

Abstract
Erectile dysfunction (ED) impacts the wellness and quality of life of millions of Canadians. An evaluation focused on the identification of reversible and irreversible underlying factors is recommended for patients presenting with ED. Through a shared decision-making model framework, the goal of ED treatment is to improve functional outcomes and enhance sexual satisfaction while minimizing adverse effects associated with treatment. Given that ED is assessed and treated by multiple different types of health practitioners, the purpose of this guideline is to provide the best available evidence to facilitate care delivery through a Canadian lens. After a narrative review of ED assessment and treatment for general readership, five key clinical questions relating to priority areas of ED are assessed using the GRADE and evidence-to-decision-making frameworks.
Introduction
Erectile dysfunction (ED) is the inability to achieve or maintain an erection sufficient for satisfactory sexual performance. Penile erection requires a complex integration between vascular, neural, and endocrine systems leading to adequate arterial dilatation, trabecular smooth muscle relaxation, and activation of the corporal veno-occlusive mechanism.1
ED is highly prevalent, with both the Canadian Study of Erectile Dysfunction2 and the Massachusetts Male Aging Study (MMAS)3 reporting high rates of men experiencing ED, with a higher prevalence and severity associated with aging. For example, in the MMAS, approximately 40% of men in their 40s experienced ED of varying degrees of severity and the prevalence of ED increases about 10% per decade. Additionally, as a man ages, the proportion of men with a higher severity of ED increases. In the MMAS, the prevalence of severe ED tripled from 5% in men in their 40s to 15% in men in their 70s.
ED can be categorized as organic, psychogenic, or mixed based on the patient’s history and examination findings. Organic ED is typically classified by its underlying pathophysiological mechanism(s), which include: vasculogenic (most common), neurogenic, structural, and hormonal.1 Psychogenic ED can be generalized or situational and may be related to a history of psychosocial stress, performance anxiety, and mental illness.4
There are many modifiable and non-modifiable risk factors associated with primarily vasculogenic ED, including advancing age, diabetes mellitus, dyslipidemia, hypertension, obesity, metabolic syndrome, sedentary lifestyle, and smoking.5–7 There is a large body of evidence suggesting that ED and cardiovascular and cerebrovascular diseases share the same risk factor profile and that ED may serve as an early warning sign for the future development of vascular events in some populations.5,8 In spite of this established link, some studies have demonstrated that ED is not an independent risk predictor of future vascular events and that established risk predictors, such as the Framingham risk score, are superior.9,10 Therefore, it remains controversial whether a diagnosis of ED alone should initiate a more thorough cardiovascular evaluation. Patient factors, such as age, ED severity, and duration and the presence of other cardiovascular risk factors, should guide clinicians when deciding if further investigations or optimization of cardiovascular health is required, in collaboration with other healthcare providers.5,8,11–13
ED is common after trauma (pelvic trauma and penile fracture), surgery (pelvic, penile, and urethral), and radiation therapy.14–18 Specifically, the Prostate Cancer Outcome Study19 reported 78.8% of post-prostatectomy patients not having erections firm enough for intercourse two years after surgery compared to 60.8% of men having ED two years following prostate radiotherapy. After 15 years from the time of treatment, the prevalence of ED increases further to 87% post-prostatectomy and 94% post-radiotherapy.19 ED is also frequently associated with other urological conditions, such as lower urinary tract symptoms/benign prostatic hyperplasia20 and chronic prostatitis/chronic pelvic pain syndrome.21
The impacts of ED go beyond the physical loss of function and the inability of having sexual intercourse. ED has a significant impact on the psychosocial health, well-being, and quality life for both the patient and their partner22,23 and can negatively impact relationships.24 It is critical for the clinician to be aware of these potential negative effects on the couple. Including the partner during ED assessment and treatment has been shown to improve patient outcomes.25,26
Methods
A guideline panel of 10 members, including male sexual health, urology, and guideline methodology experts, was established. The goal of the panel was to address relevant and priority issues and questions surrounding current ED practice and to produce an impactful document for learners and practitioners.
The guideline panel met and generated a broad list of topics and clinical questions relating to ED. In addition, each panel member selected and surveyed two community urologists practicing in their region to generate a second list of clinical questions that were felt to be relevant to the practice of a general urologist. Thirty questions were compiled and the panel selected the five most important questions through individual ratings based on perceived topic priority, identified practice variation, and expected feasibility of answering the question (see Appendix; available at cuaj.ca). These five questions were addressed systematically using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach and the evidence-to-decision (EtD) framework.27,28
The GRADE approach enabled the panel to appreciate the certainty in the evidence for each outcome, and overall, as very low, low, moderate, or high.29,30 The EtD framework assisted the panel in making clinical recommendations by considering desirable effects, undesirable effects, balance of the effects (net benefit), certainty in estimates of effect, patients’ values and preferences, resources required, cost-effectiveness, equity, feasibility, and acceptability.31 Summary of findings (SoF) and EtD framework tables using the GRADEpro GTD application32,33 are available in the Appendix (at cuaj.ca).
The panel chose improvements in erectile function (measured by the International Index of Erectile Function [IIEF]-EF score34) and quality of life as critical outcomes, and adverse events as an important outcome, to be collected during the literature review. The panel used the generally accepted minimal clinically important difference (MCID) of 4 in the IIEF-EF score as a significant improvement in erectile function, however, the panel recognizes the limitation that the MCID varies based on the baseline severity of ED (mild: 2; moderate: 5; severe: 7).35
Effect estimates were derived from studies contained in existing systematic reviews that addressed the five chosen clinical questions and by reproducing some of the review stages to ensure the most accurate effect estimates were calculated. These review steps included appraisal of the reviews, review of additional literature to locate any missing major trials, determining the risk of bias in the included studies, and performing the meta-analyses again.
Interpreting recommendations in the GRADE framework emphasizes the role of shared decision-making and patient values and preferences. In this framework, recommendations can be for or against and strong or conditional. A strong recommendation indicates that the panel believes that a significant majority of patients would choose the recommended course of action when aware of the available evidence. A conditional recommendation implies that the panel believes that most patients would want the recommended course of action, however, a substantial proportion would not. For clinicians, this means that when a weak recommendation is made the “best” course of action will rely on elucidating patient values and preferences in a shared decision-making process.
Background and narrative overview of ED
Patient assessment
The cornerstone of the assessment of patients with ED is a detailed history and physical exam. Screening laboratory testing to rule out associated conditions should be considered for patients presenting with ED, depending on the clinical context. Specialized tests, including imaging, are of limited value and are not recommended except in special circumstances.
History
A detailed history should include medical and psychological comorbidities, medications, substance use history (tobacco, alcohol, drugs), surgical and pelvic radiation history, a history of pelvic trauma, and previous treatments for sexual dysfunction. A detailed psychosocial and sexual history is key to a comprehensive assessment. While the underlying cause of ED is often multifactorial, key questions related to psychosocial factors and sexual history can point towards psychogenic and situational factors contributing to sexual dysfunction (Table 1). It has been hypothesized that excessive pornography use may contribute to sexual dysfunction during partnered sex,36 especially in younger patients with ED. However, this association is not clearly demonstrated in the empirical literature and requires further study.37, 38 Comorbid sexual conditions, such as premature ejaculation (PE), anorgasmia, low libido, and Peyronie’s disease (PD), should be identified in the initial assessment of any patients with ED, as the presence of these comorbid conditions will impact further assessment and management of ED.
Table 1.
Questions that may help to differentiate psychogenic from organic erectile dysfunction
| Question | Psychogenic ED | Organic ED |
|---|---|---|
| Presence of nocturnal erections? | Often present | Reduced |
| Presence of erection during masturbation or with alternate partners? | Often present | Reduced |
| Significant recent psychosocial stress? | Strong impact | Minimal impact |
| Feelings of performance anxiety around sexual activity? | Strong impact | Minimal impact |
| Situational variability of erectile dysfunction (improved while on vacation)? | Potential for wide variability | Minimal variability |
Assessment tools
Validated questionnaires and assessment tools (Table 2) can be useful in the initial diagnosis and followup of ED patients, especially when evaluating a patient’s response to treatment. While these assessment tools do not replace a detailed history and physical exam, they are cost-effective and non-threatening for patients to complete;39 however, these tools have varying degrees of utility in clinical practice. These assessment tools were originally validated in the heterosexual population, however, the IIEF has also been shown to be efficacious in the men who have sex with men (MSM) population.40
Table 2.
Erectile dysfunction validated assessment tools
| Tool | Summary |
|---|---|
| Erection Hardness Scale (EHS) | Self-reported assessment of penile hardness on a scale of 0 (no engorgement) to 4 (complete rigidity) |
| Sexual Health Inventory of Men (SHIM) | Five questions that provide a score out of 25 for the subjective patient-reported assessment of erectile dysfunction |
| International Inventory of Erectile Function (IIEF) | Fifteen questions exploring five domains (desire, erectile function, intercourse satisfaction, orgasmic function, and overall sexual satisfaction) of sexual function |
Physical examination
Physical examination is a helpful adjunct to assess a patient’s overall body habitus, level of virilization, and genital anatomy to identify any comorbid medical and/or sexual conditions.41 Table 3 summarizes the key features of the physical examination for patients with ED.
Table 3.
Physical exam for erectile dysfunction
| Area | Factors to be assessed |
|---|---|
| Overall | Blood pressure, body habitus, virilization, mood, gynecomastia |
| Penis and groins | Penile length and girth, presence of penile plaques, phimosis, frenular tether, meatal stenosis, quality of femoral pulses |
| Testicles | Volume and consistency |
Laboratory testing
In patients with either suspected vasculogenic or idiopathic ED, a baseline hemoglobin A1C, fasting glucose, and lipid profile should be considered to rule out occult diabetes and dyslipidemia. Patients with symptoms associated with testosterone deficiency or failure of phosphodiesterase type-5 inhibitors (PDE5is) should consider having a morning serum total testosterone level drawn.41
Specialized testing
Specialized testing, including nocturnal penile tumescence (NPT) and penile duplex ultrasound (PDU), is rarely required in the routine assessment of patients with ED. These tests can be used to differentiate between organic and non-organic causes of ED when the patient’s history is conflicting and in medico-legal cases. NPT estimates nocturnal penile rigidity42 and PDU measures arterial inflow (to assess arterial insufficiency) and venous outflow (to assess for venous leak) after the injection of a vasoactive substance.43 Both tests provide little practical information beyond what can be obtained from a detailed history and should only be obtained in limited situations by subspecialists in sexual medicine.
Treatment options
Overview
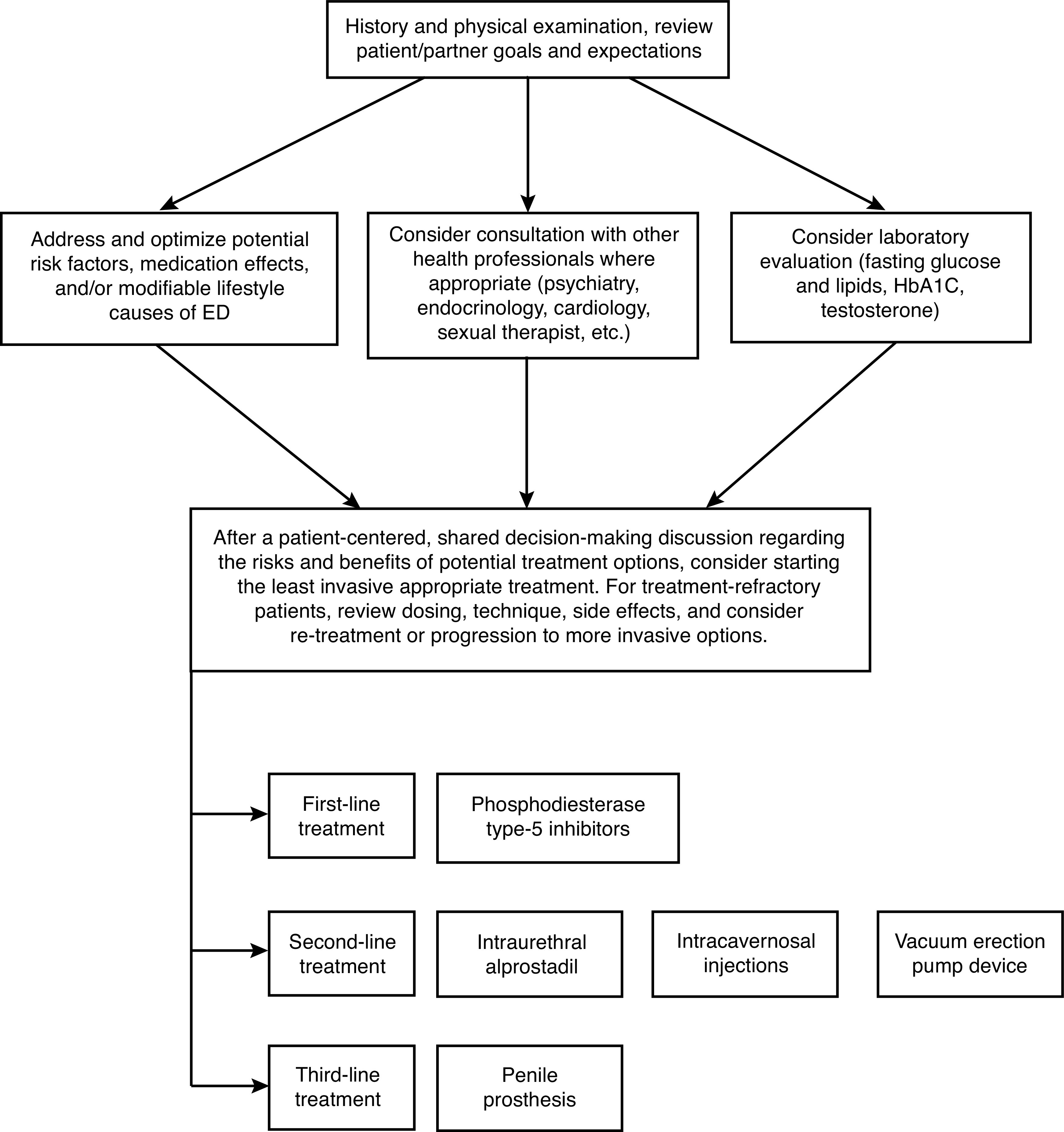
In Canada, primary care providers (PCPs) appropriately identify, investigate, and initiate first-line treatments in the vast majority of patients with ED. In the contemporary model of ED care, patients may be referred to urologists after failure of first-line therapy, as second-line therapies may be outside the practice pattern of PCPs.44 A patient-centered, shared decision-making model is advocated when discussing treatment options with the patient and their partner. Management of ED typically follows a stepwise progression from conservative measures to first-line PDE5is through to second- and third-line treatment options; however, specific patient factors and expectations may influence treatment decisions and the usual stepwise progression of treatment options (Fig. 1).
Fig. 1.
Management summary of erectile dysfunction.
Conservative treatment options
Conservative measures should be offered and continuously addressed with all patients with ED, especially if comorbidities or lifestyle habits are negatively impacting erectile function.45 These measures include exercise/physical activity,46 smoking cessation,47 reducing alcohol47 and cannabis consumption,48 and dietary changes. Additionally, the nitric oxide synthase substrates L-arginine and citrulline have been evaluated in limited studies49–51 but further confirmatory work is required prior to recommending their use in ED at this time. Clinicians should consider early referral for sexual counselling for patients experiencing ED, especially when there is concern for a psychogenic component.4,52,53 Sexual counselling may be a helpful adjunct to medical management and may improve relationship satisfaction and overall sexual functioning.54
Low-intensity shockwave therapy (Li-SWT)
Low-intensity shockwave therapy (Li-SWT) is a treatment option proposed for patients with mild to moderate ED. Li-SWT is administered with a wand-like device delivering low-intensity shockwaves to different areas of the penis in multiple sessions. Li-SWT is hypothesized to work by inducing angiogenesis through growth factor activation55 and inducing nerve regeneration,56 thereby reversing pathophysiological processes to improve erectile function. Although widely offered in numerous centers in Canada, often by non-urologists, Li-SWT is not Health Canadaor FDA-approved for clinical use for ED. The clinical use of Li-SWT for ED is addressed in the key clinical recommendation section of this guideline.
Phosphodiesterase type-5 inhibitors
Phosphodiesterase type-5 inhibitors (PDE5is) are a class of oral agents that facilitate a penile erection by promoting vascular and cavernosal smooth muscle relaxation in response to sexual stimulation.57 The PDE5is approved by Health Canada include sildenafil, tadalafil, and vardenafil. Each medication has unique pharmacokinetic and pharmacodynamic properties58 (Table 4). Patients initiating PDE5is should be counselled regarding potential side effects, including headache, flushing, dyspepsia, and nasal stuffiness, which are universal in all three drugs, with alterations in color vision (sildenafil and vardenafil) and myalgias (tadalafil) being more drug-specific.58,59 Absolute contraindications to PDE5is include intermittent or regular use of nitroglycerin or organic nitrates and hypersensitivity to any component of the tablet.58 Patients with an unsatisfactory response to PDE5is should first be counselled regarding proper use of the medication and may require a potential dose adjustment.60
Table 4.
Comparison of the properties of PDE5-inhibitors
| Property | Sildenafil | Tadalafil | Vardenafil |
|---|---|---|---|
| >TMAX | 30–120 minutes (median 60 minutes) | 30–360 minutes (median 120 minutes) | 30–120 minutes (median 60 minutes) |
| T½ | 4 hours | 17.5 hours | 4 hours |
| Absorption | Fatty meals cause a mean delay in TMAX of 60 minutes | Not affected by food | Fatty meals cause a reduction in CMAX |
| Available doses | 25 mg, 50 mg, 100 mg PRN | 2.5 mg, 5 mg daily 5 mg, 10 mg, 20 mg PRN |
10 mg oral dissolvable tablet 2.5 mg, 5 mg, 10 mg, 20 mg PRN |
| Maximum dose | 100 mg daily | 20 mg daily | 20 mg daily |
| Efficacy | Each of the PDE5 inhibitors offers similar efficacy | ||
| Dose adjustments may be needed for |
|
|
|
| Contraindications | Any patient using organic nitrates either regularly or intermittently Known hypersensitivity to any component of the tablet |
||
| Side effects (five most common in order of frequency when compared to placebo) | Headache, flushing, dyspepsia, nasal congestion, alteration in color vision | Headache, dyspepsia, back pain, myalgia, nasal congestion | Headache, flushing, rhinitis, dyspepsia, sinusitis |
Please consult the individual product monographs for additional information. Adapted from references 44 and 58. CrCl: creatinine clearance; PRN: as needed.
The panel strongly recommends PDE5is as the first-line pharmacological treatment for ED, given their impressive clinical efficacy and safety profile in a wide range of patients. A comprehensive systematic review by Yuan and colleagues61 reports a clinically significant mean improvement in the IIEF-EF score of 6.03 (95% confidence interval [CI] 5.38, 6.68) for sildenafil (12 randomized controlled trials [RCTs], 3404 patients), 8.07 (95% CI 7.18, 8.96) for tadalafil (eight RCTs, 1877 patients), and 7.05 (95% CI 5.60, 8.50) for vardenafil (six RCTs, 1151 patients). These drugs also have a strong safety profile, with the effect estimate for relative risk of serious adverse events being 1.38 (95% CI 0.67, 2.83) for sildenafil (10 RCTs, 2431 patients), 1.46 (95% C: 0.63, 3.37) for tadalafil (eight RCTs, 1967 patients), and 1.49 (95% CI 0.79, 2.83) for vardenafil (10 RCTs, 3628 patients) compared to placebo. Conceptualized another way with considering baseline risks in the included studies, out of 1000 patients taking the drug, on average, eight will experience a serious adverse event with sildenafil, seven with tadalafil, and eight with vardenafil.
Intraurethral alprostadil
Intraurethral alprostadil, known as MUSETM (Medicated Urethral System for Erection), is a second-line option for men with ED. It is effective for select patients but has failed to gain a significant market share due suboptimal efficacy and urethral discomfort.62 Dose titration with an “in-office” trial is advised to improve success.63 Since it does not require an injection, some patients prefer it over intracavernosal injection (ICI).64
Vacuum erection pump device
Vacuum erection pump devices (VED) consist of a cylindrical chamber placed over the penis coupled with a manual or mechanical pump to generate a vacuum. The negative pressure generated promotes blood flow into the penis, which is trapped by a constriction ring placed at the base of the penis and can be maintained safely for up to 30 minutes.65 Given the mechanics involved, VED is considered a more cumbersome and labor-intensive way to achieve an erection. However, 90% of patients will achieve a functional erection with adequate instruction and practice.66 VED can be associated with penile numbness, pain, bruising, and painful ejaculation. VED has no absolute contraindications, making it a reasonable option for those who cannot tolerate or have contraindications to other medical or surgical options.
Intracavernosal injection
Intracavernosal injection (ICI) was the first pharmacological treatment available for ED and involves the delivery of vasoactive agents directly into the corpus cavernosum prior to intercourse. Single-agent alprostadil has been shown to be highly effective and generally well-tolerated, with up to 94% of patients being able to achieve an erection sufficient for intercourse.67 Side effects include pain at the injection site, penile bruising, penile pain, penile scarring/curvature, and priapism. Although not approved by Health Canada, the addition of papaverine and phentolamine to alprostadil, often referred to as “Trimix,” has been shown to be even more efficacious than alprostadil monotherapy while maintaining an acceptable side effect profile and less penile pain.68 Prior to prescribing ICI, patients or their partners need to have the manual dexterity to prepare and perform the injection and a teaching session is advised to ensure proper injection technique and dose titration.69
Penile prosthesis
While not all non-surgical options need to be attempted prior to considering placement of a penile prosthesis, all non-surgical options should at least be discussed with the patient prior to considering surgical intervention. There are two types of prosthesis, malleable and inflatable, and both are surgically implanted into the corporal bodies to allow the patient to regain penile rigidity. The presence of clinically significant penile curvature, which may only be evident during activation of the device, should be discussed preoperatively and surgically corrected at the time of device implantation. Satisfaction rates are high for both implantnaive patients and those undergoing surgical revision of an existing device.70 Patients considering a penile prosthesis need to be aware that postoperative penile length can be negatively affected by corporal fibrosis or previous prostatectomy and the glans will remain flaccid post-implant.71 Mechanical failure does occur with inflatable devices over time, but almost 50% will still be functional after 20 years of use.72 Rare but serious late complications include infection or erosion of the device, which in certain cases, can lead to refractory and permanent ED.
Clinical recommendations using GRADE
Summary of recommendations (Table 5)
Table 5.
CUA erectile dysfunction guideline: Summary of recommendations
| 1. Among patients with erectile dysfunction, should daily tadalafil be preferentially prescribed instead of on-demand tadalafil? | |
| We suggest against the preferential use of daily tadalafil rather than on-demand tadalafil for patients with erectile dysfunction | Conditional recommendation, low levels of certainty in evidence |
| 2. Among patients with erectile dysfunction, should low-intensity shockwave therapy (Li-SWT) be recommended over no treatment? | |
| We suggest against the use of low-intensity shockwave therapy for patients with erectile dysfunction | Conditional recommendation, low levels of certainty in evidence |
| 3. Among patients with erectile dysfunction and a hypogonadal testosterone level, should testosterone replacement be used as monotherapy compared to no treatment? | |
| We suggest against the use of testosterone as monotherapy for patients with erectile dysfunction and a hypogonadal testosterone level | Conditional recommendation, low levels of certainty in evidence |
| 4. Among patients with erectile dysfunction, does increasing physical activity improve erectile function compared to usual activity? | |
| We suggest increasing physical activity, rather than usual activity, among patients with erectile dysfunction | Conditional recommendation, low levels of certainty in evidence |
| 5. Among patients with post-prostatectomy erectile dysfunction, should penile rehabilitation with scheduled PDE5 inhibitor be used over no intervention? | |
| We suggest against the use of scheduled PDE5 inhibitor for penile rehabilitation among patients with post-prostatectomy erectile dysfunction | Conditional recommendation, low levels of certainty in evidence |
1. Among patients with ED, should daily tadalafil be preferentially prescribed instead of on-demand tadalafil?
Based on the available evidence, the panel conditionally recommends against preferentially prescribing daily tadalafil instead of on-demand tadalafil for patients presenting with ED. However, certain patient-centered factors may influence what dosing regimen the patient ultimately decides to pursue.
The panel reviewed eight RCTs73–80 comparing improvement in erectile function between on-demand tadalafil (n=749) and daily tadalafil (n=749) over a followup period of 8–12 weeks. The meta-analysis demonstrates a mean increase in the IIEF-EF score of 0.8 (95% CI −0.32, 1.93), favoring daily tadalafil, with a moderate certainty of evidence. This small difference is not clinically significant. Additionally, pooled analyses of 17 on-demand and four daily tadalafil placebo-controlled trials demonstrated both treatment regimens are similarly efficacious across a broad spectrum of clinical subgroups.81 Based on RCT data, there is virtually no meaningful difference in side effects or discontinuation rates between either dosing regimen.
Patient-centered factors influencing daily dosing preference
Although treatment efficacy and side effect profiles are very similar between on-demand and daily tadalafil, certain patient-centered factors need to be considered when a decision on dosing frequency is made with the patient. Numerous studies have shown that daily tadalafil increases sexual spontaneity, improves sexual self-confidence, and there is less of a concern regarding timing of medication and the associated anticipatory anxiety that can be experienced in some patients taking on-demand tadalafil.76,79,82 A study by Conaglen and colleagues found that female partners preferred daily dosing compared to on-demand regimens.83 In patients experiencing comorbid lower urinary tract symptoms, daily tadalafil (5 mg) is an approved treatment option and has been shown to decrease symptom scores significantly more than on-demand dosing.78 Additionally, daily tadalafil may be more cost-effective than on-demand dosing, depending on the frequency of use and whether a low (2.5 mg) or high (5 mg) daily dose regimen is required to achieve an adequate erection.
2. Among patients with ED, should Li-SWT be recommended over no treatment?
Based on the available evidence, the panel conditionally recommends against Li-SWT as a treatment for patients with ED at this time.
The panel reviewed seven RCTs84–90 comparing improvement in erectile function between patients treated with Li-SWT (n=293) or a sham treatment (n=202). The studies had different treatment protocols (shockwave machines, energy levels, duration of treatment, and schedule of treatments), various sham treatments, inconsistent followup timing, short followup, and varying metrics, resulting in significant heterogeneity between the studies. Combining the results of all seven RCTs demonstrates a mean increase in the IIEF-EF score of 4.08 (95% CI 1.57, 6.58) with a very low certainty of evidence, given that three trials84,86,90 have a high risk of bias. If these three studies are removed, combining the results of the remaining four studies results in a mean increase in the IIEF-EF score of 2.07 (95% CI 0.19, 3.96) with a moderate certainty of evidence. Given the quality of the evidence, the panel has more confidence in this latter result, indicating that Li-SWT is unlikely to have a noticeable clinical improvement in erectile function.
Fojecki and colleagues88 collected quality of life data using the Sexual Quality of Life for Men (SQoL-M) tool91 in their study of 118 patients. Given the crossover design, the sham group had received five penile Li-SWT treatments compared to 10 in the treatment arm at the 18-week mark when the SQoL-M was re-administered after baseline. The Li-SWT arm scored 2.1 points higher (95% CI −7.9, 12.1) than the sham group with a very low certainty of the evidence, indicating no significant improvement in sexual quality of life between 10 vs. five Li-SWT treatments.
Li-SWT is believed to be a safe procedure with virtually no short-term adverse effects92,93 reported, but more research is required to assess the possibility of longer-term adverse effects.
Concerns of introducing Li-SWT into the Canadian healthcare setting
Given the trivial desirable effects on erectile function, the uncertainty regarding the evidence and long-term effects, and concerns regarding cost-effectiveness, equity, and feasibility to deliver this treatment in the Canadian healthcare setting, the panel decided to conditionally recommend against Li-SWT for the treatment of ED at this time. Further adequately powered RCTs focusing on patient safety and more efforts to define the dose, type of machine, and patient populations most likely to benefit are required. Additionally, longer-term clinical efficacy using validated and standardized protocols needs to be established before this modality should be offered to men with ED outside of a clinical trial.
3. Among patients with ED and a hypogonadal testosterone level, should testosterone replacement be used as monotherapy compared to no treatment?
Based on the available evidence, the panel conditionally recommends against using testosterone as monotherapy to improve erectile function in patients with a hypogonadal testosterone level.
Testosterone replacement is the mainstay of therapy for patients with a hypogonadal level of testosterone and symptoms consistent with testosterone deficiency syndrome (TDS), as outlined in other clinical guidelines.94 Patients initiating testosterone therapy need to be informed of both the potential benefits and risks of treatment, including side effects and serious adverse events. Testosterone therapy improves overall sexual function and sexual quality of life in patients with TDS,95 however, the panel wanted to address the specific question of whether testosterone therapy alone improved erectile function in patients with low testosterone levels.
The panel reviewed six RCTs96–101 that randomized hypogonadal patients with ED to treatment with testosterone replacement (n=457) or placebo (n=459) and compared improvement in erectile function between these two arms. The followup period in these studies ranged from 3–12 months. The baseline testosterone level to be enrolled in the studies differed (range <8 to <15 nmol/L) and there was some heterogeneity in the testosterone replacement regimens used, with four studies using testosterone gel at 50 mg/d,97,98,100,101 one study using a testosterone patch at 50 mg/d,96 and one study using intramuscular (IM) testosterone undecanoate 1000 mg/12 weeks.99 Additionally, these studies did not routinely report what the testosterone levels were at the end of the study. Despite the heterogeneity and methodological considerations, these six RCTs were chosen because they had the least risk of bias among other RCTs published on this topic. Our meta-analysis demonstrates a mean increase in IIEF-EF score of 2.65 (95% CI 0.81, 4.48) with testosterone therapy compared to placebo with a moderate certainty in evidence, indicating testosterone therapy alone unlikely leads to a clinically significant improvement in erectile function in this patient population. These findings are similar to the meta-analysis conducted by Corona and colleagues, which included six studies only including participants with a baseline testosterone level below 8 nmol/L.95 In this meta-analysis, the mean increase in IIEF-EF score is 2.95 (95% CI 1.86, 4.03), which remains below the MCID.
Dual PDE5i and testosterone therapy
While current evidence does not support the use of testosterone as monotherapy for the treatment of ED in patients with a hypogonadal testosterone level, there is some evidence to supports its use as a combination therapy to salvage patients who have failed PDE5is. Numerous non-controlled trials have shown promising results, especially in patients with lower testosterone levels. However, the degree of erectile function improvement is not as profound in controlled trials.102,103 Three RCTs104–106 randomized 326 PDE5 inhibitor non-responders with low to low-normal testosterone levels to combination treatment with either testosterone or placebo over a followup period ranging from 4–16 weeks. The meta-analysis of these three trials demonstrated a mean increase in the IIEF-EF score of 1.68 (95% CI 0.30, 3.07) favoring testosterone combination therapy with a low certainty of evidence. Given this uncertainty, sufficiently powered controlled trials with longer followup are required to definitely address this claim.
4. Among patients with ED, does increasing physical activity improve erectile function compared to usual activity?
Based on the available evidence, the panel conditionally recommends for patients to increase their physical activity to improve their erectile function.
The panel reviewed five RCTs107–111 comparing improvement of erectile function between patients continuing their regular physical activity level (n=149) or an increased physical activity level (n=217) over a followup period ranging from 2–24 months. In addition to ED, participants in the RCTs also had obesity,107 ischemic heart disease,108 hypertension,109 and metabolic syndrome.111 Two studies treated both the intervention and control arms with PDE5is as part of the study design.110,111 The exact prescribed physical activity and exercise routines differed among the trials, however, the goal in each trial was to increase exercise tolerance through aerobic and/or resistance training. The meta-analysis demonstrates a mean increase in the IIEF-EF score of 3.77 (95% CI 2.04, 5.50), favoring an increased physical activity level, with a low certainty of evidence. Although the improvement in IIEF-EF score is borderline for clinical significance, the safety, relatively low cost, wide accessibility, and acceptability of physical activity in the general population influenced the panel to conditionally recommend an increase in physical activity in the ED population. There is a linear relationship between physical activity and overall health status and regular physical activity is a proven primary and secondary prevention strategy in numerous medical conditions, many of which are also associated with ED.112
5. Among patients with post-prostatectomy ED, should penile rehabilitation with scheduled PDE5is be used over no intervention?
Based on the available evidence, the panel conditionally recommends against penile rehabilitation with scheduled PDE5is following radical prostatectomy (RP).
Sexual dysfunction is a significant survivorship concern impacting patients undergoing localized treatment for prostate cancer, with the vast majority of patients having some functional impact after treatment despite advancements in surgical technique. Recovery of erectile function is dependent on both treatment and patient-related factors, and a subset of patients will not experience recovery.19,113 Penile rehabilitation is the concept of using interventions to promote the natural recovery of erectile function after an insult to the erectile mechanism, which occurs after RP, external beam radiation therapy (EBRT), brachytherapy, and other localized prostate cancer treatments. Although there is controversy surrounding the utility and ways to perform penile rehabilitation,114 most studies focus on scheduled PDE5is for variable periods of time leading up to and following RP.
In the post-RP population, the panel reviewed five RCTs80,115–118 that randomized patients to placebo or no treatment (n=372) or to scheduled PDE5-is (n=385) and compared erectile function restoration rates. The followup period in these studies ranged from 24–48 weeks. Given methodological issues with these studies leading to a very low certainty of the evidence, the pooled effect estimate suggests that in every 1000 patients who receive penile rehabilitation with scheduled PDE5is, only 28 more patients (95% CI 50 fewer, 138 more) experienced ED resolution compared to placebo, which is not statistically significant (relative risk [RR] 1.11 [95% CI: 0.80, 1.55]).
Sexual quality of life was assessed using the Expanded Prostate Cancer Index Composite (sexual domain) in Montorsi’s scheduled tadalafil vs. placebo RCT (n=280) and the results suggest little to no difference compared to placebo after the cessation of active therapy.80
Serious adverse events and treatment discontinuation due to any cause (RR 0.98, 95% CI 0.72, 1.34) did not significantly differ between scheduled PDE5-inhibitor and placebo in two RCTs (n=403) that addressed this,80, 118 albeit the certainty of evidence is very low.
Penile rehabilitation post-radiotherapy
There is insufficient evidence for the panel to make any recommendation for penile rehabilitation following treatment with EBRT and brachytherapy for prostate cancer. Radiation damage affects the erectile mechanism differently than surgical injury, with the pathophysiological factors leading to ED being more cumulative and delayed with radiation.119 Despite this, proponents of penile rehabilitation believe scheduled PDE5is may limit the damage radiation causes in vascular and cavernous tissues. Scheduled PDE5is after EBRT have been shown to be efficacious in the short-term after radiation therapy, with three RCTs120–122 demonstrating a cumulative increase in IIEF-EF score of 6.10 (95% CI 4.69, 7.52) compared to placebo after six weeks of treatment. These studies did not assess longer-term erectile function rates or the protective effect of PDE5is. A small trial of 27 patients compared daily sildenafil treatment taken for six months around the time of prostate brachytherapy (n=14) vs. placebo (n=13) and this trial failed to show an improvement in erectile function at one and two years following treatment.123 A larger RCT by Zelefsky and colleagues124 had a similar trial design but included men with EBRT and brachytherapy, and although patients previously receiving the six months of scheduled sildenafil demonstrated higher median erectile function scores at 12 months following therapy (26 vs. 21.5, p=0.018), the median IIEF-EF of both arms was identical at 25 at the two-year mark. Although there is insufficient data to make a recommendation, limited evidence suggests that scheduled PDE5is taken around the time of radiation therapy (EBRT and/or brachytherapy) do not offer any long-term protective effects against future ED.
Future directions requiring further study
As technology evolves and a further understanding of the pathophysiological processes contributing to ED develops, we can expect that treatment options to improve erectile function will continue to advance. Regenerative therapies aim to restore the structure and function of the erectile tissue and offer a “cure” to the disease process as opposed to merely treating the symptoms of ED.125 Preclinical and early human studies have explored regenerative approaches for treating ED, such as stem cell therapy (SCT), platelet rich plasma (PRP), and amniotic fluid matrices. However, these options are currently not approved for use outside of clinical trials and remain experimental.125,126
Stem cell therapy
Stem cells function to release growth factors, cytokines, and chemokines in a paracrine fashion to promote wound healing and rebuild damaged tissues.127 There have been several small phase 1–3 human trials evaluating SCT for treating ED, but there is significant variability between protocols, inadequate adverse event reporting, and a lack of long-term followup.128–131
Platelet-rich plasma
Platelet-rich plasma (PRP) is autologous blood plasma that contains supraphysiologic platelet concentrations132 and numerous growth factors implicated in erection recovery.133 Penile bruising is common after injection and the protocol for injections and growth factor activation is not well-studied or universally accepted. Despite the global use of PRP to treat ED, there are a limited number of peer-reviewed human studies to support this experimental regenerative therapy.134
Amniotic fluid matrices
Dehydrated human amnion/chorion membranes have been applied to cavernous nerves during RP as a source of implantable neurotrophic factors, growth factors, cytokines, proteases, and inhibitors of inflammatory and fibrotic pathways.125,135 Limited human studies have applied these grafts during robotic-assisted RP with promising clinical outcomes of expedited recovery in erectile function.136,137 The long-term efficacy, side effects, and oncological consequences of these grafts are unknown at this time and require future study.
Limitations and unanswered questions
This guideline primarily focused on patients with ED as a single presenting symptom. However, patients presenting with ED often have other concurrent elements of sexual dysfunction (low libido, orgasmic dysfunction, ejaculatory dysfunction), PD, testosterone deficiency, lower urinary tract symptoms/BPH, prostatitis/pelvic pain, psychological or psychiatric conditions, and other medical problems (neurological, gastrointestinal) that influence both their erectile function directly, and more broadly, quality of life as it relates to sexual function. Due to the complexity of the interactions between these factors and the lack of comprehensive studies assessing all of these factors together, the panel was not able to provide recommendations that address the impact these factors have, individually or collectively, on ED therapy. Therefore, the recommendations in this guideline need to be contextualized based on the patient’s history and presenting symptoms and conditions that may be influencing sexual function in its entirety.
Given the methodology of ED therapeutic trial design, most studies referenced in this guideline compare an intervention to placebo and don’t assess combination therapy. Synergistic effects of multiple treatments are not specifically addressed in this guideline, however, may be appropriate depending on the clinical scenario.
It is well-known that the MCID in erectile function score depends on initial ED severity, with greater improvements in IIEF-EF score necessary for satisfactory results in patients with more severe ED.35 Moreover, the underlying cause of ED may impact treatment response depending on its mechanism of action. Given the methodological challenges in data reporting, including the lack of power and routine reporting of underlying ED etiology, the vast majority of studies do not perform subgroup analyses based on either severity of ED or on the primary cause of ED.17 This limitation significantly impacts the panel’s ability to make recommendations for specific subgroups of patients with ED based on the current literature.
The panel identified several deficits in the body of literature focussing on ED assessment and treatment, including a lack of quality-of-life metrics, patient-reported outcomes other than erectile function, assessment of partner satisfaction, and a lack of harms data (particularly for some treatments). This made it challenging for the panel to comment on some of the a priori outcomes that were felt to be important when a patient has to make an ED treatment decision. Hopefully, future ED studies include these important measures in their design.
Conclusions
These guidelines were developed using transparent and rigorous methods to provide the healthcare community with the most current data and recommendations regarding ED patient assessment and treatment through the Canadian lens. Special attention was taken to provide clarity on the most controversial aspects of ED treatment in Canada today.
Evaluating a patient with ED requires a sufficiently detailed yet focussed history and physical exam to establish an etiological working diagnosis. Reversible factors contributing to ED should be identified and corrected, including promoting positive lifestyle changes that optimize overall health. In patients requesting treatment, it is reasonable to begin with conservative and less invasive therapies and introduce additional therapeutic measures when necessary, through a shared decision-making process with the patient and their partner.
Supplementary Information
Footnotes
Appendix available at cuaj.ca
See related commentary on page 323
Competing interests: Dr. Flannigan has been an advisory board member for Acerus; has received honoraria for speaking and educating from Boston Scientific and Paladin Labs; and participated in a clinical trial on the injection of novel lidocaine polymer for chronic scrotal pain supported by Sustained Therapeutics. Dr. Patel has been an advisory board member for Aytu Biosciences; a consultant for Boston Scientific and Nestle Health; and gave a talk on men’s health for Boston Scientific and Paladin. Dr. Krakowsky has been an advisory board member for Acerus, Felix, Paladin, Pfizer, Sprout, and Verity. Dr. Brock has been an advisory board member for and holds investments in Boston Scientific. Dr. Yafi has been a consultant/speaker for Acerus, Antares Pharma, Clarus Therapeutics, Coloplast, and Cynosure; an advisory board member for Coloplast, Cynosure, and Promescent; and received a research grant from Viome. No other author or reviewer reports any competing personal or financial interests related to this work.
References
- 1.Gratzke C, Angulo J, Chitaley K, et al. Anatomy, physiology, and pathophysiology of erectile dysfunction. J Sex Med. 2010;7:445–75. doi: 10.1111/j.1743-6109.2009.01624.x. [DOI] [PubMed] [Google Scholar]
- 2.Canadian Diabetes Association Clinical Practice Guidelines Expert C. Brock G, Harper W. Erectile dysfunction. Can J Diabetes. 2013;37(Suppl 1):S150–2. doi: 10.1016/j.jcjd.2013.01.041. [DOI] [PubMed] [Google Scholar]
- 3.Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J Urol. 1994;151:54–61. doi: 10.1016/s0022-5347(17)34871-1. [DOI] [PubMed] [Google Scholar]
- 4.Rosen RC. Psychogenic erectile dysfunction. Classification and management. Urol Clin North Am. 2001;28:269–78. doi: 10.1016/s0094-0143(05)70137-3. [DOI] [PubMed] [Google Scholar]
- 5.Vlachopoulos CV, Terentes-Printzios DG, Ioakeimidis NK, et al. Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: A systematic review and meta-analysis of cohort studies. Circ Cardiovasc Qual Outcomes. 2013;6:99–109. doi: 10.1161/CIRCOUTCOMES.112.966903. [DOI] [PubMed] [Google Scholar]
- 6.Corona G, Petrone L, Mannucci E, et al. Assessment of the relational factor in male patients consulting for sexual dysfunction: The concept of couple sexual dysfunction. J Androl. 2006;27:795–801. doi: 10.2164/jandrol.106.000638. [DOI] [PubMed] [Google Scholar]
- 7.Salonia A, Castagna G, Sacca A, et al. Is erectile dysfunction a reliable proxy of general male health status? The case for the International Index of Erectile Function-Erectile Function domain. J Sex Med. 2012;9:2708–15. doi: 10.1111/j.1743-6109.2012.02869.x. [DOI] [PubMed] [Google Scholar]
- 8.Ewane KA, Lin HC, Wang R. Should patients with erectile dysfunction be evaluated for cardiovascular disease? Asian J Androl. 2012;14:138–44. doi: 10.1038/aja.2011.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Inman BA, Sauver JL, Jacobson DJ, et al. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clin Proc. 2009;84:108–13. doi: 10.4065/84.2.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Araujo AB, Hall SA, Ganz P, et al. Does erectile dysfunction contribute to cardiovascular disease risk prediction beyond the Framingham risk score? J Am Coll Cardiol. 2010;55:350–6. doi: 10.1016/j.jacc.2009.08.058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dong JY, Zhang YH, Qin LQ. Erectile dysfunction and risk of cardiovascular disease: Meta-analysis of prospective cohort studies. J Am Coll Cardiol. 2011;58:1378–85. doi: 10.1016/j.jacc.2011.06.024. [DOI] [PubMed] [Google Scholar]
- 12.Gandaglia G, Briganti A, Jackson G, et al. A systematic review of the association between erectile dysfunction and cardiovascular disease. Eur Urol. 2014;65:968–78. doi: 10.1016/j.eururo.2013.08.023. [DOI] [PubMed] [Google Scholar]
- 13.Chew KK, Finn J, Stuckey B, et al. Erectile dysfunction as a predictor for subsequent atherosclerotic cardiovascular events: findings from a linked-data study. J Sex Med. 2010;7:192–202. doi: 10.1111/j.1743-6109.2009.01576.x. [DOI] [PubMed] [Google Scholar]
- 14.Feng C, Xu YM, Barbagli G, et al. The relationship between erectile dysfunction and open urethroplasty: A systematic review and meta-analysis. J Sex Med. 2013;10:2060–8. doi: 10.1111/jsm.12181. [DOI] [PubMed] [Google Scholar]
- 15.Johnsen NV, Kaufman MR, Dmochowski RR, et al. Erectile dysfunction following pelvic fracture uethral injury. Sex Med Rev. 2018;6:114–23. doi: 10.1016/j.sxmr.2017.06.004. [DOI] [PubMed] [Google Scholar]
- 16.El-Assmy A, El-Tholoth HS, Abou-El-Ghar ME, et al. Risk factors of erectile dysfunction and penile vascular changes after surgical repair of penile fracture. Int J Impot Res. 2012;24:20–5. doi: 10.1038/ijir.2011.41. [DOI] [PubMed] [Google Scholar]
- 17.Capogrosso P, Pozzi EP, Celentano V, et al. Erectile recovery after radical pelvic surgery: Methodological challenges and recommendations for data reporting. J Sex Med. 2020;17:7–16. doi: 10.1016/j.jsxm.2019.09.013. [DOI] [PubMed] [Google Scholar]
- 18.Gaither TW, Awad MA, Osterberg EC, et al. The natural history of erectile dysfunction after prostatic radiotherapy: A systematic review and meta-analysis. J Sex Med. 2017;14:1071–8. doi: 10.1016/j.jsxm.2017.07.010. [DOI] [PubMed] [Google Scholar]
- 19.Resnick MJ, Koyama T, Fan KH, et al. Long-term functional outcomes after treatment for localized prostate cancer. N Engl J Med. 2013;368:436–45. doi: 10.1056/NEJMoa1209978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Seftel AD, de la Rosette J, Birt J, et al. Coexisting lower urinary tract symptoms and erectile dysfunction: A systematic review of epidemiological data. Int J Clin Pract. 2013;67:32–45. doi: 10.1111/ijcp.12044. [DOI] [PubMed] [Google Scholar]
- 21.Li HJ, Kang DY. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: A meta-analysis. World J Urol. 2016;34:1009–17. doi: 10.1007/s00345-015-1720-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chevret M, Jaudinot E, Sullivan K, et al. Impact of erectile dysfunction (ED) on sexual life of female partners: Assessment with the Index of Sexual Life (ISL) questionnaire. J Sex Marital Ther. 2004;30:157–72. doi: 10.1080/00926230490262366. [DOI] [PubMed] [Google Scholar]
- 23.Korfage IJ, Pluijm S, Roobol M, et al. Erectile dysfunction and mental health in a general population of older men. J Sex Med. 2009;6:505–12. doi: 10.1111/j.1743-6109.2008.01111.x. [DOI] [PubMed] [Google Scholar]
- 24.Colson MH. Couple, ways of couples coping, and erectile dysfunction. Gynecol Obstet Fertil. 2007;35:129–34. doi: 10.1016/j.gyobfe.2006.10.034. [DOI] [PubMed] [Google Scholar]
- 25.Fisher WA, Eardley I, McCabe M, et al. Erectile dysfunction (ED) is a shared sexual concern of couples II: Association of female partner characteristics with male partner ED treatment seeking and phosphodiesterase type 5 inhibitor utilization. J Sex Med. 2009;6:3111–24. doi: 10.1111/j.1743-6109.2009.01432.x. [DOI] [PubMed] [Google Scholar]
- 26.Li H, Gao T, Wang R. The role of the sexual partner in managing erectile dysfunction. Nat Rev Urol. 2016;13:168–77. doi: 10.1038/nrurol.2015.315. [DOI] [PubMed] [Google Scholar]
- 27.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–6. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Alonso-Coello P, Schunemann HJ, Moberg J, et al. GRADE evidence to decision (EtD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016;353:i2016. doi: 10.1136/bmj.i2016. [DOI] [PubMed] [Google Scholar]
- 29.Guyatt GH, Oxman AD, Kunz R, et al. What is “quality of evidence” and why is it important to clinicians? BMJ. 2008;336:995–8. doi: 10.1136/bmj.39490.551019.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–6. doi: 10.1016/j.jclinepi.2010.07.015. [DOI] [PubMed] [Google Scholar]
- 31.Alonso-Coello P, Oxman AD, Moberg J, et al. GRADE evidence to decision (EtD) frameworks: A systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016;353:i2089. doi: 10.1136/bmj.i2089. [DOI] [PubMed] [Google Scholar]
- 32.Guyatt GH, Oxman AD, Santesso N, et al. GRADE guidelines: 12. Preparing summary of findings tablesbinary outcomes. J Clin Epidemiol. 2013;66:158–72. doi: 10.1016/j.jclinepi.2012.01.012. [DOI] [PubMed] [Google Scholar]
- 33.Guyatt GH, Thorlund K, Oxman AD, et al. GRADE guidelines: 13. Preparing summary of findings tables and evidence profiles-continuous outcomes. J Clin Epidemiol. 2013;66:173–83. doi: 10.1016/j.jclinepi.2012.08.001. [DOI] [PubMed] [Google Scholar]
- 34.Rosen RC, Cappelleri JC, Gendrano N., 3rd The International Index of Erectile Function (IIEF): A stateof-the-science review. Int J Impot Res. 2002;14:226–44. doi: 10.1038/sj.ijir.3900857. [DOI] [PubMed] [Google Scholar]
- 35.Rosen RC, Allen KR, Ni X, et al. Minimal clinically important differences in the erectile function domain of the International Index of Erectile Function scale. Eur Urol. 2011;60:1010–6. doi: 10.1016/j.eururo.2011.07.053. [DOI] [PubMed] [Google Scholar]
- 36.Park BY, Wilson G, Berger J, et al. Is internet pornography causing sexual dysfunctions? A review with clinical reports. Behav Sci (Basel) 2016:6. doi: 10.3390/bs6030017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Grubbs JB, Gola M. Is pornography use related to erectile functioning? Results from cross-sectional and latent growth curve analyses. J Sex Med. 2019;16:111–25. doi: 10.1016/j.jsxm.2018.11.004. [DOI] [PubMed] [Google Scholar]
- 38.Landripet I, Stulhofer A. Is pornography use associated with sexual difficulties and dysfunctions among younger heterosexual men? J Sex Med. 2015;12:1136–9. doi: 10.1111/jsm.12853. [DOI] [PubMed] [Google Scholar]
- 39.Montorsi F, Adaikan G, Becher E, et al. Summary of the recommendations on sexual dysfunctions in men. J Sex Med. 2010;7:3572–88. doi: 10.1111/j.1743-6109.2010.02062.x. [DOI] [PubMed] [Google Scholar]
- 40.Coyne K, Mandalia S, McCullough S, et al. The International Index of Erectile Function: Development of an adapted tool for use in HIV-positive men who have sex with men. J Sex Med. 2010;7:769–74. doi: 10.1111/j.1743-6109.2009.01579.x. [DOI] [PubMed] [Google Scholar]
- 41.Ghanem HM, Salonia A, Martin-Morales A. SOP: Physical examination and laboratory testing for men with erectile dysfunction. J Sex Med. 2013;10:108–10. doi: 10.1111/j.1743-6109.2012.02734.x. [DOI] [PubMed] [Google Scholar]
- 42.Elhanbly S, Elkholy A. Nocturnal penile erections: The role of RigiScan in the diagnosis of vascular erectile dysfunction. J Sex Med. 2012;9:3219–26. doi: 10.1111/j.1743-6109.2012.02954.x. [DOI] [PubMed] [Google Scholar]
- 43.Sikka SC, Hellstrom WJ, Brock G, et al. Standardization of vascular assessment of erectile dysfunction: Standard operating procedures for duplex ultrasound. J Sex Med. 2013;10:120–9. doi: 10.1111/j.1743-6109.2012.02825.x. [DOI] [PubMed] [Google Scholar]
- 44.Bella AJ, Lee JC, Carrier S, et al. 2015 CUA Practice guidelines for erectile dysfunction. Can Urol Assoc J. 2015;9:23–9. doi: 10.5489/cuaj.2699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Burnett AL, Nehra A, Breau RH, et al. Erectile dysfunction: AUA guideline. J Urol. 2018;200:633–41. doi: 10.1016/j.juro.2018.05.004. [DOI] [PubMed] [Google Scholar]
- 46.Silva AB, Sousa N, Azevedo LF, et al. Physical activity and exercise for erectile dysfunction: Systematic review and meta-analysis. Br J Sports Med. 2017;51:1419–24. doi: 10.1136/bjsports-2016-096418. [DOI] [PubMed] [Google Scholar]
- 47.Allen MS, Walter EE. Health-related lifestyle factors and sexual dysfunction: A meta-analysis of populationbased research. J Sex Med. 2018;15:458–75. doi: 10.1016/j.jsxm.2018.02.008. [DOI] [PubMed] [Google Scholar]
- 48.Pizzol D, Demurtas J, Stubbs B, et al. Relationship between cannabis use and erectile dysfunction: A systematic review and meta-analysis. Am J Mens Health. 2019;13:1557988319892464. doi: 10.1177/1557988319892464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Rhim HC, Kim MS, Park YJ, et al. The potential role of arginine supplements on erectile dysfunction: A systemic review and meta-analysis. J Sex Med. 2019;16:223–34. doi: 10.1016/j.jsxm.2018.12.002. [DOI] [PubMed] [Google Scholar]
- 50.El Taieb M, Hegazy E, Ibrahim A. Daily oral l-arginine plus tadalafil in diabetic patients with erectile dysfunction: A double-blinded, randomized, controlled clinical trial. J Sex Med. 2019;16:1390–7. doi: 10.1016/j.jsxm.2019.06.009. [DOI] [PubMed] [Google Scholar]
- 51.El-Wakeel LM, Fouad FA, Saleem MD, et al. Efficacy and tolerability of sildenafil/l-arginine combination relative to sildenafil alone in patients with organic erectile dysfunction. Andrology. 2020;8:143–7. doi: 10.1111/andr.12671. [DOI] [PubMed] [Google Scholar]
- 52.Andersson E, Walén C, Hallberg J, et al. A randomized controlled trial of guided internet-delivered cognitive behavioral therapy for erectile dysfunction. J Sex Med. 2011;8:2800–9. doi: 10.1111/j.1743-6109.2011.02391.x. [DOI] [PubMed] [Google Scholar]
- 53.Titta M, Tavolini IM, Dal Moro F, et al. Sexual counseling improved erectile rehabilitation after non-nerve-sparing radical retropubic prostatectomy or cystectomy—results of a randomized prospective study. J Sex Med. 2006;3:267–73. doi: 10.1111/j.1743-6109.2006.00219.x. [DOI] [PubMed] [Google Scholar]
- 54.Banner LL, Anderson RU. Integrated sildenafil and cognitive-behavior sex therapy for psychogenic erectile dysfunction: a pilot study. J Sex Med. 2007;4:1117–25. doi: 10.1111/j.1743-6109.2007.00535.x. [DOI] [PubMed] [Google Scholar]
- 55.Qiu X, Lin G, Xin Z, et al. Effects of low-energy shockwave therapy on the erectile function and tissue of a diabetic rat model. J Sex Med. 2013;10:738–46. doi: 10.1111/jsm.12024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Campbell JD, Burnett AL. Neuroprotective and nerve-regenerative approaches for treatment of erectile dysfunction after cavernous nerve injury. Int J Mol Sci. 2017;18 doi: 10.3390/ijms18081794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Goldenberg MM. Safety and efficacy of sildenafil citrate in the treatment of male erectile dysfunction. Clin Ther. 1998;20:1033–48. doi: 10.1016/s0149-2918(98)80103-3. [DOI] [PubMed] [Google Scholar]
- 58.Huang SA, Lie JD. Phosphodiesterase-5 (PDE5) inhibitors in the management of erectile dysfunction. P T. 2013;38:407–19. [PMC free article] [PubMed] [Google Scholar]
- 59.Doggrell S. Do vardenafil and tadalafil have advantages over sildenafil in the treatment of erectile dysfunction? Int J Impot Res. 2007;19:281–95. doi: 10.1038/sj.ijir.3901525. [DOI] [PubMed] [Google Scholar]
- 60.Park NC, Kim TN, Park HJ. Treatment strategy for non-responders to PDE5 inhibitors. World J Mens Health. 2013;31:31–5. doi: 10.5534/wjmh.2013.31.1.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Yuan J, Zhang R, Yang Z, et al. Comparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: A systematic review and network meta-analysis. Eur Urol. 2013;63:902–12. doi: 10.1016/j.eururo.2013.01.012. [DOI] [PubMed] [Google Scholar]
- 62.Fulgham PF, Cochran JS, Denman JL, et al. Disappointing initial results with transurethral alprostadil for erectile dysfunction in a urology practice setting. J Urol. 1998;160:2041–6. doi: 10.1097/00005392-199812010-00028. [DOI] [PubMed] [Google Scholar]
- 63.Guay AT, Perez JB, Velasquez E, et al. Clinical experience with intraurethral alprostadil (MUSE) in the treatment of men with erectile dysfunction. A retrospective study. Medicated urethral system for erection. Eur Urol. 2000;38:671–6. doi: 10.1159/000020360. [DOI] [PubMed] [Google Scholar]
- 64.Urciuoli R, Cantisani TA, Carlini M, et al. Prostaglandin E1 for treatment of erectile dysfunction. Cochrane Database Syst Rev. 2004;(2):CD001784. doi: 10.1002/14651858.CD001784.pub2. [DOI] [PubMed] [Google Scholar]
- 65.Bosshardt RJ, Farwerk R, Sikora R, et al. Objective measurement of the effectiveness, therapeutic success and dynamic mechanisms of the vacuum device. Br J Urol. 1995;75:786–91. doi: 10.1111/j.1464-410x.1995.tb07392.x. [DOI] [PubMed] [Google Scholar]
- 66.Witherington R. Vacuum constriction device for management of erectile impotence. J Urol. 1989;141:320–2. doi: 10.1016/s0022-5347(17)40752-x. [DOI] [PubMed] [Google Scholar]
- 67.Linet OI, Ogrinc FG. Efficacy and safety of intracavernosal alprostadil in men with erectile dysfunction. The Alprostadil Study Group. N Engl J Med. 1996;334:873–7. doi: 10.1056/NEJM199604043341401. [DOI] [PubMed] [Google Scholar]
- 68.Govier FE, McClure RD, Weissman RM, et al. Experience with triple-drug therapy in a pharmacological erection program. J Urol. 1993;150:1822–4. doi: 10.1016/s0022-5347(17)35905-0. [DOI] [PubMed] [Google Scholar]
- 69.Domes T, Chung E, DeYoung L, et al. Clinical outcomes of intracavernosal injection in postprostatectomy patients: A single-center experience. Urology. 2012;79:150–5. doi: 10.1016/j.urology.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 70.Lledo-Garcia E, Jara-Rascon J, Moncada Iribarren I, et al. Penile prosthesis first and replacement surgeries: Analysis of patient and partner satisfaction. J Sex Med. 2015;12:1646–53. doi: 10.1111/jsm.12932. [DOI] [PubMed] [Google Scholar]
- 71.Bennett N, Henry G, Karpman E, et al. Inflatable penile prosthesis implant length with baseline characteristic correlations: preliminary analysis of the PROPPER study. Transl Androl Urol. 2017;6:1167–74. doi: 10.21037/tau.2017.12.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Chierigo F, Capogrosso P, Deho F, et al. Long-term followup after penile prosthesis implantation—survival and quality of life outcomes. J Sex Med. 2019;16:1827–33. doi: 10.1016/j.jsxm.2019.08.001. [DOI] [PubMed] [Google Scholar]
- 73.McMahon C. Comparison of efficacy, safety, and tolerability of on-demand tadalafil and daily dosed tadalafil for the treatment of erectile dysfunction. J Sex Med. 2005;2:415–25. doi: 10.1111/j.1743-6109.2005.20360.x. ; discussion 25–7. [DOI] [PubMed] [Google Scholar]
- 74.Ciammella P, Badellino S, Botticella A, et al. 7012 Evaluation of the efficacy and safety of tadalafil 20 mg on demand vs. tadalafil 5 mg once a day in the treatment of erectile dysfunction following curative radiotherapy for prostatic carcinoma: Preliminary results of a randomized, phase 2 trial. Eur J Cancer Suppl. 2009;7:410. doi: 10.1016/S1359-6349(09)71390-4. [DOI] [Google Scholar]
- 75.Ricardi U, Gontero P, Ciammella P, et al. Efficacy and safety of tadalafil 20 mg on demand vs. tadalafil 5 mg once a day in the treatment of post-radiotherapy erectile dysfunction in prostate cancer men: A randomized, phase 2 trial. J Sex Med. 2010;7:2851–9. doi: 10.1111/j.1743-6109.2010.01890.x. [DOI] [PubMed] [Google Scholar]
- 76.Rubio-Aurioles E, Porst H, Kim ED, et al. A randomized open-label trial with a crossover comparison of sexual self-confidence and other treatment outcomes following tadalafil once a day vs. tadalafil or sildenafil on-demand in men with erectile dysfunction. J Sex Med. 2012;9:1418–29. doi: 10.1111/j.1743-6109.2012.02667.x. [DOI] [PubMed] [Google Scholar]
- 77.Jamshidian H, Borhan A, Kooraki S, et al. Evaluation of the efficacy of once-daily use of tadalafil vs. on-demand use. Is there a cumulative effect? J Pak Med Assoc. 2012;62:1195–8. [PubMed] [Google Scholar]
- 78.Kang DH, Lee JY, Chung JH, et al. Comparison of efficacy for erectile function and lower urinary tract symptoms of tadalafil 20 mg on-demand and 5 mg once daily in patients with erectile dysfunction. Int J Clin Pract. 2012;66:813–20. doi: 10.1111/j.1742-1241.2012.02946.x. [DOI] [PubMed] [Google Scholar]
- 79.Hatzimouratidis K, Buvat J, Buttner H, et al. Psychosocial outcomes after initial treatment of erectile dysfunction with tadalafil once daily, tadalafil on demand or sildenafil citrate on demand: Results from a randomized, open-label study. Int J Impot Res. 2014;26:223–9. doi: 10.1038/ijir.2014.15. [DOI] [PubMed] [Google Scholar]
- 80.Montorsi F, Brock G, Stolzenburg JU, et al. Effects of tadalafil treatment on erectile function recovery following bilateral nerve-sparing radical prostatectomy: a randomised placebo-controlled study (REACTT) Eur Urol. 2014;65:587–96. doi: 10.1016/j.eururo.2013.09.051. [DOI] [PubMed] [Google Scholar]
- 81.Brock G, Ni X, Oelke M, et al. Efficacy of continuous dosing of tadalafil once daily vs. tadalafil on-demand in clinical subgroups of men with erectile dysfunction: A descriptive comparison using the integrated tadalafil databases. J Sex Med. 2016;13:860–75. doi: 10.1016/j.jsxm.2016.02.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Peng Z, Yang L, Dong Q, et al. Efficacy and safety of tadalafil once-a-day vs. tadalafil on-demand in patients with erectile dysfunction: A systematic review and meta-analyses. Urol Int. 2017;99:343–52. doi: 10.1159/000477496. [DOI] [PubMed] [Google Scholar]
- 83.Conaglen HM, Conaglen JV. Investigating women’s preference for sildenafil or tadalafil use by their partners with erectile dysfunction: The partners’ preference study. J Sex Med. 2008;5:1198–207. doi: 10.1111/j.1743-6109.2008.00774.x. [DOI] [PubMed] [Google Scholar]
- 84.Vardi Y, Appel B, Kilchevsky A, et al. Does low intensity extracorporeal shock wave therapy have a physiological effect on erectile function? Short-term results of a randomized, double-blind, sham-controlled study. J Urol. 2012;187:1769–75. doi: 10.1016/j.juro.2011.12.117. [DOI] [PubMed] [Google Scholar]
- 85.Yee CH, Chan ES, Hou SS, et al. Extracorporeal shockwave therapy in the treatment of erectile dysfunction: A prospective, randomized, double-blinded, placebo-controlled study. Int J Urol. 2014;21:1041–5. doi: 10.1111/iju.12506. [DOI] [PubMed] [Google Scholar]
- 86.Srini VS, Reddy RK, Shultz T, et al. Low-intensity extracorporeal shockwave therapy for erectile dysfunction: A study in an Indian population. Can J Urol. 2015;22:7614–22. [PubMed] [Google Scholar]
- 87.Kitrey ND, Gruenwald I, Appel B, et al. Penile low-intensity shock wave treatment is able to shift PDE5i non-responders to responders: A double-blind, sham-controlled study. J Urol. 2016;195:1550–5. doi: 10.1016/j.juro.2015.12.049. [DOI] [PubMed] [Google Scholar]
- 88.Fojecki GL, Tiessen S, Osther PJ. Effect of low-energy linear shockwave therapy on erectile dysfunction—a double-blinded, sham-controlled, randomized clinical trial. J Sex Med. 2017;14:106–12. doi: 10.1016/j.jsxm.2016.11.307. [DOI] [PubMed] [Google Scholar]
- 89.Kalyvianakis D, Hatzichristou D. Low-intensity shockwave therapy improves hemodynamic parameters in patients with vasculogenic erectile dysfunction: A triplex ultrasonography-based, sham-controlled trial. J Sex Med. 2017;14:891–7. doi: 10.1016/j.jsxm.2017.05.012. [DOI] [PubMed] [Google Scholar]
- 90.Kim KS, Jeong HC, Choi SW, et al. Electromagnetic low-intensity extracorporeal shock wave therapy in patients with erectile dysfunction: A sham-controlled, double-blind, randomized, prospective study. World J Mens Health. 2020;38:236–42. doi: 10.5534/wjmh.190130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Abraham L, Symonds T, Morris MF. Psychometric validation of a sexual quality of life questionnaire for use in men with premature ejaculation or erectile dysfunction. J Sex Med. 2008;5:595–601. doi: 10.1111/j.1743-6109.2007.00749.x. [DOI] [PubMed] [Google Scholar]
- 92.Gruenwald I, Appel B, Kitrey ND, et al. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013;5:95–9. doi: 10.1177/1756287212470696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Schoofs E, Fode M, Capogrosso P, et al. Current guideline recommendations and analysis of evidence quality on low-intensity shockwave therapy for erectile dysfunction. Int J Impot Res. 2019;31:209–17. doi: 10.1038/s41443-019-0132-0. [DOI] [PubMed] [Google Scholar]
- 94.Grober ED, Krakowsky Y, Khera M, et al. Canadian Urological Association guideline on testosterone deficiency in men: Evidence-based Q&A. Can Urol Assoc J. 2021;15:E234–43. doi: 10.5489/cuaj.7252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Corona G, Rastrelli G, Morgentaler A, et al. Meta-analysis of results of testosterone therapy on sexual function based on International Index of Erectile Function scores. Eur Urol. 2017;72:1000–11. doi: 10.1016/j.eururo.2017.03.032. [DOI] [PubMed] [Google Scholar]
- 96.Allan CA, Forbes EA, Strauss BJ, et al. Testosterone therapy increases sexual desire in ageing men with low-normal testosterone levels and symptoms of androgen deficiency. Int J Impot Res. 2008;20:396–401. doi: 10.1038/ijir.2008.22. [DOI] [PubMed] [Google Scholar]
- 97.Chiang HS, Hwang TI, Hsui YS, et al. Transdermal testosterone gel increases serum testosterone levels in hypogonadal men in Taiwan with improvements in sexual function. Int J Impot Res. 2007;19:411–7. doi: 10.1038/sj.ijir.3901562. [DOI] [PubMed] [Google Scholar]
- 98.Chiang HS, Cho SL, Lin YC, et al. Testosterone gel monotherapy improves sexual function of hypogonadal men mainly through restoring erection: Evaluation by IIEF score. Urology. 2009;73:762–6. doi: 10.1016/j.urology.2008.10.019. [DOI] [PubMed] [Google Scholar]
- 99.Hackett G, Cole N, Bhartia M, et al. Testosterone replacement therapy with long-acting testosterone undecanoate improves sexual function and quality-of-life parameters vs. placebo in a population of men with type 2 diabetes. J Sex Med. 2013;10:1612–27. doi: 10.1111/jsm.12146. [DOI] [PubMed] [Google Scholar]
- 100.Jones TH, Arver S, Behre HM, et al. Testosterone replacement in hypogonadal men with type 2 diabetes and/or metabolic syndrome (the TIMES2 study) Diabetes Care. 2011;34:828–37. doi: 10.2337/dc10-1233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Snyder PJ, Bhasin S, Cunningham GR, et al. Effects of testosterone treatment in older men. N Engl J Med. 2016;374:611–24. doi: 10.1056/NEJMoa1506119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Aversa A, Francomano D, Lenzi A. Does testosterone supplementation increase PDE5-inhibitor responses in difficult-to-treat erectile dysfunction patients? Expert Opin Pharmacother. 2015;16:625–8. doi: 10.1517/14656566.2015.1011124. [DOI] [PubMed] [Google Scholar]
- 103.Alhathal N, Elshal AM, Carrier S. Synergetic effect of testosterone and phophodiesterase-5 inhibitors in hypogonadal men with erectile dysfunction: A systematic review. Can Urol Assoc J. 2012;6:269–74. doi: 10.5489/cuaj.11291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Buvat J, Montorsi F, Maggi M, et al. Hypogonadal men non-responders to the PDE5 inhibitor tadalafil benefit from normalization of testosterone levels with a 1% hydroalcoholic testosterone gel in the treatment of erectile dysfunction (TADTEST study) J Sex Med. 2011;8:284–93. doi: 10.1111/j.1743-6109.2010.01956.x. [DOI] [PubMed] [Google Scholar]
- 105.Shabsigh R, Kaufman JM, Steidle C, et al. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J Urol. 2004;172:658–63. doi: 10.1097/01.ju.0000132389.97804.d7. [DOI] [PubMed] [Google Scholar]
- 106.Spitzer M, Basaria S, Travison TG, et al. Effect of testosterone replacement on response to sildenafil citrate in men with erectile dysfunction: A parallel, randomized trial. Ann Intern Med. 2012;157:681–91. doi: 10.7326/0003-4819-157-10-201211200-00004. [DOI] [PubMed] [Google Scholar]
- 107.Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: A randomized controlled trial. JAMA. 2004;291:2978–84. doi: 10.1001/jama.291.24.2978. [DOI] [PubMed] [Google Scholar]
- 108.Kalka D, Domagala Z, Dworak J, et al. Association between physical exercise and quality of erection in men with ischemic heart disease and erectile dysfunction subjected to physical training. Kardiol Pol. 2013;71:573–80. doi: 10.5603/KP.2013.0120. [DOI] [PubMed] [Google Scholar]
- 109.Lamina S, Okoye CG, Dagogo TT. Managing erectile dysfunction in hypertension: The effects of a continuous training programme on biomarker of inflammation. BJU Int. 2009;103:1218–21. doi: 10.1111/j.1464-410X.2008.08254.x. [DOI] [PubMed] [Google Scholar]
- 110.Maio G, Saraeb S, Marchiori A. Physical activity and PDE5 inhibitors in the treatment of erectile dysfunction: Results of a randomized controlled study. J Sex Med. 2010;7:2201–8. doi: 10.1111/j.1743-6109.2010.01783.x. [DOI] [PubMed] [Google Scholar]
- 111.Maresca L, D’Agostino M, Castaldo L, et al. Exercise training improves erectile dysfunction (ED) in patients with metabolic syndrome on phosphodiesterase-5 (PDE-5) inhibitors. Monaldi Arch Chest Dis. 2013;80:177–83. doi: 10.4081/monaldi.2013.5234. [DOI] [PubMed] [Google Scholar]
- 112.Warburton DER, Nicol CW, Bredin SSD. Health benefits of physical activity: The evidence. CMAJ. 2006;174:801–9. doi: 10.1503/cmaj.051351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Robinson JW, Moritz S, Fung T. Meta-analysis of rates of erectile function after treatment of localized prostate carcinoma. Int J Radiat Oncol Biol Phys. 2002;54:1063–8. doi: 10.1016/s0360-3016(02)03030-4. [DOI] [PubMed] [Google Scholar]
- 114.Clavell-Hernandez J, Wang R. The controversy surrounding penile rehabilitation after radical prostatectomy. Transl Androl Urol. 2017;6:2–11. doi: 10.21037/tau.2016.08.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Aydogdu O, Gokce MI, Burgu B, et al. Tadalafil rehabilitation therapy preserves penile size after bilateral nerve-sparing radical retropubic prostatectomy. Int Braz J Urol. 2011;37:336–44. doi: 10.1590/s1677-55382011000300007. ; discussion 44–6. [DOI] [PubMed] [Google Scholar]
- 116.Montorsi F, Brock G, Lee J, et al. Effect of nightly vs. on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol. 2008;54:924–31. doi: 10.1016/j.eururo.2008.06.083. [DOI] [PubMed] [Google Scholar]
- 117.Pace G, Del Rosso A, Vicentini C. Penile rehabilitation therapy following radical prostatectomy. Disabil Rehabil. 2010;32:1204–8. doi: 10.3109/09638280903511594. [DOI] [PubMed] [Google Scholar]
- 118.Padma-Nathan H, McCullough AR, Levine LA, et al. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res. 2008;20:479–86. doi: 10.1038/ijir.2008.33. [DOI] [PubMed] [Google Scholar]
- 119.van der Wielen GJ, Mulhall JP, Incrocci L. Erectile dysfunction after radiotherapy for prostate cancer and radiation dose to the penile structures: A critical review. Radiother Oncol. 2007;84:107–13. doi: 10.1016/j.radonc.2007.07.018. [DOI] [PubMed] [Google Scholar]
- 120.Watkins Bruner D, James JL, Bryan CJ, et al. Randomized, double-blinded, placebo-controlled crossover trial of treating erectile dysfunction with sildenafil after radiotherapy and short-term androgen deprivation therapy: Results of RTOG 0215. J Sex Med. 2011;8:1228–38. doi: 10.1111/j.1743-6109.2010.02164.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Incrocci L, Koper PC, Hop WC, et al. Sildenafil citrate (Viagra) and erectile dysfunction following external beam radiotherapy for prostate cancer: A randomized, double-blind, placebo-controlled, cross-over study. Int J Radiat Oncol Biol Phys. 2001;51:1190–5. doi: 10.1016/s0360-3016(01)01767-9. [DOI] [PubMed] [Google Scholar]
- 122.Incrocci L, Slagter C, Slob AK, et al. A randomized, double-blind, placebo-controlled, cross-over study to assess the efficacy of tadalafil (Cialis) in the treatment of erectile dysfunction following three-dimensional conformal external-beam radiotherapy for prostatic carcinoma. Int J Radiat Oncol Biol Phys. 2006;66:439–44. doi: 10.1016/j.ijrobp.2006.04.047. [DOI] [PubMed] [Google Scholar]
- 123.Ilic D, Hindson B, Duchesne G, et al. A randomized, double-blind, placebo-controlled trial of nightly sildenafil citrate to preserve erectile function after radiation treatment for prostate cancer. J Med Imaging Radiat Oncol. 2013;57:81–8. doi: 10.1111/j.1754-9485.2012.02461.x. [DOI] [PubMed] [Google Scholar]
- 124.Zelefsky MJ, Shasha D, Branco RD, et al. Prophylactic sildenafil citrate improves select aspects of sexual function in men treated with radiotherapy for prostate cancer. J Urol. 2014;192:868–74. doi: 10.1016/j.juro.2014.02.097. [DOI] [PubMed] [Google Scholar]
- 125.Campbell JD, Milenkovic U, Usta MF, et al. The good, bad, and the ugly of regenerative therapies for erectile dysfunction. Transl Androl Urol. 2020;9:S252–61. doi: 10.21037/tau.2019.10.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.SMSNA position statement on restorative therapies for ED [press release] Mar 27, 2018. [Accessed Aug 17, 2021]. Available at: https://www.issm.info/news/public-policy/smsna-releases-position-statement-on-restorative-therapies-for-erectile-dys/
- 127.Matz EL, Terlecki R, Zhang Y, et al. Stem cell therapy for erectile dysfunction. Sex Med Rev. 2019;7:321–8. doi: 10.1016/j.sxmr.2017.12.008. [DOI] [PubMed] [Google Scholar]
- 128.Al Demour S, Jafar H, Adwan S, et al. Safety and potential therapeutic effect of two intracavernous autologous bone marrow-derived mesenchymal stem cells injections in diabetic patients with erectile dysfunction: An open-label, phase 1 clinical trial. Urol Int. 2018;101:358–65. doi: 10.1159/000492120. [DOI] [PubMed] [Google Scholar]
- 129.Yiou R. Stem-cell therapy for erectile dysfunction. Biomed Mater Eng. 2017;28:S81–S5. doi: 10.3233/BME-171627. [DOI] [PubMed] [Google Scholar]
- 130.He M, von Schwarz ER. Stem-cell therapy for erectile dysfunction: A review of clinical outcomes. Int J Impot Res. 2021;33:271–7. doi: 10.1038/s41443-020-0279-8. [DOI] [PubMed] [Google Scholar]
- 131.Lokeshwar SD, Patel P, Shah SM, et al. A systematic review of human trials using stem cell therapy for erectile dysfunction. Sex Med Rev. 2020;8:122–30. doi: 10.1016/j.sxmr.2019.08.003. [DOI] [PubMed] [Google Scholar]
- 132.Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries: A review. Curr Rev Musculoskelet Med. 2008;1:165–74. doi: 10.1007/s12178-008-9032-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Epifanova MV, Gvasalia BR, Durashov MA, et al. Platelet-rich plasma therapy for male sexual dysfunction: Myth or reality? Sex Med Rev. 2020;8:106–13. doi: 10.1016/j.sxmr.2019.02.002. [DOI] [PubMed] [Google Scholar]
- 134.Scott S, Roberts M, Chung E. Platelet-rich plasma and treatment of erectile dysfunction: Critical review of literature and global trends in platelet-rich plasma clinics. Sex Med Rev. 2019;7:306–12. doi: 10.1016/j.sxmr.2018.12.006. [DOI] [PubMed] [Google Scholar]
- 135.Lei J, Priddy LB, Lim JJ, et al. Identification of extracellular matrix components and biological factors in micronized dehydrated human amnion/chorion membrane. Adv Wound Care (New Rochelle) 2017;6:43–53. doi: 10.1089/wound.2016.0699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Razdan S, Bajpai RR, Sanchez MA. A matched and controlled longitudinal cohort study of dehydrated human amniotic membrane allograft sheet used as a wraparound nerve bundles in robotic-assisted laparoscopic radical prostatectomy: A puissant adjunct for enhanced potency outcomes. J Robot Surg. 2019;13:475–81. doi: 10.1007/s11701-018-0873-7. [DOI] [PubMed] [Google Scholar]
- 137.Patel VR, Samavedi S, Bates AS, et al. Dehydrated human amnion/chorion membrane allograft nerve wrap around the prostatic neurovascular bundle accelerates early return to continence and potency following robot-assisted radical prostatectomy: Propensity score-matched analysis. Eur Urol. 2015;67:977–80. doi: 10.1016/j.eururo.2015.01.012. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.