

Abstract
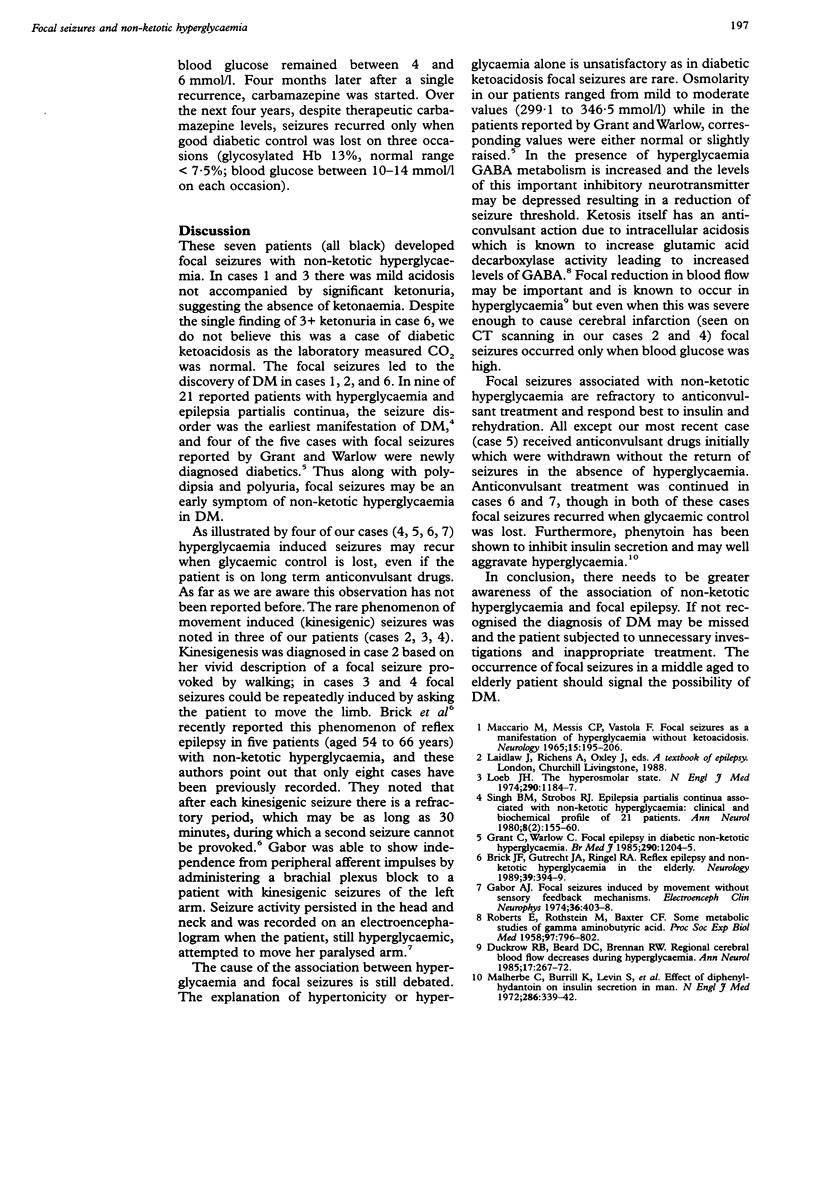
The clinical features of seven patients with non-ketotic hyperglycaemia who developed focal seizures are presented. All patients were alert except one who was mildly confused. Glucose values varied from 17.8 to 55.1 mmol/l, while calculated osmolarity values were elevated in all cases to a mild or moderate extent (299.1 to 346.5 mmol/l). In three cases diabetes mellitus was a new diagnosis. Four patients had recurrent episodes of focal seizures when glycaemic control was lost. Movement induced or kinesigenic seizures were seen in three cases and epilepsia partialis continua in one case. Seizures associated with hyperglycaemia are resistant to anticonvulsant treatment and respond best to insulin and rehydration. Focal seizures in adults may indicate diabetes mellitus.
Full text
PDF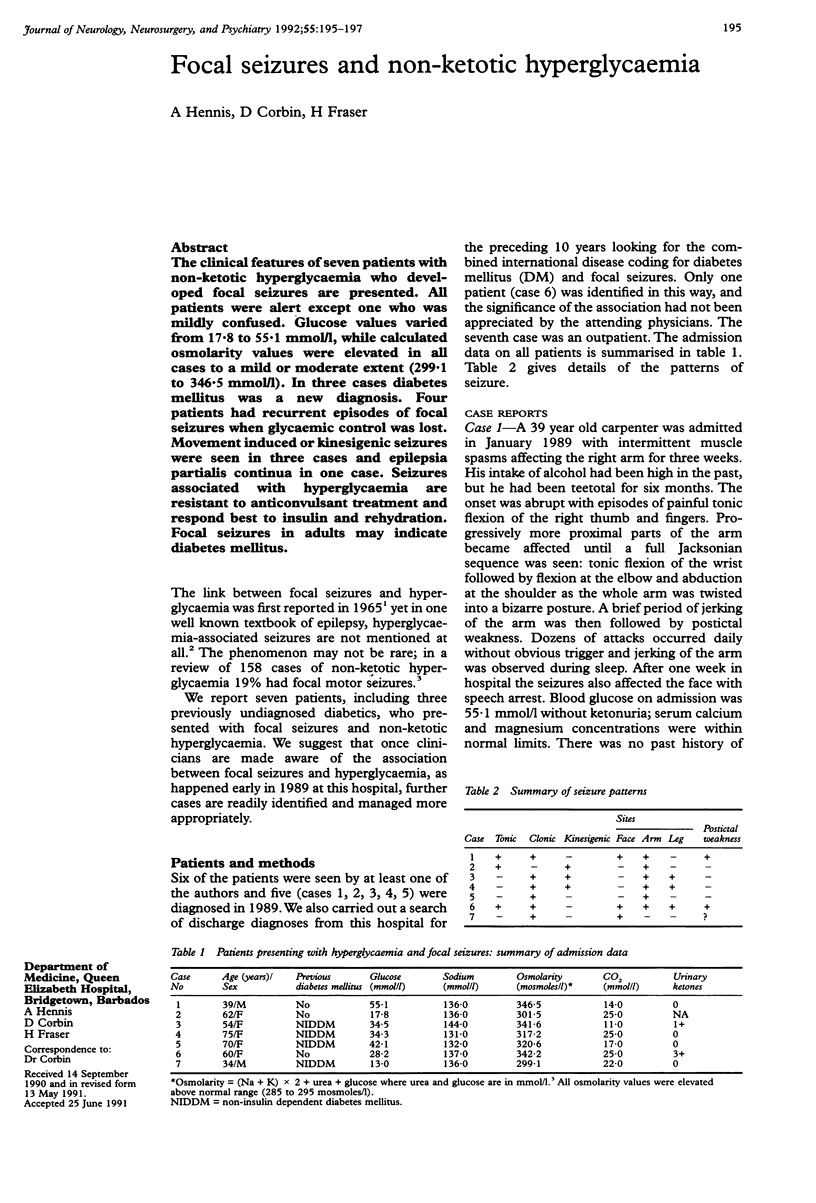

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Brick J. F., Gutrecht J. A., Ringel R. A. Reflex epilepsy and nonketotic hyperglycemia in the elderly: a specific neuroendocrine syndrome. Neurology. 1989 Mar;39(3):394–399. doi: 10.1212/wnl.39.3.394. [DOI] [PubMed] [Google Scholar]
- Duckrow R. B., Beard D. C., Brennan R. W. Regional cerebral blood flow decreases during hyperglycemia. Ann Neurol. 1985 Mar;17(3):267–272. doi: 10.1002/ana.410170308. [DOI] [PubMed] [Google Scholar]
- Gabor A. J. Focal seizures induced by movement without sensory feedback mechanisms. Electroencephalogr Clin Neurophysiol. 1974 Apr;36(4):403–408. doi: 10.1016/0013-4694(74)90190-4. [DOI] [PubMed] [Google Scholar]
- Grant C., Warlow C. Focal epilepsy in diabetic non-ketotic hyperglycaemia. Br Med J (Clin Res Ed) 1985 Apr 20;290(6476):1204–1205. doi: 10.1136/bmj.290.6476.1204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loeb J. N. The hyperosmolar state. N Engl J Med. 1974 May 23;290(21):1184–1187. doi: 10.1056/NEJM197405232902107. [DOI] [PubMed] [Google Scholar]
- MACCARIO M., MESSIS C. P., VASTOLA E. F. FOCAL SEIZURES AS A MANIFESTATION OF HYPERGLYCEMIA WITHOUT KETOACIDOSIS. A REPORT OF SEVEN CASES WITH REVIEW OF THE LITERATURE. Neurology. 1965 Mar;15:195–206. doi: 10.1212/wnl.15.3.195. [DOI] [PubMed] [Google Scholar]
- Malherbe C., Burrill K. C., Levin S. R., Karam J. H., Forsham P. H. Effect of diphenylhydantoin on insulin secretion in man. N Engl J Med. 1972 Feb 17;286(7):339–342. doi: 10.1056/NEJM197202172860702. [DOI] [PubMed] [Google Scholar]
- ROBERTS E., ROTHSTEIN M., BAXTER C. F. Some metabolic studies of gamma-aminobutyric acid. Proc Soc Exp Biol Med. 1958 Apr;97(4):796–802. doi: 10.3181/00379727-97-23883. [DOI] [PubMed] [Google Scholar]
- Singh B. M., Strobos R. J. Epilepsia partialis continua associated with nonketotic hyperglycemia: clinical and biochemical profile of 21 patients. Ann Neurol. 1980 Aug;8(2):155–160. doi: 10.1002/ana.410080205. [DOI] [PubMed] [Google Scholar]