

Abstract
Background
Sexual orientation is usually developed during the adolescence, which coincides with the eating disorders peak onset. This paper aims to explore existing literature to identify whether there is an association between sexual orientation and eating disorder‐related eating behaviours (EDrEBs) in this age‐group.
Methods
This review was based on the PRISMA guidelines, covering the published articles between 1990 and 2021. A meta‐analysis of the proportion of sexual orientation and the adjusted odds ratio (OR) with 95% confident intervals was reported.
Results
Ten studies (412,601 participants) were included in this review. The results demonstrated adolescents identified as minority sexual orientation, particularly homosexual males were with higher OR of EDrEBs, as follows: Homosexual (binge eating: M = 7.20, F = 2.14; purging: M = 5.40, F = 2.41; diet pills use: M = 3.50, F = 2.59; dieting: M = 3.10, F = 1.75); Bisexual (binge eating: M = 4.60, F = 2.26; purging: M = 4.44, F = 2.37; diet pills use: M = 3.42, F = 2.30; dieting: M = 2.36, F = 1.86).
Conclusions
Adolescents who were of a minority sexual orientation were more vulnerable to EDrEBs than their heterosexual peers. Healthcare professionals and sexual minority communities should be primed to facilitate earlier recognition and access to services in these vulnerable groups.
Keywords: adolescents, binge eating, diet pill use, dieting, eating behavior, eating disorder, meta analysis, purging, sexual minorities, sexual orientation
Key points
Adolescents who were of a minority sexual orientation were more vulnerable to eating disorder‐related eating behaviours (EDrEBs) than their heterosexual peers.
Although this higher vulnerability applies to both sexes, sexual minority (SMin) adolescent males appear to have higher ORs than their SMin female counterparts in comparison to their respective reference heterosexual group.
The highest odds ratio (OR) for EDrEBs, i.e. binge eating, purging, diet pill use, was been observed in homosexual males.
Abbreviations
- CI
confident interval
- EDs
eating disorders
- EDrEBs
eating disorder‐related eating behaviours
- F
Female
- M
Male
- NOS
Newcastle Ottawa Scale
- OR
odds ratio
- RevMan
Review Manager (ccochrane’s bespoke software)
- SMin
sexual minority
1. INTRODUCTION
1.1. Rationale
Eating disorders (EDs) are mental illnesses characterised by disturbances in eating behaviours, and associated thoughts and emotions (APA & APIR, 2013). They could present with an intense preoccupation with body weight or shape (Fairburn & Harrison, 2003; Field et al., 2012) that was either vocalised or acted on. Eating disorders have the highest mortality and morbidity rate among psychological disorders (Lozano et al., 2012). The most common symptoms include food restriction, binging, purging (which includes vomiting, laxative use and use of diet pills) and over‐exercise. Therefore, ED‐related eating behaviours (EDrEBs) were focussed on in this review. The following definitions were used for this article:
Dieting: a persistent behaviour aiming to reduce energy intake using various methods, such as decreasing portion size or skipping meals, aiming to control weight gain or achieve weight loss, and food restriction. This is also considered similar to fasting, for the scope of this review.
Purging: a compensatory behaviour following the ingestion of food that includes self‐induced vomiting and laxative misuse.
Binge eating: the over‐consumption of a large amount of food in a short period, associated with loss of self‐control during eating and subsequent feelings of guilt (Fairburn & Beglin, 1994; Klingenspor, 2002).
Diet pills use: use pills or drugs to lose or control weight during the last 30 days (Watson et al., 2017).
A recent review (Parker & Harriger, 2020) illustrate that SMin may experience a greater incidence of EDrEB than their heterosexual and cisgender counterparts, for both adults and adolescents. Shearer et al. (2015) studied adolescents and young adults as subjects ranging from 14 to 24 and demonstrated that homosexual and bisexual males and bisexual females had an increased risk for disordered eating symptoms. Gigi et al. (2016) showed that bisexual adult males have higher reported levels of disordered eating and body dissatisfaction than heterosexual adult males. The association between sexual orientation and EDs has been mainly explored in adults, but less in adolescents.
Sexual orientation was described as how people are sexually attracted to others, literally considered as a continuum from ‘exclusive attraction to the opposite sex’ to ‘exclusive attraction to the same sex on the other’ (Ellis et al., 1987). This was different to gender identity, which was a more complicated concept as it involves both private and public components regarding how one presents oneself to themselves and others (Bailey et al., 2016). Heterosexuality and homosexuality are located at two opposing ends of the spectrum, whilst bisexuality usually slides between them. Sexual orientation develops during puberty (Ott et al., 2011), with the average age of realizing sexual attraction being about 10 years old (Herdt & McClintock, 2000) and recognition of minority sexual orientation being estimated between the ages of 14–21 years (Ettinger, 2004). The fluidity of sexual orientation cannot be ignored during adolescence (Diamond, 2016; Srivastava et al., 2022). In this review, information about sexual orientation was self‐reported by the participants in the studies that were included in this review and reflected the participant's self‐identity at that time. The ‘heterosexual’ was used as the reference group as this constitutes the sexual majority at the time of writing. Also note, only the cisgender population would be included in this study and discussion. The controversy about transgender and related gender identity was acknowledged by authors and confirmed that beyond the scope.
The authors acknowledge the complexity of explaining human sexual behaviours and identities and the sensitivity with which this needs to be carried out. It was felt that any extended exploration of definitions was beyond the scope of this paper, and it was agreed to adopt the definitions and use of language from the literature reviewed unless this was felt to be discriminatory or suggestive of negative connotations.
2. OBJECTIVES
Most studies have investigated EDrEBs among the adult population, but less was known about the adolescent period and their transition to adulthood, an important period of individual growth and development. Notably, EDs may occur at any age but are known to peak around 15–19 years of age (Micali et al., 2013). Previous research has confirmed that sexuality plays a role in EDs symptomatology (Cella et al., 2013). This study systematically reviews and evaluates published literature on the relationship between EDrEBs and sexual orientation among adolescents.
3. METHODS
This study was designed according to the PRISMA guidelines (Page et al., 2021).
3.1. Eligibility criteria
Inclusion and exclusion criteria for the study selection are outlined in Table 1.
TABLE 1.
Study selection eligibility criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
3.2. Information sources
The electronic literature resources used to identify the studies for this article were Web of Science, PubMed and Medline by Ovid Version, and PsycInfo (search date 01.03.2019 for initial search by ZC and DP, with a later search for any updates conducted by ZC on 31.03.2021). The reference section of identified articles was reviewed to ensure that no other relevant articles were missed.
3.3. Search strategy
The following terms were used for this search, with the Boolean operator ‘AND’. The term ‘sexual orientation’ was related to either ‘homosexual’ OR ‘non‐heterosexual’ OR ‘gender minority’ OR ‘SMin populations’ OR ‘sexual minorities’ OR ‘lesbian, gay, bisexual’ OR ‘bisexuality’ OR ‘homosexuality’. The term ‘EDs symptoms’ was related with either ‘feeding and EDs’ OR ‘anorexia nervosa’ OR ‘bulimia nervosa’ OR ‘binge ED’ OR ‘disordered eating’ OR ‘eating behaviours’ OR ‘eating pathology’. The search included articles from January 1990 to March 2021. We chose to start the search from January 1990 as the interest in sexual orientation started around that time with a referent paper (Ellis et al., 1987).
3.4. Study selections process
1044 publications were identified from the database search. No unpublished relevant studies were obtained. Authors ZC and DP jointly screened these and removed duplicate articles. Any disputes on the eligibility of the articles were initially discussed between the two independent reviewers (ZC, DP) and any unresolved disputes were discussed with the wider team (EC, KC). Of the remaining 590 articles, 527 papers were further excluded after the screening of the investigated population, and a further 53 were excluded with exclusion criteria, leaving 10 eligible for inclusion in the qualitative review (Figure 1). Finally, 10 papers were included in the meta‐analysis. Two reviewers (ZC, DP) performed the eligibility assessment. Data extraction was triple checked.
FIGURE 1.
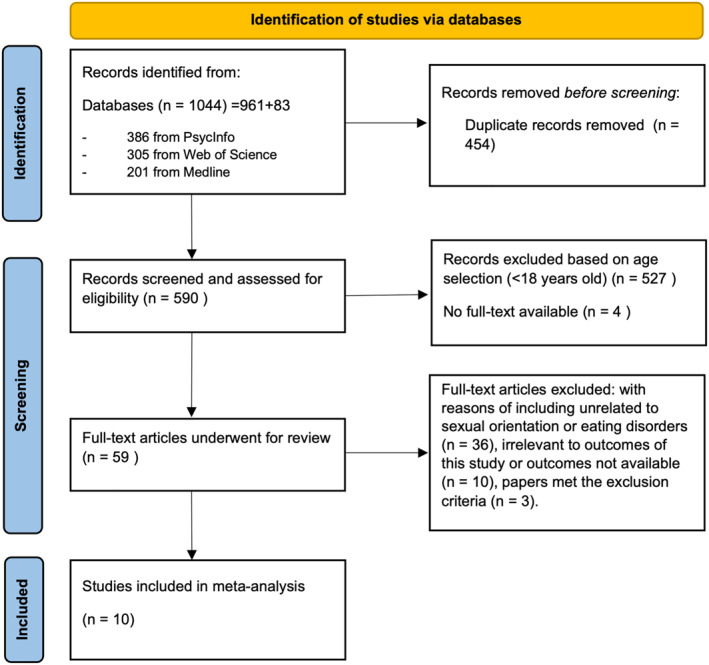
Flow diagram for the selection of studies on sexual orientation in adolescents
3.5. Data collection process
Data were extracted from the selected articles based on the inclusion and exclusion criteria, using the PRISMA guideline for quantitative research (Page et al., 2021). Unpublished data were not sought. Endnote was used to manage the studies and the whole assessment. RevMan was used to analyse the data and to produce forest and funnel plots.
3.6. Data items
The information extracted included:
Characteristics of study participants, including country, type, sample size, age, biological sex and sexual orientation, and data resources;
-
Outcome measures included:
Proportion of participants' sexual orientation identity;
ORs of ED symptoms in each subgroup for different sexual orientation identities.
3.7. Risk of bias in individual studies
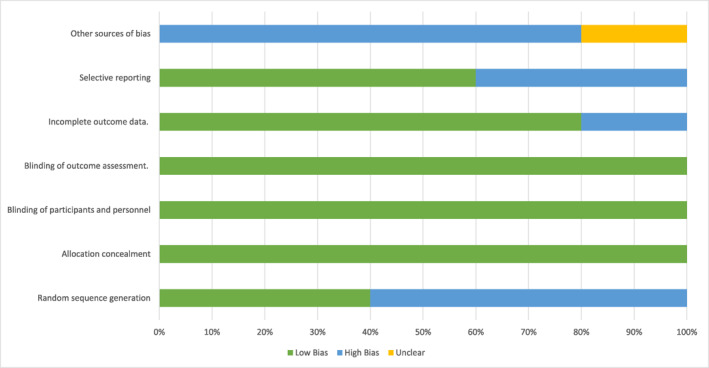
This review used a component approach to assess the risk of bias. The Cochrane ‘Risk of Bias’ tool (Table 2) was used to assess risk in individual studies (Moher et al., 2009). This tool comprises five domains: selection, performance, attrition, reporting and other bias. Each type of bias was assessed as ‘unclear’, ‘low’, or ‘high’, according to criteria indicated in the PRISMA guidelines (Page et al., 2021). For the determination of the validity of eligible studies, the reviewer ZC worked independently, to examine the adequacy of sample representation, blinding of methods and assessment, and the extent of loss to follow‐up.
TABLE 2.
The Cochrane ‘Risk of Bias’ table for the review
|
3.8. Effect measures
Measured outcome was extracted from included studies in the form of:
ORs of EDrEBs, including dieting, purging, using diet pills, and binge eating;
The sexual orientation stratified comparison of ORs;
The biological sex stratified comparison of ORs among SMin.
The relationship between the distribution of sexual orientation and the OR of EDrEBs was the primary outcome. The results were sex‐stratified. Self‐reported body image and dissatisfaction, the self‐assessment of body maturation, and weight concern were listed as secondary outcomes. In some papers, sexual attraction and relationship status were treated as additional outcomes.
3.9. Synthesis of result
Following the assessment of methodological quality, papers were grouped according to whether they were quantitative, qualitative or opinion‐based. Qualitative research data were extracted using the Newcastle Ottawa Scale (NOS). The GRADE table was then used to assess the quality of evidence (Guyatt et al., 2008a, 2008b).
Studies that included quantitative data were analysed further and the adjusted OR with 95% confident intervals (CI) for sexual orientation and EDs symptoms were determined. The distribution of OR in the studies reviewed were illustrated through forest plots and were sex‐stratified for the various sexual orientation. Subgroup analysis was used to illustrate the differences between diverse sexual orientation. Quantitative analyses were divided into 3 main categories: (1) heterosexual as the referent group; (2) homosexual subgroup; and (3) bisexual. Some papers also examined the fourth, ‘mostly heterosexual’, subgroup. Each subgroup was stratified as female and male individuals.
3.10. Planned methods of analysis
Statistical analysis was completed by the RevMan and Excel. The effect size was subjected to a random effects model. Heterogeneity was measured by the RevMan and expressed as the degree of inconsistency or I 2. Sensitivity analyses were pre‐specified. The outcome effects were tested according to quality components, such as allocation concealment, blinding of participants and personnel and blinding of outcome assessment.
3.11. Risk of bias across studies
The risk of publication bias was assessed using the funnel plot asymmetry evaluation. Each forest plot was made by the log OR of its standard error.
3.12. Confidence in cumulative evidence
As a systematic review, this study was able to avoid some, but not all, potential biases. For instance, when selecting studies for review, the authors of the selected articles were masked to allow the reviewer ZC to evaluate the articles in their own right based on the completeness of results. The authors acknowledge that there was evidence of publication bias in this systematic review as grey literature was not included. Attention was paid to the risk of other sources of bias including the heterogeneity of the studies and selective reporting bias occurring as a result of the extraction of data from the title and abstract of papers.
4. RESULTS
4.1. Study selection
Only 63 articles met the full eligibility criteria of this systematic review from the outset. A further 27 articles contained information on adolescents' sexual orientation and EDrEBs. Of these, 10 articles allowed for data extraction for the adolescent group (see PRISMA diagram for details as to how these were chosen). Therefore, the total sample size included in this systematic review was 10. Apart from Calzo et al. (2015) which only included male participants (Figure 2), the rest of the included studies contained adolescent girls and boys, 52.69% and 47.31% respectively. From the 10 studies included in this systematic review, approximately 88.07% (80.7%–94.9%) of the sample identified as heterosexual whilst 6.78% (0.97%–10.8%) identified as either homosexual or bisexual.
FIGURE 2.

Biological Sex Distribution among the Included Studies
4.2. Study characteristics
As shown in Figure 1, a total of 10 studies involving 495,818 participants (analytic sample for review n = 412,601) were identified for inclusion in this review. The mean age for the analytic sample was 15.3 years (SD = 3.55).
The characteristics of these included studies were reported in detail in Table 3. Only one paper (Calzo et al., 2015) solely examined the OR of EDrEBs in the adolescent male group (Figure 2). In most studies, sexual orientation was categorised as ‘heterosexual’, ‘bisexual’, ‘homosexual’ and ‘unsure’. However, Yu et al. (2018) reviewed ED symptoms in relation to ‘sexual partner’ choice (Figure 2). In this review, those sexual orientation that were expressed as ‘mostly heterosexual’ or as ‘unsure’ were not included in SMin group. Not all EDrEBs were explored in all of the 10 papers, with some exploring some of these EDrEDs (Figure 3). Therefore, the data related to each EDrEB in each study was collected and extracted and analysed quantitatively.
TABLE 3.
Summary of the characteristics of 10 included studies in this review
| Authors and year of publication | Country | Type of study | Total no. of patients | No. of patients included in review | Age | Gender | Sexual orientation | Data resource | Summary of results |
|---|---|---|---|---|---|---|---|---|---|
| Austin, 2004 | US | Cohort | 10,583 | 9817 | Aged 12–17 |
|
|
GUTS 1999 |
Mostly heterosexual girls and boys are a newly identified group at increased risk of eating disorder symptoms. Gay/bisexual boys were also at increased risk. |
| Austin, 2009 | US | Cohort | 13,795 | 13,795 | Aged 12–18 |
|
|
GUTS 1998/1999/2000/2001/2003/2005 |
The risk of eating disordered behaviours in homosexual, bisexual, mostly heterosexual subgroup exist and need to be paid attention. |
| Austin, 2013 | US | Cohort | 24,591 | 24,591 |
|
|
|
YRBSS 2005/2007 |
LGB youths for diverse ethnicities may need interventions for reduce eating disorders and obesity. |
| Calzo, 2015 | US | Cohort | 9652 | 5623 | Aged 15–18 | Male |
|
GUTS |
Sexual minority males (i.e., mostly heterosexual, gay, and bisexual) were more likely than completely heterosexual males to be lean‐concerned at ages 17–18. |
| Calzo, 2018 | UK | Cohort | 5048 | 5048 | Age = 14; Age = 16 |
|
|
ALSPAC |
By mid‐adolescence, sexual minority youth in the UK had elevated risk for eating disorder symptoms, suggesting the need for early prevention efforts. |
| Calzo, 2019 | US | Cohort | 322,687 | 308,569 | Aged 14–17 |
|
|
YRBS 2009–2015 |
Odds of fasting increased with greater frequency of monthly binge drinking among heterosexual adolescent female youth, and odds of diet pill use increased with greater frequency of monthly binge drinking among heterosexual adolescent male youth. Disordered eating behaviour prevalence was particularly pronounced among adolescents who binge drank and who were not sure of their sexual orientation identity. |
| Katz‐Wise, 2014 | US | Cohort | 13,952 | 13,952 | Aged 9–14 |
|
|
GUTS 1996 |
Sexual orientation differences in BMI were partly explained by child abuse and weight‐related behaviours in females. |
| Watson, 2017 | Canada | Cross‐sectional survey | 26,002 | 26,002 | Aged 12–18 |
|
|
YRBS 1999/2001/2003/2005/2007/2009/2011/2013 |
The prevalence of disordered eating among youth has significant decrease, but the disparities remain. |
| Yu, 2018 | South Korea | Cohort | 67266 | 3044 | Aged 12‐18 |
|
|
K_CDC questionnaire | Those reporting partners of both sexes had higher odds and those with no sexual partners had lower odds of disordered weight control behaviors. Those with same‐sex partners only were not significantly different in disordered weight control behaviors from those with other‐sex partners only for girls or boys. |
| Zullig, 2017 | US | Cohort | 2242 | 2,60 |
|
|
|
YRBS 2013 | High school‐aged sexual minority youth subgroups are a priority target population for increased efforts to prevent disordered eating. |
FIGURE 3.
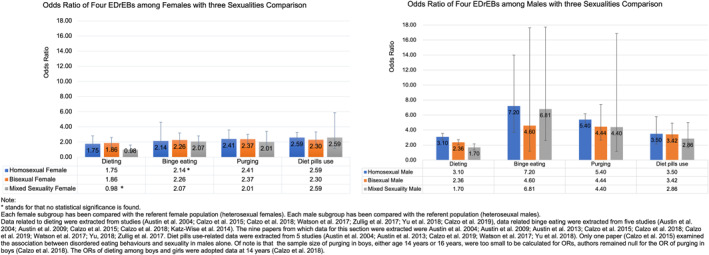
OR of four EDrEBs among three sexualities comparison stratified by biological sex
The majority of included papers used OR of diverse EDrEBs in different sexual orientation as the primary outcome. This review summarises 3 sexual orientation sub‐groups (i.e. (1) homosexuality, (2) bisexuality, (3) mixed sexuality for comparison. All the subtypes were discussed with the sex‐stratified structure. All the OR uses heterosexuality data as referent and for cases where this was sub‐divided into ‘mostly’ or ‘completely’ heterosexual groups, the ‘completely heterosexual’ category was then chosen as the referent group.
4.3. Risk of bias in studies
Table 4 (GRADE table) highlights the assessment of the risk of bias within the studies.
TABLE 4.
The grade table for included studies
| Study | Original | Rate down ↓ | Rate up ↑ | Sum quality of evidence | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Risk of bias | Imprecision | Inconsistency | Indirectness | Publication bias | Large magnitude of effect | Dose‐response gradient | Residual confounding | |||
| Austin et al., 2004 | Low | −1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | Low |
| Austin et al., 2009 | Low | −1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | Low |
| Austin et al., 2013 | Low | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | High |
| Calzo et al., 2015 | Low | −1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | Moderate |
| Calzo et al., 2018 | Low | −1 | −1 | 0 | 0 | 0 | 0 | 0 | 1 | Very low |
| Calzo et al., 2019 | Low | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | High |
| Katz‐Wise et al., 2014 | Low | −1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | Low |
| Watson et al., 2017 | Low | −1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | Low |
| Yu et al., 2018 | Low | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | High |
| Zullig et al., 2017 | Low | −1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | Moderate |
Note: Positive mark before the number stands for rating up, negative mark before the number stands for rating down. The number after positive or negative marks represents the extent of seriousness, 1 for serious, 2 for very serious. And, 0 stands for the no up in these rate‐up items, also no down in these rate‐down items. In the summary part, the ‘high quality’ stands for that further research is very unlikely to change our confidence in the estimate of effect; ‘moderate’ is that further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate; ‘low’ is that further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate; ‘very low’ indicates that any estimate of effect is very uncertain.
4.4. Risk of bias across studies
The risk of bias across studies was assessed using the NOS table. Eight of the included papers were rated as ‘good’ with an overall mean quality score of 7 stars out of 9 (Table 5). Austin et al. (2013) and Calzo et al. (2018) had the highest ratings with 8 out of possible 9 stars—the loss of a star being due to the use of self‐reported selection methodology in the ascertainment of exposure. Two papers (Austin et al., 2009; Calzo et al., 2015) were rated as fair, with a score of 6 out of a total of 9.
TABLE 5.
The Newcastle Ottawa Scale (NOS) table for included studies
| Study (author and publication of year) | Selection | Comparability | Outcome | Summary | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the exposed cohort | Selection of the non‐exposed cohort | Ascertainment of exposure | Demonstration that outcome of interest was not present at the start of study | Comparability of cohorts on the basis of the design or analysis controlled for confounders | Assessment of outcome | Was follow‐up long enough for outcomes to occur | Adequacy of follow‐up of cohorts | Total amount of stars/9 | The quality of evidence | |
| Austin, et al., 2004 | c) | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | b) ★ | 7 | Good |
| Austin, et al., 2009 | c) | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | c) | 6 | Fair |
| Austin, et al., 2013 | b) ★ | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | b) ★ | 8 | Good |
| Calzo, et al., 2015 | c) | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | c) | 6 | Fair |
| Calzo, et al., 2018 | b) ★ | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | b) ★ | 8 | Good |
| Calzo, 2019 | b) ★ | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | c) | 7 | Good |
| Katz‐Wise, 2014 | c) | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | b) ★ | 7 | Good |
| Watson, et al., 2017 | b) ★ | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | a) ★ | c) | 7 | Good |
| Yu, 2018 | b) ★ | a) ★ | c) | a) ★ | a) ★; b) ★ | a) ★ | b) | b) ★ | 7 | Good |
| Zullig, et al., 2017 | b) ★ | a) ★ | c) | a) ★ | a) ★; b) ★ | b) ★ | b) | b) ★ | 7 | Good |
4.5. Results of syntheses
Sex‐stratified analysis was adopted in this review. Each sexual orientation sub‐group was analysed using the forest plot using the random effect model and OR illustrating with 95% CI (Figure 4, 5, 6). The results are discussed below and are presented based on the stratified sexual orientation and these were stratified as follows:
Homosexual group: participants who identified themselves as homosexual.
Bisexual group: participants who identified themselves as bisexual.
Mixed sexuality group: participants who identified themselves as either homosexuals or bisexuals and their sexual orientation is fluid in this context.
FIGURE 4.
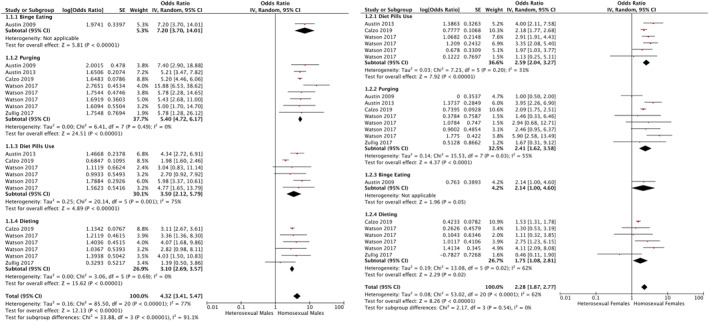
Forest Plot of the ORs of four EDrEBs among the homosexuality stratified by biological sex
FIGURE 5.
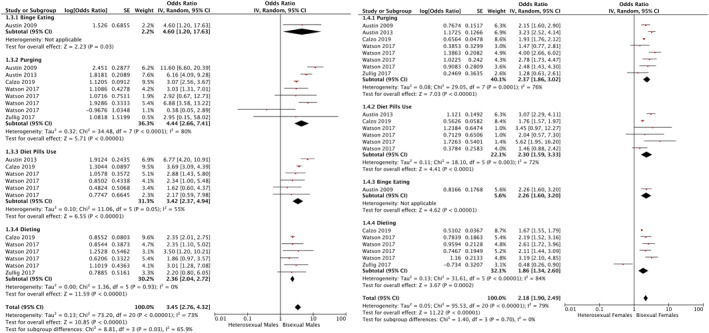
Forest Plot of the ORs of four EDrEBs among the bisexuality stratified by biological sex
FIGURE 6.
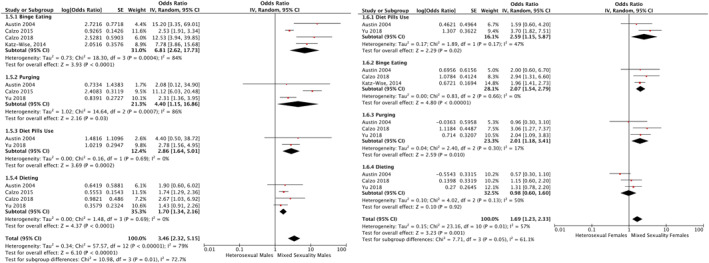
Forest Plot of the ORs of four EDrEBs among the mixed sexuality stratified by biological sex
Austin, 2004, Katz‐Wise, 2014, Calzo, 2015, Calzo, 2018 and Yu, 2018s studies combined sexual minorities groups (e.g. homosexual and bisexual group), resulting in data extraction for the specific groups (mentioned above) being inaccessible.
4.5.1. Homosexual group
Both females and males participants who identified as homosexual have shown a great vulnerability to 4 analysed EDrEBs than their heterosexual counterparts. The EDrEBs were more marked in the homosexual male group in comparison to the homosexual female counterparts.
Homosexual males
Data demonstrated that homosexual males have the highest ORs across all the four EDrEBs, referent to the heterosexual male group (Binge eating: 7.20 [3.70,14.01], p < 0.00001; Purging: 5.40 [4.72, 6.17], p < 0.00001, I 2 = 0%; Diet pills use: 3.50 [2.12,5.79], p < 0.00001, I 2 = 75%; Dieting: 3.10 [2.69,3.57], p < 0.00001, I 2 = 0%) (Figure 3). Data showed that homosexual males had the highest odds for binge eating behaviour (OR = 7.20), followed by purging, diet pills use and dieting when compared with heterosexual males.
The comparison of homosexuality across the biological sexes also illustrated that the males have much higher ORs for all the listed EDrEBs than their female counterparts. Specifically, homosexual males were approximately 3 times more likely to binge eat than homosexual females and 2.24 times more likely to purge than homosexual females among adolescents. Homosexual males have a higher OR at 3.50 for diet pill use (in comparison to the referent heterosexual males) whilst homosexual females have an OR at 2.59 (in comparison to the referent heterosexual females), indicating that the homosexual individuals had increased odds of this behaviour in comparison to their heterosexual counterparts. It was noted that homosexual males have higher dieting OR at 3.10 than homosexual females at 1.75.
When comparing the EDrEBs across different male sexual orientation (i.e. bisexual male subgroup and mixed sexuality male subgroup), the homosexual male group remained the more susceptible sub‐group for all of the analysed EDrEBs. Homosexual males have the highest OR (at 7.20) of binge eating than bisexual males (OR = 4.60), mixed sexuality males (OR = 6.81), and heterosexual adolescent males (OR = 1.00). This pattern is less marked purging (homosexual males OR = 5.40; bisexual males = 4.44; mixed sexuality group = 4.40) and dieting (homosexual males OR = 3.10; bisexual males = 2.36; mixed sexuality group = 1.70) and diet pill use (homosexual males OR = 3.50; bisexual males OR = 3.42; mixed sexuality male OR = 2.86).
Homosexual females
Data illustrated that homosexual females have a relatively higher ORs of the listed EDrEBs, referent to the heterosexual female group (Diet pills use: 2.59 [2.04, 3.27], p < 0.00001, I 2 = 31%; Purging: 2.41 [1.62,3.58], p < 0.00001; Binge eating: 2.14 [1.00,4.60] 1 , p = 0.05; Dieting: 1.75 [1.08,2.81], p = 0.02, I 2 = 62%) (Figure 3). Particularly for using diet pills, homosexual adolescent females have the highest OR at 2.59 among the analysed EDrEBs. The behavioural risk ranking for homosexual females was relatively similar for diet pills, followed by purging, and binge eating and the odds for dieting was the lowest (at 1.75, though still statistically significant p = 0.02) in comparison to the female heterosexual referent group.
The comparison of biological sex across homosexuality has been completed in the homosexual males section (see above). Data differences between sexual orientation across biological female groups illustrated another pattern to that described above for biological males. Both homosexual females (OR = 2.59 [2.04, 3.27]) and mixed sexuality females (OR = 2.59 [1.15, 5.87]) were more likely to use diet pills than bisexual females (OR = 2.30). Homosexual females have the highest OR (at 2.41) of purging than bisexual females (OR = 2.37), mixed sexuality females (OR = 2.01), and heterosexual adolescent females (OR = 1.00). However, the bisexual females were more likely to binge eat (bisexual females OR = 2.26; homosexual females = 2.14; mixed sexuality females = 2.07) and diet (bisexual females OR = 1.86; homosexual females = 1.75; mixed sexuality group = 0.98).
4.5.2. Bisexual group
Bisexuality showed a clear vulnerability to four EDrEBs compared with the referent heterosexual population but appeared to be less vulnerable than their homosexual counterparts (see Section 1 above).
Bisexual males
Bisexual males also exhibited relative higher ORs for the four EDrEBs in comparison to the referent to the heterosexual male group with the following ranking (Binge eating: 4.60 [1.20, 17.63], p = 0.03; Purging: 4.44 [2.66, 7.41], p < 0.00001, I 2 = 80%; Diet pills use: 3.42 [2.37, 4.94], p < 0.00001, I 2 = 55%; Dieting: 2.36 [2.04, 2.72], p < 0.00001, I 2 = 0%) (Figure 3).
Bisexual males were nearly 2 times more likely to binge eat and purge than their bisexual female counterparts (Binge eating OR: bi‐males = 4.60 vs. bi‐females = 2.26; Purge OR: bi‐males 4.44 vs. bi‐females = 2.37). This higher biological male to female tend continues, though was less marked for diet pill use (Diet pill use OR: bi‐males = 3.42 vs. bi‐females = 2.30) and dieting (Dieting OR: bi‐males = 2.36 vs. bi‐females = 1.86). Despite these observed trends, no significant difference was found across the 2 biological sexes for any of the EDrEBs.
Bisexual females
The difference across the 4 analysed EDrEBs in bisexual females is less marked, though dieting was observed to have the lowest odds. However these were still noticeably higher (and statistically significant) in comparison to their referent heterosexual female group (Purging: 2.37 [1.86, 3.02], p < 0.00001, I 2 = 76%; Diet pills use: 2.30 [1.59, 3.33], p < 0.00001, I 2 = 72%; Binge eating: 2.26 [1.60, 3.20], p < 0.00001; Dieting: 1.86 [1.34, 2.60], p = 0.0002, I 2 = 84%) (Figure 3).
4.5.3. Mixed sexuality (homosexual or bisexual in‐between)
Mixed sexuality exhibited a relative vulnerability to four EDrEBs compared with the referent heterosexual population, except for the mixed sexuality females at dieting.
Mixed sexuality males
Mixed sexuality males have relative higher ORs of the listed four EDrEBs in comparison referent to the heterosexual male group, presented in high‐to‐low OR: Binge eating: 6.81 [2.62,17.73], p < 0.0001, I 2 = 84%; Purging: 4.40 [1.15, 16.86], p = 0.03, I 2 = 86%; Diet pills use: 2.86 [1.64, 5.01], p = 0.0002, I 2 = 0%; Dieting: 1.70 [1.34, 2.16], p < 0.0001, I 2 = 0% (Figure 3).
Mixed sexuality males were observed to have higher odds across all four EDrEBs than their mixed sexuality female counterparts, though the difference between the 2 biological sexes is most marked for binge eating and purging behaviours (Binge eating OR: mix‐males = 6.81 vs. mix‐females = 2.07; Purge OR: mix‐males 4.40 vs. mix‐females = 2.01; Diet pill use OR: mix‐males = 2.86 vs. mix‐females = 2.59; Dieting OR: mix‐males = 1.70 vs. mix‐females = 0.98).
Mixed sexuality females
Mixed sexuality females show a slightly different picture, in that they have higher odds for three of the four EDrEBs, that is, diet pills use (OR = 2.59 [1.15, 5.87], p = 0.02, I 2 = 47%), binge eating (OR = 2.07 [1.54, 2.79], p < 0.00001, I 2 = 0%) and purging (OR = 2.01 [1.18, 3.41], p = 0.01, I 2 = 17%). However, their dieting behaviour is comparable to their heterosexual referent group (OR = 0.98 [0.60, 1.60], p = 0.92, I 2 = 50%) (Figure 3).
4.5.4. Sexual minority
In short, SMin groups including subjects identified as homosexual, bisexual and mixed sexuality groups, were more susceptible to most EDrEBs when compared to the referent homosexual population.
Generally, SMin males were more vulnerable than SMin females, proved with higher ORs of each EDrEBs than SMin females with binge eating being the most common EDrEB in SMin adolescents, followed by purging.
As Calzo et al.’s (2015) study included only male participants, this impacted the sex‐stratified analysis. If Calzo et al.’s (2015) data was to be excluded from the analysis, the OR among SMin males would be much higher at 8.02 [5.34, 12.05] (p < 0.00001, I 2 = 0%).
4.6. Publication bias
With regards to the outcome of the four EDrEBs types in SMin females versus heterosexual females, the funnel plot was asymmetrical indicating possibly publication bias. Conversely, in SMin males versus heterosexual males, the plot was symmetrical and hence publication bias was unlikely (Figure 7).
FIGURE 7.
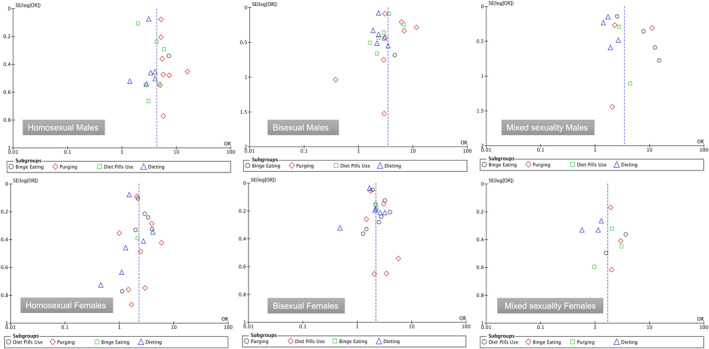
Funnel Plot of the ORs of four EDrEBs among different sexual orientations stratified by biological sex
5. DISCUSSION
5.1. Summary of evidence
This review aimed to systematically evaluate the published literature on sexual orientation and EDrEBs in adolescents. Data of 4 EDrEBs were drawn from 10 studies to calculate the corresponding ORs, the majority of which were rated as of ‘good’ quality.
The results were based on the analytic data from 10 studies (n = 412,601) exploring EDrEBs in different sexual orientation. All SMin individuals were more likely to develop EDrEBs. Homosexual males were noted to be the most vulnerable SMin group.
5.2. Commentary
Results from this meta‐analysis suggest that individuals of a minority sexual orientation are generally at higher ORs (and therefore more vulnerable) to dieting, binge eating, purging and diet pills use, with homosexuality having the greater odds of EDrEBs. Homosexuality has been widely discussed as a susceptible population for EDrEBs amongst both males and females (French et al., 1996; McClain & Peebles, 2016; Moore & Keel, 2003), even as early on as adolescents (age <18) (Austin et al., 2004, 2009, 2013; Calzo et al., 2015, 2018), young adult homosexual male group (Feldman & Meyer, 2007; Russell & Keel, 2002) and adult homosexual females in (Meneguzzo et al., 2018; Moore & Keel, 2003). This was similar to the results attained in this meta‐analysis.
Stress associated with being in a SMin group, that could be caused by external factors (such as stigma, discrimination and prejudice) (Parker & Harriger, 2020) or internal ones (such as cognitive dissonance in relation to their sexual orientation, fear of ‘coming out’).
All these factors that pre‐dispose these groups to more EDrEBs as an unhealthy coping mechanism or could also be secondary to body dissatisfaction and weight/shape concerns (Parker & Harriger, 2020), both being key aspects of anorexia and bulimia nervosa.
Bisexuality has distinct characteristics of sexual orientation. Bisexuality lies in‐between the heterosexual and the homosexual orientation continuum, which means that it could present with characteristics of either orientation in addition to having distinct characteristics. It is interesting to note, that despite the added stresses faced by bisexual individuals, such as the sexual objectification, internalised biphobia and invisibility and erasure of their sexual orientation by others (Taylor et al., 2019), bisexual individuals, particularly male bisexuals are less likely to experience EDrEBs. This is not the case for bisexual females who are more likely to resort to dieting and binge‐eating than their homosexual female counterparts which could imply that they are more vulnerable to the bisexual stressors mentioned above.
5.3. Future research
There is paucity of research in this cohort of individuals. Further studies are encouraged to focus on the association and risk factors between homosexuality/bisexuality and EDrEBs amongst adolescents, a critical developmental period and to explore whether the association with EDrEBs changes over time.
5.4. Limitations
This review has several limitations which should be taken into consideration when interpreting these results. The authors note that there is a standardized measurement for sexual orientation is lacking. Calzo et al. (2015) adopted the term ‘SMin’ to cover all the minorities' sexual orientation. 5 studies (Austin et al., 2013, 2004, 2009; Calzo et al., 2018; Katz‐Wise et al., 2014) adopted the categories ‘mostly heterosexual’ and ‘completely heterosexual’, whilst 3 studies (Calzo et al., 2019; Watson et al., 2017; Zullig et al., 2017) only mention a ‘heterosexual’ group. For this meta‐analysis, the ‘mostly heterosexual’ group were not included in this study to avoid heterogeneity of the referent group, which means that this data was not analysed.
Most of the participants in studies included in this review self‐identified as white and most of the results (7 out of 10) were carried out in the United States, and the remaining 3 studies were carried out in the United Kingdom, Canada and South Korea. This can impact the generalisability of the results as a range of ethnic/socio‐cultural variations appears lacking in the published data. Further research on the influence of sociocultural factors on both the articulation of sexual orientation and the stigma associated with mental health and EDrEBs should be considered.
Finally, limited published data/articles on adolescent SMin groups and EDrEBs will undoubtedly impact the results of this meta‐analysis. In addition, some studies were noted to have used the same population cohort (i.e. Growing Up Today Study 1999 (n = 2), Youth Risk Behaviour Surveys 2009–2011 (n = 2) and the year 2013 (n = 3), which highlights that some of the published data is secondary analysis from the original dataset.
Over‐exercise is a common EDrEBs seen in clinical practice. Unfortunately, there was no data on this EDrEB in the included studies and therefore this was not looked at.
6. CONCLUSION
This review included a sample of n = 412,601 and highlighted that SMin individuals have higher ORs of EDrEBs in adolescents. This is particularly noticeable in males, with the highest odds being observed in homosexual males across all the EDrEBs, that is, binge eating, purging, dieting and diet pills use of all groups.
In conclusion, all SMin groups had higher OR for the four EDrEBs reviewed in this paper in comparison to the respective referent heterosexual group. Although this extra vulnerability applies to both sexes, adolescent males appear to have higher ORs than their SMin female counterparts in comparison to the respective reference heterosexual group, with homosexual males being the most vulnerable. Healthcare professionals and SMin communities should be primed to facilitate earlier recognition (through selective prevention) and access to services in these vulnerable groups.
Cao, Z. , Cini, E. , Pellegrini, D. , & Fragkos, K. C. (2023). The association between sexual orientation and eating disorders‐related eating behaviours in adolescents: A systematic review and meta‐analysis. European Eating Disorders Review, 31(1), 46–64. 10.1002/erv.2952
ENDNOTE
This data is solely calculated from (Austin et al., 2009)'s article.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- American Psychiatric Association (APA), Joint Information Service of the American Psychiatric Association and the National Association for Mental, H., American Medico‐Psychological, A., & American Psychiatric Institute for Research (APIR) and, E . (2013). Desk reference to diagnostic criteria from DSM‐5. American Psychiatric Association. [Google Scholar]
- Austin, S. , Nelson, L. A. , Birkett, M. A. , Calzo, J. P. , & Everett, B. (2013). Eating disorder symptoms and obesity at the intersections of gender, ethnicity, and sexual orientation in US high school students. American Journal of Public Health, 103(2), e16–e22. 10.2105/AJPH.2012.301150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Austin, S. , Ziyadeh, N. , Kahn, J. A. , Camargo, C. A., Jr. , Colditz, G. A. , & Field, A. E. (2004). Sexual orientation, weight concerns, and eating‐disordered behaviors in adolescent girls and boys. Journal of the American Academy of Child & Adolescent Psychiatry, 43(9), 1115–1123. 10.1097/01.chi.0000131139.93862.10 [DOI] [PubMed] [Google Scholar]
- Austin, S. B. , Ziyadeh, N. J. , Corliss, H. L. , Rosario, M. , Wypij, D. , Haines, J. , & Field, A. E. (2009). Sexual orientation disparities in purging and binge eating from early to late adolescence. Journal of Adolescent Health, 45(3), 238–245. 10.1016/j.jadohealth.2009.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey, J. M. , Vasey, P. L. , Diamond, L. M. , Breedlove, S. M. , Vilain, E. , & Epprecht, M. (2016). Sexual orientation, controversy, and science. Psychological Science in the Public Interest, 17(2), 45–101. 10.1177/1529100616637616 [DOI] [PubMed] [Google Scholar]
- Calzo, J. P. , Austin, S. B. , & Micali, N. (2018). Sexual orientation disparities in eating disorder symptoms among adolescent boys and girls in the UK. European Child & Adolescent Psychiatry, 27(11), 1483–1490. 10.1007/s00787-018-1145-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calzo, J. P. , Masyn, K. E. , Corliss, H. L. , Scherer, E. A. , Field, A. E. , & Austin, S. B. (2015). Patterns of body image concerns and disordered weight‐ and shape‐related behaviors in heterosexual and sexual minority adolescent males. Developmental Psychology, 51(9), 1216–1225. 10.1037/dev0000027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calzo, J. P. , Turner, B. C. , Marro, R. , & Phillips, G. L. (2019). Alcohol use and disordered eating in a US sample of heterosexual and sexual minority adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 58(2), 200–210. 10.1016/j.jaac.2018.09.437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cella, S. , Iannaccone, M. , & Cotrufo, P. (2013). Influence of gender role orientation (masculinity versus femininity) on body satisfaction and eating attitudes in homosexuals, heterosexuals and transsexuals. Eating and Weight Disorders‐Studies on Anorexia Bulimia and Obesity, 18(2), 115–124. 10.1007/s40519-013-0017-z [DOI] [PubMed] [Google Scholar]
- Diamond, L. M. (2016). Sexual fluidity in male and females. Current Sexual Health Reports, 8(4), 249–256. 10.1007/s11930-016-0092-z [DOI] [Google Scholar]
- Ellis, L. , Burke, D. , & Ames, M. (1987). Sexual orientation as a continuous variable: A comparison between the sexes. The Official Publication of the International Academy of Sex Research, 16(6), 523–529. 10.1007/BF01541716 [DOI] [PubMed] [Google Scholar]
- Ettinger, S. (2004). Sexual orientation in child and adolescent health. In Ettinger S. & Perrin E. (Eds.), (Vol. 32, pp. 224‐227).
- Fairburn, C. G. , & Beglin, S. J. (1994). Assessment of eating disorders: Interview or self‐report questionnaire? International Journal of Eating Disorders, 16(4), 363–370. 10.1002/1098-108X(199412)16:4<363::AID-EAT2260160405>3.0 [DOI] [PubMed] [Google Scholar]
- Fairburn, C. G. , & Harrison, P. J. (2003). Eating disorders. The Lancet, 361(9355), 407–416. 10.1016/S0140-6736(03)12378-1 [DOI] [PubMed] [Google Scholar]
- Feldman, M. B. , & Meyer, I. H. (2007). Eating disorders in diverse lesbian, gay, and bisexual populations. International Journal of Eating Disorders, 40(3), 218–226. 10.1002/eat.20360 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field, A. E. , Sonneville, K. R. , Micali, N. , Crosby, R. D. , Swanson, S. A. , Laird, N. M. , & Horton, N. J. (2012). Common eating disorders predictive of adverse outcomes are missed by the DSM‐IV and DSM‐5 classifications. Neuropsychiatrie de l'Enfance et de l'Adolescence, 60(5), S65. 10.1016/j.neurenf.2012.05.251 [DOI] [Google Scholar]
- French, S. A. , Story, M. , Remafedi, G. , Resnick, M. D. , & Blum, R. W. (1996). Sexual orientation and prevalence of body dissatisfaction and eating disordered behaviors: A population‐based study of adolescents. International Journal of Eating Disorders, 19(2), 119–126. 10.1002/(SICI)1098-108X(199603)19:2<119::AID-EAT2>3.0.CO;2-Q [DOI] [PubMed] [Google Scholar]
- Gigi, I. , Bachner‐Melman, R. , & Lev‐Ari, L. (2016). The association between sexual orientation, susceptibility to social messages and disordered eating in men. Appetite, 99, 25–33. 10.1016/j.appet.2015.12.027 [DOI] [PubMed] [Google Scholar]
- Guyatt, G. H. , Oxman, A. D. , Vist, G. E. , Kunz, R. , Falck‐Ytter, Y. , Alonso‐Coello, P. , & Schünemann, H. J. (2008a). Rating quality of evidence and strength of recommendations: Grade: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ British Medical Journal, 336(7650), 924–926. 10.1136/bmj.39489.470347.ad [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guyatt, G. H. , Oxman, A. D. , Vist, G. E. , Kunz, R. , Falck‐Ytter, Y. , & Schünemann, H. J. (2008b). Rating quality of evidence and strength of recommendations: Grade: What is "quality of evidence" and why is it important to clinicians? BMJ British Medical Journal, 336(7651), 995–998. 10.1136/bmj.39490.551019.be [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herdt, G. , & McClintock, M. (2000). The magical age of 10. The Official Publication of the International Academy of Sex Research, 29(6), 587–606. 10.1023/A:1002006521067 [DOI] [PubMed] [Google Scholar]
- Katz‐Wise, S. L. , Jun, H. J. , Corliss, H. L. , Jackson, B. , Haines, J. , & Austin, S. B. (2014). Child abuse as a predictor of gendered sexual orientation disparities in body mass index trajectories among U.S. youth from the Growing up Today Study. Journal of Adolescent Health, 54(6), 730–738. 10.1016/j.jadohealth.2013.11.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klingenspor, B. (2002). Gender‐related self‐discrepancies and bulimic eating behavior. Sex Roles. Journal of Research, 47(1–2), 51–64. 10.1023/A:1020631703798 [DOI] [Google Scholar]
- Lozano, R. , Naghavi, M. , Foreman, K. , Lim, S. , Shibuya, K. , Aboyans, V. , Lipshultz, S. E. , Adair, T. , Aggarwal, R. , Ahn, S. Y. , AlMazroa, M. A. , Alvarado, M. , Anderson, H. R. , Anderson, L. M. , Andrews, K. G. , Atkinson, C. , Baddour, L. M. , Barker‐Collo, S. , Bartels, D. H. , … Murray, C. J. L. (2012). Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the global burden of disease study 2010. The Lancet, 380(9859), 2095–2128. 10.1016/S0140-6736(12)61728-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClain, Z. , & Peebles, R. (2016). Body image and eating disorders among lesbian, gay, bisexual, and transgender youth. Pediatric Clinics of North America, 63(6), 1079–1090. 10.1016/j.pcl.2016.07.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meneguzzo, P. , Collantoni, E. , Gallicchio, D. , Busetto, P. , Solmi, M. , Santonastaso, P. , & Favaro, A. (2018). Eating disorders symptoms in sexual minority women: A systematic review. European Eating Disorders Review, 26(4), 275–292. 10.1002/erv.2601 [DOI] [PubMed] [Google Scholar]
- Micali, N. , Hagberg, K. W. , Petersen, I. , & Treasure, J. L. (2013). The incidence of eating disorders in the UK in 2000‐2009: Findings from the general practice research database. BMJ Open, 3(5), e002646. 10.1136/bmjopen-2013-002646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moher, D. , Liberati, A. , Tetzlaff, J. , & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta‐analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264. 10.7326/0003-4819-151-4-200908180-00135 [DOI] [PubMed] [Google Scholar]
- Moore, F. , & Keel, P. K. (2003). Influence of sexual orientation and age on disordered eating attitudes and behaviors in women. International Journal of Eating Disorders, 34(3), 370–374. 10.1002/eat.10198 [DOI] [PubMed] [Google Scholar]
- Ott, M. , Corliss, H. , Wypij, D. , Rosario, M. , & Austin, S. (2011). Stability and change in self‐reported sexual orientation identity in young people: Application of mobility metrics. The Official Publication of the International Academy of Sex Research, 40(3), 519–532. 10.1007/s10508-010-9691-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Page, M. J. , McKenzie, J. E. , Bossuyt, P. M. , Boutron, I. , Hoffmann, T. C. , Mulrow, C. D. , Shamseer, L. , Tetzlaff, J. M. , Akl, E. A. , Brennan, S. E. , Chou, R. , Glanville, J. , Grimshaw, J. M. , Hrobjartsson, A. , Lalu, M. M. , Li, T. , Loder, E. W. , Mayo‐Wilson, E. , McDonald, S. , & Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. 10.1136/bmj.n71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parker, L. L. , & Harriger, J. A. (2020). Eating disorders and disordered eating behaviors in the LGBT population: A review of the literature. J Eat Disord, 8(1), 51. 10.1186/s40337-020-00327-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell, C. J. , & Keel, P. K. (2002). Homosexuality as a specific risk factor for eating disorders in men. International Journal of Eating Disorders, 31(3), 300–306. 10.1002/eat.10036 [DOI] [PubMed] [Google Scholar]
- Shearer, A. , Russon, J. , Herres, J. , Atte, T. , Kodish, T. , & Diamond, G. (2015). The relationship between disordered eating and sexuality amongst adolescents and young adults. Eating Behaviors, 19, 115–119. 10.1016/j.eatbeh.2015.08.001 [DOI] [PubMed] [Google Scholar]
- Srivastava, A. , Winn, J. , Senese, J. , 4th, Goldbach, J. T. , & Goldbach, J. T. (2022). Sexual orientation change among adolescents and young adults: A systematic review. Archives of Sexual Behavior, 51(7), 3361–3376. 10.1007/s10508-022-02394-5 [DOI] [PubMed] [Google Scholar]
- Taylor, J. , Power, J. , Smith, E. , & Rathbone, M. (2019). Bisexual mental health: Findings from the 'Who I Am' study. Australian journal of general practice, 48(3), 138–144. 10.31128/AJGP-06-18-4615 [DOI] [PubMed] [Google Scholar]
- Watson, R. J. , Adjei, J. , Saewyc, E. , Homma, Y. , & Goodenow, C. (2017). Trends and disparities in disordered eating among heterosexual and sexual minority adolescents. International Journal of Eating Disorders, 50(1), 22–31. 10.1002/eat.22576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu, K. Y. , Kim, Y. , Calzo, J. P. , Levinson, J. A. , & Austin, S. (2018). Sex of sexual partners and disordered weight control behaviors in a nationally representative sample of South Korean adolescents. Psychiatry Research, 262, 1–5. 10.1016/j.psychres.2018.01.028 [DOI] [PubMed] [Google Scholar]
- Zullig, K. J. , Matthews‐Ewald, M. R. , & Valois, R. F. (2017). Relationship between disordered eating and self‐identified sexual minority youth in a sample of public high school adolescents. Eating and Weight Disorders, 24(3), 565–573. 10.1007/s40519-017-0389-6 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.