

Abstract
Objective:
Youth with poorly-controlled asthma are at increased risk for sleep disturbances caused by nocturnal symptoms like coughing. Asthma-related sleep disturbances can have downstream consequences for youth with asthma and their families. This study aims to describe (1) sleep disturbances in adolescents with poorly-controlled asthma and their caregivers and (2) the relationship between sleep and asthma management.
Methods:
Adolescents with poorly-controlled asthma and their caregivers completed the Family Asthma Management System Scale (FAMSS), a semi-structured interview that assesses youth asthma management within the family context. Interviews were audio-recorded and transcribed. Two authors coded each transcript for sleep-related data in NVivo using descriptive content analysis.
Results:
Thirty-three adolescents ages 12–15 years old (M = 13.2, SD = 1.2) with poorly-controlled asthma and their caregivers participated in this study. Four main themes emerged: sleep difficulties, sleep environment, sleep and self-management, and fatigue and self-management. 42% of youth and caregivers reported worse nocturnal asthma symptoms (e.g. coughing) that caused frequent nighttime awakening. Approximately 27% of caregivers expressed distress over their child’s nocturnal asthma and described their management strategies (e.g. co-sleeping, nighttime symptom monitoring). Adolescents described sleepiness as a barrier to asthma self-management tasks (e.g. medication adherence, response to exacerbation).
Conclusion:
Interview responses demonstrated the considerable interrelationship of sleep and asthma management in adolescents with poorly-controlled asthma. Asthma providers should consider discussing sleep difficulties with their adolescent patients and their families. Addressing these difficulties may help adolescents improve their asthma self-management and help caregivers better cope with their child’s disease.
Keywords: Adolescents, family, sleep disturbance, fatigue, self-management
Introduction
Asthma, the most common chronic childhood illness in the United States, affects approximately 5.5 million youth (1). Asthma management is complex and includes symptom monitoring, trigger avoidance, medication adherence, consistent medical care, and other preventative lifestyle factors (2). Qualitative data from focus groups suggest that as youth transition into adolescence, asthma management responsibilities shift such that adolescents manage their disease independently. Adolescents are more likely to experience difficulties with asthma self-management including suboptimal adherence to inhaled corticosteroids (ICS), poor symptom monitoring during exacerbations, ineffective response to symptoms, and lack of symptom prevention (3–5). Therefore, adolescents with asthma are at risk for increased morbidity, poor asthma control, and lower quality of life (QOL) (6–10).
The relationship of sleep and asthma self-management difficulties among adolescents is understudied. Overall, adolescents get fewer hours of sleep compared to school-age children because of developmental changes, decreased parental supervision, increased technology use, and demanding school schedules (11). Shorter sleep duration is associated with the onset of asthma symptoms in adolescents and young adults (12,13). Further, adolescents with poorly-controlled asthma are at an increased risk of sleep disturbances (14). Frequent sleep disturbances from nocturnal asthma symptoms, like coughing or wheezing, can lead to fragmented sleep and shorter sleep duration (12,15–17). Previous research has suggested a bidirectional relationship between sleep quality and asthma symptoms; poor sleep quality can contribute to an increase in severity of symptoms, and more severe symptoms can cause poor sleep (15,18,19). In general, adolescents with poorly-controlled asthma have worse sleep hygiene compared to adolescents with controlled asthma (17).
Sustained poor sleep quality has downstream consequences for adolescents with asthma and their families. Relationships exist between poor sleep quality and markers of poor health including reduced immune system functioning and metabolic/endocrine regulation (15). Furthermore, children (20) and adolescents (17) with asthma that have poor sleep quality can experience delayed emotional and physical growth as well as impaired learning and cognitive development. Youth with frequent nighttime asthma symptoms are more likely to miss school and their caregivers are more likely to miss work and experience increased symptoms of anxiety or depression compared to youth without nocturnal symptoms (20,21). Moreover, nocturnal asthma often disrupts adolescents and their caregivers’ ability to effectively self-manage their asthma and attain asthma control (17,20).
Additional research is necessary to understand the cyclical relationship between sleep and asthma management in adolescents with poorly controlled asthma. The objective of this study is to explore how adolescents with poorly-controlled asthma and their caregivers describe (1) their sleep disturbances related to asthma and (2) the relationship between sleep and asthma self-management tasks. To our knowledge, this is the first study to use qualitative methods to specifically study sleep and asthma management in early adolescence (12–15 years-old), a developmental window that is critical for sleep habits and asthma self-management.
Methods
Procedures
The Institutional Review Board approved all recruitment and study procedures. Medical providers identified participants in a pediatric pulmonary clinic in a children’s hospital located in the southeastern United States. Study staff recruited families for participation in a larger study focused on asthma management in adolescents (22). We analyzed baseline data for the current study. Families received compensation for their participation in this study.
Trained study staff screened potential participants for eligibility. Eligible youth had a physician-verified diagnosis of persistent asthma as defined by the National Asthma Education Prevention Program, were 12–15 years old, were prescribed an ICS, and had poorly-controlled asthma (2). Uncontrolled asthma was operationalized as having a score ≤ 19 on the Asthma Control Test or demonstrating any of the following symptoms in the past two weeks: more than 4 days of daytime asthma symptoms, 1 or more nights of nighttime awakenings, more than 4 days of normal activity limitation, or more than 4 days of using short-acting beta antagonist (i.e. rescue inhaler) (23,24). Excluded youth were unable to read or speak English, had an intellectual disability, and/or were current participants of another asthma intervention. Caregivers provided informed consent and youth provided assent.
Data collection
Baseline study visits occurred in participants’ homes, research spaces, or private community spaces. Caregivers provided basic demographic information. We assessed perceptions of family socioeconomic status via the question, “Which of these phrases describes best your family’s economic status?” Response options included “poor,” “almost poor,” “living check to check,” “living comfortably,” or “living very well.”
The Family Asthma Management System Scale (FAMSS), a semi-structured clinical interview, was audio-recorded and used to assess the management of children’s asthma within the family context (25,26). The FAMSS includes seven core domains: (1) asthma knowledge (3 questions), (2) symptom assessment (5 questions), (3) response to symptoms and exacerbations (3 questions), (4) environmental control (5 questions), (5) medication adherence (7 questions), (6) collaboration with health provider (5 questions), (7) and balanced integration of asthma and family life (5 questions) (26) . The FAMSS includes a series of free response questions. For example, one free response question asks, “When does [child’s name] have the most trouble? Is there a time of year? Is there a time of the day?” Participants also provide self-reported responses using a 5-point Likert scale (e.g. “On a five-point scale from 1 = very uncomfortable to 5 = very comfortable, how comfortable do you feel asking your child’s doctor about asthma?”) (26).
All FAMSS interviewers participated in multiple training sessions conducted by the senior author for the administration of the FAMSS. Study staff attended 21 consensus meetings (22% of FAMSS interviews included) with one of the interview developers to ensure consistency to FAMSS procedures. Study staff members independently rated interviews and then reviewed ratings together to achieve a “consensus” rating for each interview. Interrater reliability was acceptable across FAMSS subscales (ICC range = 0.68–0.95). For the purposes of this manuscript, we qualitatively analyzed all sleep-related free responses from the FAMSS interviews to gain a more in-depth understanding of the dyad’s personal experiences with sleep and asthma management.
Data analysis
Study staff de-identified and transcribed audio recordings verbatim, and each transcription was verified by an independent study staff member. Transcripts were imported into NVivo (Version 12.0.0.71 Plus; QSR International, 2018), a qualitative software program. The first and second authors reviewed each line of the transcripts and coded all sleep-related content. We created and referenced a codebook (see Table 2) with the definition of each code and fictional examples. An audit trail tracked all changes made during the coding process, and any discrepancies between coders were resolved through discussion.
Table 2.
Codebook.
| Theme | Code | Definition |
|---|---|---|
| Sleep difficulties | Worse Symptoms at Night | Child experiences worse asthma symptoms at night or during sleep. |
| Disturbed Child Sleep | Child’s sleep is impacted; asthma symptoms interfere with child’s sleep. | |
| Disturbed Caregiver Sleep | Caregiver’s sleep is impacted; asthma management behaviors or worries related to asthma interfere with caregiver sleep. | |
| Fear of Sleep | Child is scared or worried to sleep due to asthma symptoms. | |
| Sleep environment | Trigger Avoidance | The family discusses avoiding triggers in child’s sleeping environment. |
| Inhaler by bedside | Inhaler is stored by the child’s bed. | |
| Sleep and Self-Management | Caregiver Monitoring of Symptoms During Sleep | Caregiver monitors child’s symptoms while child is asleep. |
| Sleep as Response to Exacerbation | The child takes a nap or sleeps as part of their response to an exacerbation | |
| Fatigue and self-management | Influence on Willingness to Take Medications | Fatigue impacts the child’s willingness to take asthma medications |
| Early Warning Sign | Fatigue is an early warning sign or sign that the child might start having asthma symptoms. | |
| Symptom to Monitor During an Exacerbation | Observing the child’s level of fatigue helps families determine how well a medication is working. | |
| Medication Side Effect | Fatigue is a side effect of asthma medications. |
Following the coding of all data, initial codes were collapsed into broader themes and organized into a hierarchy (27). Qualitative methods and participant quotes demonstrated the meaning and significance of participants’ sleep-related experiences (28). The primary author removed “filler” words (e.g. “um”) in the reported quotations to increase readability; however, the remaining parts of each quotation are reported verbatim. We utilized descriptive content analysis and synthesized data into thematic descriptions in accordance with Sandelowski & Barroso (29). Some percentages were included to increase the clinical utility of the data. However, in an effort to follow published guidelines on qualitative research, not all responses were quantified (29,30).
Results
Participants
Participants included 33 adolescents (age 12–15 years) and their caregivers. Adolescents were primarily Black/African American (63.6%). Caregivers included mothers (87.9%) and grandmothers (12.1%); 34.4% obtained post-secondary education. Descriptive statistics were computed using SPSS (Version 25). See Table 1 for additional demographic information.
Table 1.
Youth and caregiver demographic characteristics.
| (SD) | n (%) | |
|---|---|---|
| Age | ||
| Child age | 13.2 (1.2) | |
| Caregiver age | 43.0 (9.3) | |
| Youth gender | ||
| Male | 18 (54.5) | |
| Female | 15 (45.5) | |
| Youth race/Ethnicity | ||
| Black/African American | 21 (63.6) | |
| White/Caucasian | 5 (15.2) | |
| Hispanic/Latinx | 3 (9.1) | |
| Multiracial | 3 (9.1) | |
| Asian | 1 (3.0) | |
| Family economic status | ||
| “Living check to check” or “Almost poor” | 24 (72.7) | |
| “Living very well” or “Living comfortably” | 9 (27.3) | |
Thematic structure
Four main sleep-related themes emerged: sleep difficulties, sleep environment, sleep and self-management, and fatigue and self-management. Each main theme included 2–4 sub-categories. We sorted all adolescent and caregiver sleep-related responses into these sub-categories. See Figure 1 for the coding tree.
Figure 1.
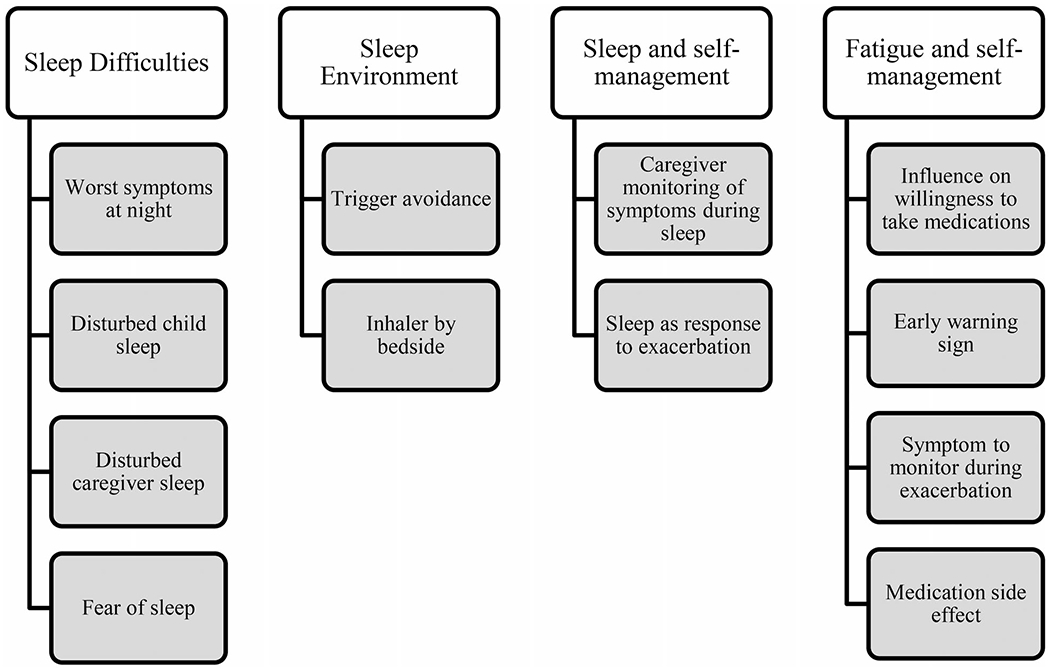
Coding tree.
Sleep difficulties
Both adolescents and caregivers experienced sleep difficulties. Almost half of dyads reported that adolescents (42%) experience worse asthma symptoms at night. When asked if there is a time of day in which their child experiences worse asthma symptoms, one caregiver reported “Especially at night she go to coughin’, like coughing a lot, and I go ohh that asthma actin’ up.” Nocturnal asthma symptoms included coughing, shortness of breath, and wheezing. Overall, the dyads’ responses indicated that nighttime asthma symptoms were frequent and concerning to the family.
One third of adolescents reported sleep disturbances caused by nocturnal asthma symptoms, most often coughing. A few adolescents reported delayed awakening from nocturnal asthma symptoms which cause them to wake gasping for air. For example, one adolescent stated, “It’s like when I wake up from my sleep it’s already a little too late because right when I wake up I’m like (gasps) and I don’t know why I wouldn’t wake up earlier and know what is happening.” One adolescent expressed the need to re-awaken at night to continue breathing treatments saying, “like all night, every 4 hours, I was doing breathing treatments.” One caregiver reported their child having a fear of sleep because of their nocturnal asthma symptoms.
Similarly, almost one third of caregivers (27%) experienced sleep disturbances due to their child’s asthma symptoms. Several caregivers expressed distress regarding their child’s nocturnal asthma symptoms which inhibited their sleep. For example, one caregiver recounted, “I used to have to sleep on the floor besides his bed because I was afraid he might stop breathing one time and not start back.” Another caregiver shared a similar concern that “all a sudden he can be gagging and I can’t sleep so I have to stay up all night so that’s my worry cause like I’m like is he breathing or is he not.” One caregiver recounted an experience in which they had to wake their child and administer treatment during an exacerbation because “he did not wake up.”
The reports from dyads in our sample clearly illustrate a connection between nocturnal asthma symptoms and sleep disturbances for both adolescents and their caregivers. Since many adolescents experience more severe symptoms at night, caregivers often feel pressure to remain vigilant at night to protect their children.
Sleep environment
Almost half of dyads (48%) described advice they received from professionals regarding modifications to the adolescent’s home environment that could help them avoid nighttime asthma triggers and better respond to nighttime exacerbations. For example, one caregiver was encouraged to implement dust mite control measures by covering their child’s mattress and pillows and washing the child’s bedding weekly. Several other dyads reported frequent cleaning of bedding, toys, carpeting, and AC vents to avoid triggering the adolescent’s asthma during sleep. A few caregivers reported restricting adolescents’ exposure to stuffed animals in their sleeping environment with one caregiver reporting that they “keep them all in plastic.” Finally, one dyad reported keeping asthma medication by the adolescent’s bedside for easy access at night and explained that, “the doctor said it needs to be beside him when he sleeps.”
Sleep and self-management
Both adolescents and caregivers modified their sleep behaviors in an effort to manage the adolescent’s asthma. Many caregivers (27%) reported nighttime symptom monitoring as an asthma management strategy. One parent explained, “I don’t get no sleep because I’m listening for everything. I’m like ‘is he breathing?’ Start touching him to make sure he’s breathing.” One caregiver explained that they chose to co-sleep with their child to better monitor their asthma, reporting “I still sleep with my two boys, I’ll be honest, I have them sleep with me.” Another caregiver reported also monitoring their child’s asthma symptoms during naps stating that “…if he’s taking a nap, I’m monitoring it. I’m watching him, I’m watching his breathing patterns and all that.” Some of the caregivers expressed that monitoring their adolescent’s nighttime symptoms is an expected part of managing their child’s asthma. For example, one caregiver explained that “To have a child that has problems with breathing and you have to be on standby and on guard… You have to keep a close eye and close ear on him.” Many caregivers explained their need to remain alert overnight, and some caregivers shared their anxious thoughts regarding their child’s nocturnal asthma.
A few adolescents (6%) endorsed the use of sleep as a strategy for managing asthma exacerbations. When an interviewer asked one adolescent what they would do if their quick relief medication was not working, they responded “jump in my bed and be lazy.” Another adolescent reported trying to “sleep it off” as a response to asthma exacerbations. Although only a few adolescents reported sleeping as a response to symptoms, this behavior is concerning as it is contraindicated and the adolescents did not seem aware of the potential negative consequences associated with this response strategy (2).
Fatigue and self-management
Several caregivers (24%) and a few adolescents (9%) reported that fatigue or sleepiness influences their willingness to administer or take asthma medications. While reflecting on how they most frequently miss doses of their ICS at nighttime, one adolescent reported that they can be “…really sleepy and…just like go straight to bed” instead of taking their medication. Several caregivers reported fatigue as a barrier to properly administering medication to their adolescents. One caregiver explained, “If he’s gone to bed in his room, if I’m sleepy or tired or whatever, but, from there, have to glance at the cabinet or ‘did you take your medicine?’ So sometimes, I forget too.” Additionally, a few adolescents (6%) reported fatigue as a side effect of their medication. One caregiver reported, “I don’t want him to take it (medication) during homework or anything because it makes him tired.”
Several dyads (24%) described fatigue as an early warning sign that often precedes exacerbation. For example, while explaining what happens before their child has an exacerbation, one caregiver reported, “you can tell he’s about to have one because he start laying around a lot.” Other caregivers used words like “sluggish,” “sleepy,” and “lethargic” to describe their children’s behavior immediately before an exacerbation. In addition, a few dyads (12%) expressed fatigue as a symptom to monitor during an exacerbation. For example, one adolescent reported that their breathing has improved following an exacerbation when they “don’t feel tired” and rather feel “more awake.” Similarly, one caregiver reported fatigue as a sign that their child’s treatment is not working by saying, “if it’s not working her signs she lay around she just she go back to bed.” There appeared to be a consistent pattern in which caregivers monitored their child’s fatigue as a sign of an upcoming exacerbation and/or as an indication of treatment efficacy.
Discussion
The results of this qualitative study demonstrate a relationship between sleep and asthma self-management in adolescents with poorly-controlled asthma. Both adolescents and caregivers reported various asthma-related sleep disturbances. Dyads described some aspects of sleep and sleep disturbances as barriers to components of asthma management (e.g. medication adherence). In general, interview responses from both adolescents and their caregivers demonstrated the importance of sleep and asthma management in adolescents with poorly-controlled asthma. It is clear that sleep disturbances can be a burden for both adolescents and their caregivers.
Previous literature demonstrates a bidirectional relationship between sleep disturbances and asthma control (15,18,19,31). In line with previous research, findings from our study suggest adolescents with poorly-controlled asthma experience sudden nocturnal symptoms throughout the night, which can result in fragmented sleep and poor sleep quality overall. Adolescents and their caregivers also discussed how poor sleep and fatigue can be a barrier to ICS adherence and self-management, which could lead to worse asthma control. Taken together, these findings support a potentially bidirectional process in which poor sleep contributes to poor asthma management and poor asthma management contributes to poor sleep.
Consistent with extant literature, caregivers of adolescents with poorly-controlled asthma described experiencing frequent sleep disturbances and feelings of fear or anxiety regarding their child’s nocturnal asthma (20). Some caregivers made substantial sacrifices to manage their child’s nocturnal asthma. For example, one caregiver reported co-sleeping with her child as a mechanism for symptom monitoring. Although co-sleeping is associated with sleep disruption in school-age children, less is known about the impact of co-sleeping on adolescents (32). Co-sleeping is also more prevalent within certain cultures (33). Previous research suggests a negative relationship between caregiver QOL and youth (children and adolescents) nocturnal asthma symptoms; as youth nocturnal asthma symptoms increase, caregiver QOL tends to decrease (34–36). Caregiver responses from the current study are congruent with previous findings and demonstrate that caregivers can experience a high level of burden associated with their child’s asthma-related sleep disturbances.
Approximately half of dyads described advice they received from medical providers about modifying the adolescent’s sleep environment to avoid triggers and prevent exacerbations. Many of these behaviors were described as part of the family’s permanent routine (e.g. “…her sheets are washed once a week”). Other advice involved avoiding cleaning products, other chemicals, and strong fragrances like perfume. However, it is unclear whether all dyads actually heeded this advice and made environmental accommodations.
In general, adolescents reported fatigue as a normal part of their daily life, but dyads differed in how they interpreted and responded to fatigue. Adolescent reports supported previous literature demonstrating sleepiness as a barrier to medication adherence in youth with asthma (37). This finding is especially critical for the current sample as all participating adolescents were prescribed a daily ICS to help manage their poorly-controlled asthma. Additionally, a few adolescents reported fatigue as a side effect to their ICS which is also supported by extant literature (38,39). Consistent with previous research, several adolescents reported monitoring their fatigue as an early warning sign for exacerbation or indication of the severity of symptoms (2,40).
The impairment in sleep was longstanding for some families; however, dyads generally commented on current sleep-related experiences. On average, caregivers more frequently expressed concern about their adolescent’s nocturnal asthma compared to the adolescents themselves. This finding is consistent with previous literature demonstrating that caregivers tend to exhibit higher rates of anxiety and fear regarding their child’s asthma symptoms compared to youth with asthma (41). Sleep disturbances in both adolescents and their caregivers influenced medication adherence. This finding is concerning considering that medication adherence is one of the most critical aspects of asthma management, especially for adolescents with persistent asthma. In some cases, sleepiness or fatigue was detrimental to the adolescent as it was part of a response to symptoms or a barrier to ICS adherence. However, in other instances, monitoring their fatigue allowed adolescents and caregivers to track worsening asthma symptoms and respond appropriately to manage or prevent impending exacerbations.
We acknowledge that the current study has the following limitations. We used convenience sampling from the same geographic region and all caregivers were female. Therefore, these findings may not be generalizable to adolescents with asthma and their caregivers from more diverse backgrounds. It is possible that some reported nocturnal symptoms could be associated with obstructive sleep apnea (OSA) since youth with poorly-controlled asthma are at increased risk for OSA (42). Although we are unable to distinguish between symptoms associated with asthma versus OSA, both result in sleep difficulties with similar implications for asthma management (43). Additionally, given that this study is based on secondary analysis of data collected for a larger intervention, the interview probes were not tailored to specific sleep and asthma management research questions. While the dyadic nature of the FAMSS interview allows for both child and caregiver perspectives, the presence of a family member could have limited adolescents’ disclosure. Although there was a predetermined sample size of 33 dyads, previous qualitative research suggests that this sample size is appropriate for this study (44,45).
Future quantitative studies should utilize a longitudinal approach to examine the directionality and significance of the relationship between sleep and asthma management in adolescents with poorly-controlled asthma. A more representative sample would allow for greater generalizability and a richer understanding of the role of sleep in asthma. Since the current study did not include sleep-focused interview probes, it is possible that our results underestimate the frequency and significance of asthma-related sleep disturbances. Additionally, this research would benefit from inquiring about daytime symptoms experienced by youth with nocturnal asthma to better understand the downstream consequences of the youth and caregiver reported sleep disturbances. Future research should build off the current literature regarding sleep and pediatric asthma by specifically assessing sleep disturbances as well as how families perceive sleep/fatigue to be related to asthma self-management tasks. Previous research in this area has focused primarily on school age children (46–48). Future research should address this gap in the literature by focusing on adolescent populations.
Despite these limitations, this study makes a contribution to the literature by giving a voice to adolescents with poorly-controlled asthma and their caregivers. Through qualitatively describing the sleep-related experiences of adolescents with asthma and their caregivers, healthcare providers and researchers will have a more in-depth understanding of patient and caregiver perspectives. It is important that providers and researchers understand the sleep difficulties that patients with poorly-controlled asthma and their caregivers may face. Clinicians should screen adolescents with asthma and their caregivers for sleep difficulties and engage families in a discussion of nighttime triggers. Providers might also screen for excessive daytime sleepiness and consider cognitive-behavioral and other behavioral treatments as these are effective in treating various sleep concerns among adolescents (49,50). These discussions and resulting caregiver awareness may help adolescents with poorly-controlled asthma and their caregivers reduce asthma-related sleep disturbances and improve aspects of asthma management.
Funding
This work was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development under Grant R21HD083830.
Footnotes
Declaration of interest
The authors report no conflicts of interest.
References
- 1.Centers for Disease Control and Prevention. Most recent national asthma data. 2020. Available from: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm [last accessed 1 October 2020].
- 2.National Heart, Lung, and Blood Institute. Expert Panel Report 3 (EPR-3): guidelines for the diagnosis and management of asthma-summary report 2007. Available from: https://www.nhlbi.nih.gov/sites/default/files/media/docs/EPR-3_Asthma_Full_Report_2007.pdf [last accessed 1 October 2020].
- 3.Bruzzese J-M, Bonner S, Vincent EJ, Sheares BJ, Mellins RB, Levison MJ, Wiesemann S, Du Y, Zimmerman BJ, Evans D, et al. Asthma education: the adolescent experience. Patient Educ Couns. 2004;55(3):396–406. doi: 10.1016/j.pec.2003.04.009. [DOI] [PubMed] [Google Scholar]
- 4.Mammen J, Rhee H. Adolescent asthma self-management: a concept analysis and operational definition. Pediatr Allergy Immunol Pulmonol. 2012;25(4):180–189. doi: 10.1089/ped.2012.0150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mammen J, Rhee H, Norton SA, Butz AM, Halterman JS, Arcoleo K. An integrated operational definition and conceptual model of asthma self-management in teens. J Asthma. 2018;55(12):1315–1327. doi: 10.1080/02770903.2017.1418888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sullivan PW, Ghushchyan V, Navaratnam P, Friedman HS, Kavati A, Ortiz B, Lanier B. The national burden of poorly controlled asthma, school absence and parental work loss among school-aged children in the United States. J Asthma. 2018;55(6):659–667. doi: 10.1080/02770903.2017.1350972. [DOI] [PubMed] [Google Scholar]
- 7.Vahlkvist S, Pedersen S. Fitness, daily activity and body composition in children with newly diagnosed, untreated asthma. Allergy Eur J Allergy Clin Immunol. 2009;64(11):1649–1655. doi: 10.1111/j.1398-9995.2009.02081.x. [DOI] [PubMed] [Google Scholar]
- 8.Vahlkvist S, Inman MD, Pedersen S. Effect of asthma treatment on fitness, daily activity and body composition in children with asthma. Allergy Eur J Allergy Clin Immunol. 2010;65(11):1464–1471. doi: 10.1111/j.1398-9995.2010.02406.x. [DOI] [PubMed] [Google Scholar]
- 9.Netz M, Fedele DA, Sweenie R, Baker D, Light M, McQuaid EL. Asthma management responsibility, control, and quality of life among emerging adolescents. J Pediatr Psychol. 2020;45(1):40–49. doi: 10.1093/jpepsy/jsz069. [DOI] [PubMed] [Google Scholar]
- 10.Naimi DR, Apter AJ. Adolescents and asthma. In: Harver A, Kotses H, eds. Asthma, health and society. Boston, MA: Springer; 2010. doi: 10.1007/978-0-387-78285-0_12. [DOI] [Google Scholar]
- 11.Carskadon MA. Sleep in adolescents: the perfect storm. Pediatr Clin North Am. 2011;58(3):637–647. doi: 10.1016/j.pcl.2011.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.do Amaral Estanislau NR, Jordão EA, de Azevedo Abreu G, Bloch KV, Kuschnir MC, Felix MM, Kuschnir FC. Association between asthma and sleep hours in Brazilian adolescents: ERICA. J Pediatr. 2020. doi: 10.1016/j.jped.2020.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bakour C, Schwartz SW, Wang W, Sappenfield WM, Couluris M, Chen H, O’Rourke K. Sleep duration patterns from adolescence to young adulthood and the risk of asthma. Ann Epidemiol. 2020;49:20–26. doi: 10.1016/j.annepidem.2020.07.003. [DOI] [PubMed] [Google Scholar]
- 14.Dean BB, Calimlim BC, Sacco P, Aguilar D, Maykut R, Tinkelman D. Uncontrolled asthma among children: impairment in social functioning and sleep. J Asthma. 2010;47(5):539–544. doi: 10.3109/02770900903580868. [DOI] [PubMed] [Google Scholar]
- 15.Lewandowski AS, Ward TM, Palermo TM. Sleep problems in children and adolescents with common medical conditions. Pediatr Clin North Am. 2011;58(3):699–713. doi: 10.1016/j.pcl.2011.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chugh IM, Khanna P, Shah A. Nocturnal symptoms and sleep disturbances in clinically stable asthmatic children. Asian Pacific J Allergy Immunol. 2006;24(2-3):135–142. [PubMed] [Google Scholar]
- 17.Meltzer LJ, Ullrich M, Szefler SJ. Sleep duration, sleep hygiene, and insomnia in adolescents with asthma. J Allergy Clin Immunol Pract. 2014;2(5):562–569. doi: 10.1016/j.jaip.2014.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hanson MD, Chen E. Brief report: the temporal relationships between sleep, cortisol, and lung functioning in youth with asthma. J Pediatr Psychol. 2008;33(3):312–316. doi: 10.1093/jpepsy/jsm120. [DOI] [PubMed] [Google Scholar]
- 19.Luyster FS, Teodorescu M, Bleecker E, Busse W, Calhoun W, Castro M, Chung KF, Erzurum S, Israel E, Strollo PJ, et al. Sleep quality and asthma control and quality of life in non-severe and severe asthma. Sleep Breath. 2012;16(4):1129–1137. doi: 10.1007/s11325-011-0616-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yuksel H, Sogut A, Yilmaz O, Demet M, Ergin D, Kirmaz C. Evaluation of sleep quality and anxiety-depression parameters in asthmatic children and their mothers. Respir Med. 2007;101(12):2550–2554. doi: 10.1016/j.rmed.2007.07.025. [DOI] [PubMed] [Google Scholar]
- 21.Diette GB, Markson L, Skinner EA, Nguyen TTH, Algatt-Bergstrom P, Wu AW . Nocturnal asthma in children affects school attendance, school performance, and parents’ work attendance. Arch Pediatr Adolesc Med. 2000;154(9):923–928. doi: 10.1001/archpedi.154.9.923. [DOI] [PubMed] [Google Scholar]
- 22.Fedele DA, McConville A, Graham Thomas J, McQuaid EL, Janicke DM, Turner EM, Moon J, Abu-Hasan M. Applying interactive mobile health to asthma care in teens (AIM2ACT): development and design of a randomized controlled trial. Contemp Clin Trials. 2018;64:230–237. doi: 10.1016/j.cct.2017.09.007.Applying [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, Murray JJ, Pendergraft TB. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi: 10.1016/j.jaci.2003.09.008. [DOI] [PubMed] [Google Scholar]
- 24.Kosinski M, Nelsen L, Rizio AA, Lay-Flurrie J, von Maltzahn R, Jacques L, Schatz M, Stanford RH, Svedsater H. Psychometric properties of the asthma control test in 2 randomized clinical trials. J Allergy Clin Immunol Pract. 2021;9(1):561–563.e1. doi: 10.1016/j.jaip.2020.07.040. [DOI] [PubMed] [Google Scholar]
- 25.Klinnert MD, McQuaid EL, Gavin LA. Assessing the family asthma management system. J Asthma. 1997;34(1):77–88. doi: 10.3109/02770909709071206. [DOI] [PubMed] [Google Scholar]
- 26.McQuaid EL, Walders N, Kopel SJ, Fritz GK, Klinnert MD. Pediatric asthma management in the family context: the family asthma management system scale. J Pediatr Psychol. 2005;30(6):492–502. doi: 10.1093/jpepsy/jsi074. [DOI] [PubMed] [Google Scholar]
- 27.Ryan GW, Bernard HR. Techniques to identify themes. Field Methods. 2003;15(1):85–109. doi: 10.1177/1525822X02239569. [DOI] [Google Scholar]
- 28.Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi: 10.1093/intqhc/mzm042. [DOI] [PubMed] [Google Scholar]
- 29.Sandelowski M, Barroso J. Classifying the findings in qualitative studies. Qual Health Res. 2003;13(7):905–923. doi: 10.1177/1049732303253488. [DOI] [PubMed] [Google Scholar]
- 30.Wu YP, Thompson D, Aroian KJ, Mcquaid EL, Deatrick JA. Commentary: writing and evaluating qualitative research reports. J Pediatr Psychol. 2016;41(5):493–505. doi: 10.1093/jpepsy/jsw032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Braido F, Baiardini I, Ghiglione V, Fassio O, Bordo A, Cauglia S, Canonica GW. Sleep disturbances and asthma control: a real life study. Asian Pacific J Allergy Immunol. 2009;27(1):27–33. [PubMed] [Google Scholar]
- 32.Cortesi F, Giannotti F, Sebastiani T, Vagnoni C, Marioni P. Cosleeping versus solitary sleeping in children with bedtime problems: child emotional problems and parental distress. Behav Sleep Med. 2008;6(2):89–105. doi: 10.1080/15402000801952922. [DOI] [PubMed] [Google Scholar]
- 33.Airhihenbuwa CO, Iwelunmor JI, Ezepue CJ, Williams NJ, Jean-Louis G. I sleep, because we sleep: a synthesis on the role of culture in sleep behavior research. Sleep Med. 2016;18:67–73. doi: 10.1016/j.sleep.2015.07.020. [DOI] [PubMed] [Google Scholar]
- 34.Fagnano M, Bayer AL, Isensee CA, Hernandez T, Halterman JS. Nocturnal asthma symptoms and poor sleep quality among urban school children with asthma. Acad Pediatr. 2011;11(6):493–499. doi: 10.1016/j.acap.2011.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Vila G, Hayder R, Bertrand C, Falissard B, De Blic J, Mouren-Simeoni M-C, Scheinmann P. Psychopathology and quality of life for adolescents with asthma and their parents. Psychosomatics. 2003;44(4):319–328. doi: 10.1176/appi.psy.44.4.319. [DOI] [PubMed] [Google Scholar]
- 36.Silva CM, Barros L, Simões F. Health-related quality of life in paediatric asthma: childrens and parents perspectives. Psychol Heal Med. 2015;20(8):940–954. doi: 10.1080/13548506.2014.969745. [DOI] [PubMed] [Google Scholar]
- 37.Blaakman SW, Cohen A, Fagnano M, Halterman JS. Asthma medication adherence among urban teens: a qualitative analysis of barriers, facilitators and experiences with school-based care. J Asthma. 2014;51(5):522–529. doi: 10.3109/02770903.2014.885041. [DOI] [PubMed] [Google Scholar]
- 38.Foster JM, Aucott L, van der Werf RHW, van der Meijden MJ, Schraa G, Postma DS, van der Molen T. Higher patient perceived side effects related to higher daily doses of inhaled corticosteroids in the community: a cross-sectional analysis. Respir Med. 2006;100(8): 1318–1336. doi: 10.1016/j.rmed.2005.11.029. [DOI] [PubMed] [Google Scholar]
- 39.Foster JM, Sanderman R, Van Der Molen T, Mueller T, Van Sonderen E. Personality influences the reporting of side effects of inhaled corticosteroids in asthma patients. J Asthma. 2008;45(8):664–669. doi: 10.1080/02770900802127022. [DOI] [PubMed] [Google Scholar]
- 40.Garbutt J, Highstein G, Nelson KA, Rivera-Spoljaric K, Strunk R. Detection and home management of worsening asthma symptoms. Ann Allergy Asthma Immunol. 2009;103(6):469–473. doi: 10.1016/S1081-1206(10)60262-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Callery P, Milnes L, Verduyn C, Couriel J. Qualitative study of young people’s and parents’ beliefs about childhood asthma. Br J Gen Pract. 2003;53(488):185–190. [PMC free article] [PubMed] [Google Scholar]
- 42.Kheirandish-Gozal L, Dayyat EA, Eid NS, Morton RL, Gozal D. Obstructive sleep apnea in poorly controlled asthmatic children: effect of adenotonsillectomy. Pediatr Pulmonol. 2011;46(9):913–918. doi: 10.1002/ppul.21451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kier C, Hom S, Qureshi F. Asthma and sleep. J Asthma Allergy Educ. 2012;3(3):99–105. doi: 10.1177/2150129711427904. [DOI] [Google Scholar]
- 44.Boddy CR. Sample size for qualitative research. QMR. 2016;19(4):426–432. doi: 10.1108/QMR-06-2016-0053. [DOI] [Google Scholar]
- 45.Sandelowski M Sample size in qualitative research. Res Nurs Health. 1995;18(2):179–183. doi: 10.1002/nur.4770180211. [DOI] [PubMed] [Google Scholar]
- 46.Koinis-Mitchell D, Kopel SJ, Seifer R, LeBourgeois M, McQuaid EL, Esteban CA, Boergers J, Nassau J, Farrow M, Fritz GK, et al. Asthma-related lung function, sleep quality, and sleep duration in urban children. Sleep Health. 2017;3(3):148–156. doi: 10.1016/j.sleh.2017.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Martin SR, Boergers J, Kopel SJ, McQuaid EL, Seifer R, LeBourgeois M, Klein RB, Esteban CA, Fritz GK, Koinis-Mitchell D, et al. Sleep hygiene and sleep outcomes in a sample of urban children with and without asthma. J Pediatr Psychol. 2017;42(8):825–836. doi: 10.1093/jpepsy/jsx052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Daniel LC, Boergers J, Kopel SJ, Koinis-Mitchell D. Missed sleep and asthma morbidity in urban children. Ann Allergy Asthma Immunol. 2012;109(1):41–46. doi: 10.1016/j.anai.2012.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Blake MJ, Sheeber LB, Youssef GJ, Raniti MB, Allen NB . Systematic review and meta-analysis of adolescent cognitive-behavioral sleep interventions. Clin Child Fam Psychol Rev. 2017;20(3):227–249. doi: 10.1007/s10567-017-0234-5. [DOI] [PubMed] [Google Scholar]
- 50.Paavonen EJ, Huurre T, Tilli M, Kiviruusu O, Partonen T. Brief behavioral sleep intervention for adolescents: an effectiveness study. Behav Sleep Med. 2016;14(4):351–366. doi: 10.1080/15402002.2015.1007993. [DOI] [PubMed] [Google Scholar]