

Abstract
Background
Establishment of a secure airway is a critical part of neonatal resuscitation in the delivery room and the neonatal intensive care unit. Videolaryngoscopy has the potential to facilitate successful endotracheal intubation, and decrease adverse consequences of a delay in airway stabilization. Videolaryngoscopy may enhance visualization of the glottis and intubation success in neonates. This is an update of a review first published in 2015, and updated in 2018.
Objectives
To determine the effectiveness and safety of videolaryngoscopy compared to direct laryngoscopy in decreasing the time and attempts required for endotracheal intubation and increasing the success rate on first intubation attempt in neonates (0 to 28 days of age).
Search methods
In November 2022, we updated the search for trials evaluating videolaryngoscopy for neonatal endotracheal intubation in CENTRAL, MEDLINE, Embase, CINAHL, and BIOSIS. We also searched abstracts of the Pediatric Academic Societies, clinical trials registries (www.clinicaltrials.gov; www.controlled-trials.com), and reference lists of relevant studies.
Selection criteria
Randomized controlled trials (RCTs), quasi‐RCTs, cluster‐RCTs, or cross‐over trials, in neonates (0 to 28 days of age), evaluating videolaryngoscopy with any device used for endotracheal intubation compared with direct laryngoscopy.
Data collection and analysis
Three review authors performed data collection and analysis, as recommended by Cochrane Neonatal. Two review authors independently assessed studies identified by the search strategy for inclusion.
We used the GRADE approach to assess the certainty of the evidence.
Main results
The updated search yielded 7786 references, from which we identified five additional RCTs for inclusion, seven ongoing trials, and five studies awaiting classification. Three studies were included in the previous version of the review. For this update, we included eight studies, which provided data on 759 intubation attempts in neonates. We included neonates of either sex, who were undergoing endotracheal intubation in international hospitals. Different videolaryngoscopy devices (including C‐MAC, Airtraq, and Glidescope) were used in the studies.
For the primary outcomes; videolaryngoscopy may not reduce the time required for successful intubation when compared with direct laryngoscopy (mean difference [MD] 0.74, 95% confidence interval [CI] ‐0.19 to 1.67; 5 studies; 505 intubations; low‐certainty evidence). Videolaryngoscopy may result in fewer intubation attempts (MD ‐0.08, 95% CI ‐0.15 to 0.00; 6 studies; 659 intubations; low‐certainty evidence). Videolaryngoscopy may increase the success of intubation at the first attempt (risk ratio [RR] 1.24, 95% CI 1.13 to 1.37; risk difference [RD] 0.14, 95% CI 0.08 to 0.20; number needed to treat for an additional beneficial outcome [NNTB] 7, 95% CI 5 to 13; 8 studies; 759 intubation attempts; low‐certainty evidence).
For the secondary outcomes; the evidence is very uncertain about the effect of videolaryngoscopy on desaturation or bradycardia episodes, or both, during intubation (RR 0.94, 95% CI 0.38 to 2.30; 3 studies; 343 intubations; very‐low certainty evidence). Videolaryngoscopy may result in little to no difference in the lowest oxygen saturations during intubation compared with direct laryngoscopy (MD ‐0.76, 95% CI ‐5.74 to 4.23; 2 studies; 359 intubations; low‐certainty evidence). Videolaryngoscopy likely results in a slight reduction in the incidence of airway trauma during intubation attempts compared with direct laryngoscopy (RR 0.21, 95% CI 0.05 to 0.79; RD ‐0.04, 95% CI ‐0.07 to ‐0.01; NNTB 25, 95% CI 14 to 100; 5 studies; 467 intubations; moderate‐certainty evidence).
There were no data available on other adverse effects of videolaryngoscopy. We found a high risk of bias in areas of allocation concealment and performance bias in the included studies.
Authors' conclusions
Videolaryngoscopy may increase the success of intubation on the first attempt and may result in fewer intubation attempts, but may not reduce the time required for successful intubation (low‐certainty evidence). Videolaryngoscopy likely results in a reduced incidence of airway‐related adverse effects (moderate‐certainty evidence).
These results suggest that videolaryngoscopy may be more effective and potentially reduce harm when compared to direct laryngoscopy for endotracheal intubation in neonates.
Well‐designed, adequately powered RCTS are necessary to confirm the efficacy and safety of videolaryngoscopy in neonatal intubation.
Keywords: Child; Humans; Infant, Newborn; Intensive Care Units, Neonatal; Intubation, Intratracheal; Intubation, Intratracheal/adverse effects; Laryngoscopy; Resuscitation
Plain language summary
Does the placement of a breathing tube using video assistance (videolaryngoscopy) increase the success and safety of the procedure in newborn babies?
Key Messages
Videolaryngoscopy may increase the success of placing a breathing tube on the first attempt, and may result in slightly fewer tries by a care provider to place the breathing tube in sick newborn babies, but it does not reduce the amount of time it takes to place the breathing tube.
Videolaryngoscopy likely results in slightly less injury to the newborn baby's airway while the breathing tube is being placed.
We need better studies to understand the role of videolaryngoscopy in different practice areas and with different care providers doing the placement.
What is the problem?
One in 100 newborn babies may need a breathing tube placed in their mouth or nose to keep them alive when they have difficulty breathing. Placing a breathing tube using direct laryngoscopy (without video assistance) may be challenging in newborns because their mouths and airways are small, and not all care providers are experienced.
What is videolaryngoscopy?
Seeing the airway by a video while placing the breathing tube is called videolaryngoscopy. This may make it easier and safer to place the breathing tube. This also may help trainees when they are learning this life‐saving skill.
What did we want to find out?
We wanted to find out if using videolaryngoscopy increased the success and safety of the placement of a breathing tube compared to the direct laryngoscopy technique, in babies who were 0 to 28 days old.
What did we do?
We searched for studies that were trying to find out whether video devices were better than the standard approach without video assistance (direct laryngoscopy) for placing breathing tubes in babies. The studies could measure time, the number of attempts, the success rate of the first attempt to place the breathing tube, or side effects.
We compared and summarized the results of the studies, and rated our confidence in the evidence, based on factors such as study methods and sizes.
What did we find?
We found eight eligible studies, which included 759 intubation attempts in newborn babies. They reported time, the number of attempts, the success rate of the first attempt to place the breathing tube, and side effects. In summary:
Videolaryngoscopy may increase the success of placing a breathing tube on the first attempt, and may result in slightly fewer tries by a care provider to place the breathing tube in sick newborn babies, but does not reduce the amount of time it takes to place the breathing tube.
Videolaryngoscopy may have little or no effect on how many babies have episodes of low oxygen or low heart rate (or both) while the breathing tube is being placed, but the evidence is very uncertain. Videolaryngoscopy may result in little or no difference in the lowest levels of oxygen while the breathing tube is being placed.
Videolaryngoscopy likely results in slightly less injury to the newborn baby’s airway while the breathing tube is being placed.
There were no data available on other adverse effects while the breathing tube is being placed.
What are the limitations of the evidence?
We found that the included studies were small, we were unable to assess the risk of bias in some, and the study results varied. The care providers who placed the breathing tube knew which device was being used. This decreases our confidence in the results of the review, and the results of further research could differ from the results of this review.
Funding and equipment support was provided in some of the included studies. In some cases, funding sources and declarations of interest were not stated.
How up to date is this evidence?
The evidence is up to date to November 2022.
Summary of findings
Summary of findings 1. Videolaryngoscopy compared with conventional direct laryngoscopy for tracheal intubation in neonates.
|
Videolaryngoscopy compared with conventional direct laryngoscopy for tracheal intubation in neonates | ||||||
|
Patient or population: neonates (0 to 28 days of age) who needed tracheal intubation Settings: operating room, delivery room, or neonatal intensive care unit Intervention: videolaryngoscopy Comparison: conventional direct laryngoscopy | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of intubations (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk with conventional, direct laryngoscopy | Corresponding risk with videolaryngoscopy | |||||
| Time required for successful intubation | The mean duration was 35.75 seconds | The mean duration was 37.89 seconds | 505 (5) | ⊕⊕⊝⊝
Lowa |
MD 0.74 (95% CI ‐0.19 to 1.67) | |
| Number of intubation attempts | The mean number of attempts was 1.39 | The mean number of attempts was 1.25 | ‐ | 659 (6) | ⊕⊕⊝⊝
Lowb |
MD ‐0.08 (95% CI ‐0.58 to 0.00) |
| Success rate at first attempt | Population at risk | RR 1.24 (1.13 to 1.37) | 759 (8) | ⊕⊕⊝⊝
Lowc |
||
| 585 per 1000 | 731 per 1000 | |||||
| Non‐airway‐related adverse effects: desaturation or bradycardia episodes, or both | Population at risk | RR 0.94 (0.38 to 2.30) | 343 (3) | ⊕⊝⊝⊝ Very lowd | ||
| 51 per 1000 | 48 per 1000 | |||||
| Non‐airway‐related adverse effects: lowest saturations during intubation | The mean saturation was 56.21% | The mean saturation was 55.06% | ‐ | 359 (2) | ⊕⊕⊝⊝
Lowe |
MD ‐0.76 (95% CI ‐5.74 to 4.23) |
| Airway‐related adverse effects: airway trauma | Population at risk | RR 0.21 (0.05 to 0.79) | 467 (5) | ⊕⊕⊕⊝
Moderatef |
||
| 46 per 1000 | 0 per 1000 | |||||
| *The basis for the assumed risk is the mean value across control groups. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI), or the mean difference between the control and intervention groups, with its 95% CI. CI: confidence interval; MD: mean difference; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded one level for study limitations (due to high risk/unclear risk of bias), and downgraded one level for serious inconsistency (due to the high I² value of 80%) bDowngraded one level for study limitations (due to high risk/unclear risk of bias), and downgraded one level for moderate inconsistency (due to the high I² value of 53%) cDowngraded one level for study limitations (due to high risk/unclear risk of bias), and downgraded one level for moderate inconsistency (due to the high I² value of 63%) dDowngraded one level for study limitations (due to high risk/unclear risk of bias), downgraded one level for serious inconsistency (due to the high I² value of 60%), and downgraded one level for imprecision eDowngraded one level for study limitations (due to high risk/unclear risk of bias) and downgraded one level for imprecision fDowngraded one level for study limitations (due to high risk/unclear risk of bias)
Background
Description of the condition
Endotracheal intubation is a life‐saving procedure performed in neonates in many clinical situations. Preterm birth, birth asphyxia, respiratory failure, and respiratory problems, including congenital anatomic abnormalities of the airway, may require rapid and immediate endotracheal intubation to secure the airway, optimize oxygenation, and achieve adequate ventilation. Successful intubation, for both experienced providers and those learning the skill, requires adequate visualization of the airway and related structures. Improved visibility may avoid prolonged or repeated intubation attempts. Several aspects of the anatomy of the neonatal airway, including the small size of the mouth and airway; the disproportionately large tongue, epiglottis, and arytenoids; extensive secretions; and the keyhole appearance of the glottis, further complicate the process of intubation. The limited visibility often makes it difficult to train junior colleagues in the technique of neonatal endotracheal intubation. Supervisors of intubation training rely mainly on the feedback from the trainee, rather than on visual confirmation. In addition, low pulmonary reserve and high oxygen consumption in small infants limit the time for instruction and correction during direct laryngoscopy. Thus, the instructors often cannot recognize the trainee's problem, and have to perform the tracheal intubation themselves. This delays learning and achievement of proficiency in tracheal intubation for the trainee (Weiss 2001). Videolaryngoscopy can assist both the trainer and the trainee to identify anatomical structures in the airway, and enhance the success of intubation (Vanderhal 2009).
Description of the intervention
Direct laryngoscopy, using the appropriate size of the Miller straight or the Macintosh laryngoscope blade, relies on achieving a direct line of sight between the intubator and the glottis of the neonate, and is the standard procedure for neonatal endotracheal intubation. Videolaryngoscopy is a form of indirect laryngoscopy in which the clinician does not directly view the larynx. Instead, laryngeal visualization is achieved with a fiberoptic or digital laryngoscope, inserted transnasally or transorally (Pott 2008). These devices contain high‐resolution microcameras and video monitors, which improve the view of the laryngeal inlet, independent of the line of sight. Videolaryngoscopic techniques have been widely used in adult endotracheal intubation, and a variety of video‐based devices have been developed. Technological advances have allowed a miniaturized device to be used in neonates.
Videolaryngoscopes can be classified as: integrated channel laryngoscopes (CTrach, Pentax Airway Scope, Airtraq), laryngoscopes with video stylets (Bonfils), and rigid blade laryngoscopes (C‐MAC, GlideScope, Truview EVO₂, McGrath [Healy 2012]). There have been many adult and pediatric trials with these devices. The GlideScope allows for superior laryngeal visualization in both routine and difficult airways in adults without the need for direct line of sight (Xue 2006), which facilitates faster learning compared with the Macintosh laryngoscope (Lim 2005). One randomised controlled trial of 203 pediatric participants, which compared GlideScope with direct laryngoscopy, found that the GlideScope provided a laryngoscopic view equal to or better than that of direct laryngoscopy, but required a longer time for intubation (Kim 2008). The McGrath videolaryngoscope had a success rate of 98% in 147 adults (Shippey 2007), and provided improved laryngeal views in participants with known difficult airways (Shippey 2008). Similarly, the Pentax Airway Scope enables even less‐experienced operators to obtain an optimal view (Asai 2008), and faster and more successful intubation on first attempt for novices, compared with the Macintosh device (Hirabayashi 2007; Hirabayashi 2008).
One meta‐analysis of adult studies on videolaryngoscopy found no clear difference between the videolaryngoscope (GlideScope) and direct laryngoscope in successful first‐attempt intubation or time to intubation (Griesdale 2012). In the same review, in two studies examining non‐experts, successful first‐attempt intubation (risk ratio [RR] 1.8, 95% confidence interval [CI] 1.4 to 2.4) and time to intubation (mean difference [MD] ‐43 seconds, 95% CI ‐72 to ‐14) were improved using the GlideScope. These benefits were not seen with intubation experts. The videolaryngoscope provided improved glottic visualization, particularly in people with potential or simulated difficult airways. One study evaluated the C‐MAC videolaryngoscope in adults, and found that a diverse group of anesthesia providers achieved a higher intubation success rate on the first attempt with the C‐MAC in people with predictors of difficult intubation (Aziz 2012). Pediatric studies reported time to intubation, number of intubation attempts, adverse effects of the laryngoscopic procedure, and the view of the airway (Fiadjoe 2012; Singh 2009; Vlatten 2009). Time required for successful intubation was significantly longer in the videolaryngoscopy group compared with the direct laryngoscopy group. There was no clear difference in the number of intubation attempts between the two groups. There was airway trauma (minor gum bleeds) only in the direct laryngoscopy group in one study (Singh 2009), which was not observed in two other studies (Fiadjoe 2012; Vlatten 2009). The studies reported better visualization of the airway with the videolaryngoscope (Fiadjoe 2012; Singh 2009; Vlatten 2009).
Videolaryngoscopes are portable, and can be used in both the delivery room and the neonatal intensive care unit (NICU) for neonates requiring endotracheal intubation. Videolaryngoscopes may be especially useful for neonates in whom a difficult airway is anticipated, for example in Pierre‐Robin sequence, oral or neck masses, cleft palate, pharyngeal perforation, or subglottic stenosis. One preliminary report by Vanderhal and colleagues, in 47 infants weighing between 530 g and 6795 g, using the Kaplan‐Berci videolaryngoscope, showed promise for the use of this technique to improve airway management, evaluation, and teaching (Vanderhal 2009). Significant differences exist between videolaryngoscopy and direct laryngoscopy for the airway view obtained, and the technique needed to insert the endotracheal tube into the trachea. These differences may necessitate appropriate training curricula for videolaryngoscopy compared with direct laryngoscopic intubation.
How the intervention might work
Intubation is a common life‐saving procedure in the NICU. It may be performed emergently in the delivery room or NICU, or non‐urgently for neonates going for surgery or for surfactant administration. The intubation may be attempted by trainees with varying degrees of skill and experience, and the neonates may have airway or facial abnormalities that may make the procedure more challenging than usual. Tracheal intubation by direct laryngoscopy in neonates is an important but sometimes difficult skill to master, which requires regular practice to maintain. The limited literature reviewing research in intubation success for trainees in pediatrics suggests that this vital skill needs to be reinforced (Falck 2003; Roberts 2006). The number of episodes that pediatric residents have for neonatal intubation has been decreasing due to several reasons, including decreased time for residents in the NICU with varying neonate acuity, duty hours restrictions, and competition with other learners (nurse practitioners, respiratory therapists) who need to intubate to maintain their own skills. Successful direct laryngoscopy requires alignment of the oral, pharyngeal, and laryngeal axes so that the vocal cords can be visualized (Thong 2009). The consequences of poorly performed intubation attempts, such as airway injury, prolonged hypoxia, and other hemodynamic disturbances, are potentially serious (Maharaj 2006). The Neonatal Resuscitation Program guidelines recommend that an intubation attempt should not be longer than 30 seconds (Kattwinkel 2011). The intubator may also need to modify the technique in real time during their attempt, under the guidance of the supervisor, to achieve the optimal view of the glottis for intubation. Adverse events during endotracheal intubation may be reduced by a technique that is not dependent upon achieving the 'line of sight' required by direct laryngoscopy.
A videolaryngoscope collects electronically processed images from a camera attached at its tip. Images of the airway are visualized on a monitor, which results in improved glottic visualization compared with direct laryngoscopy. Videolaryngoscopy‐assisted intubation removes the need for direct line of sight, which is especially helpful for trainees learning intubation skills in a clinical setting. There is less cervical manipulation and spontaneous ventilation can be preserved during attempts. Videolaryngoscopy may also prove more effective in training scenarios, and may allow trainees to rapidly acquire and maintain their competency of this vital procedural skill.
Why it is important to do this review
Establishment of a secure airway is a critical part of neonatal resuscitation. Videolaryngoscopy is a technique that has the potential to facilitate successful intubation and decrease adverse consequences of failure or delay of airway stabilization. The costs of videolaryngoscopes (ranging upwards from a few thousand US dollars), personnel training and orientation, equipment storage and maintenance have to be balanced with the benefits achieved. The effects of videolaryngoscopy on improving neonatal outcomes have not been reviewed thus far. In this review, we compared direct laryngoscopy with videolaryngoscopy for endotracheal intubation in neonates.
Objectives
To determine the effectiveness and safety of videolaryngoscopy compared to direct laryngoscopy in decreasing the time and attempts required for endotracheal intubation and increasing the success rate on first intubation attempt in neonates (0 to 28 days of age).
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials (RCTs), quasi‐RCTs, cluster‐RCTs, or cross‐over trials in neonates, evaluating videolaryngoscopy for endotracheal intubation compared with direct laryngoscopy. We considered studies that were published as full‐text articles, abstracts, or as unpublished data.
Types of participants
Neonates (0 to 28 days of age) who required intubation in the delivery room, operating room, or neonatal intensive care unit. Studies that included participants who were neonates and those beyond the neonatal period were included if the data pertaining to neonates were separately extractable for neonates. We excluded studies where data for neonates were not separately extractable, or if less than five neonates were included in the study.
Types of interventions
Videolaryngoscopy with any device used for neonatal endotracheal intubation compared with direct laryngoscopy. Videolaryngoscopes available for neonatal use include GlideScope, C‐MAC, Airtraq, Pentax Airway Scope, Truview, and Neoview.
Types of outcome measures
All outcomes (both primary and secondary) were assessed during and immediately after the endotracheal intubation attempt. No outcomes needed neonate follow‐up after the intubation procedure. We did not exclude studies based on the non‐reporting of outcomes of interest.
Primary outcomes
Time required for successful intubation, defined as total time in seconds from the first insertion of the laryngoscope blade into the mouth until final confirmation of endotracheal tube (ETT) placement by any or a combination of the following: clinical exam (auscultation, visible vapor in the ETT, adequate chest rise); increase in saturation of peripheral oxygen (SpO₂); presence of end‐tidal carbon dioxide (ET‐CO₂); or chest radiograph
Number of intubation attempts: insertion and removal of the laryngoscope blade was defined as an attempt, irrespective of the success of the intubation
Success rate at first attempt
Secondary outcomes
-
Non‐airway‐related adverse effects:
first mean blood pressure in mmHg (as measured by a cuff or an arterial line) taken after tracheal intubation
desaturation (O₂ saturation less than 95%) or bradycardia (heart rate less than 100 beats per minute) episodes, or both
lowest recorded O₂ saturation (%) from the start of tracheal intubation to normalization of saturation (O₂ saturation greater than 95%)
duration of hypoxia (O₂ saturation less than 80%) during and after tracheal intubation
time to attain normal saturation in seconds, from the start of tracheal intubation
duration of bradycardia during and after tracheal intubation
time to attain normal heart rate in seconds, from the start of tracheal intubation
Airway‐related adverse effects: airway trauma to oral, pharyngeal and laryngeal structures, including lacerations and perforations, assessed by visual or laryngoscopic exam
Search methods for identification of studies
Electronic searches
We updated the search in November 2022 in the following databases, for relevant trials. We limited the date from 2017 to 2022 because this is an update of the previous review.
Cochrane Central Register of Controlled Trials (CENTRAL; 2021, Issue 6) in the Cochrane Library (searched November 7, 2022)
MEDLINE (2017 to November 7, 2022) and PREMEDLINE OVID (2017 to November 7, 2022)
Embase (via Elsiever, embase.com; 2017 to November 7, 2022)
CINAHL EbscoHost (2017 to November 7, 2022)
BIOSIS (via Web of Science; 2017 to November 7, 2022)
Search strategies are provided in Appendix 1. At the time of publication, a PRESS (peer review of search strategies) was conducted. Subsequent updates of this review will take PRESS comments into account. For details see Appendix 2.
Searching other resources
We searched conference abstracts as follows:
Pediatric Academic Societies (American Pediatric Society, Society for Pediatric Research, and European Society for Paediatric Research), Pediatric Research (2017 to 2022);
Abstracts2view (2017 to 2022);
Proceedings First (2017 to 2022).
We searched two trial registries:
We searched the reference lists of identified clinical trials, and the review authors' personal files (2022).
Data collection and analysis
We used the standardized method of Cochrane Neonatal for conducting a systematic review (neonatal.cochrane.org/). For each included study, we collected information regarding the method of randomization, blinding, intervention, stratification, and whether the trial was single or multicenter. We noted information regarding trial participants, including age and setting where intubation was performed. We analyzed the clinical outcomes listed in Types of outcome measures.
Selection of studies
We downloaded all titles and abstracts retrieved by electronic searching to a reference management database, EndNote, and removed duplicates. Two review authors (MP and NN) independently assessed the titles and the abstracts of studies identified by the search strategy for inclusion eligibility. If this could not be done reliably by title and abstract, we obtained the full‐text version for assessment. We resolved any differences by discussion; if required, we consulted a third review author (KL). We identified and recorded reasons for exclusion of the ineligible studies. We resolved disagreements through discussion. We listed studies that initially appeared to meet the inclusion criteria but that we later excluded, in the Characteristics of excluded studies table. We collated multiple reports of the same study so that each study, rather than each report, was the unit of interest in the review. We provided any information we obtained about ongoing studies. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram (Page 2021). We obtained the full‐text version of all eligible studies for risk of bias assessment and data extraction.
Data extraction and management
We designed forms for trial inclusion or exclusion, data extraction, and for requesting additional published information from authors of the original reports. Two review authors (KL, NN) independently extracted data using a data extraction form. We piloted the form within the review team, using a sample of two included studies.
We intend to use a data form integrated with a modified version of the Cochrane Effective Practice and Organisation of Care Group data collection checklist in future updates (Cochrane EPOC Group 2017).
We extracted the following characteristics from each included study.
Administrative details: study author(s); published or unpublished; year of publication; year in which study was conducted; presence of vested interest; details of other relevant papers cited
Study characteristics: study registration, study design type, study setting, number of study centers and location; informed consent; ethics approval, details of any run‐in period (if applicable), completeness of follow‐up (e.g. greater than 80%)
Participants: number randomised, number lost to follow‐up/withdrawn, number analyzed, mean gestational age (GA), GA age range, mean chronological age (CA), CA age range, sex, severity of condition, diagnostic criteria, inclusion criteria, and exclusion criteria
Interventions: initiation, dose, and duration of administration
Outcomes as listed under Types of outcome measures.
We resolved any disagreements by discussion. We described ongoing studies identified by our search, when available, detailing the primary author, research question(s), methods, outcome measures, and an estimate of the reporting date in the Characteristics of ongoing studies table. For queries, or cases in which additional data were required, we contacted study investigators/authors for clarification. Two review authors (MP, NN) used Cochrane statistical software for data entry (Review Manager 2020). We replaced standard error of the mean (SEM) with the corresponding standard deviation (SD).
Assessment of risk of bias in included studies
Two review authors (KL and NN) independently assessed the risk of bias (low, high, or unclear) of the eight included trials using the Cochrane RoB 1 tool for the following domains (Higgins 2017):
sequence generation (selection bias);
allocation concealment (selection bias);
blinding of participants and personnel (performance bias);
blinding of outcome assessment (detection bias);
incomplete outcome data (attrition bias);
selective reporting (reporting bias);
any other bias.
Any disagreements were resolved by discussion, or if required, by a third review author (MP). See Appendix 3 for a more detailed description of risk of bias for each domain.
Measures of treatment effect
Dichotomous data (Cochran’s Q)
For dichotomous data, we reported results using risk ratios (RR) and risk differences (RD) with 95% confidence intervals (CIs). We calculated the number needed to treat for an additional beneficial outcome (NNTB), or number needed to treat for an additional harmful outcome (NNTH) with 95% CIs if there was reduction (or increase) in RD with respective 95% CIs.
Continuous data
For continuous data, we used the mean difference (MD) when outcomes were measured in the same way between trials. We used the standardized mean difference (SMD) to combine trials that measured the same outcome but used different methods. When trials reported continuous data as median and interquartile range (IQR), and data passed the test of skewness, we converted median to mean and estimate the standard deviation as IQR/1.35. If data were not reported in an RCT in a format that we could enter directly into a meta‐analysis, we converted them to the required format, using the information in Chapter 6 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2022).
Unit of analysis issues
After the initial review, we changed the unit of analysis from participants to intubation attempts, as it was impossible to separate the number of intubations for each participant. We did not identify any unit of analysis issues during this update.
We performed the primary analysis per individual intubation randomised. If we include cluster‐randomized trials in future updates, we will abstract information on the study design and unit of analysis for each study, indicating whether clustering of observations is present due to allocation to the intervention at the group level, or clustering of individually randomised observations (e.g. neonates requiring intubation in the delivery room). We will abstract available statistical information needed to account for the implications of clustering on the estimation of outcome variances, such as design effects or intra‐cluster correlations, and whether the study adjusted results for the correlations in the data. In cases where the study does not account for clustering, we will ensure that appropriate adjustments are made to the effective sample size following Cochrane guidance (Higgins 2022). Where possible, we will derive the intra‐cluster correlation (ICC) for these adjustments from the trial itself, or from a similar trial. If an appropriate ICC is unavailable, we will conduct sensitivity analyses to investigate the potential effect of clustering, by imputing a range of values of ICC.
If trials have multiple arms that are compared against the same control condition that will be included in the same meta‐analysis, we will either combine groups to create a single pair‐wise comparison, or select the pair of interventions that are most relevant to the review question and exclude the others. In the meta‐analysis and data synthesis, we will only include the first‐phase data from cross‐over trials.
Dealing with missing data
We performed analysis on an intention‐to‐treat basis for all included outcomes. Whenever possible, we analyzed all participants in the treatment group to which they were randomised, regardless of the actual treatment received. For all important missing data (in the outcomes) or unclear data, we contacted the authors for clarifications and additional information. In the case of missing data, we described the number of participants with missing data in the Results section and the Characteristics of included studies table. Some studies expressed data of certain outcomes in ways that could not be used for comparison in this review. In these cases, we attempted to obtain the raw data for inclusion. We addressed the potential impact of missing data on the findings of the review in the Discussion.
Assessment of heterogeneity
We attempted to describe the clinical diversity and methodological variability of the evidence in the review text, and with study tables describing study characteristics, including design features, population characteristics, and intervention details.
To assess statistical heterogeneity, we visually inspected forest plots, and described the direction and magnitude of effects and the degree of overlap between confidence intervals. We considered the statistics generated in forest plots that measure statistical heterogeneity. We used the I² statistic to quantify inconsistency among the trials in each analysis. We also considered the P value from the Chi² test to assess if this heterogeneity was significant (P < 0.1).
In outcomes that had substantial heterogeneity, we explored possible explanatory factors, using prespecified subgroup analyses.
We graded the degree of heterogeneity as:
less than 40% may represent low heterogeneity;
30% to 60% may represent moderate heterogeneity;
50% to 90% may represent substantial heterogeneity;
more than 75% may represent considerable heterogeneity
We used a rough guideline to interpret the I²value rather than a simple threshold, and our interpretation took into account that measures of heterogeneity (I² and Tau²) are estimated with high uncertainty when the number of studies is small (Deeks 2022).
Assessment of reporting biases
We planned to assess reporting bias by comparing the stated primary outcomes and secondary outcomes and reported outcomes. We could not obtain study protocols of all included studies to compare outcomes reported in the protocols to those reported in the studies.
We planned to investigate reporting and publication bias by examining the degree of asymmetry of a funnel plot if there were more than 10 included studies. Our review only included eight studies for meta‐analysis, and hence, the ability to detect publication bias was largely diminished. We noted our inability to rule out possible publication bias or small‐study effects.
Data synthesis
We performed statistical analyses according to the recommendations of Cochrane Neonatal. We used Review Manager 5 software to perform statistical analysis (Review Manager 2020).
For categorical outcomes, we calculated the estimates of RR and RD, each with its 95% CI; for continuous outcomes, we calculated the MD or the SMD, each with its 95% CI. We used a fixed‐effect model to combine data where it was reasonable to assume that studies were estimating the same underlying treatment effect.
Subgroup analysis and investigation of heterogeneity
Currently, we do not have data for meaningful subgroup analyses. In future updates of the review, when data are available, we plan to carry out the following subgroup analyses of factors that may contribute to heterogeneity in the effects of the intervention. We believe the following subgroups are justifiable due to size of the airway and mouth (birth weight categories), experience in intubation (personnel), distortion of the airway (malformations), ease of handling (type of equipment), and urgency (emergent or not), all of which may decrease the success of the intubation procedure.
Birth weight groups
1500 g or less
More than 1500 g
Personnel groups
Personnel with less than one year of tracheal intubation experience
Personnel with one to three years of tracheal intubation experience
Personnel with greater than three years of tracheal intubation experience
Presence of airway malformations
Airway malformations
No airway malformations
Type of neonatal videolaryngoscopy equipment
Integrated channel laryngoscope (CTrach, Pentax AWS, Airtaq)
Video stylets (Bonfils)
Rigid blade laryngoscopes (C‐MAC, GlideScope, McGrath, Truview)
Direct laryngoscope
Setting
Emergent
Non‐emergent
We will interpret tests for subgroup differences in effects with caution, given the potential for confounding with other study characteristics and the observational nature of the comparisons. In particular, subgroup analyses with fewer than five studies per category are unlikely to be adequate to ascertain valid difference in effects, and will not be highlighted in our results. When subgroup comparisons are possible, we will undertake a stratified meta‐analysis and a formal statistical test for interaction to examine subgroup differences that could account for effect heterogeneity (e.g. Cochran’s Q test, meta‐regression [Higgins 2021; Higgins 2022]).
Sensitivity analysis
We had planned to explore methodologic heterogeneity of eligible trials using sensitivity analyses, but could not undertake any because we only included eight studies.
In future updates, if data are available, we intend to perform the following sensitivity analyses:
characteristics of bias (high risk of bias compared to those at low risk of bias);
characteristics of participants (e.g. participants in some RCTs meet the age range criteria of the review); characteristics of publications status (e.g. RCTs published as abstract only and RCTs published in full);
characteristic of the outcome (e.g. time point of assessment or means of measurement);
characteristics of the comparator.
There is no formal statistical test that can be used for sensitivity analysis, therefore, if data are available in future updates, we intend to make informal comparisons between the different ways of estimating the effect under different assumptions. We will not use changes in the P values to judge whether there is a difference between the main analysis and sensitivity analysis, since statistical significance may be lost when fewer studies are included. We plan to report sensitivity analysis results in tables rather than forest plots if data are available.
Summary of findings and assessment of the certainty of the evidence
We used the GRADE approach, as outlined in the GRADE Handbook, to assess the certainty of the evidence for the following (clinically relevant) outcomes (Schünemann 2013).
Primary outcomes
Time required for successful intubation
Number of intubation attempts
Success rate at first attempt
Secondary outcomes:
Desaturation or bradycardia episodes, or both, during intubation
Lowest oxygen saturation during intubation
Airway trauma
Two review authors independently assessed the certainty of the evidence for each of the outcomes (KL, NN). We considered evidence from RCTs as high certainty, but downgraded the evidence one level for serious (or two levels for very serious) limitations based upon the following: design (risk of bias), consistency across studies, directness of the evidence, precision of estimates, and presence of publication bias. We used GRADEpro GDT 2022 to create Table 1 to report the certainty of the evidence.
The GRADE approach results in an assessment of the certainty of a body of evidence in one of four grades.
High: we are very confident that the true effect lies close to that of the estimate of the effect
Moderate: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect
Very low: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect
Results
Description of studies
Results of the search
Our searches, updated in November 2022, identified 8883 references; after removing 2099 duplicates, 6764 references were available for screening. We excluded 6735 references based on title and abstract; included eight; excluded eight; classified five as awaiting assessment; and identified seven ongoing studies. For details see Figure 1.
1.
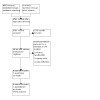
PRISMA flow diagram depicting the study selection process
We included eight studies: five new (Bartle 2019; Kamath 2020a; Salama 2019; Singh 2009; Tao 2019); and three from the previous version of this review (Moussa 2016; O'Shea 2015; Volz 2018).
We excluded eight studies: three new, which included few neonates (Jagannathan 2017; Manov 2020; Saran 2019); and three from the previous version of this review (Fiadjoe 2012; Komasawa 2017; Parmekar 2017; Sørensen 2012; Vlatten 2009).
We listed five trials as awaiting classification, as we are waiting for a response from the authors regarding full‐text availability or neonatal specific data (Chae 2022; Galante 2018a; Garcia‐Marcinkiewicz 2020; Jain 2018; Yumul 2013).
We identified seven ongoing trials: (ACTRN12614001134617; CTRI/2021/06/034029; CTRI/2022/04/041925; CTRI/2022/07/044293; DRKS00020792; NCT04295902; NCT04994652).
We identified, but did not include, one trial listed as withdrawn on clinicaltrials.gov (NCT01793727).
Included studies
Our updated search strategy identified five RCTs that were eligible for inclusion. These were added to the three trials included in the previous version of the review (Lingappan 2018). These eight studies, with a total of 759 intubations, randomised intubations performed on neonates using videolaryngoscopy or direct laryngoscopy (Bartle 2019; Kamath 2020a; Moussa 2016; O'Shea 2015; Salama 2019; Singh 2009; Tao 2019; Volz 2018). Refer to the Characteristics of included studies table for details. The studies included neonates of either sex, undergoing the procedure of endotracheal intubation in international centers, with the procedure being performed in hospitals in Australia, Canada, China, Egypt, India, the UK, and the US. Different videolaryngoscopes (including C‐MAC, Airtraq, and Glidescope) were used in these studies. These studies involved trainees as well as providers who were proficient in neonatal intubation.
Included studies
Bartle 2019 conducted a feasibility study of 40 intubations, in which neonates in the neonatal unit were randomised to videolaryngoscopy or direct laryngoscopy with a standard neonatal laryngoscope. The number of attempts to successful intubation was recorded, as was the confidence of the trainer, trainee, and nursing staff in the success of intubation.
Kamath 2020a randomly assigned neonates undergoing routine surgery who required tracheal intubation to intubation with AirTraq optical laryngoscope or Miller laryngoscope (32 in each group). Primary outcomes were intubation time, number of attempts, percentage of glottic opening score, and visual analog scale for intubation. Airway trauma and hemodynamic variables were recorded.
Moussa 2016 randomly assigned pediatric residents in the first to third year to endotracheal intubation (213 intubations) with a conventional laryngoscope or the videolaryngoscope C‐MAC VL. The primary outcome was the success rate of endotracheal intubation. The secondary outcomes were time to successful intubation, number of bradycardia episodes, lowest oxygen saturation during the procedure, the occurrence of mucosal trauma, the reason for intubation failure, and recognition of problems related to intubation by supervisor and resident.
O'Shea 2015 randomised physicians with less than six months' tertiary neonatal experience to perform endotracheal intubation with or without the modified traditional Miller videolaryngoscope screen visible to the instructor (sample size of 206 intubations). The primary outcome was first‐attempt intubation success rate confirmed by colorimetric detection of expired carbon dioxide.
Salama 2019 randomised tracheal intubation in laterally positioned neonates undergoing elective surgical repair of meningocele or myelomeningocele (60 intubations) to GlideScope cobalt videolaryngoscope or standard Miller direct laryngoscope by senior anesthesiologists. The primary outcome was the laryngeal view, graded using the percentage of glottis opening (POGO) score. Secondary outcomes were time to best glottis view, endotracheal tube passage time, intubation time, POGO scores after optimal external laryngeal maneuvers, intubation attempts, and overall success rate of intubation. Any trauma caused during laryngoscopy and any decrease in oxygen saturation < 95% were recorded.
Singh 2009 randomised neonates undergoing surgery under general anesthesia (60 intubations) to direct or videolaryngoscopy performed by senior anesthesiologists. Outcomes were the view of the glottis at laryngoscopy scored according to the Cormack and Lehane grading criteria, time to intubation, and the number of intubation attempts required. Oxygen saturation and complications related to intubation were recorded.
Tao 2019 randomised infants undergoing elective surgery to be intubated by attending anesthesiologists with either GlideScope videolaryngoscope or direct laryngoscope (sample size 70 intubations). The primary outcome was time to intubation. Secondary outcomes were the success rate of first intubation attempt, number of intubation attempts, Cormack and Lehane grade of laryngoscope view, and adverse events (trauma, desaturation, or bradycardia episodes).
Volz 2018 randomised neonatal intubations (141 intubations) by first and second‐year pediatric residents using videolaryngoscopy or direct laryngoscopy. The primary outcome was successful intubation within two attempts.
Excluded studies
We excluded eight studies (Fiadjoe 2012; Jagannathan 2017; Komasawa 2017; Manov 2020; Parmekar 2017; Saran 2019; Sørensen 2012; Vlatten 2009; see Characteristics of excluded studies table).
Fiadjoe 2012 randomised infants aged less than one year who underwent elective surgery to videolaryngoscopy or conventional direct laryngoscopy for intubations. Outcomes were intubation time, time to best view, percentage of glottic opening score, and intubation success. This study was excluded as there were no neonates.
Jagannathan 2017 randomised tracheal intubations to direct laryngoscopy or videolaryngoscopy. The primary outcome was the median difference in the total time for successful tracheal intubation. Secondary outcomes assessed were tracheal intubation attempts, time to best glottic view, time for tracheal tube entry, percentage of glottic opening score, airway maneuvers needed, and complications. This study was excluded because it included fewer than five neonates.
Manov 2020, randomised infants less than one year of age undergoing elective tracheal intubation to intubation using King Vision videolaryngoscope or direct laryngoscope. Primary outcomes were the time taken for intubation, and the first‐attempt intubation success rate. This study was excluded because it included fewer than five neonates.
Saran 2019 randomised infants aged one day to six months requiring intubation under general anesthesia by trainees to videolaryngoscopy or direct laryngoscopy followed by verbal feedback. Primary outcome was first attempt success rate secondary outcomes were time to best view, time to intubation, ease of intubation, maneuvers used, and complications. This study was excluded because it included fewer than five neonates.
Sørensen 2012 randomised children aged two years or younger scheduled for elective cleft lip/palate surgery to intubation with the videolaryngoscope or direct laryngoscope. The primary end point was success rate, defined as intubation on first attempt. Secondary end points were time for intubation, tube positioning in front of the glottis, and intubation. This study was excluded as there were no neonates.
Vlatten 2009 randomised children aged four years or less to direct laryngoscopy or videolaryngoscopy. Reported outcomes were time to best view, time to intubate, and percentage of glottis opening seen. This study was excluded as there were no neonates.
Komasawa 2017 and Parmekar 2017 were conducted using manikins and did not include human neonates; thus, they were excluded.
Studies awaiting classification
We listed five trials as awaiting classification, as we are waiting for a response from the authors regarding full‐text availability or neonatal‐specific data (Chae 2022, Galante 2018a; Garcia‐Marcinkiewicz 2020; Jain 2018; Yumul 2013); see Characteristics of studies awaiting classification table.
Chae 2022 randomised 40 children less than a year of age (10 of which were neonates) to direct laryngoscope or videolaryngoscope. The primary outcome was time to intubation (TTi); the secondary outcomes were time to best view (TTBV) with and without the backward, upward, rightward, and posterior pressure (BURP) maneuver, the percentage of glottis opening (POGO) score with and without the BURP maneuver, Cormack and Lehane Laryngeal View [CL] grade with and without the BURP maneuver, effects of the BURP maneuver on glottic view, number of attempts, rate of first attempt success, incidence of desaturation, lowest SpO₂ during intubation, and presence of intraoral bleeding. We contacted the first author for further details about neonate‐specific outcomes; we are awaiting a reply.
Galante 2018a randomised infants one year of age or younger, to intubation using direct laryngoscopy versus videolaryngoscopy by an experienced anesthesiologist. Time taken for intubation, intubation attempts, ease of intubation, and percentage of glottic opening score were reported. We contacted the first author for further details about the number of neonates included; we are awaiting a reply.
Garcia‐Marcinkiewicz 2020 conducted a multicenter randomised controlled trial that compared videolaryngoscopy to direct laryngoscopy performed by anesthesia clinicians (attendings, fellows, or resident anesthetists). The primary outcome was the proportion of participants with successful orotracheal intubation on the first attempt. Secondary outcomes were number of intubation attempts, time to successful orotracheal intubation, proportion of unsuccessful intubations with the randomly assigned device, and proportion of non‐severe and severe complications. We contacted the first author for further details about the number of neonates included; we are awaiting a reply.
Jain 2018 randomised infants to undergo tracheal intubation with either a videolaryngoscope or direct laryngoscope in the left lateral position, by experienced anesthetists. The primary outcome was total time for tracheal intubation. Secondary outcomes were intubation difficulty score, laryngoscope view, success rate, number of attempts, and optimizing maneuvers required. We contacted the first author for further details about the number of neonates included; we are awaiting a reply.
Yumul 2013 randomised children less than three years of age to tracheal intubation by experienced anesthesiologists using direct laryngoscopy or videolaryngoscopy. Outcomes were time to glottic view, time to placement of the tube, time to observe an end‐tidal CO₂ waveform, number of intubation attempts, rating of glottic view, need to change to a different intubating device, and use of an adjuvant airway device. We contacted the first author for details of included neonatal data; we are awaiting a reply.
Ongoing studies
We identified seven ongoing trials (ACTRN12614001134617; CTRI/2021/06/034029; CTRI/2022/04/041925; CTRI/2022/07/044293; DRKS00020792; NCT04295902; NCT04994652); see Characteristics of ongoing studies table.
Risk of bias in included studies
The risk of bias of the eight included studies is depicted in Figure 2 and Figure 3.
2.

Risk of bias graph: review authors' judgments about each risk of bias item, presented as percentages across all included studies
3.

Risk of bias summary: review authors' judgments about each risk of bias item for each included study
Allocation
We judged seven studies at low risk of bias, and one study at unclear risk of bias for randomization (Kamath 2020a).
We judged five studies at low risk of bias, and three studies at unclear risk for allocation concealment (Kamath 2020a; Singh 2009; Volz 2018).
Blinding
Performance bias
We judged the risk of performance bias as high in all studies, as none of the studies could be blinded, and the participant knew which device he or she was using. In addition, in the studies with trainees, participants knew if the supervisor had access to the videolaryngoscope screen during their attempt, and the risk of performance bias on the trainee and the supervisor was high but unavoidable in such studies.
Detection bias
None of the studies explicitly reported blinding of outcome assessors. However, outcomes, such as successful intubation and time to intubation, were assessed using objective criteria, so we assessed the risk of detection bias as low for seven studies, and unclear for Kamath 2020a.
Incomplete outcome data
We judged all eight included studies to be at low risk of attrition bias.
Selective reporting
Kamath 2020a did not report all outcomes in the abstract, so we judged the risk of selective reporting as unclear. We judged there was low risk of selective reporting bias in the remaining seven studies.
Other potential sources of bias
In one study, nearly two‐thirds of the intubations were nasotracheal (Moussa 2016). In the included study that was published as an abstract, the full risk of bias was unclear, as the full details of the study were unavailable (Kamath 2020a).
Effects of interventions
See: Table 1
Videolaryngoscopy versus conventional direct laryngoscopy
Primary outcomes
Time required for successful intubation
Five studies reported this outcome (Kamath 2020a; Moussa 2016; O'Shea 2015; Singh 2009; Tao 2019). Videolaryngoscopy may not reduce the time required for successful intubation when compared to direct laryngoscopy (mean difference [MD] 0.74, 95% confidence interval [CI] ‐0.19 to 1.67; I² = 80%; 5 studies; 505 intubations; low‐certainty evidence; Analysis 1.1).
1.1. Analysis.

Comparison 1: Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL), Outcome 1: Time required for successful intubation (seconds)
Number of intubation attempts
Six studies reported this outcome (Bartle 2019; Kamath 2020a; Moussa 2016; O'Shea 2015; Salama 2019; Tao 2019). Videolaryngoscopy may result in a slight reduction in the number of intubation attempts (MD ‐0.08, 95% CI ‐0.15 to 0.00; I² = 53%; 6 studies; 659 intubations; low‐certainty evidence; Analysis 1.2).
1.2. Analysis.

Comparison 1: Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL), Outcome 2: Number of intubation attempts
Success rate at first attempt
All eight studies reported this outcome. Videolaryngoscopy may increase the success of intubation at the first attempt (risk ratio [RR] 1.24, 95% CI 1.13 to 1.37; risk difference [RD] 0.14, 95% CI 0.08 to 0.20; number needed to treat for an additional beneficial outcome [NNTB] 7, 95% CI 5 to 13; I² = 63%; 8 studies; 759 intubations; low‐certainty evidence; Analysis 1.3).
1.3. Analysis.

Comparison 1: Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL), Outcome 3: Success rate at first attempt
Secondary outcomes
Non‐airway‐related adverse effects: desaturation or bradycardia episodes, or both
Three studies reported this outcome (Moussa 2016; Salama 2019; Tao 2019). The evidence is very uncertain about the effect of videolaryngoscopy on desaturation or bradycardia episodes, or both, during intubation (RR 0.94, 95% CI 0.38 to 2.30; I² = 60%; 3 studies; 343 intubations; very low‐certainty evidence; Analysis 1.4).
1.4. Analysis.

Comparison 1: Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL), Outcome 4: Non‐airway‐related adverse effects: desaturation or bradycardia episodes, or both
Non‐airway‐related adverse effects: lowest recorded O₂ saturations during intubation
Two studies reported this outcome (Moussa 2016; O'Shea 2015). Videolaryngoscopy may result in little to no difference in the lowest saturations during intubation when compared with direct laryngoscopy (MD ‐0.76, 95% CI ‐5.74 to 4.23; I² = 0%; 2 studies; 359 intubations; low‐certainty evidence; Analysis 1.5).
1.5. Analysis.

Comparison 1: Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL), Outcome 5: Non‐airway‐related adverse effects: lowest saturations during intubation
Non‐airway‐related adverse effects: other than desaturations or bradycardia during intubation
None of the studies reported on other secondary outcomes, namely, first mean blood pressure in mmHg taken after tracheal intubation; duration of hypoxia during and after tracheal intubation; time to attain normal saturation in seconds, from the start of tracheal intubation; duration of bradycardia during and after tracheal intubation; time to attain normal heart rate in seconds, from the start of tracheal intubation.
Airway‐related adverse effects: airway trauma
Five studies reported this outcome (Kamath 2020a; Moussa 2016; Salama 2019; Singh 2009; Tao 2019). Videolaryngoscopy likely results in a slight reduction in the incidence of airway trauma during intubation attempts when compared with direct laryngoscopy (RR 0.21, 95% CI 0.05 to 0.79; RD ‐0.04, 95% CI ‐0.07 to ‐0.01; I² = 0%; 5 studies; 467 intubations; moderate‐certainty evidence; Analysis 1.6).
1.6. Analysis.

Comparison 1: Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL), Outcome 6: Airway‐related adverse effects: airway trauma
Discussion
Summary of main results
We included eight randomised controlled trials that compared videolaryngoscopy with conventional, direct laryngoscopy for endotracheal intubation in neonates (Bartle 2019; Kamath 2020a; Moussa 2016; O'Shea 2015; Salama 2019; Singh 2009; Tao 2019; Volz 2018).
The evidence suggests that videolaryngoscopy may not reduce the time required for successful intubation when compared with direct laryngoscopy (low‐certainty evidence). Videolaryngoscopy may result in a slight decrease in the number of intubation attempts (low‐certainty evidence), and may increase the success of intubation on the first attempt (low‐certainty evidence).
Videolaryngoscopy likely decreases the incidence of airway trauma (moderate‐certainty evidence). The evidence is very uncertain about the effect of videolaryngoscopy on desaturation or bradycardia episodes, or both, during intubation (very low‐certainty evidence). The evidence suggests that videolaryngoscopy may result in little to no difference in the lowest oxygen saturations during intubation when compared with direct laryngoscopy. There were no data available on other adverse effects of videolaryngoscopy.
Overall completeness and applicability of evidence
The current increase in interest in videolaryngoscopy as a clinical teaching tool is in the wake of duty hours restrictions and decreasing intubation opportunities for trainees to gain competence in the procedure. The number of intubation opportunities is further decreased by the presence of additional advanced providers, such as respiratory therapists and nurse practitioners, and the growing adaptation of non‐invasive respiratory support in preterm neonates. Even though this review showed that videolaryngoscopy increased the success of intubation on the first attempt and decreased the incidence of airway‐related trauma events, the proficiency of the intubator varied, and the procedures were carried out in different care environments (neonatal intensive care unit, delivery room, operating room). In addition, the cost of videolaryngoscopes may be prohibitive, and availability may be limited for these devices in some low‐resource settings.
We are awaiting neonatal data from investigators of five studies in order to further classify these trials (Chae 2022, Galante 2018a; Garcia‐Marcinkiewicz 2020; Jain 2018; Yumul 2013). We identified seven ongoing trials, which we will assess for inclusion in future updates as their data become available (ACTRN12614001134617; CTRI/2021/06/034029; CTRI/2022/04/041925; CTRI/2022/07/044293; DRKS00020792; NCT04295902; NCT04994652).
Quality of the evidence
We assessed the certainty of evidence using GRADE methodology (Guyatt 2008); we downgraded the evidence to moderate‐certainty, low‐certainty, or very low‐certainty, on the basis of high risk of bias in the included studies, imprecision, and inconsistency (Figure 2; Figure 3). We could not assess publication bias, as we identified only eight studies. We judged all eight included studies to be at high risk of performance bias since none of the studies could blind the intervention.
We downgraded the certainty of the evidence for time required for intubation, number of intubation attempts, and success rate at first attempt to low certainty (serious inconsistency and high risk of bias). We downgraded the certainty of the evidence for non‐airway‐related adverse effects of desaturation or bradycardia, or both, to very low (inconsistency, imprecision, and high risk of bias). We downgraded the certainty of the evidence for non‐airway‐related adverse effect of lowest saturation during intubation to low certainty (imprecision and high risk of bias). We downgraded the certainty of the evidence for airway‐related adverse effects to moderate (risk of bias).
Potential biases in the review process
We used the standard methods of Cochrane Neonatal to conduct this systematic review. We strove to decrease biases in the review process. Two review authors performed the literature search using an inclusive search strategy, and combined their results. Our search strategy identified eight randomised controlled trials, which measured prespecified neonatal outcomes. We pursued the investigators of published randomised controlled trials and conference proceedings for data and missing information with variable success. Two review authors independently assessed the risk of bias in the eight included trials. We discussed and addressed potential biases during the search for eligible studies, and inclusion or exclusion of studies.
Agreements and disagreements with other studies or reviews
We found no other reviews that quantitatively synthesized data from trials of videolaryngoscopy for endotracheal intubation in neonates.
Authors' conclusions
Implications for practice.
Videolaryngoscopy may increase the success of intubation on the first attempt, and may result in fewer intubation attempts, but does not reduce the time required for successful intubation (low‐certainty evidence). Videolaryngoscopy likely results in fewer airway‐related adverse effects (moderate‐certainty evidence).
These results suggest that videolaryngoscopy may be more effective and potentially reduce harm when compared to direct laryngoscopy for endotracheal intubation in neonates.
Implications for research.
Well‐designed, randomised controlled trials are necessary to confirm the efficacy, safety, and cost‐effectiveness of videolaryngoscopy in neonatal intubation. Such trials should also evaluate the setting of intubation (emergent versus non‐emergent), the use of pre‐medication versus no pre‐medication, and the proficiency of those performing the procedure. Clinically relevant adverse outcomes, such as a decrease in oxygen saturation, prolonged bradycardia, or hypoxia, should be reported in future studies. A comparison of videolaryngoscopy and direct laryngoscopy in neonates with airway malformations also needs further evaluation. In addition, the usefulness of videolaryngoscopy as a teaching tool for trainees warrants further study.
What's new
| Date | Event | Description |
|---|---|---|
| 12 May 2023 | New search has been performed | We updated our search in Nov 2022, added new eligible studies, and revised our meta‐analysis. We included five new studies with 296 participants in the updated review (Bartle 2019; Kamath 2020a; Salama 2019; Singh 2009; Tao 2019). We included one study awaiting classification (Chae 2022), and four ongoing studies (ACTRN12614001134617; CTRI/2021/06/034029; CTRI/2022/04/041925; CTRI/2022/07/044293). We updated our methods to the new Cochrane standards. |
| 12 May 2023 | New citation required but conclusions have not changed | Conclusions not changed |
History
Protocol first published: Issue 7, 2012 Review first published: Issue 2, 2015
| Date | Event | Description |
|---|---|---|
| 4 April 2018 | Feedback has been incorporated | Editorial feedback incorporated on the review update |
| 28 November 2017 | New citation required and conclusions have changed | No studies were available for the previous publication of the review. The update now includes data from 3 studies. |
Acknowledgements
We would like to thank Cochrane Neonatal: Fiona Russell, Jane Cracknell, and Michelle Fiander, Managing Editors; and Roger Soll and Bill McGuire, Co‐coordinating Editors, who provided editorial and administrative support. We thank Michelle Fiander for the PRESS review of search strategies in this review and recommendations for changes to search strategies in future updates.
We thank Dr Ibtihal Siddiq Abdelgadir (Consultant Paediatrician, Sidra Medicine; Assistant Professor, Weill Cornell Medical College) for peer review of this manuscript.
We would like to acknowledge Amy Sisson, Information Specialist at the Texas Medical Center library for developing and running the initial search strategies.
We thank Thomas Shaw for his work on the protocol and original publication of the review. We thank Yolanda Brousseau at Cochrane Neonatal for help with the 2013 search in Embase.
The methods section of this review was based on a standard template used by Cochrane Neonatal.
Appendices
Appendix 1. Search strategies 2022
SEARCH DATE: November 2022
MEDLINE OVID
Total: 1371
| 1 | exp Intubation/ | 54,834 |
| 2 | (laryngoscopy or laryngoscope).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub‐heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 22,112 |
| 3 | 'direct laryngoscopy'.mp. | 2,303 |
| 4 | ('video laryngoscopy' or videolaryngoscopy).mp. | 1,277 |
| 5 | Glidescope.mp. | 649 |
| 6 | McGrath.mp. | 398 |
| 7 | (Pentax or 'airway scope').mp. | 546 |
| 8 | C‐MAC.mp. | 241 |
| 9 | Truview.mp. | 73 |
| 10 | (Airtraq or 'optical layrngoscope').mp. | 387 |
| 11 | LMA CTrach.mp. | 53 |
| 12 | Neoview.mp. | 0 |
| 13 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 | 71,759 |
| 14 | exp Infant, Premature, Diseases/ or exp Infant, Newborn/ or exp Infant/ or 'infant ‐ newborn'.mp. | 1,172,642 |
| 15 | neonat*.mp. | 306,912 |
| 16 | newborn*.mp. | 782,924 |
| 17 | 14 or 15 or 16 | 1,413,024 |
| 18 | 13 and 17 | 9,725 |
| 19 | limit 18 to yr="2017 ‐Current" | 1,371 |
Embase (Embase.com)
Total : 3109 ('intubation'/exp OR 'intubation' OR laryngoscopy OR laryngoscope OR 'direct laryngoscopy' OR 'video laryngoscopy' OR 'videolaryngoscopy' OR glidescope OR mcgrath:ta,ab,kw,ti OR pentax OR 'airway scope' OR 'c mac' OR truview OR airtraq OR 'optical laryngoscope' OR 'lma ctrach' OR neoview) AND ('infant ‐ newborn'/exp OR 'infant ‐ newborn' OR neonat* OR newborn*) AND (2017:py OR 2018:py OR 2019:py OR 2020:py OR 2021:py)
CINAHL Ebsco
Total: 128 "intubation OR ( laryngoscopy or laryngoscope ) OR 'direct laryngoscopy' OR ( 'video laryngoscopy' or videolaryngoscopy ) AND ( infant or newborn or neonat* )"
https://search.ebscohost.com/login.aspx?direct=true&db=rzh&bquery=%26quot%3bintubation+OR+(+laryngoscopy+or+laryngoscope+)+OR+%26%2339%3bdirect+laryngoscopy%26%2339%3b+OR+(+%26%2339%3bvideo+laryngoscopy%26%2339%3b+or+videolaryngoscopy+)+AND+(+infant+or+newborn+or+neonat*+)%26quot%3b&cli0=DT1&clv0=201701‐202106&type=1&searchMode=Standard&site=ehost‐live
Cochrane CENTRAL (via Wiley)
Total: 519 #1 intubation 18343 #2 laryngoscopy or laryngoscope 5054 #3 'direct laryngoscopy' 1025 #4 'video laryngoscopy' or videolaryngoscopy 867 #5 #1 or #2 or #3 or #4 19844 #6 infant 52663 #7 newborn 27732 #8 neonat* 34880 #9 #6 or #7 or #8 73153 #10 #5 and #9 2199 Trials – 1935; date (2017‐2021) 519
Appendix 2. PRESS: peer review of search strategies
PRESS: July 13, 2022
M. Fiander
| Dear Mohan and colleagues, Comments in this assessment should be considered for subsequent updates of this review. Best wishes, Michelle |
| Search strategies for bibliographic databases: presentation of terms is fine; though it is useful to see the number of results per line in all strategies |
| Search strategies for other sources: revisions required: for future versions of this review, please provide strategies/search terms used for trial registries |
| Translation/Structure of search: revisions suggested: use more sensitive neonatal population terms; ensure MeSH are used for relevant concepts; see note below in Subject Headings. |
| Boolean and proximity operators: revisions suggested: adjacency searching is powerful, and it is strongly recommended (video near laryngoscop* for example); will identify references not found by the Medline strategy as presented in this review |
| Subject headings: revisions suggested: aside from intubation and infant, I cannot determine if subject headings were used in MEDLINE, e.g. MeSH laryngoscopy or laryngoscopes |
| Text word searching: revisions required: search fields are not always specified; in the future, please include; truncation is not used and should be for all keyword terms; although it does not negatively impact the search, It is redundant to search 'video laryngoscopy' if laryngoscopy is searched |
| Spelling/syntax; line numbers: seem fine |
| Limits and filters: date limit is provided; suggest more sensitive neonatal terms be used in subsequent updates; although the omission of RCT filter does not adversely affect the search, author might save screening time by using one |
| OVERALL EVALUATION: revisions required for future searches |
| Author reply. OK |
| PRESS reviewer Declaration of interest: I am an Information Specialist and Managing Editor with Cochrane Neonatal Group |
| I am happy to be acknowledged in the published review: Michelle Fiander, Information Specialist |
Appendix 3. Risk of bias tool
1. Sequence generation (checking for possible selection bias). Was the allocation sequence adequately generated?
For each included study, we categorized the method used to generate the allocation sequence as:
low risk (any truly random process, e.g. random number table; computer random number generator);
high risk (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number); or
unclear risk.
2. Allocation concealment (checking for possible selection bias). Was allocation adequately concealed?
For each included study, we categorized the method used to conceal the allocation sequence as:
low risk (e.g. telephone or central randomization; consecutively numbered sealed opaque envelopes);
high risk (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth); or
unclear risk.
3. Blinding of participants and personnel (checking for possible performance bias). Was knowledge of the allocated intervention adequately prevented during the study?
For each included study, we categorized the methods used to blind study participants and personnel from knowledge of which intervention a participant received. Blinding was assessed separately for different outcomes or class of outcomes. We categorized the methods as:
low risk, high risk, or unclear risk for participants; and
low risk, high risk, or unclear risk for personnel.
4. Blinding of outcome assessment (checking for possible detection bias). Was knowledge of the allocated intervention adequately prevented at the time of outcome assessment?
For each included study, we categorized the methods used to blind outcome assessment. Blinding was assessed separately for different outcomes or class of outcomes. We categorized the methods as:
low risk for outcome assessors;
high risk for outcome assessors; or
unclear risk for outcome assessors.
5. Incomplete outcome data (checking for possible attrition bias through withdrawals, dropouts, protocol deviations). Were incomplete outcome data adequately addressed?
For each included study and for each outcome, we described the completeness of data, including attrition and exclusions from the analysis. We noted whether attrition and exclusions were reported, the numbers included in the analysis at each stage (compared with the total number of randomized participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported or supplied by the trial authors, we re‐included missing data in the analysis. We categorized the methods as:
low risk (< 20% missing data);
high risk (≥ 20% missing data); or
unclear risk.
6. Selective reporting bias. Were reports of the study free of suggestion of selective outcome reporting?
For each included study, we described how we investigated the possibility of selective outcome reporting bias and what we found. For studies in which study protocols were published in advance, we compared prespecified outcomes versus outcomes eventually reported in the published results. If the study protocol was not published in advance, we contacted study authors to gain access to the study protocol. We assessed the methods as:
low risk (where it was clear that all the study's prespecified outcomes and all expected outcomes of interest to the review were reported);
high risk (where not all the study's prespecified outcomes were reported; one or more reported primary outcomes were not prespecified outcomes of interest, or were reported incompletely so data could not be used; study failed to include results of a key outcome that would have been expected to have been reported); or
unclear risk.
7. Other sources of bias. Was the study apparently free of other problems that could have put it at a high risk of bias?
For each included study, we described any important concerns we had about other possible sources of bias (e.g. whether there was a potential source of bias related to the specific study design or whether the trial was stopped early due to some data‐dependent process). We assessed whether each study was free of other problems that could put it at risk of bias as:
low risk;
high risk; or
unclear risk
If needed, we explored the impact of the level of bias by undertaking sensitivity analyses.
Data and analyses
Comparison 1. Videolaryngoscopy (VDL) versus conventional direct laryngoscopy (CDL).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Time required for successful intubation (seconds) | 5 | 505 | Mean Difference (IV, Fixed, 95% CI) | 0.74 [‐0.19, 1.67] |
| 1.2 Number of intubation attempts | 6 | 659 | Mean Difference (IV, Fixed, 95% CI) | ‐0.08 [‐0.15, ‐0.00] |
| 1.3 Success rate at first attempt | 8 | 759 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [1.13, 1.37] |
| 1.4 Non‐airway‐related adverse effects: desaturation or bradycardia episodes, or both | 3 | 343 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.38, 2.30] |
| 1.5 Non‐airway‐related adverse effects: lowest saturations during intubation | 2 | 359 | Mean Difference (IV, Fixed, 95% CI) | ‐0.76 [‐5.74, 4.23] |
| 1.6 Airway‐related adverse effects: airway trauma | 5 | 467 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.21 [0.05, 0.79] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bartle 2019.
| Study characteristics | ||
| Methods | Feasibility study in which neonates were randomised to videolaryngoscopy with C‐MAC or direct laryngoscopy for intubation. Randomized controlled trial, with randomization performed using concealment allocation. The study was performed at two centers in the United Kingdom. | |
| Participants | Any infant (either sex) who required oral intubation was eligible for inclusion. Infants were not recruited if they were in extremis requiring immediate intubation by a senior experienced operator who used his/her own preferred method. Any baby with a congenital airway malformation was not included. Some babies were excluded as they were felt to be too small for the equipment to be effective. None of the procedures were carried out in emergency delivery circumstances. The sample size was 40 intubations. | |
| Interventions | Videolaryngoscopy with Storz C‐MAC videolaryngoscope (size 1 or size 0 Miller blade) compared to direct laryngoscopy with standard neonatal laryngoscope. 40 intubations were performed in 39 babies (21 babies in the video laryngoscopy group and 18 in the direct laryngoscopy group). | |
| Outcomes | Number of attempts to successful intubation (initially determined clinically and then confirmed by chest radiograph with or without capnography) and confidence of accurate tube placement (trainee, trainer, and supporting staff confidence). Author was contacted and provided number of intubation attempts for each group. | |
| Notes | Performed across two sites: the local neonatal unit at Royal Devon and Exeter NHS Foundation Trust; the neonatal intensive care unit at Derriford Hospital, Plymouth. Funding sources/declarations of interest were not stated | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Statistician provided a block randomization list, which ensured that the envelopes were distributed evenly between the two units. |
| Allocation concealment (selection bias) | Low risk | Randomization was performed using concealment of allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants could not be blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Successful intubation was determined clinically, and subsequently confirmed by a chest radiograph with or without capnography. The research and development team performed independent data collection and entry of the data. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | One participant who was allocated to the control group was withdrawn. Outcomes were published for the remaining participants. |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. One participant in the experimental group was not included in the author's unpublished report of the number of intubation attempts. |
| Other bias | Low risk | Not at risk |
Kamath 2020a.
| Study characteristics | ||
| Methods | Randomized study comparing videolaryngoscopy with AirTraq to direct laryngoscopy for intubation. The study was conducted in India. | |
| Participants | Neonates of American Society of Anesthesiologists (ASA) class I and II posted for routine surgery requiring tracheal intubation. Sample size for the study was 64 neonates. Exclusion criteria were not stated. | |
| Interventions | Videolaryngoscopy with AirTraq optical laryngoscope compared to direct laryngoscopy with Miller laryngoscope. 64 neonates (32 in the videolaryngoscopy group and 32 in the direct laryngoscopy) group were included. | |
| Outcomes | Intubation time, the number of attempts, percentage of glottic opening score, the visual analog scale for intubation, hemodynamic variables (at baseline, during intubation, and 1.3 and 5 minutes after intubation), and airway trauma during intubation were measured. | |
| Notes | Conference abstract. Funding sources/declarations of interest were not stated. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Bias unclear in conference abstract |
| Allocation concealment (selection bias) | Unclear risk | Bias unclear in conference abstract |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants could not be blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Bias unclear in conference abstract |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | It appears that each group randomised 32 neonates, and outcomes were reported for all neonates randomised. |
| Selective reporting (reporting bias) | Unclear risk | Bias unclear in conference abstract |
| Other bias | Low risk | unknown |
Moussa 2016.
| Study characteristics | ||
| Methods | A non‐blinded, randomised controlled trial with cross‐over of only the experimental group in the second phase. All intubations were performed with direct laryngoscopy in the second phase. The study was conducted in Canada. Randomization was by concealed allocation using a table of random numbers stratified by year of residency training. | |
| Participants | All intubations attempted by residents in the NICU were included. Intubations performed on neonates with major oral, cervical, or upper airway malformations, emergency intubations, and unexpected difficult intubations (that needed an anesthetist to secure airway) were excluded from the study. Sample size based on power analysis was 100 intubations per group. 112 intubations were studied in the direct laryngoscopy group and 101 intubations in the video laryngoscopy group. | |
| Interventions | Endotracheal intubation with conventional laryngoscope (Rusch, Teleflex Medical, Markham, Canada) with Miller blade size 00, 0, or 1, or the videolaryngoscope C‐MAC VL (Karl Storz, Tuttlingen, Germany) with blade size 0 or 1 | |
| Outcomes | Primary outcome: success rate of endotracheal intubation, defined as correct anatomical placement of the ETT in ≤ 3 attempts (confirmed by change in color of the carbon dioxide detector, vapor in the endotracheal tube, thoracic expansion, assessment of bilateral lung air entry, absence of air entry in the stomach by auscultation, and improvement of neonate's clinical parameters) Secondary outcomes: number of attempts, time to successful intubation, number of bradycardia episodes and lowest oxygen saturation during procedure, mucosal trauma, number of failures, and reason for intubation failure |
|
| Notes | Performed at the University of Montreal, Canada. Study was funded by American Academy of Pediatrics Neonatal Resuscitation Program Young Investigator Award and a Medical Education Research Grant from Direction de l'enseignement, Centre Hospotalier Universitaire Sainte‐Justine. Nondedicated educational grant from Ikaria Canada Inc. used to purchase the videolaryngoscope. Karl‐Storz Endoscopy loaned equipment (videolaryngoscope intubation blades) for this study, although they were not involved in study design, data collection, analysis, or publication. Ikaria Canada Inc. was not involved in study design, data collection, analysis, or publication. The authors declared no potential conflicts of interest. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Table of random numbers stratified by year of residency training |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes with the allocation group |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Study could not be blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Change in color of the carbon dioxide detector, vapor mist in the endotracheal tube, thoracic expansion, assessment of bilateral lung air entry, absence of air entry in the stomach by auscultation, and improvement of clinical parameters were used as objective criteria to assess intubation success. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 34 out of 37 enrolled residents completed the study; outcomes were reported for 34 residents. |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. |
| Other bias | Unclear risk | More than two‐thirds of intubations were nasotracheal |
O'Shea 2015.
| Study characteristics | ||
| Methods | Randomized controlled trial to compare intubation success by physicians with < 6 months' tertiary neonatal experience in neonates, with or without the videolaryngoscope screen visible to the instructor. Randomization was achieved through computer‐generated, variable‐size block‐randomization sequence, and allocation concealment was used. The study was conducted in Australia. | |
| Participants | Infants without facial or airway anomalies in the delivery room or intensive care unit. Infants were eligible if they needed intubation, and the intervention was going to be performed orally by a pediatric resident in their first 6 months of tertiary neonatal training. The unit of randomization was the intubation attempt, and only the first attempt was analyzed. 206 intubations were assessed. | |
| Interventions | All intubations were performed using the modified traditional Miller videolaryngoscope (LaryFlex, Acutronics, Hirzel, Switzerland) with the videolaryngoscope screen either visible to the instructor or covered during intubation. 104 intubations were assessed in the group with the video laryngoscopy screen visible to the instructor, and 102 intubations were performed with the videolaryngoscopy screen covered. | |
| Outcomes | First‐attempt intubation success rate confirmed by colorimetric detection of expired carbon dioxide. Secondary outcomes included the infant’s lowest heart rate, oxygen saturation, and duration of the attempt. | |
| Notes | Single‐center, unblinded study conducted in 2013 to 2014 at the Royal Women's Hospital, Melbourne, Australia, a tertiary perinatal centre. Funded by The Royal Women’s Hospital, Melbourne, Australia, and the Australian National Health and Medical Research Council Program (grant 606789). In Vitro Technologies provided a videolaryngoscope for the duration of the study but had no part in study design or data analysis. The authors indicated they had no financial relationships or conflicts of interest relevant to this article to disclose. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated, variable‐sized, block randomization sequence used |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, opaque envelopes with randomization cards |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participant could potentially know if the supervisor had access to the videolaryngoscope screen during their attempt, which could impact their performance. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Primary outcome was success at the intubation attempt. Endotracheal tube placement was confirmed by a colorimetric exhaled carbon dioxide detector, which is an objective criterion to assess intubation success. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | After randomization, only 7 neonates were excluded (3 in the intervention group and 4 in the control group); analysis on an intention‐to‐treat basis |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. |
| Other bias | Unclear risk | unknown |
Salama 2019.
| Study characteristics | ||
| Methods | Prospective randomised study comparing videolaryngoscopy with GlideScope to direct laryngoscopy for tracheal intubation in laterally positioned neonates. Random allocation was performed using computer‐generated numbers, using allocation concealment. The study was conducted in Egypt. | |
| Participants | American Society Anesthesiology physical status I or II neonates with normal craniofacial anatomy presenting for elective surgical repair of meningocele or myelomeningocele under general anesthesia. Exclusion criteria included the presence of suspected difficult intubation, high risk of pulmonary aspiration, and hemodynamic instability. | |
| Interventions | GlideScope videolaryngoscope compared to standard Miller direct laryngoscope. 60 neonates (30 in the videolaryngoscopy group and 30 in the direct laryngoscopy group) were included in the study. | |
| Outcomes | The primary outcome was the laryngeal view, graded using the POGO score. Secondary outcomes were time to the best glottis view, endotracheal tube passage time, intubation time, POGO scores after optimal external laryngeal maneuvers, intubation attempts, and overall success rate of intubation. Any trauma caused during laryngoscopy and any decrease in oxygen saturation < 95% were recorded. | |
| Notes | There were no funding sources for the study and authors disclosed no conflicts of interest with the study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomization was performed by an independent statistician in a 1:1 ratio. |
| Allocation concealment (selection bias) | Low risk | Allocation concealment was done by sequentially numbered, sealed, opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants could not be blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Except for the percentage of glottic opening score, all data were recorded by an independent observer not involved in the study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants randomised to each group were included in the outcomes. |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. |
| Other bias | Unclear risk | unknown |
Singh 2009.
| Study characteristics | ||
| Methods | Prospective randomised study to compare the Truview infant EVO2 laryngoscope with the Miller straight blade laryngoscope. The study was conducted in India. | |
| Participants | Neonates and infants of either sex undergoing surgery under general anesthesia, weighing 1 to 10 kg. Exclusion criteria included raised intracranial pressure, high risk for pulmonary aspiration of gastric contents, such as gastric outlet obstruction and bowel stasis, coagulopathy, and presence of any pathology of head and neck. 60 neonates and infants were enrolled in the study. | |
| Interventions | Intubation performed using the Truview infant blade (videolaryngoscopy group; 30 neonates and infants) compared with the Miller blade number 0 (direct laryngoscopy group; 30 neonates and infants) | |
| Outcomes | Number of attempts required for intubation, time for intubation, and the view of the glottis at laryngoscopy were scored according to the Cormack and Lehane grading criteria, were measured. Inability to intubate after three attempts was considered a failure to intubate. Hemoglobin, oxygen saturation, and all complications related to intubation were also recorded. | |
| Notes | Funding sources/declarations of interest were not stated | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomization done by chit in a box technique. |
| Allocation concealment (selection bias) | Unclear risk | No details given. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants could not be blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Time to intubation and intubation attempts were measured using objective criteria. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants randomised to each group were included in the outcomes. |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. |
| Other bias | Unclear risk | unknown |
Tao 2019.
| Study characteristics | ||
| Methods | Randomized study comparing videolaryngoscopy using GlideScope to direct laryngoscopy. Stratified block randomization and allocation concealment were used. This study was conducted in China. | |
| Participants | American Society of Anesthesiologists physical status I and II neonates scheduled to undergo elective surgery under general anesthesia. Neonates with increased intracranial pressure or increased risk of aspiration were excluded. 70 neonates of either sex were enrolled in the study. | |
| Interventions | GlideScope videolaryngoscope using size 1 blade compared to direct laryngoscope using Macintosh size 1 blade. 70 neonates were enrolled in the study (35 in the videolaryngoscopy group and 35 in the direct laryngoscopy group). | |
| Outcomes | The primary outcome was time to intubation. Secondary outcomes were the success rate of the first intubation attempt, number of intubation attempts, Cormack and Lehane grade of glottis view, and adverse events (trauma, desaturation, or bradycardia episodes). | |
| Notes | The study had no sources of funding support, and authors declared no conflicts of interest. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified blocked randomization |
| Allocation concealment (selection bias) | Low risk | An envelope containing the allocation information was given to the anesthesiologist who performed the intubation, and the anesthesiologist opened the envelope immediately before induction of anesthesia. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants could not be blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | An observer, who was blinded to neonate group assignment, was responsible for recording the time to intubation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants randomised to each group were included in the outcomes. |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. |
| Other bias | Unclear risk | unknown |
Volz 2018.
| Study characteristics | ||
| Methods | Randomized controlled trial to compare intubation success by first and second‐year pediatric residents in neonates, with or without guidance from the supervisor using videolaryngoscopy. 1:1 randomization and allocation concealment were used. This study was conducted in the United States. | |
| Participants | First‐ and second‐year pediatric residents were approached for inclusion in the study. Exclusion criteria included residents who declined participation in the study. 48 residents (with 24 in each group) were randomised. | |
| Interventions | Study intervention was resident coaching during intubation, with or without the use of video as a coaching tool; residents were identified as the study subjects. Videolaryngoscopy was performed using the C‐MAC laryngoscope with Miller blade size 0 or 1 (Karl Storz Co.), and direct laryngoscopy was performed using the Rusch laryngoscope with Miller blade size 00, 0, or 1 (Teleflex, Morrisville, NC). 101 non‐emergent intubations were analyzed (61 in the videolaryngoscopy group and 40 in the direct laryngoscopy group). | |
| Outcomes | Successful endotracheal intubation (defined as the placement of an endotracheal tube in the infant’s trachea) within two attempts. Intubations were confirmed by auscultation of breath sounds, observation of equal chest wall movement, change in a colorimetric carbon dioxide detector, presence of mist in the endotracheal tube, and chest radiograph. | |
| Notes | There was no funding support for the study, and the authors disclosed no conflicts of interest. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Residents were randomised by pulling concealed names out of a box using a 1:1 randomization scheme. |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Participants were not blinded to their assigned groups. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators who performed data analysis were blinded to the participants’ assigned study groups. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No participants were excluded. |
| Selective reporting (reporting bias) | Low risk | Investigators reported all outcomes that were specified in the protocol. |
| Other bias | Unclear risk | unknown |
ETT: endotracheal tube; NICU: neonatal intensive care unit ; POGO: percentage of glottis opening
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Fiadjoe 2012 | No neonates included in the study |
| Jagannathan 2017 | Included less than 5 neonates |
| Komasawa 2017 | Study in simulation |
| Manov 2020 | Included less than 5 neonates |
| Parmekar 2017 | Study conducted in neonatal manikins |
| Saran 2019 | Included less than 5 neonates |
| Sørensen 2012 | No neonates included in the study |
| Vlatten 2009 | Participants aged < 4 years, but no neonates |
Characteristics of studies awaiting classification [ordered by study ID]
Chae 2022.
| Methods | 40 infants under 12 months old were recruited from a single tertiary hospital from March 2020 to September 2021, and were randomly assigned to the direct laryngoscope group (N = 19, neonates = 4, infants = 15) or UEscope group (N = 21, neonates = 6, infants = 15). The UEscope may be a better choice for tracheal intubation than conventional direct laryngoscope in neonates and infants. |
| Participants | In this prospective, randomised, parallel, single‐blinded clinical trial, 40 neonates and infants who underwent elective general surgery in a single tertiary hospital between March 2020 and September 2021 were prospectively enrolled. Infants up to 12 months of age were included. Infants with a history of head and neck surgery or radiation therapy, possible congenital abnormality of the cervical vertebrae, and/or a history of tracheostomy, cricothyroidotomy, or intubation were excluded. |
| Interventions | During the study period, children were randomly assigned to two groups: the UEscope group (UE) and the conventional direct laryngoscope group (DL). |
| Outcomes | The primary outcome: time to intubation (TTI) using the UEscope compared to TTI when using the conventional direct laryngoscope for intubation in neonates and infants. The secondary outcomes: time to best view (TTBV), TTBV with and without the effects of the backward, upward, rightward, and posterior pressure (BURP) maneuver, the POGO score with and without the BURP maneuver, CL grade with and without the BURP maneuver, effects of the BURP maneuver on glottic view, number of attempts, rate of first attempt success, incidence of desaturation, lowest SpO₂ during intubation, and presence of intraoral bleeding |
| Notes | We are awaiting outcomes specific for neonates included in this study from the authors. Although the quality of glottic view was comparable in both groups, the TTI was significantly lower in the UEscope group in both the intention‐to‐treat (difference in the median between the groups ‐19.34 s, 95% CI ‐28.82 to ‐1.75; P = 0.0144), and as treated (difference in the median between the groups ‐11.24 s, 95% CI ‐21.73 to 0; P = 0.0488) analyses. |
Galante 2018a.
| Methods | Randomized trial to compare AirTraq optical laryngoscope versus Miller blade for ease of intubation |
| Participants | Neonates and infants age 0 to 1 year (98 participants), undergoing tracheal intubation during pediatric anesthesia and critical care procedures |
| Interventions | Intubation with AirTraq optical laryngoscope or conventional laryngoscope with Miller blade |
| Outcomes | Intubation attempts, time taken for intubation, ease of intubation, and percentage of glottic opening score |
| Notes | We contacted the first author for further details about number of neonates included, and are waiting for a reply. |
Garcia‐Marcinkiewicz 2020.
| Methods | Multicenter, randomised controlled trial comparing standard videolaryngoscopy using Storz C‐MAC Miller videolaryngoscope to direct laryngoscopy performed by anesthesia clinicians |
| Participants | Infants (aged < 12 months) under general anesthesia (564 participants). Inclusion criteria were undergoing a non‐cardiac procedure lasting longer than 30 minutes that required general anesthesia and orotracheal intubation by an anesthesiologist. Exclusion criteria were history of difficult intubation, history of craniofacial abnormalities, or prediction of difficult intubation that was based on physical examination. |
| Interventions | Videolaryngoscopy using Storz C‐MAC Miller videolaryngoscope compared to direct laryngoscopy. 564 infants were randomly assigned: 282 (50%) to video laryngoscopy and 282 (50%) to direct laryngoscopy |
| Outcomes | The primary outcome was the proportion of participants with successful orotracheal intubation on the first attempt. Secondary outcomes were the number of intubation attempts; time to successful orotracheal intubation; proportion of unsuccessful intubations with the randomly assigned device; and proportion of non‐severe and severe complications. |
| Notes | We contacted the first author for further details about the number of neonates included; we are awaiting a reply. |
Jain 2018.
| Methods | Prospective, randomised controlled trial to compare the intubation conditions achieved with the C‐MAC videolaryngoscope and the Miller laryngoscope in lateral position in infants |
| Participants | 64 children, less than one year of age, classified as American Society of Anesthesiologists physical status I to III, requiring endotracheal intubation. All children with anticipated difficult intubation or bag mask ventilation, hemodynamic instability, and raised intracranial pressure were excluded from the study. Children having a high risk for pulmonary aspiration of gastric contents requiring rapid sequence intubation were also not included in the trial. |
| Interventions | Randomized to intubation (N = 32) with C‐MAC videolaryngoscope or Miller laryngoscope (N = 32) |
| Outcomes | The primary outcome was total time for tracheal intubation. Secondary outcomes were intubation difficulty score, laryngoscope view, success rate, number of attempts, and optimizing maneuvers required. |
| Notes | We contacted the first author for further details about the number of neonates included; we are awaiting a reply. |
Yumul 2013.
| Methods | Randomized trial comparing the Video Miller device to a commonly used Miller blade for performing direct laryngoscopy and tracheal intubation in young children after a standardized inhalation induction of general anesthesia |
| Participants | Children younger than 3 years of age undergoing general anesthesia; sample size not available |
| Interventions | Intubation with Video Miller device or with a standard pediatric Miller blade |
| Outcomes | Time to glottic view, time to placement of the tube, time to observe an end‐tidal CO₂ waveform, number of intubation attempts, rating of glottic view, need to change to a different intubating device, and use of an adjuvant airway device |
| Notes | We contacted the first author for neonate data; we are awaiting a reply. |
BURP: backward, upward, rightward, and posterior pressure; CI: confidence interval; POGO: percentage of glottis opening; s: second; TTBV: time to best view; TTI: time to intubation
Characteristics of ongoing studies [ordered by study ID]
ACTRN12614001134617.
| Study name | HEADS UP Study. A randomised controlled clinical trial comparing C‐MACTM videolaryngoscope intubation with direct laryngoscope intubation in neonates |
| Methods | Randomized trial of babies born at ≥ 24 completed weeks' gestation, and requiring endotracheal intubation in the delivery room, or delivery theater, or in the neonatal intensive care unit, and aged 0 to 6 months Exclusion criteria: infants with major oral or upper airway malformation, emergency intubations, and babies < 24 weeks' gestation |
| Participants | Babies 0 to 6 months of age |
| Interventions | Intubation with C‐MAC videolaryngoscope versus direct laryngoscope |
| Outcomes | First attempt success rate; time to intubation; proportion of intubations occurring within the 30‐second American Academy of Pediatric guidelines; stability of infant during the intubation, measured by the length of time of hypoxia, based on infants saturations and heart rate; rate of complications related to intubation, such as trauma to lips, gums, pharynx, lacerations or perforation; and acceptability of the videolaryngoscope by the operator |
| Starting date | 2014 |
| Contact information | Sarah.Bellhouse@sswahs.nsw.gov.au |
| Notes | Date first registered: 24 October 2014 The principal investigator will be contacted for information regarding trial status. |
CTRI/2021/06/034029.
| Study name | Comparison of two videolaryngoscopes with direct laryngoscope for endotracheal intubation in neonates undergoing surgery under general anaesthesia |
| Methods | Randomized, parallel‐group trial Method of generating randomization sequence: permuted block randomization, fixed method of allocation concealment: sequentially numbered, sealed, opaque envelopes; blinding and masking: participant and outcome assessor blinded |
| Participants | Inclusion criteria: all term neonates of either sex undergoing surgical procedures under general anesthesia |
| Interventions | Interventions Intervention 1: C‐MAC Miller videolaryngoscope McGrath‐MAC videolaryngoscope: the technique of intubation will be similar in both McGrath MAC and C‐MAC Miller videolaryngoscopes. Laryngoscopic view will be graded by the intubating anesthesiologist using POGO score and modified Cormack‐Lehane grading. The tracheal intubation will be considered successful in presence of bilateral equal chest expansion, bilateral equal breath sounds on chest auscultation, and by appearance of square wave capnographic traces on the monitor. An attempt of intubation will be terminated if oxygen saturation (SpO₂) falls below 95%. Intervention 2: C‐MAC Miller videolaryngoscope and McGrath‐MAC videolaryngoscope: group A participants will be intubated using C‐MAC Miller and group B participants will be intubated using McGrath‐MAC videolaryngoscope. Laryngoscopic view will be graded by the intubating anesthesiologist using POGO score and modified Cormack‐Lehane grading. The tracheal intubation will be considered successful in presence of bilateral equal chest expansion, bilateral equal breath sounds on chest auscultation, and by appearance of square wave capnographic traces on the monitor. Intervention 3: C‐MAC Miller videolaryngoscope: C‐MAC Miller videolaryngoscope blade size 0 will be used for endotracheal intubation. Laryngoscopic view will be graded by the intubating anesthesiologist using POGO score and modified Cormack‐Lehane grading. The tracheal intubation will be considered successful in presence of bilateral equal chest expansion, bilateral equal breath sounds on chest auscultation, and by appearance of square wave capnographic traces on the monitor. Intervention 4: C‐MAC Miller videolaryngoscope: group A participants will be intubated using C‐MAC Miller videolaryngoscope blade 0. Laryngoscopic view will be graded. |
| Outcomes | Primary outcome 1. total time taken for successful endotracheal intubation Time point: at the time of intubation Secondary outcome 1. time for achieving the best glottic view, tube passage time, total tube insertion time 2. POGO score (percentage of glottic opening) 3. number of attempts for intubation 4. Cormack and Lehane grading (modified) 5. necessity of external laryngeal manipulation or repositioning of laryngoscope 6. number of attempts for successful intubation; time point: at the time of intubation |
| Starting date | Not yet recruiting |
| Contact information | Name: Nidhi Agrawal Address: Department of Anaesthesia and Intensive care. Ground floor, main operation theatre building. Safdarjung hospital and Vardhman Mahavir Medical College, New Delhi 110029, Delhi, India Telephone: 9811030408 Email: nidhi.agrawal1970@gmail.com Affiliation: Vardhman Mahavir Medical College and Safdarjung Hospital |
| Notes | Date of registration: 7 June 2021 |
CTRI/2022/04/041925.
| Study name | Comparison of MacGrath video laryngoscope with conventional Macintosh laryngoscope for endotracheal intubation in neonatal patients with normal airway: a prospective randomised comparative study |
| Methods | Condition: health condition 1: O ‐ Medical and Surgical |
| Participants | Inclusion criteria: 1. neonates posted for elective and emergency surgery under general anesthesia requiring endotracheal intubation 2. age: up to 1 month 3. gender: either gender 4. ASA I & II Exclusion criteria: 1. neonates with difficult airway: mouth opening of < 2 cm, Mallampatti class IV, limited neck extension, anatomical abnormality of airway 2. H/O convulsion 3. URTI (upper respiratory tract infection) 4. Preexisting laryngeal or tracheal pathology 5. Neonates' parents/guardian not willing for participation |
| Interventions | Intervention 1: Macintosh laryngoscope: Intubation is performed with Macintosh laryngoscope Intervention 2: Macgrath video laryngoscope: Intubation is performed with MacGrath video laryngoscope Control intervention1: Macgrath video laryngoscope and Macintosh laryngoscope: in one group intubation is performed with MacGrath video laryngoscope and in another group intubation is performed with Macintosh laryngoscope |
| Outcomes | Primary outcome: intubation time (time point: the time from insertion of the blade between the teeth until the first effective ventilation confirmed by capnography) secondary outcomes: 1. Cormack & Lehane grading 2. No. of attempts of device insertion (maximum 2), defined as each time the device was removed past the gum or teeth 3. Glottic exposure time: time from introduction of laryngoscope from teeth/gum till visualization of glottis 4. Optimization maneuvers required for intubation, i.e. BURP 5. Vital parameters: hemodynamic parameters, i.e. heart rate, SpO₂ are to be noted |
| Starting date | Not yet recruiting |
| Contact information | Name: Dr Neha Cheraya Address: Department of Anaesthesiology, New Surgical Block, Ssg Hospital, Vadodara. 390001 Vadodara, GUJARAT India Telephone: 9374679837 Email: ngcheraya@gmail.com Affiliation: Ssg Hospital,Vadodara |
| Notes | Date of registration: 19 April 2022 |
CTRI/2022/07/044293.
| Study name | Comparison of video laryngoscope versus Macintosh laryngoscope for elective tracheal intubation in infants ‐ a randomised interventional study |
| Methods | Comparison of video laryngoscope versus Macintosh laryngoscope for elective tracheal intubation in infants ‐ a randomised interventional study at SMS medical college, during 2021 to 2023 |
| Participants | Inclusion criteria: patients of either sex; aged younger than 1 year; ASA grade I & II; undergoing elective pediatric surgery requiring endotracheal intubation |
| Interventions | Intervention: video laryngoscopy: Tuoren video laryngoscope is used with 1 number blade for intubation in infants undergoing elective surgery up to 10 minutes after induction Control intervention: conventional MacIntosh laryngoscope used with blade 0 and 1 for intubation in infants undergoing elective surgery up to 10 minutes after induction |
| Outcomes | Primary outcome: to determine the time taken for intubation in both groups; time point: maximum, within 3 minutes Secondary outcomes: 1. First attempt intubation success rate; time point: within 1 minute of intubation 2. Complication rate in both groups; time point: within 1 minute of intubation 3. Ease of intubation score in both groups; time point: within 1 minute of intubation 4. Intubation difficult score in both groups; time point: within 1 minute of intubation |
| Starting date | Not yet recruiting |
| Contact information | Name: Pratibha Rathore Address: Department of Anaesthesiology,SMS Medical College and attached Hospitals, Adarsh Nagar, Jaipur 302004 Jaipur, RAJASTHAN India Telephone: 9414446473 Email: pratibha.rathore3@gmail.com Affiliation: SMS Medical College and attached Hospitals, Adarsh Nagar, Jaipur, Rajasthan |
| Notes | Date first registered: 25 July 2022 |
DRKS00020792.
| Study name | Evaluating the feasibility and safety of video laryngoscopy for routine nasotracheal intubation in neonates ‐ a randomised controlled pilot trial |
| Methods | Randomized controlled trial pilot study |
| Participants | Neonates. Inclusion criteria: indication for endotracheal intubation, age < 44 weeks postmenstrual age. Exclusion criteria: declined participation, equipment failure, personnel not confident, intubation outside neonatal intensive care unit or delivery suite |
| Interventions | Nasotracheal intubation using video laryngoscopy (Acutronic Infantview) compared with conventional laryngoscopy |
| Outcomes | Primary outcome: first‐pass success rate Secondary outcomes: adverse events, desaturations, COMFORTneo score, endotracheal tube position on X‐ray, Cormack‐Lehane classification system, and questionnaires on satisfaction and perception |
| Starting date | Approval date 29 August 2019 |
| Contact information | |
| Notes | Date first registered: 06 August 2021 |
NCT04295902.
| Study name | Laryngoscopy for neonatal and infant aIrway management wIth supplemental oxygEn (OPTIMISE): a multicenter prospective randomised controlled trial |
| Methods | Randomized trial to compare tracheal intubation first attempt success rate with the C‐MAC indirect videolaryngoscope compared to a standard direct laryngoscope, either in the operating room or intensive care unit, to demonstrate that with oxygen supplementation, the difference in the first‐attempt success rate in favor of VL is negligible |
| Participants | inclusion criteria: Infants up to three months of age requiring tracheal intubation in the pediatric operating room or the pediatric or neonatal intensive care unit Exclusion criteria: prediction of difficult intubation, congenital heart disease, cardiopulmonary collapse, intubation for emergency surgical and non‐surgical indications |
| Interventions | Intubation with C‐MAC indirect videolaryngoscope with Miller blades compared to direct laryngoscope with Miller blades |
| Outcomes | Primary outcome: tracheal intubation first attempt success rate Secondary outcomes: occurrence and duration of moderate and severe desaturation, overall number of attempts, time required for intubation, first EtCO₂ after successful intubation, percentage of glottic opening score, use of additional devices, and respiratory complications |
| Starting date | 4 January 2020 |
| Contact information | Thomas Riva, MD (thomasriva@me.com). |
| Notes | First registered: 05 March 2020 |
NCT04994652.
| Study name | Video‐ or direct laryngoscopy for endotracheal intubation in newborns (VODE) |
| Methods | The investigators will study newborn infants who are undergoing intubation at the discretion of their treating clinicians in delivery room or in the neonatal intensive care unit (NICU) |
| Participants | Term and preterm infants of any gender will be eligible to participate. Babies with upper airway anomalies will be ineligible. |
| Interventions | Participants will be randomly assigned in a 1:1 ratio to video or standard group. Intubation success will be determined in both groups using an exhaled carbon dioxide detector or flow sensor. Caregivers and outcome assessors will not be masked to group assignment. The investigators will enroll 214 babies to the study. |
| Outcomes | Primary outcome: 1. intubation success at first attempt, time frame: 5 minutes, confirmed with an exhaled carbon dioxide detector or flow sensor Secondary Outcomes
|
| Starting date | 4 September 2021 |
| Contact information | Colm PF O'Donnell, MB PhD 35316373100 codonnell@nmh.ie |
| Notes | Estimated study completion date: 31 October 2023 |
Differences between protocol and review
We changed the unit of analysis from participant to intubation attempts. The reason for this change is that it was impossible to separate the number of intubations for each participant.
We added the secondary outcome; desaturation (O₂ saturation less than 95%) or bradycardia (heart rate less than 100 beats per minute) episodes, or both, to account for studies that reported episodes of desaturation and/or bradycardia without details of the event.
We added the methodology and plan for summary of findings tables and GRADE recommendations, which were not included in the original protocol.
We updated our methods to the new Cochrane standards.
Contributions of authors
KL, NN, and MP reviewed the literature, performed the analysis, and wrote the review.
JA and CF critiqued, and helped to incorporate peer review comments into the review.
Sources of support
Internal sources
-
None, Other
none
External sources
-
Vermont Oxford Network, USA
Cochrane Neonatal Reviews are produced with support from Vermont Oxford Network, a worldwide collaboration of health professionals dedicated to providing evidence‐based care of the highest quality for newborn infants and their families.
Declarations of interest
KL: works as a health professional in Neonatology at Children's Hospital of Philadelphia, USA
NN: works as a health professional in Neonatology at Baylor College of Medicine/Texas Children's Hospital, USA
JA: works as a health professional in Neonatology at Boston Children’s Hospital, USA
CF: works as a health professional in Neonatology at Texas Children's Hospital, USA
MP: works as a health professional in Neonatology at Baylor College of Medicine/Texas Children's Hospital, USA; he is an Associate Editor for Cochrane Neonatal, however, he was not involved in the editorial process for this review
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Bartle 2019 {published and unpublished data}
- Bartle DG, Powell R, Pearson K, Adeboye TS. Video vs direct laryngoscopy. Success rates and confidence: a feasibility study. Infant 2019;15(5):1-4. [DOI: 10.1007/s12630-016-0792-x] [DOI] [Google Scholar]
Kamath 2020a {published data only}
- Kamath N, Dogra N, Gupta A. Comparison of ease of intubation with airtraq optical laryngoscope versus Miller laryngoscope in neonates – a randomised interventional study. Indian Journal of Anaesthesia 2020;64(13):S24-5. [Google Scholar]
Moussa 2016 {published data only}
- Moussa A, Luangxay Y, Tremblay S, Lavoie J, Aube G, Savoie E, et al. Videolaryngoscope for teaching neonatal endotracheal intubation: a randomized controlled trial. Pediatrics 2016;137(3):e20152156. [DOI: 10.1542/peds.2015-2156] [PMID: ] [DOI] [PubMed] [Google Scholar]
O'Shea 2015 {published data only}
- O'Shea JE, Thio M, Kamlin CO, McGrory L, Wong C, John J, et al. Videolaryngoscopy to teach neonatal intubation: a randomized trial. Pediatrics 2015;136(5):912-9. [DOI: 10.1542/peds.2015-1028] [PMID: ] [DOI] [PubMed] [Google Scholar]
Salama 2019 {published data only}
- Salama ER, El Amrousy D. GlideScope® cobalt video laryngoscope versus direct Miller laryngoscope for lateral position-tracheal intubation in neonates with myelodysplasia: a prospective randomized study. Saudi Journal of Anaesthesia 2019;13:28-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Singh 2009 {published data only}
- Singh R, Singh P, Vajifdar H. A comparison of Truview infant EVO2 laryngoscope with the Miller blade in neonates and infants. Paediatric Anaesthesia 2009;19(4):338-42. [DOI: 10.1111/j.1460-9592.2009.02929.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
Tao 2019 {published data only}
- Tao B, Liu K, Zhao P, Wang D, Liu Y, Yin H. Comparison of glidescope video laryngoscopy and direct laryngoscopy for tracheal intubation in neonates. Anesthesia and Analgesia 2019;129(2):482-6. [DOI] [PubMed] [Google Scholar]
Volz 2018 {published data only}
- Volz S, Stevens TP, Dadiz R. A randomized controlled trial: does coaching using video during direct laryngoscopy improve residents’ success in neonatal intubations? Journal of Perinatology May 2018;38(8):1074-80. [PMID: ] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Fiadjoe 2012 {published and unpublished data}
- Fiadjoe JE, Gurnaney H, Dalesio N, Sussman E, Zhao H, Zang X, et al. A prospective randomized equivalence trial of the GlideScope Cobalt video laryngoscope to traditional direct laryngoscopy in neonates and infants. Anesthesiology 2012;116(3):622-8. [DOI: 10.1097/ALN.0b013e318246ea4d] [PMID: ] [DOI] [PubMed] [Google Scholar]
Jagannathan 2017 {published data only}
- Jagannathan N, Hajduk J, Sohn L, Huang A, Sawardekar A, Albers B, et al. Randomized equivalence trial of the King Vision aBlade videolaryngoscope with the Miller direct laryngoscope for routine tracheal intubation in children < 2 yr of age. British Journal of Anesthesia 2017;118(6):932-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
Komasawa 2017 {published data only}
- Komasawa N, Hattori K, Mihara R, Minami T. Direct laryngoscopy training is important for videolaryngoscopy skill acquisition. British Journal of Anaesthesia 2017;118(2):269-70. [DOI: 10.1093/bja/aew458] [PMID: ] [DOI] [PubMed] [Google Scholar]
Manov 2020 {published and unpublished data}
- Manirajan M, Bidkar PU, Sivakumar RK, Lata S, Srinivasan G, Jha AK. Comparison of paediatric King Vision™ videolaryngoscope and Macintosh laryngoscope for elective tracheal intubation in children of age less than 1 year: a randomised clinical trial. Indian Journal of Anesthesia 2020;64(11):943-8. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Parmekar 2017 {published data only}
- Parmekar S, Arnold JL, Anselmo C, Pammi M, Hagan J, Fernandes CJ, et al. Mind the gap: can videolaryngoscopy bridge the competency gap in neonatal endotracheal intubation among pediatric trainees? A randomized controlled study. Journal of Perinatology 2017;37(8):979-83. [DOI: 10.1038/jp.2017.72] [PMID: ] [DOI] [PubMed] [Google Scholar]
Saran 2019 {published data only}
- Saran A, Dave NM, Karnik PP. Efficacy and safety of videolaryngoscopy-guided verbal feedback to teach neonatal and infant intubation. A prospective randomised cross-over study. Indian Journal of Anesthesia 2019;63(10):791-6. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sørensen 2012 {published data only}
- Sørensen M, Holm-Knudsen R. Endotracheal intubation with Airtraq® versus Storz® videolaryngoscope in children younger than two years – a randomized pilot-study. BMC Anesthesiology 2012;12:7. [DOI: 10.1186/1471-2253-12-7] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Vlatten 2009 {published data only}
- Vlatten A, Aucoin S, Litz S, Macmanus B, Soder C. A comparison of the STORZ video laryngoscope and standard direct laryngoscopy for intubation in the pediatric airway – a randomized clinical trial. Paediatric Anaesthesia 2009;19(11):1102-7. [DOI: 10.1111/j.1460-9592.2009.03127.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Chae 2022 {published and unpublished data}
- Chae MS, Chung JH, Shim JW, Park JS, Bae JH, Lee HM. Comparison of the UE scope video laryngoscope with the traditional direct laryngoscope in neonates and infants: a randomized clinical trial. Children (Basel, Switzerland) 2022;9(8):1161. [DOI: 10.3390/children9081161] [DOI] [PMC free article] [PubMed] [Google Scholar]
Galante 2018a {published data only}
- Galante D, Consani G. Use of tracheal intubation with Miller laryngoscope versus the AirTraq Optical laryngoscope in pediatric patient. Pediatric Critical Care Medicine 2018;19:67. [Google Scholar]
Garcia‐Marcinkiewicz 2020 {published data only}
- Garcia-Marcinkiewicz AG, Kovatsis PG, Hunyady AI, Olomu PN, Zhang B, Sathyamoorthy M, et al. First-attempt success rate of video laryngoscopy in small infants (VISI): a multicentre, randomised controlled trial. Lancet 2020;396:10266. [DOI] [PubMed] [Google Scholar]
Jain 2018 {published data only}
- Jain D, Mehta S, Gandhi K, Arora S, Parikh B, Abas M. Comparison of intubation conditions with CMAC Miller videolaryngoscope and conventional Miller laryngoscope in lateral position in infants: a prospective randomized trial. Paediatric Anaesthesia 2018;28(3):226-30. [DOI] [PubMed] [Google Scholar]
Yumul 2013 {published and unpublished data}
- NCT01371032. Study to compare Video Miller Device to direct laryngoscopy [A randomized, prospective study to compare the Video Miller Device to direct laryngoscopy using a standard pediatric Miller Blade for tracheal intubation of children < 3 years of age undergoing general anesthesia]. https://clinicaltrials.gov/ct2/show/NCT01371032 (first received 10 June 2011).
- Yumul R, Elvir Lazo OL, Glenn T, Mathoni A, Filsinger DB, Hemaya EG, et al. A randomized, prospective study comparing the video Miller device to a standard pediatric Miller blade for direct laryngoscopy and tracheal intubation of young children. In: Scientific Abstract Guide, Anesthesiology 2013, Annual meeting of American Society of Anesthesiologists, October 12 - 16, 2013; San Francisco, California. San Francisco, California: American Society of Anesthesiologists, 2013:101.
References to ongoing studies
ACTRN12614001134617 {unpublished data only}
- ACTRN12614001134617. A randomised controlled clinical trial comparing C-MAC (™) videolaryngoscope intubation with direct laryngoscope intubation in neonates. The HEADS UP Study. anzctr.org.au/Trial/Registration/TrialReview.aspx?id=367096 (first received 24 October 2014).
CTRI/2021/06/034029 {published data only}
- CTRI/2021/06/034029. Comparison of two videolaryngoscopes with direct laryngoscope for endotracheal intubation in neonates undergoing surgery under general anaesthesia. trialsearch.who.int/Trial2.aspx?TrialID=CTRI/2021/06/034029 (first received 7 June 2021).
CTRI/2022/04/041925 {published data only}
- CTRI/2022/04/041925. Comparison of MacGrath video laryngoscope and Macintosh laryngoscope for intubation in neonatal patients. trialsearch.who.int/Trial2.aspx?TrialID=CTRI/2022/04/041925 (first received 19 April 2022).
CTRI/2022/07/044293 {published data only}
- CTRI/2022/07/044293. P.G. Study plan, comparison of video laryngoscope versus Macintosh laryngoscope for elective tracheal intubation in infants - a randomised interventional study at SMS meical college, during 2021-2023. trialsearch.who.int/Trial2.aspx?TrialID=CTRI/2022/07/044293 (first received 25 July 2022).
DRKS00020792 {published data only}
- DRKS00020792. Evaluating the feasibility and safety of video laryngoscopy for routine nasotracheal intubation in neonates – a randomized controlled pilot trial. drks.de/DRKS00020792 (first received 7 February 2020).
NCT04295902 {unpublished data only}
- NCT04295902. Laryngoscopy for neonatal and infant airway management wIth supplemental oxygen (OPTIMISE): a multi-center prospective randomized controlled trial. clinicaltrials.gov/ct2/show/NCT04295902 (first received 5 March 2020).
NCT04994652 {published data only}
- NCT04994652. Video or direct laryngoscopy for endotracheal intubation in newborns (VODE). clinicaltrials.gov/ct2/show/NCT04994652 (first received 6 August 2021).
Additional references
Asai 2008
- Asai T, Enomoto Y, Shimizu K, Shingu K, Okuda Y. The Pentax-AWS video-laryngoscope: the first experience in one hundred patients. Anesthesia and Analgesia 2008;106(1):257-9. [DOI: 10.1213/01.ane.0000287647.46165.bc] [PMID: ] [DOI] [PubMed] [Google Scholar]
Aziz 2012
- Aziz MF, Dillman D, Fu R, Brambrink AM. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology 2012;116(3):629-36. [DOI: 10.1097/ALN.0b013e318246ea34] [PMID: ] [DOI] [PubMed] [Google Scholar]
Cochrane EPOC Group 2017
- Cochrane Effective Practice and Organisation of Care (EPOC). Data collection form. EPOC Resources for review authors, 2017. Available from epoc.cochrane.org/resources/epoc-specific-resources-review-authors (accessed 11 June 2022).
Deeks 2022
- Deeks JJ, Higgins JPT, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor)s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
Falck 2003
- Falck AJ, Escobedo MB, Baillargeon JG, Villard LG, Gunkel JH. Proficiency of pediatric residents in performing neonatal endotracheal intubation. Pediatrics 2003;112(6 Pt 1):1242-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT 2022 [Computer program]
- GRADEpro GDT. McMaster University and Evidence Prime, Version accessed 12 December 2022. Hamilton (ON): McMaster University (developed by Evidence Prime), 2022. Available at gradepro.org.
Griesdale 2012
- Griesdale DE, Liu D, McKinney J, Choi PT. Glidescope(R) video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. Canadian Journal of Anaesthesia 2012;59(1):41-52. [DOI: 10.1007/s12630-011-9620-5] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 2008
- Guyatt GH. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Healy 2012
- Healy DW, Maties O, Hovord D, Kheterpal S. A systematic review of the role of videolaryngoscopy in successful orotracheal intubation. BMC Anesthesiology 2012;12:32. [DOI: 10.1186/1471-2253-12-32] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2017
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (updated September 2020). Available from www.training.cochrane.org/handbook.
Higgins 2021
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Notes on subgroup analyses and meta‐regression. In: Introduction to Meta‐Analysis . John Wiley & Sons, Ltd, 2021:213-9. [DOI: 10.1002/9780470743386.ch21] [DOI] [Google Scholar]
Higgins 2022
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors) . Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.. Cochrane Collaboration, 2022. [Google Scholar]
Hirabayashi 2007
- Hirabayashi Y, Seo N. Tracheal intubation by non-anaesthetist physicians using the Airway Scope. Emergency Medicine Journal 2007;24(8):572-3. [DOI: 10.1136/emj.2007.048546] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hirabayashi 2008
- Hirabayashi Y, Seo N. Airway Scope: early clinical experience in 405 patients. Journal of Anesthesia 2008;22(1):81-5. [DOI: 10.1007/s00540-007-0580-4] [PMID: ] [DOI] [PubMed] [Google Scholar]
Kattwinkel 2011
- Kattwinkel J. Textbook of Neonatal Resuscitation. 6th edition. Elk Grove Village (IL): American Academy of Pediatrics and American Heart Association, 2011. [Google Scholar]
Kim 2008
- Kim JT, Na HS, Bae JY, Kim DW, Kim HS, Kim CS, et al. GlideScope video laryngoscope: a randomized clinical trial in 203 paediatric patients. British Journal of Anaesthesia 2008;101(4):531-4. [DOI] [PubMed] [Google Scholar]
Lim 2005
- Lim TJ, Lim Y, Liu EH. Evaluation of ease of intubation with the GlideScope or Macintosh laryngoscope by anaesthetists in simulated easy and difficult laryngoscopy. Anaesthesia 2005;60(2):180-3. [DOI: 10.1111/j.1365-2044.2004.04038.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
Maharaj 2006
- Maharaj CH, Costello JF, Higgins BD, Harte BH, Laffey JG. Learning and performance of tracheal intubation by novice personnel: a comparison of the Airtraq and Macintosh laryngoscope. Anaesthesia 2006;61(7):671-7. [DOI: 10.1111/j.1365-2044.2006.04653.x] [PMID: ] [DOI] [PubMed] [Google Scholar]
NCT01793727
- NCT01793727. Learning curve of the Infant Glidescope® Cobalt Video Laryngoscope in anesthesiology residents. clinicaltrials.gov/show/NCT01793727 (first received 15 February 2013).
Page 2021
- Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 2021;372:n160. [DOI: 10.1136/bmj.n160] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pott 2008
- Pott LM, Murray WB. Review of video laryngoscopy and rigid fiberoptic laryngoscopy. Current Opinion in Anaesthesiology 2008;21(6):750-8. [DOI: 10.1097/ACO.0b013e3283184227] [PMID: ] [DOI] [PubMed] [Google Scholar]
Review Manager 2020 [Computer program]
- Review Manager 5 (RevMan 5). Version 5.4. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2020.
Roberts 2006
- Roberts KD, Leone TA, Edwards WH, Rich WD, Finer NN. Premedication for nonemergent neonatal intubations: a randomized, controlled trial comparing atropine and fentanyl to atropine, fentanyl, and mivacurium. Pediatrics 2006;118(4):1583-91. [DOI: 10.1542/peds.2006-0590] [PMID: ] [DOI] [PubMed] [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
Shippey 2007
- Shippey B, Ray D, McKeown D. Case series: the McGrath videolaryngoscope – an initial clinical evaluation. Canadian Journal of Anaesthesia 2007;54(4):307-13. [PMID: ] [DOI] [PubMed] [Google Scholar]
Shippey 2008
- Shippey B, Ray D, McKeown D. Use of the McGrath videolaryngoscope in the management of difficult and failed tracheal intubation. British Journal of Anaesthesia 2008;100(1):116-9. [DOI] [PubMed] [Google Scholar]
Thong 2009
- Thong SY, Lim Y. Video and optic laryngoscopy assisted tracheal intubation – the new era. Anaesthesia and Intensive Care 2009;37(2):219-33. [PMID: ] [DOI] [PubMed] [Google Scholar]
Vanderhal 2009
- Vanderhal AL, Berci G, Simmons CF Jr, Hagiike M. A videolaryngoscopy technique for the intubation of the newborn: preliminary report. Pediatrics 2009;124(2):e339-46. [DOI: 10.1542/peds.2008-3653] [PMID: ] [DOI] [PubMed] [Google Scholar]
Weiss 2001
- Weiss M, Schwarz U, Dillier CM, Gerber AC. Teaching and supervising tracheal intubation in paediatric patients using videolaryngoscopy. Pediatric Anesthesia 2001;11(3):343-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Xue 2006
- Xue F, Zhang G, Liu J, Li X, Sun H, Wang X, et al. A clinical assessment of the GlideScope videolaryngoscope in nasotracheal intubation with general anesthesia. Journal of Clinical Anesthesia 2006;18(8):611-5. [DOI: 10.1016/j.jclinane.2006.03.018] [PMID: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Lingappan 2015
- Lingappan K, Arnold JL, Shaw TL, Fernandes CJ, Pammi M. Videolaryngoscopy versus direct laryngoscopy for tracheal intubation in neonates. Cochrane Database of Systematic Reviews 2015, Issue 2. Art. No: CD009975. [DOI: 10.1002/14651858.CD009975.pub3] [DOI] [PubMed] [Google Scholar]
Lingappan 2018
- Lingappan K, Arnold JL, Fernandes CJ, Pammi M. Videolaryngoscopy versus direct laryngoscopy for tracheal intubation in neonates. Cochrane Database of Systematic Reviews 2018, Issue 6. Art. No: CD009975. [DOI: 10.1002/14651858.CD009975.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]