

Abstract
The Hierarchical Taxonomy of Psychopathology (HiTOP) is a novel diagnostic system grounded in empirical research into the architecture of mental illness. Its basic units are continuous dimensions—as opposed to categories—that are organized into a hierarchy according to patterns of symptom co-occurrence observed in quantitative studies. Previous HiTOP discussions have focused on existing evidence regarding the model’s structure and ability to account for neurobiological, social, cultural, and clinical variation. The present article looks ahead to the next decade of applied research and clinical practice using the HiTOP rubric. We highlight ten topics where HiTOP has the potential to make significant breakthroughs. Research areas include genetic influences, environmental contributions, neural mechanisms, real-time dynamics, and lifespan development of psychopathology. We also discuss development of novel assessments, forecasting methods, and treatments. Finally, we consider implications for clinicians and educators. For each of these domains, we propose directions for future research and venture hypotheses as to what HiTOP will reveal about psychopathology.
Keywords: diagnosis, Diagnostic and Statistical Manual of Mental Disorders (DSM), dimensional models, Hierarchical Taxonomy of Psychopathology (HiTOP)
The purpose of classification systems in science is to organize data and generate hypotheses. In health applications, they guide treatment and provision of services. Classification systems are indispensable, but in the mental health field, they are also contentious. This article describes a new approach to diagnosing mental disorders, and it suggests ways it can be applied to answer significant questions about etiology and treatment.
Traditional taxonomies such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) and International Classification of Diseases (ICD) usually describe mental disorders in terms of categorical diagnoses that are either present or absent. These manuals assume that mental disorders--such as major depression, alcohol use disorder, and schizophrenia--are qualitatively different from one another and from mental health (Krueger et al., 2018). Most areas of scientific inquiry have followed this lead. Academic journals and research foundations are divided according to the diagnostic boundaries drawn by DSM and ICD. Clinicians specialize in treating patients who meet certain diagnostic criteria. Patients use diagnostic labels to make meaning of their difficulties. Moreover, diagnostic boundaries inform public attitudes and discourse about contemporary concerns (e.g., the causes of gun violence, the impact of COVID-19) and existential questions (what is success, happiness?) (Conway et al., 2019).
The categorical conceptualization is not consistent with evidence, given that to date no form of psychopathology has been found to be a discrete class (Haslam et al. 2020; Krueger et al. 2018). Moreover, comorbidity (excessive co-occurrence among putatively distinct diagnoses), heterogeneity (many different ways to qualify for a given diagnosis), and unreliability (across time and raters) make diagnostic categories unwieldy in many settings (Kotov et al., 2017). There is concern that these drawbacks limit the significance and pace of scientific discovery (Gordon & Redish, 2016).
Here we discuss an alternative approach, the Hierarchical Taxonomy of Psychopathology (HiTOP), that aims to overcome such issues (Kotov et al., 2017). It is developed by the HiTOP consortium, an international team of scientists that seeks to organize mental disorders according to consistent evidence in the literature. HiTOP is an empirical classification that assembles constructs identified in quantitative analysis of psychopathology data. The HiTOP approach has intellectual roots in the concept of numerical taxonomy (Sneath & Sokal, 1973), in which classification systems are undergirded by formal statistical models, chosen because they show evidence of structural validity (Loevinger, 1957). That is, models are selected and refined based on their correspondence with available data on empirical associations among psychopathological signs and symptoms. In contrast, many DSM diagnoses are based on assumed coherence--not confirmed by data--among signs and symptoms. For example, posttraumatic stress disorder (PTSD) is comprised of symptoms that are common after trauma rather than because they occur together, and the resulting syndrome is extremely heterogeneous (Galatzer-Levy & Bryant, 2013).
Figure 1 diagrams the HiTOP model, which is a work in progress. At the bottom of the hierarchy, symptom components and maladaptive traits are basic units of mental illness, the most atomistic level of analysis. They represent bundles of the same symptoms that make up DSM categories. For instance, problems with falling asleep, recurrent awakenings, and daytime sleepiness, which often present together, form an insomnia symptom component. The syndrome level represents the tendency for these basic units to co-occur in predictable patterns. Moving up the hierarchy, syndromes coalesce into subfactors and spectra, which, in turn, are components of a general factor of psychopathology (also called the p factor) that represents problems common to all mental health conditions. The lower layer of Figure 1 shows how primary features of specific DSM disorders may relate to the HiTOP structure, with the understanding that these placements are approximate at best, owing to the problems of comorbidity and heterogeneity that are part and parcel of categorical disorders.
Figure 1: HiTOP Working Model.
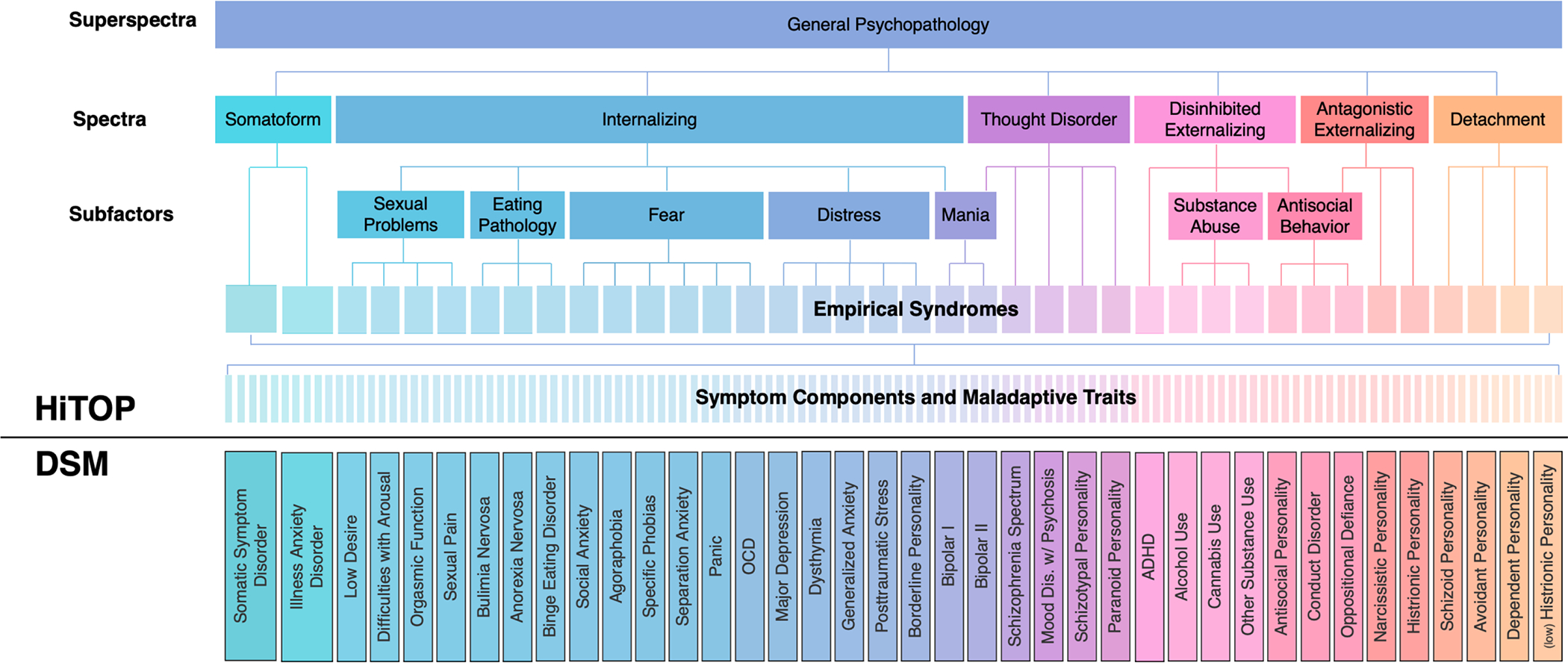
Note. HiTOP working model. Thin vertical lines represent the nested relationship between broader and narrower concepts. DSM diagnoses are not part of the HiTOP model, as reflected in the solid line separating HiTOP from DSM concepts. Still, HiTOP is based on the same signs and symptoms that compose DSM diagnoses, and the color scheme symbolizes where the primary features of DSM disorders are likely to fall in the HiTOP structure. OCD = obsessive-compulsive disorder; ADHD = attention-deficit/hyperactivity disorder.
Two primary features distinguish HiTOP as a research and clinical framework. First, it deals in dimensions, because all available evidence indicates that people differ on mental health problems in terms of degree, not kind. This view destigmatizes mental disorders by emphasizing the fundamental continuity of individual differences in psychopathology. It also marks a departure from the “case-control” design, ubiquitous in health research, which compares people who cross the threshold for a categorical diagnosis (cases) to all those below threshold (controls). This approach artificially splits a continuum into two categories, sacrificing information and reliability of phenotypes (Chmielewski et al., 2005; Markon et al., 2011).
Second, HiTOP is hierarchical. It disentangles more general (higher level) versus narrow (lower level) features of mental illness. Scientists and clinicians can focus on a particular level depending on their goals. For instance, social anxiety could be viewed in terms of avoidance of social situations and physiological arousal (symptom components), or a general tendency to avoid threatening situations (fear subfactor), or a basic predisposition to negative affect (internalizing spectrum) (Figure 1). This structure parallels other hierarchies of individual differences in psychology, such as cognitive ability and personality.
We have outlined the motivation, structure, and validity of HiTOP elsewhere (Kotov et al., 2017, 2020, 2021; Krueger et al., 2021; Watson et al., 2022). The present article pulls together insights from these recent reviews and other scholarship on dimensional nosologies to speculate about HiTOP’s potential to reshape psychological research and practice over the coming years. We identify unanswered questions (and corresponding avenues for future research) and articulate specific hypotheses for investigators to pursue. Table 1 summarizes the different assumptions behind traditional diagnoses and HiTOP, and it lists our predictions of where a HiTOP-based approach to research, practice, and training will lead. We expect that a number of our predictions will be disproven, but that testing them will nevertheless advance our understanding of psychopathology and its treatment.
Table 1.
Differences between HiTOP and traditional diagnoses in assumptions and testable predictions about HiTOP
| Assumptions | |||
|---|---|---|---|
| Area | Traditional diagnosis | HiTOP | Our Prediction |
| Genetics | Each disorder has a distinct and discrete set of genetic vulnerabilities. | Genetic vulnerabilities are continuously distributed throughout population with some risk variants common and others distinct between psychopathology constructs. | 1. HiTOP hierarchical structure will reveal which genetic vulnerabilities are common and which are specific across psychopathology. 2. Refined dimensional phenotypes will increase statistical power of gene discovery studies. |
| Brain-behavior connections | Disorders are the product of specific and discrete neural abnormalities. | Psychopathology is an extreme expression of alterations in biobehavioral systems. Numerous neural alterations contribute cumulatively to graded individual differences in symptoms. | HiTOP’s comprehensive and dimensional approach will reveal: 1. Stronger associations with neural processes than traditional diagnoses. 2. How a process contributes to multiple forms of psychopathology. |
| Development | Disorders are influenced by distinct developmental processes, which produce differences in typical age of onset. | Psychopathology progresses from subclinical to clinical forms in continuous fashion. Different forms of psychopathology are interconnected across the lifespan. | HiTOP framework will: 1. Allow identification of symptoms in early development that are powerful predictors of later full-blown psychopathology. 2. Reveal developmental processes that explain evolution of one form of psychopathology to another. |
| Environment | Environmental exposures affect mental health by increasing risk of one or more discrete disorder. | Exposures contribute in graded fashion to increasing severity of symptoms. Many exposures affect general dimensions, but others have effects on specific dimensions. | HiTOP hierarchy will allow: 1. Delineation of specific environmental risks from general ones. 2. Identification of pathways by which combinations of exposures lead to different forms of psychopathology. |
| Within-person variability | Diagnoses may reflect different patterns of illness course over months or years, but limited to general descriptions such as age of onset and remission status. | Psychopathology constructs are dynamic systems that are sensitive to effects of symptom triggers and daily rhythms. | HiTOP allows measurement of dimensions of interest in real time, which will show that: 1. Symptoms that occur together across people also change together within a person. 2. Variability in a symptom over time is consequential for prognosis and treatment. 3. Future exacerbations can be predicted by a pattern of change in subclinical symptoms. |
| Assessment | Differential diagnosis based on a clinical interview is necessary to accurately assess psychopathology. | Brief self-reports can accurately assess most psychopathology, are highly scalable, and elevated scores can be confirmed by interview when desired. | 1. HiTOP will support development of brief screeners, detailed self-reports, interviews, and digital observational measures. 2. These assessments will provide more explanatory and predictive power than diagnostic interviews for both researchers and clinicians. |
| Clinical decision-making | Diagnostic category forms the basis for much of clinician decision-making. | Forms of psychopathology are dimensions on which multiple ranges can be specified, each tailored to a specific clinical action. | HiTOP will enable development of purpose-made ranges, which will offer better guidance to clinicians and bring mental-health services in line with general medicine. |
| Intervention | Treatments are indicated for specific disorders and their efficacy should be studied for each disorder. | Transdiagnostic interventions are more appropriate due to comorbidity and heterogeneity of disorders. Transdiagnostic treatments target general or specific features of psychopathology instead of individual disorders. | Treatments for general HiTOP dimensions will be more efficient (less time to learn, applicable to more patients) and treatments for specific dimensions will be more effective than disorder-based interventions. |
| Prediction | Presence vs absence of a disorder is optimal for characterizing risk of poor outcomes. | Different outcomes are best predicted by different levels of the HiTOP hierarchy. | 1. Higher-level dimensions will best predict outcomes that span many circumstances. 2. Lower-level dimensions will best predict outcomes limited to specific circumstances. |
| Training | Research knowledge is oriented around categorical diagnoses and clinical training is organized by disorder. | Providers should consider “the whole person,” and trainees benefit from learning transtheoretical principles and interventions that apply across diagnostic categories. | Surveys of learners who have been exposed to HiTOP will show a preference for HiTOP, compared to categorical nosologies, in terms of comprehensiveness, descriptiveness, and ease- of-use. |
1. How can HiTOP help identify genetic contributions to risk for psychopathology?
Most research on psychiatric genetics has taken a cases vs. controls approach to research design in the context of Genome-Wide Association Studies (GWAS) (Smoller, 2019). The frequency of polymorphisms across the genome is compared between cases (e.g., people who meet traditional DSM criteria for a mental disorder) and controls (people who do not meet those criteria). One of the most intriguing discoveries is that there is so much genetic overlap between different disorders (Anttila et al., 2018). If clinical disorders are distinct, why do they appear to arise from a common set of genes, and what sets different disorders apart?
HiTOP can foster genetic discoveries about different mental health problems in three ways. First, the HiTOP structure can help to organize and collectively analyze results from GWASs of different disorders. Such a multivariate strategy has more statistical power, all else equal, than single-disorder analyses to identify novel genetic loci that are common to multiple disorders and to identify loci unique to phenotypically related disorders (e.g., Linnér et al., 2021). Second, HiTOP can spur new discoveries by refining phenotypes. A disorder may be too heterogenous for genetic interrogation. Using HiTOP as a map, researchers can move down the hierarchy to focus on more homogeneous components. A third possibility is to reconsider the use of case-control designs altogether. Rather than stitch together post hoc the genetics of mental disorders by combining GWAS results of discrete disorders studied in different samples, advances could be made by genetically interrogating the entire dimensional structure of psychopathology in the same sample.
Predictions and Recommendations.
Debates about best ways forward in psychiatric genetics center on the choice between larger GWAS sample sizes and depth of phenotyping (Sanchez-Roige & Palmer, 2020), but breadth of phenotyping is often left out of these discussions despite the fact that it offers a necessary route to investigating what is common and what is unique about different mental disorders. Analyses of existing data can address some of this tension by modeling dimensional phenotypes to identify new loci and to characterize specificity of their effects (Waszczuk et al., 2020). But the most powerful solution is carry out genetic discovery in a large population-based study with a full HiTOP assessment; it will identify genetic signatures that unify and distinguish features of different mental health problems at different levels of the hierarchy.
2. Can HiTOP help identify stronger and clearer brain-behavior connections?
Growing evidence suggests that HiTOP phenotyping increases size and specificity of brain-behavior associations. First, studies that compared HiTOP dimensions to DSM diagnoses on neural markers found stronger effects for HiTOP (Martin et al., 2021; Reininghaus et al., 2019). If replicated, this pattern would indicate that dimensions provide more tractable targets for research on neural substrates of psychopathology than traditional categories. Second, the hierarchical organization of HiTOP can aid in resolving brain-behavior links. For example, the hierarchy can help to determine whether a neural process makes general or specific contributions to psychopathology (Kaczkurkin et al., 2019; Karcher et al., 2021). It also can identify neural processes that affect different components of a heterogeneous disorder in opposite directions, and thus are obscured in studies focused on disorders (Kircanski et al., 2018; Weinberg et al., 2016). Third, the available literature suggests that HiTOP spectra map onto basic biobehavioral systems (Michelini et al., 2021). For example, the internalizing spectrum is connected to negative valence systems, disinhibited externalizing to positive valence systems, and antagonistic externalizing to affiliation and attachment processes. The interface between neurobiology and psychopathology is complex, but this cross-walk can facilitate both translation of basic research on biobehavioral systems to clinical applications and development of new animal models for psychopathology (Donaldson & Hen, 2015).
Predictions and Recommendations.
HiTOP phenotyping will reveal stronger brain-behavior links than have been found in research on categorical disorders (Latzman et al., 2020). Moreover, this research will find that some neural processes contribute to many forms of psychopathology (i.e., underpin spectra), others influence a single phenotype, and some others affect multiple phenotypes but in opposite directions.
3. Can HiTOP help understand the development of mental disorders?
Existing classification systems take snapshots of lives, but lives are like a film; they move, shift, and change. A developmental perspective on mental disorders invites new research about continuity and change in psychopathology. We highlight three questions. First, is there a general early-life vulnerability to psychopathology that gives rise to, or differentiates into, increasingly distinct syndromes? Most people who will develop a mental disorder show troubling signs early in life (i.e., by adolescence). Early onset is associated with greater persistence of disorder, greater subsequent diversification of disorders, and reduced likelihood of remission and recovery (Caspi et al., 2020; Kessler et al., 1995; Kim-Cohen et al., 1993). These findings underscore the importance of targeting prevention efforts early in life and raise the question of whether there are key early-life symptoms that portend poor prognosis (McGorry & Hickie, 2019). HiTOP can be used to identify whether and which dimensions act as drivers of illness course.
Second, can developmental information refine classification systems? For example, within the externalizing spectrum, developmental results have highlighted etiological distinctions between adolescence-limited and life-course persistent antisocial behavior and provided an impetus to reform juvenile-justice and mental-health services (Moffitt, 2018). Developmental data have also raised questions about ADHD. Looking backwards, adult-onset ADHD cases have different cognitive and mental-disorder histories than childhood-onset ADHD cases have when followed forward. Are adult-onset and childhood ADHD the same syndromes, and do they merit different treatment approaches (Moffitt et al., 2015)? HiTOP can serve as a guide to answer these developmental questions in a systematic away, by interrogating developmental differences in the same putative syndrome both within and across different levels of the hierarchy.
Third, what gives rise to comorbidity? Most people who have one mental disorder tend to have other co-occurring conditions. For instance, people with a major depressive disorder diagnosis are diagnosed with generalized anxiety disorder at much higher rates than would be expected by chance (e.g., Brown et al., 2001). Moreover, few people retain just one mental disorder over their lives; the more typical pattern is to shift between different disorders (Plana-Ripoll et al., 2019; Caspi et al., 2020). One explanation for these developmental-epidemiological findings is that different conditions have the same causes but are expressed differently depending on environmental (e.g., availability of drugs) or maturational (e.g., physical and cognitive capabilities) opportunities and constraints. An alternative explanation is that causal interactions and reinforcement between symptoms may lead to the emergence of comorbidity over time. If so, higher level dimensions may be products of interactions between many different causes rather than a reflection of shared causes. The HiTOP structure explicitly recognizes comorbidity, but is agnostic about how it emerges. It is best viewed as a phenotypic map against which competing developmental hypotheses can be evaluated.
Predictions and Recommendations.
Every age group has its unique mental health challenges, but all contemporaneous mental disorders are connected to a past and a future. Ultimately, HiTOP will need to inform and be informed by life-course research. Toward this end, measurement development is needed on two fronts. First, longitudinal assessments of the HiTOP structure in the same people followed over time are needed to identify which are the key early-life symptoms that should be treated and ultimately prevented in order to reduce the lifelong burden of mental illness. Second, obtaining accurate lifetime retrospective reports of mental disorders is a priority for research and practice. As we discuss in Section 6, new HiTOP measurement tools are being developed. Because longitudinal measurements are not always feasible, these methods will need to be refined in order to also gather retrospective information too. Such information is needed to understand how different syndromes and their components are linked over time and to support strategic treatment planning in patients’ lives. Developing reliable retrospective measurement tools is an opportunity for collaboration between cognitive scientists, psychopathologists, and clinicians (e.g., Axinn et al., 2020).
4. How does HiTOP help identify environmental contributions to risk for mental illness?
Numerous environmental risks for psychopathology have been identified, yet few—arguably none—appear to be specific etiological markers for any categorical disorder. Stated differently, environmental effects are known to be largely non-specific, akin to genetic pleiotropy. Potent risks, such as childhood abuse/neglect, peer bullying, and crime victimization each predict a wide range of psychological disorders, including anxiety, depression, conduct disorder, psychosis, substance abuse, and eating disorders (Schaefer et al., 2018).
This multifinality, where one exposure confers vulnerability to various categorical disorders, raises the possibility that environmental effects are strongest at higher level dimensions, which encompass diverse syndromes, symptoms, and maladaptive traits. This possibility is testable in the HiTOP framework, but not DSM. Indeed, with HiTOP, investigators can empirically map effects onto a host of dimensional phenotypes, ranging from broad to narrow (Conway et al., 2019). Presumably some exposures will have their biggest impact on higher level phenotypes (e.g., internalizing), whereas others will confer risk primarily for narrow symptom components and maladaptive traits (e.g., social interaction anxiety).
Predictions and Recommendations.
Mapping environmental exposures onto the hierarchy of broad and narrow psychopathology conditions will help to delineate general from specific environmental risks. That is, some environments will have an impact on higher level HiTOP dimensions, whereas others will primarily affect narrower, more specific symptoms and traits. We predict there will be a pattern to these associations, such that higher level dimensions will capture contributions of multifaceted exposures that affect many parts of people’s lives (e.g., poverty), whereas specific symptom components and maladaptive traits will have strongest associations with more limited, circumscribed exposures (e.g., airplane crash, parental criticism of child’s physical appearance). However, we acknowledge that even fairly narrow stressors tend to occur against a backdrop of other acute events and chronic strains (Hammen, 2005), such that homing in on the signal of any such event will be challenging in typical observational research designs.
5. How can HiTOP help understand abnormal behavior in real-time?
Symptom triggers, frequency, duration, and rhythm, are essential to understanding psychopathology. For example, physiological reactivity to trauma reminders is a prototypic symptom of PTSD, and emotional instability is a core feature of borderline personality disorder. These patterns are assessed by asking reporters to recollect past experiences, but such recall is often inaccurate (Schuler et al., 2021; Shiffman, Stone, & Hufford, 2008). Now psychopathology can be tracked in real-time using surveys and passive sensing collected with smartphones (Gillan & Rutledge, 2021). HiTOP dimensions can be measured in real-time more readily than diagnoses (e.g., Wright & Simms, 2016); indeed, diagnoses were not designed to track daily fluctuations.
Real-time monitoring of HiTOP constructs will provide answers to many fundamental questions. First, it is unknown whether psychopathology dimensions observed between people also define a person’s experience over time. For example, one question is whether the internalizing spectrum is temporally coherent—meaning that depression, anxiety, and insomnia tend to occur simultaneously—or if these symptoms usually occur at different times. Second, symptom co-variation over time might reveal novel constructs (Wright & Woods 2020). For instance, anhedonia that accompanies sad mood may be different from anhedonia that is mood-independent. Third, fluctuation of symptoms may predict negative outcomes beyond the symptom mean level. For example, occasional drug binges are more harmful than steady use at moderate levels (Roerecke & Rehm, 2010), but whether this is true for other psychopathology is unclear. Fourth, changes in symptom fluctuation may be warning signs of a coming episode, such as reduced mood variability may predict depression onset (van de Leemput et al., 2014). However, such patterns have not been studied systematically.
Predictions and Recommendations.
HiTOP dimensions will show temporal coherences, meaning that their symptoms will not only occur in the same people, but also will change in concert over time for a given person. However, we expect that additional constructs may emerge from real-time data, defined by covariation of symptoms within a person, even though these symptoms may not typically occur in the same people. A key point in this regard is that technological innovations in real-time symptom monitoring produce extensive data on patterning of symptoms both within and between persons. There are substantial challenges to modeling such intensive longitudinal data, but key methodological developments for detecting temporal patterns in symptom data are already being made (e.g., Lane et al., 2019). The HiTOP approach embraces such opportunities because it is not beholden to traditional categorical psychopathology diagnoses, and instead encourages potential discoveries about how symptoms unfold over finer grained timescales.
We also predict that variability over time will prove clinically useful, so it will be important to monitor not only current levels of HiTOP constructs, but also their variability (i.e., how much they fluctuate around typical level). Moreover, analyses of symptom changes will reveal warning signs of coming exacerbations.
6. How can I assess HiTOP constructs in my research project?
Many HiTOP-conformant measures already exist and are in clinical use (Kotov et al., 2017). The consortium assembled a battery of self-report scales to assess HiTOP in clinical and research applications (https://hitop.unt.edu/clinical-tools/hitop-digital-assessment-and-tracker-hitop-dat). This battery includes 56 dimensions, offers automated administration, requires 45 minutes to complete, and is free to use. A screening version can be completed in 4 minutes. Supporting materials (e.g., billing codes, webinars, and a manual) are available, and the battery is used in a dozen clinics in the US (Jonas et al., 2021). Moreover, the consortium is developing measures based specifically on the HiTOP model (Simms et al., 2020). A self-report inventory will be available for researchers in 2022, followed by clinical tool, a brief screening version, and a semi-structured interview.
Four questions remain for HiTOP measurement. First, this toolkit should be expanded to include psychopathology not currently described in HiTOP (e.g., autism, paraphilias). Second, existing HiTOP-conformant measures are reporter-based. Other modalities should be incorporated into the HiTOP battery. This includes performance-based instruments, such as neuropsychological tests, and observational tools, such as signatures of psychopathology in natural language (Liang et al., 2019). Third, HiTOP instruments have to be adapted to new cultures, as most are available only in English. Fourth, adaptation of measures to certain demographic strata may be needed. Previous research found consistent psychopathology structures across age, gender, race/ethnicity, and sexual orientation (Eaton, 2014; Eaton et al., 2012; He & Li, 2021; McElroy et al., 2018) as well as 24 Western and 25 non-Western societies (Ivanova et al., 2007, 2015, 2019; Krueger et al., 2003). However, only some elements of HiTOP have been tested in these studies.
Predictions and Recommendations.
HiTOP will prove to be a useful target—dimensional, reliable, and scalable—for development of observational instruments. The resulting digital observational HiTOP assessments will augment existing clinical measures and reduce the field’s dependence on reporter-based measures. Moreover, research on the full HiTOP model will reveal that it is largely consistent across societies and demographic groups.
7. Can HiTOP dimensions guide clinical decisions about individual patients?
Although dimensions are highly informative when examining populations, decisions about an individual are usually dichotomous (e.g., to treat or to wait, to hospitalize or not). Consequently, practitioners benefit from explicit ranges on dimensions that indicate a particular clinical action. For example, blood pressure is a continuous score categorized into normal, elevated, stage-1, and stage-2 hypertension to enable clinical actions tailored to a patient’s blood pressure level (Whelton et al., 2018). Lacking ranges validated for a specific action, statistical deviance may serve as a guide to help clinicians interpret scores in reference to the general population. Many medical (Nichols et al., 2007) and psychological tests—such as the Wechsler Intelligence Scale for Adults (Wechsler, 2008) and Minnesota Multiphasic Personality Inventory (Ben-Porath & Tellegen, 2020)—specify cutoffs based on statistical deviance. Following existing conventions, the HiTOP assessment battery currently specifies four ranges: non-clinical (elevation <1.00 SD above general population mean), mild (1.00–1.49 SD), moderate (1.5–1.99 SD), and severe (≥2.00 SD) (Ruggero et al., 2019). These descriptors offer useful heuristics for interpretation of HiTOP profiles.
The consortium’s long-term goal is to develop purpose-made ranges on HiTOP dimensions that can guide specific clinical actions, such as preventive intervention or treatment intensity. These ranges can be set based on probability of a future negative outcome (e.g., where risk of a suicide attempt is sufficiently elevated to require action) or benefits of a given treatment relative to its costs (cf. electroconvulsive therapy for mild versus severe depression; Kellner, Obbels, & Sienaert, 2019).
Predictions and Recommendations.
Purpose-made ranges will prove a useful addition to statistical deviance ranges. Their development will require not only rigorous science but also consensus of stakeholders, including patients and their families, as value judgments are inherent in evaluation of costs and benefits. Medicine offers many successful examples of purpose-made ranges (e.g., Whelton et al., 2018).
8. How can HiTOP reorient intervention efforts?
Most interventions are designed to address a single categorical diagnosis. This produces research inefficiencies. For instance, selective serotonin reuptake inhibitors are efficacious for the internalizing spectrum generally, but have been tested in hundreds of studies to establish efficacy for each internalizing diagnosis (Cipriani et al., 2018; Gosmann et al. 2021). This also creates a mismatch between diagnosis-specific treatments and patients with multiple disorders who are very common in clinical practice (Ruggero et al., 2019). It is often infeasible to address these complaints one at a time; moreover, professionals lack the time needed to master treatment manuals developed for each of the many diagnoses they encounter (Barlow et al., 2014).
Transdiagnostic interventions—treatments that cross DSM boundaries—are attracting attention. The Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders (UP) is a leading example of a psychotherapy directed at a general dimension (Barlow et al., 2014). The UP targets the substrate of HiTOP’s internalizing spectrum (i.e., pathological responses to emotion). Randomized clinical trials show that the UP reduces internalizing symptoms, and it is non-inferior to comparable interventions matched to patients’ primary DSM anxiety or depression diagnosis (Leonardo et al., 2021). Psychotherapy development aimed at other HiTOP spectra is underway (Dalgleish et al., 2020; Hopwood et al., 2020).
Transdiagnostic interventions are not limited to higher-level dimensions (Mullins-Sweatt et al., 2020). Exposure therapies focus on the avoidance tendencies underlying HiTOP’s fear subfactor (relevant to various phobias) (Craske et al., 2014). Sleep restriction therapy addresses insomnia, a narrow component rather than a heterogeneous disorder. Likewise, behavioral activation is often used to treat anhedonia, another narrow dimension (Dimidjian et al., 2011).
Predictions and Recommendations.
Most leading psychotherapies were developed through randomized controlled trials that matched a discrete treatment package to a discrete categorical diagnosis. They were created and marketed with a DSM label in mind. In contrast, there are no “name brand” psychotherapies for HiTOP dimensions. This might be an unfamiliar situation for most clinicians, particularly those who prioritize “empirically supported therapies,” who are used to choosing a therapy protocol with proven effectiveness for a given condition. There are at least two ways forward to integrate psychotherapy research and practice with HiTOP in this context. First, psychotherapy researchers can design and test treatments that are deliberately geared toward HiTOP dimensions. This is the case for the UP, and similar psychotherapy programs are under development (Dalgleish et al., 2020). We speculate that transdiagnostic intervention programs that target higher level HiTOP dimensions will be as effective as diagnosis-based treatments, but easier to disseminate and more acceptable to clinicians.
Second, HiTOP may provide a path toward psychotherapy integration, in which clinicians, operating outside the constraints of diagnosis-specific psychotherapy protocols, are able to draw therapeutic strategies from different theoretical orientations (e.g., cognitive-behavioral, psychodynamic) based on the clinical scenario at hand. There have been a number of attempts to align psychotherapeutic techniques from different therapy schools with HiTOP spectra (Hopwood et al., 2020; Mullins-Sweatt et al., 2020), but these efforts are just beginning. Meanwhile, research on psychotherapy integration has identified transtheoretical principles of change that reflect core clinical strategies that work across psychotherapy schools/orientations (Goldfried, 1980, 2019). Thus, there are parallel developments that challenge the demarcation of diagnostic categories, on the one hand, and psychotherapy schools, on the other. By taking the focus off DSM-based therapy protocols, HiTOP could help shift the conversation to transtheoretical strategies that work for different expressions of psychopathology (see Castonguay et al., 2019).
9. What level of the hierarchy should I use for prediction?
Diagnostic manuals push scientists to focus on syndromes, but HiTOP is more flexible. Investigators can select predictors at any level of Figure 1 based on expected match with the outcome at hand. This match depends on the nature of the outcome (Paunonen, 1998). Typically, more global, multifaceted outcomes (e.g., school failure) correlate strongest with broad individual differences (e.g., externalizing superspectrum, p-factor), whereas less complex outcomes (e.g., managing one’s study time) are traced to narrower traits (e.g., inattention). For example, research finds that the internalizing spectrum predicts mortality (a very complex outcome with manifold causal influences), whereas individual DSM anxiety and depressive diagnoses (e.g., major depressive disorder, panic disorder) contribute little additional predictive utility (Kim et al., 2021).
The key point is that investigators can empirically test—not just assume—which level of breadth conveys the most predictive information for a given outcome (Kotov et al., 2016). This process of discovering where the information, or validity, lies in the hierarchy helps researchers to refine theoretical and predictive models of the causes and consequences of mental illness.
Predictions and Recommendations.
We expect that higher level dimensions will best predict outcomes that span many circumstances, whereas lower-level dimensions will best predict outcomes limited to specific circumstances. For example, well-being is a very general outcome, not tied to any situation; social functioning is somewhat specific, as not all contexts are social; legal problems are fairly narrow; and fear of air travel is very narrow. These outcomes should relate differentially to dimensions at higher vs lower levels of the HiTOP system.
10. What are HiTOP’s implications for training scientists and practitioners?
Today, research training in clinical psychology is anchored to the categorical model of diagnosis. This passes along to trainees an unnecessarily fragmented view of available knowledge of the causes and consequences of psychopathology. It is not unusual to learn about the study of depression in one course and the study of anxiety in another. Separate textbooks, seminar series, and laboratory spaces are delineated by the different DSM categories they address. Yet, as reviewed above, the antecedents of and mechanisms driving these conditions often overlap substantially. HiTOP promotes a more integrative perspective that has the potential to unify research literatures.
By the same token, HiTOP challenges trainees to consider more precise theories of psychopathology. Instead of “a peer rejection account of social anxiety”, “a peer rejection account of generalized anxiety disorder”, and so on, students are encouraged to reflect on ways that peer rejection might influence both higher level dimensions (e.g., fear, distress) and lower level dimensions (e.g., performance anxiety, uncontrollable worry) of psychopathology. This perspective lends itself to more nuanced theory about the causes and nature of mental health conditions (for an example, see Conway et al., 2012).
Categorical divisions are problematic clinically as well. Students often are urged to specialize in treatment of a single disorder as they advance in training programs. This mirrors the physical layout of hospitals, where clinics for, say, PTSD, alcohol use disorder, and eating disorder are housed in different wings of the building. This creates treatment silos, where the patient’s symptoms are viewed through the lens of a single diagnostic construct.
Part of HiTOP’s promise is that it breaks up these silos. It represents a more holistic approach that encourages trainees to consider the “whole person” when making clinical decisions and administering treatment. The HiTOP system provides a richer palette of mental health conditions for trainees than a single diagnosis or small subset of diagnoses that are the focus of many training programs.
This perspective may also open the door to more effective training in case formulation for beginning psychotherapists. Therapists are often trained to match a treatment protocol to a particular categorical diagnosis. Even though traditional diagnoses are very heterogeneous, students learn to approach them with a “one size fits all” protocol (e.g., a manualized cognitive-behavioral therapy for panic disorder) (Boswell et al., 2020). This procedure overlooks potentially important differences between people with the same diagnosis regarding how the condition began, is maintained, and responds to treatment. By taking the focus off the traditional category labels and onto a more comprehensive assessment of specific dimensions of psychopathology, HiTOP could promote more nuanced, person-specific case formulation.
Predictions and Recommendations.
Surveys of learners who have been exposed to HiTOP will show a preference for HiTOP, compared to categorical nosologies, in terms of comprehensiveness, descriptiveness, and ease of use (see, e.g., Morey, Skodol, & Oldham, 2014). Psychotherapy trainees who look beyond the DSM label will adopt a more personalized, flexible approach to case formulation and treatment.
Conclusion
Traditional diagnoses were built on the assumption of discrete boundaries that separate mental disorders from one another and from mental health. This hypothesis puts limitations on the ways psychologists study, assess, treat, and learn about psychopathology (see Table 1).
HiTOP arises from the same basic units of psychopathology found in DSM, but it rearranges these symptoms and maladaptive traits into a hierarchy of dimensional components, in much the same way that cognitive ability and personality domains are structured. Researchers and practitioners can focus on the levels of the hierarchy that match their objectives, as opposed to relying on a traditional syndrome (e.g., social phobia) as the sole unit of analysis. Recent research suggests that this way of diagnosing psychopathology leads to new insights across many psychological subfields (e.g., genetics, neurobiology, intervention science).
This article brings together ideas from recent HiTOP scholarship to propose a research plan for the next decade or so. We outline key questions that we hope will guide this program of research, and we offer our predictions based on available evidence. Whatever the outcome, this research will help to determine whether HiTOP can accelerate efforts to reduce the burden of mental illness.
Public Significance Statement:
The Hierarchical Taxonomy of Psychopathology (HiTOP) is a rubric for diagnosing mental health conditions. Its basic units are dimensions, on which people differ as a matter of degree, not kind, and these dimensions are arranged in a hierarchy such that psychologists can choose the level of breadth that is appropriate for a given research or clinical task. This article maps the frontiers of HiTOP as it relates to science, practice, and training.
Acknowledgments
This work was supported by the National Institute of Mental Health (grant number R01MH122537).
References
- Anttila V, Bulik-Sullivan B, Finucane HK, Walters RK, Bras J,… & Baum L (2018). Analysis of shared heritability in common disorders of the brain. Science, 360(6395). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Axinn WG, Chardoul S, Gatny H, Ghimire DJ, Smoller JW, Zhang Y, & Scott KM (2020). Using life history calendars to improve measurement of lifetime experience with mental disorders. Psychological Medicine, 50(3), 515–522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barlow DH (2000). Unraveling the mysteries of anxiety and its disorders from the perspective of emotion theory. American Psychologist, 55(11), 1247–1263. [DOI] [PubMed] [Google Scholar]
- Barlow DH, Sauer-Zavala S, Carl JR, Bullis JR, & Ellard KK (2014). The nature, diagnosis, and treatment of neuroticism: Back to the future. Clinical Psychological Science, 2(3), 344–365. [Google Scholar]
- Ben-Porath YS, & Tellegen A (2020). Minnesota Multiphasic Personality Inventory-3 (MMPI-3): Technical manual. University of Minnesota Press. [Google Scholar]
- Boswell JF, Constantino MJ, & Goldfried MR (2020). A proposed makeover of psychotherapy training: Contents, methods, and outcomes. Clinical Psychology: Science and Practice, 27(3), Article e12340. [Google Scholar]
- Brown TA, Campbell LA, Lehman CL, Grisham JR, & Mancill RB (2001). Current and lifetime comorbidity of the DSM-IV anxiety and mood disorders in a large clinical sample. Journal of Abnormal Psychology, 110(4), 585. [DOI] [PubMed] [Google Scholar]
- Cai N, Revez JA, Adams MJ, Andlauer TF, Breen G, Byrne EM, . . . Hamilton SP (2020). Minimal phenotyping yields genome-wide association signals of low specificity for major depression. Nature Genetics, 52(4), 437–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspi A, Houts RM, Ambler A, Danese A, Elliott ML, Hariri A, … & Moffitt TE (2020). Longitudinal assessment of mental health disorders and comorbidities across 4 decades among participants in the Dunedin birth cohort study. JAMA Network Open, 3(4), e203221–e203221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Struve M, Whelan R, Banaschewski T, Barker GJ, Bokde AL, … & IMAGEN Consortium. (2014). Neural and cognitive correlates of the common and specific variance across externalizing problems in young adolescence. American Journal of Psychiatry, 171(12), 1310–1319. [DOI] [PubMed] [Google Scholar]
- Castonguay LG, Constantino MJ, & Beutler LE (Eds.). (2019). Principles of change: How psychotherapists implement research in practice. Oxford University Press. [Google Scholar]
- Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, … & Geddes JR (2018). Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Focus, 16(4), 420–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway CC, Forbes MK, Forbush KT, Fried EI, Hallquist MN, Kotov R, … & Eaton NR (2019). A hierarchical taxonomy of psychopathology can transform mental health research. Perspectives on Psychological Science, 14(3), 419–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway CC, Hammen C, & Brennan PA (2012). Expanding stress generation theory: Test of a transdiagnostic model. Journal of Abnormal Psychology, 121, 754–766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craske MG, Treanor M, Conway CC, Zbozinek T, & Vervliet B (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dalgleish T, Black M, Johnston D, & Bevan A (2020). Transdiagnostic approaches to mental health problems: Current status and future directions. Journal of Consulting and Clinical Psychology, 88, 179–195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dimidjian S, Barrera M Jr, Martell C, Muñoz RF, & Lewinsohn PM (2011). The origins and current status of behavioral activation treatments for depression. Annual Review of Clinical Psychology, 7, 1–38. [DOI] [PubMed] [Google Scholar]
- Donaldson ZR, & Hen R (2015). From psychiatric disorders to animal models: a bidirectional and dimensional approach. Biological Psychiatry, 77(1), 15–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eaton NR (2014). Transdiagnostic psychopathology factors and sexual minority mental health: evidence of disparities and associations with minority stressors. Psychology of Sexual Orientation and Gender Diversity, 1, 244–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eaton NR, Keyes KM, Krueger RF, Balsis S, Skodol AE, Markon KE, … & Hasin DS (2012). An invariant dimensional liability model of gender differences in mental disorder prevalence: evidence from a national sample. Journal of Abnormal Psychology, 121(1), 282–288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galatzer-Levy IR, & Bryant RA (2013). 636,120 ways to have posttraumatic stress disorder. Perspectives on Psychological Science, 8(6), 651–662. [DOI] [PubMed] [Google Scholar]
- Gandal MJ, Haney JR, Parikshak NN, Leppa V, Ramaswami G, Hartl C, … & Geschwind DH (2018). Shared molecular neuropathology across major psychiatric disorders parallels polygenic overlap. Science, 359(6376), 693–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillan CM, & Rutledge RB (2021). Smartphones and the neuroscience of mental health. Annual Review of Neuroscience, 44, 129–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldfried MR (1980). Toward the delineation of therapeutic change principles. American Psychologist, 35, 991–999 [DOI] [PubMed] [Google Scholar]
- Goldfried MR (2019). Obtaining consensus in psychotherapy: What holds us back?. American Psychologist, 74, 484–496. [DOI] [PubMed] [Google Scholar]
- Gordon JA, & Redish AD (2016). On the cusp. Current challenges and promises in psychiatry. In Redish AD & Gordon JA (Eds.), Computational psychiatry: New perspectives on mental illness (pp. 3–14). Cambridge, MA: MIT Press. [Google Scholar]
- Gosmann NP, Costa MDA, Jaeger MDB, Motta LS, Frozi J, Spanemberg L, … & Salum GA (2021). Selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors for anxiety, obsessive-compulsive, and stress disorders: A 3-level network meta-analysis. PLoS medicine, 18(6), e1003664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hammen C (2005). Stress and depression. Annual Review of Clinical Psychology, 1, 293–319. [DOI] [PubMed] [Google Scholar]
- Haslam N, McGrath MJ, Viechtbauer W, & Kuppens P (2020). Dimensions over categories: A meta-analysis of taxometric research. Psychological Medicine, 50, 1418–1432. [DOI] [PubMed] [Google Scholar]
- He Q, & Li JJ (2021). Factorial invariance in hierarchical factor models of mental disorders in African American and European American youths. Journal of Child Psychology and Psychiatry, 62(3), 289–298. [DOI] [PubMed] [Google Scholar]
- Hopwood CJ, Bagby RM, Gralnick T, Ro E, Ruggero C, Mullins-Sweatt S, … & Zimmermann J (2020). Integrating psychotherapy with the hierarchical taxonomy of psychopathology (HiTOP). Journal of Psychotherapy Integration, 30, 477–497. [Google Scholar]
- Ivanova MY, Achenbach TM, Dumenci L, Rescorla LA, Almqvist F, Weintraub S, … & Verhulst FC (2007). Testing the 8-syndrome structure of the child behavior checklist in 30 societies. Journal of Clinical Child and Adolescent Psychology, 36(3), 405–417. [DOI] [PubMed] [Google Scholar]
- Ivanova MY, Achenbach TM, Rescorla LA, Turner LV, Árnadóttir HA, Au A, … & Zasępa E (2015). Syndromes of collateral-reported psychopathology for ages 18–59 in 18 societies. International Journal of Clinical and Health Psychology, 15(1), 18–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ivanova MY, Achenbach TM, Rescorla LA, Guo J, Althoff RR, Kan KJ, … & Verhulst FC (2019). Testing syndromes of psychopathology in parent and youth ratings across societies. Journal of Clinical Child & Adolescent Psychology, 48(4), 596–609. [DOI] [PubMed] [Google Scholar]
- Jonas K, Stanton K, Simms L, Mullins-Sweatt S, Gillett D, Dainer E, … Ruggero C (2021, October 5). HiTOP Digital Assessment and Tracker (HiTOP-DAT) Manual. Retrieved from osf.io/8hngd [Google Scholar]
- Kaczkurkin AN, Park SS, Sotiras A, Moore TM, Calkins ME, … & Satterthwaite TD (2019). Evidence for dissociable linkage of dimensions of psychopathology to brain structure in youths. American Journal of Psychiatry, 176, 1000–1009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karcher NR, Michelini G, Kotov R, & Barch DM (2021). Associations between resting-state functional connectivity and a hierarchical dimensional structure of psychopathology in middle childhood. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 6(5), 508–517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kellner CH, Obbels J, & Sienaert P (2019). When to consider electroconvulsive therapy (ECT). Acta Psychiatrica Scandinavica, 141, 304–315. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. [DOI] [PubMed] [Google Scholar]
- Keyes KM, Eaton NR, Krueger RF, McLaughlin KA, Wall MM, Grant BF, & Hasin DS (2012). Childhood maltreatment and the structure of common psychiatric disorders. The British Journal of Psychiatry, 200(2), 107–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim H, Turiano NA, Forbes MK, Kotov R, Krueger RF, Eaton NR, & HiTOP Utility Workgroup. (2021). Internalizing psychopathology and all-cause mortality: A comparison of transdiagnostic vs. diagnosis-based risk prediction. World Psychiatry, 20, 276–282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, & Poulton R (2003). Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort. Archives of General Psychiatry, 60(7), 709–717. [DOI] [PubMed] [Google Scholar]
- Kircanski K, White LK, Tseng WL, Wiggins JL, Frank HR, Sequeira S, … & Brotman MA (2018). A latent variable approach to differentiating neural mechanisms of irritability and anxiety in youth. JAMA Psychiatry, 75(6), 631–639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotov R, Foti D, Li K, Bromet EJ, Hajcak G, & Ruggero CJ (2016). Validating dimensions of psychosis symptomatology: Neural correlates and 20-year outcomes. Journal of abnormal psychology, 125(8), 1103–1119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotov R, Krueger RF, Watson D, Achenbach TM, Althoff RR, Bagby RM, … & Zimmerman M (2017). The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies. Journal of Abnormal Psychology, 126, 454–477. [DOI] [PubMed] [Google Scholar]
- Kotov R, Jonas KG, Carpenter WT, Dretsch MN, Eaton NR, Forbes MK, … & HiTOP Utility Workgroup. (2020). Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): I. Psychosis superspectrum. World Psychiatry, 19(2), 151–172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotov R, Krueger RF, Watson D, Cicero DC, Conway CC, DeYoung CG, … & Wright AG (2021). The Hierarchical Taxonomy of Psychopathology (HiTOP): A quantitative nosology based on consensus of evidence. Annual Review of Clinical Psychology, 17. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Caspi A, Moffitt TE, & Silva PA (1998). The structure and stability of common mental disorders (DSM-III-R): a longitudinal-epidemiological study. Journal of Abnormal Psychology, 107, 216–227. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Chentsova-Dutton YE, Markon KE, Goldberg D, & Ormel J (2003). A cross-cultural study of the structure of comorbidity among common psychopathological syndromes in the general health care setting. Journal of abnormal psychology, 112(3), 437–447. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Hobbs KA, Conway CC, Dick DM, Dretsch MN, Eaton NR, … & HiTOP Utility Workgroup. (2021). Validity and utility of the Hierarchical Taxonomy of Psychopathology (HiTOP): II. Externalizing superspectrum. World Psychiatry, 20, 171–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger RF, Kotov R, Watson D, Forbes MK, Eaton NR, Ruggero CJ, … & Zimmermann J (2018). Progress in achieving quantitative classification of psychopathology. World Psychiatry, 17(3), 282–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Krueger RF, Rathouz PJ, Waldman ID, & Zald DH (2017). A hierarchical causal taxonomy of psychopathology across the life span. Psychological Bulletin, 143(2), 142–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lane ST, Gates KM, Pike HK, Beltz AM, & Wright A (2019). Uncovering general, shared, and unique temporal patterns in ambulatory assessment data. Psychological methods, 24(1), 54–69. 10.1037/met0000192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Latzman RD, DeYoung CG, & HiTOP Neurobiological Foundations Workgroup (2020). Using empirically-derived dimensional phenotypes to accelerate clinical neuroscience: The Hierarchical Taxonomy of Psychopathology (HiTOP) framework. Neuropsychopharmacology, 45(7), 1083–1085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leonardo C, Aristide S, & Michela B (2021). On the efficacy of the Barlow Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: A systematic review and meta-analysis. Clinical Psychology Review, 101999. [DOI] [PubMed] [Google Scholar]
- Liang Y, Zheng X, & Zeng DD (2019). A survey on big data-driven digital phenotyping of mental health. Information Fusion, 52, 290–307. [Google Scholar]
- Linner RK, Mallard TT, Barr PB, Sanchez-Roige S, Madole JW, Driver MN, … & Dick DM (2021). Multivariate genomic analysis of 1.5 million people identifies genes related to addiction, antisocial behavior, and health. Nature Neuroscience, 24, 1367–1376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loevinger J (1957). Objective tests as instruments of psychological theory. Psychological Reports, 3, 635–694. [Google Scholar]
- Mackey S, Allgaier N, Chaarani B, Spechler P, Orr C, … & ENIGMA Addiction Working Group. (2019). Mega-analysis of gray matter volume in substance dependence: general and substance-specific regional effects. American Journal of Psychiatry, 176, 119–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin EA, Jonas KG, Lian W, Foti D, Donaldson KR, Bromet EJ, & Kotov R (2021). Predicting Long-Term Outcomes in First-Admission Psychosis: Does the Hierarchical Taxonomy of Psychopathology Aid DSM in Prognostication? Schizophrenia Bulletin. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McArdle JJ, Ferrer-Caja E, Hamagami F, & Woodcock RW (2002). Comparative longitudinal structural analyses of the growth and decline of multiple intellectual abilities over the life span. Developmental Psychology, 38(1), 115–142. [PubMed] [Google Scholar]
- McElroy E, Belsky J, Carragher N, Fearon P, & Patalay P (2018). Developmental stability of general and specific factors of psychopathology from early childhood to adolescence: dynamic mutualism or p-differentiation?. Journal of Child Psychology and Psychiatry, 59(6), 667–675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGorry PD, & Hickie IB (Eds.). (2019). Clinical Staging in Psychiatry. Cambridge University Press. [Google Scholar]
- McLaughlin KA (2016). Future directions in childhood adversity and youth psychopathology. Journal of Clinical Child & Adolescent Psychology, 45(3), 361–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michelini G, Palumbo IM, DeYoung CG, Latzman RD, & Kotov R (2021). Linking RDoC and HiTOP: A new interface for advancing psychiatric nosology and neuroscience. Clinical Psychology Review, 102025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moffitt TE (2018). Male antisocial behaviour in adolescence and beyond. Nature Human Behaviour, 2, 177–186. [PMC free article] [PubMed] [Google Scholar]
- Moffitt TE, Houts R, Asherson P, Belsky DW, Corcoran DL, Hammerle M, … & Caspi A (2015). Is adult ADHD a childhood-onset neurodevelopmental disorder? Evidence from a four-decade longitudinal cohort study. American Journal of Psychiatry, 172, 967–977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morey LC, Skodol AE, & Oldham JM (2014). Clinician judgments of clinical utility: A comparison of DSM-IV-TR personality disorders and the alternative model for DSM-5 personality disorders. Journal of Abnormal Psychology, 123(2), 398–405. [DOI] [PubMed] [Google Scholar]
- Mullins-Sweatt SN, Hopwood CJ, Chmielewski M, Meyer NA, Min J, Helle AC, & Walgren MD (2020). Treatment of personality pathology through the lens of the hierarchical taxonomy of psychopathology: Developing a research agenda. Personality and Mental Health, 14(1), 123–141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray AL, Eisner M, & Ribeaud D (2016). The development of the general factor of psychopathology ‘p factor’ through childhood and adolescence. Journal of Abnormal Child Psychology, 44(8), 1573–1586 [DOI] [PubMed] [Google Scholar]
- Nichols JH, Christenson RH, Clarke W, Gronowski A, Hammett-Stabler CA, Jacobs E, … & Zucker ML (2007). Executive summary. The National Academy of Clinical Biochemistry Laboratory Medicine Practice Guideline: evidence-based practice for point-of-care testing. Clinica Chimica Acta, 379(1–2), 14–28. [DOI] [PubMed] [Google Scholar]
- Olino TM, Bufferd SJ, Dougherty LR, Dyson MW, Carlson GA, & Klein DN (2018). The development of latent dimensions of psychopathology across early childhood: Stability of dimensions and moderators of change. Journal of Abnormal Child Psychology, 46(7), 1373–1383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paunonen SV (1998). Hierarchical organization of personality and prediction of behavior. Journal of Personality and Social Psychology, 74, 538–556. [Google Scholar]
- Plana-Ripoll O, Pedersen CB, Holtz Y, Benros ME, Dalsgaard S, De Jonge P, … & McGrath JJ (2019). Exploring comorbidity within mental disorders among a Danish national population. JAMA Psychiatry, 76(3), 259–270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plomin R, DeFries JC, Knopik VS, & Neiderhiser JM (2016). Top 10 replicated findings from behavioral genetics. Perspectives on Psychological Science, 11(1), 3–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reininghaus U, Böhnke JR, Chavez-Baldini U, Gibbons R, Ivleva E, Clementz BA, et al. Transdiagnostic dimensions of psychosis in the Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP). World Psychiatry. 2019. Feb;18(1):67–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richmond-Rakerd LS, D’Souza S, Milne BJ, Caspi A, & Moffitt TE (2021). Longitudinal associations of mental disorders with physical diseases and mortality among 2.3 million New Zealand citizens. JAMA Network Open, 4(1), e2033448–e2033448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts BW, Walton KE, & Viechtbauer W (2006). Patterns of mean-level change in personality traits across the life course: a meta-analysis of longitudinal studies. Psychological Bulletin, 132, 1–25. [DOI] [PubMed] [Google Scholar]
- Roerecke M, & Rehm J (2010). Irregular heavy drinking occasions and risk of ischemic heart disease: a systematic review and meta-analysis. American Journal of Epidemiology, 171(6), 633–644. [DOI] [PubMed] [Google Scholar]
- Ruggero CJ, Kotov R, Hopwood CJ, First M, Clark LA, Skodol AE, … & Zimmermann J (2019). Integrating the Hierarchical Taxonomy of Psychopathology (HiTOP) into clinical practice. Journal of consulting and clinical psychology, 87(12), 1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanchez-Roige S, & Palmer AA (2020). Emerging phenotyping strategies will advance our understanding of psychiatric genetics. Nature Neuroscience, 23(4), 475–480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmaal L, Pozzi E, Ho TC, Van Velzen LS, Veer IM, Opel N, … & Veltman DJ (2020). ENIGMA MDD: seven years of global neuroimaging studies of major depression through worldwide data sharing. Translational psychiatry, 10(1), 1–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuler K, Ruggero CJ, Mahaffey B, Gonzalez A, Callahan L, J., Boals A, … & Kotov R (2021). When hindsight is not 20/20: ecological momentary assessment of PTSD symptoms versus retrospective report. Assessment, 28(1), 238–247. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Stone AA, & Hufford MR (2008). Ecological momentary assessment. Annual review of clinical psychology, 4, 1–32. [DOI] [PubMed] [Google Scholar]
- Simms LJ, Wright AG, Cicero D, Kotov R, Mullins-Sweatt SN, Sellbom M, … & Zimmermann J (2022). Development of measures for the Hierarchical Taxonomy of Psychopathology (HiTOP): a collaborative scale development project. Assessment, 10731911211015309. [DOI] [PubMed] [Google Scholar]
- Smoller JW (2019). Psychiatric genetics begins to find its footing. American Journal of Psychiatry, 176(8), 609–614. [DOI] [PubMed] [Google Scholar]
- Sneath PH & Sokal RR (1973). Numerical Taxonomy: The Principles and Practice of Numerical Classification. 1st Edition, W. H. Freeman, San Francisco. [Google Scholar]
- van de Leemput IA, Wichers M, Cramer AO, Borsboom D, Tuerlinckx F, Kuppens P, … & Scheffer M (2014). Critical slowing down as early warning for the onset and termination of depression. Proceedings of the National Academy of Sciences, 111(1), 87–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Venables NC, Foell J, Yancey JR, Kane MJ, Engle RW, Patrick CJ. Quantifying Inhibitory Control as Externalizing Proneness: A Cross-Domain Model. Clinical Psychological Science. 2018. Jul;6(4):561–80. [Google Scholar]
- Waszczuk MA, Eaton NR, Krueger RF, Shackman AJ, Waldman ID, Zald DH, … & Kotov R (2020). Redefining phenotypes to advance psychiatric genetics: Implications from hierarchical taxonomy of psychopathology. Journal of Abnormal Psychology, 129, 143–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waszczuk MA, Miao J, Docherty AR, Shabalin AA, Jonas KG, Michelini G, & Kotov R (2021). General v. specific vulnerabilities: Polygenic risk scores and higher-order psychopathology dimensions in the Adolescent Brain Cognitive Development (ABCD) Study. Psychological Medicine, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, Levin-Aspenson HF, Waszczuk MA, Conway CC, Dalgleish T, Dretsch MN, … & HiTOP Utility Workgroup. (2022). Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): III. Emotional dysfunction superspectrum. World Psychiatry, 21, 26–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler D (2008). Wechsler Adult Intelligence Scale (4th ed.). San Antonio, TX: NCS Pearson Inc. [Google Scholar]
- Weinberg A, Meyer A, Hale-Rude E, Perlman G, Kotov R, Klein DN, & Hajcak G (2016). Error-related negativity (ERN) and sustained threat: Conceptual framework and empirical evaluation in an adolescent sample. Psychophysiology, 53(3), 372–385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C, … & Wright JT (2018). 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology, 71(19), e127–e248. [DOI] [PubMed] [Google Scholar]
- Widiger TA, Sellbom M, Chmielewski M, Clark LA, DeYoung CG, Kotov R, … & Wright AG (2019). Personality in a hierarchical model of psychopathology. Clinical Psychological Science, 7(1), 77–92. [Google Scholar]
- Wright AG, & Simms LJ (2016). Stability and fluctuation of personality disorder features in daily life. Journal of Abnormal Psychology, 125(5), 641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright AG, & Woods WC (2020). Personalized models of psychopathology. Annual Review of Clinical Psychology, 16, 49–74. [DOI] [PubMed] [Google Scholar]