the causes of congenital heart disease and, clinically, have allowed more accurate definition of the pathogeneses of congenital heart disease in patients of all ages and even prenatally. Information is presented on new molecular testing techniques and their application to congenital heart disease, both isolated and associated with other congenital anomalies or syndromes. Recent advances in the understanding of copy number variants, syndromes, RASopathies, and heterotaxy/ciliopathies are provided. Insights into new research with congenital heart disease models, including genetically manipulated animals such as mice, chicks, and zebrafish as well as human induced pluripotent stem cell–based approaches are provided to allow an understanding of how future research breakthroughs for congenital heart disease are likely to happen. It is anticipated that this review will provide a large range of health care–related personnel, including pediatric cardiologists, pediatricians, adult cardiologists, thoracic surgeons, obstetricians, geneticists, genetic counselors, and other related clinicians, timely information on the genetic aspects of congenital heart disease. The objective is to provide a comprehensive basis for interdisciplinary care for those with congenital heart disease.
Keywords: AHA Scientific Statements; heart defects, congenital; genetics
This review has been compiled to provide information for clinicians about new developments in our understanding of the genetic contributions to the pathogenesis of congenital heart disease (HD), providing an update of the 2007 American Heart Association scientific statement on this subject.1 Not included in this review that is intended to cover genetic aspects of structural heart defects are the aortopathies, arrhythmia/channelopathies, and isolated cardiomyopathies for which there are recent reviews.2–5 At the time the previous scientific statement was published, genetic testing techniques such as chromosomal microarray and next-generation sequencing (NGS) were not in wide use. Since the rapid dissemination of these testing modalities and others described in this review, discoveries of numerous pathogenic copy number variants (CNVs) and gene mutations have significantly advanced our understanding of the causes of congenital HD. Because of the availability of new genomic technologies, the pace of discovery of new genes for congenital HD is now very rapid.
CONGENITAL HD EPIDEMIOLOGY AND IMPORTANCE OF IDENTIFYING A GENETIC BASIS FOR CONGENITAL HD
Current research indicates that congenital HD is the most common birth defect, affecting nearly 10 to 12 per 1000 liveborn infants (1%–1.2%).6–8 Not all individuals with congenital HD are diagnosed early, so the actual prevalence has been difficult to determine, but one estimate from Canada suggested that the overall prevalence is 13.1 per 1000 children and 6.1 per 1000 adults.9 Their data also suggested that congenital HD prevalence increased 11% in children and 57% in adults from 2000 to 2010. The impact of successful medical and surgical management of congenital HD on the survival of individuals with congenital HD is likely contributing to a large extent to its increased prevalence among older children and adults. More and more patients with severe types of congenital HD are surviving into their 30s and beyond. Of note, estimates of congenital HD incidence and prevalence have not included cases of isolated bicuspid aortic valve (BAV), unarguably a form of congenital HD. Because the population prevalence of BAV is 1% to 2% (based on studies at autopsy and of liveborn infants and healthy adolescents), the total prevalence of congenital HD is closer to 2% to 3%.10–12
Epidemiological studies have suggested that a genetic or environmental cause can be identified in 20% to 30% of congenital HD cases.13 Single-gene disorders are found in 3% to 5%, gross chromosomal anomalies/aneuploidy in 8% to 10%, and pathogenic CNVs in 3% to 25% of those with congenital HD as part of a syndrome, and in 3% to 10% among those with isolated congenital HD. The largest genetic study of congenital HD with NGS suggested that 8% and 2% of cases are attributable to de novo autosomal dominant and inherited autosomal recessive variation, respectively.14 Environmental causes are identifiable in 2% of congenital HD cases. The unexplained remainder of congenital HD is presumed to be multifactorial (oligogenetic or some combination of genetic and environmental factors).13
Uncovering a genetic pathogenesis for congenital HD is increasingly clinically relevant, in part because of the aforementioned improved survival. For the clinician caring for a child or adult with congenital HD, important reasons for determining the genetic cause can include (1) assessing recurrence risks for the offspring of the congenital HD survivor, additional offspring of the parents, or other close relatives; (2) evaluating for associated extracardiac involvement; (3) assessing risk for neurodevelopmental delays for newborns and infants; and (4) providing more accurate prognosis for the congenital HD and outcomes for congenital HD–related interventions.
MOLECULAR TECHNIQUES AND DIAGNOSIS
Human Genetic Variation
In addition to aneuploidies and large chromosomal rearrangements, the past 10 years of genetics research has advanced a contemporary understanding of normal and pathogenic human genetic variation based on the concept of detecting individual differences relative to a reference sequence defined as normal. The human reference sequence for both medical and research use was released by the Human Genome Project in 2000 and has been corrected and refined in subsequent years.15,16 Multiple individuals were included in the creation of the reference, which can be thought of not as the genome of a single person but as being composed of genetic information from as many as 20 to 25 individuals.17 A single-nucleotide polymorphism (SNP) is a change in a single nucleotide of DNA (eg, reference GGTCTC, alternative GGTGTC). An insertion or deletion (INDEL) is a change in multiple nucleotides that results in a difference in length relative to the reference sequence (eg, reference GGTCTC, alternatives GGTGCGTC or GGTTC). CNVs constitute large insertions or deletions of DNA, frequently defined as >1000 nucleotides in length, and can occur anywhere throughout the genome (these lesions can also be referred to as microdeletions or microduplications). Each of these types of genetic variation has well-described causal roles in a variety of different diseases, including congenital HD, to be discussed in later sections.
Technologies and Testing Paradigms
Genetic testing can be divided into 2 categories; genomic tests capture ≥1 types of variation at all locations within the human genome, whereas targeted tests capture information about ≥1 select genetic locations (Table 1). There is now significant overlap between the types of variation detectable by different testing technologies. Genomic tests can offer an unbiased approach to detecting clinically relevant genetic variation, whereas targeted assays test a specific hypothesis about ≥1 genes or loci involved in disease.18 Many tests use, in some form, the principle of DNA hybridization by which a sequence of DNA can be separated into 2 complementary strands (eg, ATCGGTC binding to TAGCCAG), and these individual strands will bind very specifically to a synthetic complementary strand (for a specific region of the genome, genetic sequence, or series of genes) under appropriately controlled chemical conditions.
Table 1.
Clinical Tests
| Genomic vs Targeted | Aneuploidies and Chromosomal Rearrangements | Copy Number Variation | SNPs and INDELS | Example of Clinical Use | |
|---|---|---|---|---|---|
| Karyotype | Genomic | +++ | + | − | Confirmation of trisomy 21 |
| Array CGH | Genomic | ++ | +++ | − | Multiple congenital anomalies without obvious syndromic association |
| FISH | Targeted | + | + | − | Suspected 22q11.2 deletion syndrome |
| Gene panel testing | Targeted | − | + | +++ | Suspected monogenic disease with a small differential diagnosis |
| Exome sequencing | Genomic | − | − | +++ | Broad genetic differential diagnosis without obvious syndromic association, or previous negative panel testing |
| Genome sequencing | Genomic | + | + | +++ | Broad genetic differential diagnosis without obvious syndromic association, or previous negative panel testing and need for rapid turnaround time |
Sensitivity of tests for the types of genetic variation are indicated as not detected (−), low (+), medium (++), or high (+++). Array CGH indicates comparative genomic hybridization using arrays; FISH, fluorescence in situ hybridization; INDEL, insertion or deletion; and SNP, single-nucleotide polymorphism.
Large Genetic Variation
Karyotyping, a genomic test, is the gold standard for detecting aneuploidies and large chromosomal rearrangements that occur throughout the genome; it is performed on metaphase chromosomes in an automated or semiautomated process before review by a cytogeneticist. In comparative genomic hybridization (CGH), the copy number of DNA sequences from a subject is compared to those DNA from a control or reference by hybridizing both to DNA probes spaced throughout the human genome. Most commercially available CGH tests (which use arrays and thus are called array CGH) also test for common (not diseaserelated) SNPs to provide additional information regarding unusual conditions, such as uniparental disomy. As indicated by the name, an array CGH is a genomic test and is used to detect CNVs; depending on the specifics of the commercial platform used, it can detect a lower size limit of ≈100 000 nucleotides.19 Fluorescence in situ hybridization (FISH) is a targeted test in which a probe for a specific region of the genome is hybridized against metaphase chromosomes from the patient to detect for CNVs at a specific genetic locus. At many institutions, FISH and karyotypes are falling out of common usage, being largely supplanted by array CGH or SNP genotyping arrays (collectively referred to as chromosome microarrays or CMAs).20
Small Genetic Variation
The detection of SNPs and INDELs for clinical genetic testing now almost universally uses NGS technologies, also known as sequencing by synthesis or short-read sequencing. Gene panel tests are targeted tests and rely on either hybridization or polymerase chain reaction to capture the regions of genes (typically 1 to 100 genes) that encode for protein sequences. Whole exome sequencing (WES) is a genomic test that captures (by hybridization) the protein coding regions of all 18 000 human genes (≈1.5% of the entire genome), followed by NGS. Whole genome sequencing is a genomic test that obtains genetic information from the entire human genome without a complex capture process followed by NGS, although functionally the analysis of the data obtained is usually limited to the protein-coding regions of the genome.21 After generation of the sequencing information by NGS, gene panel tests, exome sequencing, and genome sequencing all require a subsequent bioinformatic analysis to detect and classify SNPs and INDELs in genes relevant to the disease under consideration.22,23 Most gene panel tests now offer concurrent detection of deletion or duplication (arising from a CNV) of the small number of genes on the panel test,24 and this is an emerging offering from some providers of clinical exome-sequencing services.
Practical Considerations
In contemporary practice, genetic counselors and other qualified clinicians are essential for the appropriate and ethical application of any genetic test in the clinical setting. Genetic counselors with extensive disease- and gene-specific domain knowledge are often the primary interpreters of genetic information detected on panel, exome, and genome tests in subspecialty clinics that do not include a medical geneticist.25,26 Just as with all other medical tests, each technique in modern genetic testing can display false-positive and false-negative results for specific types of genetic variation, which can often be linked to the fundamental technical aspects of the sequencing chemistries and bioinformatics used in processing a specific test.27,28 In addition, the genetic testing will not always yield a “yes” or “no” result; variants of unknown significance are commonly identified, and the communication of results to the family is best accomplished by genetic counselors, geneticists, and qualified clinicians with expertise in congenital HD.
Emerging Technologies
There are a number of additional technologies that have entered or will shortly enter clinical use, of which 2 will be discussed here. The sequencing of fetal cell-free DNA (fcfDNA) is commonly used in the prenatal setting as a screening tool for aneuploidies. Whole blood from a pregnant woman contains DNA from the fetal trophoblastic cells that can be separated by centrifugation. Once the fcfDNA is separated, the ratio of genetic information can be sampled and compared between different chromosomes to detect aneuploidies,29 and in the future, clinical testing could also be expanded to include detection of specifi subchromosomal deletions or duplications such as the 22q11.2 deletion. However, current implementations of fcfDNA technology display measurably lower sensitivity and specificity for aneuploidy relative to gold standard tests such as FISH testing of amniotic fluid.30
Additional advances in sequencing technology that effectively increase the length of sampling for DNA (current NGS sample size is ≈100–250 nucleotides; long-read sequencing is often >10 000 nucleotides) are more robust for detecting structural variation. Once perfected and when cost-effective, long-read sequencing will allow for the robust detection of SNPs/INDELs and CNVs simultaneously with a single clinical test.31
CHROMOSOMAL ANEUPLOIDIES AND CNVs ASSOCIATED WITH CONGENITAL HD
Aneuploidies
Aneuploidy is an abnormal number of chromosomes, and aneuploidies that most commonly survive to term include trisomy 21, 18, and 13 and sex chromosome aneuploidies such as Turner syndrome (Appendix). There is an increased risk of many aneuploidies with increasing maternal age. Increasingly, aneuploidies are detected prenatally with noninvasive prenatal diagnostic screening, and in this section, aneuploidies commonly associated with congenital HD such as Down syndrome and Turner syndrome are presented. Information on other aneuploidies is present in the Appendix. Less common aneuploidies such as trisomy 8 and 9 survive to term only when they are mosaic. Fetal echocardiograms allow for early and accurate diagnosis of the cardiac anatomy when aneuploidies are detected.
Down Syndrome
Down syndrome is the most common aneuploidy and is usually caused by trisomy 21. It is also the most common chromosome abnormality associated with congenital HD.32
Common Features
The common features of Down syndrome include characteristic facial features; short stature; hypotonia; intellectual disability ranging from mild to moderate; behavioral issues including problems with attention, obsessive/compulsive behavior, and tantrums; and a range of congenital anomalies, including ≈40% to 50% with congenital HD. Individuals with Down syndrome often experience a gradual decline in cognition and have an increased risk of Alzheimer disease. Health supervision guidelines are available and treatment is based on specific clinical manifestations.33
Cardiac Features
Congenital HD is frequently diagnosed in infants and children with Down syndrome (40%–50%). The most common congenital HDs include atrioventricular septal defect (AVSD), ventricular septal defect (VSD), atrial septal defect (ASD), patent ductus arteriosus (PDA), and tetralogy of Fallot.34 Congenital HD and cardiac complications are common causes of mortality in patients with Down syndrome, contributing to 13% of deaths in childhood and 23% of deaths in adulthood.35 Individuals with Down syndrome have increased risk of pulmonary hypertension, as well as congenital respiratory tract anomalies, pulmonary abnormalities, and hypotonia, each of which can lead to worse outcomes after surgery.36 One subset of patients with Down syndrome that has a higher surgical risk is those undergoing single-ventricle palliation. Among those patients undergoing staged single-ventricle palliation, individuals with Down syndrome had higher in-hospital mortality rates.37
Prevalence
Down syndrome occurs in ≈1 in 800 newborns. Approximately 5300 babies with Down syndrome are born in the United States each year, and ≈200 000 people in the United States have Down syndrome. The risk of having a child with Down syndrome increases with advanced maternal age.
Molecular Genetics
Most individuals with Down syndrome have trisomy 21, but rarely, Down syndrome results from a translocation of chromosome 21 with another chromosome (commonly 21, 14, or 13) or mosaicism in a subset of cells.
Cardiovascular Genotype/Phenotype Correlations
The vast majority of individuals with Down syndrome have trisomy 21, so there is little genotype/phenotype correlation. However, in general for individuals with mosaicism, the lower the level of mosaicism for trisomy 21, the less severe the cognitive deficits are.
Turner Syndrome
Turner syndrome is another common chromosomal condition, caused by loss of part or all of an X chromosome in females.
Common Features
The most common features of Turner syndrome include short stature, early loss of ovarian function manifesting as delayed puberty and delayed menarche (and in adult women, anovulation and infertility), lymphedema, webbed neck, low posterior hairline, cubitus valgus, congenital HD, skeletal anomalies, renal anomalies, and developmental delays, nonverbal learning disabilities, and behavioral problems in some girls.
Treatment with growth hormone is often beneficial, ideally beginning in early childhood, and can increase final adult height by 8 to 10 cm. Estrogen replacement therapy is usually started at the time of normal puberty, around 12 years of age, to initiate normal timing of breast development and to help prevent osteoporosis. Estrogen and progesterone are given to support menstruation.
Cardiac Features
Cardiac structural anomalies usually involve the left side of the heart and most commonly include BAV and coarctation of the aorta and less commonly partial anomalous pulmonary venous return and hypoplastic left heart syndrome (HLHS). All patients with Turner syndrome should have a baseline echocardiogram and cardiac evaluation and follow-up as necessary based on the baseline evaluation. Aortic root dilatation is present in 3% to 8% and can lead to dissecting aneurysms and rupture. BAV, coarctation of the aorta, and systemic hypertension are associated with aortic dilatation and dissection.38–40 Serial aortic arch imaging by echocardiogram or magnetic resonance imaging for adolescents should be performed every 5 years if there is no history of aortic dilation, BAV, or hypertension, and more frequent screening can be beneficial for individuals with risk factors for aortic dissection.41 Up to 40% of girls with Turner syndrome have hypertension, which should be treated aggressively.38 A cardiovascular and renal evaluation should be completed when hypertension is identified.
Prevalence
Turner syndrome occurs in ≈1 in 2000 to 1 in 2500 live female births.42
Molecular Genetics
The exact genetic abnormality found on karyotype analysis varies and can include classic 45,X but also individuals who are mosaic 45,X with another cell line, including 46,XX, 47,XXX, or 46,XY, as well as individuals with structural abnormalities of the X chromosome, including deletions and translocations of the X chromosome. Array CGH is useful to define precisely the extent of the deletions or translocation. For mosaic individuals, the phenotype is generally less severe as the percentage of 45,X cells decreases. It is important to determine whether there are any cells with a Y chromosome using an SRY polymerase chain reaction test, because this can be associated with gonadal dysgenesis that might require surgical removal of gonadal tissue to prevent the increased risk of cancer.
Cardiovascular Genotype/Phenotype Correlations
The prevalence of cardiovascular abnormalities in individuals with Turner syndrome varies between 20% and 40% and is higher with monosomy X relative to those with structural abnormalities of the X chromosome and in girls with a more pronounced clinical phenotype.38,39,43,44
COPY NUMBER VARIANTS
Review of Types of CNVs
CNVs range widely in size from single genes to large segmental deletions or duplications of millions of base pairs. In general, deletions are more deleterious than duplications because of the sensitivity in gene dosage for many genes that do not tolerate haploinsufficiency. CNVs that encompass multiple genes can have a wide range of phenotypic effects because of the additive impact of individual genes on individual phenotypes or the pleiotropic effects of single genes on multiple phenotypes. Identification of the relevant gene for congenital HD within a CNV interval requires mapping of multiple patients with overlapping CNVs to identify a critical interval and ultimately a single gene within the critical interval that is associated consistently with congenital HD. Additional supportive evidence for the congenital HD gene is provided by examples of patients with point mutations within that single gene within the critical region who have congenital HD.
Association of Pathogenic CNVs as a Class With Clinical Outcome
On average as a group, children with pathogenic CNVs associated with congenital HD have poorer outcomes than children without pathogenic CNVs. At least part of the explanation for the worse outcome could be an association with extracardiac manifestations that impact medical care. In one series of 58 patients with congenital HD and other dysmorphic features or other anomalies, 20.7% of the patients had potentially pathogenic CNVs that ranged in size from 240 kb to 9.6 Mb.45 In another series of 422 children with non-syndromic, isolated congenital HD followed up prospectively from before their first surgery, there was an increased frequency of potentially pathogenic CNVs in 12.1% of congenital HD subjects compared with 5% of control subjects, and in this series, the presence of a CNV was associated with significantly decreased transplant-free survival after surgery, with an adjusted 2.6-fold increased risk of death or transplantation.46 Beyond survival, putatively pathogenic CNVs that were more frequent in congenital HD patients with single-ventricle physiology (13.9% of 223 affected individuals compared with 4.4% of control subjects) were associated with worse linear growth and worse neurocognitive outcomes.47 There is undoubtedly heterogeneity in outcomes across CNVs, and future studies will require refined analyses specific to the individual CNV to determine which ones are associated with differential prognosis when controlling for the cardiac anatomy, as well as studying the other associated anomalies, ventricular function, and arrhythmias that could account for differential outcomes.
Many new CNVs associated with congenital HD have been identified over the past 10 years and now have been observed in sufficient numbers of patients to define the clinical features associated with them.48 Most of the CNVs are flanked by repeat sequences that lead to nonallelic homologous recombination and recurrent de novo deletions or duplications of the same interval, although a minority of patients have smaller or larger CNVs associated with less or more severe phenotypes, respectively. There are several common principles that apply across the CNVs. Each of the CNVs includes contiguous gene deletions or duplications, and generally deletions are associated with greater severity of neurocognitive phenotype. Because each of the CNVs includes multiple genes, it is not always clear whether the overall phenotype is caused by the effects of multiple genes on multiple aspects of the phenotype or whether certain single genes within the interval have pleiotropic effects on multiple aspects of the phenotype. For each of the CNVs discussed below, the associated congenital HD is incompletely penetrant. It is usually unclear what the other determinants of congenital HD are, but it is likely that they are interacting with genetic factors either on the opposite allele or genetic variants in cis on the same chromosome or in trans on other chromosomes, as well as nongenetic factors. Most CNVs are associated with effects on behavior and cognition, and many are associated with growth effects that are independent of the congenital HD and are important to appreciate when assessing clinical outcomes.
DESCRIPTIONS OF SPECIFIC CNVs ASSOCIATED WITH CONGENITAL HD
In this section, several CNVs are highlighted. The Appendix provides information on other less frequent CNVs.
22q11.2 Deletion Syndrome
The 22q11.2 deletion syndrome (22q11.2DS) is the most common microdeletion syndrome, with a prevalence estimated at 1 per 5950 live births.49 The clinical features of the 22q11.2DS are those described for the DiGeorge and velocardiofacial syndromes and the Takao conotruncal anomaly face syndrome, although the phenotype can vary, even within a family.50 Although highly overlapping, the 22q11.2DS and DiGeorge and velocardiofacial syndromes are not synonymous, because nearly 10% of patients with DiGeorge and velocardiofacial syndromes do not have a 22q11.2 deletion, and not all patients with 22q11.2 deletion will demonstrate classic features of DiGeorge and velocardiofacial syndromes.
Common Features
Frequent clinical features include dysmorphic facies, congenital HD (especially conotruncal malformations and aortic arch anomalies), palatal malformations, learning difficulties, and immunodeficiency. Facial features are characteristic but can be relatively subtle, especially in infants. Facial dysmorphisms include myopathic facies, tubular nose with bulbous nasal tip, hypoplastic alae nasi, and low-set or dysplastic ears. Additional findings include hypocalcemia, significant feeding and swallowing problems (including regurgitation through the nose), constipation, renal anomalies, hearing loss, laryngotracheoesophageal anomalies, growth hormone deficiency, autoimmune disorders, seizures, central nervous system anomalies, skeletal abnormalities, ophthalmologic abnormalities, enamel hypoplasia, and malignancies (rare). Behavioral and learning disabilities become more evident in school-aged children, whereas psychiatric disorders often become manifest in adolescence and adulthood (Table 2). Delays in emergence of language, intellectual disability, and learning differences (nonverbal learning disability with verbal IQ significantly greater than the performance IQ) are common. Autism or autism spectrum disorder is found in ≈20% of children, and psychiatric illness (schizophrenia) is present in 25% of adults. Attention deficit disorder, anxiety, perseveration, and difficulty with social interactions are also common.51
Table 2.
Common Clinical Features of 22q11.2DS and Most Common Age at Presentation
| Clinical Feature | Infancy | Toddler/School Age | Adolescent/Adult |
|---|---|---|---|
| Congenital HD (conotruncal defects and interrupted aortic arch) | X | X | |
| Characteristic facial features | X | X | |
| Palatal abnormalities (velopharyngeal insufficiency, hypernasal speech) | X | X | |
| Feeding problems/nasal regurgitation of feeds | X | ||
| Hypocalcemia | X | ||
| Immune deficiency/thymus anomalies | X | X | |
| Learning difficulties (nonverbal learning disability) | X | ||
| Psychiatric disease (autism, schizophrenia in adults) | X |
22q11.2DS indicates 22q11.2 deletion syndrome; and HD, heart disease.
Cardiovascular Features
Conotruncal malformations account for 70% of the heart defects associated with a 22q11.2 deletion.52 The most common cardiovascular defects include tetralogy of Fallot (20%), truncus arteriosus (6%), conoventricular VSD (14%), type B interruption of the aortic arch (IAA), and other aortic arch anomalies (13%).53–56 ASDs, pulmonary valve stenosis (PVS), HLHS, double-outlet right ventricle, transposition of the great arteries (TGA), vascular rings, and heterotaxy syndrome are less common but have also been reported.
Prevalence
The estimated prevalence of the 22q11.2 deletion among various cardiovascular malformations is 1.9%.52
Molecular Genetics
The majority of 22q11.2 deletions are de novo, but they are inherited from a parent in an autosomal dominant fashion in 6% to 28% of cases.50 It is not unusual in familial cases for one of the parents to be diagnosed with the 22q11.2 deletion only after their child is diagnosed.50,57
It is important to identify the cardiac patient with a 22q11.2 deletion by CMA to offer accurate genetic counseling and familial screening and to allow for identification of associated noncardiac features that require specific management. For example, there is a higher operative mortality in some patients with 22q11.2 deletion.58,59 It is important for clinicians to be aware of a 22q11.2 deletion to plan surgery and postoperative care, particularly with respect to immunologic issues and calcium metabolism. Affected individuals should receive leukocyte-depleted and cytomegalovirus-negative blood products to prevent serious graft-versus-host disease or overwhelming infection.
Given the frequency of 22q11.2 deletions in the congenital HD population, it is reasonable to test all individuals with IAA type B, truncus arteriosus, tetralogy of Fallot, VSD (malalignment, conoseptal hypoplasia, or perimembranous) with aortic arch anomaly, or isolated aortic arch anomaly (Table 3). Clinical assessment for syndromic features alone might not consistently identify the infant carrying a 22q11 deletion, because facial features can evolve with time. Therefore, routine screening of individuals with selected types of congenital HD using CMA is warranted either prenatally or postnatally.
Table 3.
Suggested Patients With Congenital HD to Test for a 22q11.2 Deletion
| All fetuses with interrupted aortic arch, truncus arteriosus, tetralogy of Fallot, VSD,* or aortic arch anomaly (if amniocentesis performed for diagnostic purposes) |
| All newborns/infants/children/adolescents/adults with: |
| Interruption of aortic arch |
| Truncus arteriosus |
| Tetralogy of Fallot |
| VSD* with aortic arch anomaly |
| Isolated aortic arch anomaly |
| Congenital HD and additional feature of 22q11.2DS |
22q11.2DS indicates 22q11.2 deletion syndrome; HD, heart disease; and VSD, ventricular septal defect.
Malalignment, conoseptal hypoplasia, perimembranous.
Cardiovascular Genotype/Phenotype Correlations
The estimated 22q11.2 deletion frequency is particularly high for IAA (22%–48%),42,60 truncus arteriosus (12%–35%), tetralogy of Fallot (8%–13%), and isolated aortic arch anomalies (24%).42,60,61 In patients with VSDs, the deletion frequency is low overall42 (2%) but higher when associated with aortic arch anomaly (right aortic arch, cervical location or abnormal branching pattern, and discontinuous branch pulmonary arteries).60 For IAA, 22q11.2 deletions are specifi associated with type B (accounting for more than half of the cases of type B interruption) and not commonly associated with type A. Among those with tetralogy of Fallot, the strongest association with 22q11.2 deletions is for those with pulmonary atresia.60 A 22q11.2 deletion is infrequent in children with double-outlet right ventricle (2%)42 and those with TGA. Aortic root dilation has been described with 22q11.2 deletions either in association with a conotruncal defect or other cardiac defect or as an isolated finding 62,63 Tetralogy of Fallot with aortic arch abnormalities is the most frequent congenital HD with aortic dilation in 22q11.2DS.62
Phenotypic Variability and Related Conditions
22q11.2DS is a contiguous gene deletion syndrome, and >40 genes are deleted in the most common deletion. Deletion of several genes within this region contributes to the cardiac and noncardiac features. The size of the deletion can be precisely determined by CMA. The vast majority (97%) of affected individuals will have either a common recurrent ≈3-Mb deletion or a smaller, less common ≈1.5-Mb nested deletion. Smaller or larger deletions can contribute to atypical clinical phenotypes. Mutations outside the interval or on the nondeleted 22q11.2 allele are also known to modify the phenotype. An example of this is Bernard-Soulier syndrome, an autosomal recessive trait, which includes giant platelets, thrombocytopenia, and a prolonged bleeding time. One cause of Bernard-Soulier syndrome is biallelic loss-of-function mutations in the gene encoding the β-subunit of the platelet glycoprotein GPIb (GPIBB), which resides in the 22q11.2 critical region. Several cases of Bernard-Soulier syndrome have been reported in which a 22q11.2del was combined with a loss-of-function GP1BB mutation on the nondeleted allele. Although rare, the occurrence of these 2 conditions together can potentially place the 22q11.2 individual at risk for life-threatening bleeding in conjunction with surgeries and procedures.64
Duplication of the same 22q11.2 CNV region causes an extremely variable disorder with a phenotype that ranges from normal to learning disability and, infrequently, congenital defects including heart defects. Generally, the duplication is associated with milder and more variable manifestations than the deletion. The duplication can be either de novo or inherited from a phenotypically normal parent.65 Congenital HD occurs in 15% with similar defects as 22q11.2DS.66 The associated features are largely neurobehavioral and range from apparently normal to intellectual disability/learning disability, delayed development, or hypotonia. Many of the reported series likely suffer from ascertainment bias compared with phenotypes in unselected population-based cohorts.65,67
A small number of individuals have distal deletions of 1.4 to 2.1 Mb of 22q11.2 that do not overlap with the DiGeorge proximal 22q11.2 deletion. Patients with the distal deletion share some overlapping neurobehavioral features, including speech delay and learning disabilities, with proximal 22q11.2DS, but this represents a distinct genomic disorder.68 Other clinical features include prematurity, problems with growth, cleft palate, skeletal anomalies, and congenital HD including truncus arteriosus and BAV.68 CRKL and MAPK1 are the genes in this region that might play a role in cardiac development.69
A recent study compared rare CNVs outside the common 22q11.2 deletion region in 607 22q11.2DS subjects with congenital HD compared with 339 22q11.2DS subjects with normal cardiac anatomy. Although there was no significant difference in the overall burden of rare CNVs, an overabundance of CNVs affecting cardiac-related genes was detected in 22q11.2DS individuals with congenital HDs, which suggests that CNVs outside the 22q11.2 region might contain genes that modify risk for congenital HDs in some 22q11.2DS patients.70 Finally, another recent study has shown that the phenotypic variability observed in a subset of individuals with 22q11.2DS is attributable to other mutations on the nondeleted chromosome.71
Williams-Beuren Syndrome
Williams-Beuren syndrome or Williams syndrome (WS) is a contiguous gene deletion syndrome caused by deletion at 7q11.23.
Common Features
Clinical manifestations (Table 4) include dysmorphic features, characteristic cardiovascular defects (vascular stenoses, elastin arteriopathy), a specifi cognitive profile, unique personality characteristics (“social personality”), growth abnormalities, connective tissue and skeletal abnormalities, and endocrine abnormalities (infantile hypercalcemia, hypercalciuria, hypothyroidism, and early puberty). Feeding difficulties during infancy often lead to poor weight gain. Adults have short stature (less than third percentile) and tend to be overweight or obese and to have complications of systemic hypertension, diabetes mellitus, and diverticulosis.72
Table 4.
Clinical Features of Williams Syndrome
| Cardiovascular |
|---|
| Elastin arteriopathy: any artery may be narrowed; can be multiple |
| Supravalvular aortic stenosis: most common (75%) and most clinically significant |
| Pulmonary arterial stenosis: common in infancy |
| Aortic/mitral valve defects |
| Systemic hypertension |
| Distinctive facies |
| Stellate iris pattern |
| Broad forehead, bitemporal narrowing |
| Periorbital fullness |
| Malar flattening |
| Short nose, broad nasal tip, long philtrum |
| Full lips/wide mouth/small, widely spaced teeth |
| Craniofacial |
| Recurrent otitis media |
| Malocclusion |
| Ophthalmologic |
| Strabismus |
| Hyperopia |
| Neurological |
| Cognitive disability: strength in language; extreme weakness in visuospatial |
| Unique personality: overfriendliness, empathy, generalized anxiety, specific phobias |
| Hyperacusis |
| Connective tissue abnormalities |
| Hoarse voice |
| Inguinal/umbilical hernia |
| Bowel/bladder diverticulae |
| Rectal prolapse |
| Joint limitation or laxity/soft, lax skin |
| Growth abnormalities |
| Prenatal growth deficiency |
| Infantile failure to thrive |
| Constipation |
| Adult height less than third percentile |
| Overweight/obese |
| Endocrine |
| Hypercalcemia/hypercalciuria |
| Hypothyroidism |
| Adult diabetes mellitus |
| Renal/bladder disorders |
| Structural anomalies |
| Nephrocalcinosis |
| Chronic urinary tract infections |
Cardiovascular Features
Frequent cardiovascular anomalies include supravalvular aortic stenosis (SVAS), often in combination with supravalvular pulmonary artery stenosis and branch pulmonary artery stenosis. The SVAS can progress during childhood and is the most common abnormality requiring surgical intervention. In contrast, the branch pulmonary artery stenosis often regresses with time.73,74 These arterial abnormalities constitute an elastin arteriopathy or vasculopathy caused by deletion of the ELN gene. Any artery can be narrowed, including the ascending aorta, aortic arch, and descending thoracic and abdominal aorta, as well as central and peripheral arteries including the coronary arteries, carotid and cerebral arteries, mesenteric arteries, renal arteries, and pulmonary arteries. Affected arteries typically have thickened walls and narrowed lumens. There is an increased risk of anesthesia-related complications and sudden cardiac death. Risk factors include myocardial ischemia attributable to coronary stenosis or severe biventricular outflow tract obstruction, but the causative mechanisms have not been fully delineated.75–79
Prevalence
WS occurs in 1 per 7500 to 20 000 births.
Molecular Genetics
The vast majority of affected individuals with a clinical diagnosis of WS have been found by FISH or deletion/duplication testing to have a microdeletion at chromosome 7q11.23, typically a recurrent 1.5- to 1.8-Mb deletion of the Williams-Beuren syndrome critical region that encompasses ELN, the gene encoding elastin.80 Most cases arise de novo, although parent-to-child transmission with an autosomal dominant pattern of inheritance has been reported. As with other contiguous gene deletion syndromes, WS has a broad range of phenotypic variability. The size of the deletion can be precisely determined by CMA. Although there is wide phenotypic variability even among individuals with the typical deletion, smaller or larger deletions might contribute to atypical clinical phenotypes.
Given the clinical variability of WS and the fact that the physical and developmental signs can be relatively subtle during infancy, it is not unusual for the diagnosis to be confirmed only after identification of a characteristic cardiovascular defect such as SVAS. The severity of SVAS and other vascular defects tends to be greater in males, and infants and children with more severe vascular involvement tend to be diagnosed with WS at younger ages than those with trivial or no cardiovascular involvement.81,82
Because SVAS is very common in WS and uncommon in the general population, it is appropriate to consider testing all patients with SVAS at the time of diagnosis of the cardiovascular defect. Furthermore, if peripheral pulmonary artery stenosis persists beyond infancy, it is also appropriate to consider testing for WS. Similarly, if any of the defects associated with the elastin arteriopathy, including coronary artery ostial stenosis, renal artery stenosis, and middle aortic syndrome (abdominal coarctation), are diagnosed at any age, testing for WS should be considered.
Cardiovascular Genotype/Phenotype Correlations
Point mutations or small intragenic deletions of ELN have been found in the autosomal dominant disorder familial SVAS without other characteristics of WS. The vascular disease in the nonsyndromic familial SVAS is indistinguishable from that seen in WS. Of note, CNVs in the 7q11.23 region have been found to be associated with autism in a study of >4000 individuals who did not have WS,83 and dilation of the ascending aorta occurs in almost half of individuals with 7q11.23 duplication syndrome.84,85
General Clinical Recommendations
Early diagnosis of WS is important to optimize management of other potential medical problems (Table 4).86 Renal anomalies are common, and a renal ultrasound is recommended at baseline and as needed.87 Endocrine abnormalities include idiopathic hypercalcemia, hypercalciuria, hypothyroidism, subclinical hypothyroidism, and early puberty.72 Hypercalcemia and hypercalciuria can be treated with appropriate diet and medication. Hypercalcemia occurs most commonly in the first year of life, whereas hypercalciuria can persist and occur at any age. Hypercalcemia can lead to nephrocalcinosis and renal failure. Obesity, abnormal oral glucose tolerance tests, and diabetes mellitus are common, especially in adults.72 Systemic hypertension is also common and often presents during childhood or adolescence.88 About half of adults with WS will have high blood pressure. Intellectual disability is common and usually mild, but with a specific cognitive profile with strengths in verbal short-term memory and language and extreme weakness in visuospatial constructive cognition.89 An early diagnosis of WS allows for enhancement of learning and development in children with WS. Attention deficit disorder and anxiety are common. Whereas deletion of ELN accounts for the cardiovascular and connective tissue abnormalities in WS, deletion of additional genes in the Williams-Beuren syndrome critical region (LIMK1, GTF2I, STX1A, BAZ1B, CLIP2, GTF2IRD1, NCF1) has been implicated in other manifestations of WS.72
Jacobsen Syndrome (11q Terminal Deletion Disorder)
Since Jacobsen’s initial report in 1973,90 >200 patients with Jacobsen syndrome (JS) have been reported. JS is a clinically recognizable contiguous gene deletion syndrome involving deletions from subband 11q23 to the telomere, ranging in size from 7 to 16 Mb.
Common Features
Clinical manifestations include dysmorphic features, growth retardation sometimes associated with IGF-1 (insulin-like growth factor 1) deficiency, cognitive and behavioral dysfunction, congenital HD, thrombocytopenia and platelet dysfunction (Paris-Trousseau syndrome), recurrent infections, immune deficiency, and ophthalmologic, gastrointestinal, and genitourinary problems.91,92
A prospective study of 110 patients with the 11q terminal deletion disorder, diagnosed by karyotype rather than CMA, provided detailed delineation of the clinical manifestations, as well as a comprehensive set of recommendations for the clinical management of patients with this disorder. Molecular analysis of the deletion breakpoints in 65 patients defined genetic “critical regions” for 14 clinical phenotypes, as well as for the neuropsychiatric profiles 91 Subsequent studies have implicated causative genes for a number of these clinical phenotypes, including heart defects (see Molecular Genetics).92
Cardiovascular Features
More than half of affected individuals have congenital HD, most of whom require surgical intervention. About one-third of patients with heart defects have a membranous VSD, and another third have left ventricular outflow tract defects with various degrees of hypoplasia or obstruction of the mitral valve, left ventricle, aortic valve, or aorta. This spectrum includes mitral stenosis, BAV, aortic valve stenosis, coarctation of the aorta, Shone complex, and HLHS. HLHS is highly overrepresented in patients with JS (5%–10%), an estimated frequency that is 1000 to 2000 times that of the general population. The other one-third of children with congenital HD have a variety of heart defects including double-outlet right ventricle, TGA, AVSD, secundum ASD, dextrocardia, aberrant right subclavian artery, PDA, persistent left superior vena cava, tricuspid atresia, type B IAA, truncus arteriosus, and PVS.
Prevalence
The prevalence of JS is estimated to be 1 in 50000 to 1 in 100 000 live births.
Molecular Genetics
Diagnosis of JS is currently accomplished by CMA. Through a combination of human genetic techniques and using genetically engineered animal models, ETS1 has been identified as the causal gene for congenital HD in JS.92 Homozygous deletion of Ets1 caused VSDs and abnormal ventricular morphology with nearly 100% penetrance in mice in a C57/B6 background but not in an FVBN-1 background.93 The fact that homozygous Ets1 knockout mice do not have heart defects in at least 1 strain strongly implies the presence of a genetic modifier. Most recently, a patient with a complex congenital HD including mitral atresia and hypoplastic left ventricle was found to carry a de novo frameshift mutation in ETS1, likely a loss-of-function mutation, providing further confirmation that loss of ETS1 is the cause of congenital HD in JS.94
Cardiovascular Genotype/Phenotype Correlations
There is no correlation between the size of the deletion and whether or not there is congenital HD or what the specific congenital HD is. Using FISH, Grossfeld and colleagues91 found that the smallest terminal deletion associated with a congenital HD (HLHS) was ≈7 Mb (cardiac critical region).
Thombocytopenia and Platelet Dysfunction
Nearly all patients with JS have Paris-Trousseau syndrome, characterized by thrombocytopenia and platelet dysfunction, and heterozygous loss of the FLI1 gene has been identified as the cause.92 The thrombocytopenia presents in the neonatal period. Platelet dysfunction persists in older individuals, despite normal platelet counts. Risk for bleeding is one of the most common causes of mortality in JS and likely places these patients at increased risk for the development of brain hemorrhages.91,92,95 Platelet transfusion or desmopressin may be necessary for bleeding and high-risk procedures.
Cognitive Function and Behavior
Cognitive function ranges from normal intelligence to moderate cognitive disability. Nearly half of the patients have mild cognitive disability, with a characteristic neuropsychiatric profile demonstrating near-normal receptive language ability but mild to moderate impairment in expressive language, with full-scale IQs typically in the 60s to 70s.91 The severity of intellectual disability correlates with the size of the deletion; those with the largest deletions (>12 Mb) have the most severe intellectual disability (IQ <50).96 Approximately one-half of all JS patients fulfill the diagnostic criteria for autism, and candidate genes for autism (RICS) and intellectual disability (BSX-1) have been identified.96,97
General Clinical Recommendations
Individuals with suspected or confirmed JS should have a thorough genetics evaluation. The extent of the deletion can be precisely delineated by CMA in the proband. Most deletions are de novo, with only 8% resulting from a parental translocation, or in rare cases from a relatively mildly affected parent carrying an 11q deletion.91 Parents should be screened for a translocation or deletion. Patients with JS require coordinated multisystem care. A cardiac evaluation including an echocardiogram is recommended at baseline and as needed. Careful monitoring of the platelet count is necessary in infancy and early childhood, and once the platelet count normalizes, platelet function studies should be evaluated periodically. Neurocognitive and behavioral difficulties are common. Baseline and ongoing evaluations by a neuropsychologist and behavioral specialist are recommended, as well as brain imaging at baseline and as needed. Patients should be screened for ophthalmologic issues including exotropia, amblyopia, refractive errors, ptosis, and retinal artery tortuosity. Common gastrointestinal issues include failure to thrive, constipation, and pyloric stenosis. Genitourinary anomalies include cryptorchidism and renal anomalies. A baseline renal ultrasound is recommended.
1p36 Deletion
The 1p36 deletion syndrome is the second most common deletion syndrome.
Common Features
Clinical features include dysmorphic facies, intellectual disability ranging from mild to severe, hypotonia, seizures, structural brain abnormalities, congenital heart defects, ophthalmologic and vision issues, hearing loss, skeletal abnormalities, and genitourinary anomalies.98
Among individuals with the 1p36 deletion, there is a range of neurocognitive disability, but ≈90% of individuals have severe to profound intellectual disability, and 75% are nonverbal. Behavioral disorders include autism, tantrums, self-mutilation, stereotypies, and hyperphagia. Structural brain abnormalities include dilation of the lateral ventricles, cortical atrophy, and hypoplasia or agenesis of the corpus callosum. Seizures are present in approximately half of the individuals with the 1p36 deletion.
Cardiac Features
Structural heart defects include ASD, VSD, valvular abnormalities, PDA, tetralogy of Fallot, coarctation of the aorta, infundibular stenosis of the right ventricle, and Ebstein’s anomaly.99,100 In addition, 27% of individuals with the 1p36 deletion have cardiomyopathy, 23% with left ventricular noncompaction and 4% with dilated cardiomyopathy.99
Prevalence
The prevalence of 1q36 deletion is 1 in 5000 to 10000 births, with a 2:1 female-to-male ratio.99–101
Molecular Genetics
This condition is identified by CMA testing. The deletion varies in size and can extend to >5 Mb.
1q21.1 Deletion
Common Features
Recurrent 1.35-Mb deletions of 1q21.1 are typically associated with microcephaly, mild intellectual disability, mildly dysmorphic features, short stature, eye abnormalities (strabismus, chorioretinal and iris colobomas, microphthalmia, hypermetropia, Duane anomaly, and cataracts), and sensorineural hearing loss.102,103 Less commonly, there are other associated findings, including congenital HD, genitourinary alterations, skeletal malformations (craniosynostosis, scoliosis), and seizures. The associated psychiatric and behavioral anomalies include autistic spectrum disorder, attention deficit hyperactivity disorder, mood disorder, and sleep disturbances.104 Neurocognitive issues are generally global, with generalized learning disabilities and challenges with gross motor development and coordination.
Cardiac Features
The types of congenital HD include PDA, truncus arteriosus, VSD, ASD, tetralogy of Fallot, BAV, dilation of the ascending aorta, aortic insufficiency, coarctation of the aorta, IAA, anomalous origin of the right coronary artery, PVS, and TGA.105
Prevalence
The prevalence of the 1q21.1 microdeletion is ≈0.2% of individuals with developmental delays, intellectual disabilities, or congenital abnormalities.106
Molecular Genetics
The condition is identified by CMA. The gene responsible for congenital HD within the interval is possibly GJA5, which encodes for a cardiac gap junction protein connexin 40.107
1q21.1 Duplication
The reciprocal duplication of 1q21.1 is also associated with congenital HD, more commonly tetralogy of Fallot but also including VSD, TGA, and PVS.106,108,109 Again, the gene responsible for congenital HD within the interval is possibly GJA5.107 Other congenital malformations associated with the CNV include hypospadias, clubbed feet, hemivertebrae, and hip dysplasia. There is a tendency toward larger head size. Some individuals have neurobehavioral manifestations, including intellectual disabilities, developmental delay, expressive language delay, learning disabilities, features of autism, or attention deficit hyperactivity disorder, but others have no neurobehavioral problems.104,110
8p23.1 Deletion
Deletions of 8p23.1 are associated with congenital HD, congenital diaphragmatic hernia, growth impairment, microcephaly, behavioral problems including hyperactivity and impulsivity, mild to moderate intellectual disability, and developmental delays.111,112 Types of congenital HD typically associated include ASD, AVSD, and PVS. There are also several reported cases of more complex cardiac anatomy including hypoplastic right ventricle, double-outlet right ventricle, and double-inlet left ventricle. The gene most likely responsible for the congenital HD is GATA binding protein 4 (GATA4) encoding a zinc finger transcription factor.113
WELL-CHARACTERIZED SYNDROMES CAUSED BY SINGLE-GENE VARIATION
During the past 10 to 15 years, a period of active gene discovery, the molecular basis of many syndromes has been identified Numerous syndromes caused by single-gene variants (traditionally referred to as mutations) have additionally been found to be genetically heterogeneous, which means that an individual variant in >1 gene is capable of causing a similar condition (Table 5). Several selected syndromes are discussed in more detail with regard to their cardiac malformations, including Alagille, Holt-Oram, Char, Ellis-van Creveld, Adams-Oliver, Kabuki, and CHARGE syndromes. Table 5 can be consulted for details of multiple other genetic syndromes.
Table 5.
Genes and Loci Associated With Congenital HD
| Syndrome | Gene(s) | Loci | Cardiac Disease | % Congenital HD | Other Clinical Findings | References |
|---|---|---|---|---|---|---|
| Very commonly associated | ||||||
| Alagille | JAG 1 | 20p12.2 | PPS, TOF, PA | >90 | Bile duct paucity, posterior embryotoxon, butterfly vertebrae, renal defects | 114, 115 |
| NOTCH2 | 1p12-p11 | |||||
| CFC | BRAF | 7q34 | PVS, ASD, HCM | 75 | Curly hair, sparse eyebrows, feeding problems, developmental delay, intellectual disability | 116 |
| KRAS | 12p12.1 | |||||
| MAP2K1 | 15q22.31 | |||||
| MAP2K2 | 19p13.3 | |||||
| Cantu | ABCC9 | 12p12.1 | PDA, BAV, HCM, CoA, PE, AS | 75 | Hypertrichosis at birth, macrocephaly, narrow thorax, coarse facies, macroglossia, broad hands, advanced bone age | 117, 118 |
| Char | TFAP2B | 6p12.3 | PDA, VSD | 58 | Wide-set eyes, down-slanting palpebral fissures, thick lips, hand anomalies | 119, 120 |
| CHARGE | CHD7 | 8q12 | TOF, PDA, DORV, AVSD, VSD | 75–85 | Coloboma, choanal atresia, genital hypoplasia, ear anomalies, hearing loss, developmental delay, growth retardation, intellectual disability | 121 |
| Costello | HRAS | 11p15.5 | PVS, ASD, VSD, HCM, arrhythmias | 44–52 | Short stature, feeding problems, broad facies, bitemporal narrowing, redundant skin, intellectual disability | 122 |
| 22q11.2DS | TBX1 | 22q11.2 | Conotruncal defects, VSD, IAA, ASD, VR | 74–85 | Cleft palate, bifid uvula, velopharyngeal insufficiency, microcephaly, hypocalcemia, immune deficit, psychiatric disorder, learning disability | 54 |
| deletion | ||||||
| Ellis-van Creveld | EVC | 4p16.2 | Common atrium | 60 | Skeletal dysplasia, short limbs, polydactyly, short ribs, dysplastic nails, respiratory insufficiency | 123, 124 |
| EVC2 | 4p16.2 | |||||
| Holt-Oram | TBX5 | 12q24.1 | VSD, ASD, AVSD, conduction defects | 50 | Absent, hypoplastic, or triphalangeal thumbs; phocomelia; defects of radius; limb defects more prominent on left | 125 |
| Kabuki | KMT2D KDM6A | 12q13 Xp11.3 | CoA, BAV, VSD, TOF, TGA, HLHS | 50 | Growth deficiency, wide palpebral fissures, large protuberant ears, fetal finger pads, intellectual disability, clinodactyly | 126, 127 |
| Noonan | PTPN11 | 12q24.13 | Dysplastic PVS, ASD, TOF, AVSD, HCM, VSD, PDA | 75 | Short stature, hypertelorism, down-slanting palpebral fissures, ptosis, low posterior hairline, pectus deformity, bleeding disorder, chylothorax, cryptorchidism | 128 |
| SOS1 | 2p22.1 | |||||
| RAF1 | 3p25.2 | |||||
| KRAS | 12p12.1 | |||||
| NRAS | 1p13.2 | |||||
| RIT1 | 1q22 | |||||
| SHOC2 | 10q25.2 | |||||
| SOS2 | 14q21.3 | |||||
| BRAF | 7q34 | |||||
| VACTERL association | Unknown | VSD, ASD, HLHS, PDA, TGA, TOF, TA | 53–80 | Vertebral anomalies, anal atresia, tracheoesophageal fistula, renal anomalies, radial dysplasia, thumb hypoplasia, single umbilical artery | 129 | |
| Williams-Beuren | 7q11.23 | 7q11.23 | SVAS, PAS, VSD, ASD | 80 | Unusual facies, thick lips, strabismus, stellate iris pattern, intellectual disability | 130 |
| deletion (ELN) | ||||||
| Frequently associated | ||||||
| Carpenter | RAB23 | 6p11.2 | VSD, ASD, PDA, PS, TOF, TGA | 50 | Craniosynostosis, brachydactyly, syndactyly, polydactyly, obesity | 131 |
| Coffin-Siris | ARID1B | 6q25 | ASD, AVSD, VSD, MR, PDA, PS, DEX, AS | 20–44 | Developmental delay, coarse facies, | 132, 133 |
| SMARCB1 | 22q11 | hypoplastic distal phalanges, short stature, | ||||
| ARID1A | 1p36.1 | intellectual disability | ||||
| SMARCB1 | 22q11.23 | |||||
| SMARCA4 | 19p13.2 | |||||
| SMARCE1 | 17q21.2 | |||||
| Cornelia deLange | NIPBL | 5p13 | PVS, VSD, ASD, PDA | 33 | Microbrachycephaly, synophrys, arching eyebrows, growth retardation, intellectual disability, micromelia | 134 |
| SMC1L1 | Xp11.22 | |||||
| SMC3 | 10q25 | |||||
| Goldenhar | Unknown | VSD, PDA, TOF, CoA, conotruncal defects | 32 | Hemifacial microsomia, epibulbar dermoids, microtia, hemivertebrae | 135 | |
| Mowat-Wilson | ZEB2 | 2q22.3 | VSD, CoA, ASD, PDA, PAS | 54 | Short stature, microcephaly, Hirschsprung disease, intellectual disability, seizures | 136, 137 |
| Rubinstein-Taybi | CBP | 16p13.3 | PDA, VSD, ASD, HLHS, BAV | 33 | Microcephaly, growth retardation, down-slanting palpebral fissures, low-set malformed ears, prominent or beaked nose, intellectual disability, broad thumbs and toes | 138 |
| EP300 | 22q13.2 | |||||
| Smith-Lemli-Opitz | DHCR7 | 11q12–13 | AVSD, HLHS, ASD, PDA, VSD | 50 | Microcephaly, ptosis, genital anomalies, renal anomalies, broad nasal tip with anteverted nostrils, intellectual disability, syndactyly | 139 |
| Occasionally associated | ||||||
| Adams-Oliver | ARHGAP31 | 3q13 | ASD, VSD, CoA, HLHS, DORV | 20 | Aplasia cutis congenita, terminal transverse defects of hands, fingers, toes, feet | 140, 141 |
| DOCK6 | 19p13.2 | |||||
| RBPJ | 4p15.2 | |||||
| EOGT | 3p14.1 | |||||
| NOTCH1 | 9q34.3 | |||||
| DLL4 | 15q15.1 | |||||
| Baller-Gerold | RECQL4 | 8q24.3 | VSD, TOF, subaortic disease | 25 | Craniosynostosis, micrognathia, small mouth, radial aplasia/hypoplasia, imperforate anus, renal anomalies | 142 |
| Beckwith-Wiedemann | CDKNIC | 11p15.4 | VSD, HLHS, PS | 6.5 | Macrosomia, macroglossia, omphalocele, risk of malignancy | 143 |
| Coffin-Lowry | RSK2 | Xp22.2 | LVNC, MVP, AVA | 5–14 | Growth deficiency, coarse facies, everted lower lip, hypodontia, intellectual disability | 144 |
| Duane-radial ray (Okihiro) | SALL4 | 20q13.2 | ASD, PVS, VSD | <10 | Unilateral or bilateral Duane anomaly, hypoplasia of thumbs, hypoplastic radius and ulna, renal malformations, ear anomalies | 145 |
| Fragile X | FMR1 | Xq27.3 | MVP, aortic dilation | <10 | Macrocephaly, intellectual disability, hand flapping, speech abnormality, autism spectrum disorder, macroorchidism, seizures, prominent forehead, large ears | 146 |
| Nance-Horan | NHS | Xp22.13 | TOF, VSD, PDA | <10 | Congenital cataracts, strabismus, peg-shaped supernumerary teeth, other dental anomalies, prominent ears, brachymetacarpalia | 147 |
| Peter’s Plus | B3GALTL | 13q12.3 | ASD, VSD, PVS, BPV, subvalvular AS | <30 | Short limb growth deficiency, intellectual disability, autism spectrum disorder, prominent forehead, cupid’s bow upper lip, cleft lip ± cleft palate, Peter’s anomaly, cataracts, hydronephrosis | 148,149 |
| Roberts | ESC02 | 8p21.1 | ASD, AS | <20 | Growth deficiency of prenatal onset, cleft lip ± cleft palate, hypertelorism, sparse hair, hypomelia with variable limb reduction defects, cryptorchidism | 150 |
| Robinow | RDR2 (AR) | 9q22 | RVOTO | 29 AD | Macrocephaly, frontal bossing, prominent eyes, small upturned nose, short forearms, hemivertebrae, hypoplastic phalanges of hands and toes, hypoplastic genitalia | 151, 152 |
| WNT5A (AD) | 13 AR | |||||
| Saethre-Chotzen | TWIST | 7p21p22 | VSD | <10 | Craniosynostosis, brachycephaly, high flat forehead, hypertelorism, ptosis, partial cutaneous syndactyly, broad great toes, strabismus | 153 |
| Short rib polydactyly type I | DYNC2H1 | 11q22.3 | TGA, DORV, DOLV, AVSD, HRH | <25 | Short stature, postaxial polydactyly of hands or feet, short horizontal ribs, small iliac bones, polycystic kidneys, early death from respiratory insufficiency | 154 |
| Simpson-Golabi-Behmel | GPC3 | Xq26.2 | TGA, VSD, PVS, CoA, AS, PDA, BAV, CM | 26 | Macrosomia, coarse face, macroglossia, hepatosplenomegaly, nephromegaly, variable cognitive disability | 155, 156 |
| Sotos | NSD1 | 5q35.3 | ASD, PDA, VSD | 21 | Excessive size, large hands and feet, prominent forehead, hypotonia, variable intellectual disability, scoliosis, advanced bone age | 157 |
| Townes-Brocks | SALL1 | 16p12.1 | ASD, TOF, VSD, TA, PA, PDA | 14–25 | Auricular anomalies, preauricular tags, hearing loss, thumb hypoplasia/polydactyly, imperforate anus, renal agenesis, multicystic kidney, microphthalmia | 158 |
22q11.2DS indicates 22q11.2 deletion syndrome; AD, autosomal dominant; AR, autosomal recessive; AS, aortic stenosis; ASD, atrial septal defect; AVA, aortic valve anomaly; AVSD, atrioventricular septal defect; BAV, bicuspid aortic valve; BPV, bicuspid pulmonary valve; CFC, cardiofaciocutaneous; CHARGE, coloboma, heart defects, choanal atresia, retarded growth and development, genital anomalies, and ear anomalies; CM, cardiomyopathy; CoA, coarctation of the aorta; DEX, dextrocardia; DOLV, double-outlet left ventricle; DORV, double-outlet right ventricle; HCM, hypertrophic cardiomyopathy; HD, heart disease; HLHS, hypoplastic left heart; HRH, hypoplastic right heart; IAA, interruption of aortic arch; LVNC, left ventricular noncompaction; MR, mitral regurgitation; MVP, mitral valve prolapse; OFD, oral-facial-digital; PA, pulmonary atresia; PAS, pulmonary artery stenosis; PDA, patent ductus arteriosus; PE, pericardial effusion; PPS, peripheral pulmonary stenosis; PS, pulmonary stenosis; PVS, pulmonary stenosis; RVOTO, right ventricular outflow tract obstruction; SVAS, supravalvular aortic stenosis; TA, truncus arteriosus; TGA, transposition of great arteries; TOF, tetralogy of Fallot; VACTERL, association of vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal and limb anomalies; VR, vascular ring; and VSD, ventricular septal defect.
Alagille Syndrome
Alagille syndrome (ALGS) is an autosomal dominant syndromic disorder characterized by cardiovascular, hepatic, orthopedic, and ophthalmologic complications.
Common Features
Recognizable Facial Features
Children with ALGS have a prominent forehead, deeply set eyes, hypertelorism, straight nose with a bulbous tip, and pointed chin.
Development
Mild gross motor delays are reported in 16% of individuals,159 and mild intellectual disability is seen in only 2%. Neurovascular accidents, likely secondary to prestenotic vessel aneurysms, occur in up to 15% of cases and can cause significant neurological compromise.160
Hepatic
There is considerable intrafamilial and interfamilial variability in the hepatic complications of ALGS, and some individuals have no detectable liver disease. The most common complications are chronic cholestasis, elevated liver enzymes, hypercholesterolemia, or liver failure.161 Infants with ALGS can present with jaundice, cholestasis, and pruritis. The typical pathological finding is paucity of the bile ducts on liver biopsy. It is estimated that ≈15% of affected individuals will require liver transplantation.160
Ophthalmologic
More than 80% will have posterior embryotoxon, an anterior chamber defect, by slit-lamp examination.160,162 Although not of any functional significance to vision, it is a useful marker for diagnosis. Additional complications include Axenfeld anomaly, Rieger anomaly, optic disk drusen, and retinal pigmentary changes.163
Orthopedic
It is estimated that 30% to 90% of individuals with ALGS have butterfly vertebrae by radiography.159 Butterfly vertebrae are typically not of any clinical consequence but are a useful marker for diagnosis. Less commonly reported skeletal features include hemivertebrae, spina bifida occulta, and rib anomalies.
Renal
Kidney complications including small hyperechoic kidneys, uteropelvic obstruction, renal tubular acidosis, hypertension, and renal artery stenosis are reported in ≈40%.164
Cardiovascular Features
Two-thirds of those with ALGS have peripheral or branch pulmonary stenosis or other arterial narrowing (aortic coarctation, renal artery, middle aortic syndrome, Moya-moya, basilar, and middle cerebral arteries).159 Structural cardiac defects are also reported, including tetralogy of Fallot (7%–15% of cases), aortic stenosis, ASD, and VSD.160
Prevalence
There is no known racial or ethnic predilection for ALGS. There is an estimated incidence of 1:30000 to 1:50000 live births.159,165
Molecular Genetics
Pathogenic variants in JAG1 cause >90% of ALGS, with 89% attributable to sequence variants and 5% to 7% attributable to partial or complete gene deletions.159 An estimated 1% to 2% of individuals who meet clinical criteria for ALGS and do not have a JAG1 mutation will have a NOTCH2 sequence variant.115 The Jagged1 and Notch proteins are part of the Notch signaling pathway, which is important to regulation of cell fate in many cell types during development.159
Cardiovascular Genotype/Phenotype Correlations
Overall, there are no differences in the cardiovascular phenotype based on causative gene or mutation type (sequence variant versus deletion). However, there have been 2 variants reported for which affected individuals had cardiac but not liver disease, and further analysis demonstrated that the amount of JAG1 protein produced was more than in other ALGS variants but less than in wild type.166 Because the characteristic facial features can be subtle and the presentation variable, it is important to consider a diagnosis of ALGS in those with characteristic cardiovascular findings, even in the absence of overt liver disease.
Holt-Oram Syndrome
Holt-Oram syndrome (HOS) is an autosomal dominant disorder often referred to as heart-hand syndrome because of the 2 most common features: congenital HD and radial ray defects.
Common Features
Orthopedic
Radial ray abnormalities can be unilateral or bilateral and, when bilateral, can be symmetrical or asymmetrical. The penetrance of upper limb anomalies in HOS is complete but ranges from subtle carpal abnormalities without functional consequence only seen by radiogram to complete phocomelia (the hand attached close to the trunk). Other reported abnormalities include triphalangeal thumb, absent thumb, radius hypoplasia or aplasia, and radioulnar synostosis.167,168
Family History
Because there is considerable intrafamilial phenotypic variability, a family history of a first-degree relative with a septal defect, cardiac conduction disease, or radial ray abnormality can provide a clue to the diagnosis.
Cardiac Features
Three quarters of those with HOS have congenital HD, most commonly involving the atrial or ventricular septum. ASDs can present as common atrium, often with atrial isomerism.169 Cardiac conduction disease is seen in those with or without congenital HD. Sinus bradycardia, first-degree atrioventricular heart block, and complete heart block with or without atrial fibrillation are all reported coincident with or subsequent to the time of congenital HD diagnosis (if present).167 This has led to the recommendation that all individuals with HOS have an annual screening ECG.
Prevalence
HOS has an estimated prevalence of between 0.7 and 1 per 100 000.169
Molecular Genetics
Seventy percent of cases are caused by a heterozygous pathogenic variant in TBX5, <1% by a partial or complete gene deletion.125 Most variants result in a null allele and haploinsufficiency. TBX5 is a transcription factor and is an essential regulator of limb and cardiac development, particularly the cardiac septum and conduction system.168
Cardiovascular Genotype/Phenotype Correlations
Pathogenic missense variants at the 5ʹend of the T-box are associated with more serious cardiac defects.170
Char Syndrome
Char syndrome is an autosomal dominant familial PDA syndrome.
Common Features
Recognizable Facial Features
Flat midface, flat nasal bridge, broad nasal tip, hypertelorism, down-slanting palpebral fissures, mild ptosis, short philtrum, and everted lips are among the recognizable facial features.171
Orthopedic
Aplasia or hypoplasia of the middle phalanges of the fifth fingers is part of the diagnostic triad (along with typical facial features and PDA) of Char syndrome.172
Other
Case reports indicate a number of additional features can be seen in Char syndrome, including hypodontia, foot anomalies (joint fusion, clinodactyly, polydactyly, syndactyly), strabismus, and other hand anomalies (interstitial polydactyly, distal symphalangism of the fifth fingers, and third finger hypoplasia).172
Cardiac Features
The primary cardiac finding is PDA. Other heart defects, including VSD and more complex congenital HDs, have been reported.172
Prevalence
The prevalence has not been determined, but it is thought to be quite rare.
Molecular Genetics
Approximately half of families who have the diagnostic triad of Char syndrome (recognizable facial features, aplasia or hypoplasia of the middle phalanges of the fifth fingers, and PDA) will have a heterozygous pathogenic variant in TFAP2B.119 The majority of mutations affect the highly conserved C-terminal half of the protein’s basic domain that is essential for DNA binding.
Cardiovascular Genotype/Phenotype Correlations
There are no known genotype-phenotype correlations with regard to cardiovascular complications. There have been reports of TFAP2B pathogenic variants in cases of PDA without the facial or orthopedic findings of Char syndrome.173
Ellis-van Creveld Syndrome
Ellis-van Creveld syndrome (EVC) is an autosomal recessive skeletal dysplasia associated with a characteristic cardiac finding of a primary atrial septation defect resulting in a common atrium.123
Common Features
Recognizable Facial Features
Individuals with EVC can have a characteristic appearance of the mouth, with a short upper lip bound by frenula to the alveolar ridge.
Dental
A variety of dental abnormalities are reported, including natal teeth, partial adontia, small teeth, delayed tooth eruption, conical teeth, and enamel hypoplasia.174,175
Hair and Nails
The nails are often hypoplastic, and hair can be scant or fine.176
Growth
There is prenatal-onset short stature; adult stature is in the range of 43 to 60 inches.177
Orthopedic
The characteristic skeletal findings include postaxial polydactyly, usually of the hands, short limbs (with increasing severity from the proximal to distal portions of the limbs), and short ribs. Hand radiographs often show short, broad middle phalanges and hypoplastic distal phalanges, and sometimes carpal bone abnormalities.175 Bone age is usually delayed.
Cardiac Features
It has been estimated that 50% to 60% of cases have congenital HD, characteristically common atrium. Abnormalities of the mitral and tricuspid valves, PDA, VSD, and HLHS are also reported.178 The severity of the congenital HD is the main determinant of morbidity and mortality.175
Prevalence
The worldwide prevalence is not known. There is a founder mutation among the Amish, and large kindreds from Mexico, Ecuador, and Brazil that have also been reported.123
Molecular Genetics
Two-thirds of cases of EVC are caused by homozygous or compound heterozygous mutations in EVC or EVC2.123,179 These 2 genes are in a 5ʹ to 5ʹ (head-to-head) orientation in close proximity and are thought to share a common, bidirectional promoter.180
Cardiovascular Genotype/Phenotype Correlations
No cardiovascular genotype-phenotype correlations have been reported.
Adams-Oliver Syndrome
Adams-Oliver syndrome (AOS) is an inherited malformation syndrome in which cardiac, scalp, and limb defects are present. There is genetic heterogeneity, with both autosomal dominant and autosomal recessive forms.
Common Features
Skin and Scalp Defects
There is considerable variability in the extent of aplasia cutis congenita in affected individuals, ranging from total absence of an area of scalp skin and skull to vertex hairless patches.
Orthopedic
Limb defects can include terminal transverse reduction defects of hands or feet, short distal phalanges, syndactyly, ectrodactyly, and polydactyly.
Central Nervous System
Brain anomalies occur in 35% of affected individuals, including microcephaly, encephalocele, neuronal migration anomalies, thin or absent corpus callosum, and enlarged ventricles. Some evidence of vascular sequelae in the brain has been documented, with calcification, periventricular leukomalacia, and stroke/ thrombosis.140
Ophthalmologic
Ophthalmologic findings are uncommon in AOS but do occur, including retinal folds/detachment, cataract, and optic nerve hypoplasia.140
Cardiovascular Features
One-fourth of individuals with AOS have congenital HD, often left-sided obstructive malformations such as BAV, aortic stenosis, HLHS, coarctation of the aorta, and parachute mitral valve. Other defects include VSD, ASD, tetralogy of Fallot, and other conotruncal defects.181 Vascular lesions such as hepatic thrombosis, PVS,141,182 intracranial vascular lesions, and limb vascular anomalies have also been described.
Prevalence
There is an estimated incidence of 0.44 per 100000 live births.183 This could be a significant underestimate, because not all clinical features are present in all affected individuals.
Molecular Genetics
Six genes are currently involved in the pathogenesis of AOS. Two genes, ARHGAP31 (autosomal dominant gain-of-function mutations) and DOCK6 (homozygous loss-of-function mutations), are part of the CDC42/RAC1 pathway. The other 4 genes (RBPJ, EGOT, NOTCH1, and DLL4) are part of the Notch signaling pathway, which regulates cell fate in many cell types.140
Cardiovascular Genotype/Phenotype Correlation
Pathogenic variants of NOTCH1 are associated with a 42% occurrence of congenital HD and vasculopathy in AOS.141,184 The other 5 genes associated with AOS do not have as frequent vasculopathies or cardiac malformations. Additionally, NOTCH1 gene variants have been associated with autosomal dominant left ventricular outflow defects (most commonly BAV and calcific aortic stenosis) without evidence of AOS185 and familial BAV without evidence of AOS.186
Kabuki Syndrome
Kabuki syndrome (KS) has both X-linked and autosomal dominant pathogeneses. The syndrome is characterized by specific facial features, skeletal anomalies, congenital HD, renal anomalies, intellectual disability, and growth deficiency.
Common Features
Recognizable Facial Features
Children with KS have long palpebral fissures, eversion of lateral one-third of the lower eyelid, arched eyebrows with sparse lateral third, large dysplastic ears, cleft palate, and depressed nasal tip.187
Development
Mild to moderate intellectual disability is seen in 82% to 90% of individuals, with one-third having expressive and receptive language difficulties. There can be associated autism spectrum disorder, communication difficulties, and repetitive behavior.
Orthopedic
More than 80% have skeletal findings such as vertebral anomalies, scoliosis, hip dislocation, short incurved fifth fingers, brachydactyly, and hyperextensible joints.188
Urogenital Anomalies
Cryptorchidism, duplicated collecting system, single fused kidney, and hypospadias have been reported.188
Other
Growth deficiency is present in 55% and hearing loss in 28% to 40%, with immunodeficiency and persistent fetal finger pads also common.189
Cardiovascular Features
Congenital HD occurs in 40% to 70% of individuals with KS.126,127 There is a predominance of left-sided obstructive defects, including coarctation of the aorta, BAV, and HLHS.190 The most common cardiac malformations are coarctation of the aorta, ASD, and VSD. Other defects include double-outlet right ventricle, pulmonary stenosis, mitral atresia/stenosis, and partial anomalous pulmonary venous return.191–193
Prevalence
The prevalence in Japan was estimated at 1:32 000,194 as the initial patients described were Japanese. A minimum birth incidence of 1:86000 in Australia and New Zealand has been calculated.195
Molecular Genetics
KS is caused mainly by pathogenic variants in the KMT2D (MLL2) and KDM6A genes. Only a few cases with a Kabuki-like phenotype have been described with RAP1A and RAP1B and HNKRNPK variants.196 Germline dominant, usually truncating, variants in KMT2D cause most cases of KS (75%).197 Pathogenic variants in the X-linked gene KDM6A are found in ≈5% of individuals with KS, which are also generally truncating variants but with a few whole-gene deletions described.198 It has been noticed that KS and CHARGE have some overlapping clinical features. Additionally, there are a number of patients with a Kabuki-like syndrome who are under investigation for related genes in the CHARGE/Kabuki spectrum, as well as heterogeneous nuclear ribonucleoprotein K (HNRNPK) haploinsufficiency.199 Furthermore, a KMT2D novel variant has been found in 2 generations of a family with choanal atresia, which also suggests a connection to CHARGE syndrome.200
Cardiovascular Genotype/Phenotype Correlations
A preponderance of males compared with females with left-sided obstructive lesions has been described among KMT2D patients.196 Those with KDM6A mutations have a frequency of congenital HD of 45%, with a higher prevalence of right-sided congenital HD.196
CHARGE Syndrome
The acronymic name of this condition includes C for coloboma, H for heart defects, A for choanal atresia, R for retarded growth and development, G for genital anomalies, and E for ear anomalies. CHARGE syndrome is inherited as an autosomal dominant condition, but it is usually sporadic. Diagnostic criteria are helpful in determining a clinical diagnosis for individuals suspected of having CHARGE syndrome.121,201
Common Features
Recognizable Facial Features
Characteristic facial features can include orofacial clefts, unilateral or bilateral facial palsy, and malformed protruding ear pinnae.
Development
Marked developmental delay is usual. Motor skills are delayed with hypotonia. Delayed language development can result from hearing loss and reduced vision. The intellectual outcome is variable, with up to 50% with good outcome.202 If microcephaly, brain malformations, and extensive coloboma are present, these suggest a poorer intellectual outcome.
Ophthalmologic
More than 80% to 90% of individuals will have unilateral or bilateral colobomas variably affecting the iris, retina, choroid, or optic discs, sometimes associated with microphthalmia. Vision is variably affected by the colobomas.
Ears and Hearing
Malformed external ear pinnae, anomalies of the ossicles, Mondini cochlea defect, and absent or small semicircular canals are present in >90% of affected individuals. Hearing loss is extremely common and varies from mild to profound.203,204
Respiratory
Bilateral or unilateral choanal atresia is present in >50%, necessitating immediate evaluation and possibly tracheostomy.
Gastrointestinal
Individuals can have severe swallowing difficulties, aspiration problems, gastroesophageal reflux, and tracheoesophageal fistula. Feeding problems are very common, and gastrostomy feeding measures are often required.204
Genital/Renal
Males can have cryptorchidism and micropenis, and both males and females can have hypogonadotropic hypogonadism.203 Occasional renal anomalies such as horseshoe kidney and renal dysgenesis are found.
Orthopedic
Hand anomalies including polydactyly and occasional scoliosis are possible.
Cardiovascular Features
Three-fourths of those with CHARGE have congenital HD, and these are often complex.205 These can be conotruncal defects, including tetralogy of Fallot, IAA, truncus arteriosus, and double-outlet right ventricle. Multiple other abnormalities have been seen in CHARGE, including vascular rings, aortic arch anomalies, AVSD, septal defects, and PDA.206
Prevalence
CHARGE syndrome occurs in 1 in 8500 births.207
Molecular Genetics
CHARGE syndrome is caused by pathogenic variants in the CHD7 gene in the majority of individuals suspected clinically of having the syndrome.203 A few rare instances of exon, whole gene, or large contiguous deletions have been found.208 Most affected individuals are the only family member with clinical findings; however, some familial cases of CHARGE syndrome have been described.209 Many individuals with familial CHD7 variants are mildly affected and do not completely fulfill the diagnostic criteria for CHARGE syndrome.210 Some of these more mildly affected individuals were only recognized after a more seriously affected family member was found to have a CHD7 pathogenic variant. Some families in which there are affected siblings and unaffected parents are likely examples of gonadal mosaicism. In recent years, marked overlap in clinical features with CHARGE syndrome has been seen in individuals eventually discovered to have KS, 22q11.2 deletion, or Kallmann syndrome.200,210
Cardiovascular Genotype/Phenotype Correlations
Congenital HD is more commonly found in individuals with truncating variants of CHD7 (80%) than with missense or splice-site variants (58%).205
THE RASOPATHIES
The RASopathies are a group of autosomal dominant disorders with overlapping cardiac, growth, facial, and neurodevelopmental features. They are so named because they are caused by pathogenic variants in genes that encode proteins in or with close interaction with the RAS/ mitogen-activated protein kinase pathway, which plays an important role in cellular programs, including apoptosis, development, differentiation, proliferation, and transformation. Somatic mutations in genes in the pathway have long been known to cause hematologic cancers and solid tumors. More recently, germline sequence variants have been found to cause Noonan syndrome (NS) and other uncommon phenotypically related disorders, including cardiofaciocutaneous syndrome (CFC), Costello syndrome (CS), and Noonan syndrome with multiple lentigines (NSML). Collectively, these disorders are termed the RASopathies. Although it has more unique features than it has overlapping features to NS, CFC, CS, and NSML, neurofibromatosis type 1 is often included as a RASopathy. Because it infrequently presents with significant cardiac complications (2% of cases), neurofibromatosis type 1 will not be further discussed here.211
Noonan Syndrome
Individuals with NS have characteristic facial features and structural and functional abnormalities involving multiple organ syndromes and a high incidence of cardiac abnormalities.
Common Features
Recognizable Facial Features
The facial features of NS change with age.212 They can be subtle during infancy (tall forehead, widely spaced prominent eyes that slant down, depressed nasal bridge, bulbous nasal tip, and low-set ears), more obvious during childhood (ptosis and neck webbing also seen), and change again during adolescence (eyes less prominent, nasal root pinched with a thin bridge, and the shape of the face is that of an inverted triangle). In adulthood, the features are most often mild, although some adults retain significant, readily recognizable dysmorphisms.
Eye and Ear
An estimated 80% of those with NS have a structural eye abnormality, including ptosis (50%), strabismus (40%), refractive error (60%), posterior segment abnormalities (6%), and anterior segment abnormalities (60%).213 A minority have conductive hearing loss attributable to middle ear effusion (20%) or sensorineural hearing loss (10%).214
Gastrointestinal
Early feeding problems related to hypotonia and delayed gastrointestinal motor development, gastroesophageal reflux, chronic constipation, and intestinal malrotation respond well to medical management and feeding therapy.215 It is not uncommon for early feeding issues to be significant enough to require temporary placement of a gastrostomy feeding tube.
Growth and Endocrine
The most common endocrine complications include hypothyroidism, pubertal delay, and short stature. The pathogenesis for the short stature can be nutritional, attributable to growth hormone deficiency, or attributable to growth hormone insensitivity.216 Short stature in NS is a Food and Drug Administration–approved indication for growth hormone therapy. Looking across studies, there is a mean gain in height of 9.5 to 13 cm for boys and 9 to 9.8 cm for girls with growth hormone therapy.128 Treatment outcomes are best with earlier initiation and longer duration.217 To date, there is no evidence that treatment with growth hormone exacerbates the cardiac complications of NS.128
Hematology
Coagulation factor deficiencies, thrombocytopenia, and platelet aggregation abnormalities have all been reported218; however, only a small proportion of those with abnormalities on coagulation testing have functional bleeding problems. The observed rate of postoperative bleeding complications in a cohort of 142 individuals with NS was <2% (half of the cohort had been screened preoperatively for a coagulopathy and half had not).219
NS attributable to PTPN11 mutations is associated with an increased risk of hematologic malignancies, including acute lymphoblastic leukemia and juvenile myelomonocytic leukemia. Myeloproliferative disorders are also more common in NS than in the general pediatric population and are associated with a benign course in 40% and an aggressive course in 15%.220
Lymphatic
Lymphatic abnormalities are thought to affect ≈20% of individuals.221 Peripheral edema can be seen during infancy and usually regresses during the first year. It can occur or recur in adolescence or adulthood. Chylous effusion is a regularly reported complication of cardiac surgery. Less commonly, pulmonary, intestinal, and testicular lymphangiectasia are reported.222
Neurological, Cognitive, and Behavioral
Seizures are reported in a minority of cases (10%–13%) and include generalized, temporal lobe, and febrile seizures.223 Structural brain abnormalities are rare, but there are multiple case reports of symptomatic Chiari I malformation.224 There are highly variable neurocognitive and behavioral outcomes that depend, in part, on the causative gene. Gross and fine motor development are often delayed because of hypotonia, congenital HD, or orthopedic issues.225 Although many school-aged children require individualized education plans or special education instruction, intellectual disability is uncommon (6%–23% across studies).226
Orthopedic
The most commonly reported orthopedic complications include radioulnar synostosis, pectus carinatum and excavatum, scoliosis, and pes planus.227
Renal and Genitourinary
Renal anomalies, including vesicoureteral reflux, hydronephrosis, and dysplastic kidney, are seen in 10% to 20% of individuals.128 The majority of males have cryptorchidism (80%).
Cardiac Features
Cardiovascular involvement is observed in 80% to 90% of affected individuals, comprising congenital HD and hypertrophic cardiomyopathy (HCM).222,228 The most common congenital HD is PVS, seen in roughly 40% of patients and often with dysplastic valve leaflets, but other prevalent lesions include aortic coarctation, mitral valve anomalies, ASDs, and tetralogy of Fallot. HCM, seen in up to 20% of patients, can vary from a mild, stable form, typically presenting in toddlers, to a severe, rapidly progressive form that presents in early infancy and is often life-threatening.229 Arterial defects such as aneurysms (coronary, aortic, pulmonary, intracranial) and coronary atresia have also been observed.230,231
Prevalence
Systematic epidemiological studies have not been completed, but a prevalence of 1:1000 to 1:2500 has been estimated.232
Molecular Genetics
NS is an autosomal dominant disorder with complete penetrance and variable expressivity. Fifty percent of cases are explained by heterozygous PTPN11 missense pathologic variants.233 PTPN11 encodes SHP2, a phosphatase that has an active and inactive conformation. Pathogenic variants alter residues that stabilize the inactive state, activating SHP2 and leading to increased RAS/ERK (extracellular signal-regulated kinase)/MAPK (mitogen-activated protein kinase) activation.234 It is estimated that an additional 30% of cases can be explained by a variant in one of multiple genes in the RAS MAPK pathway including SOS1, RAF1, RIT1, KRAS, SHOC2, NRAS, SOS2, and BRAF.212 Case reports or small case series implicate other genes in the pathway, including A2ML1, LZTR1, MYST4, RASA2, RRAS, SPRY1, and SYN-GAP1.235 Approximately half of the cases are de novo, and the other half are inherited. In the nonfamilial cases, there is an association with advanced paternal age.236
Cardiovascular Genotype/Phenotype Correlations
PTPN11-associated NS is more likely to cause PVS and less likely to cause HCM.234 Septal defects are more common in those with SOS1-associated NS.237 Although only ≈20% of patients with NS have HCM, 95% of those with a RAF1 mutation and 75% with a RIT1 mutation have it.238,239
Other RASopathies
CFC, CS, and NSML are among the other RASopathies. They share common features, including developmental delays, short stature, ptosis, hypertelorism, macrocephaly, and cardiac involvement. There is such significant phenotypic overlap that it can be challenging, particularly during infancy, to make the diagnosis based on clinical features alone.
Common Features
Cardiofaciocutaneous Syndrome
In contrast to NS, CFC is characterized by more significant feeding issues (often requiring long-term gastrostomy tube use) and cognitive delays (with the majority of individuals in the mild to moderate intellectual disability range) and by a variety of cutaneous abnormalities, including hyperkeratosis, ichthyosis, keratosis pilaris, ulerythema ophryogenes, and xerosis.240 CFC is considerably rarer than NS, with an estimated prevalence of 1 in 810 000.241
Costello Syndrome
Features most often seen in those with CS but not in NS include coarse facial features, loose and soft skin with deep creases of the palms and soles, bronzing of the skin during childhood, papillomata of the face and perianal region, and an increased risk for malignant tumors.242 Like NS and CFC, feeding issues are common and often require use of a gastrostomy tube. Intellectual disabilities are much more common than in NS but less severe than those seen in CFC. CS has an estimated birth prevalence of 1 in 300 000 to 1 in 1 200 000.241
NS With Multiple Lentigines
NSML (formerly known as LEOPARD syndrome) has the unique finding of multiple lentigines of the face, back, and upper trunk that number in the thousands by adulthood. There is a higher prevalence of sensorineural hearing loss and a lower prevalence of short stature than is reported in NS.243 The overall prevalence of NSML is unknown. Mild learning issues are reported in ≈30% of individuals, but intellectual disability is rare.244
Cardiac Features
Three-fourths of individuals with a RASopathy have a cardiac abnormality, which is the second most common reason a child comes to medical attention (after admission to a neonatal intensive care unit).245 Although there are a wide variety of cardiovascular diagnoses reported, PVS, HCM, and ASD are the most common complications reported in each of the RASopathies. The majority of individuals with NSML have HCM compared with only one-fifth of those with NS.246 CS can be complicated by arrhythmia, usually supraventricular tachycardia, and most distinctive is chaotic atrial rhythm/multifocal atrial tachycardia.242
Molecular Genetics
The majority of cases of CFC are caused by a heterozygous pathogenic variant in BRAF, MAP2K1, MAP2K2, or KRAS. HRAS is the only gene in which pathogenic variants are known to cause CS, and >95% of variants affect amino acid p.Gly12 or p.Gly13.247 Ninety percent of NSML cases are caused by loss-of-function variants in PTPN11 that impair SHP2 catalytic activity.248 Less than 5% of NSML cases have been ascribed to a heterozygous pathogenic variant in RAF1, BRAF, or MAP2K1.
Clinical Genetic Testing
Potential approaches include single-gene testing, multigene panel testing, and more comprehensive genomic approaches such as whole-exome or whole-genome sequencing. Because there is significant genetic heterogeneity for a given diagnosis and extensive phenotypic overlap between diagnoses, multigene panel testing that includes all of the RASopathy genes is likely the most cost-effective and clinically indicated approach. A molecular genetic diagnosis allows for specific prognosis, anticipatory guidance, and recurrence risk estimates for families.
Suggested Cardiac Follow-up
If not completed already, an evaluation with a cardiologist, including an echocardiogram and ECG, is indicated at the time of diagnosis. Follow-up is tailored to the individual findings, ideally informed by the spectrum of disease and natural history of cardiac abnormalities in the RASopathies. If no cardiac disease is detected, repeat evaluation with a cardiologist is indicated every 5 years throughout childhood and adulthood.128,222
HETEROTAXY AND CILIOPATHIES
Cilia Structure and Function
Cilia are ancient organelles with a broad range of biological functions that center on sending and receiving signals to and from the extracellular environment. Abnormal cilia structure and function result in diverse diseases, including syndromic ciliopathies, primary ciliary dyskinesia (PCD), and heterotaxy syndrome.249 Finally, there is growing evidence that abnormal function of cilia can result in isolated congenital HD.250,251
All cilia extend from a basal body and contain doublet microtubules (Figure [C]). These doublets extend as the axoneme, a highly ordered arrangement that is recognizable by transmission electron microscopy. Motile cilia are primarily found on epithelial cells that line the respiratory tract, brain ventricles, and oviducts. These cilia function to propel cells or extracellular fluid and are characterized by 9 microtubule doublets surrounding a central pair, a “9+2” arrangement that is visible by electron microscopy of cross-sectional views (Figure [A]). Absence or dysfunction of motile cilia causes PCD. A special subtype of motile cilia are the cilia found on the left-right organizer (LRO) that have a “9+0” arrangement but are motile. In contrast, sensory cilia have a “9+0” arrangement of microtubules (Figure [B]) but are nonmotile cilia. These cilia extend from the surface of almost all cell types in the human body, including epithelial cells lining the kidney tubules and bile ducts, as well as nonepithelial cells such as chondrocytes and neurons.252 These cilia are responsible for sensing the extracellular environment, are important for transducing signals, and play a role in intercellular signaling during developmental patterning.
Figure. Ciliary structure.
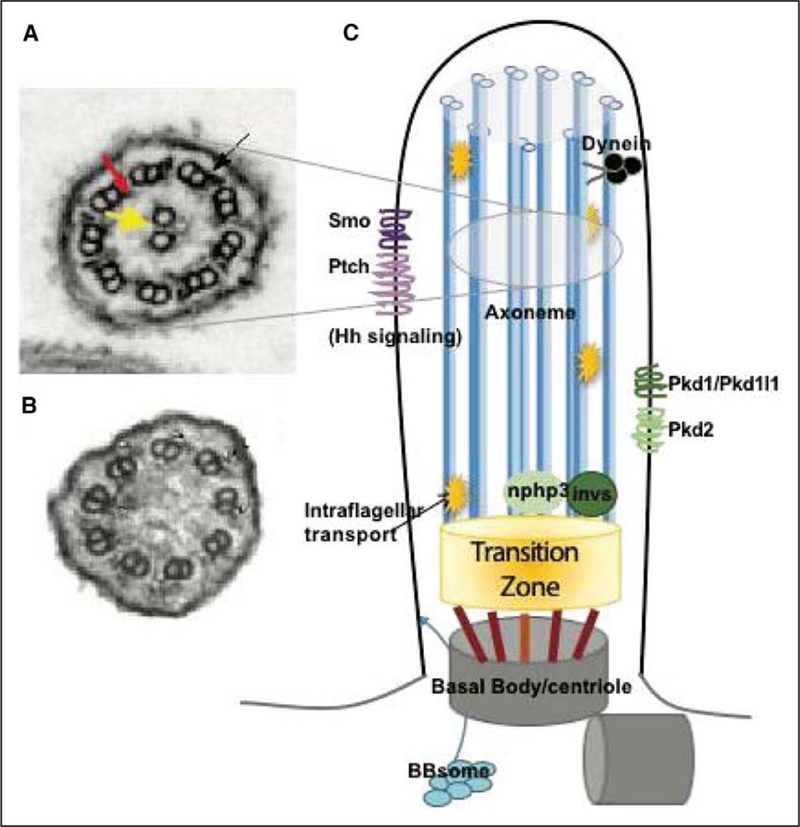
A, Transmission electron microgram (TEM) cross section of a 9+2 motile cilium. The central pair is indicated by the yellow arrowhead. Outer dynein arms (black arrow) and inner dynein arms (red arrow) are shown linking the 9 sets of microtubule doublets. Location in the ciliary axoneme in (C) is indicated. B, TEM of a 9+0 sensory cilium; note the absence of central pair. C, Diagrammatic representation of a cilium indicating structures that have been linked to congenital heart disease. Hh indicates hedgehog.
Cilia in Heart Development
The best understood role for cilia in heart development is establishing left-right (LR) asymmetry. The heart has striking asymmetries along the LR axis, all of which depend on global LR positional cues that originate from a ciliated LRO early in development, before cardiac morphogenesis. The LRO is highly conserved among vertebrates253 and functions through motile LRO cilia to generate directional fluid flow.254 Sensing this flow requires functional polycystin channels localized to the LRO sensory cilia.255,256 Activation of the sensory LRO cilia leads to LR asymmetrical gene expression of genes including cerl2, nodal, lefty, and pitx2. The precise mechanisms that connect asymmetrical signals to heart development remain unknown. Finally, asymmetrical left-sided signals are constrained by a midline barrier.249,257 This framework predicts relationships between gene variants that result in abnormal cilia function and the specific associated cardiac laterality defects (Table 6).
Table 6.
Summary of Ciliopathies
| Ciliopathy | Features | Gene(s) | Cardiac Defects |
|---|---|---|---|
| Primary ciliary dyskinesia | Bronchiectasis, sinusitis, otitis media, infertility, situs defects | AK7, ARMC4, C21orf59, CCDC103, CCDC114, CCDC151, CCDC39, CCDC40, CCDC65, CCNO, DNAAF1, DNAAF2, DNAAF3, DNAAF5, DNAH11, DNAH5, DNAH6, DNAI2, DNAL1, DNAJB13, DRC1, DYX1C1, GAS8, HEATR2, HYDIN, LRRC6, MCIDAS, NME8, PIH1D3, RPGR, TXNDC3, RSPH1, RSPH3, RSPH4A, RSPH9, SPAG1, TTC25, ZMYND10 | Dextrocardia; heterotaxy spectrum heart defects in ≈12%; heterotaxy not thought to occur with genes associated with central pair or radial spoke |
| Polycystic kidney disease | Renal cysts; hepatic fibrosis; autosomal dominant and recessive forms | GANAB, PKHD1, PKD1, PKD2 | Reported association with aortic dilation |
| Nephronophthisis | Renal cysts with or without extrarenal symptoms | NPHP1–4, IQCB1, CEP290, ANKS6, GLIS2, CEP83, CEP164, RPGRIP1L, NEK8, SDCCAG8, TMEM67, TTC21B, DCDC2, IFT172, WDR19, ZNF423 | Reported in conjunction with allelic syndromes |
| Meckel-Gruber syndrome | Renal cysts, CNS anomalies (encephalocele), polydactyly, hepatic fibrosis, congenital heart defects | MKS1, TMEM216, TMEM67, CEP290, RPGRIP1L, CC2D2A, NPHP3, TCTN2, B9D1, B9D2, TMEM231, KIF14, TMEM107 | Situs inversus; heterotaxy; HLHS |
| Joubert and related syndromes | Hypoplasia of the cerebellar vermis (molar tooth sign), dysregulated breathing pattern, retinal dystrophy, renal anomalies | AH1, C5ORF42, CC2D2A, CSPP1, TMEM216, NPHP1, CEP290, TMEM67, RPGRIP1L, INPP5E, TCTN2, MKS1, CEP104, CEP120, CEP41, KIAA0556, PDE6D, PIBF1, TCTN1, TCTN3, ARL13B, CEP41, KIAA0586, TMEM237, TMEM231, TMEM138, KIAA0753, TMEM107, KIF7, OFD1, C2CD3, IFT172, ARL13B, ZNF423, TTC21B, PDE60, POC18, B9D2, B9D1 | Laterality defects; heart defects including septal defects, aortic valve anomalies, coarctation; in some cases, associated with features of OFD |
| Bardet-Biedl syndrome | Obesity, polydactyly, retinitis pigmentosa, anosmia, congenital heart defects | BBS1, 2, ARL6 (BBS3), 4, 5, MKKS (BBS6), 7, TTC8 (BBS8), 9, 10, TRIM32 (BBS11), 12. MKS1, CEP290, WDPCP, SDCCAG8, IFT27, IFT172, LZTFL1, BBIP1, IFT27; modifiers MKS3, CCDC28B | Heart defects with incomplete penetrance (7%–50%); AS, PDA, PS, ASD, VSD, cardiomyopathy |
| Oral-facial-digital syndromes (types I-XVI and unclassified) | Oral cavity, face, and digit anomalies; CNS abnormalities; cystic kidney disease | OFD1, TMEM216, C5orf42, TMEM107, TCTN3, TMEM231, TMEM138, KIAA0753, SCLT1, C2CD3, DDX59, WDPCP, INTU, TMEM231, IFT57 | Mitral and tricuspid valve dysplasia, TOF, VSD, CoA, hypoplastic LV |
| Alström syndrome | Dilated cardiomyopathy, obesity, sensorineural hearing loss, retinitis pigmentosa, endocrine abnormalities, renal and hepatic disease | ALMS1 | Dilated cardiomyopathy |
| McKusick-Kaufman syndrome | Urogenital anomalies including hydrometrocolpos, postaxial polydactyly, congenital heart defects | MKKS | AVC defects, ASD, VSD, TOF, PDA, hypoplastic LV, LSVC; defects in ≈14% |
| Ellis van Creveld syndrome | Skeletal dysplasia; congenital heart defects; polydactyly; ectodermal dysplasia | EVC, EVC2 | AVC defects, APVR, septal defects |
| Short rib thoracic dysplasias including Jeune chondrodysplasia, Saldino-Mainzer | Skeletal dysplasia; thoracic deformities; polydactyly; renal cysts; retinitis pigmentosa | IFT80, DYNC2H1, TTC21B, WDR19, NEK1, WDR35, WDR60, IFT140, IFT172, WDR34, CEP120, KIAA0586, DYNC2LI1, IFT52, TCTEX1D2 | Rare; septal defects, laterality defects |
| Cranioectodermal dysplasia (Sensenbrenner syndrome) | Cranioectodermal dysplasia; narrow thorax, dental anomalies, hepatic and renal involvement | IFT122, WDR35, IFT 43, WDR19 | PDA, ASD, VSD, PS, LVH in 25%–50% |
| Carpenter syndrome | Acrocephaly; polysyndactyly, hypogenitalism, obesity, congenital heart defects | RAB23, MEGF8, RAB23 | PDA, PS, VSD, situs inversus, heterotaxy |
APVR indicates anomalous pulmonary vein return; AS, aortic stenosis; ASD, atrial septal defect; AVC, atrioventricular canal; CNS, central nervous system; CoA, coarctation of the aorta; HLHS, hypoplastic left heart syndrome; LSVC, left superior vena cava; LV, left ventricle; LVH, left ventricular hypertrophy; OFD, oral-facial-digital; PDA, patent ductus arteriosus; PS, pulmonary stenosis; TOF, tetralogy of Fallot; and VSD, ventricular septal defect.
Beyond their role at the LRO in establishing LR asymmetry, cilia are found in cardiac tissue, including the second heart field, where cilia are required for signaling via the sonic hedgehog pathway. Mouse and human mutations affecting ciliary hedgehog signaling, including genes important for syndromic ciliopathies such as MKS1 (Meckel-Gruber syndrome type 1, Bardet-Biedl syndrome type 13),250 MKKS (Bardet-Biedl syndrome type 6, McKusick-Kaufman syndrome),258 and EVC and EVC2 (Ellis-van Creveld syndrome)123,259,260 lead to atrioventricular canal defects without accompanying laterality defects. Cilia are also found on embryonic myocardial cells, in mesenchymal cells in the developing AV valves, and in the developing vasculature.261,262 It is possible that in these settings, they could function to integrate mechanical signals such as those generated by cardiac contraction or blood flow with cardiovascular development.
Heterotaxy Syndrome
Common Features
Heterotaxy, from the Greek heteros (different) and taxis (arrangement), refers to any placement of organs along the LR axis that deviates from complete situs solitus and complete situs inversus and includes left atrial isomerism (LAI) and right atrial isomerism (RAI). In LAI, there are 2 “left” sides with 2 left atrial appendages, absent sinus node, and multiple spleens; conversely, in RAI, there are 2 right atrial appendages, bilateral sinus nodes, and absent spleen. In both LAI and RAI, the liver is located at the midline, and abnormal positioning of the gall bladder and stomach is common. Abnormalities of spleen number (asplenia or polysplenia) can result in functional asplenia that requires management. Gut malrotation poses a risk for volvulus. Extrahepatic biliary atresia is a severe extracardiac complication that affects prognosis and mortality rate. Central nervous system abnormalities can also be seen.263–265 Heterotaxy is also associated with PCD, with one study finding that 37% of heterotaxy patients had features suggesting the possibility of PCD.266 In a minority of cases, heterotaxy can be identified in patients with other genetic syndromes such as trisomy 13, 22q11.2DS, CHARGE syndrome, or a syndromic ciliopathy. However, the majority of cases of heterotaxy do not occur as part of a larger genetic syndromic condition, and intellectual development is usually normal.
Cardiac Features
Heterotaxy is associated with congenital HD in 50% to 95% of cases; the majority of cases with heterotaxy spectrum including RAI, levocardia with abdominal situs inversus (isolated levocardia), or dextrocardia with abdominal situs solitus (isolated dextrocardia) have significant congenital HD, which leads to major morbidity and mortality.265 Notably, LAI is not always associated with significant intracardiac defects. Heterotaxy can be associated with almost all known congenital HD. The most prominent cardiac findings are atrioventricular canal defects that are frequently unbalanced and associated with other congenital HD such as malposed great vessels. Right ventricular obstruction and anomalous pulmonary venous return are more commonly observed in RAI, whereas left ventricular obstruction, interrupted inferior vena cava, and rhythm disturbances resulting from an absent sinus node are more commonly associated with LAI. The hallmark of congenital HD in heterotaxy, however, is that there is no absolutely defined pattern to the possible combination of cardiac and vascular defects.
Prevalence
Heterotaxy is estimated to occur in 1 per 10 000 live-births265 and constitutes ≈3% of congenital HD cases. Its incidence could be underestimated because of subtle or clinically insignificant findings of laterality disorders, such as bilateral superior vena cava.
Molecular Genetics
Aneuploidies, complex chromosomal rearrangements, and microdeletions have all been identified in patients with heterotaxy.263,267 Clinically relevant CNVs have been identified in 15% to 26% of patients with heterotaxy syndrome.268–272 Heterotaxy has the highest relative risk among all classes of congenital HDs, which supports a strong genetic component.273 Autosomal dominant, autosomal recessive, and X-linked inheritance patterns have all been described, but unlike other types of congenital HD, de novo sequence variants are not major contributors to heterotaxy.14,274,275 Pathogenic variants in the X-linked transcription factor ZIC3, a zinc-finger transcription factor that is required to form a functional LRO276 and is required to direct heart looping, causes heterotaxy in up to 5% of males and a smaller percentage of females with heterotaxy.277–281 ZIC3 pathogenic variants are identified in ≈75% of pedigrees with possible X-linked inheritance. Although penetrance is high, at least 1 case of nonpenetrance has been identified.282
Although many genes linked to heterotaxy are associated with cilia and LRO structure and function, there are many additional genes, including SHROOM3, GRK5, and ANKS3, that have been reported to contribute to heterotaxy with functions distinct from cilia. Sequence variants in genes required for propagation of the asymmetrical signal at the left lateral plate mesoderm, including NODAL, CFC1, LEFTY2, GDF1, SMAD2, and ACVR2B, have been associated with human laterality disturbances.283–285 Environmental modifiers such as maternal diabetes mellitus and monozygotic twinning have also been associated with heterotaxy spectrum defects.
Cardiovascular Genotype/Phenotype Correlations
One of the hallmarks of inherited laterality disorders is the broad range of both laterality and cardiac phenotypes that result from any given mutation. For example, loss-of-function variants in ZIC3 have been correlated with a range of phenotypes ranging from classic heterotaxy with variable extracardiac manifestations to isolated congenital HD.
Primary Ciliary Dyskinesia
The link between ciliary defects and congenital HD was first identified when Bjorn Afzelius identified defective ciliary structure in electron microscopic analysis of tracheal cilia with Kartagener’s triad, a syndrome consisting of respiratory disease, male infertility, and situs inversus in 50% of affected patients.286
Common Features
Kartagener syndrome is a subset of PCD, a disorder defined by abnormal ciliary motility in the airway epithelia. PCD is a highly heterogeneous disorder with pathogenic variants in >39 genes identified (Table 6), of which 23 have been linked to cardiac abnormalities.287 Not surprisingly, a retrospective study of patients diagnosed with PCD identified heterotaxy in a subset of the cohort.288 Neonatal respiratory distress (not related to cardiovascular malformations) is a frequent manifestation of PCD. Chronic wet, productive cough, daily rhinitis, recurrent or chronic bacterial infections of the lower airways, recurrent sinusitis, and otitis media are common features. Bronchiectasis is seen in adults. The diagnosis of PCD is made through sequencing PCD genes, by either WES or dedicated PCD panels, combined with nasal ciliary biopsy and analysis of ciliary structure and motility. Low nasal nitric oxide is a useful marker of PCD, but testing is not reliable in infants and young children.
Cardiac Features
Situs inversus totalis (mirror image reversal of all organs), the most common laterality phenotype associated with PCD, is part of the spectrum of laterality disorders resulting from ciliary dysfunction (Table 6) and occurs in 40% to 50% of cases. At least 12.1% of patients with classic PCD exhibit heterotaxy.289 Because a diagnosis of PCD in patients with congenital HD is inherently challenging given the difficulty in differentiating whether respiratory symptoms are primary or secondary to the underlying cardiac pathology and the medical and surgical interventions required to manage the congenital HD, it is possible that some patients thought to have isolated congenital HD actually have congenital HD as part of PCD.
Prevalence
The prevalence of PCD is not known with certainty, but PCD is estimated to affect ≈1 per 20 000 individuals.
Molecular Genetics
PCD is most commonly inherited as an autosomal recessive condition, although a rare association of X-linked PCD with retinitis pigmentosa has been described and a new X-linked form of PCD has recently been identified.290 There are at least 39 genes known to cause PCD, with additional candidate genes identified in animal models. The number of PCD-causing genes that can also cause isolated congenital HD is unknown, but recent work shows that predicted damaging variants are found in genes required for ciliary motility and function in patients with congenital HD.14
Cardiovascular Genotype/Phenotype Correlations
Absence of cilia motility in the setting of otherwise normal sensation and signal propagation results in random LR asymmetry: random movement of extraembryonic fluid is still able to trigger a “left identity” signal that is randomly distributed between the anatomic right and left side of the embryo. This leads to the characteristic phenotype observed in the setting of PCD caused by ciliary motility components such as the axonemal dynein DNAH5, DNAH11, and the dynein assembly factor DNAI1. Patients with PCD pathogenic variants most commonly present with randomization of situs (resulting in situs inversus or situs solitus) and only rarely with heterotaxy.288
Syndromic Sensory Ciliopathies
The sensory ciliopathies are a group of genetically and phenotypically heterogeneous disorders caused by abnormalities in the sensory or signaling functions of cilia. They are inherited in an autosomal dominant, autosomal recessive (most common), or X-linked pattern. Organs most commonly affected are those in which nonmotile sensory cilia play important roles, such as the eyes, ears, skeleton, brain, kidney, and liver.291–296 Abnormal signal transduction via hedgehog, Hippo, and Wnt pathways underlies a variety of patterning defects and congenital anomalies identified in these syndromes, although other developmental pathways are also involved.
Common Features
Eye and Ear
Retinitis pigmentosa and cone-rod dystrophy are common eye findings. Sensorineural hearing loss occurs in a variety of ciliopathies.
Central Nervous System
Structural defects have been described, including the classic brain stem malformations (molar tooth sign) in Joubert syndrome, Dandy-Walker malformation, and neural tube defects, including encephalocele, holoprosencephaly, and agenesis of the corpus callosum.
Growth and Endocrine
Obesity is seen as a result of abnormal energy homeostasis/hypothalamic dysfunction and is common in Bardet-Biedl, Alstrom, and Carpenter syndromes. Diabetes mellitus is the most common endocrine abnormality.
Skeletal
Dwarfism, thoracic dysplasia, short limbs, and polydactyly characterize a variety of ciliopathies, some of which are perinatal lethal. Four groups with major skeletal involvement include the cranioectodermal dysplasias, the short-rib thoracic dysplasias, EVC, and the oral-facialdigital syndromes.
Hepatic
Prototypical features are hepatic fibrosis and hepatic cysts. Liver disease in ciliopathies is not a primary disease of the hepatocytes but rather is a developmental defect of the portobiliary system.
Renal
Polycystic kidneys are common features of many ciliopathies. Nephronophthisis is characterized by renal cysts, tubular basement membrane disruption, and tubulointerstitial fibrosis.
Skin
Ectodermal dysplasia affects hair, skin, teeth, and nails.
Cardiac Features
Congenital HDs and laterality defects occur in a subset of sensory ciliopathies (Tables 6 and 7). In addition to situs abnormalities of the heart, atrioventricular canal defects, septal defects, and valve defects can occur with reduced penetrance. The mechanistic basis of the congenital HDs has not yet been established for each syndrome. Findings of laterality defects should reflect disruption of LRO function, whereas isolated congenital HDs might result from abnormalities of cilia within the heart. Cardiomyopathy is identified in Alstrom syndrome.
Table 7.
The Relationship of Ciliary Components Shown in Figure 1 and the Associated Congenital HD
| Gene | Molecular Function | Cardiac Phenotype | Reference | |
|---|---|---|---|---|
| LRO formation | GDF1 | LRO formation | RAI, congenital HD | 297 |
| GALNT11 | LRO formation | HTX | 271 | |
| Centriole | MKKS | Centriole | Congenital HD | 258 |
| NEK2 | Centriole | HTX | 271 | |
| Transition zone/inversion compartment | NPHP2 | SI, TGA | 298–300 | |
| NPHP3 | VSD, HTX | 301, 302 | ||
| ANKS6 | SI, congenital HD | 303 | ||
| NEK8 | Congenital HD, HTX | 304 | ||
| Ciliary motility | DNAAF3 | Dynein assembly | SI | 305 |
| CCDC39 | Dynein assembly | SI, HTX | 306 | |
| CCDC40 | Dynein assembly | SI | 307 | |
| CCDC103 | Dynein assembly | S1, HTX | 308 | |
| HEATR2 | Dynein assembly | SI, HTX, congenital HD | 309 | |
| ARMC4 | Dynein assembly | SI | 310 | |
| DYX1C1 | Dynein assembly | SI, HTX, congenital HD | 311 | |
| C210RF59 | Dynein assembly | SI, HTX | 312 | |
| SPAGI | Dynein assembly | SI | 313 | |
| CCDC151 | Dynein assembly | SI, HTX, congenital HD | 314 | |
| PIHID3 | Dynein assembly | SI | 290 | |
| DNAAF1 | Dynein assembly | SI | 315, 316 | |
| DNAAF2 | Dynein assembly | SI | 317 | |
| DNAH5 | Dynein outer arm | SI, HTX, congenital HD | 288, 318 | |
| TXNDC3 | Dynein outer arm | SI, HTX | 319 | |
| DNAH11 | Dynein outer arm | SI | 320 | |
| DNA11 | Dynein intermediate chain | SI, HTX, congenital HD | 321, 322 | |
| DNALI | Dynein light chain | SI | 288, 323, 324 | |
| CCDC114 | Dynein docking | SI, HTX, congenital HD | 325 | |
| TTC25 | Dynein docking | SI | 326 | |
| LRRC6 | Dynein transcription | SI | 320 | |
| ZMYND10 | Dynein transcription | SI | 327 | |
| CCDC11 | Centriole | SI, HTX | 328, 329 | |
| 330 | ||||
| Polycystin complex | PKD2 | SI | 331 | |
| PKD1L1 | HTX | 332 | ||
| Other | EVC | Hedgehog signaling | AVC | 123 |
| EVC2 | Hedgehog signaling | AVC | 123 | |
| MKS1 | Hedgehog signaling | AVC | 250 | |
| DCHS1 | Mitral prolapse | 333 | ||
AVC indicates atrioventricular canal; HD, heart disease; HTX, heterotaxy; LRO, left-right organizer; RAI, right atrial isomerism; SI, situs inversus; TGA, transposition of the great arteries; and VSD, ventricular septal defect.
Prevalence
The prevalence varies by syndrome subtype, but all syndromes are quite rare, with estimates ranging from 1:50 000 to 1:1 000 000. There are examples of founder effects, with the incidence of Meckel-Gruber as high as 1:9000 in some populations (Finnish).292
Molecular Genetics
As seen in Table 7, several of the disorders have allelic overlap. For example, Joubert syndrome and Meckel-Gruber syndrome share many of the same genetic causes. More than 140 genes have been established as causative for syndromic sensory ciliopathies, along with >200 additional candidate genes.293 Most cases are caused by loss of gene function.
Genotype-Phenotype Correlations
How the same allele causes disparate phenotypes for many of the ciliopathies is not fully apparent. For the multisystem disorders, specific organ involvement or severity can correlate with the particular gene involved. For example, in a patient with Joubert syndrome, pathogenic variants in NPHP1, a gene that can also cause nephronophthisis, are more likely to be found in association with renal involvement. Modifier alleles and digenic inheritance have been described, and these presumably affect phenotypic presentation. In some cases, the variant type (eg, loss of function versus missense) will dictate presentation. Genotype-phenotype correlations have not been described for cardiac presentations.
Isolated Congenital HD Related to Ciliary Defects
General
Studies of the mouse model predict that ciliary defects will be identified that cause recessively inherited isolated congenital HD in the absence of a syndromic ciliopathy or PCD,251 and recent studies show an over-representation of rare, predicted damaging variants in recessive genes in patients with isolated congenital HD versus control subjects.14
Cardiac Features
Recent work on large cohorts of patients with severe mitral valve prolapse identified that mutations affecting DCHS1 are linked to congenital mitral valve defects,333 and DCHS1 localizes to the base of the ciliary apparatus.334 In addition, patients with situs inversus with or without TGA have been identified with a deletion that affects NPHP2 (inversin), and mutations that affect GDF1 have been associated with RAI (Table 6). In the future, genomic analyses of large cohorts of congenital HD will likely yield additional cilia genes with a role in congenital HD and begin to establish more focused genotype-phenotype correlations.
Clinical Genetic Testing in Ciliopathies
Clinical genetic testing is directed on the basis of the differential established through medical history, including family history, and physical examination. All patients with heterotaxy should have CMA because of associations with chromosome abnormalities and pathogenic CNVs. In addition, strong consideration should be given to ZIC3 testing, particularly in males with heterotaxy. Recurrence risk estimates are substantially impacted by test results. Although additional studies are necessary to further establish the prevalence of PCD in patients with heterotaxy, consideration should be given to evaluation for PCD, because respiratory and pulmonary management could be optimized to improve the higher than expected surgical morbidity and mortality in this patient group.335 Genetic testing for PCD is available through multigene panels. Concern for syndromic ciliopathies should prompt molecular testing for these disorders via ciliopathy panels or exome sequencing.
The Impact of Ciliopathy Pathologic Variants on Clinical Outcomes in Patients With Congenital HD
One of the challenging aspects of caring for patients requiring surgical repair of congenital HD is the variation in postoperative outcomes even for patients with anatomically and physiologically identical congenital HD. Respiratory complications are one of the most important modulators of postoperative outcome that can be influenced by genetic pathogenesis of the congenital HD. If patients at increased risk for respiratory and other complications can be identified preoperatively, it might be possible to modify their care and improve clinical outcomes. Pathological variants in ciliary genes are known to cause heterotaxy, some types of nonheterotaxy congenital HD,251,288 and PCD.286,336 Poor mucociliary clearance leads to infection and inflammation that damage the airway, and it is especially important to note that patients with ciliary dysfunction depend entirely on cough for mucociliary clearance, a function that is compromised in patients on mechanical ventilatory support, such as postoperative congenital HD patients. With this in mind, it is not surprising that patients with congenital HD, heterotaxy, and associated airway ciliary dysfunction have a higher rate of respiratory complication postoperatively than similar patients without airway ciliary dysfunction.335 These finding suggest that prospective knowledge of which patients might have airway ciliary dysfunction could improve postoperative outcome by tailored modifications to their respiratory care. In addition, immotile cilia are found in the kidney and brain, and it is possible that cilial defects impact the kidney’s response to injury,337 neurodevelopment,338,339 and metabolic function.339
NONSYNDROMIC CONGENITAL HD ATTRIBUTABLE TO SINGLE-GENE VARIATION
As discussed earlier, numerous genes have been implicated in the pathogenesis of congenital HD when it occurs in the setting of a genetic syndrome, but the identification of the genetic contributors of nonsyndromic congenital HD has proved to be more challenging. Although initial insights were based on studies of large, multigenerational kindreds in which multiple family members were affected with a cardiac malformation, these families are relatively uncommon, and the congenital HD is often less severe. With the elucidation of an increasing number of genes involved in the molecular regulation of cardiac morphogenesis by either a better understanding of cardiac developmental regulation through model organism studies or through identification of candidate cardiac genes within microdeletions/microduplications in individuals with congenital HD, there has been a relative explosion of rare sequence variants in these heart development genes identified in children with congenital HD. Establishing disease causality, especially of a specific variant, remains a challenge. These genes mostly encode transcription factors, signaling molecules, or structural proteins important in cardiac development, structure, and function. The genes most strongly associated with congenital HD are briefly discussed in Transcription Factors, Cell Signaling and Adhesion Molecules, and Structural Proteins. Detailed information about the associated cardiac phenotypes and references to supporting studies are reviewed in Anderson et al340 and Fahed et al341 and are provided in Table 8. In addition to these “gold standard” congenital HD genes, there are several hundred genes with purported roles in cardiac development and congenital HD, and advances in genomic technology over the past 3 years have enabled us to unravel the genomic architecture of isolated or nonsyndromic congenital HD at a rapid pace. Many of the congenital HD genes identified to date can be assigned to one of the following functional categories.
Table 8.
Disease Genes for Nonsyndromic Congenital Cardiovascular Disease
| Gene | Cardiovascular Malformation | Nonsyndromic (NS) or Syndromic (S) | Gene MIM | References |
|---|---|---|---|---|
| Transcription factors | ||||
| CITED2 | ASD, VSD | NS | 602937 | 342 |
| GATA4 | ASD, VSD, AVSD, PVS, TOF | NS | 600576 | 113, 343–350 |
| GATA6 | PTA, TOF | NS | 601656 | 351–355 |
| MED13L | TGA | NS | 608771 | 356 |
| NR2F2 | AVSD, AS, CoA, VSD, HLHS, TOF | NS | 107773 | 357 |
| NKX2–5 | ASD, atrioventricular conduction delay, TOF, HLHS | NS | 600584 | 358–363 |
| NKX2.6 | PTA | NS | 611770 | 364, 365 |
| TBX20 | ASD, VSD, MS, DCM | NS | 606061 | 366–369 |
| ZFPM2/FOG2 | TOF, DORV | NS | 603693 | 370–372 |
| Cell signaling and adhesion proteins | ||||
| ACVR1/ALK2 | AVSD | NS | 102576 | 373 |
| CRELD1 | ASD, AVSD | NS | 607170 | 374–376 |
| GJA1 | HLHS, VSD, PA | S (oculodentodigital dysplasia) and NS | 121014 | 377–379 |
| JAG1 | TOF, PVS, PAS | S (Alagille syndrome) and NS | 601920 | 380-382 |
| NOTCH1 | BAV, AS, HLHS, TOF, PVS | S (Adams-Oliver syndrome) and NS | 190198 | 141, 185, 383–385 |
| PDGFRA | TAPVR | NS | 173490 | 386 |
| SMAD6 | BAV, CoA, AS | NS | 602931 | 387 |
| TAB2 | BAV, AS, TOF | NS | 605101 | 388 |
| Structural proteins | ||||
| ACTC1 | ASD, HCM, DCM, LVNC | NS | 102540 | 389, 390 |
| DCHS1 | MVP | NS | 603057 | 333 |
| ELN | SVAS | S (Williams-Beuren syndrome) and NS | 130160 | 80, 391–393 |
| MYH6 | ASD, HCM, DCM | NS | 160710 | 394–396 |
| MYH7 | Ebstein’s anomaly, LVNC, HCM, DCM | NS | 160760 | 397, 398 |
| MYH11 | PDA, TAA | NS | 160745 | 399, 400 |
AS indicates aortic valve stenosis; ASD, atrial septal defect; AVSD, atrioventricular septal defect; BAV, bicuspid aortic valve; CoA, coarctation of aorta; DCM, dilated cardiomyopathy; DORV, double-outlet right ventricle; HCM, hypertrophic cardiomyopathy; HLHS, hypoplastic left heart syndrome; LVNC, left ventricular noncompaction cardiomyopathy; MIM, Mendelian Inheritance in Man; MS, mitral valve stenosis; MVP, mitral valve prolapse; NS, nonsyndromic; PA, pulmonary atresia; PAS, pulmonary artery stenosis; PDA, patent ductus arteriosus; PS, pulmonic valve stenosis; PTA, persistent truncus arteriosus; PVS, pulmonary vein stenosis; S, syndromic; SVAS, supravalvar aortic stenosis; TAA, thoracic aortic aneurysm; TAPVR, total anomalous pulmonary venous return; TGA, transposition of great arteries; TOF, tetralogy of Fallot; and VSD, ventricular septal defect.
Transcription Factors
Initial insights into the genetic pathogenesis of non-syndromic congenital HD were based on the discovery of disease-causing sequence variants in critical cardiac transcription factors identified as important for normal heart development in multiple animal model systems.401 Mutations in the transcription factor gene NKX2–5 were reported in multiple familial and sporadic cases of congenital HD, with the first report in 1998 in 4 kindreds with autosomal dominant congenital HD.358 Familial ASD with atrioventricular conduction abnormalities is the primary cardiac phenotype associated with NKX2–5 mutations, but additional phenotypes include VSD, tetralogy of Fallot, subvalvar aortic stenosis, pulmonary atresia, and mitral valve abnormalities (reviewed in Stallmeyer et al362 and Ellesøe et al363) These discoveries have been supported by the reports of similar cardiac phenotypes in mouse models harboring mutations in Nkx2.5.402–404
A similar approach identified heterozygous mutations in GATA4, a gene encoding another important cardiac transcription factor, in familial congenital HD.113 The predominant and most penetrant phenotype is secundum ASD but can include VSD, PVS, AVSD, and tetralogy of Fallot (reviewed in Prendiville et al405). Evidence supporting these genetic associations has come from analysis of mice haploinsufficient for Gata4 or harboring disease-causing Gata4 mutations. These mouse models have replicated human disease phenotypes.347,406,407 Additionally, another member of the GATA family of transcription factors, GATA6, has been implicated in sporadic and familial congenital HD, with lesions including persistent truncus arteriosus, PVS, ASD, and PDA.351 The link between GATA6 mutations and human disease was expanded by the identification of de novo inactivating mutations in GATA6 in ≈50% (15 of 27) of individuals with pancreatic agenesis, among whom 90% had congenital HD.354
Another important transcription factor family linked to congenital HD is the Tbox family. Besides the association with syndromic congenital HD (TBX5 with HOS, TBX1 with cardiac lesions in 22q11.2DS), mutations in TBX5 and TBX1 might be responsible for nonsyndromic congenital HD.408,409 In addition, mutations in another family member, TBX20, were identified in 2 families with cardiac septation defects, mitral valve stenosis, and dilated cardiomyopathy.366 Mutations in TBX20 have subsequently been described in other cardiac malformations, including tetralogy of Fallot, truncus arteriosus, and double-outlet right ventricle. Other cardiac transcription factors implicated in congenital HD pathogenesis are listed in Table 8.369
Cell Signaling and Adhesion Molecules
Although mutations in the Notch signaling pathway are a cause of ALGS as well as AOS (both discussed previously),141 this pathway is also implicated in nonsyndromic congenital HD. Garg et al reported a multigeneration family with autosomal dominant cardiovascular disease in which 9 members had aortic valve disease, primarily BAV, but also 1 member with tetralogy of Fallot.185 Since then, mutations in NOTCH1 have been implicated in familial nonsyndromic congenital HD, predominantly affecting the cardiac outflow tract and semilunar valves.384 A recent report using clinical exome sequencing in a patient with HLHS identified a NOTCH1 mutation although affected paternal family members had mostly right-sided heart lesions,385 which suggests that the phenotype might not be limited to the left-sided semilunar valve.383 Pathological sequence variants in other cardiac developmental signaling pathway genes have also been identified in patients with congenital HD (Table 8).
Structural Proteins
Mutations in sarcomeric genes, known to cause cardiomyopathy, have also been reported in congenital HD, for example, α-cardiac actin (ACTC1) and myosin heavy chain 6 (MYH6) mutations in familial ASD,389,394 β-myosin heavy chain (MYH7) mutations in Ebstein’s anomaly of the tricuspid valve and left ventricular noncompaction cardiomyopathy,397,398 and myosin heavy chain 11 (MYH11) mutations in PDA, usually in association with thoracic aortic aneurysms.399,400 As discussed, elastin (ELN) haploinsufficiency causes syndromic congenital HD in WS, whereas point mutations in ELN cause supravalvular aortic stenosis and other large artery stenoses without a syndromic phenotype.392,393
Recent Insights Into the Complex Genetic Architecture of Nonsyndromic Congenital HD
Given the large number of genes that contribute to congenital HD, NGS is being increasingly used in both research and clinical settings in congenital HD patients. In one of the earliest studies led by the Pediatric Cardiac Genomics Consortium that used WES in 362 severe congenital HD cases (parent-offspring trios), congenital HD cases showed a significant excess of proteinaltering de novo sequence variants in genes expressed in the developing heart, with particular enrichment of histone-modifying genes that regulate expression of key developmental genes.275 Of note, the involvement of histone modifier mutations in several forms of congenital HD suggests that epigenetic modifications more broadly (eg, ones that alter DNA methylation or noncoding RNAs) might prove relevant for congenital HD pathogenesis.275,410 De novo point variants in several hundred genes together contributed to ≈10% of severe congenital HD. Of note, the vast majority of variants were “private” in that they were not identified in more than 1 individual. The same group performed exome sequencing of 1213 congenital HD parent-offspring trios and identified an excess of protein-damaging de novo variants in genes highly expressed in the developing heart and brain. These potentially disease-causing variants accounted for 20% of patients with syndromic congenital HD, that is, congenital HD with neurodevelopmental disabilities and extracardiac congenital anomalies, but only 2% of patients with isolated congenital HD. These findings revealed shared genetic contributions to congenital HD, neurodevelopment, and extracardiac anomalies.274
A large international study using WES of 1891 probands found a significant enrichment of de novo protein-truncating variants but not inherited protein-truncating variants in known congenital HD genes in syndromic congenital HD. Conversely, in nonsyndromic congenital HD, there was a significant enrichment of protein-truncating variants inherited from unaffected parents in congenital HD genes. The study further identified 3 genome-wide significant syndromic congenital HD disorders caused by de novo variants in CHD4, CDK13, and PRKD1. This study underscored the distinct genetic architectures of syndromic versus nonsyndromic congenital HD.411
Although these studies involved heterogeneous cohorts of congenital HD, WES of a targeted cohort of nonsyndromic AVSD cases provided important insights into congenital HD genetic architecture, including the identification of NR2F2, a novel potentially causal gene in patients with nonsyndromic AVSD.357 Because NR2F2 mutations explained <5% of AVSDs, the investigators also performed a candidate gene search of 112 potential AVSD-associated genes and found a significant enrichment of rare, damaging variants in 6 genes, 3 of which were known syndrome-associated genes (NIPBL, CHD7, and CEP152).412 This highlighted that syndrome-associated genes can contribute to nonsyndromic congenital HD. A follow-up study identified an even larger gene set enriched for potential disease-contributing variants compared with control subjects, with 32% of trios carrying at least 1 putatively disease-associated variant, either inherited or de novo, across a heterogeneous group of loci.413 Together, these studies revealed the complex and oligogenic origins of AVSDs, as well as the ability of NGS to unravel some of this complexity.
Finally, a recent study using mouse forward genetics identified sequence variants in novel genes not previously associated with congenital HD, Sap130 and Pcdha9, as being digenic causes of HLHS. Sap130 mediated left ventricular hypoplasia, whereas Pcdha9 increased penetrance of aortic valve abnormalities. The investigators also identified a subject with HLHS with both SAP130 and PCDHA13 sequence variants.414 This study highlighted that complex congenital HD can be caused by synergy between variants in multiple developmental genes rather than a single gene.
In summary, in recent years, NGS approaches in isolated congenital HD have revealed the following:
There are several hundred genes that either cause or contribute to congenital HD.275
Sequence variants in congenital HD genes can cause both sporadic and inherited congenital HD.
Sequence variants in congenital HD genes can cause both syndromic and nonsyndromic congenital HD, with strong association of de novo variants with syndromic CHD274 and of inherited variants with nonsyndromic congenital HD.411
There is phenotypic heterogeneity, with sequence variants in the same genes often associated with different cardiac phenotypes, not only between families but also within families. This discordance in phenotype among family members was further highlighted in a Danish national study in which only 50% of siblings had the same type of congenital HD as the proband.415
Family studies often show incomplete segregation even in familial congenital HD, with could be attributable in part to incomplete penetrance but could also be related to oligogenic origins of congenital HD.413 The occurrence of multiple variants in some patients might explain why some affected individuals have a more severe phenotype.414
Clinical Implications
The above findings have clinical implications. Although several laboratories offer congenital HD gene panels of various sizes for clinical testing, the relatively large numbers of genes involved and the role of novel and ultra-rare variants in causing rare disorders coupled with the oligogenic origins of some of the more complex congenital HDs suggest that a genome-wide search for congenital HD–associated variants might be cost-effective in the future as the accuracy of variant interpretation improves. Experience, challenges, and cost-effectiveness of clinical exome sequencing have been reported recently.385,400 Also, given the overlap in genes associated with syndromic and nonsyndromic congenital HD, it is important to continue medical follow-up of patients with nonsyndromic congenital HD caused by a syndrome-associated gene, because noncardiac findings can sometimes manifest later than cardiac findings Additional clinical implications of knowledge of genetic pathogenesis in screening, surveillance, and management of congenital HD have been discussed in detail in a recent American Heart Association scientific statement.416
FUNCTIONALITY OF CONGENITAL HD GENES
Widespread exome and genome sequencing of congenital HD patients is uncovering an ever-increasing number of candidate disease genes and disease-causing variants.274,417 These sequence variants and candidate disease genes need to be studied in model systems to rapidly and accurately determine which variants are responsible for congenital HD causation, to characterize pathogenic mechanisms, and to identify new candidate genes for evaluation in clinical studies. Several in vitro and in vivo model systems are available, each with its own strengths and weaknesses. In vivo animal models, including mammalian (eg, mouse), “other” vertebrate (eg, zebrafish, frog, and chick), and invertebrate (eg, fruit fly) organisms, allow evaluation of the impact of genetic perturbations on cardiac development and function within the context of an intact organism. Recently, in vitro strategies have been developed in cell and tissue engineered models that complement the animal models and facilitate mechanistic studies.418 In combination, these in vivo and in vitro model systems enable the elucidation of pathogenic mechanisms, the discovery of additional candidate congenital HD genes, and the development of novel, molecularly targeted therapeutic strategies.
Mouse Models
Because of the high degree of conservation between mouse and human cardiac development and the availability of well-established techniques for genetic manipulation, the mouse model has been used to study heart development for >25 years, resulting in an extensive knowledge base with bountiful reagents and resources. These key features have made the murine system the most widely studied animal model of cardiovascular development.
The mouse genome can be modified by many techniques. These can be grouped into methods that randomly insert DNA sequences into the genome (transgenesis) and those that modify an endogenous locus (targeted mutagenesis). Transgenesis, performed by introduction of foreign DNA (using a targeting vector) into a fertilized oocyte, is most commonly used to direct expression of a gene in an altered form or at an ectopic time, location, or level. The targeting vector used to modify the endogenous locus can be engineered to inactivate the gene (knockout), to introduce recombinase sites into the gene so that it can be conditionally inactivated by a second recombinase allele (eg, flank gene with loxP sites [floxed] that can be excised at a specific time in a specific tissue by Cre recombinase), or to modify the endogenous gene (knockin). More recently, nucleases that can be programmed to cut the genome at a single specific site (eg, CRISPR/Cas9) have expedited targeted mutagenesis by dramatically increasing the efficiency of site-directed mutagenesis.419
These techniques for modifying the mouse genome have been used to study cardiovascular development and disease in a number of ways.420 Transgenesis is often used for gain-of-function experiments, in which a promoter with specific spatiotemporal expression properties is used to drive a gene of interest. The opposite loss-of-function strategy is achieved by constitutive gene knockout or by excising an essential portion of a floxed gene of interest using Cre recombinase, expressed from a transgene or knocked into a second locus so that it is expressed in a known spatiotemporal domain. Gene knockout approaches have traditionally focused on coding regions. However, this strategy will also be useful to test the functional importance of conserved transcriptional regulatory elements that have been linked to congenital HD causation using high-throughput mapping technologies.421–424
Cre recombinase is also often used to dissect a cell’s developmental history, a technique known as genetic lineage tracing.425 Here, Cre recombination is used to activate expression of a reporter gene such as LacZ or GFP in a particular tissue beginning at a selected developmental stage. Because reporter activation involves modification of the genome, it is transmitted to all of the progeny of the Cre-expressing cells. Lineage tracing has been critical to deduce the developmental events that generate the heart, including the contributions of the second heart field, which adds cells onto the arterial and venous ends of the linear heart tube to form parts of the atria and most of the right ventricle and outflow tract,426 as well as the contribution of the dorsal mesenchymal protrusion to form portions of the atrioventricular septae at the crux of the heart.427,428 In spite of the similarities between mouse and human cardiac development, there also can be important differences. Because of practical considerations, congenital HD gene defects are often modeled in mice as homozygous gene knockouts, whereas most congenital HD mutations are heterozygous point or truncating mutations.274,417 These point mutations can result in partial gain or loss of function or could have dominant-negative activity that is imperfectly modeled by gene knockout. Biologically, gene dosage and redundancy are important factors that influence the expression of mutations, and these parameters often vary between species. For instance, haploinsufficiency of TBX1 in 22q11 deletion syndromes is an important contributor to congenital HD429; however, Tbx1 haploinsufficiency is well tolerated in mouse models, and a more severe reduction of Tbx1 dosage is required to produce cardiac defects.430 Genetic modifiers modulate the expression of gene mutations in human congenital HD.48 Exploration of genetic modifiers in mouse models can be productive405,431 but is rarely undertaken because these experiments are time and resource intensive. As a result of these technical and biological factors, mouse models often yield important principles and genetic pathways responsible for congenital HDs, but genotype-phenotype relationships can differ between the mouse and the human.
As noted above, cost and time are important considerations when developing mouse models of congenital HD. Creating a new mouse allele and characterizing it can take 6 to 12 months, and in models that require combining several different alleles, breeding mice to obtain the required genotype can be a critical practical bottleneck. Acquiring the correct mouse alleles for an experiment can also be time consuming and expensive. In some cases, these practical limitations can be circumvented through in vivo gene transfer and somatic mutagenesis.432 Adeno-associated virus has proven to be an extremely efficient method for postnatal gene transfer to cardiomyocytes, and adeno-associated virus can be combined with CRISPR/Cas9 to efficiently introduce somatic mutations into cardiomyocytes. Although it is possible to deliver adeno-associated virus to late-stage mouse embryos,433 unfortunately at the present time, adeno-associated virus transduction of mid-gestation mouse embryos and noncardiomyocytes (such as endothelial cells and valve cells) is inefficient and thus not applicable to many heart development studies.
Zebrafish and Other Vertebrate Models
The limitations of the mouse model have led to the use of alternative vertebrate models to study cardiovascular development. The zebrafish has become an attractive experimental model; the genes and signaling pathways involved in human cardiac development and responsible for human congenital cardiac defects are highly conserved in the zebrafish, and the zebrafish offers some important advantages for developmental studies. A key advantage of the zebrafish system over mice is that embryos are transparent and develop outside the body of the mother (ex utero), which permits the developing cardiovascular system to be imaged throughout the developmental process.434,435 One can also rapidly and economically generate genetically modified zebrafish models. Rapid screening of candidate congenital HD disease genes for essential functions in heart development can be performed with antisense strategies to diminish expression of specific genes beginning very early in development. Unfortunately, this approach, which uses stable antisense RNA constructs called morpholinos,436 can yield nonspecific morphological defects that can obscure gene function, requiring careful confirmation of observed phenotypes. Recent advances have enabled rapid and efficient stable gene targeting using CRISP-R/Cas9 approaches similar to those described above for mice.437 These approaches are more time consuming but have a lower level of nonspecific or off-target effects. One important consideration when performing targeted genetic modifications is that the zebrafish underwent a genome duplication event during evolution after divergence from its common ancestor with mammals.438 As a result, for many mammalian genes, zebrafish often have 2 different genetic loci encoding for slightly different versions of the same gene, both of which might need to be targeted to have the same developmental effect as targeting the single gene in other vertebrates.
One popular approach to verifying that newly identified variants are indeed pathogenic is to determine whether a full-length expression construct of the wild-type and mutated versions of the gene is capable of rescuing the phenotype of zebrafish that lack a functional copy of the gene. This can be readily accomplished by directly injecting capped mRNA into 2- to 4-cell-stage embryos, leading to widespread expression of wild-type or mutant transcripts of genes known or suspected to be involved in cardiac development. Furthermore, expression of a mutant form of the gene in a wild-type embryo can help rapidly validate gain-of-function variants that have a dominant-negative effect on heart development.
The ex utero development of zebrafish embryos also permits interventions that are not possible in mouse. Addition of agents to the aquatic environment of the embryo can be used to examine the teratogenic effects of environmental toxins439 or interrogate the developmental contributions of specific signaling pathways.440 The embryo can also be directly accessed, and laser energy can be used to activate a specific gene in a specific cell,441 photoconvert a green fluorescing cell to a red fluorescence (which allows examination of a particular cell with respect to the surrounding cells),442 or lesion a specifi tissue (to alter cardiovascular hemodynamics or ablate a specific group of cells).443 Transfer of cells from one very early-stage embryo to another can enable the examination of genetically modified cells when surrounded by normal cells and tissues. Each of these interventions has helped to examine specific aspects of cardiac development in a manner that would not be possible in a higher vertebrate model in which the embryo develops in utero.
A major limitation of the zebrafish model is that the zebrafish has a 2-chambered heart (1 atrium and 1 ventricle), which makes it unsuitable for examination of the developmental process of septation. However, genetic mutations that lead to septal defects in humans cause detectable cardiac phenotypes in zebrafish embryos, which means the zebrafish is still a useful screening tool to examine the pathogenicity of mutations that are suspected of causing septation defects in humans.
Other Models
Another vertebrate model system that has the benefit of developing ex utero, which enables the observation and manipulation of developmental processes, is the chick embryo. It has the additional benefit of having a 4-chambered heart that is much more similar to the human heart and can be used to study septation and other, more complex processes in cardiac morphogenesis. As with the zebrafish model, delivery of gene expression or antisense RNA constructs can be used to manipulate gene expression, allowing examination of gene functions and the developmental pathways. A strength of the chick model system is the ability to examine the effects of embryo manipulation on cardiac development. For instance, surgical interventions such as left atrial or vitelline vein ligation alter intracardiac flow patterns and result in abnormalities of cardiac morphogenesis,444,445 and ablation of specific developmental fields, such as the cardiac neural crest, allows determination of the contribution of those domains to the cardiac development. The combination of mechanical or pharmacological intervention with modification of gene expression can facilitate characterization of the effects of gene-environment interactions on heart development and is a particular strength of the chick embryo model system.
Other animal models that have been used to help characterize specific aspects of heart development include the frog (genus Xenopus), which has been very helpful in examining determination of “sidedness,”253 and the fruit fly (genus Drosophila), which has been effectively used to examine cardiomyocyte specification.446 Relatively high-throughput methods for cardiac gene knockdown and overexpression have been developed in Drosophila, which has enabled in vivo study of the functional significance of identified congenital HD mutations.447
In Vitro Model Systems
Although each animal model has its strengths in studying cardiac development and the pathological processes that cause human congenital cardiac defects, many lack the resolution to study the cellular interactions that are the foundation of organ development, and none can fully recapitulate the complex and unique genetic environment of a patient with congenital HD. Therefore, in vitro model systems, including those with the ability to directly examine the development of human patient–derived cells, have been developed to better understand cell-level interactions that guide heart development.
Although mammalian heart development cannot be fully recapitulated ex utero in culture systems, culture systems have been essential for mechanistic studies of cardiovascular development. Mammalian embryos remain viable and continue to develop for hours to days in culture environments, which permits key questions on lineage, mechanics, and molecular signaling to be studied. For example, whole embryo culture was used to dissect the interaction of vascular endothelial growth factor and calcineurin/NFAT (nuclear factor of activated T cells) signaling to regulate endocardial epithelial-mesenchymal transition.448 Culture of microdissected pharyngeal arch arteries revealed a cardiac progenitor niche in the second pharyngeal arch artery that promotes renewal and expansion of cardiac progenitor cells, perturbation of which can contribute to congenital HD.449 Atrial and ventricular explant culture has been used to demonstrate the origin of coronary endothelial cells from precursors on the atrial explant.450
Primary cell culture models have also been essential for studies of cardiovascular development. Primary fetal and neonatal cardiomyocytes can be maintained in culture for >1 week, and these systems have been essential for dissecting mechanisms that regulate cardiomyocyte survival, proliferation, and hypertrophy.451,452 Culture of epicardial cells and explants has also been critical to dissect the function of these cells in regulating growth of myocardium and coronary vasculature.453,454
Stem cell differentiation into cardiomyocytes has become a powerful method to study cardiogenesis and early heart development. Cardiac progenitor cells are scarce in developing embryos, which makes studies that require thousands to millions of cells difficult. In contrast, millions of these cells can be efficiently generated in stem cell differentiation cultures. This has allowed key regulatory steps of cardiogenesis and early heart development to be carefully dissected.455 Moreover, the availability of human pluripotent stem cells and protocols to efficiently direct their differentiation into cardiomyocytes has enabled the study of human cardiogenesis.456
The maturation of a number of transformative technologies has recently permitted the effect of gene mutations found in congenital HD patients to be studied using human “disease-in-a-dish” models. These technologies include (1) development of efficient methods for human stem cell differentiation; (2) reprogramming of somatic cells to induced pluripotent stem cells, which allows for the creation of patient-specific disease models; (3) facile genome editing, which permits rapid genetic manipulation of stem cells; and (4) development of bioengineered systems to build engineered heart tissues and assay them for relevant physiological parameters. This confluence of technical advances has allowed the impact of congenital HD mutations on cardiomyocyte gene expression, cardiac differentiation, and myocardial function to be evaluated in patient-specific genetic backgrounds, yielding new insights in disease pathogenesis.457–460 Although these advances have opened exciting new approaches to studying congenital HD pathogenesis, a number of challenges need to be overcome before they can realize their full potential. Among these are developing in vitro, stem cell–based models of cardiac morphogenesis; enhancing directed differentiation of stem cells to the full gamut of cardiac cell types; and improving the maturation of in vitro differentiated cardiomyocytes.
Although beyond the scope of this scientific statement, it is important to mention the growing role of in silico modeling of genetic variants to determine the potential effects of the variant on protein structure and function. Early algorithms relied almost entirely on the effect of the amino acid alteration on protein structure to determine whether the mutation was likely to be pathogenic. More recently, algorithms have incorporated degree of evolutionary conservation, population frequency, and, in some cases, more advanced functional modeling to determine potential pathogenicity of a novel genetic variant. Increasingly, advances in the understanding of the functions of and pathophysiological mechanisms associated with specific disease-causing variants (gained from the above in vivo and in vitro models) will allow more refined disease gene–specific mathematical modeling to assess potential pathogenicity of specific genetic variants, better characterization of disease mechanisms, and identification of structural domains suitable for pharmacological targeting.
In summary, technical advances and our expanding knowledge base have fueled dramatic advances in the in vitro and in vivo modeling of cardiac development. Continued expansion of these modeling capabilities will allow the rapid screening and adjudication of potential congenital HD disease genes and pathogenic variants and the examination of potential therapeutic approaches. Advanced bioinformatics analyses of data generated in the in vitro and in vivo developmental models and genomic/genetic/epigenetic data from patients with congenital HD have the potential to better define developmental pathways involved in cardiac development, to greatly improve our understanding of congenital HD pathogenesis, and to identify novel approaches for prevention and treatment.
ETHICAL CONSIDERATIONS
As noted above, genetic testing for congenital HD has increased over the past 10 years94,461 and is particularly helpful in diagnosing syndromes responsible for congenital HD and related noncardiac phenotypes that might require clinical management.1,341,461 Benefits of genetic testing for congenital HD include establishing a genetic diagnosis, facilitating presymptomatic screening of at-risk family members, enabling anticipatory management of congenital HD, directing clinical screening and management of associated noncardiac conditions, and accelerating the development of novel therapeutic targets.462 Because cardiac malformations constitute a significant portion of birth defects,1,341 knowledge of genetic predispositions to congenital HD could also be used by patients and their family members to support reproductive decisions and expectations, as well as to help guide prenatal and perinatal management. In addition, there is increasing evidence that certain types of genetic variations that cause congenital HD also affect clinical outcomes such as cognition, behavior, and motor skills (collectively termed neurodevelopmental performance).341 Although this is still an emerging field, it is possible that in the near future, genetic testing could help identify patients at risk for abnormalities of neurodevelopment and help target intervention strategies.
Despite these potential benefits, uncertainty about the clinical significance of many genetic variants and the complexity of conveying this information present challenges. Sequencing has uncovered many more genetic associations with congenital HD,94 but variant interpretation is imprecise, and the interplay between genetic and environmental factors that contribute to congenital HD continues to be elusive.341,463,464
With NGS, there is also the possibility that genetic variants associated with congenital HD might be discovered incidentally when testing for an unrelated phenotype, or that clinically significant incidental findings unrelated to congenital HD could be detected when testing for congenital HD. In 2013, the American College of Medical Genetics and Genomics (ACMG) recommended that certain clinically actionable secondary findings, including a number of cardiac-related variants, such as Ehlers-Danlos syndrome, familial thoracic aortic aneurysms, Marfan syndrome, and HCM, ought to be offered to all patients undergoing clinical WES or whole genome sequencing.465,466 As a result, noncardiac specialists could be challenged with communicating complex genetic findings to potentially unsuspecting patients. In these situations, referral to a cardiovascular geneticist is advisable.
On the flipside, when performing a genomic test for congenital HD, patients ought to be informed about the potential to discover incidental findings unrelated to congenital HD and should be given an opportunity to opt out of those results.466 This respects the patient’s autonomy and preserves the “right not to know.”467 Pretest and posttest counseling is also important to facilitate informed decision making, and it is essential that it be offered to patients and their families.
Additional challenges are raised when performing genetic testing in children with congenital HD. For many years, there has been a general consensus that children should only receive genetic testing that offers the potential for direct clinical benefit during childhood.1,468,469 The primary justifications for deferring testing for adult-onset conditions are respect for the child’s future autonomy and right to an open future470 and the potential psychosocial harm of knowing one’s genetic risk of disease. Targeted genetic testing is only plausible when there is a known family history of a mendelian condition that puts the child at risk for disease. In this situation, the affected family member already knows that he or she has, or is at risk for, the targeted genetic variant. In the context of genomic sequencing, however, a variant associated with an adult-onset condition that is discovered in a child could benefit parents or other family members, who would not otherwise know they are at risk.465,471 Thus, increased attention is now being paid to the potential benefit of testing to families, and some professional organizations and scholars have recommended that the presence of clinically significant genetic variants discovered incidentally during the course of clinical WES or whole genome sequencing be offered to patients, regardless of age and irrespective of age of onset.465,471,472 Comporting with standard ethical practice, children should be involved in the decision about whether to receive these incidental findings commensurate with their level of maturity and should provide assent whenever possible.473
Pretest genetic counseling for congenital HD should address the potential risks and benefits of testing, including the psychological and social impact of receiving a positive test result. Recent studies suggest that neither adults474 nor children475,476 experience significantly increased anxiety or distress after learning of their genetic status. However, the potential psychosocial impact of genetic testing can be greater when test results offer little therapeutic value and could include alterations of self-image and disruption in family relationships, including increased perceptions of child vulnerability that negatively impact development.468 These risks must be weighed against the potential psychological benefits of testing. For example, patients and families might experience relief from the reduction of uncertainty when a genetic cause is discovered.468 Additional research is needed to fully understand the impact of genetic testing for congenital HD on individuals, especially children, and their families, as well as to better appreciate how patients evaluate these trade-offs when deciding whether or not to undergo testing.
Even when the clinical and psychological benefits outweigh the risks, however, uptake of genetic testing for congenital HD can be limited if patients are concerned about the misuse of genetic information for discriminatory purposes. The 2008 Genetic Information Non-Discrimination Act (GINA) protects individuals in the United States from being discriminated against by health insurers and employers because of a genetic diagnosis.477 However, GINA does not prevent life, disability, or long-term care insurers from using genetic information to make coverage decisions. Although there have been very few documented cases of genetic discrimination, even before the passage of GINA,477 current regulatory uncertainty has the potential to negatively impact patients and families. A trustworthy system that provides robust protection against genetic discrimination is needed if we are to reap the benefits of advances in genetic testing for congenital HD that have been realized over the past 10 years.
GENETIC COUNSELING/RECURRENCE RISK/PRENATAL SCREENING
Genetic Counseling
The National Society of Genetic Counselors describes genetic counseling as the process of helping people understand and adapt to medical, psychological, and familial implications of genetic contributions to disease. This process integrates (1) interpretation of family and medical histories to assess the probability of disease occurrence or reoccurrence; (2) education about inheritance, testing, management, prevention, resources, and research; and (3) counseling to promote informed choices and adaptation to the risk or condition.478 A genetic counselor is a graduate-level trained healthcare professional who receives training in medical genetics, genomics, and counseling. In the United States and Canada, this terminal degree leads to certification through the American Board of Genetic Counseling after the individual passes a national certification examination. As of May 2017, 20 states issue and require licensure for genetic counselors to practice, and 3 states have licensure laws in progress. As the need for cardiovascular genetic counseling is increasingly recognized, genetic counseling training programs are developing curricula and clinical rotations to meet this growing need.415,479 Nevertheless, there are 3-fold more genetic counseling positions available than new graduates each year.
Genetic counselors skilled in cardiovascular genetics have become an invaluable clinical asset, helping not only to provide accurate recurrence risks but also to obtain family and medical histories, facilitate appropriate genetic testing, interpret test results, make necessary subspecialty referrals, and provide attendant psychosocial support for patients and their families. Physicians with subspecialty training in medical genetics are trained in dysmorphology, metabolism, monogenic conditions, genomics, and diagnostic testing and are able to generate a differential, determine a diagnostic evaluation approach, and provide specific management and treatment recommendations for patient care. In addition, geneticists can evaluate family members for other syndromic features and facilitate appropriate genetic testing or referrals. Studies have shown that genetics consultation increases the diagnostic rate of genetic syndromes in infants in the cardiac intensive care unit, as well as in older children with congenital HD seen for follow-up in a cardiac neurodevelopmental clinic.480,481 Single-site studies have shown underutilization of cytogenetic testing in infants with congenital HD, but multisite studies to address genetic testing practices have not been performed.482 Carey et al47 found that pathogenic CNVs are identified in >10% of single-ventricle forms of congenital HD and that patients with these cytogenetic abnormalities have more adverse outcomes. Dysmorphology evaluation is challenging in infants, and expanded testing identifies abnormalities missed even by trained dysmorphologists.47 These findings support a more comprehensive, standardized approach to genetic testing in infants with congenital HD. Algorithms have been proposed based on expert recommendation; further evidence-based investigation is necessary.13,483 Table 9 highlights indications for genetics involvement in patients with congenital HD.
Table 9.
Indications for Consultation With Genetics Professionals
| Reason for Referral | Examples/Features | Care Provider |
|---|---|---|
| Genetic testing for known familial variant | Facilitation of genetic testing for infant born to a parent with long-QT syndrome | Genetic counselor Geneticist |
| Pretest or posttest genetic counseling | Provision of educational resources and anticipatory guidance after a positive genetic test result | Genetic counselor Geneticist |
| Preconception or prenatal genetic counseling regarding recurrence risk | Parent with congenital HD interested in discussing recurrence risk for offspring before pursuing pregnancy | Genetic counselor |
| Prenatal genetic counseling regarding fetal anomaly | Discussion of prenatal genetic testing options for fetus with congenital HD | Genetic counselor |
| Family history of congenital HD, other malformations, learning disability, or multiple miscarriages | Three generations with AVSD | Genetic counselor Geneticist |
| Isolated congenital HD highly associated with specific syndromes | Interrupted aortic arch, truncus arteriosus, etc | Genetic counselor Geneticist |
| Suspicion of an underlying genetic syndrome | Intellectual disability; learning disability; autism; other cognitive impairment Dysmorphic features Short stature Congenital anomalies Endocrine abnormalities Sensory deficits such as hearing loss or visual impairment Neurological deficits | Genetic counselor Geneticist |
AVSD indicates atrioventricular septal defect; and HD, heart disease.
Genetic counseling services are valued by families.25,484 In the prenatal setting, cardiovascular genetic counseling is important for conveying information about the use and limitations of genetic testing and for providing psychosocial support to the patient and family.485,486 Recent surveys of adult congenital HD populations have demonstrated that a majority of patients lack accurate understanding of their individual recurrence risk but that provision and recall of genetic information can be significantly improved by incorporating genetics providers into routine cardiovascular care.484,487 In children, access to genetic services plays an important role in improving diagnostic yield, addressing ongoing health supervision needs of patients with genetic syndromes, and ensuring appropriate subspecialist referral.481 Unfortunately, the shortage of both geneticists and genetic counselors limits more widespread integration of services within cardiology. Telemedicine services are emerging in response to this need. Many centers are developing triage algorithms and testing new counseling models. Genetic assistants are being piloted to augment genetic counselor functions and expand capacity. Continued integration of genetic evaluation and genetic counseling are important components for improving utilization of increasingly comprehensive and affordable genetic services. Furthermore, it is becoming increasingly important that practitioners in the care of patients with congenital HD develop a level of comfort and expertise in genetic concepts and terminology. With that in mind, the American Heart Association recently published a scientific statement on enhancing provider literacy in cardiovascular genetics.415
Recurrence Risk
On the basis of epidemiological studies such as the Baltimore-Washington Infant Study and the Danish national epidemiologic study, syndromic congenital HDs are thought to constitute at least 25% of all congenital HDs.273,488,489 Identifying the underlying cause of congenital HD in these cases is important for medical management, surveillance, and communication of reproductive risks necessary for family planning. The distinction between syndromic and nonsyndromic, or isolated, congenital HD can be subtle. Technological advancements in genetic testing have increased the diagnostic yield. Studies of patients with congenital HD do not always apply the same criteria to distinguish syndromic from nonsyndromic cases, and the age of patient evaluation influences assessment.
In general, recurrence estimates are more precise for syndromic than for isolated congenital HDs, because genes and associated inheritance patterns for many congenital HD–associated monogenic conditions are already known. Importantly, not all patients with a particular syndrome will present with structural heart defects, and the proportion who do can vary considerably depending on the specific diagnosis.13 The presence or severity of a congenital HD in a parent is often not predictive of the risk for offspring. The likelihood of affected individuals reaching reproductive age or having children (reproductive fitness) is related to the new mutation rate that is a common cause of syndromic congenital HDs. As a result, some genetic syndromes that are highly penetrant for congenital HD contribute less to the congenital HD burden in the next generation than is the case for patients with isolated congenital HD or less severe lesions. Epidemiological studies can underestimate the number of familial cases because of the high rate of miscarriages of fetuses with congenital HDs and reproductive decisions to limit future pregnancies in families with a child with a congenital HD.462
As genetic testing technologies have evolved to offer higher resolution and higher diagnostic yields than those provided by conventional chromosomal analyses, CNVs have emerged as important causes of both syndromic and nonsyndromic congenital HDs. Moreover, an increasing recognition of contributing environmental490 and epigenetic factors has revealed a previously unanticipated breadth to congenital HD pathogenesis.13 Although all mendelian inheritance patterns have been identified in families with congenital HDs, the empiric sibling or offspring recurrence risk across all types of congenital HDs of 1% to 4% suggests that the majority of congenital HDs have a multifactorial pathogenesis.491,492
The study of groups of embryologically related cardiac malformations has identified subclasses of congenital HDs with strong familial clustering in first-degree relatives, ranging from 3-fold to 80-fold compared with the prevalence in the population.273,491 Heritability rates of 70% to 90% support the strong genetic contribution for some types of congenital HDs.493–495 Three classes of defects with the highest relative risk of recurrence of the same heart defect phenotype are heterotaxy, with a relative risk of 79.1 (95% confidence interval, 32.9–190); right ventricular outflow tract defects, with a relative risk of 48.6 (95% confidence interval, 27.5–85.6); and left ventricular outflow tract obstructive defects, with a relative risk of 12.9 (95% confidence interval, 7.48–22.2).273 These findings are important because they alter information on recurrence risk based on congenital HD subtype. In the case of left ventricular outflow tract obstructive defect, it also has implications for cardiac screening in family members. Not all families show evidence of similar types of congenital HDs, and familial clustering of discordant congenital HDs has also been documented, which suggests that common genetic pathways might underlie a spectrum of CHDs496 (reviewed in Landis and Ware462). Because congenital HDs are so common, the majority of cases occur in individuals without a family history despite high heritability. Although the incidence of congenital HDs appears to be similar in most populations, there are some specific types of congenital HD that show important differences.494,497,498 In addition, there is an increased rate of congenital HDs in populations with increased consanguinity, often attributed to autosomal recessive variants.462 Studies have examined rates of recurrence among first-degree relatives of patients with isolated congenital HDs and collectively suggest an overall risk of 5% to 10% for any congenital HD when either 1 parent or >2 siblings are affected499–501 or ≈3% with 1 affected child (Table 10; reviewed in Cowan and Ware13). Risk estimates for individual defects vary but are generally estimated in the range of 2% to 6%, with higher risk afforded to children of affected mothers (Table 10).13 These figures are low relative to congenital HDs with demonstrable monogenic inheritance but can still have potentially important implications, particularly with respect to future reproductive decision making and prospective screening of presumably unaffected family members.13 Family history of congenital HD remains one of the most consistently identified risk factors for identifying congenital HD prenatally.
Table 10.
Recurrence Risks for Isolated (Nonsyndromic) Congenital HDs
| Defect | Father Affected, % | Mother Affected, % | 1 Sibling Affected, % | 2 Siblings Affected, % |
|---|---|---|---|---|
| ASD | 1.5–3.5 | 4–6 | 2.5–3 | 8 |
| AVSD | 1–4.5 | 11.5–14 | 3–4 | 10 |
| VSD | 2–3.5 | 6–10 | 3 | 10 |
| AS | 3–4 | 8–18 | 2 | 6 |
| PVS | 2–3.5 | 4–6.5 | 2 | 6 |
| TOF | 1.5 | 2–2.5 | 2.5–3 | 8 |
| CoA | 2–3 | 4–6.5 | 2 | 6 |
| PDA | 2–2.5 | 3.5–4 | 3 | 10 |
| HLHS | 21495 | 2–9* | 6 | |
| TGA | 2502 | 1.5 | 5 | |
| L-TGA | 3–5 | 5–6 | NR | |
| EA | NR | 6502 | 1 | 3 |
| TrA | NR | NR | 1 | 3 |
| TA | NR | NR | 1 | 3 |
| PA | NR | NR | 1 | 3 |
Data from references 499–501 except where otherwise noted. Merged cells indicate recurrence when 1 parent is affected, irrespective of sex, and are used in the absence of sex-stratified risks. AS indicates aortic stenosis; ASD, atrial septal defect; AVSD, atrioventricular septal defect; CoA, coarctation of the aorta; EA, Ebstein’s anomaly; HD, heart disease; HLHS, hypoplastic left heart syndrome; L-TGA, congenitally corrected transposition of the great arteries; NR, not reported/insufficient data; PA, pulmonary atresia; PDA, patent ductus arteriosus; PVS, pulmonary valve stenosis; TA, tricuspid atresia; TGA, d-transposition of the great arteries; TOF, tetralogy of Fallot; TrA, truncus arteriosus; and VSD, ventricular septal defect.
Eight percent recurrence risk for HLHS; up to 22% recurrence risk for any congenital HD.495
Reprinted from Cowan and Ware13 with permission from Elsevier. Copyright © 2015, Elsevier Inc.
Preimplantation Genetic Diagnosis
Preimplantation genetic diagnosis is an assisted reproductive technology that allows screening for a genetic condition after in vitro fertilization and before implantation. Preimplantation genetic diagnosis can be used in couples at risk for passing on a genetic condition, including carriers of X-linked disorders, single-gene disorders, and chromosomal disorders.503,504 Prenatal genetic counselors provide information on risks and benefits of the procedure and work together with reproductive endocrinologists. Preimplantation genetic diagnosis has been used successfully in >100 genetic conditions, including inherited cardiac conditions such as Marfan syndrome, HCM, dilated cardiomyopathy, and muscular dystrophies.505 Preimplantation genetic diagnosis requires a clear understanding of the cause of a genetic condition within a family.
Prenatal Screening
Until 2011, noninvasive prenatal screening consisted mainly of measurements of maternal serum analytes and ultrasonography. These tests have a false-positive rate of 5% and detection rates of 50% to 95%.506 These techniques were used to provide families with information to optimize their pregnancy outcomes. In 2011, fcfDNA screening (also referred to as noninvasive prenatal testing, NIPT, or noninvasive prenatal diagnostic screening) became clinically available.507 This new testing uses bioinformatics algorithms and NGS of fetal DNA fragments present in maternal serum to estimate the probability of chromosome aneuploidy in the fetus. The ACMG has provided guidelines for the conditions for use of fcfDNA screening for aneuploidy.506 These include providing up-to-date genetic counseling concerning the new technique so that families can select diagnostic or screening options according to their personal goals. The ACMG recommends informing all pregnant women that fcfDNA screening is the most sensitive noninvasive screening for aneuploidies such as trisomy 21, trisomy 18, and trisomy 13. One review analysis, published in 2016, found the pooled sensitivities for fcfDNA screening to be 99.3% for trisomy 21, 97.4% for trisomy 18, and 97.4% for trisomy 13.508 If a positive screen test result is obtained, then the couple should be offered diagnostic testing. Screening for other autosomal aneuploidies besides trisomy 21, 18, and 13 is not yet recommended. The ACMG guidelines recommend offering fcfDNA screening to high-risk families (those with advanced maternal age or fetal anomalies on ultrasound), as well as lower-risk families.
Expanded fcfDNA screening for sex chromosome anomalies and CNVs is also currently offered by some laboratories. fcfDNA screening for sex chromosome abnormalities is less accurate than autosomal aneuploidies because of the potential for maternal X-chromosome biological variation. Clinically significant CNVs are rare in the population, and the positive predictive value is much lower than for whole chromosome aneuploidy. Therefore, at this time, the ACMG guidelines only recommend providing information on the availability of expanded use of fcfDNA screening for sex chromosome abnormalities and CNVs. If fcfDNA screening should identify a CNV or sex chromosome abnormality, then invasive diagnostic testing by chorionic villus sampling or amniocentesis is recommended by the ACMG guidelines to confirm the diagnosis.
If fetal ultrasounds or echocardiograms are abnormal, the American College of Obstetricians and Gynecologists and the Society of Maternal Fetal Medicine recommend prenatal CMA if invasive prenatal diagnosis is performed. Informed consent and comprehensive pretest and posttest genetic counseling are necessary.509 Establishing a diagnosis before delivery can facilitate medical care plans.
Indications for Fetal Echocardiography
Fetal echocardiography is now widely used to detect, characterize, and help manage congenital cardiac malformations. Indications for performing a fetal echocardiogram have been formulated and were described in a recent American Heart Association scientific statement.510 In addition to the further evaluation of concerns raised by screening ultrasounds performed as part of standard obstetrical care, specific risk factors for congenital HDs, including those related to maternal health (eg, diabetes mellitus and autoimmune conditions), maternal drug or toxin exposure, abnormalities of umbilical-placental development (eg, single umbilical artery and monochorionic twinning), and known, suspected, or potentially heritable genetic conditions, have achieved sufficient Classification of Recommendations (Class) and Level of Evidence (Level) to warrant performance of a fetal echocardiogram. As it pertains to known, suspected, or potentially heritable genetic conditions, performance of fetal echocardiograms in pregnancies in which the mother, father, or sibling has a congenital cardiac defect have been assigned a Class I/Level B indication, which means that it should be performed and that evidence from limited studies is supportive. As might be expected, the strength of Classification of Recommendation is reduced in more distantly related family members: with congenital HD in a second-degree family member, a fetal echocardiogram may be considered (Class IIb); with the nearest relative(s) with congenital HD being a third-degree or more distant family member(s), a fetal echocardiogram is not recommended (Class III). Similarly, fetal echocardiograms should be performed in pregnancies in which there is a heritable condition in a first-degree family member that is associated with a risk of heart defects (such as NS) even if the affected relative does not have a heart defect. However, for heritable cardiac conditions with a later onset of manifestation (such as HCM, Marfan syndrome, or Loeys-Dietz syndrome), fetal echocardiography may not be necessary if screening obstetrical ultrasound does not demonstrate any abnormalities.
Demonstration of noncardiac abnormalities suggestive of a potential genetic syndrome, teratogen, or malformation sequence is also an important indication to perform a fetal echocardiogram. The risk of a concomitant congenital HD in the fetus with another anomaly varies, but abnormalities of the central nervous system (microcephaly, hydrocephaly, agenesis of the corpus callosum, or other structural abnormalities), gastrointestinal system/abdomen (esophageal or duodenal atresia, diaphragmatic hernia, or omphalocele/gastroschisis), kidney (structural abnormalities), craniofacial structures, or limbs should prompt referral for evaluation with a fetal echocardiogram.511 In addition, unexplained fetal growth delay512 or features such as increased nuchal translucency513 are associated with a significant risk of congenital cardiac abnormalities and are indications for performing a fetal echocardiogram even if fcfDNA screening does not detect a chromosomal abnormality. Recent data indicate that of fetuses with increased nuchal translucency and normal karyotype, ≈10% had positive testing for NS.514 Furthermore, persistence of nuchal translucency into the second trimester as nuchal edema identified a high prevalence of NS (11 of 15 cases).515
SUMMARY
Our understanding of the role of genetics in the pathogenesis of congenital HD has advanced at a rapid pace over the past 10 to 15 years. The availability of new molecular techniques has facilitated gene discoveries that have changed the medical and cardiological care of many individuals with congenital HD. CNV detection and NGS gene panels are now in widespread use by geneticists, genetic counselors, and cardiologists for accurate diagnosis of congenital HD patients. Cardiovascular genetics clinics are now available in many major medical centers in the United States. Accurate diagnosis of congenital HD pathogenesis is allowing for determination of familial recurrence risks, providing reproductive options, identifying extracardiac manifestations of the genetic diagnosis that could affect clinical care, and improving long-term medical decisions in the care of congenital HD. Additionally, WES is now used in many centers for those congenital HD patients suspected of having a genetic disorder when no pathogenetic diagnosis was obtained by other molecular testing.
The future of understanding of other genetic factors important in the causation of congenital HD will be determined by (1) studies with larger numbers of individuals with congenital HD using existing technologies (eg, WES), as well as application of other “omic” approaches (eg, whole genome sequencing, DNA methylation analysis, RNA sequencing with discarded cardiac tissues, and increasingly advanced bioinformatics analyses), and (2) new research with animal and cell models to utilize innovative molecular technologies to study RNA expression, splicing alterations, signaling technology, transcription factor fate, and epigenetic processes.13 Current induced pluripotent stem cell and gene-editing approaches have enabled the study of human cardiomyocytes relevant for congenital HD, whereas advances in generating tissues and organoids could allow the study of genetic variation relevant to congenital HD in contexts more relevant physiologically and developmentally in the near future.
Acknowledgments
The authors thank Patricia Buenzle, University of Minnesota, for her assistance in the preparation of the manuscript.
Sources of Funding
The authors acknowledge support by the following grants: U01 HL098163 (Wendy Chung), R01 HL109758 (Vidu Garg), R35 HL135742 and UM1 HL098123 (Bruce Gelb), U01 HG006500, U19 HD077671, and U01 HG006485 (Amy McGuire), Heart and Stroke Foundation of Canada Chair in Cardiovascular Science (Seema Mital), R00 HL130523 (James Priest), 2UM1 HL098166, R01 HL 128694, R01 HL116461, and 16CSA28750006 AHA (William T. Pu), U10 HL109737 (Mark Russell), 1 P01 HL134599-01, and March of Dimes Research Foundation 6-FY16-176, R01 HL1114590-05, and AHA 13EIA 13460001 (Stephanie Ware).
Disclosures
Writing Group Disclosures
| Writing Group Member |
Employment | Research Grant |
Other Research Support |
Speakers’ Bureau/ Honoraria |
Expert Witness |
Ownership Interest |
Consultant/ Advisory Board |
Other |
|---|---|---|---|---|---|---|---|---|
| Mary Ella Pierpont | University of Minnesota | None | None | None | None | None | None | None |
| Bruce D. Gelb | Icahn School of Medicine at Mount Sinai | None | GeneDx, LabCorp, Prevention Genetics (royalties for Noonan syndrome genetic testing)* | None | None | None | None | None |
| Mark W. Russell | University of Michigan | None | None | None | None | None | None | None |
| Martina Brueckner | Yale School of Medicine | NIH (principal investigator, SC member of NIH grants)† | None | None | None | None | None | None |
| Wendy K. Chung | Columbia University | None | None | None | None | None | None | None |
| Vidu Garg | Nationwide Children’s Hospital/Ohio State University Center for Cardiovascular Research/Pediatrics | NIH/NHLBI (grant support that ended 7/31/2017)† | None | None | None | None | None | None |
| Ronald V. Lacro | Boston Children’s Hospital | None | None | None | None | None | None | None |
| Amy L. McGuire | Baylor College of Medicine | None | None | None | None | None | None | None |
| Seema Mital | The Hospital for Sick Children | None | None | None | None | None | None | None |
| James R. Priest | Stanford University School of Medicine | None | None | None | None | None | None | None |
| William T. Pu | Boston Children’s Hospital | None | None | None | None | None | None | None |
| Amy Roberts | Children’s Hospital Boston | None | None | None | None | None | None | None |
| Stephanie M. Ware | Indiana University School of Medicine | None | None | None | None | None | None | None |
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $10 000 or more during any 12-month period, or 5% or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
Modest.
Significant.
Reviewer Disclosures
| Reviewer | Employment | Research Grant |
Other Research Support |
Speakers’ Bureau/ Honoraria |
Expert Witness |
Ownership Interest |
Consultant/ Advisory Board |
Other |
|---|---|---|---|---|---|---|---|---|
| Maria Grazia Andreassi | CNR, Institute of Clinical Physiology (Italy) | None | None | None | None | None | None | None |
| Paul Grossfeld | UCSD | AHA GIA (AHA Grant-in-Aid ended December, 2017)* | None | None | None | None | None | None |
| Julien I. E. Hoffman | University of California | None | None | None | None | None | None | None |
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all reviewers are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $10000 or more during any 12-month period, or 5% or more of the person’s gross income; or (b) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
Significant.
APPENDIX
Appendix.
| Chromosome Change | Main Features | Percent With Congenital HD | Heart Anomaly | References |
|---|---|---|---|---|
| I. Aneuploidies (identifiable by routine karyotype) | ||||
| Trisomy 8 mosaicism | Widely spaced eyes, broad nasal bridge, small jaw, high arched palate, cryptorchidism, renal anomalies, skeletal/vertebral anomalies | 25 | VSD, PDA, CoA, PVS, TAPVR, TrA | 516 |
| Trisomy 9/mosaicism | Prenatal and postnatal growth retardation, microcephaly, deep-set eyes, low-set ears, severe intellectual disability | 65 | PDA, LSVC, VSD, TOF/PA, DORV | 517 |
| Trisomy 13 (Patau syndrome) | Cleft lip and palate, scalp defects, hypotelorism, microphthalmia or anophthalmia, colobomata of irides, holoprosencephaly, microcephaly, deafness, severe intellectual disability, rib abnormalities, polydactyly, omphalocele, renal abnormalities, hypospadias, cryptorchidism, uterine abnormalities | 57–80 | ASD, VSD, PDA, HLHS, laterality defects, atrial isomerism | 518, 519 |
| Trisomy 18 (Edwards syndrome) | IUGR, polyhydramnios, micrognathia, short sternum, hypertonia, rocker-bottom feet, overlapping fingers and toes, TEF, CDH, omphalocele, renal anomalies, biliary atresia, severe intellectual disability | 80–90 | ASD, VSD, PDA, TOF, DORV, TGA, CoA, BAV, BPV, polyvalvular nodular dysplasia | 518 |
| Trisomy 21 (Down syndrome) | Hypotonia, hyperextensibility, epicanthal folds, up-slanting palpebral fissures, single palmar transverse crease, clinodactyly of fifth finger, brachydactyly, variable intellectual disability, premature aging | 40–50 | AVSD, VSD, ASD, (TOF, TGA less common) | 33, 37 |
| Monosomy X (Turner syndrome, 45,X) | Lymphedema of hands and feet, widely spaced hypoplastic nipples, webbed neck, primary amenorrhea, short stature, normal intelligence or mild learning disability | 23–35 | CoA, BAV, AS, HLHS, aortic dissection | 41, 520 |
| II. Chromosome abnormalities (identifiable on karyotype and more recently using chromosomal microarray) | ||||
| 3p25 deletion | Prenatal and postnatal growth deficiency, polydactyly, microcephaly, intellectual disability, renal anomalies | 33 | VSD, AVSD, tricuspid atresia | 521 |
| Deletion 4p16.3 (Wolf-Hirschhorn syndrome) | Microcephaly, widely spaced eyes, broad nasal bridge (Greek helmet appearance), downturned mouth, micrognathia, preauricular skin tags, severe intellectual disability, seizures, growth retardation | 50–65 | ASD, VSD, PDA, LSVC, aortic atresia, dextrocardia, TOF, tricuspid atresia | 522 |
| Deletion 4q | Growth retardation, intellectual disability, cleft palate, broad nasal bridge, micrognathia, abnormal ears, genitourinary defects | 50 | VSD, PDA, AS, ASD, TOF, CoA | 523 |
| Deletion 5p (cri-du-chat) | Catlike cry, prenatal and postnatal growth retardation, round face, widely spaced eyes, epicanthal folds, single palmar transverse crease, severe intellectual disability | 30–60 | VSD, ASD, PDA | 524, 525 |
| Deletion 9p syndrome | Craniosynostosis, trigonocephaly, up-slanting palpebral fissures, abnormal ear pinnae, scoliosis, micropenis, cryptorchidism, intellectual disability | 35–50 | VSD, PDA, PVS | 526 |
| Deletion 10p | Frontal bossing, short down-slanting palpebral fissures, small low-set ears, micrognathia, cleft palate, short neck, urinary/genital and upper-limb anomalies | 42 | BAV, ASD, VSD, PDA, PVS, CoA | 527 |
| Duplication 10q24-qter | Prenatal growth retardation, intellectual disability, camptodactyly, renal anomalies, cryptorchidism | 50 | AVSD, VSD | 528 |
| III. Copy number variants (identifiable by chromosomal microarray) | ||||
| 1p36 deletion | Growth deficiency, intellectual disability, microcephaly, deep-set eyes, low-set ears, hearing loss, hypotonia, seizures, CNS defects, genital anomalies | 70 | PDA, VSD, ASD, BAV, Ebstein anomaly, noncompaction cardiomyopathy | 99 |
| 1q21.1 deletion | Short stature, microcephaly, colobomas, microphthalmia, hearing loss, seizures, mild intellectual disability, autism spectrum disorder, skeletal malformations | N/A | PDA, VSD, ASD, TrA, TOF | 102, 105 |
| 1q21.1 duplication | Large head size, hemivertebrae, variable intellectual disability, variable autistic features, hypospadias, clubfoot | N/A | TOF, TGA, PVS | 105 |
| 1q41q42 microdeletion | Growth retardation, intellectual disability, microcephaly, diaphragmatic hernia, seizures, short limbs | 40 | BAV, ASD, VSD, TGA | 529 |
| 1q43q44 microdeletion | Prenatal and postnatal growth retardation, intellectual disability, limited speech, microcephaly, deep-set eyes, microcephaly, large low-set ears, cleft palate, agenesis of corpus callosum | N/A | VSD, CoA, HLHS | 530 |
| 2q31.1 microdeletion | Prenatal and postnatal growth retardation, large ventricles, microcephaly, narrow forehead down-slanting palpebral fissures, cleft palate/cleft lip, limb defects, hypoplastic genitalia | 25 | VSD, ASD, PDA | 531 |
| 2q37 microdeletion | Short stature, obesity, intellectual disability, sparse hair, arched eyebrows, epicanthal folds, thin upper lip, small hands and feet, clinodactyly | 30 | VSD, ASD, CoA, hypoplastic aortic arch | 532, 533 |
| Deletion 7q11.23(Williams-Beuren syndrome) | Infantile hypercalcemia, skeletal and renal anomalies, cognitive deficits, “social” personality, elfin facies | 53–85 | Supravalvar AS and PS, PPS | 41, 74 |
| 8p23.1 deletion | Microcephaly, growth retardation, deep-set eyes, malformed ears, small chin, genital anomalies in males, intellectual disability | 50–75 | AVSD, PVS, VSD, TOF | 112 |
| 9q34.3 Subtelomeric deletion (Kleefstra syndrome) | Short stature, obesity, intellectual disability, microcephaly, behavior abnormalities, brain anomalies, hypertelorism, arched eyebrows, midface hypoplasia | 31–44 | ASD, VSD, TOF, pulmonary arterial stenosis | 534 |
| Deletion 11q (Jacobsen syndrome) | Growth retardation, developmental delay, thrombocytopenia, platelet dysfunction, widely spaced eyes, strabismus, broad nasal bridge, thin upper lip, prominent forehead, intellectual disability | 56 | HLHS, AS, VSD, CoA, Shone’s complex | 91, 92 |
| 15q24 microdeletion | Prenatal and postnatal growth retardation, intellectual disability, abnormal corpus callosum, microcephaly, high forehead, down-slanting palpebral fissures, tapered eyebrows, abnormal ear pinnae, hearing loss, hypospadias, scoliosis, coloboma, strabismus | 40 | PDA, pulmonary arterial stenosis, PVS | 535 |
| 16p11.2p12.2 microdeletion | Hypotonia, intellectual disability, long narrow face, deep-set eyes, low-set malformed ears | 33 | TOF, BAV, pulmonary atresia | 536 |
| 17q21 microdeletion | Abnormal hair pigmentation, up-slanting palpebral fissures, epicanthal folds, bulbous nasal tip, strabismus, ptosis, long slender fingers, hip dislocation, renal anomalies, spine deformities, cryptorchidism, global developmental delay | 27 | PVS, ASD, VSD, BAV | 537 |
| Deletion 20p12 (Alagille syndrome) | Bile duct paucity, cholestasis, skeletal or ocular anomalies, broad forehead, widely spaced eyes, underdeveloped mandible | 85–94 | Peripheral PA hypoplasia, TOF, PVS (left-sided heart lesions and septal defects less common) | 538 |
| 22q11.2DS (DiGeorge, velocardiofacial, and conotruncal anomaly face syndrome) | Hypertelorism, micrognathia, low-set posteriorly rotated ears, thymic and parathyroid hypoplasia, hypocalcemia, feeding/speech/learning/behavioral disorders, immunodeficiency, palate/skeletal/renal anomalies, learning disability | 75 | IAA-B, TrA, isolated aortic arch anomalies, TOF, conoventricular VSD | 60, 70 |
| 22q11.2 duplication | Very variable phenotype, some with velopharyngeal insufficiency, cleft palate, hearing loss, minor facial anomalies, mild learning disability to normal learning ability, hypotonia, scoliosis, frequent infections | 15 | TOF, HLHS, VSD, PVS, TrA | 66 |
| 22q13 microdeletion (Phelan-McDermid syndrome) | Normal growth, intellectual disability, dolichocephaly, dysplastic ears, pointed chin, large fleshy hands, hypotonia | >25 | PDA, VSD, ASD, TAPVR | 539 |
22q11.2DS indicates 22q11.2 deletion syndrome; AS, aortic stenosis; ASD, atrial septal defect; AVSD, atrioventricular septal defect; BAV, bicuspid aortic valve; BPV, bicuspid pulmonary valve; CDH, congenital diaphragmatic hernia; CoA, coarctation of the aorta; DORV, double-outlet right ventricle; HD, heart disease; HLHS, hypoplastic left heart syndrome; IAA-B, interrupted aortic arch type B; IUGR, intrauterine growth retardation; LSVC, persistent left superior vena cava; N/A, not available; PA, pulmonary artery; PDA, patent ductus arteriosus; PPS, peripheral pulmonary stenosis; PS, pulmonary stenosis; PVS, pulmonic valve stenosis; TAPVR, total anomalous pulmonary venous return; TEF, tracheoesophageal fistula; TGA, d-transposition of the great arteries; TOF, tetralogy of Fallot; TOF/PA, tetralogy of Fallot with pulmonary atresia; TrA, truncus arteriosus; and VSD, ventricular septal defect.
Footnotes
ARTICLE INFORMATION
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This statement was approved by the American Heart Association Science Advisory and Coordinating Committee on April 13, 2018, and the American Heart Association Executive Committee on June 25, 2018. A copy of the document is available at http://professional.heart.org/statements by using either “Search for Guidelines & Statements” or the “Browse by Topic” area. To purchase additional reprints, call 843–216-2533 or e-mail kelle.ramsay@ wolterskluwer.com.
The American Heart Association requests that this document be cited as follows: Pierpont ME, Brueckner M, Chung WK, Garg V, Lacro RV, McGuire AL, Mital S, Priest JR, Pu WT, Roberts A, Ware SM, Gelb BD, Russell MW; on behalf of the American Heart Association Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Genomic and Precision Medicine. Genetic basis for congenital heart disease: revisited: a scientific statement from the American Heart Association. Circulation. 2018;138:e653–e711. DOI: 10.1161/CIR.0000000000000606.
The expert peer review of AHA-commissioned documents (eg, scientific statements, clinical practice guidelines, systematic reviews) is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines development, visit http://professional.heart.org/statements. Select the “Guidelines & Statements” drop-down menu, then click “Publication Development.”
Permissions: Multiple copies, modification alteration, enhancement, and/or distribution of this document are not permitted without the express permission of the American Heart Association. Instructions for obtaining permission are located at https://www.heart.org/permissions. A link to the “Copyright Permissions Request Form” appears in the second paragraph (https://www.heart.org/en/about-us/statements-and-policies/copyright-request-form).
REFERENCES
- 1.Pierpont ME, Basson CT, Benson DW Jr, Gelb BD, Giglia TM, Goldmuntz E, McGee G, Sable CA, Srivastava D, Webb CL. Genetic basis for congenital heart defects: current knowledge: a scientific statement from the American Heart Association Congenital Cardiac Defects Committee, Council on Cardiovascular Disease in the Young. Circulation 2007;115:3015–3038. doi: 10.1161/CIRCULATIONAHA.106.183056 [DOI] [PubMed] [Google Scholar]
- 2.Paterick TE, Humphries JA, Ammar KA, Jan MF, Loberg R, Bush M, Khandheria BK, Tajik AJ. Aortopathies: etiologies, genetics, differential diagnosis, prognosis and management. Am J Med 2013;126:670–678. doi: 10.1016/j.amjmed.2013.01.029 [DOI] [PubMed] [Google Scholar]
- 3.Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, Blom N, Brugada J, Chiang CE, Huikuri H, Kannankeril P, Krahn A, Leenhardt A, Moss A, Schwartz PJ, Shimizu W, Tomaselli G, Tracy C. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Heart Rhythm 2013;10:1932–1963. doi: 10.1016/j.hrthm.2013.05.014 [DOI] [PubMed] [Google Scholar]
- 4.Lee TM, Hsu DT, Kantor P, Towbin JA, Ware SM, Colan SD, Chung WK, Jefferies JL, Rossano JW, Castleberry CD, Addonizio LJ, Lal AK, Lamour JM, Miller EM, Thrush PT, Czachor JD, Razoky H, Hill A, Lipshultz SE. Pediatric cardiomyopathies. Circ Res 2017;121:855–873. doi: 10.1161/CIRCRESAHA.116.309386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vacanti G, Maragna R, Priori SG, Mazzanti A. Genetic causes of sudden cardiac death in children: inherited arrhythmogenic diseases. Curr Opin Pediatr 2017;29:552–559. doi: 10.1097/MOP.0000000000000537 [DOI] [PubMed] [Google Scholar]
- 6.van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011;58:2241–2247. doi: 10.1016/j.jacc.2011.08.025 [DOI] [PubMed] [Google Scholar]
- 7.Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002;39:1890–1900. [DOI] [PubMed] [Google Scholar]
- 8.Wren C The epidemiology of cardiovascular malformations. In: Moller JH, ed. Pediatric Cardiovascular Medicine 2nd ed. West Sussex, UK: Blackwell Publishing; 2012: 268–275. [Google Scholar]
- 9.Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation 2014;130:749–756. doi: 10.1161/CIRCULATIONAHA.113.008396 [DOI] [PubMed] [Google Scholar]
- 10.Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsy study of 161 cases. Am J Cardiol 1984;53:849–855. [DOI] [PubMed] [Google Scholar]
- 11.Steinberger J, Moller JH, Berry JM, Sinaiko AR. Echocardiographic diagnosis of heart disease in apparently healthy adolescents. Pediatrics 2000;105(pt 1):815–818. [DOI] [PubMed] [Google Scholar]
- 12.Tutar E, Ekici F, Atalay S, Nacar N. The prevalence of bicuspid aortic valve in newborns by echocardiographic screening. Am Heart J 2005;150:513–515. doi: 10.1016/j.ahj.2004.10.036 [DOI] [PubMed] [Google Scholar]
- 13.Cowan JR, Ware SM. Genetics and genetic testing in congenital heart disease. Clin Perinatol 2015;42:373–393, ix. doi: 10.1016/j.clp.2015.02.009 [DOI] [PubMed] [Google Scholar]
- 14.Jin SC, Homsy J, Zaidi S, Lu Q, Morton S, DePalma SR, Zeng X, Qi H, Chang W, Sierant MC, Hung WC, Haider S, Zhang J, Knight J, Bjornson RD, Castaldi C, Tikhonoa IR, Bilguvar K, Mane SM, Sanders SJ, Mital S, Russell MW, Gaynor JW, Deanfield J, Giardini A, Porter GA Jr, Srivastava D, Lo CW, Shen Y, Watkins WS, Yandell M, Yost HJ, Tristani-Firouzi M, Newburger JW, Roberts AE, Kim R, Zhao H, Kaltman JR, Goldmuntz E, Chung WK, Seidman JG, Gelb BD, Seidman CE, Lifton RP, Brueckner M. Contribution of rare inherited and de novo variants in 2,871 congenital heart disease probands. Nat Genet 2017;49:1593–1601. doi: 10.1038/ng.3970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.International Human Genome Sequencing Consortium. Finishing the euchromatic sequence of the human genome. Nature 2004;431:931–945. [DOI] [PubMed] [Google Scholar]
- 16.Schneider VA, Graves-Lindsay T, Howe K, Bouk N, Chen HC, Kitts PA, Murphy TD, Pruitt KD, Thibaud-Nissen F, Albracht D, Fulton RS, Kremitzki M, Magrini V, Markovic C, McGrath S, Steinberg KM, Auger K, Chow W, Collins J, Harden G, Hubbard T, Pelan S, Simpson JT, Threadgold G, Torrance J, Wood JM, Clarke L, Koren S, Boitano M, Peluso P, Li H, Chin CS, Phillippy AM, Durbin R, Wilson RK, Flicek P, Eichler EE, Church DM. Evaluation of GRCh38 and de novo haploid genome assemblies demonstrates the enduring quality of the reference assembly. Genome Res 2017;27:849–864. doi: 10.1101/gr.213611.116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Osoegawa K, Mammoser AG, Wu C, Frengen E, Zeng C, Catanese JJ, de Jong PJ. A bacterial artificial chromosome library for sequencing the complete human genome. Genome Res 2001;11:483–496. doi: 10.1101/gr.169601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Xue Y, Ankala A, Wilcox WR, Hegde MR. Solving the molecular diagnostic testing conundrum for Mendelian disorders in the era of next-generation sequencing: single-gene, gene panel, or exome/genome sequencing. Genet Med 2015;17:444–451. doi: 10.1038/gim.2014.122 [DOI] [PubMed] [Google Scholar]
- 19.Martin CL, Warburton D. Detection of chromosomal aberrations in clinical practice: from karyotype to genome sequence. Annu Rev Genomics Hum Genet 2015;16:309–326. doi: 10.1146/annurev-genom-090413-025346 [DOI] [PubMed] [Google Scholar]
- 20.Bi W, Borgan C, Pursley AN, Hixson P, Shaw CA, Bacino CA, Lalani SR, Patel A, Stankiewicz P, Lupski JR, Beaudet AL, Cheung SW. Comparison of chromosome analysis and chromosomal microarray analysis: what is the value of chromosome analysis in today’s genomic array era? Genet Med 2013;15:450–457. doi: 10.1038/gim.2012.152 [DOI] [PubMed] [Google Scholar]
- 21.Priest JR. A primer to clinical genome sequencing. Curr Opin Pediatr 2017;29:513–519. doi: 10.1097/MOP.0000000000000532 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McKenna A, Hanna M, Banks E, Sivachenko A, Cibulskis K, Kernytsky A, Garimella K, Altshuler D, Gabriel S, Daly M, DePristo MA. The Genome Analysis Toolkit: a MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res 2010;20:1297–1303. doi: 10.1101/gr.107524.110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dewey FE, Grove ME, Priest JR, Waggott D, Batra P, Miller CL, Wheeler M, Zia A, Pan C, Karzcewski KJ, Miyake C, Whirl-Carrillo M, Klein TE, Datta S, Altman RB, Snyder M, Quertermous T, Ashley EA. Sequence to medical phenotypes: a framework for interpretation of human whole genome DNA sequence data. PLoS Genet 2015;11:e1005496. doi: 10.1371/journal.pgen.1005496 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tester DJ, Benton AJ, Train L, Deal B, Baudhuin LM, Ackerman MJ. Prevalence and spectrum of large deletions or duplications in the major long QT syndrome-susceptibility genes and implications for long QT syndrome genetic testing. Am J Cardiol 2010;106:1124–1128. doi: 10.1016/j.amjcard.2010.06.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Arscott P, Caleshu C, Kotzer K, Kreykes S, Kruisselbrink T, Orland K, Rigelsky C, Smith E, Spoonamore K, Larsen Haidle J, Marvin M, Ackerman MJ, Hadi A, Mani A, Ommen S, Cherny S. A case for inclusion of genetic counselors in cardiac care. Cardiol Rev 2016;24:49–55. doi: 10.1097/CRD.0000000000000081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bowdin S, Gilbert A, Bedoukian E, Carew C, Adam MP, Belmont J, Bernhardt B, Biesecker L, Bjornsson HT, Blitzer M, D’Alessandro LC, Deardorff MA, Demmer L, Elliott A, Feldman GL, Glass IA, Herman G, Hindorff L, Hisama F, Hudgins L, Innes AM, Jackson L, Jarvik G, Kim R, Korf B, Ledbetter DH, Li M, Liston E, Marshall C, Medne L, Meyn MS, Monfared N, Morton C, Mulvihill JJ, Plon SE, Rehm H, Roberts A, Shuman C, Spinner NB, Stavropoulos DJ, Valverde K, Waggoner DJ, Wilkens A, Cohn RD, Krantz ID. Recommendations for the integration of genomics into clinical practice. Genet Med 2016;18:1075–1084. doi: 10.1038/gim.2016.17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Goldfeder RL, Priest JR, Zook JM, Grove ME, Waggott D, Wheeler MT, Salit M, Ashley EA. Medical implications of technical accuracy in genome sequencing. Genome Med 2016;8:24. doi: 10.1186/s13073-016-0269-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dewey FE, Grove ME, Pan C, Goldstein BA, Bernstein JA, Chaib H, Merker JD, Goldfeder RL, Enns GM, David SP, Pakdaman N, Ormond KE, Caleshu C, Kingham K, Klein TE, Whirl-Carrillo M, Sakamoto K, Wheeler MT, Butte AJ, Ford JM, Boxer L, Ioannidis JP, Yeung AC, Altman RB, Assimes TL, Snyder M, Ashley EA, Quertermous T. Clinical interpretation and implications of whole-genome sequencing. JAMA 2014;311:1035–1045. doi: 10.1001/jama.2014.1717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gil MM, Accurti V, Santacruz B, Plana MN, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: updated meta-analysis. Ultrasound Obstet Gynecol 2017;50:302–314. doi: 10.1002/uog.17484 [DOI] [PubMed] [Google Scholar]
- 30.Grace MR, Hardisty E, Dotters-Katz SK, Vora NL, Kuller JA. Cell-free DNA screening: complexities and challenges of clinical implementation. Obstet Gynecol Surv 2016;71:477–487. doi: 10.1097/OGX.0000000000000342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Merker JD, Wenger AM, Sneddon T, Grove M, Zappala Z, Fresard L, Waggott D, Utiramerur S, Hou Y, Smith KS, Montgomery SB, Wheeler M, Buchan JG, Lambert CC, Eng KS, Hickey L, Korlach J, Ford J, Ashley EA. Long-read genome sequencing identifies causal structural variation in a Mendelian disease. Genet Med 2018;20:159–163. doi: 10.1038/gim.2017.86 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hartman RJ, Rasmussen SA, Botto LD, Riehle-Colarusso T, Martin CL, Cragan JD, Shin M, Correa A. The contribution of chromosomal abnormalities to congenital heart defects: a population-based study. Pediatr Cardiol 2011;32:1147–1157. doi: 10.1007/s00246-011-0034-5 [DOI] [PubMed] [Google Scholar]
- 33.Bull MJ; Committee on Genetics. Health supervision for children with Down syndrome [published correction appears in Pediatrics. 2011;128:1212]. Pediatrics 2011;128:393–406. doi: 10.1542/peds.2011-1605 [DOI] [PubMed] [Google Scholar]
- 34.Allen HD, Driscoll D J, Shaddy RE, Feltes TF. Moss and Adams’ Heart Disease in Infants, Children, and Adolescents: Including the Fetus and Young Adult 8th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2013. [Google Scholar]
- 35.Bittles AH, Bower C, Hussain R, Glasson EJ. The four ages of Down syndrome. Eur J Public Health 2007;17:221–225. doi: 10.1093/eurpub/ckl103 [DOI] [PubMed] [Google Scholar]
- 36.Landis BJ, Cooper DS, Hinton RB. CHD associated with syndromic diagnoses: peri-operative risk factors and early outcomes. Cardiol Young 2016;26:30–52. doi: 10.1017/S1047951115001389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fudge JC Jr, Li S, Jaggers J, O’Brien SM, Peterson ED, Jacobs JP, Welke KF, Jacobs ML, Li JS, Pasquali SK. Congenital heart surgery outcomes in Down syndrome: analysis of a national clinical database. Pediatrics 2010;126:315–322. doi: 10.1542/peds.2009-3245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sybert VP. Cardiovascular malformations and complications in Turner syndrome. Pediatrics 1998;101:E11. [DOI] [PubMed] [Google Scholar]
- 39.Lin AE, Lippe B, Rosenfeld RG. Further delineation of aortic dilation, dissection, and rupture in patients with Turner syndrome. Pediatrics 1998;102:e12. [DOI] [PubMed] [Google Scholar]
- 40.Bordeleau L, Cwinn A, Turek M, Barron-Klauninger K, Victor G. Aortic dissection and Turner’s syndrome: case report and review of the literature. J Emerg Med 1998;16:593–596. [DOI] [PubMed] [Google Scholar]
- 41.Gravholt CH, Andersen NH, Conway GS, Dekkers OM, Geffner ME, Klein KO, Lin AE, Mauras N, Quigley CA, Rubin K, Sandberg DE, Sas TCJ, Silberbach M, Soderstrom-Anttila V, Stochholm K, van Alfen-van derVelden JA, Woelfle J, Backeljauw PF; International Turner Syndrome Consensus Group. Clinical practice guidelines for the care of girls and women with Turner syndrome: proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. Eur J Endocrinol 2017;177:G1–G70. doi: 10.1530/EJE-17-0430 [DOI] [PubMed] [Google Scholar]
- 42.Nielsen J, Wohlert M. Chromosome abnormalities found among 34,910 newborn children: results from a 13-year incidence study in Arhus, Denmark. Hum Genet 1991;87:81–83. [DOI] [PubMed] [Google Scholar]
- 43.Gøtzsche CO, Krag-Olsen B, Nielsen J, Sørensen KE, Kristensen BO. Prevalence of cardiovascular malformations and association with karyotypes in Turner’s syndrome. Arch Dis Child 1994;71:433–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mazzanti L, Cacciari E; Italian Study Group for Turner Syndrome (ISGTS). Congenital heart disease in patients with Turner’s syndrome. J Pediatr 1998;133:688–692. [DOI] [PubMed] [Google Scholar]
- 45.Goldmuntz E, Paluru P, Glessner J, Hakonarson H, Biegel JA, White PS, Gai X, Shaikh TH. Microdeletions and microduplications in patients with congenital heart disease and multiple congenital anomalies. Congenit Heart Dis 2011;6:592–602. doi: 10.1111/j.1747-0803.2011.00582.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Kim DS, Kim JH, Burt AA, Crosslin DR, Burnham N, Kim CE, McDonald-McGinn DM, Zackai EH, Nicolson SC, Spray TL, Stanaway IB, Nickerson DA, Heagerty PJ, Hakonarson H, Gaynor JW, Jarvik GP. Burden of potentially pathologic copy number variants is higher in children with isolated congenital heart disease and significantly impairs covariate-adjusted transplant-free survival. J Thorac Cardiovasc Surg 2016;151:1147–1151. e4. doi: 10.1016/j.jtcvs.2015.09.136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Carey AS, Liang L, Edwards J, Brandt T, Mei H, Sharp AJ, Hsu DT, Newburger JW, Ohye RG, Chung WK, Russell MW, Rosenfeld JA, Shaffer LG, Parides MK, Edelmann L, Gelb BD. Effect of copy number variants on outcomes for infants with single ventricle heart defects. Circ Cardiovasc Genet 2013;6:444–451. doi: 10.1161/CIRCGENETICS.113.000189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gelb BD, Chung WK. Complex genetics and the etiology of human congenital heart disease. Cold Spring Harb Perspect Med 2014;4:a013953. doi: 10.1101/cshperspect.a013953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Botto LD, May K, Fernhoff PM, Correa A, Coleman K, Rasmussen SA, Merritt RK, O’Leary LA, Wong LY, Elixson EM, Mahle WT, Campbell RM. A population-based study of the 22q11.2 deletion: phenotype, incidence, and contribution to major birth defects in the population. Pediatrics 2003;112(pt 1):101–107. [DOI] [PubMed] [Google Scholar]
- 50.Digilio MC, Angioni A, De Santis M, Lombardo A, Giannotti A, Dallapiccola B, Marino B. Spectrum of clinical variability in familial deletion 22q11.2: from full manifestation to extremely mild clinical anomalies. Clin Genet 2003;63:308–313. [DOI] [PubMed] [Google Scholar]
- 51.McDonald-McGinn DM, Emanuel BS, Zackai EH. 22q11.2 deletion syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 52.Agergaard P, Olesen C, Østergaard JR, Christiansen M, Sørensen KM. The prevalence of chromosome 22q11.2 deletions in 2,478 children with cardiovascular malformations: a population-based study. Am J Med Genet A 2012;158A:498–508. doi: 10.1002/ajmg.a.34250 [DOI] [PubMed] [Google Scholar]
- 53.Marino B, Digilio MC, Toscano A, Anaclerio S, Giannotti A, Feltri C, de Ioris MA, Angioni A, Dallapiccola B. Anatomic patterns of conotruncal defects associated with deletion 22q11. Genet Med 2001;3:45–48. doi: 10.109700125817-200101000-00010 [DOI] [PubMed] [Google Scholar]
- 54.Cassidy SB, Allanson JE. Management of Genetic Syndromes 3rd ed. Hoboken, NJ: Wiley-Blackwell; 2010. [Google Scholar]
- 55.Goldmuntz E, Clark BJ, Mitchell LE, Jawad AF, Cuneo BF, Reed L, McDonald-McGinn D, Chien P, Feuer J, Zackai EH, Emanuel BS, Driscoll DA. Frequency of 22q11 deletions in patients with conotruncal defects. J Am Coll Cardiol 1998;32:492–498. [DOI] [PubMed] [Google Scholar]
- 56.Momma K, Kondo C, Ando M, Matsuoka R, Takao A. Tetralogy of Fallot associated with chromosome 22q11 deletion. Am J Cardiol 1995;76:618–621. [DOI] [PubMed] [Google Scholar]
- 57.Beauchesne LM, Warnes CA, Connolly HM, Ammash NM, Grogan M, Jalal SM, Michels VV. Prevalence and clinical manifestations of 22q11.2 microdeletion in adults with selected conotruncal anomalies. J Am Coll Cardiol 2005;45:595–598. doi: 10.1016/j.jacc.2004.10.056 [DOI] [PubMed] [Google Scholar]
- 58.Anaclerio S, Di Ciommo V, Michielon G, Digilio MC, Formigari R, Picchio FM, Gargiulo G, Di Donato R, De Ioris MA, Marino B. Conotruncal heart defects: impact of genetic syndromes on immediate operative mortality. Ital Heart J 2004;5:624–628. [PubMed] [Google Scholar]
- 59.Mahle WT, Crisalli J, Coleman K, Campbell RM, Tam VK, Vincent RN, Kanter KR. Deletion of chromosome 22q11.2 and outcome in patients with pulmonary atresia and ventricular septal defect. Ann Thorac Surg 2003;76:567–571. [DOI] [PubMed] [Google Scholar]
- 60.Peyvandi S, Lupo PJ, Garbarini J, Woyciechowski S, Edman S, Emanuel BS, Mitchell LE, Goldmuntz E. 22q11.2 deletions in patients with conotruncal defects: data from 1,610 consecutive cases. Pediatr Cardiol 2013;34:1687–1694. doi: 10.1007/s00246-013-0694-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.McElhinney DB, Clark BJ 3rd, Weinberg PM, Kenton ML, McDonald-McGinn D, Driscoll DA, Zackai EH, Goldmuntz E. Association of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branching. J Am Coll Cardiol 2001;37:2114–2119. [DOI] [PubMed] [Google Scholar]
- 62.John AS, McDonald-McGinn DM, Zackai EH, Goldmuntz E. Aortic root dilation in patients with 22q11.2 deletion syndrome. Am J Med Genet A 2009;149A:939–942. doi: 10.1002/ajmg.a.32770 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.John AS, Rychik J, Khan M, Yang W, Goldmuntz E. 22q11.2 deletion syndrome as a risk factor for aortic root dilation in tetralogy of Fallot. Cardiol Young 2014;24:303–310. doi: 10.1017/S1047951113000309 [DOI] [PubMed] [Google Scholar]
- 64.Kunishima S, Imai T, Kobayashi R, Kato M, Ogawa S, Saito H. Bernard-Soulier syndrome caused by a hemizygous GPIbβ mutation and 22q11.2 deletion. Pediatr Int 2013;55:434–437. doi: 10.1111/ped.12105 [DOI] [PubMed] [Google Scholar]
- 65.Wentzel C, Fernström M, Ohrner Y, Annerén G, Thuresson AC. Clinical variability of the 22q11.2 duplication syndrome. Eur J Med Genet 2008;51:501–510. doi: 10.1016/j.ejmg.2008.07.005 [DOI] [PubMed] [Google Scholar]
- 66.Portnoï MF. Microduplication 22q11.2: a new chromosomal syndrome. Eur J Med Genet 2009;52:88–93. doi: 10.1016/j.ejmg.2009.02.008 [DOI] [PubMed] [Google Scholar]
- 67.Ou Z, Berg JS, Yonath H, Enciso VB, Miller DT, Picker J, Lenzi T, Keegan CE, Sutton VR, Belmont J, Chinault AC, Lupski JR, Cheung SW, Roeder E, Patel A. Microduplications of 22q11.2 are frequently inherited and are associated with variable phenotypes. Genet Med 2008;10:267–277. doi: 10.1097/GIM.0b013e31816b64c2 [DOI] [PubMed] [Google Scholar]
- 68.Ben-Shachar S, Ou Z, Shaw CA, Belmont JW, Patel MS, Hummel M, Amato S, Tartaglia N, Berg J, Sutton VR, Lalani SR, Chinault AC, Cheung SW, Lupski JR, Patel A. 22q11.2 distal deletion: a recurrent genomic disorder distinct from DiGeorge syndrome and velocardiofacial syndrome. Am J Hum Genet 2008;82:214–221. doi: 10.1016/j.ajhg.2007.09.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Breckpot J, Thienpont B, Bauters M, Tranchevent LC, Gewillig M, Allegaert K, Vermeesch JR, Moreau Y, Devriendt K. Congenital heart defects in a novel recurrent 22q11.2 deletion harboring the genes CRKL and MAPK1. Am J Med Genet A 2012;158A:574–580. doi: 10.1002/ajmg.a.35217 [DOI] [PubMed] [Google Scholar]
- 70.Mlynarski EE, Xie M, Taylor D, Sheridan MB, Guo T, Racedo SE, McDonald-McGinn DM, Chow EW, Vorstman J, Swillen A, Devriendt K, Breckpot J, Digilio MC, Marino B, Dallapiccola B, Philip N, Simon TJ, Roberts AE, Piotrowicz M, Bearden CE, Eliez S, Gothelf D, Coleman K, Kates WR, Devoto M, Zackai E, Heine-Suñer D, Goldmuntz E, Bassett AS, Morrow BE, Emanuel BS; International Chromosome 22q11.2 Consortium. Rare copy number variants and congenital heart defects in the 22q11.2 deletion syndrome. Hum Genet 2016;135:273–285. doi: 10.1007/s00439-015-1623-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.McDonald-McGinn DM, Fahiminiya S, Revil T, Nowakowska BA, Suhl J, Bailey A, Mlynarski E, Lynch DR, Yan AC, Bilaniuk LT, Sullivan KE, Warren ST, Emanuel BS, Vermeesch JR, Zackai EH, Jerome-Majewska LA. Hemizygous mutations in SNAP29 unmask autosomal recessive conditions and contribute to atypical findings in patients with 22q11.2DS. J Med Genet 2013;50:80–90. doi: 10.1136/jmedgenet-2012-101320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Morris CA. Williams syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 73.Wessel A, Pankau R, Kececioglu D, Ruschewski W, Bürsch JH. Three decades of follow-up of aortic and pulmonary vascular lesions in the Williams-Beuren syndrome. Am J Med Genet 1994;52:297–301. doi: 10.1002/ajmg.1320520309 [DOI] [PubMed] [Google Scholar]
- 74.Eronen M, Peippo M, Hiippala A, Raatikka M, Arvio M, Johansson R, Kähkönen M. Cardiovascular manifestations in 75 patients with Williams syndrome. J Med Genet 2002;39:554–558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Conway EE Jr, Noonan J, Marion RW, Steeg CN. Myocardial infarction leading to sudden death in the Williams syndrome: report of three cases. J Pediatr 1990;117:593–595. [DOI] [PubMed] [Google Scholar]
- 76.Latham GJ, Ross FJ, Eisses MJ, Richards MJ, Geiduschek JM, Joffe DC. Perioperative morbidity in children with elastin arteriopathy. Paediatr Anaesth 2016;26:926–935. doi: 10.1111/pan.12967 [DOI] [PubMed] [Google Scholar]
- 77.Bird LM, Billman GF, Lacro RV, Spicer RL, Jariwala LK, Hoyme HE, Zamora-Salinas R, Morris C, Viskochil D, Frikke MJ, Jones MC. Sudden death in Williams syndrome: report of ten cases. J Pediatr 1996;129:926–931. [DOI] [PubMed] [Google Scholar]
- 78.Wessel A, Gravenhorst V, Buchhorn R, Gosch A, Partsch CJ, Pankau R. Risk of sudden death in the Williams-Beuren syndrome. Am J Med Genet A 2004;127A:234–237. doi: 10.1002/ajmg.a.30012 [DOI] [PubMed] [Google Scholar]
- 79.Olsen M, Fahy CJ, Costi DA, Kelly AJ, Burgoyne LL. Anaesthesia-related haemodynamic complications in Williams syndrome patients: a review of one institution’s experience. Anaesth Intensive Care 2014;42:619–624. [DOI] [PubMed] [Google Scholar]
- 80.Ewart AK, Morris CA, Atkinson D, Jin W, Sternes K, Spallone P, Stock AD, Leppert M, Keating MT. Hemizygosity at the elastin locus in a developmental disorder, Williams syndrome. Nat Genet 1993;5:11–16. doi: 10.1038/ng0993-11 [DOI] [PubMed] [Google Scholar]
- 81.Huang L, Sadler L, O’Riordan MA, Robin NH. Delay in diagnosis of Williams syndrome. Clin Pediatr (Phila) 2002;41:257–261. doi: 10.1177/000992280204100410 [DOI] [PubMed] [Google Scholar]
- 82.Sadler LS, Pober BR, Grandinetti A, Scheiber D, Fekete G, Sharma AN, Urbán Z. Differences by sex in cardiovascular disease in Williams syndrome. J Pediatr 2001;139:849–853. doi: 10.1067/mpd.2001.118889 [DOI] [PubMed] [Google Scholar]
- 83.Merla G, Brunetti-Pierri N, Micale L, Fusco C. Copy number variants at Williams-Beuren syndrome 7q11.23 region. Hum Genet 2010;128:3–26. doi: 10.1007/s00439-010-0827-2 [DOI] [PubMed] [Google Scholar]
- 84.Morris CA, Mervis CB, Paciorkowski AP, Abdul-Rahman O, Dugan SL, Rope AF, Bader P, Hendon LG, Velleman SL, Klein-Tasman BP, Osborne LR. 7q11.23 duplication syndrome: physical characteristics and natural history. Am J Med Genet A 2015;167A:2916–2935. doi: 10.1002/ajmg.a.37340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Mervis CB, Morris CA, Klein-Tasman BP, Velleman SL, Osborne LR. 7q11.23 duplication syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [PubMed] [Google Scholar]
- 86.Committee on Genetics, American Academy of Pediatrics. Health care supervision for children with Williams syndrome [published correction appears in Pediatrics. 2002;109:329]. Pediatrics 2001;107:1192–1204. [PubMed] [Google Scholar]
- 87.Pober BR, Lacro RV, Rice C, Mandell V, Teele RL. Renal findings in 40 individuals with Williams syndrome. Am J Med Genet 1993;46:271–274. doi: 10.1002/ajmg.1320460306 [DOI] [PubMed] [Google Scholar]
- 88.Broder K, Reinhardt E, Ahern J, Lifton R, Tamborlane W, Pober B. Elevated ambulatory blood pressure in 20 subjects with Williams syndrome. Am J Med Genet 1999;83:356–360. [DOI] [PubMed] [Google Scholar]
- 89.Mervis CB, Robinson BF, Bertrand J, Morris CA, Klein-Tasman BP, Armstrong SC. The Williams syndrome cognitive profile. Brain Cogn 2000;44:604–628. doi: 10.1006/brcg.2000.1232 [DOI] [PubMed] [Google Scholar]
- 90.Jacobsen P, Hauge M, Henningsen K, Hobolth N, Mikkelsen M, Philip J. An (11;21) translocation in four generations with chromosome 11 abnormalities in the offspring: a clinical, cytogenetical, and gene marker study. Hum Hered 1973;23:568–585. doi: 10.1159/000152624 [DOI] [PubMed] [Google Scholar]
- 91.Grossfeld PD, Mattina T, Lai Z, Favier R, Jones KL, Cotter F, Jones C. The 11q terminal deletion disorder: a prospective study of 110 cases. Am J Med Genet A 2004;129A:51–61. doi: 10.1002/ajmg.a.30090 [DOI] [PubMed] [Google Scholar]
- 92.Favier R, Akshoomoff N, Mattson S, Grossfeld P. Jacobsen syndrome: advances in our knowledge of phenotype and genotype. Am J Med Genet C Semin Med Genet 2015;169:239–250. doi: 10.1002/ajmg.c.31448 [DOI] [PubMed] [Google Scholar]
- 93.Ye M, Coldren C, Liang X, Mattina T, Goldmuntz E, Benson DW, Ivy D, Perryman MB, Garrett-Sinha LA, Grossfeld P. Deletion of ETS-1, a gene in the Jacobsen syndrome critical region, causes ventricular septal defects and abnormal ventricular morphology in mice. Hum Mol Genet 2010;19:648–656. doi: 10.1093/hmg/ddp532 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Glessner JT, Bick AG, Ito K, Homsy J, Rodriguez-Murillo L, Fromer M, Mazaika E, Vardarajan B, Italia M, Leipzig J, DePalma SR, Golhar R, Sanders SJ, Yamrom B, Ronemus M, Iossifov I, Willsey AJ, State MW, Kaltman JR, White PS, Shen Y, Warburton D, Brueckner M, Seidman C, Goldmuntz E, Gelb BD, Lifton R, Seidman J, Hakonarson H, Chung WK. Increased frequency of de novo copy number variants in congenital heart disease by integrative analysis of single nucleotide polymorphism array and exome sequence data. Circ Res 2014;115:884–896. doi: 10.1161/CIRCRESAHA.115.304458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Grossfeld P Brain hemorrhages in Jacobsen syndrome: a retrospective review of six cases and clinical recommendations. Am J Med Genet A 2017;173:667–670. doi: 10.1002/ajmg.a.38032 [DOI] [PubMed] [Google Scholar]
- 96.Coldren CD, Lai Z, Shragg P, Rossi E, Glidewell SC, Zuffardi O, Mattina T, Ivy DD, Curfs LM, Mattson SN, Riley EP, Treier M, Grossfeld PD. Chromosomal microarray mapping suggests a role for BSX and Neurogranin in neurocognitive and behavioral defects in the 11q terminal deletion disorder (Jacobsen syndrome). Neurogenetics 2009;10:89–95. doi: 10.1007/s10048-008-0157-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Akshoomoff N, Mattson SN, Grossfeld PD. Evidence for autism spectrum disorder in Jacobsen syndrome: identification of a candidate gene in distal 11q. Genet Med 2015;17:143–148. doi: 10.1038/gim.2014.86 [DOI] [PubMed] [Google Scholar]
- 98.Battaglia A 1p36 deletion syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 99.Battaglia A, Hoyme HE, Dallapiccola B, Zackai E, Hudgins L, McDonald-McGinn D, Bahi-Buisson N, Romano C, Williams CA, Brailey LL, Braley LL, Zuberi SM, Carey JC. Further delineation of deletion 1p36 syndrome in 60 patients: a recognizable phenotype and common cause of developmental delay and mental retardation. Pediatrics 2008;121:404–410. doi: 10.1542/peds.2007-0929 [DOI] [PubMed] [Google Scholar]
- 100.Heilstedt HA, Ballif BC, Howard LA, Kashork CD, Shaffer LG. Population data suggest that deletions of 1p36 are a relatively common chromosome abnormality. Clin Genet 2003;64:310–316. [DOI] [PubMed] [Google Scholar]
- 101.Slavotinek A, Shaffer LG, Shapira SK. Monosomy 1p36. J Med Genet 1999;36:657–663. [PMC free article] [PubMed] [Google Scholar]
- 102.Christiansen J, Dyck JD, Elyas BG, Lilley M, Bamforth JS, Hicks M, Sprysak KA, Tomaszewski R, Haase SM, Vicen-Wyhony LM, Somerville MJ. Chromosome 1q21.1 contiguous gene deletion is associated with congenital heart disease. Circ Res 2004;94:1429–1435. doi: 10.1161/01.RES.0000130528.72330.5c [DOI] [PubMed] [Google Scholar]
- 103.Haldeman-Englert CR, Jewett T. 1q21.1 recurrent microdeletion. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 104.Bernier R, Steinman KJ, Reilly B, Wallace AS, Sherr EH, Pojman N, Mefford HC, Gerdts J, Earl R, Hanson E, Goin-Kochel RP, Berry L, Kanne S, Snyder LG, Spence S, Ramocki MB, Evans DW, Spiro JE, Martin CL, Ledbetter DH, Chung WK; Simons VIP Consortium. Clinical phenotype of the recurrent 1q21.1 copy-number variant. Genet Med 2016;18:341–349. doi: 10.1038/gim.2015.78 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Digilio MC, Bernardini L, Consoli F, Lepri FR, Giuffrida MG, Baban A, Surace C, Ferese R, Angioni A, Novelli A, Marino B, De Luca A, Dallapiccola B. Congenital heart defects in recurrent reciprocal 1q21.1 deletion and duplication syndromes: rare association with pulmonary valve stenosis. Eur J Med Genet 2013;56:144–149. doi: 10.1016/j.ejmg.2012.12.004 [DOI] [PubMed] [Google Scholar]
- 106.Mefford HC, Sharp AJ, Baker C, Itsara A, Jiang Z, Buysse K, Huang S, Maloney VK, Crolla JA, Baralle D, Collins A, Mercer C, Norga K, de Ravel T, Devriendt K, Bongers EM, de Leeuw N, Reardon W, Gimelli S, Bena F, Hennekam RC, Male A, Gaunt L, Clayton-Smith J, Simonic I, Park SM, Mehta SG, Nik-Zainal S, Woods CG, Firth HV, Parkin G, Fichera M, Reitano S, Lo Giudice M, Li KE, Casuga I, Broomer A, Conrad B, Schwerzmann M, Räber L, Gallati S, Striano P, Coppola A, Tolmie JL, Tobias ES, Lilley C, Armengol L, Spysschaert Y, Verloo P, De Coene A, Goossens L, Mortier G, Speleman F, van Binsbergen E, Nelen MR, Hochstenbach R, Poot M, Gallagher L, Gill M, McClellan J, King MC, Regan R, Skinner C, Stevenson RE, Antonarakis SE, Chen C, Estivill X, Menten B, Gimelli G, Gribble S, Schwartz S, Sutcliffe JS, Walsh T, Knight SJ, Sebat J, Romano C, Schwartz CE, Veltman JA, de Vries BB, Vermeesch JR, Barber JC, Willatt L, Tassabehji M, Eichler EE. Recurrent rearrangements of chromosome 1q21.1 and variable pediatric phenotypes. N Engl J Med 2008;359:1685–1699. doi: 10.1056/NEJMoa0805384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Guida V, Ferese R, Rocchetti M, Bonetti M, Sarkozy A, Cecchetti S, Gelmetti V, Lepri F, Copetti M, Lamorte G, Cristina Digilio M, Marino B, Zaza A, den Hertog J, Dallapiccola B, De Luca A. A variant in the carboxyl-terminus of connexin 40 alters GAP junctions and increases risk for tetralogy of Fallot. Eur J Hum Genet 2013;21:69–75. doi: 10.1038/ejhg.2012.109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Rosenfeld JA, Traylor RN, Schaefer GB, McPherson EW, Ballif BC, Klopocki E, Mundlos S, Shaffer LG, Aylsworth AS; 1q21.1 Study Group. Proximal microdeletions and microduplications of 1q21.1 contribute to variable abnormal phenotypes. Eur J Hum Genet 2012;20:754–761. doi: 10.1038/ejhg.2012.6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Soemedi R, Topf A, Wilson IJ, Darlay R, Rahman T, Glen E, Hall D, Huang N, Bentham J, Bhattacharya S, Cosgrove C, Brook JD, Granados-Riveron J, Setchfield K, Bu’lock F, Thornborough C, Devriendt K, Breckpot J, Hofbeck M, Lathrop M, Rauch A, Blue GM, Winlaw DS, Hurles M, Santibanez-Koref M, Cordell HJ, Goodship JA, Keavney BD. Phenotypespecific effect of chromosome 1q21.1 rearrangements and GJA5 duplications in 2436 congenital heart disease patients and 6760 controls. Hum Mol Genet 2012;21:1513–1520. doi: 10.1093/hmg/ddr589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Brunetti-Pierri N, Berg JS, Scaglia F, Belmont J, Bacino CA, Sahoo T, Lalani SR, Graham B, Lee B, Shinawi M, Shen J, Kang SH, Pursley A, Lotze T, Kennedy G, Lansky-Shafer S, Weaver C, Roeder ER, Grebe TA, Arnold GL, Hutchison T, Reimschisel T, Amato S, Geragthy MT, Innis JW, Obersztyn E, Nowakowska B, Rosengren SS, Bader PI, Grange DK, Naqvi S, Garnica AD, Bernes SM, Fong CT, Summers A, Walters WD, Lupski JR, Stankiewicz P, Cheung SW, Patel A. Recurrent reciprocal 1q21.1 deletions and duplications associated with microcephaly or macrocephaly and developmental and behavioral abnormalities. Nat Genet 2008;40:1466–1471. doi: 10.1038/ng.279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Claeys I, Holvoet M, Eyskens B, Adriaensens P, Gewillig M, Fryns JP, Devriendt K. A recognisable behavioural phenotype associated with terminal deletions of the short arm of chromosome 8. Am J Med Genet 1997;74:515–520. [DOI] [PubMed] [Google Scholar]
- 112.Wat MJ, Shchelochkov OA, Holder AM, Breman AM, Dagli A, Bacino C, Scaglia F, Zori RT, Cheung SW, Scott DA, Kang SH. Chromosome 8p23.1 deletions as a cause of complex congenital heart defects and diaphragmatic hernia. Am J Med Genet A 2009;149A:1661–1677. doi: 10.1002/ajmg.a.32896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Garg V, Kathiriya IS, Barnes R, Schluterman MK, King IN, Butler CA, Rothrock CR, Eapen RS, Hirayama-Yamada K, Joo K, Matsuoka R, Cohen JC, Srivastava D. GATA4 mutations cause human congenital heart defects and reveal an interaction with TBX5. Nature 2003;424:443–447. doi: 10.1038/nature01827 [DOI] [PubMed] [Google Scholar]
- 114.Turnpenny PD, Ellard S. Alagille syndrome: pathogenesis, diagnosis and management. Eur J Hum Genet 2012;20:251–257. doi: 10.1038/ejhg.2011.181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.McDaniell R, Warthen DM, Sanchez-Lara PA, Pai A, Krantz ID, Piccoli DA, Spinner NB. NOTCH2 mutations cause Alagille syndrome, a heterogeneous disorder of the notch signaling pathway. Am J Hum Genet 2006;79:169–173. doi: 10.1086/505332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Pierpont ME, Magoulas PL, Adi S, Kavamura MI, Neri G, Noonan J, Pierpont EI, Reinker K, Roberts AE, Shankar S, Sullivan J, Wolford M, Conger B, Santa Cruz M, Rauen KA. Cardio-facio-cutaneous syndrome: clinical features, diagnosis, and management guidelines. Pediatrics 2014;134:e1149–e1162. doi: 10.1542/peds.2013-3189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Scurr I, Wilson L, Lees M, Robertson S, Kirk E, Turner A, Morton J, Kidd A, Shashi V, Stanley C, Berry M, Irvine AD, Goudie D, Turner C, Brewer C, Smithson S. Cantú syndrome: report of nine new cases and expansion of the clinical phenotype. Am J Med Genet A 2011;155A:508–518. doi: 10.1002/ajmg.a.33885 [DOI] [PubMed] [Google Scholar]
- 118.Grange DK, Lorch SM, Cole PL, Singh GK. Cantu syndrome in a woman and her two daughters: Further confirmation of autosomal dominant inheritance and review of the cardiac manifestations. Am J Med Genet A 2006;140:1673–1680. doi: 10.1002/ajmg.a.31348 [DOI] [PubMed] [Google Scholar]
- 119.Satoda M, Zhao F, Diaz GA, Burn J, Goodship J, Davidson HR, Pierpont ME, Gelb BD. Mutations in TFAP2B cause Char syndrome, a familial form of patent ductus arteriosus. Nat Genet 2000;25:42–46. doi: 10.1038/75578 [DOI] [PubMed] [Google Scholar]
- 120.Sweeney E, Fryer A, Walters M. Char syndrome: a new family and review of the literature emphasising the presence of symphalangism and the variable phenotype. Clin Dysmorphol 2000;9:177–182. [DOI] [PubMed] [Google Scholar]
- 121.Trider CL, Arra-Robar A, van Ravenswaaij-Arts C, Blake K. Developing a CHARGE syndrome checklist: health supervision across the lifespan (from head to toe). Am J Med Genet A 2017;173:684–691. doi: 10.1002/ajmg.a.38085 [DOI] [PubMed] [Google Scholar]
- 122.Lin AE, Alexander ME, Colan SD, Kerr B, Rauen KA, Noonan J, Baffa J, Hopkins E, Sol-Church K, Limongelli G, Digilio MC, Marino B, Innes AM, Aoki Y, Silberbach M, Delrue MA, White SM, Hamilton RM, O’Connor W, Grossfeld PD, Smoot LB, Padera RF, Gripp KW. Clinical, pathological, and molecular analyses of cardiovascular abnormalities in Costello syndrome: a Ras/MAPK pathway syndrome. Am J Med Genet A 2011;155A:486–507. doi: 10.1002/ajmg.a.33857 [DOI] [PubMed] [Google Scholar]
- 123.Ruiz-Perez VL, Ide SE, Strom TM, Lorenz B, Wilson D, Woods K, King L, Francomano C, Freisinger P, Spranger S, Marino B, Dallapiccola B, Wright M, Meitinger T, Polymeropoulos MH, Goodship J. Mutations in a new gene in Ellis-van Creveld syndrome and Weyers acrodental dysostosis [published correction appears in Nat Genet. 2000;25:125]. Nat Genet 2000;24:283–286. doi: 10.1038/73508 [DOI] [PubMed] [Google Scholar]
- 124.Ruiz-Perez VL, Tompson SW, Blair HJ, Espinoza-Valdez C, Lapunzina P, Silva EO, Hamel B, Gibbs JL, Young ID, Wright MJ, Goodship JA. Mutations in two nonhomologous genes in a head-to-head configuration cause Ellisvan Creveld syndrome. Am J Hum Genet 2003;72:728–732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.McDermott DA, Bressan MC, He J, Lee JS, Aftimos S, Brueckner M, Gilbert F, Graham GE, Hannibal MC, Innis JW, Pierpont ME, Raas-Rothschild A, Shanske AL, Smith WE, Spencer RH, St John-Sutton MG, van Maldergem L, Waggoner DJ, Weber M, Basson CT. TBX5 genetic testing validates strict clinical criteria for Holt-Oram syndrome. Pediatr Res 2005;58:981–986. doi: 10.1203/01.PDR.0000182593.95441.64 [DOI] [PubMed] [Google Scholar]
- 126.Wessels MW, Brooks AS, Hoogeboom J, Niermeijer MF, Willems PJ. Kabuki syndrome: a review study of three hundred patients. Clin Dysmorphol 2002;11:95–102. [DOI] [PubMed] [Google Scholar]
- 127.Hannibal MC, Buckingham KJ, Ng SB, Ming JE, Beck AE, McMillin MJ, Gildersleeve HI, Bigham AW, Tabor HK, Mefford HC, Cook J, Yoshiura K, Matsumoto T, Matsumoto N, Miyake N, Tonoki H, Naritomi K, Kaname T, Nagai T, Ohashi H, Kurosawa K, Hou JW, Ohta T, Liang D, Sudo A, Morris CA, Banka S, Black GC, Clayton-Smith J, Nickerson DA, Zackai EH, Shaikh TH, Donnai D, Niikawa N, Shendure J, Bamshad MJ. Spectrum of MLL2 (ALR) mutations in 110 cases of Kabuki syndrome. Am J Med Genet A 2011;155A:1511–1516. doi: 10.1002/ajmg.a.34074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Romano AA, Allanson JE, Dahlgren J, Gelb BD, Hall B, Pierpont ME, Roberts AE, Robinson W, Takemoto CM, Noonan JA. Noonan syndrome: clinical features, diagnosis, and management guidelines. Pediatrics 2010;126:746–759. doi: 10.1542/peds.2009-3207 [DOI] [PubMed] [Google Scholar]
- 129.Al-Farqani A, Panduranga P, Al-Maskari S, Thomas E. VACTERL association with double-chambered left ventricle: a rare occurrence. Ann Pediatr Cardiol 2013;6:200–201. doi: 10.4103/0974-2069.115283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Pober BR. Williams-Beuren syndrome [published correction appears in N Engl J Med. 2010;362:2142]. N Engl J Med 2010;362:239–252. doi: 10.1056/NEJMra0903074 [DOI] [PubMed] [Google Scholar]
- 131.Jenkins D, Seelow D, Jehee FS, Perlyn CA, Alonso LG, Bueno DF, Donnai D, Josifova D, Josifiova D, Mathijssen IM, Morton JE, Orstavik KH, Sweeney E, Wall SA, Marsh JL, Nurnberg P, Passos-Bueno MR, Wilkie AO. RAB23 mutations in Carpenter syndrome imply an unexpected role for hedgehog signaling in cranial-suture development and obesity. Am J Hum Genet 2007;80:1162–1170. doi: 10.1086/518047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Santen GW, Clayton-Smith J; ARID1B-CSS Consortium. The ARID1B phenotype: what we have learned so far. Am J Med Genet C Semin Med Genet 2014;166C:276–289. doi: 10.1002/ajmg.c.31414 [DOI] [PubMed] [Google Scholar]
- 133.Kosho T, Okamoto N; Coffin-Siris Syndrome International Collaborators. Genotype-phenotype correlation of Coffin-Siris syndrome caused by mutations in SMARCB1, SMARCA4, SMARCE1, and ARID1A. Am J Med Genet C Semin Med Genet 2014;166C:262–275. doi: 10.1002/ajmg.c.31407 [DOI] [PubMed] [Google Scholar]
- 134.Selicorni A, Colli AM, Passarini A, Milani D, Cereda A, Cerutti M, Maitz S, Alloni V, Salvini L, Galli MA, Ghiglia S, Salice P, Danzi GB. Analysis of congenital heart defects in 87 consecutive patients with Brachmannde Lange syndrome. Am J Med Genet A 2009;149A:1268–1272. doi: 10.1002/ajmg.a.32838 [DOI] [PubMed] [Google Scholar]
- 135.Digilio MC, Calzolari F, Capolino R, Toscano A, Sarkozy A, de Zorzi A, Dallapiccola B, Marino B. Congenital heart defects in patients with oculo-auriculo-vertebral spectrum (Goldenhar syndrome). Am J Med Genet A 2008;146A:1815–1819. doi: 10.1002/ajmg.a.32407 [DOI] [PubMed] [Google Scholar]
- 136.Garavelli L, Zollino M, Mainardi PC, Gurrieri F, Rivieri F, Soli F, Verri R, Albertini E, Favaron E, Zignani M, Orteschi D, Bianchi P, Faravelli F, Forzano F, Seri M, Wischmeijer A, Turchetti D, Pompilii E, Gnoli M, Cocchi G, Mazzanti L, Bergamaschi R, De Brasi D, Sperandeo MP, Mari F, Uliana V, Mostardini R, Cecconi M, Grasso M, Sassi S, Sebastio G, Renieri A, Silengo M, Bernasconi S, Wakamatsu N, Neri G. Mowat-Wilson syndrome: facial phenotype changing with age: study of 19 Italian patients and review of the literature. Am J Med Genet A 2009;149A:417–426. doi: 10.1002/ajmg.a.32693 [DOI] [PubMed] [Google Scholar]
- 137.Zweier C, Thiel CT, Dufke A, Crow YJ, Meinecke P, Suri M, Ala-Mello S, Beemer F, Bernasconi S, Bianchi P, Bier A, Devriendt K, Dimitrov B, Firth H, Gallagher RC, Garavelli L, Gillessen-Kaesbach G, Hudgins L, Kääriäinen H, Karstens S, Krantz I, Mannhardt A, Medne L, Mücke J, Kibaek M, Krogh LN, Peippo M, Rittinger O, Schulz S, Schelley SL, Temple IK, Dennis NR, Van der Knaap MS, Wheeler P, Yerushalmi B, Zenker M, Seidel H, Lachmeijer A, Prescott T, Kraus C, Lowry RB, Rauch A. Clinical and mutational spectrum of Mowat-Wilson syndrome. Eur J Med Genet 2005;48:97–111. doi: 10.1016/j.ejmg.2005.01.003 [DOI] [PubMed] [Google Scholar]
- 138.Hennekam RC. Rubinstein-Taybi syndrome. Eur J Hum Genet 2006;14:981–985. doi: 10.1038/sj.ejhg.5201594 [DOI] [PubMed] [Google Scholar]
- 139.Waterham HR, Hennekam RC. Mutational spectrum of Smith-Lemli-Opitz syndrome. Am J Med Genet C Semin Med Genet 2012;160C:263–284. doi: 10.1002/ajmg.c.31346 [DOI] [PubMed] [Google Scholar]
- 140.Hassed S, Li S, Mulvihill J, Aston C, Palmer S. Adams-Oliver syndrome review of the literature: refining the diagnostic phenotype. Am J Med Genet A 2017;173:790–800. doi: 10.1002/ajmg.a.37889 [DOI] [PubMed] [Google Scholar]
- 141.Stittrich AB, Lehman A, Bodian DL, Ashworth J, Zong Z, Li H, Lam P, Khromykh A, Iyer RK, Vockley JG, Baveja R, Silva ES, Dixon J, Leon EL, Solomon BD, Glusman G, Niederhuber JE, Roach JC, Patel MS. Mutations in NOTCH1 cause Adams-Oliver syndrome. Am J Hum Genet 2014;95:275–284. doi: 10.1016/j.ajhg.2014.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Van Maldergem L, Siitonen HA, Jalkh N, Chouery E, De Roy M, Delague V, Muenke M, Jabs EW, Cai J, Wang LL, Plon SE, Fourneau C, Kestilä M, Gillerot Y, Mégarbané A, Verloes A. Revisiting the craniosynostosisradial ray hypoplasia association: Baller-Gerold syndrome caused by mutations in the RECQL4 gene. J Med Genet 2006;43:148–152. doi: 10.1136/jmg.2005.031781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Elliott M, Bayly R, Cole T, Temple IK, Maher ER. Clinical features and natural history of Beckwith-Wiedemann syndrome: presentation of 74 new cases. Clin Genet 1994;46:168–174. [DOI] [PubMed] [Google Scholar]
- 144.Rogers RC, Abidi FE. Coffin-Lowry syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 145.Kohlhase J, Heinrich M, Schubert L, Liebers M, Kispert A, Laccone F, Turnpenny P, Winter RM, Reardon W. Okihiro syndrome is caused by SALL4 mutations. Hum Mol Genet 2002;11:2979–2987. [DOI] [PubMed] [Google Scholar]
- 146.Saul RA, Tarleton JC. FMR1-related disorders. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 147.Coccia M, Brooks SP, Webb TR, Christodoulou K, Wozniak IO, Murday V, Balicki M, Yee HA, Wangensteen T, Riise R, Saggar AK, Park SM, Kanuga N, Francis PJ, Maher ER, Moore AT, Russell-Eggitt IM, Hardcastle AJ. X-linked cataract and Nance-Horan syndrome are allelic disorders. Hum Mol Genet 2009;18:2643–2655. doi: 10.1093/hmg/ddp206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Maillette de Buy Wenniger-Prick LJ, Hennekam RC. The Peters’ plus syndrome: a review. Ann Genet 2002;45:97–103. [DOI] [PubMed] [Google Scholar]
- 149.Lesnik Oberstein SA, Kriek M, White SJ, Kalf ME, Szuhai K, den Dunnen JT, Breuning MH, Hennekam RC. Peters Plus syndrome is caused by mutations in B3GALTL, a putative glycosyltransferase [published correction appears in Am J Hum Genet. 2006;79:985]. Am J Hum Genet 2006;79:562–566. doi: 10.1086/507567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Goh ES, Li C, Horsburgh S, Kasai Y, Kolomietz E, Morel CF. The Roberts syndrome/SC phocomelia spectrum: a case report of an adult with review of the literature. Am J Med Genet A 2010;152A:472–478. doi: 10.1002/ajmg.a.33261 [DOI] [PubMed] [Google Scholar]
- 151.Mazzeu JF, Pardono E, Vianna-Morgante AM, Richieri-Costa A, Ae Kim C, Brunoni D, Martelli L, de Andrade CE, Colin G, Otto PA. Clinical characterization of autosomal dominant and recessive variants of Robinow syndrome. Am J Med Genet A 2007;143:320–325. doi: 10.1002/ajmg.a.31592 [DOI] [PubMed] [Google Scholar]
- 152.Person AD, Beiraghi S, Sieben CM, Hermanson S, Neumann AN, Robu ME, Schleiffarth JR, Billington CJ Jr, van Bokhoven H, Hoogeboom JM, Mazzeu JF, Petryk A, Schimmenti LA, Brunner HG, Ekker SC, Lohr JL. WNT5A mutations in patients with autosomal dominant Robinow syndrome. Dev Dyn 2010;239:327–337. doi: 10.1002/dvdy.22156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Chun K, Teebi AS, Jung JH, Kennedy S, Laframboise R, Meschino WS, Nakabayashi K, Scherer SW, Ray PN, Teshima I. Genetic analysis of patients with the Saethre-Chotzen phenotype. Am J Med Genet 2002;110:136–143. doi: 10.1002/ajmg.10400 [DOI] [PubMed] [Google Scholar]
- 154.Badiner N, Taylor SP, Forlenza K, Lachman RS, University of Washington Center for Mendelian Genomics, Bamshad M, Nickerson D, Cohn DH, Krakow D. Mutations in DYNC2H1, the cytoplasmic dynein 2, heavy chain 1 motor protein gene, cause short-rib polydactyly type I, Saldino-Noonan type. Clin Genet 2017;92:158–165. doi: 10.1111/cge.12947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Lin AE, Neri G, Hughes-Benzie R, Weksberg R. Cardiac anomalies in the Simpson-Golabi-Behmel syndrome. Am J Med Genet 1999;83:378–381. [PubMed] [Google Scholar]
- 156.Gertsch E, Kirmani S, Ackerman MJ, Babovic-Vuksanovic D. Transient QT interval prolongation in an infant with Simpson-Golabi-Behmel syndrome. Am J Med Genet A 2010;152A:2379–2382. doi: 10.1002/ajmg.a.33561 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Leventopoulos G, Kitsiou-Tzeli S, Kritikos K, Psoni S, Mavrou A, Kanavakis E, Fryssira H. A clinical study of Sotos syndrome patients with review of the literature. Pediatr Neurol 2009;40:357–364. doi: 10.1016/j.pediatrneurol.2008.11.013 [DOI] [PubMed] [Google Scholar]
- 158.Miller EM, Hopkin R, Bao L, Ware SM. Implications for genotype-phenotype predictions in Townes-Brocks syndrome: case report of a novel SALL1 deletion and review of the literature. Am J Med Genet A 2012;158A:533–540. doi: 10.1002/ajmg.a.34426 [DOI] [PubMed] [Google Scholar]
- 159.Spinner NB, Leonard LD, Krantz ID. Alagille syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [PubMed] [Google Scholar]
- 160.Emerick KM, Rand EB, Goldmuntz E, Krantz ID, Spinner NB, Piccoli DA. Features of Alagille syndrome in 92 patients: frequency and relation to prognosis. Hepatology 1999;29:822–829. doi: 10.1002/hep.510290331 [DOI] [PubMed] [Google Scholar]
- 161.Kamath BM, Bason L, Piccoli DA, Krantz ID, Spinner NB. Consequences of JAG1 mutations. J Med Genet 2003;40:891–895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Hingorani M, Nischal KK, Davies A, Bentley C, Vivian A, Baker AJ, Mieli-Vergani G, Bird AC, Aclimandos WA. Ocular abnormalities in Alagille syndrome. Ophthalmology 1999;106:330–337. doi: 10.1016/S0161-6420(99)90072-6 [DOI] [PubMed] [Google Scholar]
- 163.Makino S, Ohkubo Y, Tampo H. Optical coherence tomography and fundus autofluorescence imaging study of chorioretinal atrophy involving the macula in Alagille syndrome. Clin Ophthalmol 2012;6:1445–1448. doi: 10.2147/OPTH.S36146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Kamath BM, Podkameni G, Hutchinson AL, Leonard LD, Gerfen J, Krantz ID, Piccoli DA, Spinner NB, Loomes KM, Meyers K. Renal anomalies in Alagille syndrome: a disease-defining feature. Am J Med Genet A 2012;158A:85–89. doi: 10.1002/ajmg.a.34369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Warthen DM, Moore EC, Kamath BM, Morrissette JJ, Sanchez-Lara PA, Sanchez P, Piccoli DA, Krantz ID, Spinner NB. Jagged1 (JAG1) mutations in Alagille syndrome: increasing the mutation detection rate. Hum Mutat 2006;27:436–443. doi: 10.1002/humu.20310 [DOI] [PubMed] [Google Scholar]
- 166.Lu F, Morrissette JJ, Spinner NB. Conditional JAG1 mutation shows the developing heart is more sensitive than developing liver to JAG1 dosage. Am J Hum Genet 2003;72:1065–1070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.McDermott DA, Fong JC, Basson CT. Holt-Oram syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 168.Basson CT, Cowley GS, Solomon SD, Weissman B, Poznanski AK, Traill TA, Seidman JG, Seidman CE. The clinical and genetic spectrum of the Holt-Oram syndrome (heart-hand syndrome) [published correction appears in N Engl J Med. 1994;330:1627]. N Engl J Med 1994;330:885–891. doi: 10.1056/NEJM199403313301302 [DOI] [PubMed] [Google Scholar]
- 169.Barisic I, Boban L, Greenlees R, Garne E, Wellesley D, Calzolari E, Addor MC, Arriola L, Bergman JE, Braz P, Budd JL, Gatt M, Haeusler M, Khoshnood B, Klungsoyr K, McDonnell B, Nelen V, Pierini A, Queisser-Wahrendorf A, Rankin J, Rissmann A, Rounding C, Tucker D, Verellen-Dumoulin C, Dolk H. Holt Oram syndrome: a registry-based study in Europe. Orphanet J Rare Dis 2014;9:156. doi: 10.1186/s13023-014-0156-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Basson CT, Huang T, Lin RC, Bachinsky DR, Weremowicz S, Vaglio A, Bruzzone R, Quadrelli R, Lerone M, Romeo G, Silengo M, Pereira A, Krieger J, Mesquita SF, Kamisago M, Morton CC, Pierpont ME, Müller CW, Seidman JG, Seidman CE. Different TBX5 interactions in heart and limb defined by Holt-Oram syndrome mutations. Proc Natl Acad Sci U S A 1999;96:2919–2924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Char F Peculiar facies with short philtrum, duck-bill lips, ptosis and low-set ears–a new syndrome? Birth Defects Orig Artic Ser 1978;14(6B):303–305. [PubMed] [Google Scholar]
- 172.Gelb BD. Char syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [PubMed] [Google Scholar]
- 173.Chen YW, Zhao W, Zhang ZF, Fu Q, Shen J, Zhang Z, Ji W, Wang J, Li F. Familial nonsyndromic patent ductus arteriosus caused by mutations in TFAP2B. Pediatr Cardiol 2011;32:958–965. doi: 10.1007/s00246-011-0024-7 [DOI] [PubMed] [Google Scholar]
- 174.Hanemann JA, de Carvalho BC, Franco EC. Oral manifestations in Ellisvan Creveld syndrome: report of a case and review of the literature. J Oral Maxillofac Surg 2010;68:456–460. doi: 10.1016/j.joms.2009.07.026 [DOI] [PubMed] [Google Scholar]
- 175.Baujat G, Le Merrer M. Ellis-van Creveld syndrome. Orphanet J Rare Dis 2007;2:27. doi: 10.1186/1750-1172-2-27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176.Huber C, Cormier-Daire V. Ciliary disorder of the skeleton. Am J Med Genet C Semin Med Genet 2012;160C:165–174. doi: 10.1002/ajmg.c.31336 [DOI] [PubMed] [Google Scholar]
- 177.Jones KL, Jones MC and Campo Md. Smith’s Recognizable Patterns of Human Malformation 7th ed. Philadelphia, PA: Elsevier Saunders; 2013. [Google Scholar]
- 178.Digilio MC, Marino B, Ammirati A, Borzaga U, Giannotti A, Dallapiccola B. Cardiac malformations in patients with oral-facial-skeletal syndromes: clinical similarities with heterotaxia. Am J Med Genet 1999;84:350–356. [DOI] [PubMed] [Google Scholar]
- 179.Galdzicka M, Patnala S, Hirshman MG, Cai JF, Nitowsky H, Egeland JA, Ginns EI. A new gene, EVC2, is mutated in Ellis-van Creveld syndrome. Mol Genet Metab 2002;77:291–295. [DOI] [PubMed] [Google Scholar]
- 180.Blair HJ, Tompson S, Liu YN, Campbell J, MacArthur K, Ponting CP, Ruiz-Perez VL, Goodship JA. Evc2 is a positive modulator of Hedgehog signalling that interacts with Evc at the cilia membrane and is also found in the nucleus. BMC Biol 2011;9:14. doi: 10.1186/1741-7007-9-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Zapata HH, Sletten LJ, Pierpont ME. Congenital cardiac malformations in Adams-Oliver syndrome. Clin Genet 1995;47:80–84. [DOI] [PubMed] [Google Scholar]
- 182.Lehman A, Stittrich AB, Glusman G, Zong Z, Li H, Eydoux P, Senger C, Lyons C, Roach JC, Patel M. Diffuse angiopathy in Adams-Oliver syndrome associated with truncating DOCK6 mutations. Am J Med Genet A 2014;164A:2656–2662. doi: 10.1002/ajmg.a.36685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Martínez-Frías ML, Arroyo Carrera I, Muñoz-Delgado NJ, Nieto Conde C, Rodríguez-Pinilla E, Urioste Azcorra M, Omeñaca Teres F, García Alix A. The Adams-Oliver syndrome in Spain: the epidemiological aspects [in Spanish]. An Esp Pediatr 1996;45:57–61. [PubMed] [Google Scholar]
- 184.Southgate L, Sukalo M, Karountzos ASV, Taylor EJ, Collinson CS, Ruddy D, Snape KM, Dallapiccola B, Tolmie JL, Joss S, Brancati F, Digilio MC, Graul-Neumann LM, Salviati L, Coerdt W, Jacquemin E, Wuyts W, Zenker M, Machado RD, Trembath RC. Haploinsufficiency of the NOTCH1 receptor as a cause of Adams-Oliver syndrome with variable cardiac anomalies. Circ Cardiovasc Genet 2015;8:572–581. doi: 10.1161/CIRCGENETICS.115.001086 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Garg V, Muth AN, Ransom JF, Schluterman MK, Barnes R, King IN, Grossfeld PD, Srivastava D. Mutations in NOTCH1 cause aortic valve disease. Nature 2005;437:270–274. doi: 10.1038/nature03940 [DOI] [PubMed] [Google Scholar]
- 186.Foffa I, Ait Alì L, Panesi P, Mariani M, Festa P, Botto N, Vecoli C, Andreassi MG. Sequencing of NOTCH1, GATA5, TGFBR1 and TGFBR2 genes in familial cases of bicuspid aortic valve. BMC Med Genet 2013;14:44. doi: 10.1186/1471-2350-14-44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Dentici ML, Di Pede A, Lepri FR, Gnazzo M, Lombardi MH, Auriti C, Petrocchi S, Pisaneschi E, Bellacchio E, Capolino R, Braguglia A, Angioni A, Dotta A, Digilio MC, Dallapiccola B. Kabuki syndrome: clinical and molecular diagnosis in the first year of life. Arch Dis Child 2015;100:158–164. doi: 10.1136/archdischild-2013-305858 [DOI] [PubMed] [Google Scholar]
- 188.Adam MP, Hudgins L, Hannibal M. Kabuki syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 189.Matsumoto N, Niikawa N. Kabuki make-up syndrome: a review. Am J Med Genet C Semin Med Genet 2003;117C:57–65. doi: 10.1002/ajmg.c.10020 [DOI] [PubMed] [Google Scholar]
- 190.Yuan SM. Congenital heart defects in Kabuki syndrome. Cardiol J 2013;20:121–124. doi: 10.5603/CJ.2013.0023 [DOI] [PubMed] [Google Scholar]
- 191.Digilio MC, Marino B, Toscano A, Giannotti A, Dallapiccola B. Congenital heart defects in Kabuki syndrome. Am J Med Genet 2001;100:269–274. [DOI] [PubMed] [Google Scholar]
- 192.Digilio MC, Baban A, Marino B, Dallapiccola B. Hypoplastic left heart syndrome in patients with Kabuki syndrome. Pediatr Cardiol 2010;31:1111–1113. doi: 10.1007/s00246-010-9773-y [DOI] [PubMed] [Google Scholar]
- 193.Yoon JK, Ahn KJ, Kwon BS, Kim GB, Bae EJ, Noh CI, Ko JM. The strong association of left-side heart anomalies with Kabuki syndrome. Korean J Pediatr 2015;58:256–262. doi: 10.3345/kjp.2015.58.7.256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Niikawa N, Kuroki Y, Kajii T, Matsuura N, Ishikiriyama S, Tonoki H, Ishikawa N, Yamada Y, Fujita M, Umemoto H, Iwama Y, Kondoh I, Fukushima Y, Naka Y, Matusui I, Urakami T, Aritaki S, Hara M, Suzuki Y, Chyo H, Sugio Y, Hasegawa T, Yamanaka T, Tsukino R, Yoshida A, Nomoto N, Kawahito S, Aihara R, Toyota S, Ieshima A, Funaki H, Ishitobi K, Ogura S, Furumae T, Yoshino M, Tsuji Y, Kondoh T, Matsumoto T, Abe K, Harada N, Miike T, Ohdo S, Naritomi K, Abushwereb AK, Braun OH, Schmid E, Opitz JM, Reynolds JF. Kabuki make-up (Niikawa-Kuroki) syndrome: a study of 62 patients. Am J Med Genet 1988;31:565–589. doi: 10.1002/ajmg.1320310312 [DOI] [PubMed] [Google Scholar]
- 195.White SM, Thompson EM, Kidd A, Savarirayan R, Turner A, Amor D, Delatycki MB, Fahey M, Baxendale A, White S, Haan E, Gibson K, Halliday JL, Bankier A. Growth, behavior, and clinical findings in 27 patients with Kabuki (Niikawa-Kuroki) syndrome. Am J Med Genet A 2004;127A:118–127. doi: 10.1002/ajmg.a.20674 [DOI] [PubMed] [Google Scholar]
- 196.Digilio MC, Gnazzo M, Lepri F, Dentici ML, Pisaneschi E, Baban A, Passarelli C, Capolino R, Angioni A, Novelli A, Marino B, Dallapiccola B. Congenital heart defects in molecularly proven Kabuki syndrome patients. Am J Med Genet A 2017;173:2912–2922. doi: 10.1002/ajmg.a.38417 [DOI] [PubMed] [Google Scholar]
- 197.Paulussen AD, Stegmann AP, Blok MJ, Tserpelis D, Posma-Velter C, Detisch Y, Smeets EE, Wagemans A, Schrander JJ, van den Boogaard MJ, van der Smagt J, van Haeringen A, Stolte-Dijkstra I, Kerstjens-Frederikse WS, Mancini GM, Wessels MW, Hennekam RC, Vreeburg M, Geraedts J, de Ravel T, Fryns JP, Smeets HJ, Devriendt K, Schrander-Stumpel CT. MLL2 mutation spectrum in 45 patients with Kabuki syndrome. Hum Mutat 2011;32:E2018–E2025. doi: 10.1002/humu.21416 [DOI] [PubMed] [Google Scholar]
- 198.Banka S, Lederer D, Benoit V, Jenkins E, Howard E, Bunstone S, Kerr B, McKee S, Lloyd IC, Shears D, Stewart H, White SM, Savarirayan R, Mancini GM, Beysen D, Cohn RD, Grisart B, Maystadt I, Donnai D. Novel KDM6A (UTX) mutations and a clinical and molecular review of the X-linked Kabuki syndrome (KS2). Clin Genet 2015;87:252–258. doi: 10.1111/cge.12363 [DOI] [PubMed] [Google Scholar]
- 199.Dentici ML, Barresi S, Niceta M, Pantaleoni F, Pizzi S, Dallapiccola B, Tartaglia M, Digilio MC. Clinical spectrum of Kabuki-like syndrome caused by HNRNPK haploinsufficiency. Clin Genet 2018;93:401–407. doi: 10.1111/cge.13029 [DOI] [PubMed] [Google Scholar]
- 200.Badalato L, Farhan SM, Dilliott AA, Bulman DE, Hegele RA, Goobie SL; Care4Rare Canada Consortium. KMT2D p.Gln3575His segregating in a family with autosomal dominant choanal atresia strengthens the Kabuki/CHARGE connection. Am J Med Genet A 2017;173:183–189. doi: 10.1002/ajmg.a.38010 [DOI] [PubMed] [Google Scholar]
- 201.Verloes A Updated diagnostic criteria for CHARGE syndrome: a proposal. Am J Med Genet A 2005;133A:306–308. doi: 10.1002/ajmg.a.30559 [DOI] [PubMed] [Google Scholar]
- 202.Raqbi F, Le Bihan C, Morisseau-Durand MP, Dureau P, Lyonnet S, Abadie V. Early prognostic factors for intellectual outcome in CHARGE syndrome. Dev Med Child Neurol 2003;45:483–488. [DOI] [PubMed] [Google Scholar]
- 203.Zentner GE, Layman WS, Martin DM, Scacheri PC. Molecular and phenotypic aspects of CHD7 mutation in CHARGE syndrome. Am J Med Genet A 2010;152A:674–686. doi: 10.1002/ajmg.a.33323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204.Lalani SR, Hefner MA, Belmont JW, Davenport SLH. CHARGE syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 205.Corsten-Janssen N, Kerstjens-Frederikse WS, du Marchie Sarvaas GJ, Baardman ME, Bakker MK, Bergman JE, Hove HD, Heimdal KR, Rustad CF, Hennekam RC, Hofstra RM, Hoefsloot LH, Van Ravenswaaij-Arts CM, Kapusta L. The cardiac phenotype in patients with a CHD7 mutation. Circ Cardiovasc Genet 2013;6:248–254. doi: 10.1161/CIRCGENETICS.113.000054 [DOI] [PubMed] [Google Scholar]
- 206.Corsten-Janssen N, van Ravenswaaij-Arts CMA, Kapusta L. Congenital arch vessel anomalies in CHARGE syndrome: a frequent feature with risk for co-morbidity. Int J Cardiol Heart Vasc 2016;12:21–25. doi: 10.1016/j.ijcha.2016.05.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 207.Issekutz KA, Graham JM Jr, Prasad C, Smith IM, Blake KD. An epidemiological analysis of CHARGE syndrome: preliminary results from a Canadian study. Am J Med Genet A 2005;133A:309–317. doi: 10.1002/ajmg.a.30560 [DOI] [PubMed] [Google Scholar]
- 208.Vuorela P, Ala-Mello S, Saloranta C, Penttinen M, Pöyhönen M, Huoponen K, Borozdin W, Bausch B, Botzenhart EM, Wilhelm C, Kääriäinen H, Kohlhase J. Molecular analysis of the CHD7 gene in CHARGE syndrome: identification of 22 novel mutations and evidence for a low contribution of large CHD7 deletions. Genet Med 2007;9:690–694. doi: 10.1097GIM.0b013e318156e68e [DOI] [PubMed] [Google Scholar]
- 209.Jongmans MC, Hoefsloot LH, van der Donk KP, Admiraal RJ, Magee A, van de Laar I, Hendriks Y, Verheij JB, Walpole I, Brunner HG, van Ravenswaaij CM. Familial CHARGE syndrome and the CHD7 gene: a recurrent missense mutation, intrafamilial recurrence and variability. Am J Med Genet A 2008;146A:43–50. doi: 10.1002/ajmg.a.31921 [DOI] [PubMed] [Google Scholar]
- 210.Bergman JE, Janssen N, Hoefsloot LH, Jongmans MC, Hofstra RM, van Ravenswaaij-Arts CM. CHD7 mutations and CHARGE syndrome: the clinical implications of an expanding phenotype. J Med Genet 2011;48:334–342. doi: 10.1136/jmg.2010.087106 [DOI] [PubMed] [Google Scholar]
- 211.Lin AE, Birch PH, Korf BR, Tenconi R, Niimura M, Poyhonen M, Armfield Uhas K, Sigorini M, Virdis R, Romano C, Bonioli E, Wolkenstein P, Pivnick EK, Lawrence M, Friedman JM. Cardiovascular malformations and other cardiovascular abnormalities in neurofibromatosis 1. Am J Med Genet 2000;95:108–117. [DOI] [PubMed] [Google Scholar]
- 212.Allanson JE, Hall JG, Hughes HE, Preus M, Witt RD. Noonan syndrome: the changing phenotype. Am J Med Genet 1985;21:507–514. doi: 10.1002/ajmg.1320210313 [DOI] [PubMed] [Google Scholar]
- 213.Marin L da R, da Silva FT, de Sá LC, Brasil AS, Pereira A, Furquim IM, Kim CA, Bertola DR. Ocular manifestations of Noonan syndrome. Ophthalmic Genet 2012;33:1–5. doi: 10.3109/13816810.2011.593606 [DOI] [PubMed] [Google Scholar]
- 214.van Trier DC, van Nierop J, Draaisma JM, van der Burgt I, Kunst H, Croonen EA, Admiraal RJ. External ear anomalies and hearing impairment in Noonan Syndrome. Int J Pediatr Otorhinolaryngol 2015;79:874–878. doi: 10.1016/j.ijporl.2015.03.021 [DOI] [PubMed] [Google Scholar]
- 215.Shah N, Rodriguez M, Louis DS, Lindley K, Milla PJ. Feeding difficulties and foregut dysmotility in Noonan’s syndrome. Arch Dis Child 1999;81:28–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 216.Noordam C, van der Burgt I, Sweep CG, Delemarre-van de Waal HA, Sengers RC, Otten BJ. Growth hormone (GH) secretion in children with Noonan syndrome: frequently abnormal without consequences for growth or response to GH treatment. Clin Endocrinol (Oxf) 2001;54:53–59. [DOI] [PubMed] [Google Scholar]
- 217.Şıklar Z, Genens M, Poyrazoğlu Ş, Baş F, Darendeliler F, Bundak R, Aycan Z, Savaş Erdeve Ş, Çetinkaya S, Güven A, Abalı S, Atay Z, Turan S, Kara C, Can Yılmaz G, Akyürek N, Abacı A, Çelmeli G, Sarı E, Bolu S, Korkmaz HA, Şimşek E, Çatlı G, Büyükinan M, Çayır A, Evliyaoğlu O, İşgüven P, Özgen T, Hatipoğlu N, Elhan AH, Berberoğlu M. The growth characteristics of patients with noonan syndrome: results of three years of growth hormone treatment: a nationwide multicenter study. J Clin Res Pediatr Endocrinol 2016;8:305–312. doi: 10.4274/jcrpe.3013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 218.Briggs BJ, Dickerman JD. Bleeding disorders in Noonan syndrome. Pediatr Blood Cancer 2012;58:167–172. doi: 10.1002/pbc.23358 [DOI] [PubMed] [Google Scholar]
- 219.Perez Botero J, Ho TP, Rodriguez V, Khan SP, Pruthi RK, Patnaik MM. Coagulation abnormalities and haemostatic surgical outcomes in 142 patients with Noonan syndrome. Haemophilia 2017;23:e237–e240. doi: 10.1111/hae.13225 [DOI] [PubMed] [Google Scholar]
- 220.Kratz CP, Rapisuwon S, Reed H, Hasle H, Rosenberg PS. Cancer in Noonan, Costello, cardiofaciocutaneous and LEOPARD syndromes. Am J Med Genet C Semin Med Genet 2011;157C:83–89. doi: 10.1002/ajmg.c.30300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.White SW. Lymphedema in Noonan’s syndrome. Int J Dermatol 1984;23:656–657. [DOI] [PubMed] [Google Scholar]
- 222.Roberts AE, Allanson JE, Tartaglia M, Gelb BD. Noonan syndrome. Lancet 2013;381:333–342. doi: 10.1016/S0140-6736(12)61023-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 223.Shaw AC, Kalidas K, Crosby AH, Jeffery S, Patton MA. The natural history of Noonan syndrome: a long-term follow-up study. Arch Dis Child 2007;92:128–132. doi: 10.1136/adc.2006.104547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 224.Smpokou P, Tworog-Dube E, Kucherlapati RS, Roberts AE. Medical complications, clinical findings, and educational outcomes in adults with Noonan syndrome. Am J Med Genet A 2012;158A:3106–3111. doi: 10.1002/ajmg.a.35639 [DOI] [PubMed] [Google Scholar]
- 225.Tartaglia M, Gelb BD, Zenker M. Noonan syndrome and clinically related disorders. Best Pract Res Clin Endocrinol Metab 2011;25:161–179. doi: 10.1016/j.beem.2010.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226.Pierpont EI. Neuropsychological functioning in individuals with Noonan syndrome: a systematic literature review with educational and treatment recommendations. J Pediatr Neuropsychol 2016;2:14–33. [Google Scholar]
- 227.Reinker KA, Stevenson DA, Tsung A. Orthopaedic conditions in Ras/MAPK related disorders. J Pediatr Orthop 2011;31:599–605. doi: 10.1097/BPO.0b013e318220396e [DOI] [PubMed] [Google Scholar]
- 228.Marino B, Digilio MC, Toscano A, Giannotti A, Dallapiccola B. Congenital heart diseases in children with Noonan syndrome: an expanded cardiac spectrum with high prevalence of atrioventricular canal. J Pediatr 1999;135:703–706. [DOI] [PubMed] [Google Scholar]
- 229.Gelb BD, Roberts AE, Tartaglia M. Cardiomyopathies in Noonan syndrome and the other RASopathies. Prog Pediatr Cardiol 2015;39:13–19. doi: 10.1016/j.ppedcard.2015.01.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230.Cornwall JW, Green RS, Nielsen JC, Gelb BD. Frequency of aortic dilation in Noonan syndrome. Am J Cardiol 2014;113:368–371. doi: 10.1016/j.amjcard.2013.09.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 231.Ramond F, Duband S, Croisille P, Cavé H, Teyssier G, Adouard V, Touraine R. Expanding the cardiac spectrum of Noonan syndrome with RIT1 variant: left main coronary artery atresia causing sudden death. Eur J Med Genet 2017;60:299–302. doi: 10.1016/j.ejmg.2017.03.009 [DOI] [PubMed] [Google Scholar]
- 232.Mendez HM, Opitz JM. Noonan syndrome: a review. Am J Med Genet 1985;21:493–506. doi: 10.1002/ajmg.1320210312 [DOI] [PubMed] [Google Scholar]
- 233.Tartaglia M, Mehler EL, Goldberg R, Zampino G, Brunner HG, Kremer H, van der Burgt I, Crosby AH, Ion A, Jeffery S, Kalidas K, Patton MA, Kucherlapati RS, Gelb BD. Mutations in PTPN11, encoding the protein tyrosine phosphatase SHP-2, cause Noonan syndrome [published corrections appear in Nat Genet. 2002;30:123 and Nat Genet. 2001;29:491]. Nat Genet 2001;29:465–468. doi: 10.1038/ng772 [DOI] [PubMed] [Google Scholar]
- 234.Tartaglia M, Kalidas K, Shaw A, Song X, Musat DL, van der Burgt I, Brunner HG, Bertola DR, Crosby A, Ion A, Kucherlapati RS, Jeffery S, Patton MA, Gelb BD. PTPN11 mutations in Noonan syndrome: molecular spectrum, genotype-phenotype correlation, and phenotypic heterogeneity. Am J Hum Genet 2002;70:1555–1563. doi: 10.1086/340847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 235.Tidyman WE, Rauen KA. Expansion of the RASopathies. Curr Genet Med Rep 2016;4:57–64. doi: 10.1007/s40142-016-0100-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 236.Tartaglia M, Cordeddu V, Chang H, Shaw A, Kalidas K, Crosby A, Patton MA, Sorcini M, van der Burgt I, Jeffery S, Gelb BD. Paternal germline origin and sex-ratio distortion in transmission of PTPN11 mutations in Noonan syndrome. Am J Hum Genet 2004;75:492–497. doi: 10.1086/423493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 237.Roberts AE, Araki T, Swanson KD, Montgomery KT, Schiripo TA, Joshi VA, Li L, Yassin Y, Tamburino AM, Neel BG, Kucherlapati RS. Germline gain-of-function mutations in SOS1 cause Noonan syndrome. Nat Genet 2007;39:70–74. doi: 10.1038/ng1926 [DOI] [PubMed] [Google Scholar]
- 238.Razzaque MA, Nishizawa T, Komoike Y, Yagi H, Furutani M, Amo R, Kamisago M, Momma K, Katayama H, Nakagawa M, Fujiwara Y, Matsushima M, Mizuno K, Tokuyama M, Hirota H, Muneuchi J, Higashinakagawa T, Matsuoka R. Germline gain-of-function mutations in RAF1 cause Noonan syndrome. Nat Genet 2007;39:1013–1017. doi: 10.1038/ng2078 [DOI] [PubMed] [Google Scholar]
- 239.Yaoita M, Niihori T, Mizuno S, Okamoto N, Hayashi S, Watanabe A, Yokozawa M, Suzumura H, Nakahara A, Nakano Y, Hokosaki T, Ohmori A, Sawada H, Migita O, Mima A, Lapunzina P, Santos-Simarro F, García-Miñaúr S, Ogata T, Kawame H, Kurosawa K, Ohashi H, Inoue S, Matsubara Y, Kure S, Aoki Y. Spectrum of mutations and genotype-phenotype analysis in Noonan syndrome patients with RIT1 mutations. Hum Genet 2016;135:209–222. doi: 10.1007/s00439-015-1627-5. [DOI] [PubMed] [Google Scholar]
- 240.Siegel DH, McKenzie J, Frieden IJ, Rauen KA. Dermatological findings in 61 mutation-positive individuals with cardiofaciocutaneous syndrome. Br J Dermatol 2011;164:521–529. doi: 10.1111/j.1365-2133.2010.10122.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 241.Abe Y, Aoki Y, Kuriyama S, Kawame H, Okamoto N, Kurosawa K, Ohashi H, Mizuno S, Ogata T, Kure S, Niihori T, Matsubara Y; Costello and CFC Syndrome Study Group in Japan. Prevalence and clinical features of Costello syndrome and cardio-facio-cutaneous syndrome in Japan: findings from a nationwide epidemiological survey. Am J Med Genet A 2012;158A:1083–1094. doi: 10.1002/ajmg.a.35292 [DOI] [PubMed] [Google Scholar]
- 242.Gripp KW, Lin AE. Costello syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, Bird TD, Ledbetter N, Mefford HC, Smith RJH, Stephens K, eds. GeneReviews® Seattle, WA: University of Washington, Seattle; 1993. [Google Scholar]
- 243.Martínez-Quintana E, Rodríguez-González F. LEOPARD syndrome: clinical features and gene mutations. Mol Syndromol 2012;3:145–157. doi: 10.1159/000342251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 244.Sarkozy A, Digilio MC, Dallapiccola B. Leopard syndrome. Orphanet J Rare Dis 2008;3:13. doi: 10.1186/1750-1172-3-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 245.Jhang WK, Choi JH, Lee BH, Kim GH, Yoo HW. Cardiac manifestations and associations with gene mutations in patients diagnosed with RASopathies. Pediatr Cardiol 2016;37:1539–1547. doi: 10.1007/s00246-016-1468-6 [DOI] [PubMed] [Google Scholar]
- 246.Limongelli G, Pacileo G, Marino B, Digilio MC, Sarkozy A, Elliott P, Versacci P, Calabro P, De Zorzi A, Di Salvo G, Syrris P, Patton M, McKenna WJ, Dallapiccola B, Calabro R. Prevalence and clinical significance of cardiovascular abnormalities in patients with the LEOPARD syndrome. Am J Cardiol 2007;100:736–741. doi: 10.1016/j.amjcard.2007.03.093 [DOI] [PubMed] [Google Scholar]
- 247.Sol-Church K, Gripp KW. The molecular basis of the Costello syndrome. In: Zenker M, ed. Noonan Syndrome and Related Disorders Basel, Switzerland: Karger; 2009(17):94–103. [Google Scholar]
- 248.Kontaridis MI, Swanson KD, David FS, Barford D, Neel BG. PTPN11 (Shp2) mutations in LEOPARD syndrome have dominant negative, not activating, effects. J Biol Chem 2006;281:6785–6792. doi: 10.1074/jbc.M513068200 [DOI] [PubMed] [Google Scholar]
- 249.Yoshiba S, Hamada H. Roles of cilia, fluid flow, and Ca2+ signaling in breaking of left-right symmetry. Trends Genet 2014;30:10–17. doi: 10.1016/j.tig.2013.09.001 [DOI] [PubMed] [Google Scholar]
- 250.Burnicka-Turek O, Steimle JD, Huang W, Felker L, Kamp A, Kweon J, Peterson M, Reeves RH, Maslen CL, Gruber PJ, Yang XH, Shendure J, Moskowitz IP. Cilia gene mutations cause atrioventricular septal defects by multiple mechanisms. Hum Mol Genet 2016;25:3011–3028. doi: 10.1093/hmg/ddw155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251.Li Y, Klena NT, Gabriel GC, Liu X, Kim AJ, Lemke K, Chen Y, Chatterjee B, Devine W, Damerla RR, Chang C, Yagi H, San Agustin JT, Thahir M, Anderton S, Lawhead C, Vescovi A, Pratt H, Morgan J, Haynes L, Smith CL, Eppig JT, Reinholdt L, Francis R, Leatherbury L, Ganapathiraju MK, Tobita K, Pazour GJ, Lo CW. Global genetic analysis in mice unveils central role for cilia in congenital heart disease. Nature 2015;521:520–524. doi: 10.1038/nature14269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 252.Fliegauf M, Benzing T, Omran H. When cilia go bad: cilia defects and ciliopathies [published correction appears in Nat Rev Mol Cell Biol. 2008;9:88]. Nat Rev Mol Cell Biol 2007;8:880–893. doi: 10.1038/nrm2278 [DOI] [PubMed] [Google Scholar]
- 253.Essner JJ, Vogan KJ, Wagner MK, Tabin CJ, Yost HJ, Brueckner M. Conserved function for embryonic nodal cilia. Nature 2002;418:37–38. doi: 10.1038/418037a [DOI] [PubMed] [Google Scholar]
- 254.Nonaka S, Tanaka Y, Okada Y, Takeda S, Harada A, Kanai Y, Kido M, Hirokawa N. Randomization of left-right asymmetry due to loss of nodal cilia generating leftward flow of extraembryonic fluid in mice lacking KIF3B motor protein [published correction appears in Cell. 1999;99:117]. Cell 1998;95:829–837. [DOI] [PubMed] [Google Scholar]
- 255.McGrath J, Somlo S, Makova S, Tian X, Brueckner M. Two populations of node monocilia initiate left-right asymmetry in the mouse. Cell 2003;114:61–73. [DOI] [PubMed] [Google Scholar]
- 256.Yoshiba S, Shiratori H, Kuo IY, Kawasumi A, Shinohara K, Nonaka S, Asai Y, Sasaki G, Belo JA, Sasaki H, Nakai J, Dworniczak B, Ehrlich BE, Pennekamp P, Hamada H. Cilia at the node of mouse embryos sense fluid flow for left-right determination via Pkd2. Science 2012;338:226–231. doi: 10.1126/science.1222538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 257.Hamada H, Tam PP. Mechanisms of left-right asymmetry and patterning: driver, mediator and responder. F1000Prime Rep 2014;6:110. doi: 10.12703/P6-110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 258.Stone DL, Slavotinek A, Bouffard GG, Banerjee-Basu S, Baxevanis AD, Barr M, Biesecker LG. Mutation of a gene encoding a putative chaperonin causes McKusick-Kaufman syndrome. Nat Genet 2000;25:79–82. doi: 10.1038/75637 [DOI] [PubMed] [Google Scholar]
- 259.Sund KL, Roelker S, Ramachandran V, Durbin L, Benson DW. Analysis of Ellis van Creveld syndrome gene products: implications for cardiovascular development and disease. Hum Mol Genet 2009;18:1813–1824. doi: 10.1093/hmg/ddp098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 260.Tompson SW, Ruiz-Perez VL, Blair HJ, Barton S, Navarro V, Robson JL, Wright MJ, Goodship JA. Sequencing EVC and EVC2 identifies mutations in two-thirds of Ellis-van Creveld syndrome patients. Hum Genet 2007;120:663–670. doi: 10.1007/s00439-006-0237-7 [DOI] [PubMed] [Google Scholar]
- 261.Slough J, Cooney L, Brueckner M. Monocilia in the embryonic mouse heart suggest a direct role for cilia in cardiac morphogenesis. Dev Dyn 2008;237:2304–2314. doi: 10.1002/dvdy.21669 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 262.Goetz JG, Steed E, Ferreira RR, Roth S, Ramspacher C, Boselli F, Charvin G, Liebling M, Wyart C, Schwab Y, Vermot J. Endothelial cilia mediate low flow sensing during zebrafish vascular development. Cell Rep 2014;6:799–808. doi: 10.1016/j.celrep.2014.01.032 [DOI] [PubMed] [Google Scholar]
- 263.Sutherland MJ, Ware SM. Disorders of left-right asymmetry: heterotaxy and situs inversus. Am J Med Genet C Semin Med Genet 2009;151C:307–317. doi: 10.1002/ajmg.c.30228 [DOI] [PubMed] [Google Scholar]
- 264.Ticho BS, Goldstein AM, Van Praagh R. Extracardiac anomalies in the heterotaxy syndromes with focus on anomalies of midline-associated structures. Am J Cardiol 2000;85:729–734 [DOI] [PubMed] [Google Scholar]
- 265.Lin AE, Krikov S, Riehle-Colarusso T, Frías JL, Belmont J, Anderka M, Geva T, Getz KD, Botto LD; National Birth Defects Prevention Study. Laterality defects in the national birth defects prevention study (1998–2007): birth prevalence and descriptive epidemiology. Am J Med Genet A 2014;164A:2581–2591. doi: 10.1002/ajmg.a.36695 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 266.Shapiro AJ, Tolleson-Rinehart S, Zariwala MA, Knowles MR, Leigh MW. The prevalence of clinical features associated with primary ciliary dyskinesia in a heterotaxy population: results of a web-based survey. Cardiol Young 2015;25:752–759. doi: 10.1017/S1047951114000912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 267.Song MS, Hu A, Dyamenahalli U, Chitayat D, Winsor EJ, Ryan G, Smallhorn J, Barrett J, Yoo SJ, Hornberger LK. Extracardiac lesions and chromosomal abnormalities associated with major fetal heart defects: comparison of intrauterine, postnatal and postmortem diagnoses. Ultrasound Obstet Gynecol 2009;33:552–559. doi: 10.1002/uog.6309 [DOI] [PubMed] [Google Scholar]
- 268.Cowan JR, Tariq M, Shaw C, Rao M, Belmont JW, Lalani SR, Smolarek TA, Ware SM. Copy number variation as a genetic basis for heterotaxy and heterotaxy-spectrum congenital heart defects. Philos Trans R Soc Lond B Biol Sci 2016;371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 269.Rigler SL, Kay DM, Sicko RJ, Fan R, Liu A, Caggana M, Browne ML, Druschel CM, Romitti PA, Brody LC, Mills JL. Novel copy-number variants in a population-based investigation of classic heterotaxy. Genet Med 2015;17:348–357. doi: 10.1038/gim.2014.112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 270.Lander J, Ware SM. Copy number variation in congenital heart defects. Curr Genet Med Rep 2014;2:168–178. [Google Scholar]
- 271.Fakhro KA, Choi M, Ware SM, Belmont JW, Towbin JA, Lifton RP, Khokha MK, Brueckner M. Rare copy number variations in congenital heart disease patients identify unique genes in left-right patterning. Proc Natl Acad Sci U S A 2011;108:2915–2920. doi: 10.1073/pnas.1019645108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 272.Hagen EM, Sicko RJ, Kay DM, Rigler SL, Dimopoulos A, Ahmad S, Doleman MH, Fan R, Romitti PA, Browne ML, Caggana M, Brody LC, Shaw GM, Jelliffe-Pawlowski LL, Mills JL. Copy-number variant analysis of classic heterotaxy highlights the importance of body patterning pathways. Hum Genet 2016;135:1355–1364. doi: 10.1007/s00439-016-1727-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 273.Øyen N, Poulsen G, Boyd HA, Wohlfahrt J, Jensen PK, Melbye M. Recurrence of congenital heart defects in families. Circulation 2009;120:295–301. doi: 10.1161/CIRCULATIONAHA.109.857987 [DOI] [PubMed] [Google Scholar]
- 274.Homsy J, Zaidi S, Shen Y, Ware JS, Samocha KE, Karczewski KJ, DePalma SR, McKean D, Wakimoto H, Gorham J, Jin SC, Deanfield J, Giardini A, Porter GA Jr, Kim R, Bilguvar K, López-Giráldez F, Tikhonova I, Mane S, Romano-Adesman A, Qi H, Vardarajan B, Ma L, Daly M, Roberts AE, Russell MW, Mital S, Newburger JW, Gaynor JW, Breitbart RE, Iossifov I, Ronemus M, Sanders SJ, Kaltman JR, Seidman JG, Brueckner M, Gelb BD, Goldmuntz E, Lifton RP, Seidman CE, Chung WK. De novo mutations in congenital heart disease with neurodevelopmental and other congenital anomalies. Science 2015;350:1262–1266. doi: 10.1126/science.aac9396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 275.Zaidi S, Choi M, Wakimoto H, Ma L, Jiang J, Overton JD, Romano-Adesman A, Bjornson RD, Breitbart RE, Brown KK, Carriero NJ, Cheung YH, Deanfield J, DePalma S, Fakhro KA, Glessner J, Hakonarson H, Italia MJ, Kaltman JR, Kaski J, Kim R, Kline JK, Lee T, Leipzig J, Lopez A, Mane SM, Mitchell LE, Newburger JW, Parfenov M, Pe’er I, Porter G, Roberts AE, Sachidanandam R, Sanders SJ, Seiden HS, State MW, Subramanian S, Tikhonova IR, Wang W, Warburton D, White PS, Williams IA, Zhao H, Seidman JG, Brueckner M, Chung WK, Gelb BD, Goldmuntz E, Seidman CE, Lifton RP. De novo mutations in histone-modifying genes in congenital heart disease. Nature 2013;498:220–223. doi: 10.1038/nature12141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 276.Sutherland MJ, Wang S, Quinn ME, Haaning A, Ware SM. Zic3 is required in the migrating primitive streak for node morphogenesis and left-right patterning. Hum Mol Genet 2013;22:1913–1923. doi: 10.1093/hmg/ddt001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 277.Bedard JE, Haaning AM, Ware SM. Identification of a novel ZIC3 isoform and mutation screening in patients with heterotaxy and congenital heart disease. PLoS One 2011;6:e23755. doi: 10.1371/journal.pone.0023755 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 278.Cowan J, Tariq M, Ware SM. Genetic and functional analyses of ZIC3 variants in congenital heart disease. Hum Mutat 2014;35:66–75. doi: 10.1002/humu.22457 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 279.Ware SM, Peng J, Zhu L, Fernbach S, Colicos S, Casey B, Towbin J, Belmont JW. Identification and functional analysis of ZIC3 mutations in heterotaxy and related congenital heart defects. Am J Hum Genet 2004;74:93–105. doi: 10.1086/380998 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 280.Gebbia M, Ferrero GB, Pilia G, Bassi MT, Aylsworth A, Penman-Splitt M, Bird LM, Bamforth JS, Burn J, Schlessinger D, Nelson DL, Casey B. X-linked situs abnormalities result from mutations in ZIC3. Nat Genet 1997;17:305–308. doi: 10.1038/ng1197-305 [DOI] [PubMed] [Google Scholar]
- 281.Paulussen AD, Steyls A, Vanoevelen J, van Tienen FH, Krapels IP, Claes GR, Chocron S, Velter C, Tan-Sindhunata GM, Lundin C, Valenzuela I, Nagy B, Bache I, Maroun LL, Avela K, Brunner HG, Smeets HJ, Bakkers J, van den Wijngaard A. Rare novel variants in the ZIC3 gene cause X-linked heterotaxy. Eur J Hum Genet 2016;24:1783–1791. doi: 10.1038/ejhg.2016.91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 282.Mégarbané A, Salem N, Stephan E, Ashoush R, Lenoir D, Delague V, Kassab R, Loiselet J, Bouvagnet P. X-linked transposition of the great arteries and incomplete penetrance among males with a nonsense mutation in ZIC3. Eur J Hum Genet 2000;8:704–708. doi: 10.1038/sj.ejhg.5200526 [DOI] [PubMed] [Google Scholar]
- 283.Mohapatra B, Casey B, Li H, Ho-Dawson T, Smith L, Fernbach SD, Molinari L, Niesh SR, Jefferies JL, Craigen WJ, Towbin JA, Belmont JW, Ware SM. Identification and functional characterization of NODAL rare variants in heterotaxy and isolated cardiovascular malformations. Hum Mol Genet 2009;18:861–871. doi: 10.1093/hmg/ddn411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 284.Goldmuntz E, Bamford R, Karkera JD, dela Cruz J, Roessler E, Muenke M. CFC1 mutations in patients with transposition of the great arteries and double-outlet right ventricle. Am J Hum Genet 2002;70:776–780. doi: 10.1086/339079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 285.Roessler E, Ouspenskaia MV, Karkera JD, Vélez JI, Kantipong A, Lacbawan F, Bowers P, Belmont JW, Towbin JA, Goldmuntz E, Feldman B, Muenke M. Reduced NODAL signaling strength via mutation of several pathway members including FOXH1 is linked to human heart defects and holoprosencephaly. Am J Hum Genet 2008;83:18–29. doi: 10.1016/j.ajhg.2008.05.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286.Afzelius BA. A human syndrome caused by immotile cilia. Science 1976;193:317–319. [DOI] [PubMed] [Google Scholar]
- 287.Lucas JS, Barbato A, Collins SA, Goutaki M, Behan L, Caudri D, Dell S, Eber E, Escudier E, Hirst RA, Hogg C, Jorissen M, Latzin P, Legendre M, Leigh MW, Midulla F, Nielsen KG, Omran H, Papon JF, Pohunek P, Redfern B, Rigau D, Rindlisbacher B, Santamaria F, Shoemark A, Snijders D, Tonia T, Titieni A, Walker WT, Werner C, Bush A, Kuehni CE. European Respiratory Society guidelines for the diagnosis of primary ciliary dyskinesia. Eur Respir J 2017;49:1601090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 288.Kennedy MP, Omran H, Leigh MW, Dell S, Morgan L, Molina PL, Robinson BV, Minnix SL, Olbrich H, Severin T, Ahrens P, Lange L, Morillas HN, Noone PG, Zariwala MA, Knowles MR. Congenital heart disease and other heterotaxic defects in a large cohort of patients with primary ciliary dyskinesia. Circulation 2007;115:2814–2821. doi: 10.1161/CIRCULATIONAHA.106.649038 [DOI] [PubMed] [Google Scholar]
- 289.Shapiro AJ, Davis SD, Ferkol T, Dell SD, Rosenfeld M, Olivier KN, Sagel SD, Milla C, Zariwala MA, Wolf W, Carson JL, Hazucha MJ, Burns K, Robinson B, Knowles MR, Leigh MW; Genetic Disorders of Mucociliary Clearance Consortium. Laterality defects other than situs inversus totalis in primary ciliary dyskinesia: insights into situs ambiguus and heterotaxy. Chest 2014;146:1176–1186. doi: 10.1378/chest.13-1704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 290.Paff T, Loges NT, Aprea I, Wu K, Bakey Z, Haarman EG, Daniels JMA, Sistermans EA, Bogunovic N, Dougherty GW, Höben IM, Große-Onnebrink J, Matter A, Olbrich H, Werner C, Pals G, Schmidts M, Omran H, Micha D. Mutations in PIH1D3 cause X-linked primary ciliary dyskinesia with outer and inner dynein arm defects. Am J Hum Genet 2017;100:160–168. doi: 10.1016/j.ajhg.2016.11.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 291.Bachmann-Gagescu R, Dempsey JC, Phelps IG, O’Roak BJ, Knutzen DM, Rue TC, Ishak GE, Isabella CR, Gorden N, Adkins J, Boyle EA, de Lacy N, O’Day D, Alswaid A, Ramadevi A R, Lingappa L, Lourenço C, Martorell L, Garcia-Cazorla À, Ozyürek H, Haliloğlu G, Tuysuz B, Topçu M, Chance P, Parisi MA, Glass IA, Shendure J, Doherty D; University of Washington Center for Mendelian Genomics. Joubert syndrome: a model for untangling recessive disorders with extreme genetic heterogeneity. J Med Genet 2015;52:514–522. doi: 10.1136/jmedgenet-2015-103087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 292.Oud MM, Lamers IJ, Arts HH. Ciliopathies: genetics in pediatric medicine. J Pediatr Genet 2017;6:18–29. doi: 10.1055/s-0036-1593841 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 293.Reiter JF, Leroux MR. Genes and molecular pathways underpinning ciliopathies. Nat Rev Mol Cell Biol 2017;18:533–547. doi: 10.1038/nrm.2017.60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 294.Bruel AL, Franco B, Duffourd Y, Thevenon J, Jego L, Lopez E, Deleuze JF, Doummar D, Giles RH, Johnson CA, Huynen MA, Chevrier V, Burglen L, Morleo M, Desguerres I, Pierquin G, Doray B, Gilbert-Dussardier B, Reversade B, Steichen-Gersdorf E, Baumann C, Panigrahi I, Fargeot-Espaliat A, Dieux A, David A, Goldenberg A, Bongers E, Gaillard D, Argente J, Aral B, Gigot N, St-Onge J, Birnbaum D, Phadke SR, Cormier-Daire V, Eguether T, Pazour GJ, Herranz-Pérez V, Goldstein JS, Pasquier L, Loget P, Saunier S, Mégarbané A, Rosnet O, Leroux MR, Wallingford JB, Blacque OE, Nachury MV, Attie-Bitach T, Rivière JB, Faivre L, Thauvin-Robinet C. Fifteen years of research on oral-facial-digital syndromes: from 1 to 16 causal genes. J Med Genet 2017;54:371–380. doi: 10.1136/jmedgenet-2016-104436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 295.Franco B, Thauvin-Robinet C. Update on oral-facial-digital syndromes (OFDS). Cilia 2016;5:12. doi: 10.1186/s13630-016-0034-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 296.Parisi MA. Clinical and molecular features of Joubert syndrome and related disorders. Am J Med Genet C Semin Med Genet 2009;151C:326–340. doi: 10.1002/ajmg.c.30229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 297.Kaasinen E, Aittomäki K, Eronen M, Vahteristo P, Karhu A, Mecklin JP, Kajantie E, Aaltonen LA, Lehtonen R. Recessively inherited right atrial isomerism caused by mutations in growth/differentiation factor 1 (GDF1). Hum Mol Genet 2010;19:2747–2753. doi: 10.1093/hmg/ddq164 [DOI] [PubMed] [Google Scholar]
- 298.Otto EA, Schermer B, Obara T, O’Toole JF, Hiller KS, Mueller AM, Ruf RG, Hoefele J, Beekmann F, Landau D, Foreman JW, Goodship JA, Strachan T, Kispert A, Wolf MT, Gagnadoux MF, Nivet H, Antignac C, Walz G, Drummond IA, Benzing T, Hildebrandt F. Mutations in INVS encoding inversin cause nephronophthisis type 2, linking renal cystic disease to the function of primary cilia and left-right axis determination. Nat Genet 2003;34:413–420. doi: 10.1038/ng1217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 299.Okada M, Sugimoto K, Shimada Y, Fujita S, Yanagida H, Yagi K, Takemura T. Association of INVS (NPHP2) mutation in an adolescent exhibiting nephronophthisis (NPH) and complete situs inversus. Clin Nephrol 2008;69:135–141. [DOI] [PubMed] [Google Scholar]
- 300.van Bon BW, Koolen DA, Pfundt R, van der Burgt I, de Leeuw N, de Vries BB. Transposition of the great vessels in a patient with a 2.9 Mb interstitial deletion of 9q31.1 encompassing the inversin gene: clinical report and review. Am J Med Genet A 2008;146A:1225–1229. doi: 10.1002/ajmg.a.32289 [DOI] [PubMed] [Google Scholar]
- 301.Chaki M, Hoefele J, Allen SJ, Ramaswami G, Janssen S, Bergmann C, Heckenlively JR, Otto EA, Hildebrandt F. Genotype-phenotype correlation in 440 patients with NPHP-related ciliopathies. Kidney Int 2011;80:1239–1245. doi: 10.1038/ki.2011.284 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 302.Bergmann C, Fliegauf M, Brüchle NO, Frank V, Olbrich H, Kirschner J, Schermer B, Schmedding I, Kispert A, Kränzlin B, Nürnberg G, Becker C, Grimm T, Girschick G, Lynch SA, Kelehan P, Senderek J, Neuhaus TJ, Stallmach T, Zentgraf H, Nürnberg P, Gretz N, Lo C, Lienkamp S, Schäfer T, Walz G, Benzing T, Zerres K, Omran H. Loss of nephrocystin-3 function can cause embryonic lethality, Meckel-Gruber-like syndrome, situs inversus, and renal-hepatic-pancreatic dysplasia. Am J Hum Genet 2008;82:959–970. doi: 10.1016/j.ajhg.2008.02.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 303.Hoff S, Halbritter J, Epting D, Frank V, Nguyen TM, van Reeuwijk J, Boehlke C, Schell C, Yasunaga T, Helmstädter M, Mergen M, Filhol E, Boldt K, Horn N, Ueffing M, Otto EA, Eisenberger T, Elting MW, van Wijk JA, Bockenhauer D, Sebire NJ, Rittig S, Vyberg M, Ring T, Pohl M, Pape L, Neuhaus TJ, Elshakhs NA, Koon SJ, Harris PC, Grahammer F, Huber TB, Kuehn EW, Kramer-Zucker A, Bolz HJ, Roepman R, Saunier S, Walz G, Hildebrandt F, Bergmann C, Lienkamp SS. ANKS6 is a central component of a nephronophthisis module linking NEK8 to INVS and NPHP3. Nat Genet 2013;45:951–956. doi: 10.1038/ng.2681 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 304.Frank V, Habbig S, Bartram MP, Eisenberger T, Veenstra-Knol HE, Decker C, Boorsma RA, Göbel H, Nürnberg G, Griessmann A, Franke M, Borgal L, Kohli P, Völker LA, Dötsch J, Nürnberg P, Benzing T, Bolz HJ, Johnson C, Gerkes EH, Schermer B, Bergmann C. Mutations in NEK8 link multiple organ dysplasia with altered Hippo signalling and increased c-MYC expression. Hum Mol Genet 2013;22:2177–2185. doi: 10.1093/hmg/ddt070 [DOI] [PubMed] [Google Scholar]
- 305.Mitchison HM, Schmidts M, Loges NT, Freshour J, Dritsoula A, Hirst RA, O’Callaghan C, Blau H, Al Dabbagh M, Olbrich H, Beales PL, Yagi T, Mussaffi H, Chung EM, Omran H, Mitchell DR. Mutations in axonemal dynein assembly factor DNAAF3 cause primary ciliary dyskinesia. Nat Genet 2012;44:381–9, S1. doi: 10.1038/ng.1106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 306.Merveille AC, Davis EE, Becker-Heck A, Legendre M, Amirav I, Bataille G, Belmont J, Beydon N, Billen F, Clément A, Clercx C, Coste A, Crosbie R, de Blic J, Deleuze S, Duquesnoy P, Escalier D, Escudier E, Fliegauf M, Horvath J, Hill K, Jorissen M, Just J, Kispert A, Lathrop M, Loges NT, Marthin JK, Momozawa Y, Montantin G, Nielsen KG, Olbrich H, Papon JF, Rayet I, Roger G, Schmidts M, Tenreiro H, Towbin JA, Zelenika D, Zentgraf H, Georges M, Lequarré AS, Katsanis N, Omran H, Amselem S. CCDC39 is required for assembly of inner dynein arms and the dynein regulatory complex and for normal ciliary motility in humans and dogs. Nat Genet 2011;43:72–78. doi: 10.1038/ng.726 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 307.Becker-Heck A, Zohn IE, Okabe N, Pollock A, Lenhart KB, Sullivan-Brown J, McSheene J, Loges NT, Olbrich H, Haeffner K, Fliegauf M, Horvath J, Reinhardt R, Nielsen KG, Marthin JK, Baktai G, Anderson KV, Geisler R, Niswander L, Omran H, Burdine RD. The coiled-coil domain containing protein CCDC40 is essential for motile cilia function and left-right axis formation. Nat Genet 2011;43:79–84. doi: 10.1038/ng.727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 308.Panizzi JR, Becker-Heck A, Castleman VH, Al-Mutairi DA, Liu Y, Loges NT, Pathak N, Austin-Tse C, Sheridan E, Schmidts M, Olbrich H, Werner C, Häffner K, Hellman N, Chodhari R, Gupta A, Kramer-Zucker A, Olale F, Burdine RD, Schier AF, O’Callaghan C, Chung EM, Reinhardt R, Mitchison HM, King SM, Omran H, Drummond IA. CCDC103 mutations cause primary ciliary dyskinesia by disrupting assembly of ciliary dynein arms. Nat Genet 2012;44:714–719. doi: 10.1038/ng.2277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 309.Horani A, Druley TE, Zariwala MA, Patel AC, Levinson BT, Van Arendonk LG, Thornton KC, Giacalone JC, Albee AJ, Wilson KS, Turner EH, Nickerson DA, Shendure J, Bayly PV, Leigh MW, Knowles MR, Brody SL, Dutcher SK, Ferkol TW. Whole-exome capture and sequencing identifies HEATR2 mutation as a cause of primary ciliary dyskinesia. Am J Hum Genet 2012;91:685–693. doi: 10.1016/j.ajhg.2012.08.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 310.Hjeij R, Lindstrand A, Francis R, Zariwala MA, Liu X, Li Y, Damerla R, Dougherty GW, Abouhamed M, Olbrich H, Loges NT, Pennekamp P, Davis EE, Carvalho CM, Pehlivan D, Werner C, Raidt J, Köhler G, Häffner K, Reyes-Mugica M, Lupski JR, Leigh MW, Rosenfeld M, Morgan LC, Knowles MR, Lo CW, Katsanis N, Omran H. ARMC4 mutations cause primary ciliary dyskinesia with randomization of left/right body asymmetry. Am J Hum Genet 2013;93:357–367. doi: 10.1016/j.ajhg.2013.06.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 311.Tarkar A, Loges NT, Slagle CE, Francis R, Dougherty GW, Tamayo JV, Shook B, Cantino M, Schwartz D, Jahnke C, Olbrich H, Werner C, Raidt J, Pennekamp P, Abouhamed M, Hjeij R, Köhler G, Griese M, Li Y, Lemke K, Klena N, Liu X, Gabriel G, Tobita K, Jaspers M, Morgan LC, Shapiro AJ, Letteboer SJ, Mans DA, Carson JL, Leigh MW, Wolf WE, Chen S, Lucas JS, Onoufriadis A, Plagnol V, Schmidts M, Boldt K, Roepman R, Zariwala MA, Lo CW, Mitchison HM, Knowles MR, Burdine RD, Loturco JJ, Omran H; UK10K. DYX1C1 is required for axonemal dynein assembly and ciliary motility. Nat Genet 2013;45:995–1003. doi: 10.1038/ng.2707 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 312.Austin-Tse C, Halbritter J, Zariwala MA, Gilberti RM, Gee HY, Hellman N, Pathak N, Liu Y, Panizzi JR, Patel-King RS, Tritschler D, Bower R, O’Toole E, Porath JD, Hurd TW, Chaki M, Diaz KA, Kohl S, Lovric S, Hwang DY, Braun DA, Schueler M, Airik R, Otto EA, Leigh MW, Noone PG, Carson JL, Davis SD, Pittman JE, Ferkol TW, Atkinson JJ, Olivier KN, Sagel SD, Dell SD, Rosenfeld M, Milla CE, Loges NT, Omran H, Porter ME, King SM, Knowles MR, Drummond IA, Hildebrandt F. Zebrafish ciliopathy screen plus human mutational analysis identifies C21orf59 and CCDC65 defects as causing primary ciliary dyskinesia. Am J Hum Genet 2013;93:672–686. doi: 10.1016/j.ajhg.2013.08.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 313.Knowles MR, Ostrowski LE, Loges NT, Hurd T, Leigh MW, Huang L, Wolf WE, Carson JL, Hazucha MJ, Yin W, Davis SD, Dell SD, Ferkol TW, Sagel SD, Olivier KN, Jahnke C, Olbrich H, Werner C, Raidt J, Wallmeier J, Pennekamp P, Dougherty GW, Hjeij R, Gee HY, Otto EA, Halbritter J, Chaki M, Diaz KA, Braun DA, Porath JD, Schueler M, Baktai G, Griese M, Turner EH, Lewis AP, Bamshad MJ, Nickerson DA, Hildebrandt F, Shendure J, Omran H, Zariwala MA. Mutations in SPAG1 cause primary ciliary dyskinesia associated with defective outer and inner dynein arms. Am J Hum Genet 2013;93:711–720. doi: 10.1016/j.ajhg.2013.07.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 314.Hjeij R, Onoufriadis A, Watson CM, Slagle CE, Klena NT, Dougherty GW, Kurkowiak M, Loges NT, Diggle CP, Morante NF, Gabriel GC, Lemke KL, Li Y, Pennekamp P, Menchen T, Konert F, Marthin JK, Mans DA, Letteboer SJ, Werner C, Burgoyne T, Westermann C, Rutman A, Carr IM, O’Callaghan C, Moya E, Chung EM, Sheridan E, Nielsen KG, Roepman R, Bartscherer K, Burdine RD, Lo CW, Omran H, Mitchison HM; UK10K Consortium. CCDC151 mutations cause primary ciliary dyskinesia by disruption of the outer dynein arm docking complex formation. Am J Hum Genet 2014;95:257–274. doi: 10.1016/j.ajhg.2014.08.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 315.Duquesnoy P, Escudier E, Vincensini L, Freshour J, Bridoux AM, Coste A, Deschildre A, de Blic J, Legendre M, Montantin G, Tenreiro H, Vojtek AM, Loussert C, Clément A, Escalier D, Bastin P, Mitchell DR, Amselem S. Loss-of-function mutations in the human ortholog of Chlamydomonas reinhardtii ODA7 disrupt dynein arm assembly and cause primary ciliary dyskinesia. Am J Hum Genet 2009;85:890–896. doi: 10.1016/j.ajhg.2009.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 316.Loges NT, Olbrich H, Becker-Heck A, Häffner K, Heer A, Reinhard C, Schmidts M, Kispert A, Zariwala MA, Leigh MW, Knowles MR, Zentgraf H, Seithe H, Nürnberg G, Nürnberg P, Reinhardt R, Omran H. Deletions and point mutations of LRRC50 cause primary ciliary dyskinesia due to dynein arm defects. Am J Hum Genet 2009;85:883–889. doi: 10.1016/j.ajhg.2009.10.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 317.Omran H, Kobayashi D, Olbrich H, Tsukahara T, Loges NT, Hagiwara H, Zhang Q, Leblond G, O’Toole E, Hara C, Mizuno H, Kawano H, Fliegauf M, Yagi T, Koshida S, Miyawaki A, Zentgraf H, Seithe H, Reinhardt R, Watanabe Y, Kamiya R, Mitchell DR, Takeda H. Ktu/PF13 is required for cytoplasmic pre-assembly of axonemal dyneins. Nature 2008;456:611–616. doi: 10.1038/nature07471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 318.Hornef N, Olbrich H, Horvath J, Zariwala MA, Fliegauf M, Loges NT, Wildhaber J, Noone PG, Kennedy M, Antonarakis SE, Blouin JL, Bartoloni L, Nüsslein T, Ahrens P, Griese M, Kuhl H, Sudbrak R, Knowles MR, Reinhardt R, Omran H. DNAH5 mutations are a common cause of primary ciliary dyskinesia with outer dynein arm defects. Am J Respir Crit Care Med 2006;174:120–126. doi: 10.1164/rccm.200601-084OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 319.Duriez B, Duquesnoy P, Escudier E, Bridoux AM, Escalier D, Rayet I, Marcos E, Vojtek AM, Bercher JF, Amselem S. A common variant in combination with a nonsense mutation in a member of the thioredoxin family causes primary ciliary dyskinesia [published correction appears in Proc Natl Acad Sci U S A. 2007;104:6490.]. Proc Natl Acad Sci U S A 2007;104:3336–3341. doi: 10.1073/pnas.0611405104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 320.Wallmeier J, Shiratori H, Dougherty GW, Edelbusch C, Hjeij R, Loges NT, Menchen T, Olbrich H, Pennekamp P, Raidt J, Werner C, Minegishi K, Shinohara K, Asai Y, Takaoka K, Lee C, Griese M, Memari Y, Durbin R, Kolb-Kokocinski A, Sauer S, Wallingford JB, Hamada H, Omran H. TTC25 deficiency results in defects of the outer dynein arm docking machinery and primary ciliary dyskinesia with left-right body asymmetry randomization. Am J Hum Genet 2016;99:460–469. doi: 10.1016/j.ajhg.2016.06.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 321.Knowles MR, Leigh MW, Carson JL, Davis SD, Dell SD, Ferkol TW, Olivier KN, Sagel SD, Rosenfeld M, Burns KA, Minnix SL, Armstrong MC, Lori A, Hazucha MJ, Loges NT, Olbrich H, Becker-Heck A, Schmidts M, Werner C, Omran H, Zariwala MA; Genetic Disorders of Mucociliary Clearance Consortium. Mutations of DNAH11 in patients with primary ciliary dyskinesia with normal ciliary ultrastructure. Thorax 2012;67:433–441. doi: 10.1136/thoraxjnl-2011-200301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 322.Bartoloni L, Blouin JL, Pan Y, Gehrig C, Maiti AK, Scamuffa N, Rossier C, Jorissen M, Armengot M, Meeks M, Mitchison HM, Chung EM, Delozier-Blanchet CD, Craigen WJ, Antonarakis SE. Mutations in the DNAH11 (axonemal heavy chain dynein type 11) gene cause one form of situs inversus totalis and most likely primary ciliary dyskinesia. Proc Natl Acad Sci U S A 2002;99:10282–10286. doi: 10.1073/pnas.152337699 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 323.Zariwala MA, Leigh MW, Ceppa F, Kennedy MP, Noone PG, Carson JL, Hazucha MJ, Lori A, Horvath J, Olbrich H, Loges NT, Bridoux AM, Pennarun G, Duriez B, Escudier E, Mitchison HM, Chodhari R, Chung EM, Morgan LC, de Iongh RU, Rutland J, Pradal U, Omran H, Amselem S, Knowles MR. Mutations of DNAI1 in primary ciliary dyskinesia: evidence of founder effect in a common mutation. Am J Respir Crit Care Med 2006;174:858–866. doi: 10.1164/rccm.200603-370OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 324.Guichard C, Harricane MC, Lafitte JJ, Godard P, Zaegel M, Tack V, Lalau G, Bouvagnet P. Axonemal dynein intermediate-chain gene (DNAI1) mutations result in situs inversus and primary ciliary dyskinesia (Kartagener syndrome). Am J Hum Genet 2001;68:1030–1035. doi: 10.1086/319511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 325.Mazor M, Alkrinawi S, Chalifa-Caspi V, Manor E, Sheffield VC, Aviram M, Parvari R. Primary ciliary dyskinesia caused by homozygous mutation in DNAL1, encoding dynein light chain 1. Am J Hum Genet 2011;88:599–607. doi: 10.1016/j.ajhg.2011.03.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 326.Onoufriadis A, Paff T, Antony D, Shoemark A, Micha D, Kuyt B, Schmidts M, Petridi S, Dankert-Roelse JE, Haarman EG, Daniels JM, Emes RD, Wilson R, Hogg C, Scambler PJ, Chung EM, Pals G, Mitchison HM; UK10K. Splice-site mutations in the axonemal outer dynein arm docking complex gene CCDC114 cause primary ciliary dyskinesia. Am J Hum Genet 2013;92:88–98. doi: 10.1016/j.ajhg.2012.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 327.Kott E, Duquesnoy P, Copin B, Legendre M, Dastot-Le Moal F, Montantin G, Jeanson L, Tamalet A, Papon JF, Siffroi JP, Rives N, Mitchell V, de Blic J, Coste A, Clement A, Escalier D, Touré A, Escudier E, Amselem S. Loss-of-function mutations in LRRC6, a gene essential for proper axonemal assembly of inner and outer dynein arms, cause primary ciliary dyskinesia. Am J Hum Genet 2012;91:958–964. doi: 10.1016/j.ajhg.2012.10.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 328.Zariwala MA, Gee HY, Kurkowiak M, Al-Mutairi DA, Leigh MW, Hurd TW, Hjeij R, Dell SD, Chaki M, Dougherty GW, Adan M, Spear PC, Esteve-Rudd J, Loges NT, Rosenfeld M, Diaz KA, Olbrich H, Wolf WE, Sheridan E, Batten TF, Halbritter J, Porath JD, Kohl S, Lovric S, Hwang DY, Pittman JE, Burns KA, Ferkol TW, Sagel SD, Olivier KN, Morgan LC, Werner C, Raidt J, Pennekamp P, Sun Z, Zhou W, Airik R, Natarajan S, Allen SJ, Amirav I, Wieczorek D, Landwehr K, Nielsen K, Schwerk N, Sertic J, Köhler G, Washburn J, Levy S, Fan S, Koerner-Rettberg C, Amselem S, Williams DS, Mitchell BJ, Drummond IA, Otto EA, Omran H, Knowles MR, Hildebrandt F. ZMYND10 is mutated in primary ciliary dyskinesia and interacts with LRRC6. Am J Hum Genet 2013;93:336–345. doi: 10.1016/j.ajhg.2013.06.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 329.Moore DJ, Onoufriadis A, Shoemark A, Simpson MA, zur Lage PI, de Castro SC, Bartoloni L, Gallone G, Petridi S, Woollard WJ, Antony D, Schmidts M, Didonna T, Makrythanasis P, Bevillard J, Mongan NP, Djakow J, Pals G, Lucas JS, Marthin JK, Nielsen KG, Santoni F, Guipponi M, Hogg C, Antonarakis SE, Emes RD, Chung EM, Greene ND, Blouin JL, Jarman AP, Mitchison HM. Mutations in ZMYND10, a gene essential for proper axonemal assembly of inner and outer dynein arms in humans and flies, cause primary ciliary dyskinesia. Am J Hum Genet 2013;93:346–356. doi: 10.1016/j.ajhg.2013.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 330.Perles Z, Cinnamon Y, Ta-Shma A, Shaag A, Einbinder T, Rein AJ, Elpeleg O. A human laterality disorder associated with recessive CCDC11 mutation. J Med Genet 2012;49:386–390. doi: 10.1136/jmedgenet-2011-100457 [DOI] [PubMed] [Google Scholar]
- 331.Bataille S, Demoulin N, Devuyst O, Audrézet MP, Dahan K, Godin M, Fontès M, Pirson Y, Burtey S. Association of PKD2 (polycystin 2) mutations with left-right laterality defects. Am J Kidney Dis 2011;58:456–460. doi: 10.1053/j.ajkd.2011.05.015 [DOI] [PubMed] [Google Scholar]
- 332.Vetrini F, D’Alessandro LC, Akdemir ZC, Braxton A, Azamian MS, Eldomery MK, Miller K, Kois C, Sack V, Shur N, Rijhsinghani A, Chandarana J, Ding Y, Holtzman J, Jhangiani SN, Muzny DM, Gibbs RA, Eng CM, Hanchard NA, Harel T, Rosenfeld JA, Belmont JW, Lupski JR, Yang Y. Bi-allelic mutations in PKD1L1 are associated with laterality defects in humans. Am J Hum Genet 2016;99:886–893. doi: 10.1016/j.ajhg.2016.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 333.Durst R, Sauls K, Peal DS, deVlaming A, Toomer K, Leyne M, Salani M, Talkowski ME, Brand H, Perrocheau M, Simpson C, Jett C, Stone MR, Charles F, Chiang C, Lynch SN, Bouatia-Naji N, Delling FN, Freed LA, Tribouilloy C, Le Tourneau T, LeMarec H, Fernandez-Friera L, Solis J, Trujillano D, Ossowski S, Estivill X, Dina C, Bruneval P, Chester A, Schott JJ, Irvine KD, Mao Y, Wessels A, Motiwala T, Puceat M, Tsukasaki Y, Menick DR, Kasiganesan H, Nie X, Broome AM, Williams K, Johnson A, Markwald RR, Jeunemaitre X, Hagege A, Levine RA, Milan DJ, Norris RA, Slaugenhaupt SA. Mutations in DCHS1 cause mitral valve prolapse. Nature 2015;525:109–113. doi: 10.1038/nature14670 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 334.Dau C, Fliegauf M, Omran H, Schlensog M, Dahl E, van Roeyen CR, Kriz W, Moeller MJ, Braun GS. The atypical cadherin Dachsous1 localizes to the base of the ciliary apparatus in airway epithelia. Biochem Biophys Res Commun 2016;473:1177–1184. doi: 10.1016/j.bbrc.2016.04.036 [DOI] [PubMed] [Google Scholar]
- 335.Harden B, Tian X, Giese R, Nakhleh N, Kureshi S, Francis R, Hanumanthaiah S, Li Y, Swisher M, Kuehl K, Sami I, Olivier K, Jonas R, Lo CW, Leatherbury L. Increased postoperative respiratory complications in heterotaxy congenital heart disease patients with respiratory ciliary dysfunction. J Thorac Cardiovasc Surg 2014;147:1291–1298.e2. doi: 10.1016/j.jtcvs.2013.06.018 [DOI] [PubMed] [Google Scholar]
- 336.Horani A, Ferkol TW, Dutcher SK, Brody SL. Genetics and biology of primary ciliary dyskinesia. Paediatr Respir Rev 2016;18:18–24. doi: 10.1016/j.prrv.2015.09.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 337.Wang S, Dong Z. Primary cilia and kidney injury: current research status and future perspectives. Am J Physiol Renal Physiol 2013;305:F1085–F1098. doi: 10.1152/ajprenal.00399.2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 338.Panigrahy A, Lee V, Ceschin R, Zuccoli G, Beluk N, Khalifa O, Votava-Smith JK, DeBrunner M, Munoz R, Domnina Y, Morell V, Wearden P, Sanchez De Toledo J, Devine W, Zahid M, Lo CW. Brain dysplasia associated with ciliary dysfunction in infants with congenital heart disease. J Pediatr 2016;178:141–148.e1. doi: 10.1016/j.jpeds.2016.07.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 339.Volta F, Gerdes JM. The role of primary cilia in obesity and diabetes. Ann N Y Acad Sci 2017;1391:71–84. doi: 10.1111/nyas.13216 [DOI] [PubMed] [Google Scholar]
- 340.Andersen TA, Troelsen Kde L, Larsen LA. Of mice and men: molecular genetics of congenital heart disease. Cell Mol Life Sci 2014;71:1327–1352. doi: 10.1007/s00018-013-1430-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 341.Fahed AC, Gelb BD, Seidman JG, Seidman CE. Genetics of congenital heart disease: the glass half empty [published correction appears in Circ Res. 2013;112:e182]. Circ Res 2013;112:707–720. doi: 10.1161/CIRCRESAHA.112.300853 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 342.Sperling S, Grimm CH, Dunkel I, Mebus S, Sperling HP, Ebner A, Galli R, Lehrach H, Fusch C, Berger F, Hammer S. Identification and functional analysis of CITED2 mutations in patients with congenital heart defects. Hum Mutat 2005;26:575–582. doi: 10.1002/humu.20262 [DOI] [PubMed] [Google Scholar]
- 343.Okubo A, Miyoshi O, Baba K, Takagi M, Tsukamoto K, Kinoshita A, Yoshiura K, Kishino T, Ohta T, Niikawa N, Matsumoto N. A novel GATA4 mutation completely segregated with atrial septal defect in a large Japanese family. J Med Genet 2004;41:e97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 344.Hirayama-Yamada K, Kamisago M, Akimoto K, Aotsuka H, Nakamura Y, Tomita H, Furutani M, Imamura S, Takao A, Nakazawa M, Matsuoka R. Phenotypes with GATA4 or NKX2.5 mutations in familial atrial septal defect. Am J Med Genet A 2005;135:47–52. doi: 10.1002/ajmg.a.30684 [DOI] [PubMed] [Google Scholar]
- 345.Sarkozy A, Conti E, Neri C, D’Agostino R, Digilio MC, Esposito G, Toscano A, Marino B, Pizzuti A, Dallapiccola B. Spectrum of atrial septal defects associated with mutations of NKX2.5 and GATA4 transcription factors. J Med Genet 2005;42:e16. doi: 10.1136/jmg.2004.026740 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 346.Tomita-Mitchell A, Maslen CL, Morris CD, Garg V, Goldmuntz E. GATA4 sequence variants in patients with congenital heart disease. J Med Genet 2007;44:779–783. doi: 10.1136/jmg.2007.052183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 347.Rajagopal SK, Ma Q, Obler D, Shen J, Manichaikul A, Tomita-Mitchell A, Boardman K, Briggs C, Garg V, Srivastava D, Goldmuntz E, Broman KW, Benson DW, Smoot LB, Pu WT. Spectrum of heart disease associated with murine and human GATA4 mutation. J Mol Cell Cardiol 2007;43:677–685. doi: 10.1016/j.yjmcc.2007.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 348.Chen Y, Han ZQ, Yan WD, Tang CZ, Xie JY, Chen H, Hu DY. A novel mutation in GATA4 gene associated with dominant inherited familial atrial septal defect. J Thorac Cardiovasc Surg 2010;140:684–687. doi: 10.1016/j.jtcvs.2010.01.013 [DOI] [PubMed] [Google Scholar]
- 349.Xiang R, Fan LL, Huang H, Cao BB, Li XP, Peng DQ, Xia K. A novel mutation of GATA4 (K319E) is responsible for familial atrial septal defect and pulmonary valve stenosis. Gene 2014;534:320–323. doi: 10.1016/j.gene.2013.10.028 [DOI] [PubMed] [Google Scholar]
- 350.Chen J, Qi B, Zhao J, Liu W, Duan R, Zhang M. A novel mutation of GATA4 (K300T) associated with familial atrial septal defect. Gene 2016;575(pt 2):473–477. doi: 10.1016/j.gene.2015.09.021 [DOI] [PubMed] [Google Scholar]
- 351.Kodo K, Nishizawa T, Furutani M, Arai S, Yamamura E, Joo K, Takahashi T, Matsuoka R, Yamagishi H. GATA6 mutations cause human cardiac outflow tract defects by disrupting semaphorin-plexin signaling. Proc Natl Acad Sci U S A 2009;106:13933–13938. doi: 10.1073/pnas.0904744106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 352.Maitra M, Koenig SN, Srivastava D, Garg V. Identification of GATA6 sequence variants in patients with congenital heart defects. Pediatr Res 2010;68:281–285. doi: 10.1203/PDR.0b013e3181ed17e4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 353.Lin X, Huo Z, Liu X, Zhang Y, Li L, Zhao H, Yan B, Liu Y, Yang Y, Chen YH. A novel GATA6 mutation in patients with tetralogy of Fallot or atrial septal defect. J Hum Genet 2010;55:662–667. doi: 10.1038/jhg.2010.84 [DOI] [PubMed] [Google Scholar]
- 354.Allen HL, Flanagan SE, Shaw-Smith C, De Franco E, Akerman I, Caswell R, Ferrer J, Hattersley AT, Ellard S; International Pancreatic Agenesis Consortium. GATA6 haploinsufficiency causes pancreatic agenesis in humans. Nat Genet 2011;44:20–22. doi: 10.1038/ng.1035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 355.Yorifuji T, Kawakita R, Hosokawa Y, Fujimaru R, Yamaguchi E, Tamagawa N. Dominantly inherited diabetes mellitus caused by GATA6 haploinsufficiency: variable intrafamilial presentation. J Med Genet 2012;49:642–643. doi: 10.1136/jmedgenet-2012-101161 [DOI] [PubMed] [Google Scholar]
- 356.Muncke N, Jung C, Rüdiger H, Ulmer H, Roeth R, Hubert A, Goldmuntz E, Driscoll D, Goodship J, Schön K, Rappold G. Missense mutations and gene interruption in PROSIT240, a novel TRAP240-like gene, in patients with congenital heart defect (transposition of the great arteries). Circulation 2003;108:2843–2850. doi: 10.1161/01.CIR.0000103684.77636.CD [DOI] [PubMed] [Google Scholar]
- 357.Al Turki S, Manickaraj AK, Mercer CL, Gerety SS, Hitz MP, Lindsay S, D’Alessandro LC, Swaminathan GJ, Bentham J, Arndt AK, Louw J, Breckpot J, Gewillig M, Thienpont B, Abdul-Khaliq H, Harnack C, Hoff K, Kramer HH, Schubert S, Siebert R, Toka O, Cosgrove C, Watkins H, Lucassen AM, O’Kelly IM, Salmon AP, Bu’lock FA, Granados-Riveron J, Setchfield K, Thornborough C, Brook JD, Mulder B, Klaassen S, Bhattacharya S, Devriendt K, Fitzpatrick DF, Wilson DI, Mital S, Hurles ME; UK10K Consortium. Rare variants in NR2F2 cause congenital heart defects in humans [published correction appears in Am J Hum Genet. 2014;95:126]. Am J Hum Genet 2014;94:574–585. doi: 10.1016/j.ajhg.2014.03.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 358.Schott JJ, Benson DW, Basson CT, Pease W, Silberbach GM, Moak JP, Maron BJ, Seidman CE, Seidman JG. Congenital heart disease caused by mutations in the transcription factor NKX2–5. Science 1998;281:108–111. [DOI] [PubMed] [Google Scholar]
- 359.Benson DW, Silberbach GM, Kavanaugh-McHugh A, Cottrill C, Zhang Y, Riggs S, Smalls O, Johnson MC, Watson MS, Seidman JG, Seidman CE, Plowden J, Kugler JD. Mutations in the cardiac transcription factor NKX2.5 affect diverse cardiac developmental pathways. J Clin Invest 1999;104:1567–1573. doi: 10.1172/JCI8154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 360.Goldmuntz E, Geiger E, Benson DW. NKX2.5 mutations in patients with tetralogy of Fallot. Circulation 2001;104:2565–2568. [DOI] [PubMed] [Google Scholar]
- 361.McElhinney DB, Geiger E, Blinder J, Benson DW, Goldmuntz E. NKX2.5 mutations in patients with congenital heart disease. J Am Coll Cardiol 2003;42:1650–1655. [DOI] [PubMed] [Google Scholar]
- 362.Stallmeyer B, Fenge H, Nowak-Göttl U, Schulze-Bahr E. Mutational spectrum in the cardiac transcription factor gene NKX2.5 (CSX) associated with congenital heart disease. Clin Genet 2010;78:533–540. doi: 10.1111/j.1399-0004.2010.01422.x [DOI] [PubMed] [Google Scholar]
- 363.Ellesøe SG, Johansen MM, Bjerre JV, Hjortdal VE, Brunak S, Larsen LA. Familial atrial septal defect and sudden cardiac death: identification of a novel NKX2–5 mutation and a review of the literature. Congenit Heart Dis 2016;11:283–290. doi: 10.1111/chd.12317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 364.Heathcote K, Braybrook C, Abushaban L, Guy M, Khetyar ME, Patton MA, Carter ND, Scambler PJ, Syrris P. Common arterial trunk associated with a homeodomain mutation of NKX2.6. Hum Mol Genet 2005;14:585–593. doi: 10.1093/hmg/ddi055 [DOI] [PubMed] [Google Scholar]
- 365.Ta-Shma A, El-lahham N, Edvardson S, Stepensky P, Nir A, Perles Z, Gavri S, Golender J, Yaakobi-Simhayoff N, Shaag A, Rein AJ, Elpeleg O. Conotruncal malformations and absent thymus due to a deleterious NKX2–6 mutation. J Med Genet 2014;51:268–270. doi: 10.1136/jmedgenet-2013-102100 [DOI] [PubMed] [Google Scholar]
- 366.Kirk EP, Sunde M, Costa MW, Rankin SA, Wolstein O, Castro ML, Butler TL, Hyun C, Guo G, Otway R, Mackay JP, Waddell LB, Cole AD, Hayward C, Keogh A, Macdonald P, Griffiths L, Fatkin D, Sholler GF, Zorn AM, Feneley MP, Winlaw DS, Harvey RP. Mutations in cardiac T-box factor gene TBX20 are associated with diverse cardiac pathologies, including defects of septation and valvulogenesis and cardiomyopathy. Am J Hum Genet 2007;81:280–291. doi: 10.1086/519530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 367.Pan Y, Geng R, Zhou N, Zheng GF, Zhao H, Wang J, Zhao CM, Qiu XB, Yang YQ, Liu XY. TBX20 loss-of-function mutation contributes to double outlet right ventricle. Int J Mol Med 2015;35:1058–1066. doi: 10.3892/ijmm.2015.2077 [DOI] [PubMed] [Google Scholar]
- 368.Zhou YM, Dai XY, Huang RT, Xue S, Xu YJ, Qiu XB, Yang YQ. A novel TBX20 loss‑of‑function mutation contributes to adult‑onset dilated cardiomyopathy or congenital atrial septal defect. Mol Med Rep 2016;14:3307–3314. doi: 10.3892/mmr.2016.5609 [DOI] [PubMed] [Google Scholar]
- 369.Huang RT, Wang J, Xue S, Qiu XB, Shi HY, Li RG, Qu XK, Yang XX, Liu H, Li N, Li YJ, Xu YJ, Yang YQ. TBX20 loss-of-function mutation responsible for familial tetralogy of Fallot or sporadic persistent truncus arteriosus. Int J Med Sci 2017;14:323–332. doi: 10.7150/ijms.17834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 370.Pizzuti A, Sarkozy A, Newton AL, Conti E, Flex E, Digilio MC, Amati F, Gianni D, Tandoi C, Marino B, Crossley M, Dallapiccola B. Mutations of ZFPM2/FOG2 gene in sporadic cases of tetralogy of Fallot. Hum Mutat 2003;22:372–377. doi: 10.1002/humu.10261 [DOI] [PubMed] [Google Scholar]
- 371.De Luca A, Sarkozy A, Ferese R, Consoli F, Lepri F, Dentici ML, Vergara P, De Zorzi A, Versacci P, Digilio MC, Marino B, Dallapiccola B. New mutations in ZFPM2/FOG2 gene in tetralogy of Fallot and double outlet right ventricle. Clin Genet 2011;80:184–190. doi: 10.1111/j.1399-0004.2010.01523.x [DOI] [PubMed] [Google Scholar]
- 372.Tan ZP, Huang C, Xu ZB, Yang JF, Yang YF. Novel ZFPM2/FOG2 variants in patients with double outlet right ventricle. Clin Genet 2012;82:466–471. doi: 10.1111/j.1399-0004.2011.01787.x [DOI] [PubMed] [Google Scholar]
- 373.Smith KA, Joziasse IC, Chocron S, van Dinther M, Guryev V, Verhoeven MC, Rehmann H, van der Smagt JJ, Doevendans PA, Cuppen E, Mulder BJ, Ten Dijke P, Bakkers J. Dominant-negative ALK2 allele associates with congenital heart defects. Circulation 2009;119:3062–3069. doi: 10.1161/CIRCULATIONAHA.108.843714 [DOI] [PubMed] [Google Scholar]
- 374.Robinson SW, Morris CD, Goldmuntz E, Reller MD, Jones MA, Steiner RD, Maslen CL. Missense mutations in CRELD1 are associated with cardiac atrioventricular septal defects. Am J Hum Genet 2003;72:1047–1052. doi: 10.1086/374319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 375.Zatyka M, Priestley M, Ladusans EJ, Fryer AE, Mason J, Latif F, Maher ER. Analysis of CRELD1 as a candidate 3p25 atrioventicular septal defect locus (AVSD2). Clin Genet 2005;67:526–528. doi: 10.1111/j.1399-0004.2005.00435.x [DOI] [PubMed] [Google Scholar]
- 376.Maslen CL, Babcock D, Robinson SW, Bean LJ, Dooley KJ, Willour VL, Sherman SL. CRELD1 mutations contribute to the occurrence of cardiac atrioventricular septal defects in Down syndrome. Am J Med Genet A 2006;140:2501–2505. doi: 10.1002/ajmg.a.31494 [DOI] [PubMed] [Google Scholar]
- 377.Dasgupta C, Martinez AM, Zuppan CW, Shah MM, Bailey LL, Fletcher WH. Identification of connexin43 (alpha1) gap junction gene mutations in patients with hypoplastic left heart syndrome by denaturing gradient gel electrophoresis (DGGE). Mutat Res 2001;479:173–186. [DOI] [PubMed] [Google Scholar]
- 378.Wang B, Wen Q, Xie X, Liu S, Liu M, Tao Y, Li Z, Suo P, Shen A, Wang J, Ma X. Mutation analysis of Connexon43 gene in Chinese patients with congenital heart defects. Int J Cardiol 2010;145:487–489. doi: 10.1016/j.ijcard.2009.06.026 [DOI] [PubMed] [Google Scholar]
- 379.Izumi K, Lippa AM, Wilkens A, Feret HA, McDonald-McGinn DM, Zackai EH. Congenital heart defects in oculodentodigital dysplasia: report of two cases. Am J Med Genet A 2013;161A:3150–3154. doi: 10.1002/ajmg.a.36159 [DOI] [PubMed] [Google Scholar]
- 380.Li L, Krantz ID, Deng Y, Genin A, Banta AB, Collins CC, Qi M, Trask BJ, Kuo WL, Cochran J, Costa T, Pierpont ME, Rand EB, Piccoli DA, Hood L, Spinner NB. Alagille syndrome is caused by mutations in human Jagged1, which encodes a ligand for Notch1. Nat Genet 1997;16:243–251. doi: 10.1038/ng0797-243 [DOI] [PubMed] [Google Scholar]
- 381.Oda T, Elkahloun AG, Pike BL, Okajima K, Krantz ID, Genin A, Piccoli DA, Meltzer PS, Spinner NB, Collins FS, Chandrasekharappa SC. Mutations in the human Jagged1 gene are responsible for Alagille syndrome. Nat Genet 1997;16:235–242. doi: 10.1038/ng0797-235 [DOI] [PubMed] [Google Scholar]
- 382.Eldadah ZA, Hamosh A, Biery NJ, Montgomery RA, Duke M, Elkins R, Dietz HC. Familial tetralogy of Fallot caused by mutation in the jagged1 gene. Hum Mol Genet 2001;10:163–169. [DOI] [PubMed] [Google Scholar]
- 383.Kerstjens-Frederikse WS, van de Laar IM, Vos YJ, Verhagen JM, Berger RM, Lichtenbelt KD, Klein Wassink-Ruiter JS, van der Zwaag PA, du Marchie Sarvaas GJ, Bergman KA, Bilardo CM, Roos-Hesselink JW, Janssen JH, Frohn-Mulder IM, van Spaendonck-Zwarts KY, van Melle JP, Hofstra RM, Wessels MW. Cardiovascular malformations caused by NOTCH1 mutations do not keep left: data on 428 probands with left-sided CHD and their families. Genet Med 2016;18:914–923. doi: 10.1038/gim.2015.193 [DOI] [PubMed] [Google Scholar]
- 384.Preuss C, Capredon M, Wünnemann F, Chetaille P, Prince A, Godard B, Leclerc S, Sobreira N, Ling H, Awadalla P, Thibeault M, Khairy P, Samuels ME, Andelfinger G; MIBAVA Leducq Consortium. Family based whole exome sequencing reveals the multifaceted role of Notch signaling in congenital heart disease. PLoS Genet 2016;12:e1006335. doi: 10.1371/journal.pgen.1006335 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 385.Zahavich L, Bowdin S, Mital S. Use of clinical exome sequencing in isolated congenital heart disease. Circ Cardiovasc Genet 2017;10. doi: 10.1161/CIRCGENETICS.116.001581 [DOI] [PubMed] [Google Scholar]
- 386.Bleyl SB, Saijoh Y, Bax NA, Gittenberger-de Groot AC, Wisse LJ, Chapman SC, Hunter J, Shiratori H, Hamada H, Yamada S, Shiota K, Klewer SE, Leppert MF, Schoenwolf GC. Dysregulation of the PDGFRA gene causes inflow tract anomalies including TAPVR: integrating evidence from human genetics and model organisms. Hum Mol Genet 2010;19:1286–1301. doi: 10.1093/hmg/ddq005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 387.Tan HL, Glen E, Töpf A, Hall D, O’Sullivan JJ, Sneddon L, Wren C, Avery P, Lewis RJ, ten Dijke P, Arthur HM, Goodship JA, Keavney BD. Nonsynonymous variants in the SMAD6 gene predispose to congenital cardiovascular malformation. Hum Mutat 2012;33:720–727. doi: 10.1002/humu.22030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 388.Thienpont B, Zhang L, Postma AV, Breckpot J, Tranchevent LC, Van Loo P, Møllgård K, Tommerup N, Bache I, Tümer Z, van Engelen K, Menten B, Mortier G, Waggoner D, Gewillig M, Moreau Y, Devriendt K, Larsen LA. Haploinsufficiency of TAB2 causes congenital heart defects in humans. Am J Hum Genet 2010;86:839–849. doi: 10.1016/j.ajhg.2010.04.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 389.Matsson H, Eason J, Bookwalter CS, Klar J, Gustavsson P, Sunnegårdh J, Enell H, Jonzon A, Vikkula M, Gutierrez I, Granados-Riveron J, Pope M, Bu’Lock F, Cox J, Robinson TE, Song F, Brook DJ, Marston S, Trybus KM, Dahl N. Alpha-cardiac actin mutations produce atrial septal defects. Hum Mol Genet 2008;17:256–265. doi: 10.1093/hmg/ddm302 [DOI] [PubMed] [Google Scholar]
- 390.Greenway SC, McLeod R, Hume S, Roslin NM, Alvarez N, Giuffre M, Zhan SH, Shen Y, Preuss C, Andelfinger G, Jones SJ, Gerull B; FORGE Canada Consortium. Exome sequencing identifies a novel variant in ACTC1 associated with familial atrial septal defect. Can J Cardiol 2014;30:181–187. doi: 10.1016/j.cjca.2013.12.003 [DOI] [PubMed] [Google Scholar]
- 391.Li DY, Toland AE, Boak BB, Atkinson DL, Ensing GJ, Morris CA, Keating MT. Elastin point mutations cause an obstructive vascular disease, supravalvular aortic stenosis. Hum Mol Genet 1997;6:1021–1028. [DOI] [PubMed] [Google Scholar]
- 392.Metcalfe K, Rucka AK, Smoot L, Hofstadler G, Tuzler G, McKeown P, Siu V, Rauch A, Dean J, Dennis N, Ellis I, Reardon W, Cytrynbaum C, Osborne L, Yates JR, Read AP, Donnai D, Tassabehji M. Elastin: mutational spectrum in supravalvular aortic stenosis. Eur J Hum Genet 2000;8:955–963. doi: 10.1038/sj.ejhg.5200564 [DOI] [PubMed] [Google Scholar]
- 393.Micale L, Turturo MG, Fusco C, Augello B, Jurado LA, Izzi C, Digilio MC, Milani D, Lapi E, Zelante L, Merla G. Identification and characterization of seven novel mutations of elastin gene in a cohort of patients affected by supravalvular aortic stenosis. Eur J Hum Genet 2010;18:317–323. doi: 10.1038/ejhg.2009.181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 394.Ching YH, Ghosh TK, Cross SJ, Packham EA, Honeyman L, Loughna S, Robinson TE, Dearlove AM, Ribas G, Bonser AJ, Thomas NR, Scotter AJ, Caves LS, Tyrrell GP, Newbury-Ecob RA, Munnich A, Bonnet D, Brook JD. Mutation in myosin heavy chain 6 causes atrial septal defect. Nat Genet 2005;37:423–428. doi: 10.1038/ng1526 [DOI] [PubMed] [Google Scholar]
- 395.Posch MG, Waldmuller S, Müller M, Scheffold T, Fournier D, Andrade-Navarro MA, De Geeter B, Guillaumont S, Dauphin C, Yousseff D, Schmitt KR, Perrot A, Berger F, Hetzer R, Bouvagnet P, Özcelik C. Cardiac alpha-myosin (MYH6) is the predominant sarcomeric disease gene for familial atrial septal defects. PLoS One 2011;6:e28872. doi: 10.1371/journal.pone.0028872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 396.Granados-Riveron JT, Ghosh TK, Pope M, Bu’Lock F, Thornborough C, Eason J, Kirk EP, Fatkin D, Feneley MP, Harvey RP, Armour JA, David Brook J. Alpha-cardiac myosin heavy chain (MYH6) mutations affecting myofibril formation are associated with congenital heart defects. Hum Mol Genet 2010;19:4007–4016. doi: 10.1093/hmg/ddq315 [DOI] [PubMed] [Google Scholar]
- 397.Budde BS, Binner P, Waldmüller S, Höhne W, Blankenfeldt W, Hassfeld S, Brömsen J, Dermintzoglou A, Wieczorek M, May E, Kirst E, Selignow C, Rackebrandt K, Müller M, Goody RS, Vosberg HP, Nürnberg P, Scheffold T. Noncompaction of the ventricular myocardium is associated with a de novo mutation in the beta-myosin heavy chain gene. PLoS One 2007;2:e1362. doi: 10.1371/journal.pone.0001362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 398.Postma AV, van Engelen K, van de Meerakker J, Rahman T, Probst S, Baars MJ, Bauer U, Pickardt T, Sperling SR, Berger F, Moorman AF, Mulder BJ, Thierfelder L, Keavney B, Goodship J, Klaassen S. Mutations in the sarcomere gene MYH7 in Ebstein anomaly. Circ Cardiovasc Genet 2011;4:43–50. doi: 10.1161/CIRCGENETICS.110.957985 [DOI] [PubMed] [Google Scholar]
- 399.Zhu L, Vranckx R, Khau Van Kien P, Lalande A, Boisset N, Mathieu F, Wegman M, Glancy L, Gasc JM, Brunotte F, Bruneval P, Wolf JE, Michel JB, Jeunemaitre X. Mutations in myosin heavy chain 11 cause a syndrome associating thoracic aortic aneurysm/aortic dissection and patent ductus arteriosus. Nat Genet 2006;38:343–349. doi: 10.1038/ng1721 [DOI] [PubMed] [Google Scholar]
- 400.LaHaye S, Corsmeier D, Basu M, Bowman JL, Fitzgerald-Butt S, Zender G, Bosse K, McBride KL, White P, Garg V. Utilization of whole exome sequencing to identify causative mutations in familial congenital heart disease. Circ Cardiovasc Genet 2016;9:320–329. doi: 10.1161/CIRCGENETICS.115.001324 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 401.Olson EN. Gene regulatory networks in the evolution and development of the heart. Science 2006;313:1922–1927. doi: 10.1126/science.1132292 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 402.Ashraf H, Pradhan L, Chang EI, Terada R, Ryan NJ, Briggs LE, Chowdhury R, Zárate MA, Sugi Y, Nam HJ, Benson DW, Anderson RH, Kasahara H. A mouse model of human congenital heart disease: high incidence of diverse cardiac anomalies and ventricular noncompaction produced by heterozygous Nkx2–5 homeodomain missense mutation. Circ Cardiovasc Genet 2014;7:423–433. doi: 10.1161/CIRCGENETICS.113.000281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 403.Biben C, Weber R, Kesteven S, Stanley E, McDonald L, Elliott DA, Barnett L, Köentgen F, Robb L, Feneley M, Harvey RP. Cardiac septal and valvular dysmorphogenesis in mice heterozygous for mutations in the homeobox gene Nkx2–5. Circ Res 2000;87:888–895. [DOI] [PubMed] [Google Scholar]
- 404.Chowdhury R, Ashraf H, Melanson M, Tanada Y, Nguyen M, Silberbach M, Wakimoto H, Benson DW, Anderson RH, Kasahara H. Mouse model of human congenital heart disease: progressive atrioventricular block induced by a heterozygous Nkx2–5 homeodomain missense mutation. Circ Arrhythm Electrophysiol 2015;8:1255–1264. doi: 10.1161/CIRCEP.115.002720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 405.Prendiville T, Jay PY, Pu WT. Insights into the genetic structure of congenital heart disease from human and murine studies on monogenic disorders. Cold Spring Harb Perspect Med 2014;4:a013946. doi: 10.1101/cshperspect.a013946 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 406.Han H, Chen Y, Liu G, Han Z, Zhao Z, Tang Y. GATA4 transgenic mice as an in vivo model of congenital heart disease. Int J Mol Med 2015;35:1545–1553. doi: 10.3892/ijmm.2015.2178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 407.Misra C, Sachan N, McNally CR, Koenig SN, Nichols HA, Guggilam A, Lucchesi PA, Pu WT, Srivastava D, Garg V. Congenital heart diseasecausing Gata4 mutation displays functional deficits in vivo. PLoS Genet 2012;8:e1002690. doi: 10.1371/journal.pgen.1002690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 408.Griffin HR, Töpf A, Glen E, Zweier C, Stuart AG, Parsons J, Peart I, Deanfield J, O’Sullivan J, Rauch A, Scambler P, Burn J, Cordell HJ, Keavney B, Goodship JA. Systematic survey of variants in TBX1 in non-syndromic tetralogy of Fallot identifies a novel 57 base pair deletion that reduces transcriptional activity but finds no evidence for association with common variants. Heart 2010;96:1651–1655. doi: 10.1136/hrt.2010.200121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 409.Smemo S, Campos LC, Moskowitz IP, Krieger JE, Pereira AC, Nobrega MA. Regulatory variation in a TBX5 enhancer leads to isolated congenital heart disease. Hum Mol Genet 2012;21:3255–3263. doi: 10.1093/hmg/dds165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 410.Schulkey CE, Regmi SD, Magnan RA, Danzo MT, Luther H, Hutchinson AK, Panzer AA, Grady MM, Wilson DB, Jay PY. The maternal-age-associated risk of congenital heart disease is modifiable. Nature 2015;520:230–233. doi: 10.1038/nature14361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 411.Sifrim A, Hitz MP, Wilsdon A, Breckpot J, Turki SH, Thienpont B, McRae J, Fitzgerald TW, Singh T, Swaminathan GJ, Prigmore E, Rajan D, Abdul-Khaliq H, Banka S, Bauer UM, Bentham J, Berger F, Bhattacharya S, Bu’Lock F, Canham N, Colgiu IG, Cosgrove C, Cox H, Daehnert I, Daly A, Danesh J, Fryer A, Gewillig M, Hobson E, Hoff K, Homfray T, Kahlert AK, Ketley A, Kramer HH, Lachlan K, Lampe AK, Louw JJ, Manickara AK, Manase D, McCarthy KP, Metcalfe K, Moore C, Newbury-Ecob R, Omer SO, Ouwehand WH, Park SM, Parker MJ, Pickardt T, Pollard MO, Robert L, Roberts DJ, Sambrook J, Setchfield K, Stiller B, Thornborough C, Toka O, Watkins H, Williams D, Wright M, Mital S, Daubeney PE, Keavney B, Goodship J, Abu-Sulaiman RM, Klaassen S, Wright CF, Firth HV, Barrett JC, Devriendt K, FitzPatrick DR, Brook JD, Hurles ME; INTERVAL Study; UK10K Consortium; Deciphering Developmental Disorders Study. Distinct genetic architectures for syndromic and nonsyndromic congenital heart defects identified by exome sequencing. Nat Genet 2016;48:1060–1065. doi: 10.1038/ng.3627 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 412.D’Alessandro LC, Al Turki S, Manickaraj AK, Manase D, Mulder BJ, Bergin L, Rosenberg HC, Mondal T, Gordon E, Lougheed J, Smythe J, Devriendt K, Bhattacharya S, Watkins H, Bentham J, Bowdin S, Hurles ME, Mital S. Exome sequencing identifies rare variants in multiple genes in atrioventricular septal defect. Genet Med 2016;18:189–198. doi: 10.1038/gim.2015.60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 413.Priest JR, Osoegawa K, Mohammed N, Nanda V, Kundu R, Schultz K, Lammer EJ, Girirajan S, Scheetz T, Waggott D, Haddad F, Reddy S, Bernstein D, Burns T, Steimle JD, Yang XH, Moskowitz IP, Hurles M, Lifton RP, Nickerson D, Bamshad M, Eichler EE, Mital S, Sheffield V, Quertermous T, Gelb BD, Portman M, Ashley EA. De novo and rare variants at multiple loci support the oligogenic origins of atrioventricular septal heart defects. PLoS Genet 2016;12:e1005963. doi: 10.1371/journal.pgen.1005963 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 414.Liu X, Yagi H, Saeed S, Bais AS, Gabriel GC, Chen Z, Peterson KA, Li Y, Schwartz MC, Reynolds WT, Saydmohammed M, Gibbs B, Wu Y, Devine W, Chatterjee B, Klena NT, Kostka D, de Mesy Bentley KL, Ganapathiraju MK, Dexheimer P, Leatherbury L, Khalifa O, Bhagat A, Zahid M, Pu W, Watkins S, Grossfeld P, Murray SA, Porter GA Jr, Tsang M, Martin LJ, Benson DW, Aronow BJ, Lo CW. The complex genetics of hypoplastic left heart syndrome. Nat Genet 2017;49:1152–1159. doi: 10.1038/ng.3870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 415.Brodwall K, Greve G, Leirgul E, Tell GS, Vollset SE, Øyen N. Recurrence of congenital heart defects among siblings-a nationwide study. Am J Med Genet A 2017;173:1575–1585. doi: 10.1002/ajmg.a.38237 [DOI] [PubMed] [Google Scholar]
- 416.Mital S, Musunuru K, Garg V, Russell MW, Lanfear DE, Gupta RM, Hickey KT, Ackerman MJ, Perez MV, Roden DM, Woo D, Fox CS, Ware S; on behalf of the American Heart Association Council on Functional Genomics and Translational Biology; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Stroke Council; Council on Lifestyle and Cardiometabolic Health; Council on Quality of Care and Outcomes Research. Enhancing literacy in cardiovascular genetics: a scientific statement from the American Heart Association. Circ Cardiovasc Genet 2016;9:448–467. doi: 10.1161/HCG.0000000000000031 [DOI] [PubMed] [Google Scholar]
- 417.Zaidi S, Brueckner M. Genetics and genomics of congenital heart disease. Circ Res 2017;120:923–940. doi: 10.1161/CIRCRESAHA.116.309140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 418.Karakikes I, Ameen M, Termglinchan V, Wu JC. Human induced pluripotent stem cell-derived cardiomyocytes: insights into molecular, cellular, and functional phenotypes. Circ Res 2015;117:80–88. doi: 10.1161/CIRCRESAHA.117.305365 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 419.Doetschman T, Georgieva T. Gene editing with CRISPR/Cas9 RNA-directed nuclease. Circ Res 2017;120:876–894. doi: 10.1161/CIRCRESAHA.116.309727 [DOI] [PubMed] [Google Scholar]
- 420.Molkentin JD, Robbins J. With great power comes great responsibility: using mouse genetics to study cardiac hypertrophy and failure. J Mol Cell Cardiol 2009;46:130–136. doi: 10.1016/j.yjmcc.2008.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 421.Blow MJ, McCulley DJ, Li Z, Zhang T, Akiyama JA, Holt A, Plajzer-Frick I, Shoukry M, Wright C, Chen F, Afzal V, Bristow J, Ren B, Black BL, Rubin EM, Visel A, Pennacchio LA. ChIP-Seq identification of weakly conserved heart enhancers. Nat Genet 2010;42:806–810. doi: 10.1038/ng.650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 422.May D, Blow MJ, Kaplan T, McCulley DJ, Jensen BC, Akiyama JA, Holt A, Plajzer-Frick I, Shoukry M, Wright C, Afzal V, Simpson PC, Rubin EM, Black BL, Bristow J, Pennacchio LA, Visel A. Large-scale discovery of enhancers from human heart tissue. Nat Genet 2011;44:89–93. doi: 10.1038/ng.1006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 423.Dickel DE, Barozzi I, Zhu Y, Fukuda-Yuzawa Y, Osterwalder M, Mannion BJ, May D, Spurrell CH, Plajzer-Frick I, Pickle CS, Lee E, Garvin TH, Kato M, Akiyama JA, Afzal V, Lee AY, Gorkin DU, Ren B, Rubin EM, Visel A, Pennacchio LA. Genome-wide compendium and functional assessment of in vivo heart enhancers. Nat Commun 2016;7:12923. doi: 10.1038/ncomms12923 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 424.Zhou P, Gu F, Zhang L, Akerberg BN, Ma Q, Li K, He A, Lin Z, Stevens SM, Zhou B, Pu WT. Mapping cell type-specific transcriptional enhancers using high affinity, lineage-specific Ep300 bioChIP-seq. Elife 2017;6:e22039. doi: 10.7554/eLife.22039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 425.Papaioannou VE. Concepts of cell lineage in mammalian embryos. Curr Top Dev Biol 2016;117:185–197. doi: 10.1016/bs.ctdb.2015.10.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 426.Cai CL, Liang X, Shi Y, Chu PH, Pfaff SL, Chen J, Evans S. Isl1 identifies a cardiac progenitor population that proliferates prior to differentiation and contributes a majority of cells to the heart. Dev Cell 2003;5: 877–889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 427.Snarr BS, Wirrig EE, Phelps AL, Trusk TC, Wessels A. A spatiotemporal evaluation of the contribution of the dorsal mesenchymal protrusion to cardiac development. Dev Dyn 2007;236:1287–1294. doi: 10.1002/dvdy.21074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 428.Xie L, Hoffmann AD, Burnicka-Turek O, Friedland-Little JM, Zhang K, Moskowitz IP. Tbx5-hedgehog molecular networks are essential in the second heart field for atrial septation. Dev Cell 2012;23:280–291. doi: 10.1016/j.devcel.2012.06.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 429.Yagi H, Furutani Y, Hamada H, Sasaki T, Asakawa S, Minoshima S, Ichida F, Joo K, Kimura M, Imamura S, Kamatani N, Momma K, Takao A, Nakazawa M, Shimizu N, Matsuoka R. Role of TBX1 in human del22q11.2 syndrome. Lancet 2003;362:1366–1373. [DOI] [PubMed] [Google Scholar]
- 430.Zhang Z, Baldini A. In vivo response to high-resolution variation of Tbx1 mRNA dosage. Hum Mol Genet 2008;17:150–157. doi: 10.1093/hmg/ddm291 [DOI] [PubMed] [Google Scholar]
- 431.Winston JB, Schulkey CE, Chen IB, Regmi SD, Efimova M, Erlich JM, Green CA, Aluko A, Jay PY. Complex trait analysis of ventricular septal defects caused by Nkx2–5 mutation. Circ Cardiovasc Genet 2012;5:293–300. doi: 10.1161/CIRCGENETICS.111.961136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 432.Guo Y, VanDusen NJ, Zhang L, Gu W, Sethi I, Guatimosim S, Ma Q, Jardin BD, Ai Y, Zhang D, Chen B, Guo A, Yuan GC, Song LS, Pu WT. Analysis of cardiac myocyte maturation using CASAAV, a platform for rapid dissection of cardiac myocyte gene function in vivo. Circ Res 2017;120:1874–1888. doi: 10.1161/CIRCRESAHA.116.310283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 433.Stitelman DH, Brazelton T, Bora A, Traas J, Merianos D, Limberis M, Davey M, Flake AW. Developmental stage determines efficiency of gene transfer to muscle satellite cells by in utero delivery of adeno-associated virus vector serotype 2/9. Mol Ther Methods Clin Dev 2014;1:14040. doi: 10.1038/mtm.2014.40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 434.Staudt D, Stainier D. Uncovering the molecular and cellular mechanisms of heart development using the zebrafish. Annu Rev Genet 2012;46:397–418. doi: 10.1146/annurev-genet-110711-155646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 435.Grant MG, Patterson VL, Grimes DT, Burdine RD. Modeling syndromic congenital heart defects in zebrafish. Curr Top Dev Biol 2017;124:1–40. doi: 10.1016/bs.ctdb.2016.11.010 [DOI] [PubMed] [Google Scholar]
- 436.Blum M, De Robertis EM, Wallingford JB, Niehrs C. Morpholinos: antisense and sensibility. Dev Cell 2015;35:145–149. doi: 10.1016/j.devcel.2015.09.017 [DOI] [PubMed] [Google Scholar]
- 437.Hisano Y, Ota S, Kawahara A. Genome editing using artificial site-specific nucleases in zebrafish. Dev Growth Differ 2014;56:26–33. doi: 10.1111/dgd.12094 [DOI] [PubMed] [Google Scholar]
- 438.Amores A, Force A, Yan YL, Joly L, Amemiya C, Fritz A, Ho RK, Langeland J, Prince V, Wang YL, Westerfield M, Ekker M, Postlethwait JH. Zebrafish hox clusters and vertebrate genome evolution. Science 1998;282:1711–1714. [DOI] [PubMed] [Google Scholar]
- 439.Dai YJ, Jia YF, Chen N, Bian WP, Li QK, Ma YB, Chen YL, Pei DS. Zebrafish as a model system to study toxicology. Environ Toxicol Chem 2014;33:11–17. doi: 10.1002/etc.2406 [DOI] [PubMed] [Google Scholar]
- 440.Liu J, Stainier DY. Zebrafish in the study of early cardiac development. Circ Res 2012;110:870–874. doi: 10.1161/CIRCRESAHA.111.246504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 441.Halloran MC, Sato-Maeda M, Warren JT, Su F, Lele Z, Krone PH, Kuwada JY, Shoji W. Laser-induced gene expression in specific cells of transgenic zebrafish. Development 2000;127:1953–1960. [DOI] [PubMed] [Google Scholar]
- 442.Hatta K, Tsujii H, Omura T. Cell tracking using a photoconvertible fluorescent protein. Nat Protoc 2006;1:960–967. doi: 10.1038/nprot.2006.96 [DOI] [PubMed] [Google Scholar]
- 443.Serbedzija GN, Chen JN, Fishman MC. Regulation in the heart field of zebrafish. Development 1998;125:1095–1101. [DOI] [PubMed] [Google Scholar]
- 444.Midgett M, Thornburg K, Rugonyi S. Blood flow patterns underlie developmental heart defects. Am J Physiol Heart Circ Physiol 2017;312:H632–H642. doi: 10.1152/ajpheart.00641.2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 445.Sedmera D, Hu N, Weiss KM, Keller BB, Denslow S, Thompson RP. Cellular changes in experimental left heart hypoplasia. Anat Rec 2002;267:137–145. doi: 10.1002/ar.10098 [DOI] [PubMed] [Google Scholar]
- 446.Vogler G, Bodmer R. Cellular mechanisms of Drosophila heart morphogenesis. J Cardiovasc Dev Dis 2015;2:2–16. doi: 10.3390/jcdd2010002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 447.Zhu JY, Fu Y, Nettleton M, Richman A, Han Z. High throughput in vivo functional validation of candidate congenital heart disease genes in Drosophila. Elife 2017;6:e22617. doi: 10.7554/eLife.22617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 448.Chang CP, Neilson JR, Bayle JH, Gestwicki JE, Kuo A, Stankunas K, Graef IA, Crabtree GR. A field of myocardial-endocardial NFAT signaling underlies heart valve morphogenesis. Cell 2004;118:649–663. doi: 10.1016/j.cell.2004.08.010 [DOI] [PubMed] [Google Scholar]
- 449.Shenje LT, Andersen P, Uosaki H, Fernandez L, Rainer PP, Cho GS, Lee DI, Zhong W, Harvey RP, Kass DA, Kwon C. Precardiac deletion of Numb and Numblike reveals renewal of cardiac progenitors. Elife 2014;3:e02164. doi: 10.7554/eLife.02164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 450.Red-Horse K, Ueno H, Weissman IL, Krasnow MA. Coronary arteries form by developmental reprogramming of venous cells. Nature 2010;464:549–553. doi: 10.1038/nature08873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 451.von Gise A, Pu WT. Endocardial and epicardial epithelial to mesenchymal transitions in heart development and disease. Circ Res 2012;110:1628–1645. doi: 10.1161/CIRCRESAHA.111.259960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 452.Molkentin JD, Lu JR, Antos CL, Markham B, Richardson J, Robbins J, Grant SR, Olson EN. A calcineurin-dependent transcriptional pathway for cardiac hypertrophy. Cell 1998;93:215–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 453.Li P, Cavallero S, Gu Y, Chen TH, Hughes J, Hassan AB, Brüning JC, Pashmforoush M, Sucov HM. IGF signaling directs ventricular cardiomyocyte proliferation during embryonic heart development. Development 2011;138:1795–1805. doi: 10.1242/dev.054338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 454.Zhou B, Honor LB, He H, Ma Q, Oh JH, Butterfield C, Lin RZ, Melero-Martin JM, Dolmatova E, Duffy HS, Gise Av, Zhou P, Hu YW, Wang G, Zhang B, Wang L, Hall JL, Moses MA, McGowan FX, Pu WT. Adult mouse epicardium modulates myocardial injury by secreting paracrine factors. J Clin Invest 2011;121:1894–1904. doi: 10.1172/JCI45529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 455.Wamstad JA, Alexander JM, Truty RM, Shrikumar A, Li F, Eilertson KE, Ding H, Wylie JN, Pico AR, Capra JA, Erwin G, Kattman SJ, Keller GM, Srivastava D, Levine SS, Pollard KS, Holloway AK, Boyer LA, Bruneau BG. Dynamic and coordinated epigenetic regulation of developmental transitions in the cardiac lineage. Cell 2012;151:206–220. doi: 10.1016/j.cell.2012.07.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 456.Paige SL, Thomas S, Stoick-Cooper CL, Wang H, Maves L, Sandstrom R, Pabon L, Reinecke H, Pratt G, Keller G, Moon RT, Stamatoyannopoulos J, Murry CE. A temporal chromatin signature in human embryonic stem cells identifies regulators of cardiac development. Cell 2012;151:221–232. doi: 10.1016/j.cell.2012.08.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 457.Ang YS, Rivas RN, Ribeiro AJS, Srivas R, Rivera J, Stone NR, Pratt K, Mohamed TMA, Fu JD, Spencer CI, Tippens ND, Li M, Narasimha A, Radzinsky E, Moon-Grady AJ, Yu H, Pruitt BL, Snyder MP, Srivastava D. Disease model of GATA4 mutation reveals transcription factor cooperativity in human cardiogenesis. Cell 2016;167:1734–1749.e22. doi: 10.1016/j.cell.2016.11.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 458.Hinson JT, Chopra A, Nafissi N, Polacheck WJ, Benson CC, Swist S, Gorham J, Yang L, Schafer S, Sheng CC, Haghighi A, Homsy J, Hubner N, Church G, Cook SA, Linke WA, Chen CS, Seidman JG, Seidman CE. Heart disease: titin mutations in iPS cells define sarcomere insufficiency as a cause of dilated cardiomyopathy. Science 2015;349:982–986. doi: 10.1126/science.aaa5458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 459.Lan F, Lee AS, Liang P, Sanchez-Freire V, Nguyen PK, Wang L, Han L, Yen M, Wang Y, Sun N, Abilez OJ, Hu S, Ebert AD, Navarrete EG, Simmons CS, Wheeler M, Pruitt B, Lewis R, Yamaguchi Y, Ashley EA, Bers DM, Robbins RC, Longaker MT, Wu JC. Abnormal calcium handling properties underlie familial hypertrophic cardiomyopathy pathology in patient-specific induced pluripotent stem cells. Cell Stem Cell 2013;12:101–113. doi: 10.1016/j.stem.2012.10.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 460.Wang G, McCain ML, Yang L, He A, Pasqualini FS, Agarwal A, Yuan H, Jiang D, Zhang D, Zangi L, Geva J, Roberts AE, Ma Q, Ding J, Chen J, Wang DZ, Li K, Wang J, Wanders RJ, Kulik W, Vaz FM, Laflamme MA, Murry CE, Chien KR, Kelley RI, Church GM, Parker KK, Pu WT. Modeling the mitochondrial cardiomyopathy of Barth syndrome with induced pluripotent stem cell and heart-on-chip technologies. Nat Med 2014;20:616–623. doi: 10.1038/nm.3545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 461.Richards AA, Garg V. Genetics of congenital heart disease. Curr Cardiol Rev 2010;6:91–97. doi: 10.2174/157340310791162703 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 462.Landis BJ, Ware SM. The current landscape of genetic testing in cardiovascular malformations: opportunities and challenges. Front Cardiovasc Med 2016;3:22. doi: 10.3389/fcvm.2016.00022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 463.Fung A, Manlhiot C, Naik S, Rosenberg H, Smythe J, Lougheed J, Mondal T, Chitayat D, McCrindle BW, Mital S. Impact of prenatal risk factors on congenital heart disease in the current era. J Am Heart Assoc 2013;2:e000064. doi: 10.1161/JAHA.113.000064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 464.Blue GM, Kirk EP, Giannoulatou E, Sholler GF, Dunwoodie SL, Harvey RP, Winlaw DS. Advances in the genetics of congenital heart disease: a clinician’s guide. J Am Coll Cardiol 2017;69:859–870. doi: 10.1016/j.jacc.2016.11.060 [DOI] [PubMed] [Google Scholar]
- 465.Green RC, Berg JS, Grody WW, Kalia SS, Korf BR, Martin CL, McGuire AL, Nussbaum RL, O’Daniel JM, Ormond KE, Rehm HL, Watson MS, Williams MS, Biesecker LG; American College of Medical Genetics and Genomics. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing [published correction appears in Genet Med. 2017;19:606]. Genet Med 2013;15:565–574. doi: 10.1038/gim.2013.73 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 466.Kalia SS, Adelman K, Bale SJ, Chung WK, Eng C, Evans JP, Herman GE, Hufnagel SB, Klein TE, Korf BR, McKelvey KD, Ormond KE, Richards CS, Vlangos CN, Watson M, Martin CL, Miller DT. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics [published correction appears in Genet Med. 2017;19:484]. Genet Med 2017;19:249–255. doi: 10.1038/gim.2016.190 [DOI] [PubMed] [Google Scholar]
- 467.Andorno R The right not to know: an autonomy based approach [published correction appears in J Med Ethics. 2004;30:612]. J Med Ethics 2004;30:435–439. doi: 10.1136/jme.2002.001578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 468.American Society of Human Genetics Board of Directors; American College of Medical Genetics Board of Directors. Points to consider: ethical, legal, and psychosocial implications of genetic testing in children and adolescents. Am J Hum Genet 1995;57:1233–1241. [PMC free article] [PubMed] [Google Scholar]
- 469.Ross LF, Saal HM, David KL, Anderson RR; American Academy of Pediatrics; American College of Medical Genetics and Genomics. Technical report: ethical and policy issues in genetic testing and screening of children. Genet Med 2013;15:234–245. doi: 10.1038/gim.2012.176 [DOI] [PubMed] [Google Scholar]
- 470.Davis DS. Genetic dilemmas and the child’s right to an open future. Hastings Cent Rep 1997;27:7–15. [PubMed] [Google Scholar]
- 471.Wilfond BS, Fernandez CV, Green RC. Disclosing secondary findings from pediatric sequencing to families: considering the “benefit to families.” J Law Med Ethics 2015;43:552–558. doi: 10.1111/jlme.12298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 472.Berkman BE, Hull SC. The “right not to know” in the genomic era: time to break from tradition? Am J Bioeth 2014;14:28–31. doi: 10.1080/15265161.2014.880313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 473.American Academy of Pediatrics Committee on Bioethics. Informed consent, parental permission, and assent in pediatric practice. Pediatrics 1995;95:314–317. [PubMed] [Google Scholar]
- 474.Heshka JT, Palleschi C, Howley H, Wilson B, Wells PS. A systematic review of perceived risks, psychological and behavioral impacts of genetic testing. Genet Med 2008;10:19–32. doi: 10.1097/GIM.0b013e31815f524f [DOI] [PubMed] [Google Scholar]
- 475.Biesecker BB. Predictive genetic testing of minors: evidence and experience with families. Genet Med 2016;18:763–764. doi: 10.1038/gim.2015.191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 476.Wakefield CE, Hanlon LV, Tucker KM, Patenaude AF, Signorelli C, McLoone JK, Cohn RJ. The psychological impact of genetic information on children: a systematic review. Genet Med 2016;18:755–762. doi: 10.1038/gim.2015.181 [DOI] [PubMed] [Google Scholar]
- 477.Green RC, Lautenbach D, McGuire AL. GINA, genetic discrimination, and genomic medicine. N Engl J Med 2015;372:397–399. doi: 10.1056/NEJMp1404776 [DOI] [PubMed] [Google Scholar]
- 478.Resta R, Biesecker BB, Bennett RL, Blum S, Hahn SE, Strecker MN, Williams JL; National Society of Genetic Counselors’ Definition Task Force. A new definition of genetic counseling: National Society of Genetic Counselors’ Task Force report. J Genet Couns 2006;15:77–83. doi: 10.1007/s10897-005-9014-3 [DOI] [PubMed] [Google Scholar]
- 479.Somers AE, Ware SM, Collins K, Jefferies JL, He H, Miller EM. Provision of cardiovascular genetic counseling services: current practice and future directions. J Genet Couns 2014;23:976–983. doi: 10.1007/s10897-014-9719-2 [DOI] [PubMed] [Google Scholar]
- 480.Ahrens-Nicklas RC, Khan S, Garbarini J, Woyciechowski S, D’Alessandro L, Zackai EH, Deardorff MA, Goldmuntz E. Utility of genetic evaluation in infants with congenital heart defects admitted to the cardiac intensive care unit. Am J Med Genet A 2016;170:3090–3097. doi: 10.1002/ajmg.a.37891 [DOI] [PubMed] [Google Scholar]
- 481.Goldenberg PC, Adler BJ, Parrott A, Anixt J, Mason K, Phillips J, Cooper DS, Ware SM, Marino BS. High burden of genetic conditions diagnosed in a cardiac neurodevelopmental clinic. Cardiol Young 2017;27:459–466. doi: 10.1017/S104795111600072X [DOI] [PubMed] [Google Scholar]
- 482.Connor JA, Hinton RB, Miller EM, Sund KL, Ruschman JG, Ware SM. Genetic testing practices in infants with congenital heart disease. Congenit Heart Dis 2014;9:158–167. doi: 10.1111/chd.12112 [DOI] [PubMed] [Google Scholar]
- 483.Geddes GC, Basel D, Frommelt P, Kinney A, Earing M. Genetic testing protocol reduces costs and increases rate of genetic diagnosis in infants with congenital heart disease. Pediatr Cardiol 2017;38:1465–1470. doi: 10.1007/s00246-017-1685-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 484.van Engelen K, Baars MJ, van Rongen LT, van der Velde ET, Mulder BJ, Smets EM. Adults with congenital heart disease: patients’ knowledge and concerns about inheritance. Am J Med Genet A 2011;155A:1661–1667. doi: 10.1002/ajmg.a.34068 [DOI] [PubMed] [Google Scholar]
- 485.Jansen FA, Blumenfeld YJ, Fisher A, Cobben JM, Odibo AO, Borrell A, Haak MC. Array comparative genomic hybridization and fetal congenital heart defects: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2015;45:27–35. doi: 10.1002/uog.14695 [DOI] [PubMed] [Google Scholar]
- 486.Morales A, Allain DC, Arscott P, James E, MacCarrick G, Murray B, Tichnell C, Shikany AR, Spencer S, Fitzgerald-Butt SM, Kushner JD, Munn C, Smith E, Spoonamore KG, Tandri HS, Kay WA. At the heart of the pregnancy: what prenatal and cardiovascular genetic counselors need to know about maternal heart disease [published correction appears in J Genet Couns. 2017;26:689]. J Genet Couns 2017;26:669–688. doi: 10.1007/s10897-017-0081-z [DOI] [PubMed] [Google Scholar]
- 487.van Engelen K, Baars MJ, Felix JP, Postma AV, Mulder BJ, Smets EM. The value of the clinical geneticist caring for adults with congenital heart disease: diagnostic yield and patients’ perspective. Am J Med Genet A 2013;161A:1628–1637. doi: 10.1002/ajmg.a.35973 [DOI] [PubMed] [Google Scholar]
- 488.Ferencz C, Boughman JA, Neill CA, Brenner JI, Perry LW; Baltimore-Washington Infant Study Group. Congenital cardiovascular malformations: questions on inheritance. J Am Coll Cardiol 1989;14:756–763. [DOI] [PubMed] [Google Scholar]
- 489.Ferencz C, Neill CA, Boughman JA, Rubin JD, Brenner JI, Perry LW. Congenital cardiovascular malformations associated with chromosome abnormalities: an epidemiologic study. J Pediatr 1989;114:79–86. [DOI] [PubMed] [Google Scholar]
- 490.Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR, Elixson M, Warnes CA, Webb CL. Noninherited risk factors and congenital cardiovascular defects: current knowledge: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young. Circulation 2007;115:2995–3014. doi: 10.1161/CIRCULATIONAHA.106.183216 [DOI] [PubMed] [Google Scholar]
- 491.Burn J, Brennan P, Little J, Holloway S, Coffey R, Somerville J, Dennis NR, Allan L, Arnold R, Deanfield JE, Godman M, Houston A, Keeton B, Oakley C, Scott O, Silove E, Wilkinson J, Pembrey M, Hunter AS. Recurrence risks in offspring of adults with major heart defects: results from first cohort of British collaborative study. Lancet 1998;351:311–316. [DOI] [PubMed] [Google Scholar]
- 492.Gill HK, Splitt M, Sharland GK, Simpson JM. Patterns of recurrence of congenital heart disease: an analysis of 6,640 consecutive pregnancies evaluated by detailed fetal echocardiography. J Am Coll Cardiol 2003;42:923–929. [DOI] [PubMed] [Google Scholar]
- 493.Cripe L, Andelfinger G, Martin LJ, Shooner K, Benson DW. Bicuspid aortic valve is heritable. J Am Coll Cardiol 2004;44:138–143. doi: 10.1016/j.jacc.2004.03.050 [DOI] [PubMed] [Google Scholar]
- 494.McBride KL, Pignatelli R, Lewin M, Ho T, Fernbach S, Menesses A, Lam W, Leal SM, Kaplan N, Schliekelman P, Towbin JA, Belmont JW. Inheritance analysis of congenital left ventricular outflow tract obstruction malformations: Segregation, multiplex relative risk, and heritability. Am J Med Genet A 2005;134A:180–186. doi: 10.1002/ajmg.a.30602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 495.Hinton RB Jr, Martin LJ, Tabangin ME, Mazwi ML, Cripe LH, Benson DW. Hypoplastic left heart syndrome is heritable. J Am Coll Cardiol 2007;50:1590–1595. doi: 10.1016/j.jacc.2007.07.021 [DOI] [PubMed] [Google Scholar]
- 496.Oyen N, Poulsen G, Wohlfahrt J, Boyd HA, Jensen PK, Melbye M. Recurrence of discordant congenital heart defects in families. Circ Cardiovasc Genet 2010;3:122–128. doi: 10.1161/CIRCGENETICS.109.890103 [DOI] [PubMed] [Google Scholar]
- 497.Canfield MA, Honein MA, Yuskiv N, Xing J, Mai CT, Collins JS, Devine O, Petrini J, Ramadhani TA, Hobbs CA, Kirby RS. National estimates and race/ethnic-specific variation of selected birth defects in the United States, 1999–2001. Birth Defects Res A Clin Mol Teratol 2006;76:747–756. doi: 10.1002/bdra.20294 [DOI] [PubMed] [Google Scholar]
- 498.Pradat P, Francannet C, Harris JA, Robert E. The epidemiology of cardiovascular defects, part I: a study based on data from three large registries of congenital malformations. Pediatr Cardiol 2003;24:195–221. doi: 10.1007/s00246-002-9401-6 [DOI] [PubMed] [Google Scholar]
- 499.Calcagni G, Digilio MC, Sarkozy A, Dallapiccola B, Marino B. Familial recurrence of congenital heart disease: an overview and review of the literature. Eur J Pediatr 2007;166:111–116. doi: 10.1007/s00431-006-0295-9 [DOI] [PubMed] [Google Scholar]
- 500.Nora JJ. From generational studies to a multilevel genetic-environmental interaction. J Am Coll Cardiol 1994;23:1468–1471. [DOI] [PubMed] [Google Scholar]
- 501.Nora JJ, Nora AH. Update on counseling the family with a first-degree relative with a congenital heart defect. Am J Med Genet 1988;29:137–142. doi: 10.1002/ajmg.1320290117 [DOI] [PubMed] [Google Scholar]
- 502.Roos-Hesselink JW, Kerstjens-Frederikse WS, Meijboom FJ, Pieper PG. Inheritance of congenital heart disease. Neth Heart J 2005;13:88–91. [PMC free article] [PubMed] [Google Scholar]
- 503.Traeger-Synodinos J Pre-implantation genetic diagnosis. Best Pract Res Clin Obstet Gynaecol 2017;39:74–88. doi: 10.1016/j.bpobgyn.2016.10.010 [DOI] [PubMed] [Google Scholar]
- 504.Vermeesch JR, Voet T, Devriendt K. Prenatal and pre-implantation genetic diagnosis. Nat Rev Genet 2016;17:643–656. doi: 10.1038/nrg.2016.97 [DOI] [PubMed] [Google Scholar]
- 505.Kuliev A, Pomerantseva E, Polling D, Verlinsky O, Rechitsky S. PGD for inherited cardiac diseases. Reprod Biomed Online 2012;24:443–453. doi: 10.1016/j.rbmo.2011.12.009 [DOI] [PubMed] [Google Scholar]
- 506.Gregg AR, Skotko BG, Benkendorf JL, Monaghan KG, Bajaj K, Best RG, Klugman S, Watson MS. Noninvasive prenatal screening for fetal aneuploidy, 2016 update: a position statement of the American College of Medical Genetics and Genomics. Genet Med 2016;18:1056–1065. doi: 10.1038/gim.2016.97 [DOI] [PubMed] [Google Scholar]
- 507.Skrzypek H, Hui L. Noninvasive prenatal testing for fetal aneuploidy and single gene disorders. Best Pract Res Clin Obstet Gynaecol 2017;42:26–38. doi: 10.1016/j.bpobgyn.2017.02.007 [DOI] [PubMed] [Google Scholar]
- 508.Taylor-Phillips S, Freeman K, Geppert J, Agbebiyi A, Uthman OA, Madan J, Clarke A, Quenby S, Clarke A. Accuracy of non-invasive prenatal testing using cell-free DNA for detection of Down, Edwards and Patau syndromes: a systematic review and meta-analysis. BMJ Open 2016;6:e010002. doi: 10.1136/bmjopen-2015-010002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 509.Committee on Genetics and the Society for Maternal-Fetal Medicine. Committee Opinion No. 682: microarrays and next-generation sequencing technology: the use of advanced genetic diagnostic tools in obstetrics and gynecology. Obstet Gynecol 2016;128:e262–e268. doi: 10.1097/AOG.0000000000001817 [DOI] [PubMed] [Google Scholar]
- 510.Donofrio MT, Moon-Grady AJ, Hornberger LK, Copel JA, Sklansky MS, Abuhamad A, Cuneo BF, Huhta JC, Jonas RA, Krishnan A, Lacey S, Lee W, Michelfelder EC Sr, Rempel GR, Silverman NH, Spray TL, Strasburger JF, Tworetzky W, Rychik J; on behalf of the American Heart Association Adults With Congenital Heart Disease Joint Committee of the Council on Cardiovascular Disease in the Young and Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovascular and Stroke Nursing. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association [published correction appears in Circulation. 2014;129:e512]. Circulation 2014;129:2183–2242. doi: 10.1161/01.cir.0000437597.44550.5d [DOI] [PubMed] [Google Scholar]
- 511.Copel JA, Pilu G, Kleinman CS. Congenital heart disease and extracardiac anomalies: associations and indications for fetal echocardiography. Am J Obstet Gynecol 1986;154:1121–1132. [DOI] [PubMed] [Google Scholar]
- 512.Malik S, Cleves MA, Zhao W, Correa A, Hobbs CA; National Birth Defects Prevention Study. Association between congenital heart defects and small for gestational age. Pediatrics 2007;119:e976–e982. doi: 10.1542/peds.2006-2742 [DOI] [PubMed] [Google Scholar]
- 513.Bilardo CM, Müller MA, Pajkrt E. Outcome of fetuses with increased nuchal translucency. Curr Opin Obstet Gynecol 2001;13:169–174. [DOI] [PubMed] [Google Scholar]
- 514.Ali MM, Chasen ST, Norton ME. Testing for Noonan syndrome after increased nuchal translucency. Prenat Diagn 2017;37:750–753. doi: 10.1002/pd.5076 [DOI] [PubMed] [Google Scholar]
- 515.Vigneswaran TV, Homfray T, Allan LD, Simpson JM, Zidere V. Persistently elevated nuchal translucency and the fetal heart. J Matern Fetal Neonatal Med 2018;31:2376–2380. doi: 10.1080/14767058.2017.1342804 [DOI] [PubMed] [Google Scholar]
- 516.Schinzel A Catalogue of Unbalanced Chromosome Aberrations in Man, 2nd Edition. Chromosome Res 2002;10:1–4. doi: 10.1023/A:101427460597912375560 [DOI] [Google Scholar]
- 517.Bruns D Presenting physical characteristics, medical conditions, and developmental status of long-term survivors with trisomy 9 mosaicism. Am J Med Genet A 2011;155A:1033–1039. doi: 10.1002/ajmg.a.33928 [DOI] [PubMed] [Google Scholar]
- 518.Springett A, Wellesley D, Greenlees R, Loane M, Addor MC, Arriola L, Bergman J, Cavero-Carbonell C, Csaky-Szunyogh M, Draper ES, Garne E, Gatt M, Haeusler M, Khoshnood B, Klungsoyr K, Lynch C, Dias CM, McDonnell R, Nelen V, O’Mahony M, Pierini A, Queisser-Luft A, Rankin J, Rissmann A, Rounding C, Stoianova S, Tuckerz D, Zymak-Zakutnia N, Morris JK. Congenital anomalies associated with trisomy 18 or trisomy 13: a registry-based study in 16 European countries, 2000–2011. Am J Med Genet A 2015;167A:3062–3069. doi: 10.1002/ajmg.a.37355 [DOI] [PubMed] [Google Scholar]
- 519.Bruns D Birth history, physical characteristics, and medical conditions in long-term survivors with full trisomy 13. Am J Med Genet A 2011;155A:2634–2640. doi: 10.1002/ajmg.a.34283 [DOI] [PubMed] [Google Scholar]
- 520.Levitsky LL, Luria AH, Hayes FJ, Lin AE. Turner syndrome: update on biology and management across the life span. Curr Opin Endocrinol Diabetes Obes 2015;22:65–72. doi: 10.1097/MED.0000000000000128 [DOI] [PubMed] [Google Scholar]
- 521.Nienhaus H, Mau U, Zang KD, Henn W. Pericentric inversion of chromosome 6 in a patient with cleidocranial dysplasia. Am J Med Genet 1993;46:630–631. doi: 10.1002/ajmg.1320460605 [DOI] [PubMed] [Google Scholar]
- 522.Battaglia A, Filippi T, Carey JC. Update on the clinical features and natural history of Wolf-Hirschhorn (4p-) syndrome: experience with 87 patients and recommendations for routine health supervision. Am J Med Genet C Semin Med Genet 2008;148C:246–251. doi: 10.1002/ajmg.c.30187 [DOI] [PubMed] [Google Scholar]
- 523.Xu W, Ahmad A, Dagenais S, Iyer RK, Innis JW. Chromosome 4q deletion syndrome: narrowing the cardiovascular critical region to 4q32.2-q34.3. Am J Med Genet A 2012;158A:635–640. doi: 10.1002/ajmg.a.34425 [DOI] [PubMed] [Google Scholar]
- 524.Nguyen JM, Qualmann KJ, Okashah R, Reilly A, Alexeyev MF, Campbell DJ. 5p deletions: current knowledge and future directions. Am J Med Genet C Semin Med Genet 2015;169:224–238. doi: 10.1002/ajmg.c.31444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 525.Kondoh T, Shimokawa O, Harada N, Doi T, Yun C, Gohda Y, Kinoshita F, Matsumoto T, Moriuchi H. Genotype-phenotype correlation of 5p-syndrome: pitfall of diagnosis. J Hum Genet 2005;50:26–29. doi: 10.1007/s10038-004-0213-9 [DOI] [PubMed] [Google Scholar]
- 526.Swinkels ME, Simons A, Smeets DF, Vissers LE, Veltman JA, Pfundt R, de Vries BB, Faas BH, Schrander-Stumpel CT, McCann E, Sweeney E, May P, Draaisma JM, Knoers NV, van Kessel AG, van Ravenswaaij-Arts CM. Clinical and cytogenetic characterization of 13 Dutch patients with deletion 9p syndrome: delineation of the critical region for a consensus phenotype. Am J Med Genet A 2008;146A:1430–1438. doi: 10.1002/ajmg.a.32310 [DOI] [PubMed] [Google Scholar]
- 527.Lindstrand A, Malmgren H, Verri A, Benetti E, Eriksson M, Nordgren A, Anderlid BM, Golovleva I, Schoumans J, Blennow E. Molecular and clinical characterization of patients with overlapping 10p deletions. Am J Med Genet A 2010;152A:1233–1243. doi: 10.1002/ajmg.a.33366 [DOI] [PubMed] [Google Scholar]
- 528.Aglan MS, Kamel AK, Helmy NA. Partial trisomy of the distal part of 10q: a report of two Egyptian cases. Genet Couns 2008;19:199–209. [PubMed] [Google Scholar]
- 529.Rosenfeld JA, Lacassie Y, El-Khechen D, Escobar LF, Reggin J, Heuer C, Chen E, Jenkins LS, Collins AT, Zinner S, Babcock M, Morrow B, Schultz RA, Torchia BS, Ballif BC, Tsuchiya KD, Shaffer LG. New cases and refinement of the critical region in the 1q41q42 microdeletion syndrome. Eur J Med Genet 2011;54:42–49. doi: 10.1016/j.ejmg.2010.10.002 [DOI] [PubMed] [Google Scholar]
- 530.van Bon BW, Koolen DA, Borgatti R, Magee A, Garcia-Minaur S, Rooms L, Reardon W, Zollino M, Bonaglia MC, De Gregori M, Novara F, Grasso R, Ciccone R, van Duyvenvoorde HA, Aalbers AM, Guerrini R, Fazzi E, Nillesen WM, McCullough S, Kant SG, Marcelis CL, Pfundt R, de Leeuw N, Smeets D, Sistermans EA, Wit JM, Hamel BC, Brunner HG, Kooy F, Zuffardi O, de Vries BB. Clinical and molecular characteristics of 1qter microdeletion syndrome: delineating a critical region for corpus callosum agenesis/hypogenesis. J Med Genet 2008;45:346–354. doi: 10.1136/jmg.2007.055830 [DOI] [PubMed] [Google Scholar]
- 531.Mitter D, Chiaie BD, Lüdecke HJ, Gillessen-Kaesbach G, Bohring A, Kohlhase J, Caliebe A, Siebert R, Roepke A, Ramos-Arroyo MA, Nieva B, Menten B, Loeys B, Mortier G, Wieczorek D. Genotype-phenotype correlation in eight new patients with a deletion encompassing 2q31.1. Am J Med Genet A 2010;152A:1213–1224. doi: 10.1002/ajmg.a.33344 [DOI] [PubMed] [Google Scholar]
- 532.Casas KA, Mononen TK, Mikail CN, Hassed SJ, Li S, Mulvihill JJ, Lin HJ, Falk RE. Chromosome 2q terminal deletion: report of 6 new patients and review of phenotype-breakpoint correlations in 66 individuals. Am J Med Genet A 2004;130A:331–339. doi: 10.1002/ajmg.a.30156 [DOI] [PubMed] [Google Scholar]
- 533.Falk RE, Casas KA. Chromosome 2q37 deletion: clinical and molecular aspects. Am J Med Genet C Semin Med Genet 2007;145C:357–371. doi: 10.1002/ajmg.c.30153 [DOI] [PubMed] [Google Scholar]
- 534.Kleefstra T, Brunner HG, Amiel J, Oudakker AR, Nillesen WM, Magee A, Geneviève D, Cormier-Daire V, van Esch H, Fryns JP, Hamel BC, Sistermans EA, de Vries BB, van Bokhoven H. Loss-of-function mutations in euchromatin histone methyl transferase 1 (EHMT1) cause the 9q34 subtelomeric deletion syndrome. Am J Hum Genet 2006;79:370–377. doi: 10.1086/505693 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 535.Mefford HC, Rosenfeld JA, Shur N, Slavotinek AM, Cox VA, Hennekam RC, Firth HV, Willatt L, Wheeler P, Morrow EM, Cook J, Sullivan R, Oh A, McDonald MT, Zonana J, Keller K, Hannibal MC, Ball S, Kussmann J, Gorski J, Zelewski S, Banks V, Smith W, Smith R, Paull L, Rosenbaum KN, Amor DJ, Silva J, Lamb A, Eichler EE. Further clinical and molecular delineation of the 15q24 microdeletion syndrome. J Med Genet 2012;49:110–118. doi: 10.1136/jmedgenet-2011-100499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 536.Hempel M, Rivera Brugués N, Wagenstaller J, Lederer G, Weitensteiner A, Seidel H, Meitinger T, Strom TM. Microdeletion syndrome 16p11.2-p12.2: clinical and molecular characterization. Am J Med Genet A 2009;149A:2106–2112. doi: 10.1002/ajmg.a.33042 [DOI] [PubMed] [Google Scholar]
- 537.Koolen DA, Sharp AJ, Hurst JA, Firth HV, Knight SJ, Goldenberg A, Saugier-Veber P, Pfundt R, Vissers LE, Destrée A, Grisart B, Rooms L, Van der Aa N, Field M, Hackett A, Bell K, Nowaczyk MJ, Mancini GM, Poddighe PJ, Schwartz CE, Rossi E, De Gregori M, Antonacci-Fulton LL, McLellan MD 2nd, Garrett JM, Wiechert MA, Miner TL, Crosby S, Ciccone R, Willatt L, Rauch A, Zenker M, Aradhya S, Manning MA, Strom TM, Wagenstaller J, Krepischi-Santos AC, Vianna-Morgante AM, Rosenberg C, Price SM, Stewart H, Shaw-Smith C, Brunner HG, Wilkie AO, Veltman JA, Zuffardi O, Eichler EE, de Vries BB. Clinical and molecular delineation of the 17q21.31 microdeletion syndrome [published correction appears in J Med Genet. 2009;46:576]. J Med Genet 2008;45:710–720. doi: 10.1136/jmg.2008.058701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 538.McElhinney DB, Krantz ID, Bason L, Piccoli DA, Emerick KM, Spinner NB, Goldmuntz E. Analysis of cardiovascular phenotype and genotype-phenotype correlation in individuals with a JAG1 mutation and/or Alagille syndrome. Circulation 2002;106:2567–2574. [DOI] [PubMed] [Google Scholar]
- 539.Phelan K, McDermid HE. The 22q13.3 deletion syndrome (Phelan-McDermid syndrome). Mol Syndromol 2012;2:186–201. doi: 10.1159/000334260 [DOI] [PMC free article] [PubMed] [Google Scholar]