

Synopsis/abstract:
While many aspects of infection prevention and control (IPC) mirror institutional efforts, optimization of IPC practices in the neonatal intensive care unit (NICU) requires careful consideration of its unique population and environment, addressed here for key IPC domains. Additionally, innovative mitigation efforts to address challenges specific to limited resource settings are discussed.
Keywords: healthcare-associated infections, central line-associated bloodstream infections, low-and middle-income countries, environmental cleaning, disinfection
Introduction
Hospitalized neonates are uniquely vulnerable to healthcare-associated infections (HAIs), which are associated with increased mortality, increased length of stay and healthcare costs, and risk of neurodevelopmental disability among survivors.1-3 In the United States (US), incidence of neonatal central line-associated bloodstream infections (CLABSIs) declined significantly from 2007 to 2012, though rates have plateaued recently.4,5 Global estimates suggest a significantly higher burden of HAI among hospitalized neonates in low- and middle-income countries (LMICs).6,7 Infection prevention and control (IPC) strategies that address both patients and their environment are therefore of utmost importance in neonatal care settings, especially in the neonatal intensive care unit (NICU).8
Healthcare-associated infections in the neonate
Central line-associated bloodstream infections
CLABSIs are associated with substantial morbidity and mortality, as well as increased healthcare costs and prolonged length of stay.4,5,9 In the US, Gram-positive pathogens account for the majority of neonatal CLABSIs. Staphylococcus aureus and coagulase negative staphylococci (CONS) account for nearly half of NICU CLABSI events.10 Among Gram-negative pathogens, Escherichia coli and Klebsiella spp. are responsible for the greatest number of infections. Candida albicans remains an important fungal etiology, especially among extremely preterm neonates. Patient factors that contribute to CLABSI risk include prematurity, low birth weight, mucosal barrier injury, and critical illness.11
Catheter-associated urinary tract infection, surgical site infection, and ventilator-associated event
Due to limited use of indwelling urinary catheters in the NICU, reported catheter-associated urinary tract infection (CAUTI) rates have remained low. Despite this, standardized catheter insertion and maintenance bundles should be prioritized as part of effective infection prevention practices. Surgical site infections (SSIs) are associated with considerable morbidity, and hospital-wide prevention efforts often include the NICU. SSI surveillance may be performed locally or as part of a nework for high risk procedures common in neonates, such as ventriculoperitoneal shunt insertion or congenital heart defect repair12 Lack of a standardized neonatal ventilator-associated event (VAE) definition hampers surveillance and prevention efforts. With the availability of revised 2015 pediatric VAE guidelines, some units have opted to identify VAE using standard guidelines.13 Incorporating changes in the fraction of inspired oxygen and mean airway pressure into surveillance definitions used by NICUs could standardize VAE reporting.
Infection prevention and control infrastructure and healthcare-associated infection surveillance in the NICU
Overview of infection prevention and control infrastructure and linkage to the NICU
In the US, federal regulations require an infection control officer who is qualified to oversee a facility’s plan for surveillance, prevention, and control of HAIs. IPC programs typically have a staff of infection preventionists (IPs) and may be governed by an Infection Control Committee comprised of representatives from clinical units, hospital administration, infectious diseases, and other specialties. IPs support target areas through data dissemination, staff education, and implementation of policies and prevention activities. IPC programs will often assign a lead IP to be a liaison to the NICU and its specialized population. Annual risk assessments in the NICU inform identification of opportunities for improvement in key domains (Table 1). By collaborating within and between hospital networks, infections can be prevented, harm reduced, and healthcare costs saved.2,14
Table 1.
Key infection prevention and control domains and special considerations in the neonatal population
| IPC domain | Special considerations in neonates |
|---|---|
| HAI surveillance | NHSN reporting required for CLABSI, stratified by birth weight15 NHSN CLABSI definition provides exclusion for neonatal infections (e.g., GBS, NEC) |
| MDRO colonization | Innovative strategies to reduce transmission (e.g., parental decolonization)19 |
| HH | Potential role for wearing gloves after HH in high-risk populations97 |
| Central line insertion and maintenance | Use of umbilical catheters |
| Topical antisepsis | Povidone-iodine systemic absorption rarely linked to hypothyroidism98 Chlorhexidine use may be restricted by age and weight to reduce potential adverse effects in very preterm neonates33 |
| Medication and IV fluid preparation and administration | Small doses used in neonates may make consistent use of SDV impractical |
| Cleaning and disinfection of reused medical equipment | Specialized equipment used in neonates may be difficult to clean |
| Structure, water, and air | Multi-bed pods pose additional HAI risk due to less physical distancing between patients |
| Environmental cleaning | Avoidance of phenol in the NICU due to risk of hyperbilirubinemia99 |
| Families and visitor policies | Family-centered care and promotion of breastfeeding and human milk feeding Sibling visitation Vaccination policies for family |
| Employee health | No restrictions are necessary for healthcare workers in the NICU who receive routine immunizations |
| Exposures | High risk given critically ill patient population without or incomplete immunization against high-risk pathogens |
| IPC bundles and multimodal improvement strategies | IPC bundles linked to CLABSI risk reduction in the NICU CUSP successfully adapted to the NICU |
Abbreviations: CLABSI – central line-associated bloodstream infection; CUSP – Comprehensive Unit-based Safety Program; GBS – group B Streptococcus; HAI – healthcare-associated infection; HH – hand hygiene; IPC – infection prevention and control; IV – intravenous; MDRO – multi-drug resistant organism; MRSA – methicillin resistant Staphylococcus aureus; NEC – necrotizing enterocolitis; NHSN – National Healthcare Safety Network (NHSN); NICU – neonatal intensive care unit; SDV – single dose vial
Surveillance and reporting requirements
HAIs surveillance in the NICU is a key aspect of performance improvement. The Centers for Disease Control and Prevention (CDC) National Healthcare Safety Network (NHSN) is a surveillance system that provides data collection and reporting capabilities to identify IPC issues, benchmark progress, and comply with public reporting mandates.15 Use of standardized definitions for HAIs creates a mechanism for comparison across healthcare facilities nationally. NHSN requirements for NICUs include reporting of CLABSI events, device days, and patient days. Definitions attempt to account for neonatal infections that may not be catheter-associated (Table 1). NHSN reporting for SSIs, CAUTIs, and VAEs is not required, but these are often tracked locally. When an HAI event or near-miss is identified, root cause analysis – a systematic evaluation of the factors contributing to the event – is beneficial in identifying opportunities for improvement.16
Colonization with resistant organisms
Prospective surveillance for multi-drug resistant organism (MDRO) colonization is limited in the NICU setting and rates of resistant infections are typically lower than in other pediatric units.17 Available MDRO data within US NICUs largely focus on methicillin-resistant S. aureus (MRSA). The recent decline in the prevalence of MRSA colonization and infection in the NICU is likely due to effective IPC measures such as decolonization, cohorting, and use of personal protective equipment (PPE), as well as enhanced antimicrobial stewardship.18,19 However, reports of infections with other resistant pathogens such as Candida auris and carbapenem-resistant Enterobacteriaceae are increasing among neonates, especially in LMICs.20,21
Outbreaks
Recognition of an outbreak requires vigilance by frontline staff and the IPC team; a cluster of infections with a known neonatal pathogen, increasing incidence above baseline, or the emergence of an unusual pathogen may signify an outbreak.22 Recognition that a point source may not be identified should inform broad strategies to improve general IPC practices to contain the outbreak. In some instances, partial or complete unit closure is necessary to contain an outbreak.23
General IPC concepts and considerations in the neonate
Hand hygiene (HH)
HH is the foundation of IPC in any healthcare setting, including the NICU. The World Health Organization (WHO) recognizes five moments of HH (Box 1).24 Although WHO guidelines recommend use of alcohol-based hand rub (ABHR) for 20-30 seconds or use of soap and water for 40-60 seconds, CDC guidelines for HH in healthcare settings recommend a shorter duration of 20 seconds and 15 seconds, respectively.25,26 Use of ABHR rather than antimicrobial soap has been associated with increased compliance.27 Factors that may impede effective HH include limited access to clean water or ABHR and the wearing of artificial nails.28 Direct observation or electronic devices are typically used to monitor HH compliance. Only direct observation can properly capture HH compliance by moment and by HCW role; monitoring may be strengthened through routine observations over time or using ‘secret shoppers’ to reduce bias.29
Box 1. Moments of hand hygiene.
Before patient contact
Before aseptic task
After body fluid exposure
After patient contact
After contact with patient surroundings
Central line insertion and maintenance
Preterm and critically ill neonates commonly require placement of central venous catheters (CVCs) and arterial catheters for provision of parenteral nutrition, medication administration, and hemodynamic monitoring. Umbilical venous and arterial catheters require attention due to their associated increased risk of infection. Recommendations for CLABSI prevention include standardized processes for insertion and maintenance (Box 2).30 Topical antimicrobial ointments at the insertion site, systemic antibiotic prophylaxis, and antibiotic lock prophylaxis are not recommended. Prompt removal of central lines when no longer required is essential. Prolonged CVC presence and increased duration of parenteral nutrition has been associated with increased CLABSI risk in neonates.3,31 Potential facilitators of early line removal include daily discussion of line necessity during rounds, documentation of line necessity in the medical record, and early introduction of enteral feeds.
Box 2. Central line insertion and maintenance.
Central line insertion
Use of insertion checklist
Dedicated procedure cart
Hand hygiene
Skin antisepsis
Use of maximal barrier precautions
Sterile occlusive dressing over PICC and tunneled catheter sites
Dedicated staff for insertion of PICCs100
Central line maintenance
Daily assessment of dressing integrity
Dressing changes weekly and as needed
Prevention of insertion site bleeding
Scrubbing the hub with an appropriate antiseptic prior to access
Regular tubing changes
Reduced access frequency
Daily assessment of need and early catheter removal
Replacement of emergently placed catheters as soon as possible in a controlled setting
Replacement of UVCs with PICCs within the first week of life
Dedicated line maintenance team101
Topical antisepsis in the neonate
Selection of the appropriate topical antiseptic agent in the NICU must carefully consider patient factors (e.g., gestational age, birth weight, skin integrity) as well as intended use. Agents used for topical antisepsis in the NICU include isopropyl alcohol, povidone-iodine, and chlorhexidine. Povidone-iodine is routinely used for skin preparation prior to obtaining blood cultures and to performing surgical procedures. Associated harms include rare reports of systemic absorption with associated hypothyroidism in neonates.32 Chlorhexidine is increasingly used in the NICU, for skin preparation prior to procedures, S. aureus decolonization, and bathing for CLABSI prevention.33-35 Burns and contact dermatitis have been reported, primarily with use of alcohol-based preparations and in young preterm neonates or those with non-intact skin.36 Trace systemic absorption may occur although clinical significance is uncertain.37 Age- and weight-based guidelines are commonly applied to avoid potential side effects.33
Medication and intravenous fluid preparation and administration
Antibiotics, anti-epileptic drugs, and analgesics or sedatives may be stored in the NICU to facilitate timely administration. Injections should be prepared using aseptic technique and following recommended procedures (Box 3). Multi-dose vials (MDV) should be avoided when possible. When used, MDV should be stored appropriately, dated when first opened, and discarded within 28 days unless otherwise specified by the manufacturer. If MDV enter the immediate patient care area, their content should be reserved for a single patient. Single dose vials (SDV) should never be reused. IV fluid solution bags should only be used for a single patient. IV tubing should be changed regularly, between every 96 hours to every 7 days, except for tubing used to administer blood products or fat emulsions, which should be changed within 24 hours of the infusion or according to hospital policy.30
Box 3. Injection safety.
Preparation in area separate from immediate patient care
Aseptic technique/proper cleansing of vials prior to drawing up medication
No reuse of needles and syringes
No needles left in the septum for access
Vials discarded if visible holes in septum
Appropriate sharp disposal in puncture-resistant container accessible to healthcare workers
Scheduled emptying of sharps disposals containers
Cleaning and disinfection of reused medical equipment
Levels of disinfection required for reused devices are based on intended use, and are summarized in Table 2.38 A risk assessment should be conducted to ensure proper levels of disinfection for all devices used in the NICU. Noncritical devices and surfaces (e.g., bed rails, computer keyboards, thermometers) are a potential nidus for transmission and must be cleaned regularly.39 Similarly, hand-held equipment used by ophthalmologists on multiple patients (such as during retinopathy of prematurity exams) must be properly disinfected between use to prevent potential pathogen transmission.40 Due to its greater complexity and risk, facilities may centralize high-level disinfection (HLD) to ensure patient safety and regulatory compliance.41,42 Outbreaks have been associated with airway and gastrointestinal devices due to defective design, improper reprocessing, and automated process failure.43,44 Single use devices should never be reprocessed or reused. During an emergency, federal regulatory guidance should be consulted before single-use items are reprocessed.38 In LMICs, devices are more difficult to procure; reuse may be common, and proper HLD can be challenging.45 WHO guidelines recommend against single-use item reuse but also provide a recommended framework to ensure proper decontamination, cleaning, drying, and storage when reuse is necessary.42
Table 2.
Agents appropriate for low level disinfection and concerns within neonatal intensive care units
| Disinfecting agents Hospital-grade approved agents should be used with proper contact time |
Device examples | NICU-specific issues |
|---|---|---|
| Alcohol (ethyl or isopropyl) 70-90% | Stethoscope | Not appropriate for protein-rich materials (remove residue with soap and water) |
| Hydrogen peroxide 3-5% (non-activated) | Ultrasound probe (only on intact skin) | Can be damaging to surfaces and metals |
| Hydrogen peroxide 0.5% (activated) | Blood pressure cuff Scale |
Can be damaging to surfaces and metals |
| Household bleach (5.25%) diluted 1:500 (100 ppm) | Temperature probe (intact skin) | Can be damaging to surfaces and metals Can be damaging to sensitive electronics If diluting onsite need to mix daily Odor may be bothersome or irritating |
| Horizontal surfaces in care area (e.g., bed rails, bedside tables, keyboards, ventilators, pumps, etc.) | ||
| Quaternary ammonium compounds | Monitor leads (multi-use) | Less damaging to surfaces (e.g., electronics, ultrasound probes, etc.) When mixed with bleach can release chlorine gas, a respiratory irritant |
| Phenols/phenolics | Surfaces/floors | Not recommended for NICU (including floors) May cause hyperbilirubinemia when used on devices and bassinets99 Irritating to skin – use on surfaces only |
| Hypochlorite bleach or saline solution | Ophthalmoscope, calipers, pincers for eye exams | Can leave residue on lenses and limit use Rinsing with sterile water after cleansing can remove residue40 |
Environment
Structure, water, and air
The structure and design of a NICU may influence HAI risk. For example, transmission risk for S. aureus was noted to be higher among infants in multi-bed pods compared to those in single bed rooms.46 However, single occupancy room design is often not feasible, particularly in LMICs. NICUs with multi-bed pods could address the increased risk of HAI transmission by screening and cohorting, limiting shared equipment, or placing physical barriers between patients to prevent the potential for cross-contamination.
Colonization of plumbing fixtures has been linked to NICU outbreaks, both through direct and indirect water exposure.47 Risk mitigation such as avoiding areas of decreased flow and ensuring proper disinfection should be included in water protection programs.48 Sinks should be designated for waste disposal only or HH only.49 Sterile water for infant bathing or dry warmers for human milk should be used to avoid infections associated with tap water, if possible.50 Facilities with untreated source water should install filtration or chemical disinfection at the intake point. Environmental sampling, in the absence of an ongoing outbreak, is of unclear significance, but may be part of an environmental risk assessment.48,51,52 Understanding plumbing and building structure is important to prevent inadvertent introduction of pathogens, if a breach occurs due to a leak or renovation.53
Airflow and ventilation maintenance are guided by federal regulatory standards in the US.54 If windows open or ventilation is decentralized, ensuring adequate exchange and accounting for humidity and potential vector encroachment may be necessary.55 Because a NICU room has fewer air changes per hour than an operating room, emergent bedside surgical procedures for clinically unstable infants may pose an HAI risk. Implementing environmental control protocols during these procedures may be beneficial. A NICU should have at least one airborne isolation room (AIIR) for managing infants and their essential caregivers while preventing exposure to airborne pathogens by other infants and staff.56
Environmental cleaning
Protocols for cleaning and disinfection at regular intervals and at patient discharge should be established to prevent HAI.57,58 Bedside and environmental services (EVS) staff can share routine responsibilities, with clear delineation, to ensure regular cleaning. Routine closure of clinical areas can facilitate deep cleaning while not disrupting infant development, such as with bright lights and loud machinery.59 Adherence monitoring with regular feedback and using dedicated EVS teams are strategies to support effective cleaning.60,61
HAIs and outbreaks due to contaminated equipment requiring humidification (e.g., isolettes, ventilator drains) could result from water, environment, or clinician contamination.62,63 Small size, need for user-specific training, and frequency of use may limit appropriate cleaning of NICU-specific equipment. Increasing device and disinfectant supply may ensure clean devices are available when needed.
Mitigating risk of potential exposures in the NICU
Families and Visitors
To promote family-centered care, NICUs must balance visitation policies with limiting opportunities for infection transmission. There are reports of outbreaks introduced by visitors or caregivers, leading NICUs to opt for intermittent visitor restrictions, such as during respiratory viral season.64,65 However, restrictions might cause parent/caregiver dissatisfaction and adversely affect infant care.66 Restrictions might be avoided with strict HH adherence, shown to reduce respiratory virus transmission.66,67 Regardless of season, screening should be conducted to exclude ill individuals.
Recent guidance prioritizes HH for visitors to limit MRSA transmission within the NICU.68,69 More restrictive visitation policies may apply to young children, who may not be fully vaccinated and have difficulty complying with HH.67,70 Compliance with standard vaccination recommendations among parents and visitors may provide additional protection. Offering influenza vaccine to parents can improve vaccination rates while preventing influenza transmission.71 Ideally, visitors, in particular siblings, should show proof of proper vaccination. However, this may not be practical to implement.
Vaccines that contain inactivated organism components pose no risk of infection to NICU patients. Risk of transmission of live attenuated vaccine virus strains is very low.72 In infants the rotavirus and live attenuated influenza (LAIV) vaccines pose a theoretical risk of transmission of attenuated vaccine virus strains. Units may consider placing patients in precautions (e.g., contact for rotavirus) following receipt of vaccine for up to 2 weeks.
Employees
The CDC provides regularly updated guidance for healthcare worker vaccinations, often overseen by a system’s Employee Health/Occupational Health program.73 Special consideration should be made for seasonal influenza vaccination, as studies show that facilities that mandate seasonal influenza immunization of employees have the highest levels of coverage.74 This is especially important in settings such as the NICU where the majority of patients are age ineligible to receive a seasonal influenza immunization. Receipt of approved live-attenuated vaccines is not contraindicated in HCWs caring for severely immunocompromised patients.72,75 Care must be taken for of recipients of varicella or zoster vaccine, as virus from vesicular lesions formed at the vaccination site or elsewhere may have the potential for transmission.72 Units may consider standard screening for receipt of these vaccines during the previous 1-2 weeks, and to ask specifically about rash following receipt of VZV.72,76 Additionally, some recommend that LAIV recipients wait 1-2 weeks following immunization before caring for vulnerable patients.76 Presenteeism, the practice of coming to work despite symptoms of infectious illness, is a potential source of pathogen transmission to employees and patients alike.77 Employee Health (EH) and IPC can collaboratively promote minimal employee penalties for absences due to illness.78 Any condition preventing adequate HH should result in exclusion from care until HH may be performed. Employees with herpes zoster lesions in a single dermatome should be excluded from the care of varicella non-immune patients in the NICU until their lesions have crusted.79,80
Exposures
Despite prevention efforts, breaches in IPC or exposures to infectious agents will occur requiring a coordinated response. NICUs should collaborate with IPC and EH to develop and enforce policies to manage exposures. Pathogens of concern include severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), measles, VZV, and pertussis. Pre-emptive contact and droplet isolation of exposed infants may be necessary in multi-bed settings, where they can be assessed for the development of symptoms during the incubation period.
VZV transmission from contact with a clinician or visitor with uncovered herpes zoster lesions and the subsequent development of acute infection in a non-immune infant is rare in the post-vaccine era. Exposed non-immune infants should be moved to an AIIR during the incubation period and consideration should be given for administration of immune globulin.56 Pertussis infections pose a significant risk to non-immune neonates, and post-exposure prophylaxis may be indicated, with consideration of the limited safety data available for recommended agents.81,82 Assessing exposure events and notifying families of potential transmission risk is part of a comprehensive exposure plan recommended for NICUs.83
IPC bundles and multi-modal improvement strategies
The use of bundles to reduce HAI risk via implementation of a package of evidence-based practices is a mainstay of IPC. A 2018 systematic review and meta-analysis of 24 NICU-based studies demonstrated a 60% reduction in CLABSI rate with care bundle implementation.84 Care bundle composition varied significantly; the most common element included use of a specific protocol for skin preparation, maximal barrier precautions, and daily assessment of catheter need. IPC bundles have also been used to target other HAIs in the NICU, including VAE, and in response to outbreaks.22,85 Antimicrobial stewardship interventions should be embedded in HAI prevention bundles to link the core concepts of infection prevention and stewardship to optimize neonatal outcomes.86
Multimodal IPC improvement strategies are included in WHO core components for IPC programs and consist of five elements: (1) system change, (2) training and education, (3) monitoring and feedback, (4) reminders and communication, and (5) culture change (Figure 1).87 Multimodal strategies to reduce HAI risk include the Comprehensive Unit-based Safety Program (CUSP), first implemented to reduce CLABSI risk in adult ICUs.88 CUSP has been successfully adapted to the NICU setting, as part of a national quality collaborative.89
Figure 1. The World Health Organization multimodal infection prevention and control improvement strategy.
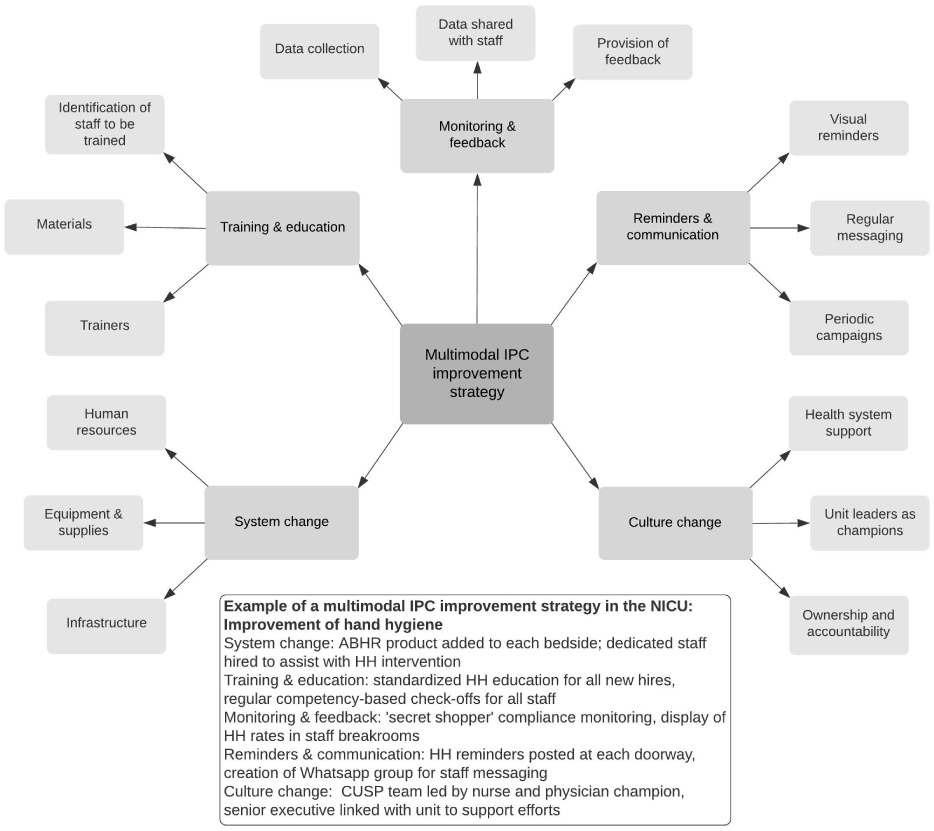
The WHO multimodal IPC improvement strategy consists of five elements and is a core component of IPC programs.87 Abbreviations: ABHR — alcohol-based hand rub; CUSP — Comprehensive Unit-based Safety Program; HH — hand hygiene; IPC — infection prevention and control; NICU — neonatal intensive care unit; WHO — World Health Organization.
Limited Resource Settings
Burden of healthcare-associated infections in low- and middle-income country NICUs
LMIC healthcare facilities increasingly care for preterm and ill neonates who are at risk for HAIs, especially due to multi-drug resistant Gram-negative pathogens.7 Given limited treatment options and increased morbidity and mortality associated with these infections, optimizing IPC practices to reduce HAI risk is a key strategy. Delivery of IPC best practices in LMIC healthcare facilities may be compromised by water supply, high patient-to-nurse ratios, facility overcrowding, PPE and HH supply shortages, reuse of single-use items, and high burden of AMR colonization and infection, among other factors.90
Innovative approaches to preventing healthcare-associated infections in limited-resource settings
Kangaroo mother care, or provision of prolonged skin-to-skin contact and exclusive breastfeeding, was developed to support thermoregulation in low birth weight neonates in LMICs and is associated with decreased risk of sepsis and mortality.91 In settings where omphalitis and associated sepsis is more common, use of topical antiseptics for cord care may be indicated to reduce risk. Chlorhexidine application to the cord has been shown to be effective in reduction of cord bacterial burden and resultant neonatal infections; data to support routine use in hospitalized neonates are scarce.92,93 Topical emollient massage, a common practice in South Asia and other LMIC settings, has been demonstrated to improve skin integrity and reduce late onset sepsis risk and mortality among hospitalized preterm neonates in LMICs.94,95 Use of sunflower seed oil or coconut oil for topical emollient massage in hospitalized neonates with an HAI risk is a promising intervention, given its acceptance by caregivers and cost-effectiveness.96
Summary
Numerous unique challenges exist within the NICU requiring innovative IPC strategies to deliver safe care to vulnerable neonates. Collaborative efforts to promote HH, standardize cleaning of specialized equipment, maintain environmental cleaning, perform HAI surveillance, and implement bundled interventions to prevent HAIs are integral to a NICU IPC program. Challenges of HAI prevention exist in both resource advantaged and limited settings can be addressed through innovation and utilization of local expertise and resources.
Key Points:
Neonatal healthcare-associated infections (HAIs) are associated with significant morbidity and mortality.
The NICU poses unique infection prevention and control (IPC) challenges due to its specialized population, equipment, and environment.
IPC in the NICU requires a collaborative relationship between unit-based staff and the hospital’s IPC program as well as local, state, and federal resources.
Innovative strategies are needed to reduce HAI risk in limited resource settings.
Clinical Care Points.
Successful IPC programs in the NICU rely on a collaborative relationship between unit-based staff and the facility’s IPC infrastructure.
HAI surveillance and root cause analyses should inform performance improvement in the NICU.
Disinfection and environmental cleaning in the NICU must consider the population, structure, and environment unique to the NICU.
IPC bundles and multimodal improvement strategies are effective in reducing HAI risks in the NICU.
Acknowledgments
Disclosures: J.J. receives support from the National Institutes of Health (K23HD100594). I.C.A. and J.K.S. have no disclosures.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Stoll BJ, Hansen NI, Adams-Chapman I, et al. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. Jama. 2004;292(19):2357–2365. [DOI] [PubMed] [Google Scholar]
- 2.Donovan EF, Sparling K, Lake MR, et al. The investment case for preventing NICU-associated infections. Am J Perinatol. 2013;30(3):179–184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Stoll BJ, Hansen N, Fanaroff AA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics. 2002;110(2 Pt 1):285–291. [DOI] [PubMed] [Google Scholar]
- 4.Patrick SW, Kawai AT, Kleinman K, et al. Health care-associated infections among critically ill children in the US, 2007-2012. Pediatrics. 2014;134(4):705–712. [DOI] [PubMed] [Google Scholar]
- 5.Hsu HE, Mathew R, Wang R, et al. Health care-associated infections among critically ill children in the US, 2013-2018. JAMA Pediatr. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosenthal VD, Lynch P, Jarvis WR, et al. Socioeconomic impact on device-associated infections in limited-resource neonatal intensive care units: findings of the INICC. Infection. 2011;39(5):439–450. [DOI] [PubMed] [Google Scholar]
- 7.Zaidi AK, Huskins WC, Thaver D, Bhutta ZA, Abbas Z, Goldmann DA. Hospital-acquired neonatal infections in developing countries. Lancet. 2005;365(9465):1175–1188. [DOI] [PubMed] [Google Scholar]
- 8.Suleyman G, Alangaden G, Bardossy AC. The role of environmental contamination in the transmission of nosocomial pathogens and healthcare-associated infections. Curr Infect Dis Rep. 2018;20(6):12. [DOI] [PubMed] [Google Scholar]
- 9.Snyder AN, Burjonrappa S. Central line associated blood stream infections in gastroschisis patients: A nationwide database analysis of risks, outcomes, and disparities. J Pediatr Surg. 2020;55(2):286–291. [DOI] [PubMed] [Google Scholar]
- 10.Weiner-Lastinger LM, Abner S, Benin AL, et al. Antimicrobial-resistant pathogens associated with pediatric healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network, 2015-2017. Infect Control Hosp Epidemiol. 2020;41(1):19–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dahan M, O’Donnell S, Hebert J, et al. CLABSI Risk Factors in the NICU: Potential for Prevention: A PICNIC Study. Infect Control Hosp Epidemiol. 2016;37(12):1446–1452. [DOI] [PubMed] [Google Scholar]
- 12.Schaffzin JK, Harte L, Marquette S, et al. Surgical site infection reduction by the Solutions for Patient Safety Hospital Engagement Network. Pediatrics. 2015;136(5):e1353–1360. [DOI] [PubMed] [Google Scholar]
- 13.Cocoros NM, Priebe GP, Logan LK, et al. A pediatric approach to ventilator-associated events surveillance. Infect Control Hosp Epidemiol. 2017;38(3):327–333. [DOI] [PubMed] [Google Scholar]
- 14.Wheeler DS, Giaccone MJ, Hutchinson N, et al. A hospital-wide quality-improvement collaborative to reduce catheter-associated bloodstream infections. Pediatrics. 2011;128(4):e995–e1004; quiz e1004-1007. [DOI] [PubMed] [Google Scholar]
- 15.Centers for Disease Control and Prevention. NHSN Patient Safety Component Manual. https://www.cdc.gov/nhsn/pdfs/pscmanual/pcsmanual_current.pdf. Published 2020. Accessed December 13, 2020. [Google Scholar]
- 16.Venier AG. Root cause analysis to support infection control in healthcare premises. J Hosp Infect. 2015;89(4):331–334. [DOI] [PubMed] [Google Scholar]
- 17.Lake JG, Weiner LM, Milstone AM, Saiman L, Magill SS, See I. Pathogen distribution and antimicrobial resistance among pediatric healthcare-associated infections reported to the National Healthcare Safety Network, 2011-2014. Infect Control Hosp Epidemiol. 2018;39(1):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ericson JE, Popoola VO, Smith PB, et al. Burden of invasive Staphylococcus aureus infections in hospitalized infants. JAMA Pediatr. 2015;169(12):1105–1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Milstone AM, Voskertchian A, Koontz DW, et al. Effect of treating parents colonized with Staphylococcus aureus on transmission to neonates in the intensive care unit: A randomized clinical trial. Jama. 2020;323(4):319–328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Armstrong PA, Rivera SM, Escandon P, et al. Hospital-associated multicenter outbreak of emerging fungus Candida auris, Colombia, 2016. Emerg Infect Dis. 2019;25(7):1339–1346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Johnson J, Robinson ML, Rajput UC, et al. High burden of bloodstream infections associated with antimicrobial resistance and mortality in the neonatal intensive care unit in Pune, India. Clin Infect Dis. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Johnson J, Quach C. Outbreaks in the neonatal ICU: a review of the literature. Curr Opin Infect Dis. 2017;30(4):395–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gramatniece A, Silamikelis I, Zahare I, et al. Control of Acinetobacter baumannii outbreak in the neonatal intensive care unit in Latvia: whole-genome sequencing powered investigation and closure of the ward. Antimicrob Resist Infect Control. 2019;8:84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.World Health Organization. Five moments for hand hygiene. https://www.who.int/gpsc/tools/Five_moments/en/. Accessed December 13, 2020, 2020.
- 25.Boyce JM, Pittet D. Guideline for hand hygiene in health-care settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep. 2002;51(Rr-16):1–45, quiz CE41-44. [PubMed] [Google Scholar]
- 26.World Health Organization. Hand hygiene: Why, how & when? https://www.who.int/gpsc/5may/Hand_Hygiene_Why_How_and_When_Brochure.pdf. Published 2009. Accessed December 13, 2020.
- 27.Cohen B, Saiman L, Cimiotti J, Larson E. Factors associated with hand hygiene practices in two neonatal intensive care units. Pediatr Infect Dis J. 2003;22(6):494–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gupta A, Della-Latta P, Todd B, et al. Outbreak of extended-spectrum beta-lactamase-producing Klebsiella pneumoniae in a neonatal intensive care unit linked to artificial nails. Infect Control Hosp Epidemiol. 2004;25(3):210–215. [DOI] [PubMed] [Google Scholar]
- 29.Chen LF, Vander Weg MW, Hofmann DA, Reisinger HS. The Hawthorne effect in infection prevention and epidemiology. Infect Control Hosp Epidemiol. 2015;36(12):1444–1450. [DOI] [PubMed] [Google Scholar]
- 30.O’Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sengupta A, Lehmann C, Diener-West M, Perl TM, Milstone AM. Catheter duration and risk of CLA-BSI in neonates with PICCs. Pediatrics. 2010;125(4):648–653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Linder N, Davidovitch N, Reichman B, et al. Topical iodine-containing antiseptics and subclinical hypothyroidism in preterm infants. J Pediatr. 1997;131(3):434–439. [DOI] [PubMed] [Google Scholar]
- 33.Johnson J, Bracken R, Tamma PD, Aucott SW, Bearer C, Milstone AM. Trends in chlorhexidine use in US neonatal intensive care units: Results from a follow-up national survey. Infect Control Hosp Epidemiol. 2016;37(9):1116–1118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.McCord H, Fieldhouse E, El-Naggar W. Current Practices of Antiseptic Use in Canadian Neonatal Intensive Care Units. Am J Perinatol. 2019;36(2):141–147. [DOI] [PubMed] [Google Scholar]
- 35.Quach C, Milstone AM, Perpête C, Bonenfant M, Moore DL, Perreault T. Chlorhexidine bathing in a tertiary care neonatal intensive care unit: impact on central line-associated bloodstream infections. Infect Control Hosp Epidemiol. 2014;35(2):158–163. [DOI] [PubMed] [Google Scholar]
- 36.Vanzi V, Pitaro R. Skin injuries and chlorhexidine gluconate-based antisepsis in early premature infants: A case report and review of the literature. J Perinat Neonatal Nurs. 2018;32(4):341–350. [DOI] [PubMed] [Google Scholar]
- 37.Chapman AK, Aucott SW, Gilmore MM, Advani S, Clarke W, Milstone AM. Absorption and tolerability of aqueous chlorhexidine gluconate used for skin antisepsis prior to catheter insertion in preterm neonates. J Perinatol. 2013;33(10):768–771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Rutala WA WD, and the Healthcare Infection Control Practices Advisory Committee (HICPAC),. Guideline for disinfection and sterilization in healthcare facilities. https://www.cdc.gov/infectioncontrol/guidelines/disinfection/. Published 2008. Updated May 2019. Accessed December 13, 2020. [Google Scholar]
- 39.v Dijk Y, Bik EM, Hochstenbach-Vernooij S, et al. Management of an outbreak of Enterobacter cloacae in a neonatal unit using simple preventive measures. J Hosp Infect. 2002;51(1):21–26. [DOI] [PubMed] [Google Scholar]
- 40.Sammons JS, Graf EH, Townsend S, et al. Outbreak of adenovirus in a neonatal intensive care unit: critical importance of equipment cleaning during inpatient ophthalmologic examinations. Ophthalmology. 2019;126(1):137–143. [DOI] [PubMed] [Google Scholar]
- 41.Rutala WA, Weber DJ. Reprocessing semicritical items: Outbreaks and current issues. Am J Infect Control. 2019;47s:A79–a89. [DOI] [PubMed] [Google Scholar]
- 42.World Health Organization PAHO. Decontamination and reprocessing of medical devices for health-care facilities. https://www.who.int/infection-prevention/publications/decontamination/en/. Published 2016. Accessed December 13, 2020.
- 43.Kenters N, Huijskens EG, Meier C, Voss A. Infectious diseases linked to cross-contamination of flexible endoscopes. Endosc Int Open. 2015;3(4):E259–265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Weber DJ, Rutala WA. Lessons from outbreaks associated with bronchoscopy. Infect Control Hosp Epidemiol. 2001;22(7):403–408. [DOI] [PubMed] [Google Scholar]
- 45.Ogunsola FT, Mehtar S. Challenges regarding the control of environmental sources of contamination in healthcare settings in low-and middle-income countries - a narrative review. Antimicrob Resist Infect Control. 2020;9(1):81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Washam MC, Ankrum A, Haberman BE, Staat MA, Haslam DB. Risk factors for Staphylococcus aureus acquisition in the neonatal intensive care unit: A matched case-case-control study. Infect Control Hosp Epidemiol. 2018;39(1):46–52. [DOI] [PubMed] [Google Scholar]
- 47.Verweij PE, Meis JF, Christmann V, et al. Nosocomial outbreak of colonization and infection with Stenotrophomonas maltophilia in preterm infants associated with contaminated tap water. Epidemiol Infect. 1998;120(3):251–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.ANSI/ASHRAE. Legionellosis: Risk management for building water systems. In. Vol 188-20182018. [Google Scholar]
- 49.Parkes LO, Hota SS. Sink-related outbreaks and mitigation strategies in healthcare facilities. Curr Infect Dis Rep. 2018;20(10):42. [DOI] [PubMed] [Google Scholar]
- 50.Molina-Cabrillana J, Artiles-Campelo F, Dorta-Hung E, et al. Outbreak of Pseudomonas aeruginosa infections in a neonatal care unit associated with feeding bottles heaters. Am J Infect Control. 2013;41(2):e7–9. [DOI] [PubMed] [Google Scholar]
- 51.Gamage SD, Kralovic SM, Roselle GA. The case for routine environmental testing for Legionella bacteria in healthcare facility water distribution systems-reconciling CDC position and guidance regarding risk. Clin Infect Dis. 2015;61(9):1487–1488. [DOI] [PubMed] [Google Scholar]
- 52.Demirjian A, Lucas CE, Garrison LE, et al. The importance of clinical surveillance in detecting legionnaires’ disease outbreaks: a large outbreak in a hospital with a Legionella disinfection system-Pennsylvania, 2011-2012. Clin Infect Dis. 2015;60(11):1596–1602. [DOI] [PubMed] [Google Scholar]
- 53.Bryce EA, Walker M, Scharf S, et al. An outbreak of cutaneous aspergillosis in a tertiary-care hospital. Infect Control Hosp Epidemiol. 1996;17(3):170–172. [DOI] [PubMed] [Google Scholar]
- 54.ANSI/ASHRAE/ASHE. Ventilation of health care facilities. In. Vol 170-20172017. [Google Scholar]
- 55.World Health Organization. Natural ventilation for infection control in health-care settings. https://www.who.int/water_sanitation_health/publications/natural_ventilation.pdf. Published 2009. Accessed February 18, 2021. [PubMed]
- 56.Kimberlin DW BM, Jackson MA, Long SS; American Academy of Pediatrics, Committee on Infectious Diseases,. Red book: 2018-2021 report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2018. [Google Scholar]
- 57.Li QF, Xu H, Ni XP, et al. Impact of relocation and environmental cleaning on reducing the incidence of healthcare-associated infection in NICU. World J Pediatr. 2017;13(3):217–221. [DOI] [PubMed] [Google Scholar]
- 58.Schulster LM CR, Arduino MJ, Carpenter J, Donlan R, Ashford D, Besser R, Fields B, McNeil MM, Whitney C, Wong S, Juranek D, Cleveland J,. Guidelines for environmental infection control in health-care facilities. Recommendations from the CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). https://www.cdc.gov/infectioncontrol/pdf/guidelines/environmental/index.html. Published 2004. Updated July 2019. Accessed December 13, 2020.
- 59.Almadhoob A, Ohlsson A. Sound reduction management in the neonatal intensive care unit for preterm or very low birth weight infants. Cochrane Database Syst Rev. 2020;1(1):Cd010333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Deshpande A, Donskey CJ. Practical approaches for assessment of daily and post-discharge room disinfection in healthcare facilities. Curr Infect Dis Rep. 2017;19(9):32. [DOI] [PubMed] [Google Scholar]
- 61.Sitzlar B, Deshpande A, Fertelli D, Kundrapu S, Sethi AK, Donskey CJ. An environmental disinfection odyssey: evaluation of sequential interventions to improve disinfection of Clostridium difficile isolation rooms. Infect Control Hosp Epidemiol. 2013;34(5):459–465. [DOI] [PubMed] [Google Scholar]
- 62.Wenger PN, Tokars JI, Brennan P, et al. An outbreak of Enterobacter hormaechei infection and colonization in an intensive care nursery. Clin Infect Dis. 1997;24(6):1243–1244. [DOI] [PubMed] [Google Scholar]
- 63.Etienne KA, Subudhi CP, Chadwick PR, et al. Investigation of a cluster of cutaneous aspergillosis in a neonatal intensive care unit. J Hosp Infect. 2011;79(4):344–348. [DOI] [PubMed] [Google Scholar]
- 64.Dunn GL, Tapson H, Davis J, Gobin M. Outbreak of Piv-3 in a neonatal intensive care unit in England. Pediatr Infect Dis J. 2017;36(3):344–345. [DOI] [PubMed] [Google Scholar]
- 65.Popoola VO, Budd A, Wittig SM, et al. Methicillin-resistant Staphylococcus aureus transmission and infections in a neonatal intensive care unit despite active surveillance cultures and decolonization: challenges for infection prevention. Infect Control Hosp Epidemiol. 2014;35(4):412–418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Murray PD, Swanson JR. Visitation restrictions: is it right and how do we support families in the NICU during COVID-19? J Perinatol. 2020;40(10):1576–1581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Linam WM, Marrero EM, Honeycutt MD, Wisdom CM, Gaspar A, Vijayan V. Focusing on families and visitors reduces healthcare associated respiratory viral infections in a neonatal intensive care unit. Pediatr Qual Saf. 2019;4(6):e242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Goldstein ND, Eppes SC, Mackley A, Tuttle D, Paul DA. A network model of hand hygiene: How good is good enough to stop the spread of MRSA? Infect Control Hosp Epidemiol. 2017;38(8):945–952. [DOI] [PubMed] [Google Scholar]
- 69.Akinboyo IC, Zangwill KM, Berg WM, Cantey JB, Huizinga B, Milstone AM. SHEA neonatal intensive care unit (NICU) white paper series: Practical approaches to Staphylococcus aureus disease prevention. Infect Control Hosp Epidemiol. 2020;41(11):1251–1257. [DOI] [PubMed] [Google Scholar]
- 70.Shui JE, Messina M, Hill-Ricciuti AC, et al. Impact of respiratory viruses in the neonatal intensive care unit. J Perinatol. 2018;38(11):1556–1565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120(3):e617–621. [DOI] [PubMed] [Google Scholar]
- 72.Kamboj M, Sepkowitz KA. Risk of transmission associated with live attenuated vaccines given to healthy persons caring for or residing with an immunocompromised patient. Infect Control Hosp Epidemiol. 2007;28(6):702–707. [DOI] [PubMed] [Google Scholar]
- 73.Advisory Committee on Immunization Practices CfDCaP. Immunization of health-care personnel: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(Rr-7):1–45. [PubMed] [Google Scholar]
- 74.Black CL, Yue X, Ball SW, et al. Influenza vaccination coverage among health care personnel - United States, 2016-17 influenza season. MMWR Morb Mortal Wkly Rep. 2017;66(38):1009–1015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Shearer WT, Fleisher TA, Buckley RH, et al. Recommendations for live viral and bacterial vaccines in immunodeficient patients and their close contacts. J Allergy Clin Immunol. 2014;133(4):961–966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Grohskopf LA, Alyanak E, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices - United States, 2019-20 influenza Season. MMWR Recomm Rep. 2019;68(3):1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Kuster SP, Böni J, Kouyos RD, et al. Absenteeism and presenteeism in healthcare workers due to respiratory illness. Infect Control Hosp Epidemiol. 2020:1–6. [DOI] [PubMed] [Google Scholar]
- 78.Szymczak JE, Smathers S, Hoegg C, Klieger S, Coffin SE, Sammons JS. Reasons why physicians and advanced practice clinicians work while sick: A mixed-methods analysis. JAMA Pediatr. 2015;169(9):815–821. [DOI] [PubMed] [Google Scholar]
- 79.Gelber SE, Ratner AJ. Hospital-acquired viral pathogens in the neonatal intensive care unit. Semin Perinatol. 2002;26(5):346–356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Friedman CA, Temple DM, Robbins KK, Rawson JE, Wilson JP, Feldman S. Outbreak and control of varicella in a neonatal intensive care unit. Pediatr Infect Dis J. 1994;13(2):152–154. [PubMed] [Google Scholar]
- 81.Schaffzin JKCB. Pertussis. In: Kline MW, ed. Rudolph’s Pediatrics. 23rd edition ed. New York, New York: McGraw Hill Medical; 2018. [Google Scholar]
- 82.Tiwari T, Murphy TV, Moran J. Recommended antimicrobial agents for the treatment and postexposure prophylaxis of pertussis: 2005 CDC Guidelines. MMWR Recomm Rep. 2005;54(Rr-14):1–16. [PubMed] [Google Scholar]
- 83.Kellie SM, Makvandi M, Muller ML. Management and outcome of a varicella exposure in a neonatal intensive care unit: lessons for the vaccine era. Am J Infect Control. 2011;39(10):844–848. [DOI] [PubMed] [Google Scholar]
- 84.Payne V, Hall M, Prieto J, Johnson M. Care bundles to reduce central line-associated bloodstream infections in the neonatal unit: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2018;103(5):F422–f429. [DOI] [PubMed] [Google Scholar]
- 85.Gokce IK, Kutman HGK, Uras N, Canpolat FE, Dursun Y, Oguz SS. Successful Implementation of a Bundle Strategy to Prevent Ventilator-Associated Pneumonia in a Neonatal Intensive Care Unit. J Trop Pediatr. 2018;64(3):183–188. [DOI] [PubMed] [Google Scholar]
- 86.Akinboyo IC, Gerber JS. Principles, policy and practice of antibiotic stewardship. Semin Perinatol. 2020:151324. [DOI] [PubMed] [Google Scholar]
- 87.World Health Organization. Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level. https://apps.who.int/iris/bitstream/handle/10665/251730/9789241549929-eng.pdf;jsessionid=1786EFF9B27E663EF00D501C4385053D?sequence=1. Published 2016. Accessed December 13, 2020. [PubMed]
- 88.Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–2732. [DOI] [PubMed] [Google Scholar]
- 89.Lin DM, Weeks K, Holzmueller CG, Pronovost PJ, Pham JC. Maintaining and sustaining the On the CUSP: stop BSI model in Hawaii. Jt Comm J Qual Patient Saf. 2013;39(2):51–60. [DOI] [PubMed] [Google Scholar]
- 90.Weinshel K, Dramowski A, Hajdu Á, et al. Gap analysis of infection control practices in low- and middle-income countries. Infect Control Hosp Epidemiol. 2015;36(10):1208–1214. [DOI] [PubMed] [Google Scholar]
- 91.Boundy EO, Dastjerdi R, Spiegelman D, et al. Kangaroo Mother Care and Neonatal Outcomes: A Meta-analysis. Pediatrics. 2016;137(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Imdad A, Mullany LC, Baqui AH, et al. The effect of umbilical cord cleansing with chlorhexidine on omphalitis and neonatal mortality in community settings in developing countries: a meta-analysis. BMC Public Health. 2013;13 Suppl 3(Suppl 3):S15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Sinha A, Sazawal S, Pradhan A, Ramji S, Opiyo N. Chlorhexidine skin or cord care for prevention of mortality and infections in neonates. Cochrane Database Syst Rev. 2015(3):Cd007835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Darmstadt GL, Saha SK, Ahmed AS, et al. Effect of topical emollient treatment of preterm neonates in Bangladesh on invasion of pathogens into the bloodstream. Pediatr Res. 2007;61(5 Pt 1):588–593. [DOI] [PubMed] [Google Scholar]
- 95.Salam RA, Darmstadt GL, Bhutta ZA. Effect of emollient therapy on clinical outcomes in preterm neonates in Pakistan: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2015;100(3):F210–215. [DOI] [PubMed] [Google Scholar]
- 96.LeFevre A, Shillcutt SD, Saha SK, et al. Cost-effectiveness of skin-barrier-enhancing emollients among preterm infants in Bangladesh. Bull World Health Organ. 2010;88(2):104–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Kaufman DA, Blackman A, Conaway MR, Sinkin RA. Nonsterile glove use in addition to hand hygiene to prevent late-onset infection in preterm infants: randomized clinical trial. JAMA Pediatr. 2014;168(10):909–916. [DOI] [PubMed] [Google Scholar]
- 98.Mitchell IM, Pollock JC, Jamieson MP, Fitzpatrick KC, Logan RW. Transcutaneous iodine absorption in infants undergoing cardiac operation. Ann Thorac Surg. 1991;52(5):1138–1140. [DOI] [PubMed] [Google Scholar]
- 99.Doan HM, Keith L, Shennan AT. Phenol and neonatal jaundice. Pediatrics. 1979;64(3):324–325. [PubMed] [Google Scholar]
- 100.Taylor T, Massaro A, Williams L, et al. Effect of a dedicated percutaneously inserted central catheter team on neonatal catheter-related bloodstream infection. Adv Neonatal Care. 2011;11(2):122–128. [DOI] [PubMed] [Google Scholar]
- 101.Holzmann-Pazgal G, Kubanda A, Davis K, Khan AM, Brumley K, Denson SE. Utilizing a line maintenance team to reduce central-line-associated bloodstream infections in a neonatal intensive care unit. J Perinatol. 2012;32(4):281–286. [DOI] [PubMed] [Google Scholar]