

Abstract
Introduction
Penile prosthesis implantation (PPI) is a treatment option recommended in clinical guidelines for erectile dysfunction (ED). However, a limited number of urologists perform PPI procedures in the United States.
Aim
To quantify the number of insured men with ED in the United States and project the number of potential candidates for PPI in 2022.
Methods
An Excel-based disease impact model was constructed using a top-down estimation approach. The starting US male population consisted of adult men from 2022 US Census data after exclusion of age-specific mortality rates from the National Vital Statistics Reports. Men with health insurance were included in the model based on insurance status data from the US Census database. ED prevalence and ED treatment rates were obtained from administrative claims data analyses—the Merative MarketScan Commercial Database (18-64 years) and the 5% Medicare Standard Analytical Files (≥65 years)—and literature-based estimates of patient-reported ED prevalence.
Outcomes
The number of men with ED in the United States and the number of potential candidates for PPI were estimated.
Results
By utilizing ED prevalence based on administrative claims, an estimated 8.3% of insured men (10,302,540 estimated men [8,882,548 aged 18-64 years and 1,419,992 aged ≥65 years]) had a diagnosis of ED and sought ED care, out of 124,318,519 eligible US men aged ≥18 years in 2022. An estimated 17.1% of men with an ED diagnosis claim could benefit from PPI in 2022 (1,759,248 men aged ≥18 years). Patient self-reported ED prevalence across all ages ranged from 5.1% to 70.2%. Scenario analyses applying the patient self-reported ED prevalence range revealed the number of men in the United States who could benefit from PPI could have been higher than 1.7 million if their ED symptoms were diagnosed by health care providers.
Clinical Implications
Most men with ED in the United States are undertreated, and many could benefit from PPI.
Strengths and Limitations
This analysis is a US population–level estimation. However, given this study utilized a variety of assumptions, the results may vary if different model assumptions are applied.
Conclusions
This disease impact model estimated that approximately 10.3 million men were diagnosed with ED by their health care providers and sought ED care in the United States in 2022. Of those, 1.7 million men could be PPI candidates and benefit from the treatment option.
Keywords: erectile dysfunction, prevalence, penile prosthesis, sexual dysfunction, census data
Introduction
Erectile dysfunction (ED) is a common condition affecting men that substantially and negatively affects intimate relationships, quality of life, and self-esteem.1–4 A prospective cross-sectional international study of 52,697 men in Brazil, China, France, Germany, Italy, Spain, the United Kingdom, and the United States between the ages of 40 and 70 years found that men with ED had significantly lower physical and mental component quality-of-life scores and significantly lower health state utilities than men without ED (all P < 0.001).4 More than half of men within the same age group experience at least partial ED, and nearly 10% have severe or complete ED.5 The prevalence and burden of ED increase as men age6; however, recent research showed a higher-than-expected prevalence of ED in young men (8% aged 20-30 years).7 The higher prevalence of ED in young men may be due to psychological factors such as anxiety.7 Men with ED are reported to have significantly higher absenteeism (7.1% vs 3.2%), presenteeism (22.5% vs 10.1%), overall work productivity impairment (24.8% vs 11.2%), and activity impairment (28.6% vs 14.5%) as compared to men without ED.4
Several medical and surgical treatment options are available for the treatment of ED, including oral and parenteral drugs, injectable vasodilator agents, vacuum erection devices, penile prosthesis implantation (PPI), lifestyle modifications, and psychosexual therapy. Oral phosphodiesterase-5 inhibitors (PDE5Is) are the most commonly used first-line treatment for ED; however, approximately one-third of men with ED do not respond to PDE5Is and some patients are not able to take oral medications due to medical conditions.8 Evidence has shown that one-third of men using PDE5Is cease use after 1 prescription and one-half cease use by 6 months.9 PPI is a definitive treatment option for ED, as recommended by the American Urological Association (AUA),10 Canadian Urological Association,11 British Association of Urological Surgeons,12 International Consultation on Sexual Medicine,13 Sexual Medical Society of North America, European Association of Urology,14 Urological Society of Australia and New Zealand,15 and Korean Society for Sexual Medicine and Andrology.16 In most cases, PPI is provided for those patients who did not respond to, did not tolerate, or were unwilling to consider other treatments. The AUA guideline states that “using the shared decision-making process as a cornerstone for care, all patients should be informed of all treatment modalities that are not contraindicated, regardless of invasiveness or irreversibility, as potential first-line treatments.”10 However, there are a limited number of implanters who can perform the procedure, potentially restricting access for men who may benefit from the treatment.17 This study aimed to estimate the number of men in the United States with ED who were seeking ED care and to identify how many men may be potential candidates for PPI as of 2022.
Methods
Model design and starting patient population
An Excel-based disease impact model was constructed via a top-down estimation approach. Top-down estimation captures national long-run average resource utilization or costs and provides approximate overall estimates.18 This is in contrast to bottom-up methods, which require local resource utilization and costs of specific inputs and capture site-level differences more appropriate for specific settings of care.18,19 Data from the 2022 US Census20 were used to determine the starting US male population (101,599,370 men aged 18-64 years and 26,727,557 men aged ≥65 years). The average age-specific mortality rates obtained from the National Vital Statistics Reports were applied to the starting population to include only the estimated men who would survive through 2022. Table 1 presents the inputs used in the disease impact model. Since this study does not involve human participants, neither institutional review board approval nor informed consent was obtained.
Table 1.
Model inputs applied to the disease impact model.
| Model input | |||
|---|---|---|---|
| Parameter | 18-64 y | ≥65 y | Source |
| Base case analysis | |||
| US male population in 2022, No. | 101,599,370 | 26,727,557 | US Census Bureau20 |
| Average mortality rates, % | 0.4 | 13.4 | Centers for Disease Control and Prevention40 |
| US insured population, % | 88.1 | 99.0 | US Census Bureau21 |
| US insured population with ED diagnosis, % | 10.0 | 6.2 | Administrative claims data analysis |
| Diagnosed population not receiving any ED treatment paid for by primary insurance, % | 94.0 | 99.5 | Administrative claims data analysis |
| US male population with moderate to severe ED, % | 18.2 | Rhoden et al24 | |
| US male population with any contraindications for penile prosthesis implantation, % | 1.0 | Assumption based on US penile prosthesis manufacturer instruction for use25,26 and American Urological Association guideline10 contraindications of treatable/transient infections | |
Abbreviation: ED, erectile dysfunction.
Men with health insurance estimates
This model included only men who were expected to have health insurance. The proportions of men with public and private health insurance were obtained from insurance status data from the US Census database (Table 1).21 US Census statistics on health insurance coverage are based on information collected in the 2020 Current Population Survey Annual Social and Economic Supplements and the American Community Survey.
Estimated number of men with ED in the United States in 2022
Estimated number of men with ED seeking ED care calculated from ED prevalence rates obtained from administrative claims databases
To obtain a conservative estimate of the number of men with ED, reflecting a documented diagnosis of ED by a health care provider, who are actively seeking care for their ED symptoms, this model applied the ED prevalence obtained from administrative claims databases: the Merative MarketScan Commercial Database for men aged 18 to 64 years and the 5% Medicare Standard Analytical Files (SAF) for men aged ≥65 years (Table 1). The Merative MarketScan Commercial Database provides comprehensive claims data for >263 million working individuals from >160 US employers and >40 US health plans.22 The 5% Medicare SAF data contains all site-of-service claims data of traditional Medicare fee-for-service beneficiaries in the United States, the majority of whom are aged >65 years. Relevant International Classification of Diseases, Tenth Revision, Clinical Modification diagnosis codes for ED from previously published literature,23 including male erectile disorder (F52.21) and male ED unspecified (N52.9), were used to identify men with ED from the databases. This conservative calculation provided the estimate for the number of men with ED diagnosed by a health care provider who were seeking care for their ED symptoms with their provider. The estimate was subsequently used to calculate the number of men who were PPI candidates and ready to consider the procedure if presented to them.
Estimated number of men with ED calculated from patient-reported ED prevalence rates obtained from published literature
The ED prevalence obtained from the administrative claims data analyses reflects a documented diagnosis of ED by health care providers, which is the number of men already seeking care for ED and likely underestimates the actual US prevalence of ED. Therefore, the model used patient-reported ED prevalence data obtained from a literature review we conducted in the PubMed.gov database to estimate a more realistic number of men with ED in the United States in 2022. This estimate provided the upper estimate of the range of the number of men with ED and was subsequently used to calculate the number of men who may benefit from PPI if their ED is diagnosed by a health care provider.
The literature search strategy to obtain the patient-reported ED prevalence data utilized the following search terms: “erectile dysfunction,” “prevalence,” and “United States.” The literature search was restricted to studies published between 2000 and 2022 and those published on human data and in English. The search identified 652 records that were individually reviewed to identify relevant studies reporting US prevalence rates for ED. All eligible studies underwent title and abstract screening, and any potentially relevant citation was screened via a full-text review. Reference lists of selected articles were searched for relevant data publications.
Studies were included for consideration (n = 53) if they evaluated the patient-reported prevalence of ED among a general population of US patients (ideally nationally representative), as these were deemed to be the best data sources for capturing diagnosed and undiagnosed ED. Studies were excluded if they were nonhuman or non-English, were conducted outside the United States, did not contain primary data (eg, literature reviews [systematic or narrative], meta-analyses, commentaries, editorials, or study designs), did not report clinical data (eg, laboratory data or biomechanical data), did not evaluate ED prevalence, or were small case series (n < 10 patients) or case studies. Data extracted from the most pertinent studies included the authors' names, publication year, data source/study population, methods of ED measurement, and the reported ED prevalence estimates with 95% CIs (if available) by age group (Table 2).
Table 2.
Published patient-reported ED prevalence rates among US population (2000-2022).
| Study | Year | Data source/study population | ED measurement | Age, y | Prevalence (95% CI), % |
|---|---|---|---|---|---|
| Kupelian41 | 2008 | Boston Area Community Health Survey | IIEF-5 | 30-79 | 20.7 |
| Laumann42 | 2007 | Male Attitudes Regarding Sexual Health Study | MMAS | ≥40 | 22.0 (19.4-24.6) |
| 40-49 | 9.1 (5.9-12.2) | ||||
| 50-59 | 15.2 (11.3-19.1) | ||||
| 60-69 | 29.4 (22.8-35.9) | ||||
| ≥70 | 54.9 (46.9-62.8) | ||||
| Derby43 | 2001 | MMAS | MMAS | 40-69 | 50.0 (45-54) |
| IIEF | 40-69 | 50.0 (42-57) | |||
| Londoño44 | 2012 | Kaiser Permanente Southern California | MMAS | 45-69 | 57.8 |
| Ansong45 | 2000 | 4 rural counties in central New York State | Two questions: Have you experienced erectile dysfunction (impotence) within the past 6 mo? Have you sought treatment for erectile dysfunction (impotence)? | 50-76 | 46.3 |
| 50-54 | 26 | ||||
| 55-59 | 34.9 | ||||
| 60-64 | 46.9 | ||||
| 65-69 | 57.8 | ||||
| 70-76 | 69.4 | ||||
| Laumann46 | 2009 | Random national sample | Two questions: Whether they had experienced erection difficulties for at least 2 mo during the previous year. Those who answered yes were then asked whether they had experienced the problem occasionally, sometimes, or frequently. | 40-80 | 22.5 (19.6-25.7) |
| Selvin47 | 2007 | NHANES | Question: How would you describe your ability to get and keep an erection adequate for satisfactory intercourse? Would you say that you are always able or almost always able to get and keep an erection, usually able to get and keep an erection, sometimes able to get and keep an erection, or never able to get and keep an erection? | ≥20 | 18.4 |
| 20-39 | 5.1 | ||||
| 40-59 | 14.8 | ||||
| 60-69 | 43.8 | ||||
| ≥70 | 70.2 | ||||
| Johannes,48 Feldman5,a | 2000, 1994 | MMAS | MMAS | 40-49 50-59 | 12.4 (9.0-16.9) 29.8 (24.0-37.0) |
| 60-69 | 46.4 (36.9-58.4) | ||||
| Fang49 | 2015 | Boston Area Community Health Survey | IIEF-5 | 29.4-79.7 | 47.5 |
| Rosen50 | 2004 | Men’s Attitudes to Life Events and Sexuality Study | Self-reported erection difficulty | 20-29 | 8 |
| 30-39 | 11 | ||||
| 40-49 | 15 | ||||
| 50-59 | 22 | ||||
| 60-69 | 30 | ||||
| 70-75 | 37 | ||||
| Goldstein51 | 2020 | National Health and Wellness Survey | Self-reported difficulty in achieving or maintaining an erection in the past 6 mo | 40-70 | 46.1 |
| Loprinzi52 | 2015 | NHANES | Question: How would you describe your ability to get and keep an erection adequate for satisfactory intercourse? | 50-85 | 53.7 |
| Foster53 | 2013 | National Health and Wellness Survey | American Urological Association–Symptom Index | ≥40 | 24.6 for ED only and 4.9 for ED with benign prostatic hyperplasia |
| Shaeer54 | 2012 | Global Online Sexuality Survey | IIEF-5 | Mean 52.4 | 37.7 had various degrees of ED: mild, 19.4; mild to moderate, 7.3; moderate, 4.4; and severe, 6.6 |
(Continued)
Table 2.
Continued
| Study | Year | Data source/study population | ED measurement | Age, y | Prevalence (95% CI), % |
|---|---|---|---|---|---|
| 18-39 | 29.7 | ||||
| 40-49 | 23.6 | ||||
| 50-59 | 30.8 | ||||
| ≥60 | 57.4 | ||||
| Smith55 | 2009 | California Men’s Health Study–Kaiser Permanente | Question: Many men have difficulty getting and keeping an erection that is rigid enough for satisfactory sexual activity. How would you describe your experience during the past year? | 45-49 | 13 |
| 50-59 | 24 | ||||
| 60-69 | 44 | ||||
| Lindau56 | 2007 | National Social Life, Health, and Aging Project | Self-reported difficulty in achieving or maintaining an erection | 57-85 | 37 |
| Francis57 | 2007 | NHANES | Self-reported ability to get and keep an erection | Complete ED | |
| Overall | 8.1 | ||||
| 40-49 | 1.23 | ||||
| 50-59 | 3.65 | ||||
| 60-69 | 14.17 | ||||
| 70-79 | 24.91 | ||||
| ≥80 | 56.02 | ||||
| Saigal58 | 2006 | NHANES | Question: How would you describe your ability to get and keep an erection adequate for satisfactory intercourse?” | Sometimes able | |
| 20-29 | 4.7 | ||||
| 30-39 | 3.4 | ||||
| 40-49 | 7.0 | ||||
| 50-59 | 19.9 | ||||
| 60-69 | 27.0 | ||||
| 70-74 | 38.7 | ||||
| ≥75 | 30.1 | ||||
| Shabsigh59 | 2005 | Cross-national survey on men’s health issues | Self-reported difficulty getting or keeping an erection | 20-75 | 25 |
| O’Leary60 | 2003 | Olmsted County Study of Urinary Symptoms and Health Status Among Men | Self-reported erectile function | 40-49 | 3 |
| 80-89 | 49 | ||||
| Kantor61 | 2002 | General medical practices in Pennsylvania | IIEF | 18-40 | 13.0 |
| 41-50 | 3.4 | ||||
| 51-60 | 28.9 | ||||
| 61-70 | 41.7 | ||||
| >70 | 66.0 | ||||
| Monga62 | 2002 | Community-dwelling older men | IIEF-5 | Complete, severe, moderate, mild ED | |
| Overall | 3, 11, 13, 24 | ||||
| 30-49 | 0, 3, 4, 12 | ||||
| 50-64 | 2, 8, 12, 32 | ||||
| 65-69 | 3, 20, 22, 30 | ||||
| 70-74 | 6, 27, 16, 27 | ||||
| 75-79 | 12, 24, 21, 29 | ||||
| ≥80 | 8, 17, 29, 38 |
Abbreviations: ED, erectile dysfunction; IIEF, International Index of Erectile Function; MMAS, Massachusetts Male Aging Study; NHANES, National Health and Nutrition Examination Survey; PPI, penile prosthesis implantation.
Self-reported ED prevalence estimates for all age groups were extracted, and the median, minimum, and maximum values were calculated. The values were then used to estimate the number of men with ED and the number of men who could benefit from PPI in the model.
Men who received no ED treatment paid by their insurance
The model then applied the rates of men with ED who had not received ED treatment to the 2 sets of estimated numbers of men with ED calculated from administrative claims databases and published literature. The rates of men with ED but without ED treatment paid by their insurers were obtained from the same administrative claims databases (Merative MarketScan Commercial Database for men with ED aged 18 to 64 years and 5% Medicare SAF for men with ED aged ≥65 years) to calculate the number of men receiving no documented treatment during that given year. The ED treatment included PDE5Is, PPI, and other ED treatments (eg, vacuum pump, intraurethral suppositories) identified via relevant codes from previously published research.23
Men who could benefit from PPI treatment estimates
For the estimation of men who were eligible for PPI, the following assumptions were made:
Few men would pay 100% out-of-pocket for PPI if they did not have insurance; hence, these patients were not included.
Men with moderate to severe ED (as estimated from Rhoden et al24; Table 1) could seek PPI after trying other ED treatments, since men with mild ED are not considered candidates for PPI.
Only men with ED without resistant infections could be considered candidates for PPI, based on products’ instruction for use25,26 and AUA guideline10 contraindications of treatable/transient infections. It was assumed that 1% of men had a resistant infection.
It was assumed that 1% of men had a resistant infection (Table 1). The assumptions were applied to 2 sets of estimated numbers of men with ED who received no ED treatment.
Results
Estimated number of men with ED seeking ED care in the United States in 2022
By using the ED diagnosis data obtained from the administrative claims data analyses, an estimated 8.3% of insured men (10,302,540 estimated men [8,882,548 aged 18-64 and 1,419,992 aged ≥65 years]) were diagnosed with ED by health care providers from the 124,318,519 eligible US men aged ≥18 years in 2022 (Figure 1).
Figure 1.
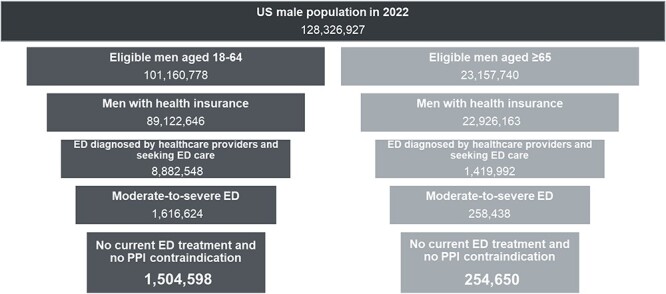
Funnel plots narrow the number of men from 2022 census data to the number of men with ED who could be PPI candidates. Data are based on ED prevalence from administrative claims databases reflecting men with ED who were diagnosed by a health care provider and seeking ED care. Abbreviations: ED, erectile dysfunction; PPI, penile prosthesis implantation.
Estimated number of men with ED calculated from patient-reported ED prevalence rates obtained from published literature
The literature review to obtain the patient-reported prevalence of ED among the general population from 2000 to 2022 identified 22 eligible publications that reported data on patient-reported ED prevalence. The ED prevalence from the included studies was assessed through different methods: International Index of Erectile Function (6 publications, 27.3%), the Massachusetts Male Aging Study–derived questionnaire (4 publications, 18.2%), and other patient self-reported questionnaires (12 publications, 54.5%). The range of patient self-reported ED prevalence across ages from 22 studies was from 3.0% to 70.2%, with a median of 27.0% (Table 2). Based on the median ED prevalence, the number of men with ED in the United States could be as high as 30,333,668.
Estimated number of men who could benefit from PPI treatment
Figure 1 shows a funnel plot that demonstrates each step to narrow down the number of men from the starting population to the number of men who could benefit from PPI treatment. The base case estimate according to administrative claims data for the rates of men with ED without ED treatment and from published literature for the proportion with moderate to severe ED revealed that 17.1% of men aged ≥18 years with an ED diagnosis could benefit from PPI (1,759,248 men in the United States). The estimated number of men with ED who could benefit from PPI, by age group, is 1,504,598 men aged 18 to 64 years and 254 ,650 men aged ≥65 years (Figure 1). By applying the patient self-reported ED prevalence range to the scenario analyses, as many as 13,436,363 men in the United States with ED could benefit from PPI if their ED condition was clinically diagnosed by a health care provider.
Discussion
The results of this study illustrate a high number of men with ED who are potential candidates for PPI. An estimated 8.3% of insured men in the United States (10,302,540) had a diagnosis of ED from 124,318,519 eligible US men aged ≥18 years in 2022. At least 1.7 million men are PPI candidates, and as many as 13.4 million US men can benefit from PPI if their self-reported ED is clinically diagnosed by a health care provider.
Penile prosthesis is a well-known alternative treatment option for ED with high satisfaction rates.27–30 IPPs provide a durable treatment, with devices functioning for up to 20 years.31 One publication showed that patients with ED who underwent penile implant surgery had significantly better erectile function and treatment satisfaction rates than patients who received PDE5Is.32 Unfortunately, PPI accessibility could be a barrier to treatment; only 4 out of 100 practicing urologists are trained to perform PPI in the United States.17 Ensuring sufficient penile prosthesis implanters could mitigate the potential physical, emotional, and social burden of untreated ED.
Large multicenter clinical trials have demonstrated the efficacy and tolerability of PDE5Is in ED among patients with varying etiologies and across a broad range of severity and age.33 However, approximately 30% to 35% of patients prescribed PDE5Is fail to respond to therapy, and an equally large proportion stops therapy for other reasons. The PDE5I prescription renewal rate has been estimated to be 62% at 3 to 4 months and 30% at 6 to 12 months.34 Reasons for failure of PDE5I treatment may include severe ED at presentation, worsening of endothelial dysfunction and progression of penile atherosclerosis, ED after radical prostatectomy, unrecognized hypogonadism, inadequate patient education and incorrect drug usage, and psychosocial factors.33 Regardless of the reason, medical therapy is evidently inadequate for a large proportion of patients with ED.
When ED goes untreated, psychological problems may ensue, such as depression, loss of self-esteem, feelings of worthlessness, interpersonal relationship strain, and cognitive issues.35,36 With respect to the association between ED and depression, one study demonstrated that treatment for ED is protective against the development of major depressive disorder within 3 years.37
Psychological impairment may also lead to missed workdays, presenteeism, and activity impairment.4,38 It is imperative that the urologic community understand the importance of addressing the scarcity of trained and practicing surgeons to ensure equitable access for patients.
The strengths of this study include the use of multiple data sources, such as nationwide population-level databases (census data, National Vital Statistics Reports data), two large administrative claims databases (Merative MarketScan Commercial Database and the 5% Medicare SAF), and a synthesis of information on patient-reported prevalence in a practice setting. This approach provided a large national sample, ensured comprehensiveness of our data, and increased the external validity of our findings to the United States. Second, an exhaustive analysis of the population-based data was done to characterize the US ED population by age (18-64 and ≥65 years) and can be valuable for clinical and policy decision-making. Third, implementing a disease impact model allowed for an estimation of the ED population size of the diagnosed and undiagnosed, which further helps with informing national policies and treatment recommendations.
There are several limitations to our study, many of which are inherent to all decision-analytic modeling studies. Models represent a simplification of disease and treatment pathways and combine data inputs from multiple sources. Model inputs from the published literature may be out-of-date given the evolving and aging population dynamics, changes to clinical care, and technological innovation. However, we expect that the estimates that we obtained are conservative and that the true number of men with ED and number of men potentially eligible for PPI are even higher. ED treatments may not have all been captured in the claims data and are likely underestimated (e.g., medications purchased out-of-pocket or online without a prescription, compounding pharmacy treatments, traditional therapies such as herbals, or lifestyle treatments). In addition, inferences cannot be drawn on the men whose other treatments failed outside of the claims data period. The ED prevalence obtained from the administrative claims data analyses reflects a documented diagnosis of ED, which is the number of men already seeking and receiving care for ED and underestimates the actual US prevalence of ED. Hence, to ensure that we were capturing men who may not have had access to ED care, we also utilized published estimates of patient-reported ED prevalence. Finally, the results of this modeling evaluation reflect US patients with public or private insurance, and results may not be generalizable to patients without health insurance, patients with Veterans Affairs or Tricare health insurance, or patients in which clinical practice and reimbursement structure, health care accessibility, and treatment accessibility may differ. Evidence suggests that military service members and veterans may be at increased risk for ED.39; however, this study did not incorporate Veterans Affairs and Tricare data.
Conclusions
This disease impact model approximated that 10.3 million men were diagnosed with ED by their health care providers and sought ED care in the United States in 2022. An estimated 17.1% of these men (1.7 million) are PPI candidates, and ensuring sufficient penile prosthesis implanters could mitigate the physical, emotional, and social burden of ED.
Acknowledgments
We thank Alysha McGovern for proofreading this manuscript.
Contributor Information
Sirikan Rojanasarot, Health Economics and Market Access, Boston Scientific, Marlborough, MA 01752, United States.
Abimbola O Williams, Health Economics and Market Access, Boston Scientific, Marlborough, MA 01752, United States.
Natalie Edwards, Health Services Consulting Corporation, Boxborough, MA 01719, United States.
Mohit Khera, Baylor College of Medicine, Houston, TX 77030, United States.
Author contributions
All authors contributed to the study design, manuscript development, and manuscript revision; read and approved the final manuscript; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by Boston Scientific.
Conflicts of interest: S.R. and A.W. are full-time employees of Boston Scientific. N.E. is an employee of Health Services Consulting Corporation, a consulting company that is paid by Boston Scientific for the services rendered. M.K. is a board-certified urologist and was not compensated for his participation in this study.
References
- 1. Litwin MS, Nied RJ, Dhanani N. Health-related quality of life in men with erectile dysfunction. J Gen Intern Med. 1998;13(3):159–166 10.1046/j.1525-1497.1998.00050.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Wagner G, Fugl-Meyer KS, Fugl-Meyer AR. Impact of erectile dysfunction on quality of life: patient and partner perspectives. Int J Impot Res. 2000;12(suppl 4):S144–S146 10.1038/sj.ijir.3900594. [DOI] [PubMed] [Google Scholar]
- 3. Penson DF. The effect of erectile dysfunction on quality of life following treatment for localized prostate cancer. Rev Urol. 2001;3(3):113–119. [PMC free article] [PubMed] [Google Scholar]
- 4. Goldstein I, Goren A, Li VW, Maculaitis MC, Tang WY, Hassan TA. The association of erectile dysfunction with productivity and absenteeism in eight countries globally. Int J Clin Pract. 2019;73(11):e13384. 10.1111/ijcp.13384. [DOI] [PubMed] [Google Scholar]
- 5. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54–61 10.1016/s0022-5347(17)34871-1. [DOI] [PubMed] [Google Scholar]
- 6. Wessells H, Joyce GF, Wise M, Wilt TJ. Erectile dysfunction. J Urol. 2007;177(5):1675–1681 10.1016/j.juro.2007.01.057. [DOI] [PubMed] [Google Scholar]
- 7. Kessler A, Sollie S, Challacombe B, Briggs K, Van Hemelrijck M. The global prevalence of erectile dysfunction: a review. BJU Int. 2019;124(4):587–599 10.1111/bju.14813. [DOI] [PubMed] [Google Scholar]
- 8. Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction: Sildenafil Study Group. N Engl J Med. 1998;338(20):1397–1404 10.1056/nejm199805143382001. [DOI] [PubMed] [Google Scholar]
- 9. Mazzola CR, Deveci S, Teloken P, Mulhall JP. Exploring the association between erectile rigidity and treatment adherence with sildenafil. J Sex Med. 2013;10(7):1861–1866 10.1111/jsm.12014. [DOI] [PubMed] [Google Scholar]
- 10. American Urological Association . Erectile dysfunction: AUA guideline. 2018. https://www.auanet.org/guidelines/erectile-dysfunction-(ed)-guideline.
- 11. Domes T, Najafabadi BT, Roberts M, et al. Canadian Urological Association guideline: erectile dysfunction. Can Urol Assoc J. 2021;15(10):310–322 10.5489/cuaj.7572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ralph D, McNicholas T. UK management guidelines for erectile dysfunction. BMJ. 2000;321(7259):499–503 10.1136/bmj.321.7259.499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Levine LA, Becher EF, Bella AJ, et al. Penile prosthesis surgery: current recommendations from the international consultation on sexual medicine. J Sex Med. 2016;13(4):489–518 10.1016/j.jsxm.2016.01.017. [DOI] [PubMed] [Google Scholar]
- 14. Medina-Polo J, García-Gómez B, Alonso-Isa M, Romero-Otero J. Clinical guidelines on erectile dysfunction surgery: EAU-AUA perspectives. Actas Urol Esp (Engl Ed). 2020;44(5):289–293 10.1016/j.acuro.2019.10.008. [DOI] [PubMed] [Google Scholar]
- 15. Chung E, Lowy M, Gillman M, Love C, Katz D, Neilsen G. Urological Society of Australia and New Zealand (USANZ) and Australasian Chapter of Sexual Health Medicine (AChSHM) for the Royal Australasian College of Physicians (RACP) clinical guidelines on the management of erectile dysfunction. Med J Aust. 2022;217(6):318–324 10.5694/mja2.51694. [DOI] [PubMed] [Google Scholar]
- 16. Ryu JK, Cho KS, Kim SJ, et al. Korean Society for Sexual Medicine and Andrology (KSSMA) guideline on erectile dysfunction. World J Mens Health. 2013;31(2):83–102 10.5534/wjmh.2013.31.2.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. American Urological Association . The state of the urology workforce and practice in the United States. Accessed October 3, 2022. https://www.auanet.org/documents/research/census/2020-State-of-Urology-Workforce-Census-Book.pdf.
- 18. Chapko MK, Liu C-F, Perkins M, Li Y-F, Fortney JC, Maciejewski ML. Equivalence of two healthcare costing methods: bottom-up and top-down. Health Econ. 2009;18(10):1188–1201 10.1002/hec.1422. [DOI] [PubMed] [Google Scholar]
- 19. Wordsworth S, Ludbrook A, Caskey F, Macleod A. Collecting unit cost data in multicentre studies: creating comparable methods. Eur J Health Econ. 2005;6(1):38–44 10.1007/s10198-004-0259-9. [DOI] [PubMed] [Google Scholar]
- 20. US Census Bureau . International Database (IDB)—population estimates and projections for 227 countries and areas: United States. Accessed July 27, 2022. https://www.census.gov/data-tools/demo/idb/#/country?COUNTRY_YR_ANIM=2022&menu=countryViz&COUNTRY_YEAR=2022&TREND_RANGE=1950,2100&TREND_STEP=10&TREND_ADD_YRS=&POP_YEARS=2021&FIPS_SINGLE=US.
- 21. US Census Bureau . Health insurance coverage in the United States: 2020. Accessed July 27, 2022. https://www.census.gov/content/dam/Census/library/publications/2021/demo/p60-274.pdf.
- 22. Watson Health . IBM MarketScan research databases for health services researchers. 2021. Accessed July 7, 2022. https://www.ibm.com/downloads/cas/OWZWJ0QO.
- 23. Burnett AL, Rojanasarot S, Amorosi SL. An analysis of a commercial database on the use of erectile dysfunction treatments for men with employer-sponsored health insurance. Urology. 2021;149:140–145 10.1016/j.urology.2020.11.051. [DOI] [PubMed] [Google Scholar]
- 24. Rhoden EL, Telöken C, Sogari PR, Vargas Souto CA. The use of the simplified International Index of Erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction. Int J Impot Res. 2002;14(4):245–250 10.1038/sj.ijir.3900859. [DOI] [PubMed] [Google Scholar]
- 25. Boston Scientific . Boston Scientific AMS 700 Inflatable Penile Prosthesis risks. Accessed July 31, 2022. https://www.bostonscientific.com/en-US/products/penile-prosthesis/ams-700-inflatable-penile-prosthesis/risks.html.
- 26. Coloplast . Coloplast Titan Inflatable Penile Prosthesis (IPP). Accessed July 31, 2022. https://iu.coloplast.us/wp-content/uploads/2022/02/USUC_Titan_PM-00479.pdf.
- 27. Ji YS, Ko YH, Song PH, Moon KH. Long-term survival and patient satisfaction with inflatable penile prosthesis for the treatment of erectile dysfunction. Korean J Urol. 2015;56(6):461–465 10.4111/kju.2015.56.6.461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Jorissen C, De Bruyna H, Baten E, Van Renterghem K. Clinical outcome: patient and partner satisfaction after penile implant surgery. Curr Urol. 2019;13(2):94–100 10.1159/000499286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Manfredi C, Fortier É, Faix A, Martínez-Salamanca JI. Penile implant surgery satisfaction assessment. J Sex Med. 2021;18(5):868–874 10.1016/j.jsxm.2021.03.007. [DOI] [PubMed] [Google Scholar]
- 30. Palasi S, Howell S, Green TP, et al. Does knowing pre-operative penile length influence patient satisfaction post penile prosthesis implantation? Int J Impot Res. 2021;34(8):776–780 10.1038/s41443-021-00472-1. [DOI] [PubMed] [Google Scholar]
- 31. Miller LE, Khera M, Bhattacharyya S, Patel M, Nitschelm K, Burnett AL. Long-term survival rates of inflatable penile prostheses: systematic review and meta-analysis. Urology. 2022;166:6–10 10.1016/j.urology.2022.03.026. [DOI] [PubMed] [Google Scholar]
- 32. Rajpurkar A, Dhabuwala CB. Comparison of satisfaction rates and erectile function in patients treated with sildenafil, intracavernous prostaglandin E1 and penile implant surgery for erectile dysfunction in urology practice. J Urol. 2003;170(1):159–163 10.1097/01.ju.0000072524.82345.6d. [DOI] [PubMed] [Google Scholar]
- 33. McMahon CN, Smith CJ, Shabsigh R. Treating erectile dysfunction when PDE5 inhibitors fail. BMJ. 2006;332(7541):589–592 10.1136/bmj.332.7541.589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Fagelman E, Fagelman A, Shabsigh R. Efficacy, safety, and use of sildenafil in urologic practice. Urology. 2001;57(6):1141–1144 10.1016/s0090-4295(01)00984-0. [DOI] [PubMed] [Google Scholar]
- 35. Al-Shaiji TF. Breaking the ice of erectile dysfunction taboo: a focus on clinician-patient communication. J Patient Exp. 2022;9:23743735221077512. 10.1177/23743735221077512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. DiMeo PJ. Psychosocial and relationship issues in men with erectile dysfunction. Urol Nurs. 2006;26(6):442–446453.. [PubMed] [Google Scholar]
- 37. Nackeeran S, Havanur A, Ory J, Althof S, Ramasamy R. Erectile dysfunction is a modifiable risk factor for major depressive disorder: analysis of a federated research network. J Sex Med. 2021;18(12):2005–2011 10.1016/j.jsxm.2021.09.016. [DOI] [PubMed] [Google Scholar]
- 38. Rojanasarot SS, Bhattacharyya SK, Burnett AL. Cost of lost productivity due to erectile dysfunction and impact of employer benefit exclusion of penile prosthesis implantation treatment. J Occup Environ Med. 2022;64(5):403–408 10.1097/jom.0000000000002449. [DOI] [PubMed] [Google Scholar]
- 39. Kolaja CA, Roenfeldt K, Armenta RF, et al. Sexual health problems among service men: the influence of posttraumatic stress disorder. J Sex Res. 2022;59(4):413–425 10.1080/00224499.2020.1855622. [DOI] [PubMed] [Google Scholar]
- 40. Centers for Disease Control and Prevention . Life table for males: United States, 2017. Accessed July 27, 2022. https://www.dir.ca.gov/osip/LifeExpectancyTables2017.pdf?msclkid=1fadce2ed07111eca000d77b93d63cc9.
- 41. Kupelian V, Link CL, Rosen RC, McKinlay JB. Socioeconomic status, not race/ethnicity, contributes to variation in the prevalence of erectile dysfunction: results from the Boston Area Community Health (BACH) survey. J Sex Med. 2008;5(6):1325–1333 10.1111/j.1743-6109.2008.00822.x. [DOI] [PubMed] [Google Scholar]
- 42. Laumann EO, West S, Glasser D, Carson C, Rosen R, Kang JH. Prevalence and correlates of erectile dysfunction by race and ethnicity among men aged 40 or older in the United States: from the male attitudes regarding sexual health survey. J Sex Med. 2007;4(1):57–65 10.1111/j.1743-6109.2006.00340.x. [DOI] [PubMed] [Google Scholar]
- 43. Derby CA, Barbour MM, Hume AL, McKinlay JB. Drug therapy and prevalence of erectile dysfunction in the Massachusetts Male Aging Study cohort. Pharmacotherapy. 2001;21(6):676–683 10.1592/phco.21.7.676.34571. [DOI] [PubMed] [Google Scholar]
- 44. Londoño DC, Slezak JM, Quinn VP, Van Den Eeden SK, Loo RK, Jacobsen SJ. Population-based study of erectile dysfunction and polypharmacy. BJU Int. 2012;110(2):254–259 10.1111/j.1464-410X.2011.10761.x. [DOI] [PubMed] [Google Scholar]
- 45. Ansong KS, Lewis C, Jenkins P, Bell J. Epidemiology of erectile dysfunction: a community-based study in rural New York State. Ann Epidemiol. 2000;10(5):293–296 10.1016/s1047-2797(00)00050-8. [DOI] [PubMed] [Google Scholar]
- 46. Laumann EO, Glasser DB, Neves RC, Moreira ED Jr, for the GSSAB Investigators’ Group . A population-based survey of sexual activity, sexual problems and associated help-seeking behavior patterns in mature adults in the United States of America. Int J Impot Res. 2009;21(3):171–178 10.1038/ijir.2009.7. [DOI] [PubMed] [Google Scholar]
- 47. Selvin E, Burnett AL, Platz EA. Prevalence and risk factors for erectile dysfunction in the US. Am J Med. 2007;120(2):151–157 10.1016/j.amjmed.2006.06.010. [DOI] [PubMed] [Google Scholar]
- 48. Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, McKinlay JB. Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts Male Aging Study. J Urol. 2000;163(2):460–463. [PubMed] [Google Scholar]
- 49. Fang SC, Rosen RC, Vita JA, Ganz P, Kupelian V. Changes in erectile dysfunction over time in relation to Framingham cardiovascular risk in the Boston Area Community Health (BACH) survey. J Sex Med. 2015;12(1):100–108 10.1111/jsm.12715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Rosen RC, Fisher WA, Eardley I, et al. The multinational Men’s Attitudes to Life Events and Sexuality (MALES) study: I. prevalence of erectile dysfunction and related health concerns in the general population. Curr Med Res Opin. 2004;20(5):607–617 10.1185/030079904125003467. [DOI] [PubMed] [Google Scholar]
- 51. Goldstein I, Goren A, Li VW, Tang WY, Hassan TA. Epidemiology update of erectile dysfunction in eight countries with high burden. Sex Med Rev. 2020;8(1):48–58 10.1016/j.sxmr.2019.06.008. [DOI] [PubMed] [Google Scholar]
- 52. Loprinzi PD, Edwards M. Association between objectively measured physical activity and erectile dysfunction among a nationally representative sample of American men. J Sex Med. 2015;12(9):1862–1864 10.1111/jsm.12977. [DOI] [PubMed] [Google Scholar]
- 53. Foster SA, Annunziata K, Shortridge EF, Freedman D, Viktrup L. Erectile dysfunction with or without coexisting benign prostatic hyperplasia in the general US population: analysis of US National Health and Wellness Survey. Curr Med Res Opin. 2013;29(12):1709–1717 10.1185/03007995.2013.837385. [DOI] [PubMed] [Google Scholar]
- 54. Shaeer O, Shaeer K. The Global Online Sexuality Survey (GOSS): the United States of America in 2011. Chapter I: erectile dysfunction among English-speakers. J Sex Med. 2012;9(12):3018–3027 10.1111/j.1743-6109.2012.02976.x. [DOI] [PubMed] [Google Scholar]
- 55. Smith JF, Caan BJ, Sternfeld B, et al. Racial disparities in erectile dysfunction among participants in the California Men’s Health Study. J Sex Med. 2009;6(12):3433–3439 10.1111/j.1743-6109.2009.01519.x. [DOI] [PubMed] [Google Scholar]
- 56. Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357(8):762–774 10.1056/NEJMoa067423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Francis ME, Kusek JW, Nyberg LM, Eggers PW. The contribution of common medical conditions and drug exposures to erectile dysfunction in adult males. J Urol. 2007;178(2):591–596 10.1016/j.juro.2007.03.127. [DOI] [PubMed] [Google Scholar]
- 58. Saigal CS, Wessells H, Pace J, Schonlau M, Wilt TJ, Urologic Diseases in America Project . Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166(2):207–212 10.1001/archinte.166.2.207. [DOI] [PubMed] [Google Scholar]
- 59. Shabsigh R, Perelman MA, Lockhart DC, Lue TF, Broderick GA. Health issues of men: prevalence and correlates of erectile dysfunction. J Urol. 2005;174(2):662–667 10.1097/01.ju.0000165389.73148.d1. [DOI] [PubMed] [Google Scholar]
- 60. O’Leary MP, Rhodes T, Girman CJ, et al. Distribution of the Brief Male Sexual Inventory in community men. Int J Impot Res. 2003;15(3):185–191 10.1038/sj.ijir.3900996. [DOI] [PubMed] [Google Scholar]
- 61. Kantor J, Bilker WB, Glasser DB, Margolis DJ. Prevalence of erectile dysfunction and active depression: an analytic cross-sectional study of general medical patients. Am J Epidemiol. 2002;156(11):1035–1042 10.1093/aje/kwf142. [DOI] [PubMed] [Google Scholar]
- 62. Monga M, Bettencourt R, Barrett-Connor E. Community-based study of erectile dysfunction and sildenafil use: the Rancho Bernardo study. Urology. 2002;59(5):753–757 10.1016/s0090-4295(02)01503-0. [DOI] [PubMed] [Google Scholar]