

Abstract
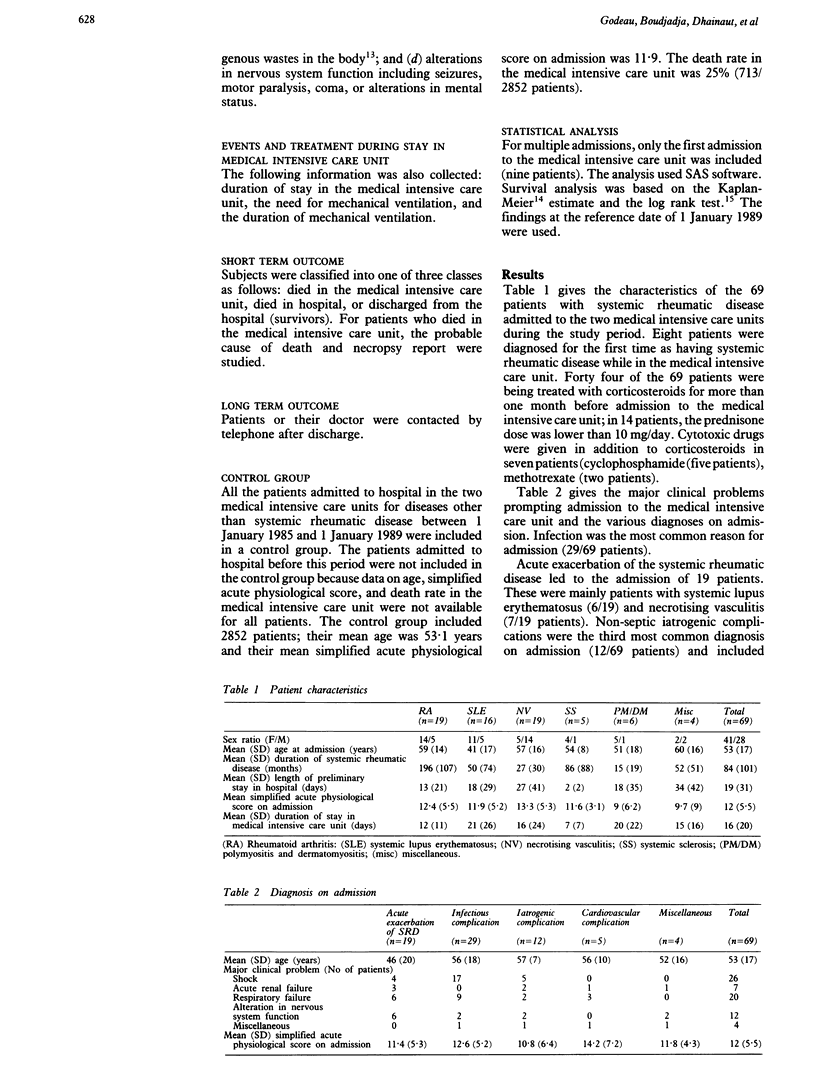
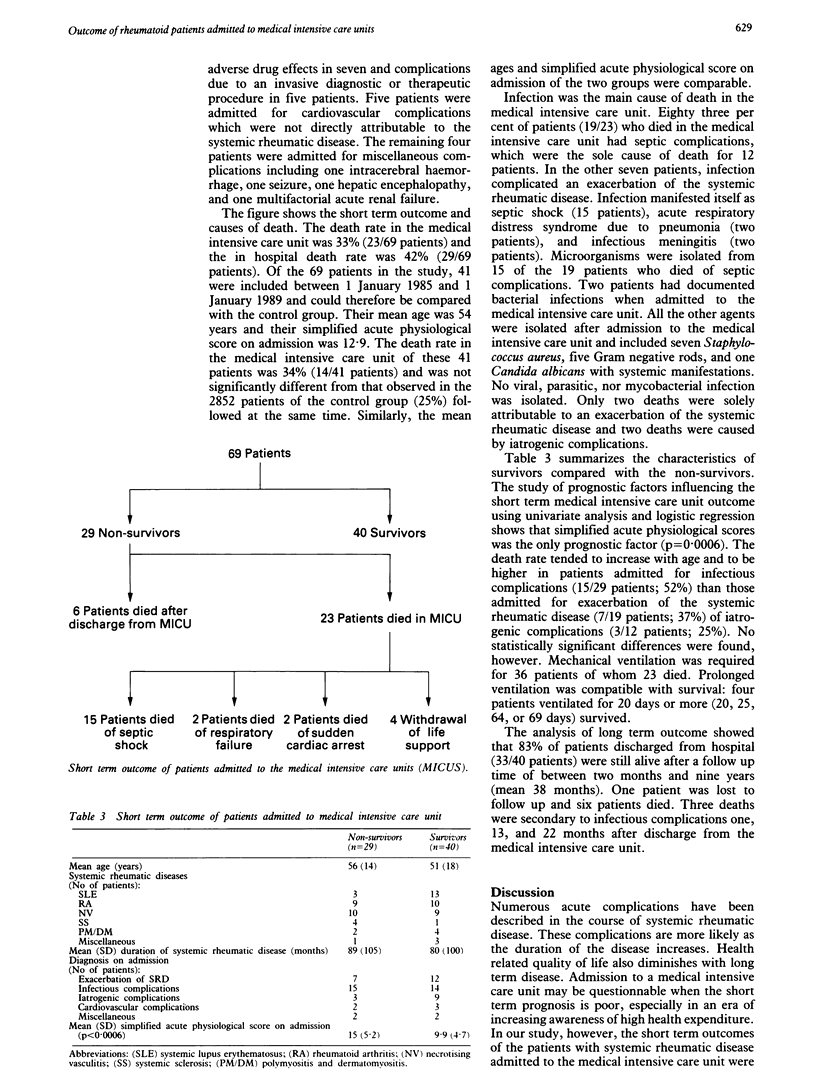
The outcome of patients admitted to intensive care units is known to be influenced by such factors as age, previous health status, severity of disease, and diagnosis. To estimate the outcome of such patients with systemic rheumatic diseases and to determine if the severity of these diseases unfavourably influences the prognosis at the time of admission to a medical intensive care unit, the clinical courses of all patients with systemic rheumatic disease admitted to two medical intensive care units between January 1978 and December 1988 were studied retrospectively. Sixty nine patients with systemic lupus erythematosus (n = 16), necrotising vasculitis (n = 19), rheumatoid arthritis (n = 19), and other systemic rheumatic diseases (n = 15) were included. The mean (SD) age on admission into the medical intensive care unit was 53 (17) years and the mean simplified acute physiological score was 12 (5.5). The principal diagnoses on admission were infectious complications (29/69 patients) and acute exacerbation of the systemic rheumatic disease (19/69 patients). The death rate in the medical intensive care unit was 33% (23/69 patients) and was similar to that of a non-selected population with comparable simplified acute physiological score. The death rate in hospital was 42% (29/69 patients). Infection was the main cause of death in the medical intensive care unit (19/23 patients) and the infection was mainly acquired in the unit. Only the simplified acute physiological score on admission was a statistically significant prognostic factor: the simplified acute physiological score in patients who died was 15 (5.2) v 9.9 (4.7) for survivors. Long term outcome analysis showed that 83% (33/40 patients) of patients were still alive after admission to the medical intensive care unit with a follow up time between two months and nine years (mean 38 months). The death rate was relatively high and was mainly due to nosocomial infections. It was not different, however, from that of nonselected patients and the long term prognosis was highly favourable. This shows that the complications are often reversible, particularly infectious applications, and justifies admission to the medical intensive care unit of this group of patients.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arnett F. C., Edworthy S. M., Bloch D. A., McShane D. J., Fries J. F., Cooper N. S., Healey L. A., Kaplan S. R., Liang M. H., Luthra H. S. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988 Mar;31(3):315–324. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- Bohan A., Peter J. B. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975 Feb 13;292(7):344–347. doi: 10.1056/NEJM197502132920706. [DOI] [PubMed] [Google Scholar]
- Bohan A., Peter J. B. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975 Feb 20;292(8):403–407. doi: 10.1056/NEJM197502202920807. [DOI] [PubMed] [Google Scholar]
- Brunet F., Lanore J. J., Dhainaut J. F., Dreyfus F., Vaxelaire J. F., Nouira S., Giraud T., Armaganidis A., Monsallier J. F. Is intensive care justified for patients with haematological malignancies? Intensive Care Med. 1990;16(5):291–297. doi: 10.1007/BF01706352. [DOI] [PubMed] [Google Scholar]
- Craven D. E., Kunches L. M., Lichtenberg D. A., Kollisch N. R., Barry M. A., Heeren T. C., McCabe W. R. Nosocomial infection and fatality in medical and surgical intensive care unit patients. Arch Intern Med. 1988 May;148(5):1161–1168. [PubMed] [Google Scholar]
- Fauci A. S. Vasculitis. J Allergy Clin Immunol. 1983 Sep;72(3):211–223. doi: 10.1016/0091-6749(83)90021-0. [DOI] [PubMed] [Google Scholar]
- Hellmann D. B., Petri M., Whiting-O'Keefe Q. Fatal infections in systemic lupus erythematosus: the role of opportunistic organisms. Medicine (Baltimore) 1987 Sep;66(5):341–348. doi: 10.1097/00005792-198709000-00002. [DOI] [PubMed] [Google Scholar]
- Knaus W. A., Draper E. A., Wagner D. P., Zimmerman J. E. Prognosis in acute organ-system failure. Ann Surg. 1985 Dec;202(6):685–693. doi: 10.1097/00000658-198512000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Gall J. R., Loirat P., Alperovitch A., Glaser P., Granthil C., Mathieu D., Mercier P., Thomas R., Villers D. A simplified acute physiology score for ICU patients. Crit Care Med. 1984 Nov;12(11):975–977. doi: 10.1097/00003246-198411000-00012. [DOI] [PubMed] [Google Scholar]
- Mitchell D. M., Spitz P. W., Young D. Y., Bloch D. A., McShane D. J., Fries J. F. Survival, prognosis, and causes of death in rheumatoid arthritis. Arthritis Rheum. 1986 Jun;29(6):706–714. doi: 10.1002/art.1780290602. [DOI] [PubMed] [Google Scholar]
- Rosner S., Ginzler E. M., Diamond H. S., Weiner M., Schlesinger M., Fries J. F., Wasner C., Medsger T. A., Jr, Ziegler G., Klippel J. H. A multicenter study of outcome in systemic lupus erythematosus. II. Causes of death. Arthritis Rheum. 1982 Jun;25(6):612–617. doi: 10.1002/art.1780250602. [DOI] [PubMed] [Google Scholar]
- Schuster D. P., Marion J. M. Precedents for meaningful recovery during treatment in a medical intensive care unit. Outcome in patients with hematologic malignancy. Am J Med. 1983 Sep;75(3):402–408. doi: 10.1016/0002-9343(83)90340-6. [DOI] [PubMed] [Google Scholar]
- Strieter R. M., Lynch J. P., 3rd Complications in the ventilated patient. Clin Chest Med. 1988 Mar;9(1):127–139. [PubMed] [Google Scholar]
- Tan E. M., Cohen A. S., Fries J. F., Masi A. T., McShane D. J., Rothfield N. F., Schaller J. G., Talal N., Winchester R. J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982 Nov;25(11):1271–1277. doi: 10.1002/art.1780251101. [DOI] [PubMed] [Google Scholar]
- Young L. S. Nosocomial infections in the immunocompromised adult. Am J Med. 1981 Feb;70(2):398–404. doi: 10.1016/0002-9343(81)90779-8. [DOI] [PubMed] [Google Scholar]
- Zizic T. M., Classen J. N., Stevens M. B. Acute abdominal complications of systemic lupus erythematosus and polyarteritis nodosa. Am J Med. 1982 Oct;73(4):525–531. doi: 10.1016/0002-9343(82)90331-x. [DOI] [PubMed] [Google Scholar]