

Abstract
The increasing prevalence of autism spectrum disorders (ASD) has led to worldwide interest in factors influencing the age of ASD diagnosis. Parents or caregivers of 237 ASD children (193 boys, 44 girls) diagnosed using the Autism Diagnostic Observation Schedule (ADOS) completed a simple descriptive questionnaire. The data were analyzed using the variable-centered multiple regression analysis and the person-centered classification tree method. We believed that the concurrent use of these two methods could produce robust results. The mean age at diagnosis was 5.8 ± 2.2 years (median 5.3 years). Younger ages for ASD diagnosis were predicted (using multiple regression analysis) by higher scores in the ADOS social domain, higher scores in ADOS restrictive and repetitive behaviors and interest domain, higher maternal education, and the shared household of parents. Using the classification tree method, the subgroup with the lowest mean age at diagnosis were children, in whom the summation of ADOS communication and social domain scores was ≥ 17, and paternal age at the delivery was ≥ 29 years. In contrast, the subgroup with the oldest mean age at diagnosis included children with summed ADOS communication and social domain scores < 17 and maternal education at the elementary school level. The severity of autism and maternal education played a significant role in both types of data analysis focused on age at diagnosis.
Keywords: Autism spectrum disorders, Age at diagnosis, Shared household, ADOS, Paternal age, Maternal education
Introduction
Autism spectrum disorders (ASD), according to The International Classification of Diseases, 10th Edition (ICD-10) [1], are neurodevelopmental conditions presenting with a range of symptoms, including impairment of communication, difficulties with social interaction, and atypical and limited patterns of behavior [2, 3].
The ASD umbrella includes autistic disorder, Asperger syndrome, pervasive developmental disorders not otherwise specified, and childhood disintegrative disorder [4]. Not only do these disorders have a significant effect on the quality of life, but they also have a considerable socioeconomic impact. The estimated global burden calculated as disability-adjusted life-years (DALY), which is an aggregation of years of life lost because of premature mortality and years lived with a disability, was 58 DALYs per 100,000 population for the autistic disorders and 53 DALYs per 100,000 for other ASDs [5].
The economic impact includes, among others, direct healthcare and special education costs and lost productivity for adults with ASD and their families/caregivers. Estimates of overall lifetime costs for individuals with ASD are in the millions of dollars, varying regionally [6].
In recent decades, we have seen a considerable increase in the reported prevalence of ASD, with recent estimates falling between 1 and 1.7%, according to studies conducted in the USA [7] and the UK [8]. No studies have specifically looked at the prevalence of autism in the Czech Republic; however, a comprehensive review of over 600 epidemiological studies worldwide (including also studies written in local languages like Arabic, Chinese, Dutch, French, etc.) did not identify regional differences in ASD prevalence, nor did it find that ethnic/cultural or socioeconomic factors had a substantial impact on prevalence [9].
It remains unclear whether the reported increase in ASD prevalence is due to an actual increase in the number of people who have autism, the result of better diagnostic tools and greater awareness, or a combination of both [10, 11]. Regardless of the cause, the increased numbers have led to a worldwide interest in studying ASD and its mechanisms.
An early autism diagnosis is essential for early intervention and treatment and enables patients to reach public support systems earlier, all of which are linked to a better prognosis, fewer autism symptoms over time, and better inclusion [10, 12]. On the other hand, delayed diagnoses are linked to increased parental stress and delays in treatments needed for better long-term trajectories [13]. Since identifying risk factors linked to delayed ASD diagnoses could potentially lead to a better diagnostic framework, it has been an area of interest in recent years.
A comprehensive review of 42 studies, written in English, published between 1990 and 2012, and indexed in PubMed, showed that higher socioeconomic status, symptom severity, and greater parental concern were associated with an earlier diagnosis [14]. The vast majority of the reviewed studies found no association between the sex of the child and age at ASD diagnosis. Furthermore, this critical and high-quality review looked at possible causes for delayed ASD diagnoses and unsurprisingly found that Asperger syndrome tends to be diagnosed at older ages than other types of ASD [14].
A 2021 Danish study supported the idea that the age at diagnosis varies relative to the subtype of ASD diagnosis and that atypical autism, Asperger syndrome, and pervasive developmental disorders not otherwise specified tend to be diagnosed at older ages [15]. This study also found an association between delayed ASD diagnosis and low parental education; however, only when compared to a group of patients that received an early autism diagnosis, not when compared to a control group with no ASD diagnosis. Lastly, this study found that being diagnosed with ADHD, language, developmental, or emotional disorders were risk factors for a delayed ASD diagnosis. The strongest association was seen in children with a previous diagnosis of ADHD [15].
In the Czech Republic, the diagnostic process of autism occurs in various settings. Two university departments (our Department of Child Psychiatry in Prague and the Department of Child Neurology in Brno) provide a diagnosis of autism during short-term hospitalizations requiring a referral from a pediatrician, child psychiatrist, neurologist, or clinical child psychologist. The process includes comprehensive assessment (e.g., psychiatric examination supplemented by specific diagnostic tools for autism, genetic examination, and an EEG). Diagnosis of autism is also provided by many but not all child psychiatrists and clinical child psychologists as outpatient care. Starting in 2016, all primary care pediatricians were obliged to begin screening all children aged 18 months for autism. All these assessments are covered by general health insurance, are free of charge, and all families are supposed to have equal access to the facilities. Besides these, services based on private payments are offered by some private providers in major towns, and we can assume they target high-income families. Regardless of the payment type, all services are generally limited by the small number of child psychiatrists with expertise in autism, which contributes to long waiting times. Due to COVID-19, waiting times now range from 1 to 2 years.
In our previous study of 160 children, we found that the ASD diagnosis age correlated negatively with maternal and paternal ages at the time of birth of the ASD child as well as with paternal and maternal education. However, it did not correlate with socioeconomic status or the number of ASD information resources available to the parents [16].
In this study, we enrolled new participants and broadened the cohort to 324 children aged 2 to 16 years. The aim of our study was to further explore the association between age at diagnosis and demographic variables, such as socioeconomic status, parental education level, age of parents, the Autism Diagnostic Observation Schedule (ADOS) scores, and intellectual disabilities.
Methods
Assessment
ICD-10 [1] was used to make a clinical diagnosis, and experienced clinicians with expertise in ASD diagnoses were involved in the study. A diagnosis was further supported by the age-appropriate modules from the Autism Diagnostic Observation Schedule (ADOS) [17] and/or the Autism Diagnostic Interview-Revised (ADI-R) [18]. The concept of the best estimate clinical diagnosis (BECD), by consensus of two experienced specialists, was used as the gold standard [19]. If there was disagreement between the ADI-R or ADOS diagnosis and the BECD, the latter was preferred. IQ testing was also performed. The Wechsler Preschool and Primary Scale of Intelligence, Fourth UK edition (WPPSI-IV), and the Wechsler Intelligence Scale for Children, Fourth UK edition (WISC-IV) were used for most children. For some autistic children, the Snijders-Oomen Nonverbal Intelligence Test, Revision 2, 5–7 (SON-R 2, 5–7) and the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley III) were alternatively used.
Previously, we created a simple descriptive questionnaire [17] focusing on (a) the family’s general situation and (b) the family’s self-education regarding autism. For this study, we used the first part that described family information, including (1) parental ages at the initial examination and ages and at the time of birth of the ASD-affected child, (2) the educational level of the parents, (3) household situation (i.e., parents living together, or being separated/ divorced), (4) marital status, and (5) family socioeconomic status (SES). We divided the participant families into three SES subgroups based on family income; this classification was based on the Czech State legal definitions in force at the beginning of the study. See our previous publication for more details on the questionnaire [16].
Most questionnaires were completed by mothers (N = 205; 88.4%). Fathers completed the questionnaires in 27 cases (11.6%); missing values were noted in 5 cases.
Sample
Responders were the parents of the 324 children referred for a diagnostic examination focused on autism at the Department of Child Psychiatry between November 2012 and June 2021. The study was approved by the Multicenter Ethics Committee of the University Hospital Motol. Parents who agreed to have their child participate in the study signed informed consent.
A diagnosis of ASD was confirmed in 237 children (73% of the referrals). The clinical characteristics of the sample are given in Table 1.
Table 1.
Clinical characteristics of the sample
| Variable | Frequency or mean/median |
|---|---|
| Gender (boys/girls) | 193/44 |
| Mean age at diagnosis (years) | 5.8 ± 2.2 |
| Median age at diagnosis (years) | 5.3 |
| Range of age at diagnosis (years) | 2.2–14.8 |
| ICD-10 diagnoses | |
| Childhood autism | 196 |
| Atypical autism | 31 |
| Asperger syndrome | 9 |
| Other childhood disintegrative disorders | 1 |
| Mental retardation in total (% of the sample) | 148 (62.4%) |
| Mild | 62 |
| Moderate | 59 |
| Severe | 10 |
| Unspecified | 17 |
ICD-10 International Classification of Diseases, 10th Edition
Family information is displayed in Table 2.
Table 2.
Family characteristics of the sample (n = 237)
| Mean (± SD, range) or frequency (%) | |
|---|---|
| Maternal | |
| Age at birth of ASD child (years) | 30.3 (± 5.2, 18.9–43.8) |
| Education | |
| Elementary | 33 (13.9%) |
| High school | 138 (58.2%) |
| University | 66 (27.8%) |
| Paternal | |
| Age at birth of ASD child (years) | 33.5 (± 6.2, 20.3–57.3) |
| Education | |
| Elementary | 45 (19.0%) |
| High school | 115 (48.5%) |
| University | 68 (28.7%) |
| Unknown | 9 (3.8%) |
| Family socioeconomic status | |
| Low | 51 (21.5%) |
| Middle | 159 (67.1%) |
| High | 22 (9.3%) |
| Unknown | 5 (2.1%) |
| Parents | |
| Live together | 179 (75.5%) |
| Separated or divorced | 58 (24.5%) |
SD standard deviation, ASD autism spectrum disorders
Data analysis
Statistical data analyses were performed using the statistical program R [20] and its psych library [21], in which the basic descriptive statistics of the data set and regression analyses were calculated. In addition, the rpart [22] and rpart.plot [23] libraries were used to build a machine learning-based classification tree.
A series of exploratory multiple regression analyses were initially computed to identify predictors of the age at which autism diagnoses were established. These predictors were then used in a machine-learning procedure that used sequential partitioning of the dataset.
The machine-learning algorithm consecutively divides the file into the best predictors of age at diagnosis. The division criterion is based on the ANOVA (i.e., the F test), meaning that the algorithm looks for the most appropriate threshold in the predictor variable, which gives the highest F value. This results in two branches in the tree plot (technically two subfiles of the data), one representing the earlier-diagnosed children and the other the later-diagnosed children. The algorithm then continues separately in each of these subfiles recursively, which leads to subsequent subdivisions. This process continues until no more significant predictors are left to further divide the subgroups.
At every node where the tree branches, two subgroups emerge that are significantly different from each other at the age of diagnosis. The predictor variable threshold is the highest significance of the F test. In each leaf of the tree, there are two numbers, i.e., the upper one is the mean age at diagnosis of its subgroup, and the lower one is the percent size of the subgroup relative to the whole sample. The division process stops when no more significant predictors are left to further divide the subgroups. The last leaves are the resulting indivisible subgroups of the original file. The darker the color, the higher the age at diagnosis the leaf represents.
Results
In 237 children with confirmed ASD diagnosis, the ADI-R was completed in 205 cases (86.5%); of those, 199 cases (97.1%) scored positively, and only 6 cases (2.9%) were negative. The ADOS was completed for 211 children (89%); of those, results were positive in 203 children (96.2%) and negative in only eight children (3.8%). None of the children diagnosed with ASD had negative scores on both the ADI-R and ADOS.
Results of multiple regression analysis showed that younger ages at autism diagnosis were predicted by higher ADOS scores in the social domain, higher ADOS scores in the restrictive and repetitive behaviors and interest domain, higher maternal education, and both parents living in the same household; at the trend level, younger ages were associated with higher family SES (see Table 3).
Table 3.
Predictors of age at diagnosis of autism
| Estimate | Std. error | t value | p | |
|---|---|---|---|---|
| (Intercept) | 14.056 | 1.105 | 12.716 | 0.000*** |
| MAT-AGE | − 0.038 | 0.034 | − 1.107 | 0.270 |
| MAT-EDU | − 0.661 | 0.258 | − 2.564 | 0.011* |
| PAT-AGE | − 0.045 | 0.028 | − 1.604 | 0.111 |
| PAT-EDU | 0.130 | 0.240 | 0.543 | 0.588 |
| shared household | − 0.875 | 0.355 | − 2.469 | 0.014* |
| SES | − 0.496 | 0.269 | − 1.843 | 0.067ǂ |
| ADOS-COM | 0.083 | 0.098 | 0.846 | 0.399 |
| ADOS-SOC | − 0.212 | 0.058 | − 3.667 | 0.000*** |
| ADOS-RRBI | − 0.243 | 0.103 | − 2.36 | 0.019* |
| MR | − 0.208 | 0.328 | − 0.633 | 0.528 |
MAT-AGE maternal age at birth of ASD child, MAT-EDU maternal education, PAT paternal, SES socioeconomic status, ADOS-COM communication domain of the Autism Diagnostic Observation Schedule, ADOS-SOC social domain of the Autism Diagnostic Observation Schedule, ADOS-RRBI restrictive and repetitive behaviors and interest domain of the Autism Diagnostic Observation Schedule, MR mental retardation
Significance codes: ***p < 0.001, **p < 0.01, *p < 0.05, ǂp < 0.1
When we applied the classification tree to the data, the youngest mean age at diagnosis (4.9 years) was found in children, in whom the summation of the ADOS communication and social domain scores was ≥ 17, and paternal age at delivery was ≥ 29 years. On the other hand, the oldest mean age at diagnosis (8.9 years) was seen in children, in whom summation of the ADOS communication and social domain scores was < 17, and maternal education was at the elementary school level (see Fig. 1).
Fig. 1.
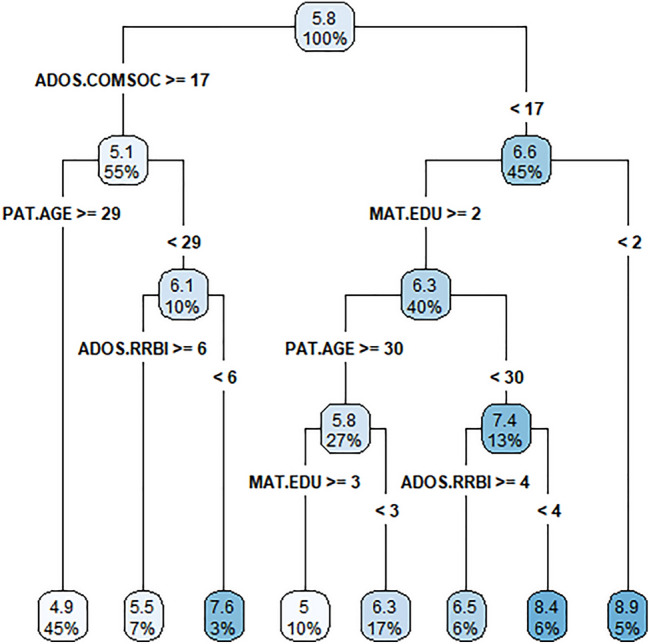
Results from the classification tree analysis of the age at diagnosis of ASD. ADOS.COMSOC summation of ADOS communication and social domain scores, PAT.AGE paternal age at birth of ASD child, MAT.EDU maternal education, ADOS.RRBI restrictive and repetitive behaviors and interest domain of the Autism Diagnostic Observation Schedule
Discussion
Our study was only the second to use the classification tree method applied to ‘age at ASD diagnosis’ (the first study [24] was limited by the fact that it was retrospective). In contrast to regression analysis, the classification tree analysis is hierarchical, which means the classification process takes place in subsequent divisions; in our opinion, this better simulates the natural diagnostic process. While multiple regression analysis is a variable-centered approach, classification tree analysis is a person-centered approach (which is more appropriate when considering the patient’s diagnosis). Furthermore, our study was the first to simultaneously use multiple regression analysis and the classification tree method on the same data. The agreement between the two methods produced what we believe are very robust results.
The age at diagnosis in our study was calculated as a mean and median. The mean age at diagnosis of 69.6 months (5.8 years) in our study was close to, though slightly older than the findings of a 2021 systematic review and meta-analysis looking at 35 studies, which found the mean age of diagnosis was 60.48 months (5.4 years) [25]. Our result is also older than a 2020 Austrian study finding, which found the mean age at diagnosis was 46.7 months (3.9 years) [26].
The median age of 63.6 months (5.3 years) found in our study was also older than the median of 52 months (4.3 years) found in a 2018 USA study [7] as well as the median age found in a 2016 UK study of 55.2 months (4.6 years) [27] but younger than the median age of 72 months (6 years) found in a 2018 Japanese study [28]. However, it is worth noting that most studies on this topic only state the mean age at diagnosis, not the median. The disadvantage is that a relatively small number of outliers may skew the results, which is why we state both in our study.
It is also important to note that our study looked at a clinical sample. This could potentially impact the waiting times between a referral by a general practitioner and evaluation by a specialist in our department, leading to an older age at diagnosis and subsequently to the older mean and median ages seen in our study. On the other hand, having a clinical sample might have contributed to high rates of confirmed ASD diagnoses in our autism diagnostic program (73%) since the first screening was done by the referring general practitioner, child psychiatrist, or psychologist. We can only speculate that a clinical sample also results in the high severity of autism in our sample, which was reflected by a relatively high value of the first classification node, which is a summation of ADOS communication and social interaction = 17. A value of 17 and higher was present in 55% of cases (i.e., 131 cases), whereas values less than 17 were found in 45% of cases (i.e., 106 patients). For comparison, the autism cut-off is 12, and the autism spectrum cut-off is 8 in ADOS Module 2; the same cut-offs are 10 and 7 in ADOS Module 3.
Another possible explanation for our study's older age at diagnosis is that health literacy in Czechia is relatively low. According to a 2016 study, Czechia ranked penultimate compared to eight other EU countries in health literacy [29].
Multiple regression analyses and the classification tree method were used to analyze the associations between age at diagnosis, demographic variables, ADOS scores, and intellectual disability. The results of the multiple regression analysis are in line with other studies using this statistical method.
The finding that younger ages at autism diagnosis correlate with higher maternal education provides further evidence for the association between age at diagnosis and parental education [15, 30]. The link between higher scores in ADOS social domain, ADOS restrictive and repetitive behaviors and interest domain, and the younger ages at diagnosis found in our study expands on a 2014 comprehensive review, which reported that symptom severity was associated with younger ages at diagnosis [14]. The association between age at diagnosis and the ADOS social and ADOS restrictive and repetitive behaviors and interest domain found in our study also agrees with the findings of a 2021 USA study that found an association between the severity of most ASD symptoms and the age at diagnosis [24]. The finding that both parents living in the same household was associated with a younger age at diagnosis also agrees with the current literature [31].
The classification tree scheme used in our study showed that children with ADOS communication and social domain scores that summed to ≥ 17 and paternal age at delivery ≥ 29 years had the youngest mean age at diagnosis. On the other hand, the oldest mean age at diagnosis was found in children with summed ADOS communication and social domain scores < 17 and maternal education at the elementary school level.
The link between specific ADOS domains and a delayed ASD diagnosis found in our study was inconsistent with a 2018 USA study [32] and the previously mentioned 2021 Danish study [15], neither of which found such an association; however, neither of these studies used the classification tree method and therefore did not take into account maternal education and paternal age, which were key covariates in the classification tree analysis of our study.
The association between age at diagnosis and ADOS communication and social domain scores was consistent with the previously mentioned USA study [24], which used factor analysis and was the first study prior to ours that applied the classification tree methodology. This study found an association between younger ages at diagnosis and deficits in communication skills, i.e., delayed language, absence of gestures, and responding to one’s name. Additionally, the study found the association even more robust than the one between age at diagnosis and overall symptom severity. However, like most other studies, this study did not consider maternal education and paternal age in their classification tree analysis.
In contrast to several US studies [33–36] and a meta-analysis of 42 studies by Daniels and Mandell [14], family socioeconomic status was not found to be a significant predictor in our study [it was significant only at the trend level (p = 0.067)]. Our SES results agree with the largest meta-analysis on the topic by Elsabbagh et al. [9], which involved over 600 studies (including studies in local languages).
Limitations
Possible limitations of our study include the fact that our study looked at a clinical sample, which could have caused the age at diagnosis in our study to be older than in population samples. The second limitation is that we did not consider comorbidities other than mental retardation, which could also influence the age at diagnosis. The third limitation is that we focused our analysis on global measures of autism as well as on family and socioeconomic circumstances rather than on particular autistic symptoms. Thus, we did not examine language development using a specific diagnostic tool other than the communication domain of ADOS, which did not influence the age at diagnosis in the multiple regression analysis (see Table 3); however, it was significant, in summation with the ADOS social domain, in classification tree analysis (see Fig. 1). The fourth limitation was related to the fact that for this research, we did not collect and analyze information regarding who referred the children to our autism diagnostic program. Therefore, we cannot confirm the Austrian findings that a referral by a pediatrician was associated with an earlier diagnosis [26]. Our results could have also been influenced by our sample, including only children, thereby excluding those diagnosed with autism in adulthood. However, autism diagnoses in adulthood in the Czech Republic are rare due to limited services for adult autistic subjects, although new data from the UK indicates that diagnosis rates among adults, females, and higher-functioning individuals are rising [37].
Conclusion
The severity of autism symptoms and maternal education impacted the age at diagnosis in both types of data analysis used in our study (i.e., multiple regression analysis and classification tree analysis).
Acknowledgements
The authors would like to thank Thomas Secrest, MSc., for his assistance with the English version of the manuscript.
Author contributions
MH conceived and designed the study and contributed to the drafts of the manuscript. TU performed the statistical analysis and commented on the manuscript. AR wrote a substantial part of the first draft of the manuscript. AK, OV, and ID collected data and commented on the manuscript drafts; ID also supervised the recruitment of patients. All authors read and approved the final manuscript.
Funding
Open access publishing supported by the National Technical Library in Prague. Our study was supported by the Ministry of Health of the Czech Republic (Grant no. NV18-04-00085 and the Project for Conceptual Development of Research Organization 00064203) and by Charles University, Prague (program Cooperatio, area Neuroscience).
Data availability
The data presented in this study is available on request from the corresponding author. The data is not publicly available due to privacy reasons.
Declarations
Conflict of interest
The authors declare no conflict of interest.
Ethics approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Multicenter Ethics Committee of the University Hospital Motol under protocol code 1480/12 on September 19, 2012.
Informed consent
Informed consent was obtained from the parents or caregivers of all subjects involved in the study.
Consent for publication
Parents or caregivers of all subjects consented to the publication of results anonymously.
References
- 1.World Health Organization . The ICD-10 classification of mental and behavioural disorders: clinical description and diagnostic guidelines. Geneva: World Health Organization; 1992. [Google Scholar]
- 2.Lai MC, Lombardo MV, Baron-Cohen S. Autism. Lancet. 2014;383:896–910. doi: 10.1016/S0140-6736(13)61539-1. [DOI] [PubMed] [Google Scholar]
- 3.Khaiman C, Onnuam K, Photchanakaew S, Chonchaiya W, Suphapeetiporn K. Risk factors for autism spectrum disorder in the Thai population. Eur J Pediatr. 2015;174:1365–1372. doi: 10.1007/s00431-015-2544-2. [DOI] [PubMed] [Google Scholar]
- 4.Fombonne E. Epidemiology of pervasive developmental disorders. Pediatr Res. 2009;65:591–598. doi: 10.1203/PDR.0b013e31819e7203. [DOI] [PubMed] [Google Scholar]
- 5.Baxter AJ, Brugha TS, Erskine HE, Scheurer RW, Vos T, Scott JG. The epidemiology and global burden of autism spectrum disorders. Psychol Med. 2015;45:601–613. doi: 10.1017/S003329171400172X. [DOI] [PubMed] [Google Scholar]
- 6.Rogge N, Janssen J. The economic costs of autism spectrum disorder: a literature review. J Autism Dev Disord. 2019;49:2873–2900. doi: 10.1007/s10803-019-04014-z. [DOI] [PubMed] [Google Scholar]
- 7.Baio J, Wiggins L, Christensen DL, et al. Prevalence of autism spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2014. Morb Mortal Wkly Rep Surveill Summ. 2018;67:1–23. doi: 10.15585/mmwr.ss6706a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baron-Cohen S, Scott FJ, Allison C, et al. Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry. 2009;194:500–509. doi: 10.1192/bjp.bp.108.059345. [DOI] [PubMed] [Google Scholar]
- 9.Elsabbagh M, Divan G, Koh YJ, et al. Global prevalence of autism and other pervasive developmental disorders: global epidemiology of autism. Autism Res. 2012;5:160–179. doi: 10.1002/aur.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Elder J, Kreider C, Brasher S, Ansell M. Clinical impact of early diagnosis of autism on the prognosis and parent-child relationships. Psychol Res Behav Manag. 2017;10:283–292. doi: 10.2147/PRBM.S117499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Weintraub K. The prevalence puzzle: Autism counts. Nature. 2011;479:22–24. doi: 10.1038/479022a. [DOI] [PubMed] [Google Scholar]
- 12.Swanson AR, Warren ZE, Stone WL, Vehorn AC, Dohrmann E, Humberd Q. The diagnosis of autism in community pediatric settings: does advanced training facilitate practice change? Autism. 2014;18:555–561. doi: 10.1177/1362361313481507. [DOI] [PubMed] [Google Scholar]
- 13.Zwaigenbaum L, Bauman ML, Stone WL, et al. Early identification of autism spectrum disorder: recommendations for practice and research. Pediatrics. 2015;136(Supplement 1):S10–S40. doi: 10.1542/peds.2014-3667C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Daniels AM, Mandell DS. Explaining differences in age at autism spectrum disorder diagnosis: a critical review. Autism. 2014;18:583–597. doi: 10.1177/1362361313480277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Avlund SH, Thomsen PH, Schendel D, Jørgensen M, Carlsen AH, Clausen L. Factors associated with a delayed autism spectrum disorder diagnosis in children previously assessed on suspicion of autism. J Autism Dev Disord. 2021;51:3843–3856. doi: 10.1007/s10803-020-04849-x. [DOI] [PubMed] [Google Scholar]
- 16.Hrdlicka M, Vacova M, Oslejskova H, et al. Age at diagnosis of autism spectrum disorders: is there an association with socioeconomic status and family self-education about autism? Neuropsychiatr Dis Treat. 2016;12:1639–1644. doi: 10.2147/ndt.s107239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lord C, Risi S, Lambrecht L, et al. The autism diagnostic observation schedule-generic: a standard measure of social and communication deficits associated with the spectrum of autism. J Autism Dev Disord. 2000;30:205–223. doi: 10.1023/A:1005592401947. [DOI] [PubMed] [Google Scholar]
- 18.Lord C, Rutter M, Le Couteur A. Autism diagnostic interview-revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord. 1994;24:659–685. doi: 10.1007/bf02172145. [DOI] [PubMed] [Google Scholar]
- 19.Kim SH, Lord C. Combining information from multiple sources for the diagnosis of autism spectrum disorders for toddlers and young preschoolers from 12 to 47 months of age. J Child Psychol Psychiatry. 2012;53:143–151. doi: 10.1111/j.1469-7610.2011.02458.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.R Core Team (2022) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. http://www.R-project.org/ Accessed May 3, 2022
- 21.Revelle W (2022) psych: Procedures for Personality and Psychological Research. Northwestern University, Evanston, Illinois, USA. Version = 2.1.9. https://CRAN.R-project.org/package=psych. Accessed 3 May 2022
- 22.Therneau T, Atkinson B (2019) rpart: Recursive Partitioning and Regression Trees. R package version 4.1–15. https://CRAN.R-project.org/package=rpart . Accessed 3 May 2022
- 23.Milborrow S (2021) rpart.plot: Plot 'rpart' Models: An Enhanced Version of 'plot.rpart'. R package version 3.1.0. https://CRAN.R-project.org/package=rpart.plot . Accessed 3 May 2022
- 24.Sicherman N, Charite J, Eyal G, et al. Clinical signs associated with earlier diagnosis of children with autism spectrum disorder. BMC Pediatr. 2021;21:96. doi: 10.1186/s12887-021-02551-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Van’t Hof M, Tisseur C, van Berckelear-Onnes I, et al. Age at autism spectrum disorder diagnosis: a systematic review and meta-analysis from 2012 to 2019. Autism. 2021;25:862–873. doi: 10.1177/1362361320971107. [DOI] [PubMed] [Google Scholar]
- 26.Primo GP, Weber C, Posada de la Paz M, Fellinger J, Dirmhirn A, Holzinger D. Explaining age at autism spectrum diagnosis in children with migrant and non-migrant background in Austria. Brain Sci. 2020;10:448. doi: 10.3390/brainsci10070448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Brett D, Warnell F, McConachie H, Parr JR. Factors affecting age at ASD diagnosis in UK: no evidence that diagnosis age has decreased between 2004 and 2014. J Autism Dev Disord. 2016;46:1974–1984. doi: 10.1007/s10803-016-2716-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kurasawa S, Tateyama K, Iwanaga R, Ohtoshi T, Nakatani K, Yokoi K. The age at diagnosis of autism spectrum disorder in children in Japan. Int J Pediatr. 2018;2018:5374725. doi: 10.1155/2018/5374725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kucera Z, Pelikan J, Steflova A. Health literacy in Czech population results of the comparative representative research. Cas Lek Cesk. 2016;155:233–241. [PubMed] [Google Scholar]
- 30.Fountain C, King MD, Bearman PS. Age of diagnosis for autism: individual and community factors across 10 birth cohorts. J Epidemiol Community Health. 2011;65:503–510. doi: 10.1136/jech.2009.104588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kalb LG, Holingue C, Pfeiffer D, et al. Parental relationship status and age at autism spectrum disorder diagnosis of their child. Autism. 2021;25:2189–2198. doi: 10.1177/13623613211013683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ozonoff S, Young GS, Brian J, et al. Diagnosis of autism spectrum disorder after age 5 in children evaluated longitudinally since infancy. J Am Acad Child Adolesc Psychiatry. 2018;57:849–857.e2. doi: 10.1016/j.jaac.2018.06.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Durkin MS, Maenner MJ, Meaney FJ, et al. Socioeconomic inequality in the prevalence of autism spectrum disorder: Evidence from a Us cross-sectional study. PLoS ONE. 2010;5:e11551. doi: 10.1371/journal.pone.0011551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.King MD, Bearman PS. Socioeconomic status and the increased prevalence of autism in California. Am Sociol Rev. 2011;76:320–346. doi: 10.1177/0003122411399389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Thomas P, Zahorodny W, Peng B, et al. The association of autism diagnosis with socioeconomic status. Autism. 2012;16:201–213. doi: 10.1177/1362361311413397. [DOI] [PubMed] [Google Scholar]
- 36.Mazurek MO, Handen BL, Wodka EL, Nowinski L, Butter E, Engelhardt CR. Age at first autism spectrum disorder diagnosis: the role of birth cohort, demographic factors, and clinical features. J Dev Behav Pediatr. 2014;35:561–569. doi: 10.1097/dbp.0000000000000097. [DOI] [PubMed] [Google Scholar]
- 37.Russell G, Stapley S, Newlove-Delgado T, et al. Time trends in autism diagnosis over 20 years: a UK population-based cohort study. J Child Psychol Psychiatry. 2022;63:674–682. doi: 10.1111/jcpp.13505. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data presented in this study is available on request from the corresponding author. The data is not publicly available due to privacy reasons.