

Abstract
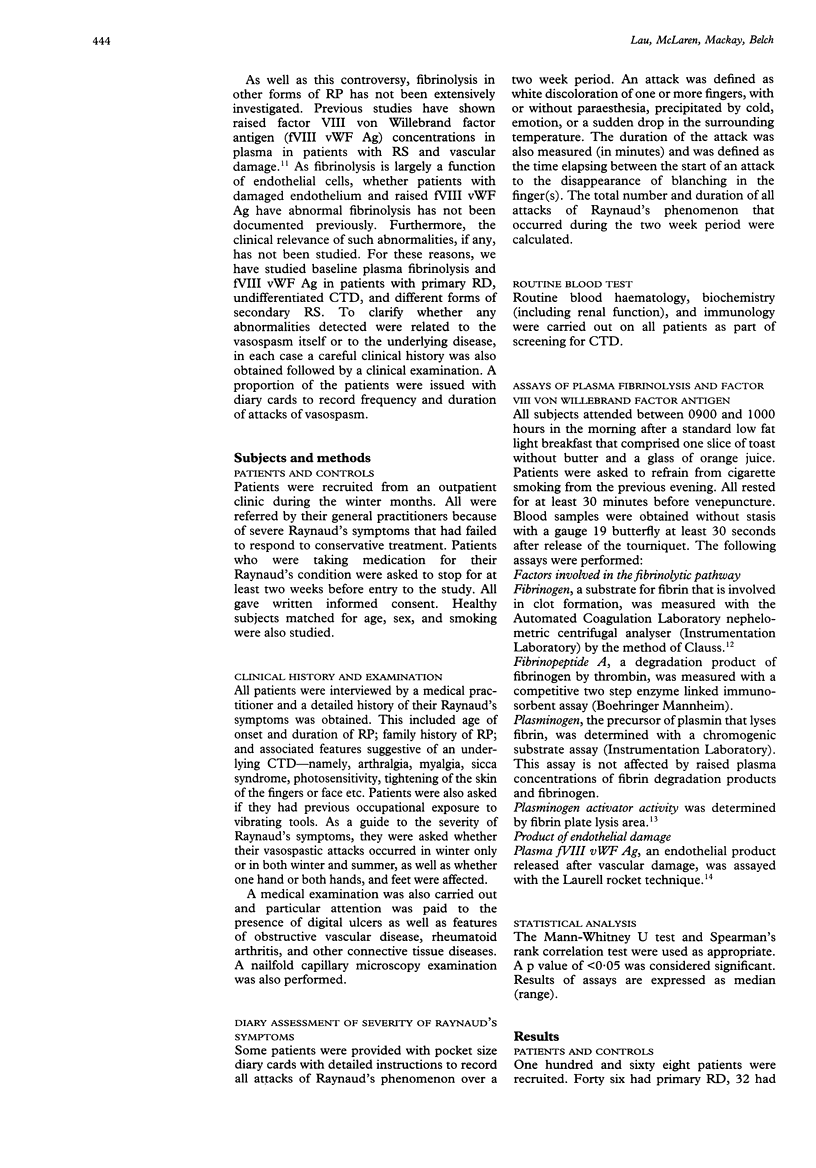
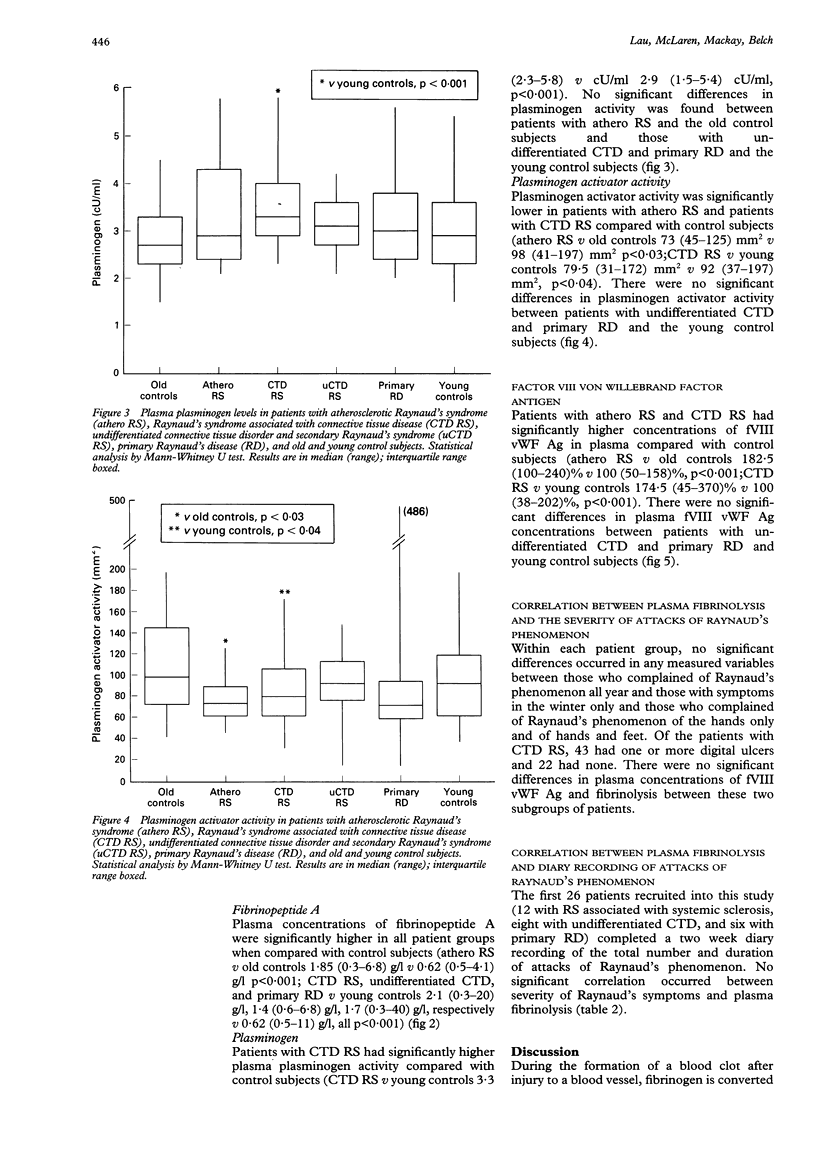
OBJECTIVES--(1) To assess if patients with various forms of Raynaud's phenomenon (RP) have abnormal plasma fibrinolysis that may contribute to diminished digital blood flow; (2) to assess whether patients with RP with evidence of endothelial damage have abnormal plasma fibrinolysis; (3) to determine the clinical relevance of abnormalities, if any, in plasma fibrinolysis in patients with RP. METHODS--One hundred and sixty eight patients with significant RP were studied--46 had primary Raynaud's disease (RD), 32 had suspected Raynaud's syndrome secondary to an undifferentiated connective tissue disorder (undifferentiated CTD), 25 had Raynaud's syndrome associated with atherosclerosis (athero RS), and 65 had an underlying connective tissue disease (CTD RS). All attended in the morning after a low fat light breakfast. After a clinical history was obtained, venous blood samples were collected without stasis for assays of plasma fibrinolysis and factor VIII von Willebrand factor antigen (fVIII vWF Ag). Results were compared with those obtained from normal subjects matched for sex and age. As patients with athero RS were significantly older than the other patients with Raynaud's phenomenon, two groups of control subjects were recruited--namely, 'old' and 'young' control subjects. RESULTS--Patients with CTD RS and athero RS had higher concentrations of fVIII vWF Ag (CTD RS median 174.5 range (45-370)% v 100 (38-202)%, p < 0.001; athero RS 182-5 (100-240)% v 100 (50-158)%, p < 0.001). Both had raised fibrinogen (CTD RS 3.25 (1.9-6.8) g/l v 2.4 (1.2-4.2) g/l, p < 0.001; athero RS 3.4 (2.2-6.2) g/l v 2.5 (1.8-3.9) g/l, p < 0.001) and both had diminished fibrinolysis with reduced plasminogen activator activity (CTD RS 79.5 (31-72) mm2 v 92 (37-197) mm2, p < 0.04; athero RS 73 (45-125) mm2 v 98 (41-197) mm2, p < 0.03). Patients with CTD RS also had raised plasminogen activity (3.3 (2.3-5.8) cU/ml v 2.9 (1.5-5.4) cU/ml, p < 0.001). On the contrary, patients with primary RD and undifferentiated CTD had normal fibrinogen and plasma fibrinolysis. Within each patient group, no significant differences in any of the measured variables were found between those who had RP all year and those who had RP in the winter only, those with RP of the hands only and of hands and feet, or those with and without digital ulcers. CONCLUSION--Diminished plasma fibrinolysis is found in patients likely to have endothelial damage (CTD RS and athero RS). These changes are probably a consequence rather than a cause of the disease.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arnett F. C., Edworthy S. M., Bloch D. A., McShane D. J., Fries J. F., Cooper N. S., Healey L. A., Kaplan S. R., Liang M. H., Luthra H. S. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988 Mar;31(3):315–324. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- Bachmann F., Kruithof I. E. Tissue plasminogen activator: chemical and physiological aspects. Semin Thromb Hemost. 1984 Jan;10(1):6–17. doi: 10.1055/s-2007-1004403. [DOI] [PubMed] [Google Scholar]
- Belch J. J., Zoma A. A., Richards I. M., McLaughlin K., Forbes C. D., Sturrock R. D. Vascular damage and factor-VIII-related antigen in the rheumatic diseases. Rheumatol Int. 1987;7(3):107–111. doi: 10.1007/BF00270462. [DOI] [PubMed] [Google Scholar]
- Brotzu G., Falchi S., Mannu B., Montisci R., Petruzzo P., Staico R. The importance of presynaptic beta receptors in Raynaud's disease. J Vasc Surg. 1989 Jun;9(6):767–771. [PubMed] [Google Scholar]
- CLAUSS A. Gerinnungsphysiologische Schnellmethode zur Bestimmung des Fibrinogens. Acta Haematol. 1957 Apr;17(4):237–246. doi: 10.1159/000205234. [DOI] [PubMed] [Google Scholar]
- Cunliffe W. J., Menon I. S. Blood fibrinolytic activity in diseases of small blood vessels and the effect of low molecular weight dextran. Br J Dermatol. 1969 Mar;81(3):220–225. doi: 10.1111/j.1365-2133.1969.tb16012.x. [DOI] [PubMed] [Google Scholar]
- Freedman R. R., Sabharal S. C., Desai N., Wenig P., Mayes M. Increased alpha-adrenergic responsiveness in idiopathic Raynaud's disease. Arthritis Rheum. 1989 Jan;32(1):61–65. doi: 10.1002/anr.1780320110. [DOI] [PubMed] [Google Scholar]
- Friedman E. I., Taylor L. M., Jr, Porter J. M. Late-onset Raynaud's syndrome: diagnostic and therapeutic considerations. Geriatrics. 1988 Dec;43(12):59-63, 67-70. [PubMed] [Google Scholar]
- Goyle K. B., Dormandy J. A. Abnormal blood viscosity in Raynaud's phenomenon. Lancet. 1976 Jun 19;1(7973):1317–1318. doi: 10.1016/s0140-6736(76)92651-9. [DOI] [PubMed] [Google Scholar]
- Jarrett P. E., Morland M., Browse N. L. Treatment of Raynaud's phenomenon by fibrinolytic enhancement. Br Med J. 1978 Aug 19;2(6136):523–525. doi: 10.1136/bmj.2.6136.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jayson M. I., Holland C. D., Keegan A., Illingworth K., Taylor L. A controlled study of stanozolol in primary Raynaud's phenomenon and systemic sclerosis. Ann Rheum Dis. 1991 Jan;50(1):41–47. doi: 10.1136/ard.50.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lau C. S., Bridges A. B., Muir A., Scott N., Bancroft A., Belch J. J. Further evidence of increased polymorphonuclear cell activity in patients with Raynaud's phenomenon. Br J Rheumatol. 1992 Jun;31(6):375–380. doi: 10.1093/rheumatology/31.6.375. [DOI] [PubMed] [Google Scholar]
- Marder V. J., Shulman N. R., Carroll W. R. High molecular weight derivatives of human fibrinogen produced by plasmin. I. Physicochemical and immunological characterization. J Biol Chem. 1969 Apr 25;244(8):2111–2119. [PubMed] [Google Scholar]
- Nilsson T. K., Johnson O. The extrinsic fibrinolytic system in survivors of myocardial infarction. Thromb Res. 1987 Dec 15;48(6):621–630. doi: 10.1016/0049-3848(87)90428-2. [DOI] [PubMed] [Google Scholar]
- PRINGLE R., WALDER D. N., WEAVER J. P. BLOOD VISCOSITY AND RAYNAUD'S DISEASE. Lancet. 1965 May 22;1(7395):1086–1088. doi: 10.1016/s0140-6736(65)92673-5. [DOI] [PubMed] [Google Scholar]
- Preliminary criteria for the classification of systemic sclerosis (scleroderma). Subcommittee for scleroderma criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee. Arthritis Rheum. 1980 May;23(5):581–590. doi: 10.1002/art.1780230510. [DOI] [PubMed] [Google Scholar]
- Tan E. M., Cohen A. S., Fries J. F., Masi A. T., McShane D. J., Rothfield N. F., Schaller J. G., Talal N., Winchester R. J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982 Nov;25(11):1271–1277. doi: 10.1002/art.1780251101. [DOI] [PubMed] [Google Scholar]