

Abstract
Narcissistic personality disorder (NPD) is a commonly encountered diagnosis, affecting approximately 1%–6% of the population, with no evidence-based treatments. Recent scholarship has focused on self-esteem dysregulation as a key component of NPD: Excessively high expectations for oneself and how one should be treated leads to brittle self-esteem and maladaptive reactions to self-esteem threats. The current article builds on this formulation, introducing a cognitive-behavioral model of narcissistic self-esteem dysregulation that clinicians can use in providing a relatable model of change for their patients. Specifically, symptoms of NPD can be seen as a set of cognitive and behavioral habits that serve to regulate difficult emotions emerging from maladaptive beliefs and interpretations of self-esteem threats. This perspective renders narcissistic dysregulation amenable to cognitive-behavioral therapy (CBT) in which patients learn skills that help them gain awareness around these habitual reactions, reshape cognitive distortions, and engage in behavioral experiments that serve to transform maladaptive belief systems that consequently free them from symptomatic reactions. Here, we provide a precis of this formulation and examples of how CBT skills can be used to treat narcissistic dysregulation. We also discuss future research that could provide empirical support for the model and test the efficacy of CBT approaches to NPD. Conclusions focus on the notion that narcissistic self-esteem dysregulation likely varies continuously in the population and transdiagnostically across disorders. Greater insight into the cognitive-behavioral mechanisms of self-esteem dysregulation could foster tools for ameliorating distress both in people with NPD and the general populace.
Keywords: Narcissistic personality disorder, cognitive-behavioral therapy, self-esteem, exposure therapy, core beliefs, narcissism, cognitive therapy
It makes sense to want to feel good about oneself. Decades of research suggest that high self-esteem—one’s evaluation of how good, competent, attractive, influential, and socially regarded one is (1–4)—portends positive mental health outcomes (5–7). However, it is possible to have too much of a good thing. A grandiose sense of self-importance, entitlement, and need for admiration can produce considerable intrapersonal and interpersonal difficulties, culminating into a diagnosis of narcissistic personality disorder (NPD) (8, 9), an impairing condition that affects 1%–6% of the U.S. population (10, 11). What distinguishes healthy self-esteem from narcissistic grandiosity? We begin by summarizing research on this question, arriving at the notion that self-esteem regulation is a transdiagnostic psychological process that becomes dysregulated in NPD. We then articulate a cognitive-behavioral formulation of narcissistic self-esteem dysregulation, showing how this dysregulation can be seen as interactions between beliefs, thoughts, feelings, and behaviors. This broadly applicable perspective offers hope for NPD treatment, as it renders self-esteem dysregulation amenable to intervention through cognitive-behavioral therapy (CBT), which has been found effective for several other psychiatric disorders. We then illustrate how key CBT techniques could be applied before concluding with a discussion of the implications of the model and future directions of research.
Narcissism and Its Treatment
Over decades of scholarship spanning psychoanalytic traditions, personality psychology, and clinical science, researchers have sought to characterize the psychological processes that drive pathological narcissism. Although numerous theoretical frameworks have been developed and continue to evolve, they share an understanding that maladaptive patterns of self-esteem regulation are central to pathological narcissism (12). Data show that, unlike normative, healthy self-esteem, which is associated with positive outcomes (5–7), narcissistic self-esteem is fragile, because it is highly contingent on achievement-related successes and feedback from the social environment (13–15).
Narcissistic self-esteem is thus conceptualized as precariously elevated. When an individual with NPD is faced with an ego threat (e.g., real or imagined criticism, failure, or reduced social regard), unrealistically high self-expectations crumple into perceived inferiority (16, 17). Individuals with NPD are, therefore, hypersensitive to ego threats, and when threatened, they respond with efforts to reduce concomitant distress and upregulate self-esteem (17–19). These regulation strategies include some of NPD’s most recognizable and maladaptive behaviors. Classic “grandiose” responses include being aggressive or devaluing toward others (20, 21), fixating on grandiose fantasies (22), or engaging in self-serving bias (23). Classic “vulnerable” responses include alienating and isolating themselves (24) by avoiding situations that may threaten self-esteem (25), relentlessly criticizing themselves (26–28), or engaging in suicidal behaviors and fantasies (29, 30). This vacillation between overly inflated and deflated self-appraisals, alongside efforts to regulate this unstable sense of self through grandiosity, flawlessness, and/or avoidance, are described in both early psychoanalytic theories of narcissism (31), the contemporary Alternative DSM-5 Model for Personality Disorders (8), and the personality disorder section of the ICD-11 (32–34).
It is important to note that research is continually adding nuance to scientific perspectives on self-esteem in NPD (35). Various frameworks differently emphasize shifts between distinct states of grandiosity (i.e., elevated self-esteem, arrogance, and entitlement) and vulnerability (i.e., shame, insecurity, and neuroticism). Scholars are working to clarify whether and how grandiosity may function to conceal ever-present vulnerability and whether fragile self-esteem is a driving force or an outcome of this process (17, 18, 26, 36). Recent proposals also offer a more complex and dynamic view beyond shifting grandiosity and vulnerability (35). In the midst of the field coming to a consensus regarding how to best conceptualize “narcissism,” we offer a cognitive-behavioral model proposing that symptoms of NPD are driven by narcissistic self-esteem dysregulation, which is characterized by fragile self-esteem (maintained by unrealistic beliefs about one’s importance, abilities, influence, or social regard) and habitual maladaptive behavioral strategies that prop up elevated self-esteem.
Despite the high prevalence of harmful outcomes of NPD, few psychotherapeutic treatments for NPD exist, and none have been empirically tested (12, 37). Existing treatments for narcissistic processes are largely psychoanalytic (38, 39). More recently, evidence-based psychotherapies for borderline personality disorder, a related but distinct diagnosis from NPD, have steadily been adapted for NPD. Transference-focused psychotherapy (40), mentalization-based treatment (41), good psychiatric management (42), and dialectical behavior therapy (43) have all adjusted protocols originally for borderline personality disorder to more directly address the unique aspects of NPD. However, none of these adapted therapies have been systematically tested, and developing accessible and pragmatic NPD treatments is critical (44, 45). Given its effective application to a wide range of disorders, CBT stands as a clear choice for guiding the development of novel NPD interventions.
The CBT Model
CBT is a family of short-term, structured, and problem-focused psychotherapeutic treatments that primarily utilize cognitive (thought- and meaning-related) and behavioral (response- and action-related) interventions aimed at improving psychological functioning (46, 47). The central theoretical model underlying CBT posits that thoughts, behaviors, and emotions dynamically influence and maintain one another. These processes ideally serve adaptive functions, such as helping individuals accomplish their goals, navigate their environment, and ultimately survive (48). However, sometimes these cognitive-behavioral systems become dysregulated and produce symptoms of psychopathology. As we illustrate later, this is particularly the case when individuals believe that they cannot cope with situations that are actually tolerable and when they maintain these beliefs by habitually avoiding or escaping unwanted emotions aroused by situations that trigger these emotions (49). CBT models have been tailored to treat specific disorders, such as major depressive disorder (50, 51), posttraumatic stress disorder (PTSD) (52, 53), and borderline personality disorder (54). Transdiagnostic approaches such as the Unified Protocol (49) and the Modular Approach to Treating Children (or MATCH) (55), have also been developed to treat multiple disorders simultaneously or serially.
A transdiagnostic CBT model is presented in Figure 1, which we illustrate using an example patient with social anxiety disorder. The patient’s highly distressing fears that they will embarrass themselves lead to chronic avoidance of social situations. CBT typically begins with psychoeducation, in which patients learn how emotions have adaptive functions (e.g., anxiety helps prepare for and avoid possible danger) and how they are are beneficial when calibrated to reality (i.e., aligned and proportionate to the facts of a given situation) (56). Through both didactic discussion and self-monitoring homework exercises, patients learn about the CBT model of psychopathology. They learn to see their symptoms as recurring cycles of thoughts, feelings, and behaviors; how these cycles emerge in response to situations because of underlying belief systems; and how habitual cognitive and behavioral reactions to these situations only serve to reinforce these beliefs, thereby maintaining their problem.
FIGURE 1.
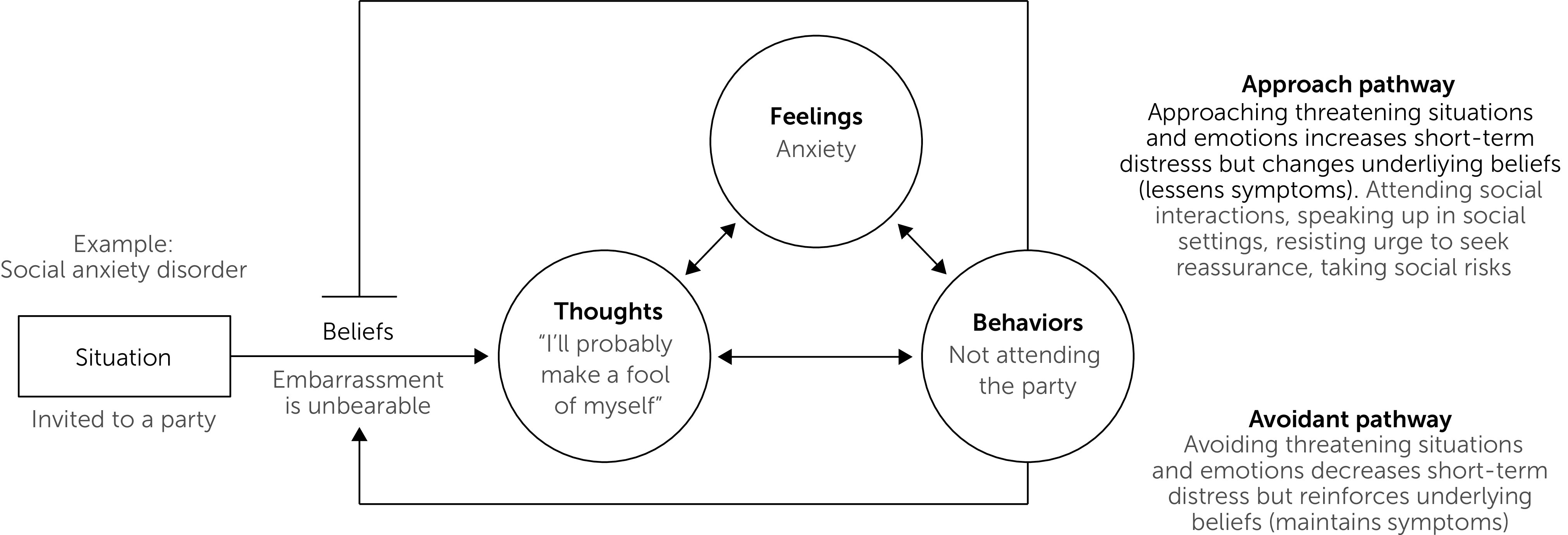
General cognitive-behavioral therapy (CBT) model, illustrated using an example patient with social anxiety disorder indicated in gray texta
aIn CBT, patients learn to see their psychological experiences as composed of three components visualized by the circles in the center of the model: thoughts (i.e., their automatic interpretations and narratives about the world), feelings (i.e., their physiological and emotional reactions), and behaviors (i.e., the ways they choose to respond to situations). These three components continuously influence each other and comprise the patient’s symptoms. These reactions emerge because of how beliefs (i.e., one’s inner network of commitments, assumptions, expectations, and predictions about the world, symbolized by the rightward-pointing arrow) interact with specific situations. For example, when this patient is invited to a party, their belief that embarrassment is unbearable leads them to think about what a fool they will be, generating substantial anxiety and a desire to avoid the party. Patients also learn how behaviors in the avoidant path (lower line ending in an arrow symbol) move them away from the situations and emotions that bring them distress. Although this often immediately reduces their distress, it only reinforces their underlying beliefs (e.g., avoiding parties keeps one “safe” from embarrassment). Because this reinforces the underlying belief, they re-experience the same reactions to similar situations in the future. Patients thus are encouraged to choose the approach pathway (upper line ending in a horizontal bar, which represents “blocking” the belief). These behaviors bring them close to their feared situations, which temporarily increases distress but helps them learn new things about the world and erode their underlying beliefs. For example, attending the party gives the patient an opportunity to learn that they can tolerate (or even enjoy) social situations. Transforming the patient’s beliefs (e.g., to “I can handle embarrassment” or “socializing can be fun, even if I might mess up”) allows them to engage with social situations with reduced distress and avoidance.
For example, when a patient is invited to a party, the belief that “embarrassment is unbearable” becomes activated, leading to a negative automatic thought (e.g., “I’ll probably make a fool of myself”) and concomitant feelings (e.g., anxiety, elevated heart rate, or tension or tightness in the pit of their stomach). Although habitual strategies for regulating these feelings (e.g., avoiding the party) may immediately reduce distress, they only reinforce the maladaptive belief that embarrassment is unbearable by generating additional evidence that one must avoid social gatherings to be “safe” from embarrassment. Reinforcing this belief means that the same cycle of symptoms will arise in future social situations. During treatment, these behaviors will consequently be labeled as part of an “avoidant” pathway that is ultimately unhelpful to long-term well-being. The patient will be encouraged to replace these avoidant responses with skills that move them down an “approach” pathway. Although approaching social situations and embarrassment (e.g., attending parties or speaking in social settings) can generate distress, doing so gives patients evidence that can erode underlying maladaptive beliefs. For example, signing up for improvisation classes and learning that they can survive an hour in the spotlight can help patients form new beliefs that embarrassment is tolerable, thus freeing them from social anxiety. Note that although this example focuses on social anxiety disorder, these dynamics are also highly relevant to narcissistic dysregulation (discussed later).
There are many CBT techniques for shifting patients from avoidance to approach pathways and transforming their underlying beliefs. Two major classes of interventions include cognitive and behavioral skills. Cognitive interventions ultimately aim to increase the flexibility with which patients think about themselves, others, and the world (57). Patients first learn about different layers of cognition, including their “automatic thoughts” (i.e., immediate, situation-specific interpretations that come to a person’s mind throughout the day), “intermediate beliefs” (i.e., general attitudes and assumptions that give rise to automatic thoughts such as, “If I don’t wash my hands, then I’ll get sick”), and “core beliefs” (i.e., the deep, long-standing, and rigid beliefs about oneself and the world that can be expressed in simple declarations like, “I’m unlovable”) (58). Patients then learn cognitive techniques that they can use to challenge and change these layers of cognition. Using cognitive restructuring to summon evidence against one’s automatic thoughts and generate alternative interpretations can help improve mood and reduce symptoms (59–62). Cognitive interventions provide patients with the skills to change their thoughts and beliefs (indicated by a circle and an arrow, respectively, in Figure 1).
Behavioral interventions challenge patients to directly change their behavior (indicated by a circle in Figure 1), giving them evidence that interrupts their beliefs (indicated by an arrow in Figure 1) and helps free them from the cycle of their symptoms. After patients develop an awareness of the behaviors they habitually use to avoid uncomfortable emotions, they then engage in “behavioral experiments,” “exposure exercises,” or “behavioral activation plans” in which they purposefully confront situations that they fear and avoid. These can be a wide variety of activities, including giving a speech in front of strangers, sending e-mails with typos in them, holding doorknobs that might have germs on them, planning positive events, or any other exercises that help them approach situations or sensations that they fear or avoid. A substantial body of research shows that behavioral exposures can drastically reduce a patient’s fear and avoidance of these situations, thereby improving their functioning (63–70). Theoretically, the patient begins to build new associations with these situations that foster the belief that they can cope (71). Of key importance is that patients learn to resist avoidant (or “safety”) behaviors during exposures (e.g., taking lorazepam before every exposure or washing their hands immediately after the exposure), as this inhibits the patient’s learning that they can cope with feared situations or emotions without avoidance (72). Some exposure exercises can be extremely distressing, meaning that providing a clear rationale for this approach and collaboratively working up to more difficult exposures are essential for the sustainability of this powerful and empirically proven intervention.
Meta-analyses show that treatments under the CBT umbrella improve symptoms and are often considered the gold-standard treatment for a wide range of psychiatric presentations (73, 74). This list includes internalizing disorders, such as major depressive disorder (66, 75), social anxiety disorder (76), panic disorder (67, 77), and PTSD (78, 79); externalizing disorders, such as drug and alcohol use (80), attention-deficit hyperactivity disorder (81), and oppositional defiant disorder (82); personality disorders, including borderline personality disorder (83, 84) and personality disorders comorbid with other disorders such as PTSD (85) or major depressive disorder (86); suicidal thoughts and behaviors (87); bipolar disorder (88); and psychosis (89, 90). The time has come to consider how CBT could be adapted for NPD and self-esteem dysregulation more broadly.
A CBT Formulation of Narcissistic Self-Esteem Dysregulation
Generating a CBT approach to NPD requires identifying the key beliefs that generate dysregulation, the habitual avoidant behaviors that reinforce those beliefs, and a potential set of cognitive and behavioral interventions that could interrupt these habits and transform maladaptive beliefs to healthier versions. We outline these three steps in the present section, drawing on the principles and literature outlined in the previous sections. A conceptual model of healthy and unhealthy self-esteem dysregulation is illustrated in Figure 2. Healthy individuals, overall, have relatively positive and stable self-esteem, which is consistently connected to reality (Figure 2A). This means that one holds reasonable expectations of oneself and how one should be treated. Healthy self-esteem is still sensitive to environmental feedback, falling when there are threats to one’s self-esteem and rising when one’s abilities and standing are affirmed. Self-esteem threats involve challenges to one’s competence, influence, attractiveness, social regard, or overall “goodness” (e.g., when rejected, when receiving negative feedback, or when performing worse than others). Scholars agree that experiences in which one suffers decreased self-esteem generate negative emotions including shame, embarrassment, envy, anxiety, and anger (13, 20, 91). These threats and concomitant emotions then activate efforts to “restore” self-esteem that both alleviate negative emotions aroused by the self-esteem threat and (when operating optimally) help the person grow their skills, social regard, and potential to contribute to society. In other words, self-esteem regulation is “the spice of life,” as it is a healthy and powerful promoter of both intrapersonal and interpersonal functioning (12). Being able to maintain this healthy self-esteem regulation circuit requires maintaining reasonable expectations for oneself and choosing constructive means for restoring self-esteem. This healthy regulation thus flows from a set of core beliefs such as “like others, I have natural strengths and weaknesses,” “I can get better at things through hard work,” and “I have inherent value.”
FIGURE 2.

Cognitive-behavioral (CBT) model of healthy and unhealthy narcissistic self-esteem, with examples indicated in gray texta
aBoth (A) and (B) show self-esteem levels fluctuating across time, with higher points on the Y axis reflecting more positive self-regard. The dark horizontal line in each panel represents feeling “neutral” about oneself, and values below this line represent feeling negatively about oneself. The gray shaded region represents self-esteem that is connected to reality (i.e., reasonable expectations of one’s own competence, influence, and social regard). (A) Healthy self-esteem and its regulation. Healthy self-esteem is typically stable and positive. However, even healthy self-esteem is responsive to negative feedback, depicted by the downward-pointing arrow (e.g., failing an examination). These “self-esteem threats” naturally trigger decreases in self-esteem and negative affect. In healthy individuals, one’s self-esteem system then launches responses that work to restore self-esteem (e.g., studying hard and passing the next examination). Underlying this person’s self-esteem is a core belief such as “I have natural strengths and weaknesses.” (B) Unhealthy self-esteem and its regulation. Here, self-esteem is frequently oscillating from unrealistically high to unrealistically low levels (e.g., “No one is as good as me” to “I’m worthless”). This unrealistically high evaluation of oneself renders self-esteem highly fragile, and daily interactions with reality threaten self-esteem (e.g., not being sufficiently praised for one’s work). This triggers a flip in self-esteem to unrealistically low levels that require excessively strong reactions to “restore” (e.g., insulting someone else’s intelligence to regain a sense of superiority). This fluctuation reflects the operation of a core belief such as, “If I’m not the best, I’m worthless.” These systems of self-esteem (dys)regulation can be understood within the CBT model depicted in Figure 1.
However, this system can easily become dysregulated, leading to narcissistic symptoms (and, in extremes, NPD). This dysregulation can take many forms, but the key point of fragility lies at the interface of unrealistic expectations of oneself and destructive means for restoring self-esteem (for examples, see Figure 2B and Table 1). If a person believes that they are not valuable unless they attain extraordinarily high standards (e.g., “if I’m not the best, I’m worthless” or “I deserve praise for all that I do”), then even quotidian experiences will threaten one’s self-esteem. Insufficient acknowledgment, minor mishaps, or exposure to more accomplished others will all trigger cognitions and emotions reflecting an extreme dip in self-esteem in which one feels incompetent and valueless. Indeed, narcissism is associated with elevated negative affect in response to others’ dominance (92). This distress can then trigger excessive behavioral reactions aimed at downregulating emotions, restoring self-esteem to unrealistically high standards (19), for example, by bringing others “down a peg,” behaving pompously, or giving up. In our model, these behavioral reactions can vary across individuals, but all aim to restore self-esteem (see Table 1 for examples). In fact, it is possible that the documented differences in “vulnerable” and “grandiose” subtypes of NPD (93, 94) could be explained by different behavioral strategies that patients use to restore their self-esteem. For instance, a “vulnerable” narcissistic profile would emerge from responses that restore esteem by removing oneself from potential sources of ego threat (e.g., not engaging during class, not responding to friends, or seeking suicide). A “grandiose” presentation would emerge from behaviors that instead elevate one’s comparative standing over others (e.g., flaunting one’s successes, putting others down, or defying rules).
TABLE 1.
Understanding psychological disorders through cognitive-behavioral therapy components
| Diagnosis | Situation | Belief | Automatic thoughts | Feelings | Behaviors | Consequences |
|---|---|---|---|---|---|---|
| Obsessive-compulsive disorder | Touching a doorknob | Contamination can kill me | “This doorknob probably has germs on it.” “I must wash to be safe.” | Disgust, anxiety, body tension | Resisting touching anything else with hands, wash immediately | Immediate reduction in distress but reinforces belief that one must wash to be safe |
| Vulnerable narcissism | Receiving negative feedback from boss | No one sufficiently understands or appreciates me | “He should have been clearer about what he wanted.” “I bet a different boss would appreciate me more.” “I should just give up.” | Anxiety, anger, self-loathing | Avoiding boss, fantasizing about “ideal” boss, suicidal ideation motivated by “showing them what they lost” | Avoidance of critiques leads to social and occupational impairment and reinforces belief that criticism is intolerable |
| Grandiose narcissism | Learning that a peer got a better score on a test | I must be the best in all ways | “It doesn’t matter, I’m still better than them.” “They’ll pay for showing me up.” | Anger, envy | Ridiculing peer for caring about grade, lying that peer got grade by cheating, fantasizing of ways to get even | Aggression and lying severely damages relationships and reinforces the notion that one must (appear to) be the best at all costs |
Special consideration should be given to the function of suicidal thoughts and behaviors (STB) in narcissistic dysregulation, particularly fantasizing about suicide or acting on suicidal urges (30). As we have noted, narcissistic dysregulation can produce immense and frequent distress, which can generate a desire to downregulate and escape these painful feelings through death. Although such a desire to escape distress can motivate STB transdiagnostically (95, 96), suicidal ideation and urges can serve additional functions in NPD, as suicide can seem like a pathway to quit a life in which one’s self-concept is irrevocably tarnished with no way to meet one’s idealized expectations (97); gain ultimate control over one’s life by permanently ending it; restoring one’s standing relative to others by vengefully showing others that they were insufficient to help; or achieving a glorified version of one’s death (30). Although these perceived benefits of dying by suicide might temporarily restore one’s sense of agency or relative standing to others, they also obviously bring immense pain to oneself and one’s community. As such, STB should be targeted early in treatment and understood within the aforementioned functional model.
To summarize this model, we propose that self-esteem regulation is a natural psychological process in human beings. People experience threats to their self-esteem, which generates aversive emotions that are regulated through learned behaviors that seek to restore self-esteem. This regulatory cycle is governed by (and, in turn, reinforces) underlying core beliefs about oneself and the world. Healthy self-esteem emerges when people have reasonable beliefs about oneself and use constructive responses to restore self-esteem. Unhealthy self-esteem emerges when people have unrealistic beliefs about themselves and others, leading to frequent self-esteem threats and immense, destructive attempts to restore self-esteem.
Furthermore, this dysregulated cycle can be understood through the lens of the CBT model described in Figure 1. When someone with NPD is exposed to a situation that threatens their self-esteem, underlying beliefs become activated that produce distorted cognitions and intense emotions. Habitual behavioral responses can momentarily reduce negative emotions and restore self-esteem, but they only reinforce the maladaptive belief, recapitulating the cycle each time the individual’s self-esteem is threatened. Specific examples of this cycle are articulated in Table 1. Behaviors indicative of classic narcissistic traits (e.g., need for admiration, fantasies of infinite success, suicidality, haughtiness, grandiose self-importance, and envy) can be understood through CBT components. Because of unrealistic underlying beliefs, any situations that threaten one’s sense of value, competence, power, and control germinate automatic thoughts organized around restoring a perceived sense of superiority. These thoughts provoke strong emotions, motivating internal and external behavioral reactions (e.g., escaping, lying, or aggressing) that may, indeed, restore a perceived sense of safety, perfection, or superiority but at the cost of healthy interpersonal functioning. Furthermore, these reactions only reinforce the underlying belief that perceived superiority is worth attaining at all costs. Although we chart only a few examples of narcissistic thought-feeling-behavior cycles, we use them to illustrate what we believe is a general process underlying dysregulated self-esteem.
The key benefit of analyzing narcissistic self-esteem dysregulation through this lens is that it opens this psychological process to modification through CBT techniques. Many relevant therapeutic skills fall under the umbrella of CBT, but we outline key potential approaches in the following text and in Table 2. CBT typically begins with psychoeducation on the CBT model and how it connects to a patient’s current symptoms. As such, we argue that patients with NPD should be informed of the diagnosis and fully brought into the conversation regarding their clinical conceptualization (42). After reviewing the models illustrated in Figures 1 and 2, therapists can assign patients to use self-monitoring exercises to gain a greater awareness of what behaviors they might use to “restore” their self-esteem, which could be maladaptive in nature. Therapists and patients can then explore and identify the deeper assumptions and beliefs that underlie these ego sensitivities. The goal of this information-gathering stage is to build a working knowledge of how patients’ habitual cognitions and avoidant behaviors emerge from and reinforce their underlying beliefs. This serves as a foundation for learning cognitive and behavioral skills that can change these habitual responses and the beliefs that produce them.
TABLE 2.
Example applications of cognitive-behavioral therapy (CBT) techniques to narcissistic dysregulation
| CBT skill | Targeted component of CBT model | Example application | Desired learning |
|---|---|---|---|
| Cognitive restructuring | Thoughts | Challenging automatic thoughts that one is worthless if one does not perform perfectly (e.g., “I either have to quit or never mess up again” vs. “Evidence shows I’m helpful even though I made a mistake”) | Habitually challenging automatic thoughts; updating core belief to recognize one’s value even if flawed |
| Behavioral exposures | Behaviors | Setting up hangout with peer who is superior on some dimension and paying them a compliment | Learning to tolerate inferiority; updating core belief that it is okay to be mediocre |
| Eliminating daily avoidance | Behaviors | Resisting daily behaviors that destructively “restore” self-esteem (e.g., excessive praise seeking, fantasizing, putting others down) | Learning healthier tools for regulating self-esteem; updating core belief that one can accept one’s unique strengths and weaknesses |
Cognitive skills for narcissistic dysregulation would help patients habitually challenge automatic thoughts that generate distress and only reinforce underlying maladaptive beliefs. Automatic cognitions are likely to suffer from classic “cognitive distortions” through which thoughts and interpretations neglect parts of reality (58). For example, cognitions might habitually deny the positive aspects of situations (e.g., thinking “I’m a failure” when patients receive both praise and critical feedback) or taking responsibility for an outcome even when all things are multiply determined (e.g., thinking “no one else is doing anything to make this project succeed” when collaborating on a project). Patients can then learn strategies for being more skeptical about these automatic thoughts and perhaps restructure them. For example, patients can learn to attend to the evidence that they still have value even when they are imperfect or that group projects benefit from shared effort and control. In these ways, habitual restructuring can help soothe negative affect in the face of self-esteem threats and regulate the patient’s behavioral attempts to restore self-esteem.
There are also several behavioral skills that could help stabilize narcissistic dysregulation. These interventions would focus on helping patients approach distressing situations, cognitions, and emotions that they typically avoid in order to learn that they can tolerate these experiences without the need for their habitual destructive reactions. This facilitates a corrective experience in which patients learn new beliefs that the situations that they typically avoid are actually tolerable. When treating narcissistic dysregulation, the goal of behavioral exposures would be to help patients approach situations that threaten self-esteem (which they typically avoid) and choose healthier behaviors to restore self-esteem rather than their typical strategies. Gaining mastery through more effective coping generates more durable self-esteem. For instance, someone with the belief that they must always be seen as the most intelligent person could practice allowing their coworker to take the lead on a project and resist urges to correct them or withdraw from the project. As is well known in exposure-based interventions, this practice can increase distress and requires clear rationale setting and collaboration to help the patient approach and learn from these exposures. One strategy would be to first identify and remove habitual avoidant behaviors in patients’ daily lives (even if they are not related to self-esteem), providing the patient with practice in habituating to strong emotions and engendering confidence in behavioral skills. The ultimate goal is for patients to develop increased willingness to approach situations they typically avoid and healthier skills for managing the emotions that are generated by them, thereby changing their underlying belief network and alleviating their overall symptoms (98).
Discussion
We outline a CBT approach to narcissistic self-esteem dysregulation that most mental health professionals can easily adapt into their practice. Narcissistic traits can be understood as a set of habitual thoughts, feelings, and behaviors that emerge because of maladaptive beliefs about oneself that essentially set unrealistic expectations for oneself and how one should be treated. When unmet, such expectations lead to rapid and extreme oscillations in self-esteem that generate strong negative emotions and require excessive and destructive reactions to restore self-esteem. However, this cycle can be regulated through cognitive and behavioral interventions that help patients modify their automatic thoughts and approach feared situations and emotions. These exercises can bring beliefs into a healthy connection with reality, relieving patients of their symptoms.
Although several treatments have been developed to aid people affected by narcissistic dysregulation (37–43), cognitive-behavioral perspectives are scarce (although not nonexistent) (99). We believe that the current formulation provides several advances beyond prior work. In particular, our model unites the perspective that self-esteem dysregulation is at the heart of NPD (12–15) with classic components of CBT theory (58). In particular, we articulate how rapid self-esteem oscillations typical of narcissistic fragility can be understood through self-perpetuating cycles of cognitive-affective-behavioral dysregulation that emerge from and reinforce maladaptive belief systems. This formulation opens the psychological processes that underlie NPD to modification through classic CBT techniques and to scientific study. Both of these advances are key for the study and treatment of NPD. Further refining a CBT formulation of NPD will allow both scientific and clinical efforts to make greater headway in understanding and treating NPD. This is especially promising, given the power that CBT has in effectively treating many other forms of psychopathology (73, 74).
Another key strength of the current model is its potential for understanding “narcissism” as a dimensional (rather than categorical) and transdiagnostic phenomenon. Scholars have questioned categorical taxonomies of psychopathology and instead advocated for identifying the dimensions that might vary continuously in a population and be shared across several disorders (32–34, 100, 101). Our model is consistent with this approach, as self-esteem (dys)regulation is a phenomenon that can vary continuously across people and emerge in several forms of psychopathology beyond NPD. In our model, everyone experiences self-esteem threats and has ways to restore self-esteem, and this system merely becomes dysregulated in NPD. We encourage additional attention to the processes that dysregulate the self-esteem system, as we believe this can help clarify what leads to NPD. We also encourage exploration of self-esteem and its dysregulation in other clinical disorders (e.g., borderline personality disorder, depression, perfectionism, obsessive-compulsive disorder, and social anxiety disorder).
It is crucial to keep in mind several limitations of our model as it stands. First and foremost, it remains largely theoretical (emerging from a synthesis of prior research and clinical observation) and, as such, has little direct empirical validation. Research is needed to establish key assumptions of the model (e.g., Do people with NPD endorse maladaptive beliefs concerning self-esteem? Do symptoms of NPD function to regulate distress and restore self-esteem?) and to test the potential use of CBT interventions to treat NPD. A second major limitation is that core beliefs are well known to be highly resistant to modification (102). This means that the CBT formulation articulated here might require incorporating additional tools and techniques, such as those of schema therapy, which has been shown to be effective in the treatment of personality disorders (103). This might be especially important in the treatment of NPD, as people who are highly ashamed of feeling inferior or incompetent are likely to use destructive reactions to restore self-esteem in the context of treatment (19, 99, 104). Borrowing techniques from dialectical behavior therapy could establish additional tools that help patients and therapists work together to address narcissistic reactions during treatment (54). A third limitation concerns the possibility that self-esteem dysregulation may only be one component of NPD, and full treatment of this disorder could require additional interventions. Other important future directions include more closely connecting the model proposed here to classic studies of self-esteem and its development (4, 5, 13, 14, 20, 105–108), investigating the utility of CBT-adjacent techniques such as motivational interviewing and mindfulness-based techniques in treating narcissistic dysregulation (109, 110), and charting how self-esteem dysregulation develops within an individual across the lifespan (106, 111–113).
In all, a cognitive-behavioral formulation of narcissistic self-esteem dysregulation could help patients diagnosed as having NPD change underlying beliefs and come to greater intrapersonal and interpersonal functioning. This model may be general enough to address transdiagnostic issues with self-esteem dysregulation, but additional clinical and empirical research are needed.
Footnotes
Dr. Nook serves on the scientific advisory board of Walden, Inc. Dr. Choi-Kain receives book royalties from Springer Publishing and the American Psychiatric Association. The other authors report no financial relationships with commercial interests.
References
- 1. Blascovich J , Tomaka J : Measures of self-esteem ; in Measures of Personality and Social Psychological Attitudes . San Diego: , Academic Press; , 1991. , pp 115 – 160 [Google Scholar]
- 2. Harter S : The Construction of the Self: A Developmental Perspective . New York: , Guilford Press; , 1999. [Google Scholar]
- 3. Rogers TB : A model of the self as an aspect of the human information processing system ; in Personality, Cognition and Social Interaction . Edited by Canton N , Kihlstrom JF . Hillsdale, NJ: , Erlbaum; , 1981. , pp 193 – 214 [Google Scholar]
- 4. Baumeister RF (ed): Self-Esteem . Boston: , Springer US; , 1993. [Google Scholar]
- 5. Mann M , Hosman CMH , Schaalma HP , et al. : Self-esteem in a broad-spectrum approach for mental health promotion . Health Educ Res 2004. ; 19 : 357 – 372 [DOI] [PubMed] [Google Scholar]
- 6. Sowislo JF , Orth U : Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies . Psychol Bull 2013. ; 139 : 213 – 240 [DOI] [PubMed] [Google Scholar]
- 7. Bolognini M , Plancherel B , Bettschart W , et al. : Self-esteem and mental health in early adolescence: development and gender differences . J Adolesc 1996. ; 19 : 233 – 245 [DOI] [PubMed] [Google Scholar]
- 8. Diagnostic and Statistical Manual of Mental Disorders , 5th ed . Washington, DC: , American Psychiatric Association; , 2013. [Google Scholar]
- 9. Kaufman SB , Weiss B , Miller JD , et al. : Clinical correlates of vulnerable and grandiose narcissism: a personality perspective . J Pers Disord 2020. ; 34 : 107 – 130 [DOI] [PubMed] [Google Scholar]
- 10. Stinson FS , Dawson DA , Goldstein RB , et al. : Prevalence, correlates, disability, and comorbidity of DSM-IV narcissistic personality disorder: results from the wave 2 national epidemiologic survey on alcohol and related conditions . J Clin Psychiatry 2008. ; 69 : 1033 – 1045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Trull TJ , Jahng S , Tomko RL , et al. : Revised NESARC personality disorder diagnoses: gender, prevalence, and comorbidity with substance dependence disorders . J Pers Disord 2010. ; 24 : 412 – 426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ronningstam E , Weinberg I : Narcissistic personality disorder: progress in recognition and treatment . Focus 2013. ; 11 : 167 – 177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Brummelman E , Thomaes S , Sedikides C : Separating narcissism from self-esteem . Curr Dir Psychol Sci 2016. ; 25 : 8 – 13 [Google Scholar]
- 14. Bosson JK , Lakey CE , Campbell WK , et al. : Untangling the links between narcissism and self-esteem: a theoretical and empirical review . Soc Pers Psychol Compass 2008. ; 2 : 1415 – 1439 [Google Scholar]
- 15. Kernis MH : Toward a conceptualization of optimal self-esteem . Psychol Inq 2003. ; 14 : 1 – 26 [Google Scholar]
- 16. Bushman BJ , Baumeister RF : Threatened egotism, narcissism, self-esteem, and direct and displaced aggression: does self-love or self-hate lead to violence? J Pers Soc Psychol 1998. ; 75 : 219 – 229 [DOI] [PubMed] [Google Scholar]
- 17. Morf CC , Rhodewalt F : Unraveling the paradoxes of narcissism: a dynamic self-regulatory processing model . Psychol Inq 2001. ; 12 : 177 – 196 [Google Scholar]
- 18. Grubbs JB , Exline JJ : Trait entitlement: a cognitive-personality source of vulnerability to psychological distress . Psychol Bull 2016. ; 142 : 1204 – 1226 [DOI] [PubMed] [Google Scholar]
- 19. Ronningstam E : Intersect between self-esteem and emotion regulation in narcissistic personality disorder—implications for alliance building and treatment . Borderline Personal Disord Emot Dysregul 2017. ; 4 : 3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Baumeister RF , Bushman BJ , Campbell WK : Self-esteem, narcissism, and aggression: does violence result from low self-esteem or from threatened egotism? Curr Dir Psychol Sci 2000. ; 9 : 26 – 29 [Google Scholar]
- 21. Twenge JM , Campbell WK : “Isn’t it fun to get the respect that we’re going to deserve?” Narcissism, social rejection, and aggression . Pers Soc Psychol Bull 2003. ; 29 : 261 – 272 [DOI] [PubMed] [Google Scholar]
- 22. Raskin R , Novacek J : Narcissism and the use of fantasy . J Clin Psychol 1991. ; 47 : 490 – 499 [DOI] [PubMed] [Google Scholar]
- 23. Campbell WK , Reeder GD , Sedikides C , et al. : Narcissism and comparative self-enhancement strategies . J Res Pers 2000. ; 34 : 329 – 347 [Google Scholar]
- 24. Johnson F : Psychological alienation: isolation and self-estrangement . Psychoanal Rev 1975. ; 62 : 369 – 405 [PubMed] [Google Scholar]
- 25. Atlas GD , Them MA : Narcissism and sensitivity to criticism: a preliminary investigation . Curr Psychol 2008. ; 27 : 62 – 76 [Google Scholar]
- 26. Ronningstam E : Narcissistic personality disorder: a current review . Curr Psychiatry Rep 2010. ; 12 : 68 – 75 [DOI] [PubMed] [Google Scholar]
- 27. Kris AO : Helping patients by analyzing self-criticism . J Am Psychoanal Assoc 1990. ; 38 : 605 – 636 [DOI] [PubMed] [Google Scholar]
- 28. Marčinko D , Jakšić N , Ivezić E , et al. : Pathological narcissism and depressive symptoms in psychiatric outpatients: mediating role of dysfunctional attitudes . J Clin Psychol 2014. ; 70 : 341 – 352 [DOI] [PubMed] [Google Scholar]
- 29. Ronningstam E , Weinberg I , Maltsberger JT : Eleven deaths of Mr. K.: contributing factors to suicide in narcissistic personalities . Psychiatry 2008. ; 71 : 169 – 182 [DOI] [PubMed] [Google Scholar]
- 30. Ronningstam E , Weinberg I , Goldblatt M , et al. : Suicide and self-regulation in narcissistic personality disorder . Psychodyn Psychiatry 2018. ; 46 : 491 – 510 [Google Scholar]
- 31. Reich A : Pathologic forms of self-esteem regulation . Psychoanal Study Child 1960. ; 15 : 215 – 232 [DOI] [PubMed] [Google Scholar]
- 32. ICD-11 Clinical Descriptions and Diagnostic Guidelines for Mental and Behavioural Disorders . Geneva: , World Health Organization; , 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Reed GM : Progress in developing a classification of personality disorders for ICD-11 . World Psychiatry 2018. ; 17 : 227 – 229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Bach B , Brown TA , Mulder RT , et al. : Development and initial evaluation of the ICD-11 Personality Disorder Severity scale: PDS-ICD-11 . Personal Ment Health 2021. ; 15 : 223 – 236 [DOI] [PubMed] [Google Scholar]
- 35. Edershile EA , Wright AGC : Narcissism dynamics . Soc Pers Psychol Compass 2022. ; 16 : 1 – 14 [Google Scholar]
- 36. Kohut H : Thoughts on narcissism and narcissistic rage . Psychoanal Study Child 1972. ; 27 : 360 – 400 [Google Scholar]
- 37. Ronningstam E : Introduction to the special issue on narcissistic personality disorder . J Pers Disord 2020. ; 34 : 1 – 5 [DOI] [PubMed] [Google Scholar]
- 38. Crisp H , Gabbard GO : Principles of psychodynamic treatment for patients with narcissistic personality disorder . J Pers Disord 2020. ; 34 : 143 – 158 [DOI] [PubMed] [Google Scholar]
- 39. Kernberg OF : Factors in the psychoanalytic treatment of narcissistic personalities . J Am Psychoanal Assoc 1970. ; 18 : 51 – 85 [DOI] [PubMed] [Google Scholar]
- 40. Diamond D , Hersh RG : Transference-focused psychotherapy for narcissistic personality disorder: an object relations approach . J Pers Disord 2020. ; 34 : 159 – 176 [DOI] [PubMed] [Google Scholar]
- 41. Drozek RP , Unruh BT : Mentalization-based treatment for pathological narcissism . J Pers Disord 2020. ; 34 : 177 – 203 [DOI] [PubMed] [Google Scholar]
- 42. Weinberg I , Finch EF , Choi-Kain LW : Implementation of good psychiatric management for narcissistic personality disorder: good enough or not good enough? in Applications of Good Psychiatric Management for Borderline Personality Disorder: A Practical Guide . Washington, DC: , American Psychiatric Publishing; , 2019. , pp 253 – 280 [Google Scholar]
- 43. Reed-Knight B , Fischer S : Treatment of narcissistic personality disorder symptoms in a dialectical behavior therapy framework: a discussion and case example ; in The Handbook of Narcissism and Narcissistic Personality Disorder: Theoretical Approaches, Empirical Findings, and Treatments . Edited by Campbell WK , Miller JD . Hoboken, NJ: , John Wiley & Sons; , 2011. , pp 466 – 475 [Google Scholar]
- 44. Choi-Kain L : Commentary on the special issue: narcissistic personality disorder: a coming of age . J Pers Disord 2020. ; 34 : 210 – 213 [DOI] [PubMed] [Google Scholar]
- 45. Kernberg OF : The almost untreatable narcissistic patient . J Am Psychoanal Assoc 2007. ; 55 : 503 – 539 [DOI] [PubMed] [Google Scholar]
- 46. Beck JS : Cognitive Behavior Therapy: Basics and Beyond , 2nd ed . New York: , Guilford Press; , 2011. [Google Scholar]
- 47. Hofmann SG , Asmundson GJG , Beck AT : The science of cognitive therapy . Behav Ther 2013. ; 44 : 199 – 212 [DOI] [PubMed] [Google Scholar]
- 48. Hayes SC , Hofmann SG , Ciarrochi J : A process-based approach to psychological diagnosis and treatment: the conceptual and treatment utility of an extended evolutionary meta model . Clin Psychol Rev 2020. ; 82 : 101908 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Barlow DH , Farchione TJ , Fairholme CP , et al. : The Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Therapist Guide . New York: , Oxford University Press; , 2011. [Google Scholar]
- 50. Martell CR , Addis ME , Jacobson NS : Depression in Context: Strategies for Guided Action . New York: , W. W. Norton & Co; , 2001. [Google Scholar]
- 51. Dimidjian S , Martell CR , Herman-Dunn R , et al. : Behavioral activation for depression ; in Clinical Handbook of Psychological Disorders: A Step-By-Step Treatment Manual . Edited by Barlow DH . The Guilford Press; , 2014. , pp 353 – 359 [Google Scholar]
- 52. Resick PA , Monson CM , Chard KM : Cognitive Processing Therapy for PTSD: A Comprehensive Manual . New York: , Guilford Publications; , 2016. [Google Scholar]
- 53. Foa EB , Hembree E , Rothbaum B : Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences Therapist Guide . New York: , Oxford University Press; , 2007. [Google Scholar]
- 54. Linehan MM : Skills Training Manual for Treating Borderline Personality Disorder . New York: , Guilford Press; , 1993. [Google Scholar]
- 55. Ward AM , Regan J , Chorpita BF , et al. : Tracking evidence based practice with youth: validity of the MATCH and standard manual consultation records . J Clin Child Adolesc Psychol 2013. ; 42 : 44 – 55 [DOI] [PubMed] [Google Scholar]
- 56. Gross JJ , Jazaieri H : Emotion, emotion regulation, and psychopathology: an affective science perspective . Clin Psychol Sci 2014. ; 2 : 387 – 401 [Google Scholar]
- 57. Barlow DH , Harris BA , Eustis EH , et al. : The unified protocol for transdiagnostic treatment of emotional disorders . World Psychiatry 2020. ; 19 : 245 – 246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Beck JS : Cognitive Therapy: Basics and Beyond . New York: , Guilford Press; , 1995. [Google Scholar]
- 59. Gross JJ : The emerging field of emotion regulation: an integrative review . Rev Gen Psychol 1998. ; 2 : 271 – 299 [Google Scholar]
- 60. Ochsner KN , Bunge SA , Gross JJ , et al. : Rethinking feelings: an FMRI study of the cognitive regulation of emotion . J Cogn Neurosci 2002. ; 14 : 1215 – 1229 [DOI] [PubMed] [Google Scholar]
- 61. Nook EC , Schleider JL , Somerville LH : A linguistic signature of psychological distancing in emotion regulation . J Exp Psychol Gen 2017. ; 146 : 337 – 346 [DOI] [PubMed] [Google Scholar]
- 62. Shurick AA , Hamilton JR , Harris LT , et al. : Durable effects of cognitive restructuring on conditioned fear . Emotion 2012. ; 12 : 1393 – 1397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Öst LG , Havnen A , Hansen B , et al. : Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993–2014 . Clin Psychol Rev 2015. ; 40 : 156 – 169 [DOI] [PubMed] [Google Scholar]
- 64. Foa EB : Prolonged exposure therapy: past, present, and future . Depress Anxiety 2011. ; 28 : 1043 – 1047 [DOI] [PubMed] [Google Scholar]
- 65. Chesham RK , Malouff JM , Schutte NS : Meta-analysis of the efficacy of virtual reality exposure therapy for social anxiety . Behav Chang 2018. ; 35 : 152 – 166 [Google Scholar]
- 66. Cuijpers P , van Straten A , Warmerdam L : Behavioral activation treatments of depression: a meta-analysis . Clin Psychol Rev 2007. ; 27 : 318 – 326 [DOI] [PubMed] [Google Scholar]
- 67. Pompoli A , Furukawa TA , Efthimiou O , et al. : Dismantling cognitive-behaviour therapy for panic disorder: a systematic review and component network meta-analysis . Psychol Med 2018. ; 48 : 1945 – 1953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Reid JE , Laws KR , Drummond L , et al. : Cognitive behavioural therapy with exposure and response prevention in the treatment of obsessive-compulsive disorder: a systematic review and meta-analysis of randomised controlled trials . Compr Psychiatry 2021. ; 106 : 152223 [DOI] [PubMed] [Google Scholar]
- 69. Parker ZJ , Waller G , Duhne PGS , et al. : The role of exposure in treatment of anxiety disorders: a meta-analysis . Int J Psychol Ther 2018. ; 18 : 111 – 141 [Google Scholar]
- 70. Powers MB , Halpern JM , Ferenschak MP , et al. : A meta-analytic review of prolonged exposure for posttraumatic stress disorder . Clin Psychol Rev 2010. ; 30 : 635 – 641 [DOI] [PubMed] [Google Scholar]
- 71. Craske MG , Treanor M , Conway CC , et al. : Maximizing exposure therapy: an inhibitory learning approach . Behav Res Ther 2014. ; 58 : 10 – 23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Craske MG , Kircanski K , Zelikowsky M , et al. : Optimizing inhibitory learning during exposure therapy . Behav Res Ther 2008. ; 46 : 5 – 27 [DOI] [PubMed] [Google Scholar]
- 73. Hofmann SG , Asnaani A , Vonk IJJ , et al. : The efficacy of cognitive behavioral therapy: a review of meta-analyses . Cognit Ther Res 2012. ; 36 : 427 – 440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Butler AC , Chapman JE , Forman EM , et al. : The empirical status of cognitive-behavioral therapy: a review of meta-analyses . Clin Psychol Rev 2006. ; 26 : 17 – 31 [DOI] [PubMed] [Google Scholar]
- 75. Hofmann SG , Curtiss J , Carpenter JK , et al. : Effect of treatments for depression on quality of life: a meta-analysis . Cogn Behav Ther 2017. ; 46 : 265 – 286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Mayo-Wilson E , Dias S , Mavranezouli I , et al. : Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis . Lancet Psychiatry 2014. ; 1 : 368 – 376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Sánchez-Meca J , Rosa-Alcázar AI , Marín-Martínez F , et al. : Psychological treatment of panic disorder with or without agoraphobia: a meta-analysis . Clin Psychol Rev 2010. ; 30 : 37 – 50 [DOI] [PubMed] [Google Scholar]
- 78. Cusack K , Jonas DE , Forneris CA , et al. : Psychological treatments for adults with posttraumatic stress disorder: a systematic review and meta-analysis . Clin Psychol Rev 2016. ; 43 : 128 – 141 [DOI] [PubMed] [Google Scholar]
- 79. Watts BV , Schnurr PP , Mayo L , et al. : Meta-analysis of the efficacy of treatments for posttraumatic stress disorder . J Clin Psychiatry 2013. ; 74 : 541 – 550 [DOI] [PubMed] [Google Scholar]
- 80. Magill M , Ray L , Kiluk B , et al. : A meta-analysis of cognitive-behavioral therapy for alcohol or other drug use disorders: treatment efficacy by contrast condition . J Consult Clin Psychol 2019. ; 87 : 1093 – 1105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Young Z , Moghaddam N , Tickle A : The efficacy of cognitive behavioral therapy for adults with ADHD: a systematic review and meta-analysis of randomized controlled trials . J Atten Disord 2020. ; 24 : 875 – 888 [DOI] [PubMed] [Google Scholar]
- 82. Battagliese G , Caccetta M , Luppino OI , et al. : Cognitive-behavioral therapy for externalizing disorders: a meta-analysis of treatment effectiveness . Behav Res Ther 2015. ; 75 : 60 – 71 [DOI] [PubMed] [Google Scholar]
- 83. Linehan MM , Comtois KA , Murray AM , et al. : Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder . Arch Gen Psychiatry 2006. ; 63 : 757 – 766 [DOI] [PubMed] [Google Scholar]
- 84. Kliem S , Kröger C , Kosfelder J : Dialectical behavior therapy for borderline personality disorder: a meta-analysis using mixed-effects modeling . J Consult Clin Psychol 2010. ; 78 : 936 – 951 [DOI] [PubMed] [Google Scholar]
- 85. Slotema CW , Wilhelmus B , Arends LR , et al. : Psychotherapy for posttraumatic stress disorder in patients with borderline personality disorder: a systematic review and meta-analysis of its efficacy and safety . Eur J Psychotraumatol 2020. ; 11 : 1796188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Banyard H , Behn AJ , Delgadillo J : Personality disorders and their relation to treatment outcomes in cognitive behavioural therapy for depression: a systematic review and meta-analysis . Cognit Ther Res 2021. ; 45 : 561 – 576 [Google Scholar]
- 87. Fox KR , Huang X , Guzmán EM , et al. : Interventions for suicide and self-injury: a meta-analysis of randomized controlled trials across nearly 50 years of research . Psychol Bull 2020. ; 146 : 1117 – 1145 [DOI] [PubMed] [Google Scholar]
- 88. Chiang KJ , Tsai JC , Liu D , et al. : Efficacy of cognitive-behavioral therapy in patients with bipolar disorder: a meta-analysis of randomized controlled trials . PLoS One 2017. ; 12 : e0176849 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Van Der Gaag M , Smit F , Bechdolf A , et al. : Preventing a first episode of psychosis: meta-analysis of randomized controlled prevention trials of 12 month and longer-term follow-ups . Schizophr Res 2013. ; 149 : 56 – 62 [DOI] [PubMed] [Google Scholar]
- 90. Jauhar S , McKenna PJ , Radua J , et al. : Cognitive-behavioural therapy for the symptoms of schizophrenia: systematic review and meta-analysis with examination of potential bias . Br J Psychiatry 2014. ; 204 : 20 – 29 [DOI] [PubMed] [Google Scholar]
- 91. Leary MR , Tambor ES , Terdal SK , et al. : Self-esteem as an interpersonal monitor: the sociometer hypothesis . J Pers Soc Psychol 1995. ; 68 : 518 – 530 [Google Scholar]
- 92. Wright AGC , Stepp SD , Scott LN , et al. : The effect of pathological narcissism on interpersonal and affective processes in social interactions . J Abnorm Psychol 2017. ; 126 : 898 – 910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Cain NM , Pincus AL , Ansell EB : Narcissism at the crossroads: phenotypic description of pathological narcissism across clinical theory, social/personality psychology, and psychiatric diagnosis . Clin Psychol Rev 2008. ; 28 : 638 – 656 [DOI] [PubMed] [Google Scholar]
- 94. Pincus AL , Lukowitsky MR : Pathological narcissism and narcissistic personality disorder . Annu Rev Clin Psychol 2010. ; 6 : 421 – 446 [DOI] [PubMed] [Google Scholar]
- 95. Bryan CJ , Rudd MD , Wertenberger E : Reasons for suicide attempts in a clinical sample of active duty soldiers . J Affect Disord 2013. ; 144 : 148 – 152 [DOI] [PubMed] [Google Scholar]
- 96. O’Brien KHM , Nicolopoulos A , Almeida J , et al. : Why adolescents attempt suicide: a qualitative study of the transition from ideation to action . Arch Suicide Res 2021. ; 25 : 269 – 286 [DOI] [PubMed] [Google Scholar]
- 97. Baumeister RF : Suicide as escape from self . Psychol Rev 1990. ; 97 : 90 – 113 [DOI] [PubMed] [Google Scholar]
- 98. Reid AM , Garner LE , Van Kirk N , et al. : How willing are you? Willingness as a predictor of change during treatment of adults with obsessive–compulsive disorder . Depress Anxiety 2017. ; 34 : 1057 – 1064 [DOI] [PubMed] [Google Scholar]
- 99. Freeman A , Fox S : Cognitive behavioral perspectives on the theory and treatment of the narcissistic character ; in Understanding and Treating Pathological Narcissism . American Psychological Association; , 2013. , pp 301 – 320 [Google Scholar]
- 100. Kotov R , Krueger RF , Watson D , et al. : The hierarchical taxonomy of psychopathology (HiTOP): a dimensional alternative to traditional nosologies . J Abnorm Psychol 2017. ; 126 : 454 – 477 [DOI] [PubMed] [Google Scholar]
- 101. Cuthbert BN , Insel TR : Toward the future of psychiatric diagnosis: the seven pillars of RDoC . BMC Med 2013. ; 11 : 126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Kellogg SH , Young JE : Schema therapy for borderline personality disorder . J Clin Psychol 2006. ; 62 : 445 – 458 [DOI] [PubMed] [Google Scholar]
- 103. Arntz A , Jacob GA , Lee CW , et al. : Effectiveness of predominantly group schema therapy and combined individual and group schema therapy for borderline personality disorder: a randomized clinical trial . JAMA Psychiatry 2022. ; 79 : 287 – 299 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Caligor E , Levy KN , Yeomans FE : Narcissistic personality disorder: diagnostic and clinical challenges . Am J Psychiatry 2015. ; 172 : 415 – 422 [DOI] [PubMed] [Google Scholar]
- 105. Pyszczynski T , Greenberg J , Solomon S , et al. : Why do people need self-esteem? A theoretical and empirical review . Psychol Bull 2004. ; 130 : 435 – 468 [DOI] [PubMed] [Google Scholar]
- 106. Rodman AM , Powers KE , Somerville LH : Development of self-protective biases in response to social evaluative feedback . Proc Natl Acad Sci U S A 2017. ; 114 : 13158 – 13163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107. Leary MR , Baumeister RF : The nature and function of self-esteem: sociometer theory . Adv Exp Soc Psychol 2000. ; 32 : 1 – 62 [Google Scholar]
- 108. Eisenberger NI , Inagaki TK , Muscatell Ka , et al. : The neural sociometer: brain mechanisms underlying state self-esteem . J Cogn Neurosci 2011. ; 23 : 3448 – 3455 [DOI] [PubMed] [Google Scholar]
- 109. Miller WR , Rollnick S : Motivational Interviewing: Helping People Change , 3rd ed . New York: , Guilford Press; , 2013. [Google Scholar]
- 110. Hayes SC , Luoma JB , Bond FW , et al. : Acceptance and commitment therapy: model, processes and outcomes . Behav Res Ther 2006. ; 44 : 1 – 25 [DOI] [PubMed] [Google Scholar]
- 111. Guindon MH : Self-Esteem Across the Lifespan: Issues and Interventions . New York: , Routledge; , 2015. [Google Scholar]
- 112. Orth U , Robins RW : Is high self-esteem beneficial? Revisiting a classic question . Am Psychol 2022. ; 77 : 5 – 17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Harris MA , Orth U : The link between self-esteem and social relationships: a meta-analysis of longitudinal studies . J Pers Soc Psychol 2020. ; 119 : 1459 – 1477 [DOI] [PubMed] [Google Scholar]