

Abstract
Robust evidence is needed for the hazardous effects of outdoor particulate matter (PM) on mortality and morbidity from all types of cancers. To summarize and meta-analyze the association between PM and cancer, published articles reporting associations between outdoor PM exposure and any type of cancer with individual outcome assessment that provided a risk estimate in cohort studies were identified via systematic searches. Of 3,256 records, 47 studies covering 13 cancer sites (30 for lung cancer, 12 for breast cancer, 11 for other cancers) were included in the quantitative evaluation. The pooled relative risks (RRs) for lung cancer incidence or mortality associated with every 10-μg/m3 PM2.5 or PM10 were 1.16 (95% confidence interval [CI], 1.10–1.23; I2 = 81%) or 1.22 (95% CI, 1.02–1.45; I2 = 96%), respectively. Increased but non-significant risks were found for breast cancer. Other cancers were shown to be associated with PM exposure in some studies but not consistently and thus warrant further investigation.
Keywords: particulate matter, air pollution, cancer, systematic review, meta-analysis
Graphical abstract
Public summary
-
•
Updated evidence for the association between PM and lung cancer risk has been provided
-
•
Associations between PM and cancer risks from 13 sites were summarized
-
•
Further studies should be conducted to fill the research gaps
Introduction
Cancer is a major public health problem, with over 19 million incident cases and 9 million deaths globally in 2020.1 To reduce the incidence and mortality of cancer, the known risk factors need to be controlled.
Air pollution, especially ambient particulate matter (PM), is a major environmental problem that can cause adverse health impacts.2,3 Inhaled particles affect the lungs by causing chronic systemic inflammation, oxidative stress, and DNA damage to lung tissues.4 In addition to depositing in airways, particles can also move into interstitial spaces between alveoli and circulate to other organs, which may be relevant for carcinogenic processes, although the potential mechanisms have not been fully explained.5 Thus, PM should not only play a role in carcinogen progression in lung cancer, but also other cancers.
There have been some systematic reviews summarizing the relationship between PM and cancers. A previous meta-analysis by the International Agency for Research on Cancer (IARC) has summarized ambient PM exposure and lung cancer risk published before 2014. However, the search was conducted only in the PubMed database and included both cohort and case-control studies.6 Similarly, a combination of all types of study design was conducted in some other articles.7, 8, 9 In addition, some reviews pooled all respiratory tract diseases or cancers of different sites together.8,10,11
Combining studies with various designs may introduce more bias and heterogeneity. Therefore, to give more robust evidence and comprehensively summarize the relationship between PM and cancer risk, we conducted a systematic literature review and meta-analysis. Our aims were to examine the association between PM and cancer-specific risk among cohort studies and to examine differences in risk between various subgroups, such as by smoking status, histological subtypes, and exposure assessment methods.
Methods
Search strategy
For this systematic review and meta-analysis, we searched MEDLINE, Embase, PsycInfo, CINAHL, EMCARE, and Scopus from the beginning of each database to 20 December 2019 and updated (last search 20 November 2020). Search terms included keywords related to cancer (“neoplasia,” “tumor,” “cancer,” “melanoma,” “leukemia,” “lymphoma,” “adenocarcinoma,” “hemangioma”), combined with keywords related to PM with an aerodynamic diameter less than or equal to 2.5 or 10 μm (PM2.5 or PM10) (“fine particles,” “particulate matter,” “particulate air pollution,” “PM2.5,” “PM10”) and specific study types (“cohort study,” “follow-up study,” “incidence study,” “concurrent study,” “prospective study,” “retrospective study,” “longitude study”) (Table S1). We also extended the search to papers or reports cited in the literature, but not in the selected databases. We included studies if the design was a cohort study; the exposure of interest was measured PM2.5 or PM10; the endpoint of interest was cancer-specific incident or mortality; authors provided a risk estimate, such as a hazard ratio (HR), relative risk (RR), or odds ratio (OR) per unit; we excluded animal experiments, and those with no language restrictions. In addition, we also checked the references cited by World Health Organization (WHO) and IARC documents and in the articles. The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines were followed to identify the studies on ambient PM and cancer incidence or mortality.
Study eligibility criteria
The criteria used to select studies were: (1) the study was published in a scholarly peer-reviewed journal; (2) the study was designed as a cohort study, with ecological studies with data for both outcome and exposure collected only at an aggregated level excluded; (3) the exposure to PM was specifically defined as PM10 or PM2.5; (4) individual outcomes for cancer (including total and site-specific cancers) were reported; (5) HR/relative risks (RR)/OR of PM exposure were reported; (6) quantitative estimates of the change in cancer incidence or mortality associated with every unit change of exposure to PM2.5 and/or PM10 were reported or could be calculated from the published data; (7) for studies with overlapping study populations and time periods, only the study with the largest sample size and/or the longest follow-up period was selected for the meta-analysis.
Study selection
Two investigators (P.Y. and S.G.) conducted title and abstract screening independently and then reviewed the full text. Disagreements were resolved by discussion with a third reviewer (R.X.).
Data extraction
For each study, the following details were extracted: (1) reference details (authors and year of publication); (2) study details (name, country, study period, study population, case numbers, outcome assessment, concentrations of PM exposure, exposure time assessment, exposure source, and confounder adjustments); (3) effect (RR/HR/OR per unit exposure and 95% confidence interval [CI]); (4) subgroup details (exposure assessment method, smoking, gender, histological subtypes, lag time).
Study quality assessment
We used the National Institute of Health (NIH) Quality Assessment of Observational Cohort and Cross-Sectional Studies (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools) to assess the study quality. The assessment was conducted by two authors (P.Y. and S.G.) independently and discussed with the third author (R.X.) for any disagreement. Nine items included in the assessment are shown in Table S2. Each item was equivalent to one score and the tallied score translated to a rating of quality. We considered articles that scored 9 as good quality; articles that scored 7–8 as fair quality, and 0–6 as poor quality. All studies included were evaluated to be good or fair (Table S3).
The overall quality of the evidence was evaluated by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system,12,13 yielding a score between high, moderate, low, and very low. We considered the cohort studies as the sources with high-quality evidence, so all studies included were marked as high as a starting point. The original score could be upgraded/downgraded according to five downgrading (risk of bias, imprecision, inconsistency, indirectness, and publication bias) and three upgrading domains (dose-response trend, residual confounding, and the magnitude of associations). Tables S4–S9 show the overall judgment for the association between PM and the risk of cancer.
Data analysis
All results were estimated with standardized increments of a 10-μg/m3 increase in exposures to PM2.5 and PM10. We calculated the RR for a standardized increment for each pollutant by applying the following formula:
where ln is the log to the base e.
To evaluate the association between PM and cancer risk, a pooled RR ratio and 95% CI was calculated from the adjusted RR ratio and 95% CI in each study. To test heterogeneity across studies, we used the Higgins I2 test to determine the percentage of the total variation. I2 was computed as follows:
where Q was Cochran's heterogeneity statistic and df indicated the degree of freedom. I2 values ranged from 0% (no heterogeneity observed) to 100% (maximal heterogeneity), with values > 75% indicating substantial heterogeneity. A random-effects model based on the DerSimonian and Laird method was used for calculating the overall RR and 95% CI values because the population and methodologies differed between the studies.14
Subgroup and sensitivity analyses were performed to evaluate the influences of selected studies and participant characteristics on pooled results. All analyses were performed with R software version 3.6.1 using the packages meta and metafor. This review was registered with PROSPERO, CRD42020161986.
Results
Study characteristics
Out of 3,256 records identified by the search, 1,058 studies were given title screening after duplicates were removed. Abstracts of the papers retrieved in the electronic search were screened manually for topic relevance and 71 potentially relevant articles underwent a further full-text review. Finally, 47 articles were included in the statistical analyses (Figure 1). Thirty articles15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44 were included in a meta-analysis of PM exposure and lung cancer risk.
Figure 1.

Study selection
For breast cancer, seven studies15,45, 46, 47, 48, 49, 50 took incidence as the endpoint, while another five studies40,51, 52, 53, 54 focused on mortality. There were 10 studies49,51,54, 55, 56, 57, 58, 59, 60, 61 reporting other cancers, which were reviewed but not included in the meta-analysis. No additional studies were identified by scanning the reference lists of previous studies or the WHO website.
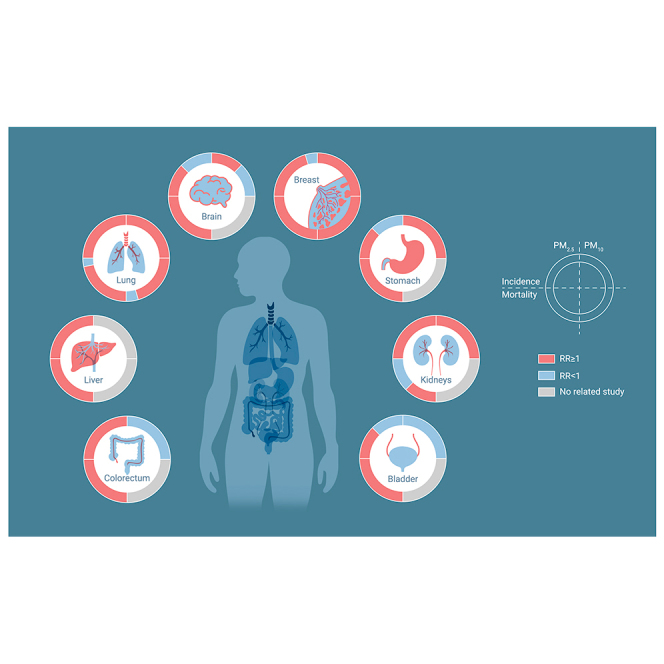
Table 1 summarizes the details of the studies included in the systematic review sorted by the publication year. Most of the studies included in the review reported adverse impacts for cancers of lung, breast, stomach, liver, and kidney, although several studies reported RRs less than 1. The associations between PM10 and colorectal or brain cancers were still not clear.
Table 1.
Summary of studies included in systematic review of cancer risk associated with PM exposure
| Number | Reference | Study | Study period | Cancer | Outcome | Exposure (mean, SD) | Exposure time assessment | Exposure assessment | Covariate adjustment |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Coleman et al. 202051 | Public National Health Interview Survey | 1987–2014 | cancer specific | mortality | PM2.5 (10.7, 2.4) | 1-, 5-, 10-, and 15-y moving average | fix monitor | age, sex, smoking status, education, income, BMI |
| 2 | Guo et al. 202055 | Taiwan National Death Registry | 2001–2016 | gastrointestinal cancer | mortality | PM2.5 (26.57, 7.6) | 2-y moving average | satellite | age, sex, smoking status, education, BMI, occupation |
| 3 | Bai et al. 201915 | OPHEC | 2001–2015 | lung and breast | incidence | PM2.5 (10.8b) | annual average | satellite | age, sex, education, income, histological subtype |
| 4 | Cheng et al. 201953 | CA MEC | 1993–2010 | breast | mortality | PM2.5c; PM10c | annual average | fix monitor | age, sex, smoking status, education, income, BMI, histological subtype |
| 5 | DuPre et al. 201952 | NHS and NHS-II | 1988–2014 | breast | mortality | PM2.5 (13.3, 3.5 [NHS], 12.9, 3.1 [NHS-II]); PM10 (22.2, 6.9 [NIS], 21.3, 6.2 [NHS-II]) | 2-y moving average | fix monitor | age, sex, smoking status, BMI, histological subtype |
| 6 | Pope et al. 201923 | National Health Interview Survey | 1986–2015 | lung | mortality | PM2.5 (10.7, 2.4) | 1986–2015 average | fix monitor | age, sex, smoking status, education, income, BMI |
| 7 | White et al. 201945 | Sister Study | 2003–2016 | breast | incidence | PM2.5c; PM10c | Age, sex, smoking status, education, income, histological subtype | ||
| 8 | Yorifuji et al. 201938 | Basic health checkups in Okayama | 2006–2016 | lung | mortality | PM2.5 (14, 1) | 2006–2010 average | satellite | age, sex, smoking status, occupation, histological subtype |
| 9 | Andersen et al. 201858 | ESCAPE | 1985–2008 | brain | incidence | PM2.5c; PM10c | annual average | fix monitor | age, sex, smoking status, education, income, histological subtype |
| 10 | Cakmak et al. 201824 | CANCHEC | 1991–2011 | lung | mortality | PM2.5c | 7-y moving average | satellite | age, sex, education, income, occupation |
| 11 | Datzmann et al. 201849 | Saxony Semi-individual Cohort Study | 2007–2014 | cancer specific | incidence | PM10 (20.9, 15.47–26.3e) | 2007 concentration | LUR model | age, sex |
| 12 | Gandini et al. 201820 | LIFE MED HISS | 1999–2008 | cancer specific | incidence | PM2.5c | annual average | fix monitor | age, sex, smoking status, education, income, BMI, occupation |
| 13 | Nagel et al. 201857 | ESCAPE | 1985–2005 | stomach and upper aerodigestive tract cancer | incidence | PM2.5c; PM10c | annual average | fix monitor | age, sex, smoking status, education, income, occupation, histological subtype |
| 14 | Pedersen et al. 201856 | ESCAPE | 1985–2005 | bladder | incidence | PM2.5c; PM10c | annual average | fix monitor | age, sex, smoking status, education, income, occupation |
| 15 | Villeneuve et al. 201846 | CNBSS | 1980–2005 | breast | incidence | PM2.5 (9.50d,6.40–12.40e) | annual average | satellite | age, sex, smoking status, education, BMI, occupation |
| 16 | Andersen et al. 201750 | Danish Nurse Cohort | 1993–2013 | breast | incidence | PM2.5 (19.7, 3.5); PM10 (23.5, 3.9) | 3-y moving average | fix monitor | age, sex, smoking status, BMI |
| 17 | Gharibvand et al. 201716 | AHS-II | 2002–2011 | lung | incidence | PM2.5 (12.9, 3.7 [noncases]; 13.1, 4.0 [cases]) | annual average | fix monitor | Sex, smoking status, education |
| 18 | Gharibvand et al. 2017a17 | AHS-II | 2002–2011 | lung | incidence | PM2.5 (12.9, 3.7 [noncases]; 13.1, 4.0 [cases]) | annual average | fix monitor | Sex, smoking status, education |
| 19 | Pedersen et al. 201759 | ESCAPE | 1985–2012 | liver | incidence | PM2.5c | annual average | fix monitor | age, sex, smoking status, education, income, occupation, histological subtype |
| 20 | Pun et al. 201725 | Medicare beneficiaries | 2000–2008 | lung | mortality | PM2.5 (12.5d, 10.3–14.3e) | 12- to 60-mo moving average | fix monitor | Smoking status, education, income, BMI |
| 21 | Turner et al. 201754 | CPS-II | 1982–2004 | cancer specific | mortality | PM2.5 (12.6, 2.8) | 1999–2004 average | fix monitor | age, sex, smoking status, education, income, BMI, occupation |
| 22 | Yin et al. 201739 | Chinese men cohort | 1990–2005 | lung | mortality | PM2.5 (43.7, 4.2–83.8e) | 2000–2005 average | satellite | age, sex, smoking status, education, BMI, occupation |
| 23 | Chen et al. 201641 | Northern China Cohort | 1998–2009 | lung | mortality | PM10 (144.34, 3.63) | 1998–2009 time dependent | fix monitor | age, sex, smoking status, education, income, BMI, occupation |
| 24 | Hart et al. 201647 | NHS-II | 1993–2011 | breast | incidence | PM2.5c; PM10c | 48-mo moving average | fix monitor | age, sex, smoking status, income, BMI, histological subtype |
| 25 | Jorgensen et al. 201660 | Danish Nurse Cohort | 1993–2013 | brain | incidence | PM2.5 (19.7, 3.5); PM10 (23.6, 3.9) | 3-y moving average | AirGIS | age |
| 26 | Raaschou et al. 201661 | ESCAPE | 1994–2013 | kidney | incidence | PM2.5c; PM10c | annual average | fix monitor | age, sex, smoking status, education, income, occupation |
| 27 | Tomczak et al. 201618 | CNBSS | 1980–2004 | lung | incidence | PM2.5 (9.5, 3.44) | 1998–2006 average | satellite | age, sex, smoking status, education, income, BMI, occupation, histological subtype |
| 28 | Wong et al. 201640 | Hong Kong Elderly Health services | 1998–2011 | cancer specific | mortality | PM2.5 (33.7, 3.2) | 1998–2001 average | fix monitor | age, sex, smoking status, education, income, BMI |
| 29 | Fischer et al. 201533 | DUELS | 2004–2011 | lung | mortality | PM10c | 2001 concentration | fix monitor | age, sex, BMI |
| 30 | Hart et al. 201521 | Netherlands Cohort Study | 1986–2003 | lung | incidence | PM2.5 (18.2, 10) | 1987–1996 average | fix monitor | age, sex, smoking status, education, income, BMI, occupation |
| 31 | To et al. 201548 | CNBSS | 1980–2013 | breast | incidence | PM2.5 (12.5, 2.4) | 1998–2006 average | satellite | age, sex, smoking status, education, income, BMI, occupation |
| 32 | Turner et al. 201526 | CPS-II | 1984–2004 | lung | mortality | PM2.5 (12.6, 2.9) | 1999–2004 average | fix monitor | age, sex, smoking status, education, income, BMI, occupation |
| 33 | Puett et al. 201444 | Nurses' Health Study | 1994–2010 | lung | incidence | PM2.5 (13.1, 3); PM10 (21.6, 6) | 72-mo cumulative average | fix monitor | age, sex, smoking status, education, income, BMI |
| 34 | Carey et al. 201336 | Clinical Practice Research Datalink | 2003–2007 | lung | mortality | PM2.5 (12.9, 1.4); PM10 (19.7, 2.3) | 2002 concentration | fix monitor | age, sex, smoking status, education, BMI |
| 35 | Cesaroni et al. 201335 | Rome Longitudinal Study | 2001–2010 | lung | mortality | PM2.5 (23, 4.4) | 1996–2001 | FARM | Sex, education, income, occupation |
| 36 | Heinrich et al. 201334 | North Rhine-Westphalia cohort | 1980s–2008 | lung | mortality | PM10 (43.7, 34.8–52.5e) | baseline year concentration | transformed from monitoring TSP | smoking status, income, occupation |
| 37 | Raaschou et al. 201322 | ESCAPE | 1990s | lung | incidence | PM2.5 (21.3, 2.7); PM10 (21.3, 2.7) | annual average | fix monitor | age, sex, smoking status, education |
| 38 | Hales et al. 201243 | New Zealand Census-Mortality Study | 1996–1999 | lung | mortality | PM10 (8.3, 8.4) | annual average | fix monitor | age, sex, smoking status, education, income |
| 39 | Lepeule et al. 201227 | Harvard Six Cities Study | 1974–2009 | lung | mortality | PM2.5 (15.9b) | 3-y moving average | fix monitor | age, sex, smoking status, BMI |
| 40 | Hart et al. 201129 | Trucking company | 1985–2000 | lung | mortality | PM2.5 (14.1, 4); PM10 (26.8, 6) | 1985–2000 average | fix monitor | age, sex, occupation |
| 41 | Katanoda et al. 201142 | Three-prefecture Cohort Study | 1995–2005 | lung | mortality | PM2.5 (10.8b) | 10-y average concentrations (1974–1983) before the baseline survey | fix monitor | age, sex, smoking status |
| 42 | Lipsett et al. 201130 | California Teachers Study | 1999–2005 | lung | mortality | PM2.5 (15.6, 4.5); PM10 (29.2, 9.7) | annual average | fix monitor | age, sex, smoking status, education, income, BMI, occupation, |
| 43 | Turner et al. 2011a28 | CPS-II | 1982–2008 | lung | mortality | PM2.5 (17.6,3.7) | 1979–1983 and 1999–2000 average | fix monitor | age, sex, smoking status, BMI, occupation |
| 44 | Brunekreef et al. 200937 | NLCS-AIR Study | 1986–1996 | lung | mortality | PM2.5 (28, 2.1) | 1987–1996 average | fix monitor | age, sex, smoking status, income |
| 45 | Pope et al. 200231 | CPS-II | 1982–1998 | lung | mortality | PM10 (28.8, 5.9) | 1979–1983 and 1999–2000 average | fix monitor | age, sex, smoking status, education, occupation |
| 46 | Abbey et al. 199932 | AHS | 1973–1992 | lung | mortality | PM10 (51.24, 16.63) | 3-y moving average | fix monitor | age, sex, smoking status, education |
| 47 | Beeson et al. 199819 | AHSMOG Study | 1973–1992 | lung | incidence | PM10 (51, 16.52) | 3-y moving average | fix monitor | age, sex, smoking status |
AHS, Adventist Health Study; AHSMOG, Adventist Health Study on Smog; CA MEC, California Multiethnic Cohort; CANCHEC, Canadian Census Health and Environment Cohort; CNBSS, Canadian National Breast Screening Study; CPS-II, Cancer Prevention Study-II; DUELS, Dutch Environmental Longitudinal Study; ESCAPE, European Study of Cohorts for Air Pollution Effects; FARM, flexible air quality regional mode; LUR, land use regression; NHS, Nurses' Health Study; NLCS-AIR, Netherlands Cohort Study-AIR; OPHEC, Ontario Population Health and Environment Cohort; TSP, total suspended PM.
Excluded in full analysis but included in subgroup analysis.
SD not available.
Mean concentration not available.
Median value.
Range.
PM and lung cancer
Because the case-fatality rate was high for lung cancer, mortality and incidence were comparable.62 Thus, it was reasonable to include both outcomes within the same meta-analysis.6 Thirty publications, including studies from the US, Europe, and Asia that covered total populations of 30.8 million and 10.6 million for PM2.5 and PM10, respectively, were included in the meta-analysis for lung cancer. Two publications16,17 from the Adventist Health and Smog (AHSMOG) Study-2 were included. One study17 that only reported adenocarcinoma of the lung was included in a subgroup analysis.
The overall pooled RRs of the change in lung cancer incidence or mortality per 10-μg/m3 increase in exposure to PM2.5 and PM10 were 1.16 (95% CI, 1.10–1.23) and 1.22 (95% CI, 1.02–1.45), respectively. The between-study variances for PM2.5 and PM10 were 81% and 96%, respectively (Figures 2 and 3, estimation by region see Figure S1). Funnel plots for both PM2.5 and PM10 were visually symmetrical. Trim and fill analyses were also conducted, showing no hypothetical negative studies were expected (Figure S2). In addition, the influence analyses showed that the overall findings remained stable after removing any specific studies (Table S10).
Figure 2.

Estimates of lung cancer risk associated with a 10-μg/m3 change in exposure to PM2.5 overall and by outcome
Figure 3.

Estimates of lung cancer risk associated with a 10-μg/m3 change in exposure to PM10 overall and by outcome
Figures 4 and 5 present subgroup analysis by region, sex, smoking status, and histological subtypes. There was no heterogeneity between different regions (p = 0.78). The estimated RR was highest among former smokers, then never smokers and current smokers for PM2.5 exposure. The difference did not reach statistical significance between groups (p = 0.68). Only limited studies reported the association between PM10 exposure and lung cancer by smoking status. Studies that took age, sex, smoking status, education, income, and occupation exposure into account were also conducted in the meta-analysis. The RR was stable with various confounder adjustments. Associations between PM2.5 and PM10 and risk for lung cancer by threshold are shown in Table S11. The RRs for studies reported the mean exposure concentration below the WHO air quality guideline threshold values of PM2.5 (10 μg/m3) and PM10 (20 μg/m3) were slightly higher than those above the threshold.
Figure 4.

Estimates of lung cancer risks associated with a 10-μg/m3 change in exposure to PM2.5 by region, sex, method of exposure assessment, histological subtypes, and confounding adjustment
Figure 5.

Estimates of lung cancer risks associated with a 10-μg/m3 change in exposure to PM10 by region, sex, method of exposure assessment, histological subtypes, and confounding adjustment
PM and breast cancer
Figures 6 and 7 show the studies included in the meta-analyses of PM and breast cancer incidence and mortality, from total populations of 3.52 million and 2.06 million included for PM2.5 and PM10, respectively. The pooled RRs for breast cancer incidence and mortality associated with PM2.5 were 1.03 (95% CI, 0.93–1.13) and 1.18 (95% CI, 0.81–1.73) per 10-μg/m3 increase. Apart from Hart et al., (2016),47 the other five studies all reported increased RR, but some were not statistically significant. For PM10, the pooled RRs for breast cancer incidence was 1.05 (95% CI, 0.93–1.19) per 10-μg/m3 increase (Figures 6 and 7, funnel plots see Figure S3). The number of studies included was insufficient to enable further subgroup analysis.
Figure 6.

Estimates of breast cancer risk associated with a 10-μg/m3 change in exposure to PM2.5
Figure 7.

Estimates of breast cancer risk associated with a 10-μg/m3 change in exposure to PM10
As breast cancer risk and prognosis vary by hormone receptor subtypes, subgroup analyses were conducted to examine possible different effects of PM exposure on hormone receptor (estrogen receptor [ER]+ progesterone receptor [PR]+ versus ER− PR−) breast cancer in some studies, but no statistically significant differences were found.45,47,53 There were also no differences between the risks of breast cancer for premenopausal or postmenopausal women.46,47 Higher PM2.5 was associated with higher stage I breast cancer mortality.52 Women who smoked or with a higher body mass index (BMI; i.e., ≥30 kg/m2) did not show a greater risk for breast cancer affected by PM2.5.48,51 No study reported male breast cancers.
PM and other cancers
Eleven studies reported other site-specific cancer risks associated with PM from North America (Public National Health Interview Survey51 and CPS-II54), Europe (ESCAPE study,56, 57, 58, 59,61 Danish Nurse Cohort Study,60 Saxony Semi-individual Cohort Study,49 and LIFE MED HISS [Mediterranean Health Interview Survey Studies]20), and Asia (Taiwan National Death Registry Study55). The LIFE MED HISS,20 CPS-II,54 and the National Health Interview Survey and mortality follow-up study in the US51 found a higher risk of bladder cancer due to PM2.5 exposure. However, there was no significant association between increased PM2.5 and risk of bladder cancer incidence in ESCAPE and also no association between PM10 and bladder cancer mortality in a Spanish study.56,63 Details for other cancers are presented in Figure 8.
Figure 8.

Estimates of other types of cancer risk associated with a 10-μg/m3 change in exposure to PM2.5 or PM10
When restricted to the never smokers, PM2.5 mortality associations observed for cancers of stomach, liver, pancreas, cervix, and Hodgkin lymphoma were still significant.51 The American CPS-II study reported statistically significant PM2.5 associations with colorectal, kidney, and bladder cancer mortality, while the associations of PM2.5 with kidney and bladder cancer appeared to be limited to men. Gastrointestinal and liver cancer mortality were reported to be associated with PM2.5 exposure in Taiwan, but not stomach cancer. The association between PM and cancer-specific risks other than lung or breast were still unclear as the findings from various cohorts were inconsistent.
Discussion
We conducted a systematic review and meta-analysis of the association between PM exposure and cancer incidence and mortality worldwide. This is the first up-to-date systematic review reporting the effect of PM exposure on all cancers comprehensively focusing on cohort studies, to our knowledge. This evidence supports regulatory authorities addressing community exposures to reduce the PM-related cancer risk.
Strong evidence suggests that cigarette smoke contributes to the development of various types of cancer, especially lung cancer.64 The National Health Interview Survey study showed different PM2.5-mortality associations with specific cancer types between the full cohort and non-smokers.51 Seven studies reported the risk of PM2.5 exposure on lung cancer in never smokers and current smokers, while six studies reported the risk in former smokers. The meta-analysis of these studies revealed higher PM2.5-related lung cancer risk among former and never smokers than current smokers, although the findings were imprecise. The risk of outdoor PM2.5 in current smokers might be obscured by the effect of smoking and an additive effect was shown among never and former smokers. Another reason might be that many of the subjects had stopped smoking prior to diagnosis, as a result of medical advice for other diseases. Limited studies reported RR with other cancers to show robust evidence.
For lung cancer, the present findings provide more strength to the evidence than was found in previous reviews. Overall, our meta-analysis suggested that long-term exposure to PM was associated with increased risk of lung cancer, and the positive association remained when analyses were adjusted for confounders like age, sex, and smoking status. However, household air pollution, which is the key risk factor for lung cancer, was not adjusted in all studies since the data were unavailable. No difference in risk between geographical regions was found, nor between males and females, which was consistent with previous studies, thus it was reasonable to pool the data from all regions.6,65 There was no significant heterogeneity between different regions, but we should be cautious when using the worldwide estimates because of heterogeneity between studies.
The pooled RRs for studies using fixed monitors were slightly higher than those using other data sources. Between-group differences were not significant for either PM2.5 or PM10, similar to the previous meta-analysis.6 Considering the access to air pollution data, some cohort studies used the annual concentration at baseline instead of long-term exposure, while some others used the average concentration during the study period. There were limited studies using moving average concentrations to estimate the long-term PM exposure effect on lung cancer risk. Furthermore, only a third of the studies considered a time-varying effect of PM exposure in analysis, which may have led to miscalculation.
The ESCAPE study reported that only lung adenocarcinoma risk was associated with PM exposure.22 Most studies reported total lung cancer risk affected by PM, while very few reported the results for lung cancer histological subtypes. Studies have shown a changing trend of different histological types of lung cancer. An increasing incidence of adenocarcinoma and a decreasing trend of squamous cell carcinoma incidence has been found in some countries, like China.66 Therefore, cohort studies for total lung cancer cases cannot accurately reflect the role of PM on different histological types. The impact of PM on different histological subtypes of lung cancer requires further study. An ecological study published recently also showed PM2.5 was associated with an increased risk of death from diseases such as cardiovascular and respiratory disease, even at low levels.67 Two studies36,43 included in our review reported average PM concentrations lower than the WHO air quality guideline threshold values for PM2.5 (10 μg/m3) and PM10 (20 μg/m3).68 The Effects of Low-level Air Pollution: A Study in Europe (ELAPSE), a large pooled cohort analysis, also suggested a linear to supra-linear shape of the PM2.5 concentration-response function with no evidence of a threshold.69
For breast cancer, we did not find a statistically significant effect of PM exposure. The studies were too limited in number to analyze subgroups. Breast cancer is a disease with a higher survival rate compared with many malignant cancers, and the incidence and mortality rates vary greatly between different stages, subtypes, ages, and ethnicities.62,70 As the 5-year survival rate is over 95% in patients diagnosed with stage I breast cancer, but about 30% in stage IV patients,70 it would not be reasonable to pool all stages together to examine the association of PM exposure and breast cancer death without adjustment for treatment. When a stratified analysis was conducted of stage I breast cancer patients, PM2.5 was associated with higher breast cancer-specific mortality.52 A potential explanation for differences among studies may be that this finding is due to differences in the proportions of cancer stages.
Hormone receptor status is a key factor in breast cancer diagnosis and treatment. A potential mechanism of how PM could increase breast cancer risk is that estrogenic particles might move from the lung to breast tissue.71 Only three articles reported the risks of PM on breast cancer stratified by hormone receptor status, but no significant differences were found between the risks for ER+ PR+ and ER− PR− breast cancers. The duration of hormone exposure is also important in breast cancer development. Two studies that were included reported the risks by menopausal status with no significant differences. Because of the rapid breast development and susceptibility of rapidly duplicating cells to environmental insults, puberty could be a critical period during which to assess the impact of exposures to PM2.5 on the breast.72,73 Limited studies focused on early lifetime PM exposure to breast cancer risk. A sister study suggested that exposure to vehicular traffic-related air pollution during childhood may be associated with increased breast cancer.74 After reviewing all these studies, there are still some research gaps to confirm whether PM exposure is a risk factor for breast cancer or not. More studies should be conducted to identify high-risk groups for PM.
Ambient air pollution was not significantly associated with incidence or death from most other cancers in the studies included. However, cancers of oral cavity, stomach, bladder, kidney, prostate, liver, colorectum, and lymphoid tissues have been inconsistently associated with PM. PM-related bladder cancer risk was observed in several ecological studies. A study from Taiwan suggested an adverse effect of PM2.5 on mortality,75 which was in line with the study from the US.76 The study using the Surveillance, Epidemiology, and End Results (SEER) program data in the US showed negative findings,77 taking bladder cancer incidence as the outcome. Wang et al. showed the significant adverse effect of PM2.5 on bladder cancer incidence, but a null effect on mortality in China.78 Other studies reporting PM10-related studies were also inconsistent with the cohort study included. Both a case-control study from Taiwan and an ecological study from Germany showed the risk of bladder cancer associated with increasing PM10 concentrations.79,80 The inconsistent results, encompassing both incidence and mortality, could be due to the limited number of studies that were conducted in different regions with concentrations of exposure.
The inconsistent results apply not only in bladder cancer studies. Kidney cancer is another example, and inconsistent conclusions were shown within similar populations. Two cohort studies from Europe gave different conclusions on PM2.5 and kidney cancer incidence, while studies from the US also showed different results for PM2.5 and mortality from kidney cancer. In ESCAPE, only vanadium in PM2.5 was found to be associated with kidney cancer,81 which revealed particles from mixed oil burning and industry that might be carcinogenic to the kidney. As PM is a complex mixture of chemical composition related to the sources, more studies focusing on sources should be conducted to clarify these inconsistent results.
This is the first systematic review and meta-analysis summarizing the association between PM and cancer risk comprehensively with searching across six databases. Focusing on cohort studies should also give more robust evidence. However, there are still some limitations to our review. Firstly, high heterogeneity existed due to general differences in population demographics, exposure assessment methods, and the covariate adjustments in different studies. Secondly, large-scale studies of PM and lung cancer risk have not yet been published from some of the most polluted countries, such as India. Thus, the associations were not completely representative of the global population. Thirdly, although 30 articles were included for the lung cancer analysis, they were still insufficient to demonstrate a dose-response relationship by conducting meta-regression and also some subgroup analyses. Finally, the definitions of smoking status varied among studies, which may lead to misclassification.
Conclusion
Our systematic review has summarized cohort studies that aimed to find the association between ambient PM and cancer risk. Current studies provide evidence of an adverse effect of outdoor PM exposure on lung cancer. Further studies of air pollution and breast, bladder, and kidney cancer should be conducted as these research gaps still exist and need to be filled. However, regulatory authorities need to reduce community exposures to PM as much as feasible.
Acknowledgments
P.Y., R.X., and T.Y. were supported by China Scholarship Council funds (number 201906210065 for P.Y., 201806010405 for R.X., and 201906320051 for T.Y.); S.L. by an Early Career Fellowship of the Australian National Health and Medical Research Council (number APP1109193); and Y.G. by Career Development Fellowships of the Australian National Health and Medical Research Council (numbers APP1107107 and APP1163693).
Author contributions
P.Y., Y.G., M.A., and S.L. designed the review. P.Y., S.G., and R.X. ran the literature search, screened records, and extracted data. P.Y., T.Y., and R.X. did statistical analyses. P.Y. and S.G. wrote the manuscript. Y.G., M.A., and S.L. provided scientific comments on the manuscript. All authors provided critical conceptual input, analyzed and interpreted data, and critically revised the report.
Declaration of interests
M.J.A. holds investigator-initiated grants from Pfizer and Boehringer-Ingelheim for unrelated research. He has undertaken an unrelated consultancy for and received assistance with conference attendance from Sanofi. He has also received a speaker's fee from GSK. All other authors declare no competing interests.
Published Online: July 13, 2021
Footnotes
Supplemental information can be found online at https://doi.org/10.1016/j.xinn.2021.100143.
Lead contact website
Supplemental information
References
- 1.IARC (International Agency for Research on Cancer) Cancer fact sheet. https://gco.iarc.fr/today/data/factsheets/cancers/39-All-cancers-fact-sheet.pdf
- 2.Yang Y., Qi J., Ruan Z., et al. Changes in life expectancy of respiratory diseases from attaining daily PM2.5 standard in China: a nationwide observational study. Innovation. 2020;1:100064. doi: 10.1016/j.xinn.2020.100064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liang D., Shi L., Zhao J., et al. Urban air pollution may enhance COVID-19 case-fatality and mortality rates in the United States. Innovation. 2020;1:100047. doi: 10.1016/j.xinn.2020.100047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Valavanidis A., Vlachogianni T., Fiotakis K., et al. Pulmonary oxidative stress, inflammation and cancer: respirable particulate matter, fibrous dusts and ozone as major causes of lung carcinogenesis through reactive oxygen species mechanisms. Int. J. Environ. Res. Public Health. 2013;10:3886–3907. doi: 10.3390/ijerph10093886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schmid O., Moller W., Semmler-Behnke M., et al. Dosimetry and toxicology of inhaled ultrafine particles. Biomarkers. 2009;14:67–73. doi: 10.1080/13547500902965617. [DOI] [PubMed] [Google Scholar]
- 6.Hamra G.B., Guha N., Cohen A., et al. Outdoor particulate matter exposure and lung cancer: a systematic review and meta-analysis. Environ. Health Perspect. 2014;122:906–911. doi: 10.1289/ehp/1408092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zhang Z., Yan W., Chen Q., et al. The relationship between exposure to particulate matter and breast cancer incidence and mortality: a meta-analysis. Medicine. 2019;98:e18349. doi: 10.1097/MD.0000000000018349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim H.B., Shim J.Y., Park B., et al. Long-term exposure to air pollution and the risk of non-lung cancer: a meta-analysis of observational studies. Perspect. Public Health. 2019;140:222–231. doi: 10.1177/1757913919891751. [DOI] [PubMed] [Google Scholar]
- 9.Chen G., Wan X., Yang G., et al. Traffic-related air pollution and lung cancer: a meta-analysis. Thorac. Cancer. 2015;6:307–318. doi: 10.1111/1759-7714.12185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kim H.B., Shim J.Y., Park B., et al. Long-term exposure to air pollutants and cancer mortality: a meta-analysis of cohort studies. Int. J. Environ. Res. Public Health. 2018;15:2608. doi: 10.3390/ijerph15112608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liu Q., Xu C., Ji G., et al. Effect of exposure to ambient PM2.5 pollution on the risk of respiratory tract diseases: a meta-analysis of cohort studies. J. Biomed. Res. 2017;31:130–142. doi: 10.7555/JBR.31.20160071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Guyatt G.H., Oxman A.D., Vist G.E., et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Guyatt G., Oxman A.D., Akl E.A., et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011;64:383–394. doi: 10.1016/j.jclinepi.2010.04.026. [DOI] [PubMed] [Google Scholar]
- 14.DerSimonian R., Laird N. Meta-analysis in clinical trials. Control Clin. Trials. 1986;7:177–188. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 15.Bai L., Shin S., Burnett R.T., et al. Exposure to ambient air pollution and the incidence of lung cancer and breast cancer in the Ontario Population Health and Environment Cohort. Int. J. Cancer. 2019;146:2450–2459. doi: 10.1002/ijc.32575. [DOI] [PubMed] [Google Scholar]
- 16.Gharibvand L., Shavlik D., Ghamsary M., et al. The association between ambient fine particulate air pollution and lung cancer incidence: results from the AHSMOG-2 study. Environ. Health Perspect. 2017;125:378–384. doi: 10.1289/EHP124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gharibvand L., Beeson W., Shavlik D., et al. The association between ambient fine particulate matter and incident adenocarcinoma subtype of lung cancer. Environ. Health. 2017;16:71. doi: 10.1186/s12940-017-0268-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tomczak A., Miller A.B., Weichenthal S.A., et al. Long-term exposure to fine particulate matter air pollution and the risk of lung cancer among participants of the Canadian National Breast Screening Study. Int. J. Cancer. 2016;139:1958–1966. doi: 10.1002/ijc.30255. [DOI] [PubMed] [Google Scholar]
- 19.Beeson W.L., Abbey D.E., Knutsen S.F. Long-term concentrations of ambient air pollutants and incident lung cancer in California adults: results from the AHSMOG study. Environ. Health Perspect. 1998;106:813–822. doi: 10.1289/ehp.106-1533247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gandini M., Scarinzi C., Bande S., et al. Long term effect of air pollution on incident hospital admissions: results from the Italian Longitudinal Study within LIFE MED HISS project. Environ. Int. 2018;121:1087–1097. doi: 10.1016/j.envint.2018.10.020. [DOI] [PubMed] [Google Scholar]
- 21.Hart J.E., Spiegelman D., Beelen R., et al. Long-term ambient residential traffic-related exposures and measurement error-adjusted risk of incident lung cancer in The Netherlands cohort study on diet and cancer. Environ. Health Perspect. 2015;123:860–866. doi: 10.1289/ehp.1408762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Raaschou-Nielsen O., Andersen Z.J., Beelen R., et al. Air pollution and lung cancer incidence in 17 European cohorts: prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE) Lancet Oncol. 2013;14:813–822. doi: 10.1016/S1470-2045(13)70279-1. [DOI] [PubMed] [Google Scholar]
- 23.Pope C.A., III, Lefler J.S., Ezzati M., et al. Mortality risk and fine particulate air pollution in a large, representative cohort of U.S. adults. Environ. Health Perspect. 2019;127:1–9. doi: 10.1289/EHP4438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cakmak S., Hebbern C., Pinault L., et al. Associations between long-term PM2.5 and ozone exposure and mortality in the Canadian Census Health and Environment Cohort (CANCHEC), by spatial synoptic classification zone. Environ. Int. 2018;111:200–211. doi: 10.1016/j.envint.2017.11.030. [DOI] [PubMed] [Google Scholar]
- 25.Pun V.C., Kazemiparkouhi F., Manjourides J., et al. Long-term PM2.5 exposure and respiratory, cancer, and cardiovascular mortality in older US adults. Am. J. Epidemiol. 2017;186:961–969. doi: 10.1093/aje/kwx166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Turner M.C., Jerrett M., Pope C.A., III, et al. Long-term ozone exposure and mortality in a large prospective study. Am. J. Respir. Crit. Care Med. 2016;193:1134–1142. doi: 10.1164/rccm.201508-1633OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lepeule J., Laden F., Dockery D., et al. Chronic exposure to fine particles and mortality: an extended follow-up of the Harvard Six Cities Study from 1974 to 2009. Environ. Health Perspect. 2012;120:965–970. doi: 10.1289/ehp.1104660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Turner M.C., Krewski D., Pope C.A., III, et al. Long-term ambient fine particulate matter air pollution and lung cancer in a large cohort of never-smokers. Am. J. Respir. Crit. Care Med. 2011;184:1374–1381. doi: 10.1164/rccm.201106-1011OC. [DOI] [PubMed] [Google Scholar]
- 29.Hart J.E., Garshick E., Dockery D.W., et al. Long-term ambient multipollutant exposures and mortality. Am. J. Respir. Crit. Care Med. 2011;183:73–78. doi: 10.1164/rccm.200912-1903OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lipsett M.J., Ostro B.D., Reynolds P., et al. Long-term exposure to air pollution and cardiorespiratory disease in the California teachers study cohort. Am. J. Respir. Crit. Care Med. 2011;184:828–835. doi: 10.1164/rccm.201012-2082OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Pope C.A., III, Burnett R.T., Thun M.J., et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA. 2002;287:1132–1141. doi: 10.1001/jama.287.9.1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Abbey D.E., Nishino N., McDonnell W.F., et al. Long-term inhalable particles and other air pollutants related to mortality in nonsmokers. Am. J. Respir. Crit. Care Med. 1999;159:373–382. doi: 10.1164/ajrccm.159.2.9806020. [DOI] [PubMed] [Google Scholar]
- 33.Fischer P.H., Marra M., Ameling C.B., et al. Air pollution and mortality in seven million adults: the Dutch Environmental Longitudinal Study (DUELS) Environ. Health Perspect. 2015;123:697–704. doi: 10.1289/ehp.1408254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Heinrich J., Thiering E., Rzehak P., et al. Long-term exposure to NO2 and PM10 and all-cause and cause-specific mortality in a prospective cohort of women. Occup. Environ. Med. 2013;70:179–186. doi: 10.1136/oemed-2012-100876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cesaroni G., Badaloni C., Gariazzo C., et al. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ. Health Perspect. 2013;121:324–331. doi: 10.1289/ehp.1205862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Carey I.M., Atkinson R.W., Kent A.J., et al. Mortality associations with long-term exposure to outdoor air pollution in a national English cohort. Am. J. Respir. Crit. Care Med. 2013;187:1226–1233. doi: 10.1164/rccm.201210-1758OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Brunekreef B., Beelen R., Hoek G., et al. Effects of long-term exposure to traffic-related air pollution on respiratory and cardiovascular mortality in The Netherlands: the NLCS-AIR study. Res. Rep. Health Eff. Inst. 2009:5–71. [discussion: 73–89] [PubMed] [Google Scholar]
- 38.Yorifuji T., Kashima S., Tani Y., et al. Long-term exposure to fine particulate matter and natural-cause and cause-specific mortality in Japan. Environ. Epidemiol. 2019;3:e051. doi: 10.1097/EE9.0000000000000051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Yin P., Brauer M., Cohen A., et al. Long-term fine particulate matter exposure and nonaccidental and cause-specific mortality in a large national cohort of Chinese men. Environ. Health Perspect. 2017;125:117002. doi: 10.1289/EHP1673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Wong C.M., Tsang H., Lai H.K., et al. Cancer mortality risks from long-term exposure to ambient fine particle. Cancer Epidemiol. Biomarkers Prev. 2016;25:839–845. doi: 10.1158/1055-9965.EPI-15-0626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chen X., Zhang L.W., Huang J.J., et al. Long-term exposure to urban air pollution and lung cancer mortality: a 12-year cohort study in northern China. Sci. Total Environ. 2016;571:855–861. doi: 10.1016/j.scitotenv.2016.07.064. [DOI] [PubMed] [Google Scholar]
- 42.Katanoda K., Sobue T., Satoh H., et al. An association between long-term exposure to ambient air pollution and mortality from lung cancer and respiratory diseases in Japan. J. Epidemiol. 2011;21:132–143. doi: 10.2188/jea.JE20100098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hales S., Blakely T., Woodward A. Air pollution and mortality in New Zealand: cohort study. J. Epidemiol. Community Health. 2012;66:468–473. doi: 10.1136/jech.2010.112490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Puett R.C., Hart J.E., Yanosky J.D., et al. Particulate matter air pollution exposure, distance to road, and incident lung cancer in the nurses' health study cohort. Environ. Health Perspect. 2014;122:926–932. doi: 10.1289/ehp.1307490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.White A.J., Keller J.P., Zhao S., et al. Air pollution, clustering of particulate matter components, and breast cancer in the sister study: a U.S.-wide cohort. Environ. Health Perspect. 2019;127:107002. doi: 10.1289/EHP5131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Villeneuve P.J., Goldberg M.S., Crouse D.L., et al. Residential exposure to fine particulate matter air pollution and incident breast cancer in a cohort of Canadian women. Environ. Epidemiol. 2018;2:e021. [Google Scholar]
- 47.Hart J.E., Bertrand K.A., DuPre N., et al. Long-term particulate matter exposures during adulthood and risk of breast cancer incidence in the Nurses' Health Study II Prospective Cohort. Cancer Epidemiol. Biomarkers Prev. 2016;25:1274–1276. doi: 10.1158/1055-9965.EPI-16-0246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.To T., Zhu J., Villeneuve P.J., et al. Chronic disease prevalence in women and air pollution - a 30-year longitudinal cohort study. Environ. Int. 2015;80:26–32. doi: 10.1016/j.envint.2015.03.017. [DOI] [PubMed] [Google Scholar]
- 49.Datzmann T., Markevych I., Trautmann F., et al. Outdoor air pollution, green space, and cancer incidence in Saxony: a semi-individual cohort study. BMC Public Health. 2018;18:715. doi: 10.1186/s12889-018-5615-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Andersen Z.J., Ravnskjaer L., Andersen K.K., et al. Long-term exposure to fine particulate matter and breast cancer incidence in the Danish Nurse Cohort Study. Cancer Epidemiol. Biomarkers Prev. 2017;26:428–430. doi: 10.1158/1055-9965.EPI-16-0578. [DOI] [PubMed] [Google Scholar]
- 51.Coleman N.C., Burnett R.T., Higbee J.D., et al. Cancer mortality risk, fine particulate air pollution, and smoking in a large, representative cohort of US adults. Cancer Causes Control. 2020;31:767–776. doi: 10.1007/s10552-020-01317-w. [DOI] [PubMed] [Google Scholar]
- 52.DuPre N.C., Hart J.E., Holmes M.D., et al. Particulate matter and traffic-related exposures in relation to breast cancer survival. Cancer Epidemiol. Biomarkers Prev. 2019;28:751–759. doi: 10.1158/1055-9965.EPI-18-0803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cheng I., Tseng C., Wu J., et al. Association between ambient air pollution and breast cancer risk: the multiethnic cohort study. Int. J. Cancer. 2019;146:699–711. doi: 10.1002/ijc.32308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Turner M.C., Krewski D., Diver W.R., et al. Ambient air pollution and cancer mortality in the Cancer Prevention Study II. Environ. Health Perspect. 2017;125:087013. doi: 10.1289/EHP1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Guo C., Chan T.C., Teng Y.C., et al. Long-term exposure to ambient fine particles and gastrointestinal cancer mortality in Taiwan: a cohort study. Environ. Int. 2020;138:105640. doi: 10.1016/j.envint.2020.105640. [DOI] [PubMed] [Google Scholar]
- 56.Pedersen M., Stafoggia M., Weinmayr G., et al. Is there an association between ambient air pollution and bladder cancer incidence? Analysis of 15 European Cohorts. Eur. Urol. Focus. 2018;4:113–120. doi: 10.1016/j.euf.2016.11.008. [DOI] [PubMed] [Google Scholar]
- 57.Nagel G., Stafoggia M., Pedersen M., et al. Air pollution and incidence of cancers of the stomach and the upper aerodigestive tract in the European Study of Cohorts for Air Pollution Effects (ESCAPE) Int. J. Cancer. 2018;143:1632–1643. doi: 10.1002/ijc.31564. [DOI] [PubMed] [Google Scholar]
- 58.Andersen Z.J., Pedersen M., Weinmayr G., et al. Long-term exposure to ambient air pollution and incidence of brain tumor: the European Study of Cohorts for Air Pollution Effects (ESCAPE) Neuro Oncol. 2018;20:420–432. doi: 10.1093/neuonc/nox163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Pedersen M., Andersen Z.J., Stafoggia M., et al. Ambient air pollution and primary liver cancer incidence in four European cohorts within the ESCAPE project. Environ. Res. 2017;154:226–233. doi: 10.1016/j.envres.2017.01.006. [DOI] [PubMed] [Google Scholar]
- 60.Jorgensen J.T., Johansen M.S., Ravnskjaer L., et al. Long-term exposure to ambient air pollution and incidence of brain tumours: the Danish Nurse Cohort. Neurotoxicology. 2016;55:122–130. doi: 10.1016/j.neuro.2016.06.003. [DOI] [PubMed] [Google Scholar]
- 61.Raaschou-Nielsen O., Pedersen M., Stafoggia M., et al. Outdoor air pollution and risk for kidney parenchyma cancer in 14 European cohorts. Int. J. Cancer. 2017;140:1528–1537. doi: 10.1002/ijc.30587. [DOI] [PubMed] [Google Scholar]
- 62.DeSantis C.E., Lin C.C., Mariotto A.B., et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J. Clin. 2014;64:252–271. doi: 10.3322/caac.21235. [DOI] [PubMed] [Google Scholar]
- 63.Turner M.C., Gracia-Lavedan E., Cirac M., et al. Ambient air pollution and incident bladder cancer risk: updated analysis of the Spanish Bladder Cancer Study. Int. J. Cancer. 2019;145:894–900. doi: 10.1002/ijc.32136. [DOI] [PubMed] [Google Scholar]
- 64.Gandini S., Botteri E., Iodice S., et al. Tobacco smoking and cancer: a meta-analysis. Int. J. Cancer. 2008;122:155–164. doi: 10.1002/ijc.23033. [DOI] [PubMed] [Google Scholar]
- 65.Cui P., Huang Y., Han J., et al. Ambient particulate matter and lung cancer incidence and mortality: a meta-analysis of prospective studies. Eur. J. Public Health. 2015;25:324–329. doi: 10.1093/eurpub/cku145. [DOI] [PubMed] [Google Scholar]
- 66.Shi J.F., Wang L., Wu N., et al. Clinical characteristics and medical service utilization of lung cancer in China, 2005-2014: overall design and results from a multicenter retrospective epidemiologic survey. Lung Cancer. 2019;128:91–100. doi: 10.1016/j.lungcan.2018.11.031. [DOI] [PubMed] [Google Scholar]
- 67.Yu W., Guo Y., Shi L., et al. The association between long-term exposure to low-level PM2.5 and mortality in the state of Queensland, Australia: a modelling study with the difference-in-differences approach. PLoS Med. 2020;17:e1003141. doi: 10.1371/journal.pmed.1003141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.World Health Organization . World Health Organization; 2006. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. [PubMed] [Google Scholar]
- 69.Hvidtfeldt U.A., Severi G., Andersen Z.J., et al. Long-term low-level ambient air pollution exposure and risk of lung cancer - a pooled analysis of 7 European cohorts. Environ. Int. 2020;146:106249. doi: 10.1016/j.envint.2020.106249. [DOI] [PubMed] [Google Scholar]
- 70.DeSantis C.E., Ma J., Gaudet M.M., et al. Breast cancer statistics, 2019. CA Cancer J. Clin. 2019;69:438–451. doi: 10.3322/caac.21583. [DOI] [PubMed] [Google Scholar]
- 71.Sutton P., Kavanaugh-Lynch M.H., Plumb M., et al. California breast cancer prevention initiatives: setting a research agenda for prevention. Reprod. Toxicol. 2015;54:11–18. doi: 10.1016/j.reprotox.2014.09.008. [DOI] [PubMed] [Google Scholar]
- 72.Hiatt R.A., Haslam S.Z., Osuch J. The breast cancer and the environment research centers: transdisciplinary research on the role of the environment in breast cancer etiology. Environ. Health Perspect. 2009;117:1814–1822. doi: 10.1289/ehp.0800120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Berkey C.S., Frazier A.L., Gardner J.D., et al. Adolescence and breast carcinoma risk. Cancer. 1999;85:2400–2409. doi: 10.1002/(sici)1097-0142(19990601)85:11<2400::aid-cncr15>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
- 74.Shmuel S., White A.J., Sandler D.P. Residential exposure to vehicular traffic-related air pollution during childhood and breast cancer risk. Environ. Res. 2017;159:257–263. doi: 10.1016/j.envres.2017.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Yeh H.L., Hsu S.W., Chang Y.C., et al. Spatial analysis of ambient PM2.5 exposure and bladder cancer mortality in Taiwan. Int. J. Environ. Res. Public Health. 2017;14:508. doi: 10.3390/ijerph14050508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Smith N.D., Prasad S.M., Patel A.R., et al. Bladder cancer mortality in the United States: a geographic and temporal analysis of socioeconomic and environmental factors. J. Urol. 2016;195:290–296. doi: 10.1016/j.juro.2015.07.091. [DOI] [PubMed] [Google Scholar]
- 77.Coleman N.C., Burnett R.T., Ezzati M., et al. Fine particulate matter exposure and cancer incidence: analysis of SEER Cancer Registry Data from 1992-2016. Environ. Health Perspect. 2020;128:107004. doi: 10.1289/EHP7246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Wang H., Gao Z., Ren J., et al. An urban-rural and sex differences in cancer incidence and mortality and the relationship with PM2.5 exposure: an ecological study in the southeastern side of Hu line. Chemosphere. 2019;216:766–773. doi: 10.1016/j.chemosphere.2018.10.183. [DOI] [PubMed] [Google Scholar]
- 79.Liu C.C., Tsai S.S., Chiu H.F., et al. Ambient exposure to criteria air pollutants and risk of death from bladder cancer in Taiwan. Inhal. Toxicol. 2009;21:48–54. doi: 10.1080/08958370802207326. [DOI] [PubMed] [Google Scholar]
- 80.Radespiel-Troger M., Geiss K., Twardella D., et al. Cancer incidence in urban, rural, and densely populated districts close to core cities in Bavaria, Germany. Int. Arch. Occup. Environ. Health. 2018;91:155–174. doi: 10.1007/s00420-017-1266-3. [DOI] [PubMed] [Google Scholar]
- 81.de Hoogh K., Wang M., Adam M., et al. Development of land use regression models for particle composition in twenty study areas in Europe. Environ. Sci. Technol. 2013;47:5778–5786. doi: 10.1021/es400156t. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.