

Abstract
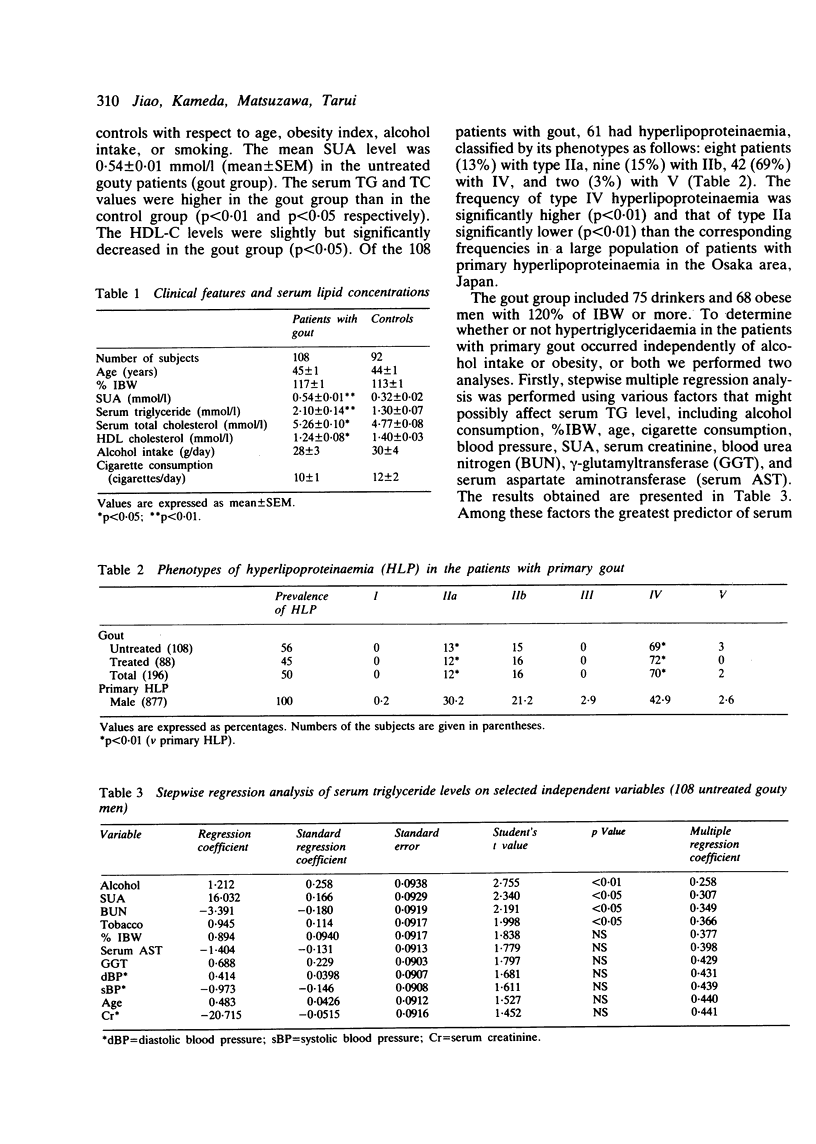
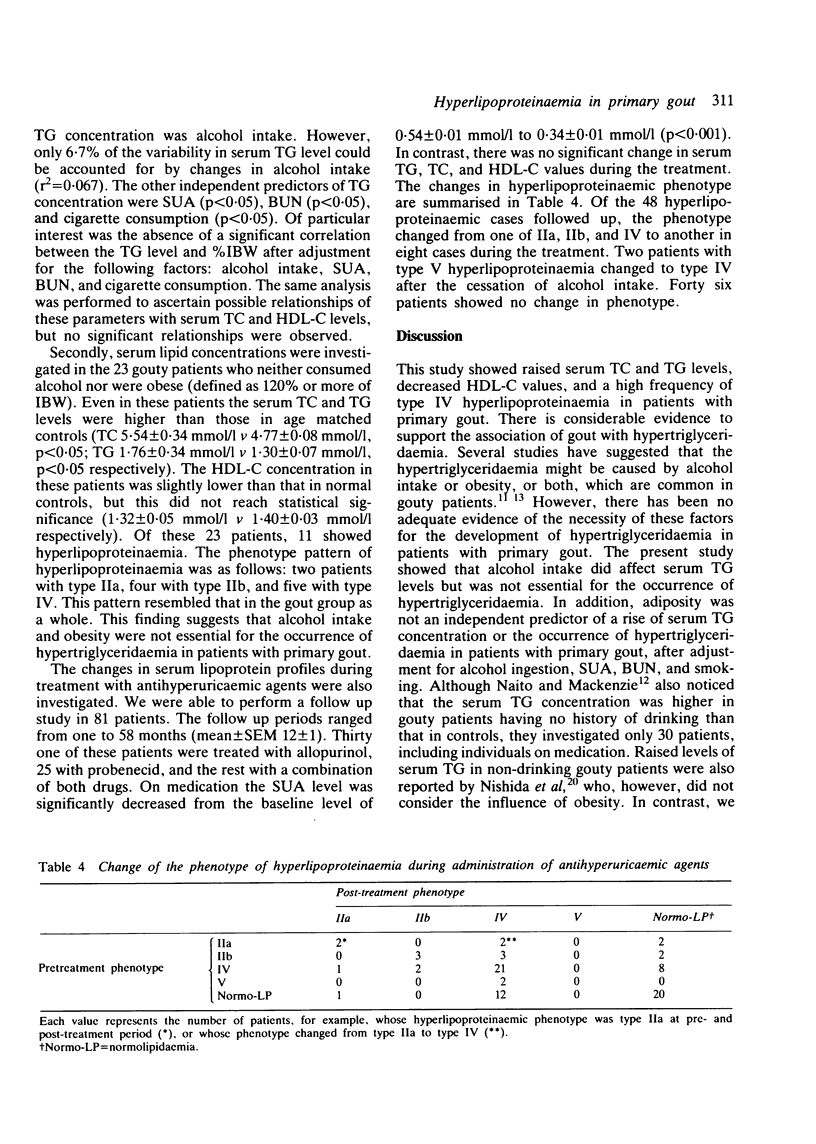
Serum lipoprotein profiles were investigated in 108 male patients with primary gout before treatment to elucidate the prevalence of each individual phenotype of coexisting hyperlipoproteinaemia and pathogenic factors responsible for it. The mean serum triglyceride (TG) and total cholesterol (TC) levels in the patients with gout were 2.10 +/- 0.14 mmol/l and 5.26 +/- 0.10 mmol/l (mean +/- SEM) respectively, which were significantly higher (p less than 0.01 and p less than 0.05 respectively) than the levels in age matched controls without gout (1.30 +/- 0.07 mmol/l and 4.77 +/- 0.08 mmol/l respectively). Serum high density lipoprotein cholesterol (HDL-C) values were slightly decreased in patients with gout compared with controls (1.24 +/- 0.08 mmol/l v 1.40 +/- 0.03 mmol/l, p less than 0.05). Hyperlipoproteinaemia was seen in 61 patients (56%), of whom patients with type IIa, IIb, and IV hyperlipoproteinaemia formed 13, 15, and 69% respectively. Thus the prevalence of type IV hyperlipoproteinaemia was high in primary gout as compared with primary hyperlipoproteinaemia with primary hyperlipoproteinaemia (69% v 43%, p less than 0.01). The independent and relative influences of clinical data of the patients upon the concentrations of serum lipids were assessed by stepwise multiple regression analysis. Two major predictors of serum TG level were alcohol intake (p less than 0.01) and serum uric acid level (p less than 0.05). The most significant predictive variable was alcohol intake, but its influence was judged to be small (r2 = 0.067). None of the other variables, including obesity index, had any significant influence. The relationships between any of these variables and serum TC or HDL-C levels were not significant. In addition, serum lipid levels were investigated in patients with neither obesity (defined as 120% or more of ideal body weight) nor a history of alcohol intake. Their serum TG and TC concentrations were also significantly higher than the respective control levels. Thus hyperlipoproteinaemia in primary gout its unlikely to be secondary to excess alcohol intake or obesity, or both. Instead, it may result from genetic factors such as a combined hyperlipidaemic trait.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beard J. T., 2nd Serum uric acid and coronary heart disease. Am Heart J. 1983 Aug;106(2):397–400. doi: 10.1016/0002-8703(83)90209-0. [DOI] [PubMed] [Google Scholar]
- Beaumont J. L., Carlson L. A., Cooper G. R., Fejfar Z., Fredrickson D. S., Strasser T. Classification of hyperlipidaemias and hyperlipoproteinaemias. Bull World Health Organ. 1970;43(6):891–915. [PMC free article] [PubMed] [Google Scholar]
- Darlington L. G., Scott J. T. Plasma lipid levels in gout. Ann Rheum Dis. 1972 Nov;31(6):487–489. doi: 10.1136/ard.31.6.487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fessel W. J. High uric acid as an indicator of cardiovascular disease. Independence from obesity. Am J Med. 1980 Mar;68(3):401–404. doi: 10.1016/0002-9343(80)90111-4. [DOI] [PubMed] [Google Scholar]
- Gibson T., Grahame R. Gout and hyperlipidaemia. Ann Rheum Dis. 1974 Jul;33(4):298–303. doi: 10.1136/ard.33.4.298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson T., Kilbourn K., Horner I., Simmonds H. A. Mechanism and treatment of hypertriglyceridaemia in gout. Ann Rheum Dis. 1979 Feb;38(1):31–35. doi: 10.1136/ard.38.1.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldstein J. L., Schrott H. G., Hazzard W. R., Bierman E. L., Motulsky A. G. Hyperlipidemia in coronary heart disease. II. Genetic analysis of lipid levels in 176 families and delineation of a new inherited disorder, combined hyperlipidemia. J Clin Invest. 1973 Jul;52(7):1544–1568. doi: 10.1172/JCI107332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grahame R., Scott J. T. Clinical survey of 354 patients with gout. Ann Rheum Dis. 1970 Sep;29(5):461–468. doi: 10.1136/ard.29.5.461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halpern M. J., Pereira Miguel M. S. Uric acid and coronary heart disease. J Am Geriatr Soc. 1974 Feb;22(2):86–87. doi: 10.1111/j.1532-5415.1974.tb06275.x. [DOI] [PubMed] [Google Scholar]
- Jacobs D. Hyperuricemia as a risk factor in coronary heart disease. Adv Exp Med Biol. 1977;76B:231–237. doi: 10.1007/978-1-4684-3285-5_33. [DOI] [PubMed] [Google Scholar]
- KOHN P. M., PROZAN G. B. Hyperuricemia; relationship to hypercholesteremia and acute myocardial infarction. J Am Med Assoc. 1959 Aug 15;170(16):1909–1912. doi: 10.1001/jama.1959.03010160025007. [DOI] [PubMed] [Google Scholar]
- Kodama T., Murase T., Itakura H., Akanuma Y., Takaku F., Nishida Y. Postheparin plasma lipoprotein lipase and hepatic triglyceride lipase activities in patients with primary asymptomatic gout. Clin Chem. 1983 Dec;29(12):2124–2125. [PubMed] [Google Scholar]
- NARAYAN K. A., NARAYAN S., KUMMEROW F. A. DISK ELECTROPHORESIS OF HUMAN SERUM LIPOPROTEINS. Nature. 1965 Jan 16;205:246–248. doi: 10.1038/205246a0. [DOI] [PubMed] [Google Scholar]
- Naito H. K., Mackenzie A. H. Secondary hypertriglyceridemia and hyperlipoproteinemia in patients with primary asymptomatic gout. Clin Chem. 1979 Mar;25(3):371–375. [PubMed] [Google Scholar]
- Nishida Y., Akaoka I., Nishizawa T., Yoshimura T. Hyperlipidaemia in gout. Clin Chim Acta. 1975 Jul 9;62(1):103–106. doi: 10.1016/0009-8981(75)90285-5. [DOI] [PubMed] [Google Scholar]
- Tiffany T. O., Morton J. M., Hall E. M., Garrett A. S., Jr Clinical evaluation of kinetic enzymatic fixed-time and integral analysis of serum triglycerides. Clin Chem. 1974 Apr;20(4):476–481. [PubMed] [Google Scholar]
- Wiedemann E., Rose H. G., Schwartz E. Plasma lipoproteins, glucose tolerance and insulin response in primary gout. Am J Med. 1972 Sep;53(3):299–307. doi: 10.1016/0002-9343(72)90172-6. [DOI] [PubMed] [Google Scholar]
- Yano K., Rhoads G., Kagan A. Epidemiology of serum uric acid among 8000 Japanese-American men in Hawaii. J Chronic Dis. 1977 Mar;30(3):171–184. doi: 10.1016/0021-9681(77)90083-2. [DOI] [PubMed] [Google Scholar]