

Abstract
Purpose –
Law enforcement is a dangerous profession not only due to assaults, accidents and homicides but also due to health risks. This study examined trends in the national frequency and rate of law enforcement jobrelated illness deaths in the United States over a 22-year period (1997–2018).
Design/methodology/approach –
Data were obtained from the National Law Enforcement Officers Memorial Fund (NLEOMF) on death frequencies related to health issues at work. Death rates were based on the total number of police officers in the United States [rate = (frequency/population at risk) × 100,000]. Trends were examined using standardized regression.
Findings –
A total of 646 deaths were attributed to job-related illness. There was a significant upward trend in overall job-related illness deaths (frequency analyses: β = 0.88, p < 0.0001; rate analyses: β = 0.82, p ≤ 0.0001) mainly driven by a significant increase in 911 cancer deaths (frequency analyses: β = 0.88, p < 0.0001; rate analyses: β = 0.88, p ≤ 0.0001). Nearly 82 percent of circulatory deaths were from a heart attack, with an average death age of 46.5 years.
Research limitations/implications –
Deaths were not included if they failed to meet medical requirements of the NLEOMF. The data are descriptive, do not estimate risk and should be interpreted cautiously.
Practical implications –
Police wellness programs may help to reduce the danger of deaths associated with job-related illness.
Originality/value –
This is among the first studies to examine frequency and rate of police health–related deaths due to job exposures.
Keywords: Cancer, Danger, Heart attacks, Job related illness, Police deaths
Introduction
Police officers serve a vital role in maintaining safety and order in the United States and throughout the world. According to the Bureau of Justice Statistics, there are over 1.1 million full-time law enforcement employees in the United States, which include about 701,000 local police officers (Hyland, 2018). Law enforcement is a dangerous job. Within the last year (2018) alone the FBI Law Enforcement Officers Killed and Assaulted (FBI LEOKA, https://ucr.fbi.gov) data reported that 55 officers died as a result of felonious incident, 45 died from accidents, and 1,766 officers were non-fatally assaulted. Recent death statistics reported by the National Law Enforcement Officers Memorial Fund (NLEOMF, 2018) reported that 1,582 officers died in the line of duty during the past decade. Tiesman et al. (2018) examined national estimates of non-fatal work injuries among police from 2003 to 2014 and found an overall rate of injury of 635/100,000, three times higher than all other U.S. workers. NLEOMF reported that in 2016, of 135 officers fatally injured, 39 percent were killed in motor vehicle crashes (Tiesman et al., 2013). Lyons et al. (2017), in a review of police injury studies, found that the most common injuries were sprains and strains and occurred primarily during resistant offenders.
The definition of danger in police work has recently been viewed as inadequate despite statistics of officers victimized by homicide, assaults and traffic accidents. Richardson et al. (2019) called for a broader definition citing that danger such as mental and physical health significantly impact police officers in their duties. A comprehensive study by White et al. (2019) addressed the definition gap by examining officer line-of-duty deaths in the United States during a 50-year period. They found that from 1970 to 2016, the rate of felonious police deaths has decreased approximately 80 percent, while non-felonious deaths have decreased by almost 70 percent. White et al. (2019) argue that these results indicate that the policing profession is actually safer now than it was almost 50 years ago.
The “other” police danger
The White et al. (2019) and Richardson et al. (2019) studies suggest that danger in policing is not confined to violence against officers alone but has a broader concept. Given this, what are other possible elements of danger which may exist in policing? Certainly a broadened definition of dangerousness should include health effects on the officer, often brought about by undue levels of stress, job-related physical strain, and lifestyle impacted by police work (Richardson et al., 2019; Gibbs, 2019; Violanti, 2014).
Police officers are subject to a wide array of physical health risks, including obesity, poor diet, fatigue and sleep deprivation due to shift work, and poor general health. Additionally, mortality studies indicate that officers die at a significantly lower age than the U.S. general population (Violanti, 2014; Vena et al., 2014).
Studies corroborate a higher prevalence of cardiovascular disease among police compared with the general population (Zimmerman, 2012; Vena et al., 2014). In a mortality cohort of police officers from 1950 to 2005, white male officers exhibited significantly higher than expected mortality from all diseases of the circulatory system and arteriosclerotic heart disease (Vena et al., 2014). The metabolic syndrome, a collection of three or more out of five cardiovascular risk components, has also been noted among police officers with an estimated prevalence of 26.7 percent among urban police officers in the eastern United States (Hartley et al., 2012). Garbarino and Magnavita (2015) found that the most common components of metabolic syndrome in police constables were hypertriglyceridemia and low HDL cholesterol, and 22.7 percent police constables were hypertensive. Interestingly, the majority of fatal heart attacks in the present study occurred in the male 40–50 years of age group. Feuer and Rosenman (1986) and Vena et al. (2014) found an inverse relationship between heart disease and age, indicating that male police officers most susceptible to heart disease were affected at younger ages.
The potential for law enforcement exposure to hazardous materials in the United States is high. This is evidenced by several police mortality studies, which show an increased risk for cancers associated with chemical exposures (Vena et al., 2014; Feur and Rosenman, 1986; Pyörälä et al., 2000). Officers are often called upon to investigate traffic accidents involving hazardous materials, or handle disaster situations where chemicals are released in the air. More than 60,000 chemicals are produced annually in the United States, of which the U.S. Department of Transportation considers approximately 2000 hazardous (DOT, 2018). Chemical hazards encountered by police may be solids, liquids or gases that most commonly enter the body by inhalation, ingestion or absorption through the skin. According to data collected by the NLEOMF (2018), the majority of cancer deaths after 2001 were among officers involved with rescue and recovery during and after the 911 terrorist attack, suggesting possible exposure to potentially harmful chemicals, carcinogens or hazardous substances. This included World Trade Center, Pentagon and Shanksville, PA locations. The majority of these deaths from cancer were due to lung cancer and associated with lung diseases.
Another source of danger exists within the milieu of law enforcement: psychological stress and trauma. Exposure to human suffering and death may also result in a negative view of life, as well as psychological effects such as post-traumatic stress disorder (PTSD) (American Psychiatric Association, 2013), depression, and suicide ideation (McCanlies et al., 2014; Austin-Ketch et al., 2012; Violanti et al., 2009). Rotating shifts often lead to inadequate sleep for officers, which lowers physiological resistance to stress (Baughman et al., 2014; Bond et al., 2013). Family life may be disrupted by shift work schedules, working holidays and strained relationships (Kirschman et al., 2014). One can add to this array of occupational exposures the recent negative public image that police face, resulting in public loss of confidence in police integrity (President’s Task Force on 21st Century Policing, 2015).
Present study
In consideration of exploring a less studied type of police danger, that of work-related health risks, the present study examined of both the frequency and rate of death due to illnesses over a 22-year period (1997–2018). Deaths may have occurred either while on duty (e.g. heart attacks) or occurred later as a result of exposure to duty-related incidents (e.g. cancer due to latency periods).
Methods
Data source
Data were obtained from the NLEOMF database (2018) for the years 1997–2018. NLEOMF is a non-profit organization founded in 1984, which tracks and maintains a comprehensive database on law enforcement officers who died as a result of a duty-related death in the United States. Information collected by the NLEOMF includes, among other things, the age, gender, years of service, date of incident, date of death, cause of death (shooting, auto accident, job related illness, terrorism, etc.) and circumstances of death (health, accidental, felonious). The present study examined the NLEOMF database category labeled “job-related illness” (previously labeled “physical stress”), which recorded health-related deaths caused by a specific on-duty incident (e.g. heart attack, hazardous materials exposure, non-traffic and training incidents).
To be included in the NLEOMF database, the decedent must have been a duly sworn law enforcement officer with full arrest powers and employed by a law enforcement agency of the United States or its territories. The law enforcement officer must have died as a direct and proximate result of a personal injury or adverse event sustained while on duty. This also includes (1) law enforcement officers who, while in an off-duty capacity, act in response to a law violation, (2) law enforcement officers who, while in an off-duty capacity, are enroute to or from a specific emergency or responding to a particular request for assistance, (3) law enforcement officers who, as required or authorized by law or condition of employment, driving his or her employer’s vehicle to or from work, and (4) law enforcement officer who, as required by law or condition of employment driving his or her own personal vehicle at work and is killed while enroute to or from work. Circulatory related deaths such as heart attacks must have occurred within the 24-h period following a specific incident while on duty (NLEOMF, 2018).
Statistical analysis
Although death frequencies are recorded by NLEOMF, death rates that consider the entire U.S. law enforcement workforce are not available. Therefore, we examined both the national frequency and rate of job-related illness deaths over a 22-year period (1997–2018). Frequency of illness-related deaths included among other details the date and cause of death. The deaths for each year in the job-related illness category were summed to get a total annual count. The rate of illness-related deaths was obtained from data on the total number of police officers employed in the United States (and therefore at risk) for each year from January 1, 1997 to December 31, 2018 from the Occupational Employment Statistics (OES) survey conducted by the Bureau of Labor Statistics (BLS, 2018). The annual rate of death was then computed as follows: rate = (frequency NLEOMF data/population at risk – all police in the United States) × 100,000.
The yearly trend in deaths due to job-related illness was examined using two approaches. The first approach (i.e. frequency analyses) utilized the raw annual counts of deaths to examine the overall trend (an unadjusted analysis that did not consider the entire population of law enforcement in the United States). In the second approach (i.e. rate analyses), the annual counts of deaths were adjusted by the annual number of police officers in the United States to compute annual death rates per 100,000 officers (adjusted analyses). Linear regression was fitted to examine the overall trend over the 22-year period by computing the standardized regression coefficients and associated p-values. In addition to the overall job-related illness death, we conducted trend analyses separately for circulatory and cancer deaths.
Results
In terms of frequency, work-related illnesses were one of the leading causes of death among police officers in the United States. In total, there were 3,645 police deaths reported to NELOMF during the 22-year study period. Of those, 646 deaths were attributed to job-related illnesses; 94.7 percent of the deceased were men. Two-thirds (58.8 percent) of the deaths were described as being “accidental” (non-traffic) at work, while the remaining 41.2 percent occurred during a felony incident. Deceased officers ranged from age 21–74 years, with the majority (74.3 percent) being in the age group 40–60 years of age. Sixty-three percent (67.5 percent) of the deceased officers served at least 15 years on the job. The largest percentage of the deaths was from the northeast (36 percent) followed by South (30 percent), Midwest (16 percent) and West (9 percent), while 10 percent of the sample having missing information on region.
Table I provides the frequency of job-related illness deaths. Circulatory related disease (52.6 percent) and cancer (35.3 percent) were the most common causes of death. Among circulatory causes, 81.8 percent were due to a fatal heart attack, stroke (2.1 percent), cardiac arrest (2.1 percent) and probable circulatory causes (14.1 percent –e.g.– collapsed during training exercise, myocardial infarction, unresponsive after chest pains) (Table II). Approximately 21 percent of deaths occurred during training situations (n = 111, 20.7 percent), 85 of those resulting from cardiac incidents. The majority of cardiac-related deaths occurred at relatively younger ages (74.3 percent in the 40–60 years age group). The average age of death due to a heart attack was 46.5 years. The majority of circulatory deaths occurred during and after atypical physical exertion or emotional strain described as:
Table I.
Death from job-related illnesses among U.S. law enforcement officers, NLEOMF, 1997–2018
| Cause of job-related illness death | Frequency | Percent |
|---|---|---|
| Circulatory | 340 | 52.6 |
| Cancer | 228 | 35.3 |
| Other causes | ||
| Hepatitis C | 6 | 0.9 |
| Accidental drug overdose | 1 | 0.2 |
| Allergic reaction | 2 | 0.3 |
| Chemical injuries | 1 | 0.2 |
| Complication of sleep apnea | 1 | 0.2 |
| Complications after surgery | 5 | 0.8 |
| Complications from injury | 5 | 0.8 |
| Died 3 months after Hurricane Katrina rescue efforts | 1 | 0.2 |
| Died in sleep following a fall and high blood pressure | 1 | 0.2 |
| Fall | 1 | 0.2 |
| Gunshot wound | 1 | 0.2 |
| Hantavirus pulmonary syndrome | 1 | 0.2 |
| Hyperthermia | 7 | 1.1 |
| Hyponatremia (water intoxication) | 1 | 0.2 |
| Ill during training | 1 | 0.2 |
| Infection | 4 | 0.6 |
| Injuries | 15 | 2.3 |
| Injuries during arrest, followed by heart surgery | 1 | 0.2 |
| Kidney failure due to hyperthermia | 1 | 0.2 |
| Kidney failure due to septic shock | 1 | 0.2 |
| Multi-organ failure | 2 | 0.3 |
| Poisonous bite | 1 | 0.2 |
| Respiratory | 9 | 1.4 |
| Seizure | 1 | 0.2 |
| Smoke inhalation and/or toxic fumes | 6 | 0.9 |
| Unknown | 2 | 0.3 |
| Total | 646 | 100 |
Table II.
Prevalence of circulatory causes of death among U.S. law enforcement officers, NELOMF, 1997–2018
| Cause of death | Frequency | Percent |
|---|---|---|
| Heart attack | 278 | 81.8 |
| Cardiac arrest | 7 | 2.1 |
| Stroke | 7 | 2.1 |
| Probable circulatory related deaths | 48 | 14.1 |
| Total | 340 | 100.0 |
A physical struggle with a suspected or convicted criminal;
Performing a search and rescue mission that requires rigorous physical activity;
Performing or assisting with emergency medical treatment;
Responding to a violation of the law or emergency situation that involves a serious injury or death;
A situation that requires either a high speed response or pursuit on foot or in a vehicle;
Other health exposures (e.g. chemicals, hazardous materials), which might cause the death of the officer;
Training incidents.
Trends
Figure 1 illustrates trends in the frequency and national rate of overall police death due to work-related illness. During the 22-year period (1997–2018), there was a strong and significant increase (upward trend) in total job-related illness deaths in both frequency (β = 0.88, p-value < 0.0001) and rate (β = 0.82, p-value < 0.0001, Figure 1). In more recent years, there was a higher rate and frequency of job-related illnesses. Comparing data for 2000–2009 and 2010–2018, there was a 57 percent increase in average frequency and a 46 percent increase in average rate of deaths per year.
Figure 1.
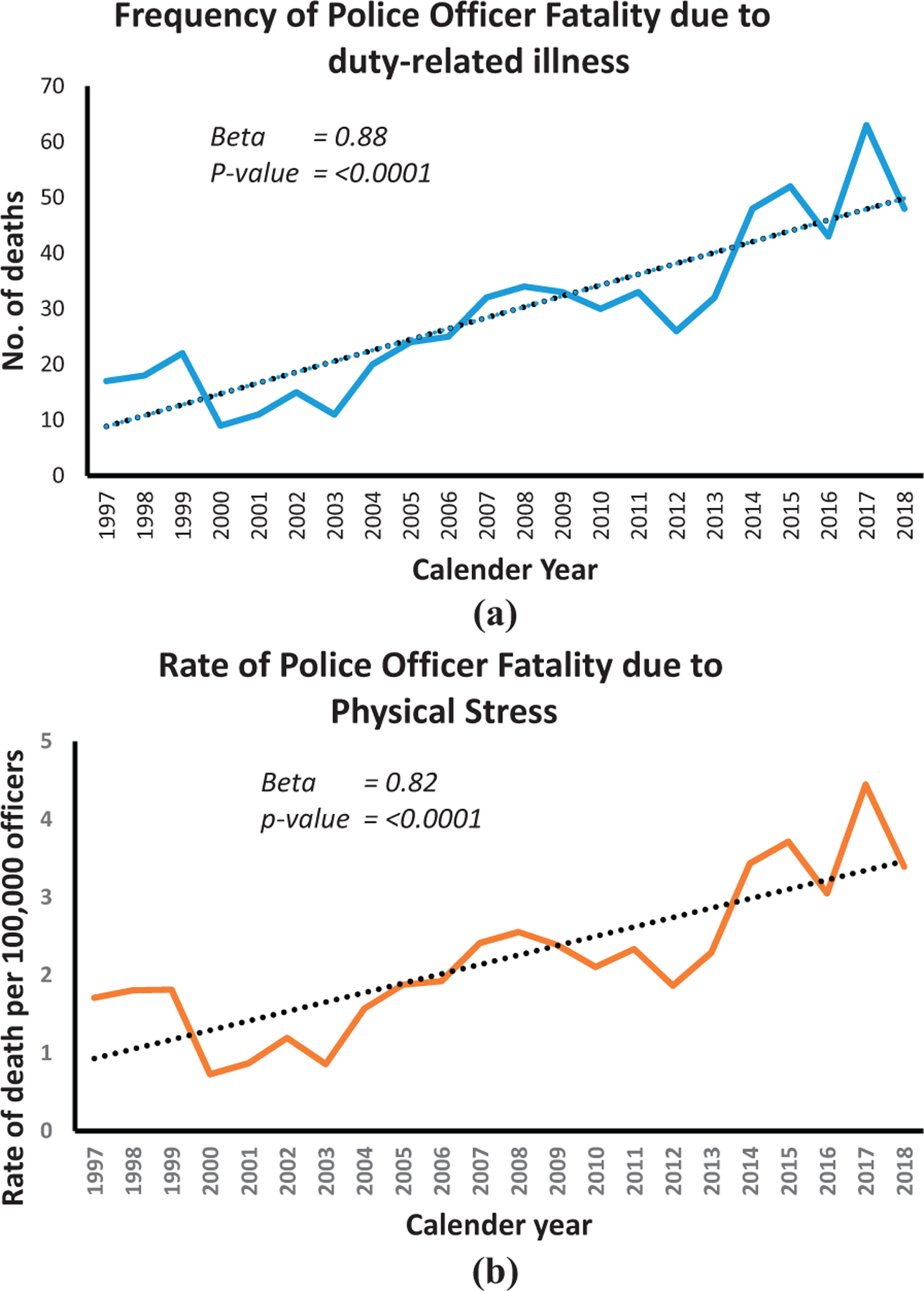
Annual trends in the frequency (a) and rate per 100,000 (b) of on-duty U.S. police deaths due to job-related illness (1997–2018)
Note(s): data on population at risk (police in the U.S. with arresting powers) were determined by accessing employment statistics from the Bureau of Labor Statistics website https://www.bls.gov/
Figure 2 shows trends in the frequency and rate of circulatory deaths. The frequency of circulatory deaths increased significantly (β = 0.44, p-value = 0.0386) but the national rate did not increase significantly (β = 0.13, p-value = 0.5569).
Figure 2.
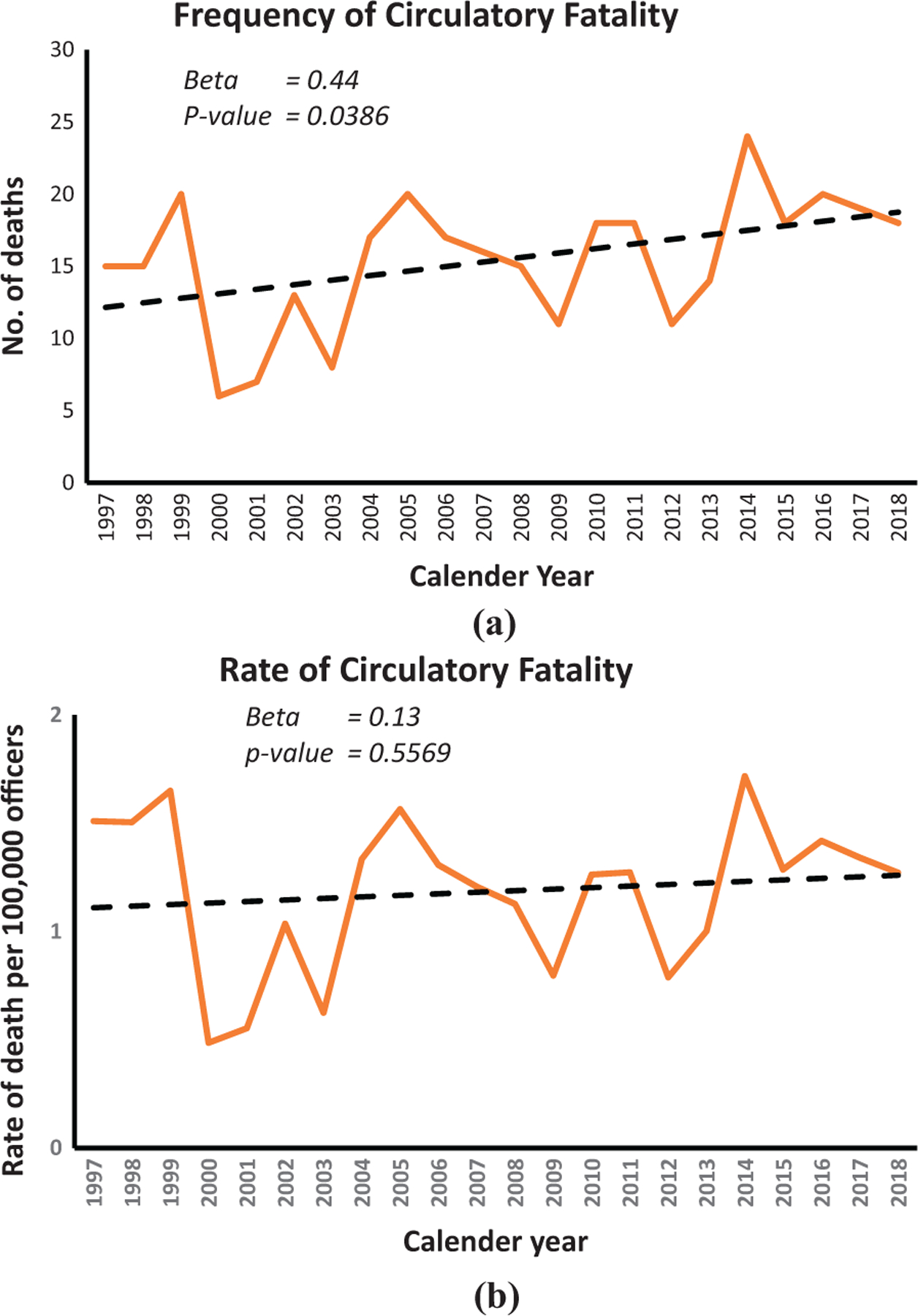
Annual trends in the frequency (a) and rate per 100,000 (b) of on-duty U.S. police deaths due to circulatory causes (1997–2018)
Note(s): data on population at risk (police in the U.S. with arresting powers) were determined by accessing employment statistics from the Bureau of Labor Statistics website https://www.bls.gov/
Figure 3 displays the frequency and rate of cancer deaths. Both the frequency and rate of cancer deaths increased significantly (β = 0.88, p-value ≤ 0.0001 and β = 0.88, p-value < 0.0001 respectively). The majority of cancer deaths occurred after September 2001, suggesting that exposure to 911 terrorist attack–related activity may have played a role. The total number and rate of all job-related illness deaths were essentially driven by the increase in cancer deaths, although circulatory deaths played a large part. Officers who died from cancer-related causes were significantly older (52.7 years of age) than those who died from either circulatory (46.3 years of age) or other causes (45.4 years of age).
Figure 3.
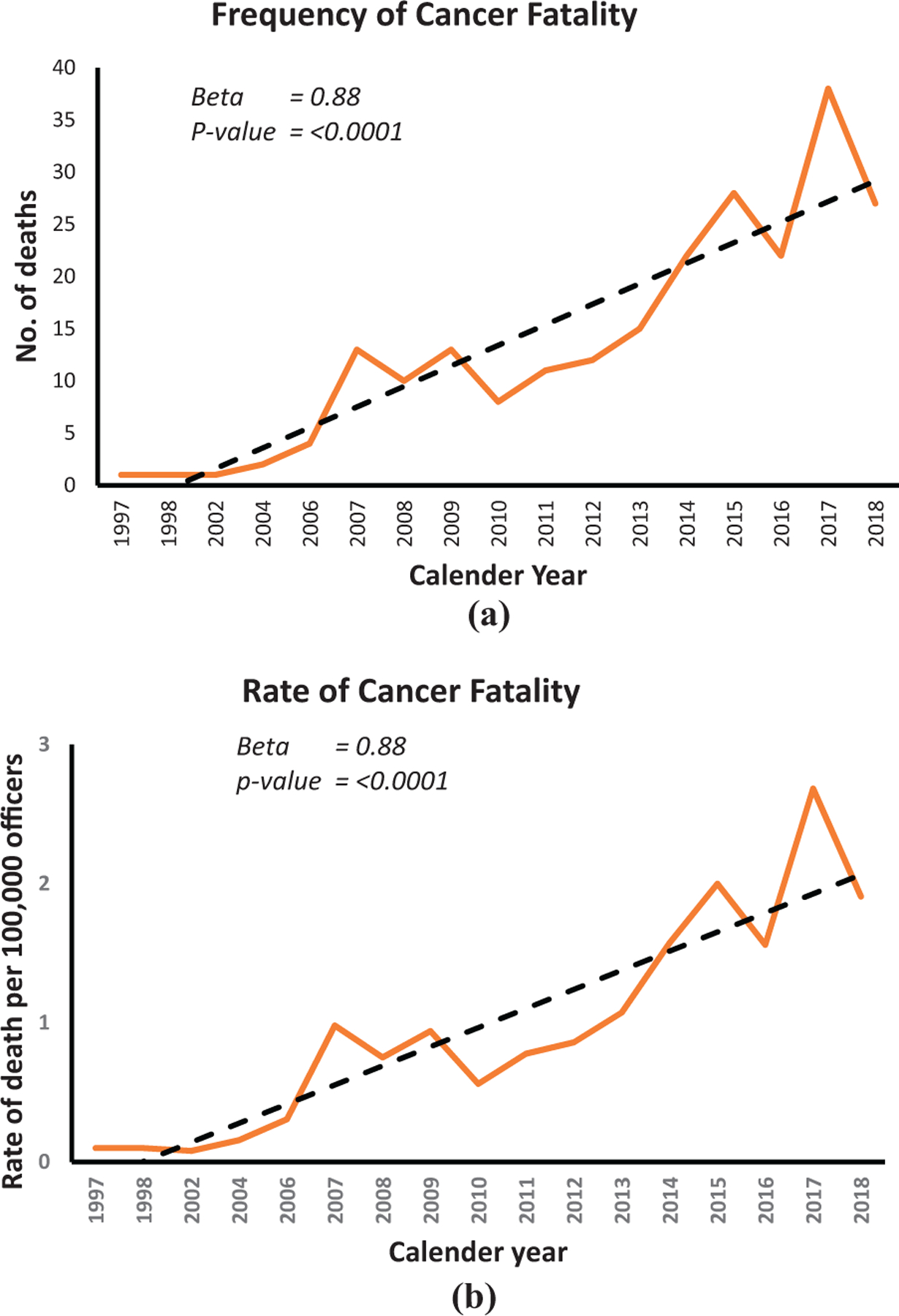
Annual trends in the frequency (a) and rate per 100,000 (b) of on-duty U.S. police deaths due to cancer causes (1997–2018)
Note(s): data on population at risk (police in the U.S. with arresting powers) were determined by accessing employment statistics from the Bureau of Labor Statistics website https://www.bls.gov/
Figure 4 displays the trend in frequency and rate of police death due to causes other than work-related illness. These deaths included auto accident and felony murder of officers. Similar to the White et al. (2019) study, police deaths from other causes including felonious murder and auto accidents decreased significantly in both frequency and rate over the 22-year period (β = −0.61, p-value = 0.0025 and β = −0.0.79 , p-value < 0.0001 respectively). Interestingly, this was in contrast to deaths from work-related health issues, which have increased over that same time period.
Figure 4.
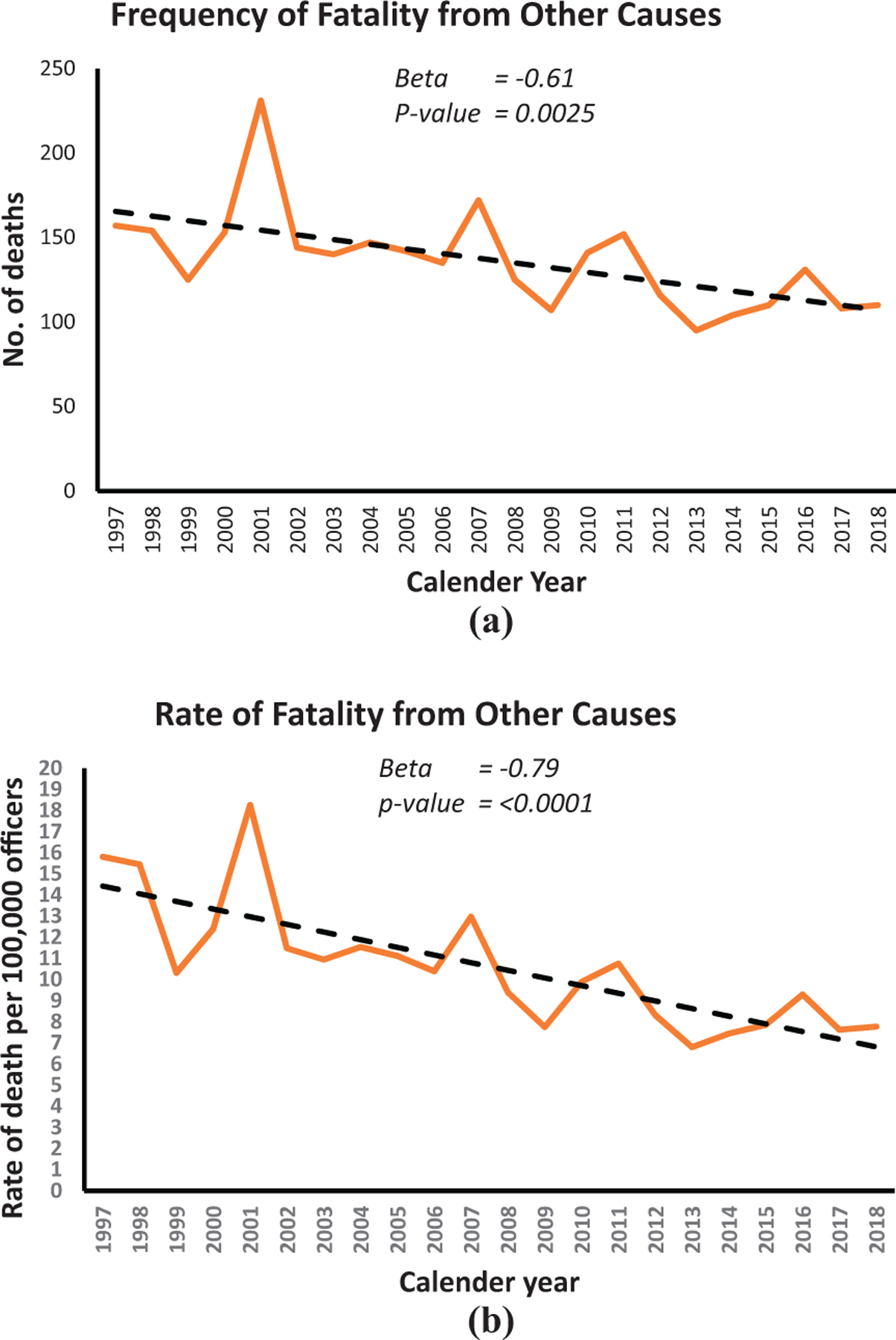
Annual trends in the frequency (a) and rate per 100,000 (b) of on-duty U.S. police deaths due to all other causes (1997–2018)
Note(s): data on population at risk (police in the U.S. with arresting powers) were determined by accessing employment statistics from the Bureau of Labor Statistics website https://www.bls.gov/
Discussion
The present study examined both the national frequency and rate of duty job-related illness deaths among police officers. Results indicated a strong and significant upward trend overall in duty-related illness police deaths during the 22-year period under investigation (1997–2018). Additionally, the rate of these deaths increased 46 percent since 2009. The finding that felonious murder and auto accidents have significantly decreased over the 22-year period, while work-related illnesses have significantly increased suggest that work-related health issues may be an additional danger and increasing problem.
Circulatory related deaths
Fifty-six percent (56.1 percent) of the deaths were related to circulatory events. Heart attacks were especially prevalent among male officers 40–60 years of age, with an average age of death of 46.5 years. The majority of cardiac events occurred after atypical physical exertion or emotional strain. Sixty-six percent of heart attacks and other causes of death occurred during events classified as “accidents” (non-felonious and non-traffic) at work. These included strenuous activity such as training exercises, lifting, falls and physical exercise. Accident prevention and safe practices education in the workplace may help to reduce such events. This is especially true during training regimens where strenuous physical activity was involved. Eighty-five heart attacks in the present study occurred during or shortly after a training session. This may necessitate further inquiry of officer health status prior to strenuous physical training exercises involving heavy exertion.
The high rate of duty-related cardiac events may be a result of the sedentary nature of police work, coupled with extreme physically challenging events without warning or warm-up time (Zimmerman, 2012; Gaines et al., 1993; Anderson et al., 2002). This sort of strenuous and unexpected activity places increased demands on the cardiovascular system, especially for persons in poor physical condition (Barnard et al., 1973; Mittleman et al., 1993a, b). Varvargou et al. (2014) found that sudden cardiac death among police officers was considerably higher when they were involved in activities other than routine non-emergency duties. Examples were the pursuit of suspects, physical altercations, restraints and maintaining order in disaster situations.
Officers who may be in poor physical condition or obese may be at higher risk for cardiac events when involved in activities involving physical exertion or strain (Ramey et al., 2009). The U.S. National Health Interview Survey data showed a higher prevalence of obesity (BMI ≥ 30 kg/m2) both in non-Hispanic white men and women working in the protective service occupations compared to the general working population (Gu et al., 2014). Wright et al. (1995) compared male police officers’ traditional cardiovascular risk factors with non-police male workers and found that police officers have a significantly higher BMI. In a statewide study on physical fitness in police officers, Violanti et al. (2016) found that officers who had higher levels of body fat were in poorer physical condition and did not perform as well on fitness tests as those with lower body fat. The prevalence of overall fitness was 4.3 times greater in male officers and 3.6 times greater in female officers in the lowest body fat percentage tertile compared with those in the highest tertile (30.3 vs 7.1 percent and 46.0 vs 12.8 percent, respectively).
Sudden and unexpected physical exertion is not the only possible precipitant of cardiac events among police. Police work has been noted as a highly stressful occupation (Webster, 2014; Shane, 2010; Elliott et al., 2016; Violanti et al., 2018), and stressful or traumatic incidents can trigger cardiovascular events. Lipovetzky et al. (2007) found that negative emotional experiences at work could trigger an acute coronary syndrome episode. This could have implications for recognizing a cardiac event as a work accident. Smyth et al. (2016) found that physical exertion or emotional upset are triggers associated with first acute myocardial infarction in men and women, and in all age groups, with no significant effect modifiers. Buckley et al. (2015) reported that episodes of intense anger and increased anxiety are associated with increased relative risk for acute coronary occlusion.
Cancer deaths
Present results indicate that 35.3 percent (n = 228) of job-related deaths were due to cancer and that cancer increased significantly in both frequency and rate. The NLEOMF data suggested that the majority of cancer deaths occurred after the 911 terrorist attacks on the World Trade Center in 2001. Officers exposed to the remnants of the attack were likely exposed to carcinogenic substances, which may have contributed to the development of cancer. Exposure to harmful and carcinogenic substances continues to be a danger to the health of police officers. Additional exposures to recent illicit drugs such as fentanyl and the various opioids also pose a health threat. Prevention involves education of officers in recognition and proper handling of hazardous substances. The National Institute of Occupational Safety and Health (NIOSH) Health Hazard Evaluation (HHE) program investigates hazardous conditions such as chemical exposure (https://www.cdc.gov/niosh/hhe/about.html). The program helps employers and employees recognize and control health hazards in their workplace. Additionally, the HHE program raises awareness of workplace health hazards and preventive measures based on their findings. Police departments experiencing personnel illnesses associated with chemical exposure may request a health hazard evaluation for assistance and prevention efforts.
Prevention: policy implications
A general statement from the American Heart Association Council on Nutrition, Physical Activity and Metabolism; the American Heart Association Council on Clinical Cardiology; and the American College of Sports Medicine suggests that “maintaining physical fitness through regular physical activity may help to reduce cardiac events because a disproportionate number of events occur in the least physically active subjects performing unaccustomed physical activity” and resonates with police populations (Thompson et al., 2007). Stressful encounters may also trigger negative physiological responses such as cardiac events. Implementation of stress-reduction programs in the workplace will help officers deal with these encounters.
Examples of successful police wellness programs
Many police organizations have begun to place an increased emphasis on physical fitness, healthy lifestyle behaviors and prevention efforts for hazardous materials exposure. The present finding that the majority of cardiac deaths occurred in younger age categories (40–50 years of age) exemplifies the need for emphasis on fitness throughout the police career. A recent legislative mandate has helped to move police wellness efforts forward. The Law Enforcement Mental Health and Wellness Act (LEMHWA) (2018) was recently passed in congress. The act called for the U.S. Department of Justice to prepare a report to congress containing recommendations on the needs of officers that concern mental and well as physical health (Spence et al. 2019).
A program initiated by the Seminole County, Florida Sheriff’s department has shown success in improving the health of officers called “Operation Thrive Wellness Challenge” (https://www.fbinaa.org/FBINAA/Staying_on_the_YBR.aspx). The program involves seven steps to initiate, develop, run and assess the program. Officers are surveyed to determine their wellness interests; command staff approves the program; and officers participate along with periodic health screenings. Points are earned for successfully practicing four key healthy habits (exercise, nutrition, sleep and stress management) and/or losing weight. LEO-specific wellness tips, strategies and support are emailed every week for eight weeks.
Through this annual wellness challenge, agencies can expect employees to achieve measurable success in the following areas:
Healthy weight loss
Reduced risk of heart disease from increased self-monitoring of blood pressure and increased exercise
Reduced risk of diabetes from improved nutrition
Improved alertness and reaction time from improved sleep
Improved health awareness from increased participation in biometric health screenings
Improved morale from the inherently fun teamwork.
(O’Malley and Nice (2016) accessed 9–19-19 https://www.fbinaa.org/FBINAA/Staying_on_the_YBR.aspx.)
Kuehl et al. (2016) developed and tested the SHIELD program specifically for police. The program consisted of 12, 30-min, team-based, scripted, peer-led sessions for six months. Team meetings were scheduled once per week and members would discuss weekly goals aloud regarding successful strategies to reach the weekly goal such as exercise, diet and sleep. Kuehl et al. (2016) base the success of the program on the team approach, which encouraged competition and peer pressure to succeed. Several years ago, the New York State Police initiated a program, which provided pay compensation for physical fitness. Trooper was tested each year in various endurance and strength activities and received extra pay according to their level of fitness. The program encouraged fitness levels and competition among the various stations, all leading to the improved levels of health. There are many other police wellness initiatives through the country to help reduce health problems among officers (Police Executive Research Forum, 2018).
There are limitations in the present study. The data are descriptive, do not estimate risk and should be interpreted cautiously. Some duty-related deaths were rejected for inclusion because they did not meet the medical requirements of the NLEOMF. Although there are no official death records included in this database; however, each death is reviewed by the Armed Forces Institute of Pathology or by other medical personnel with similar skill and expertise. A deceased officer is eligible for inclusion in the memorial database if it is determined that the officer died because of exposure while performing official duties or by exposure to hazardous materials or conditions. The NLEOMF database does not contain information on personal physical data of officers. It was therefore not possible to determine the health status of officers either before or after work-related incidents, which may have caused their deaths. Information such as obesity, smoking, diet, prior illnesses and other lifestyle factors were not available. Additionally, the NLEOMF database do not contain information on whether the various law enforcement departments promote healthier living for the police officers.
In conclusion, it is noteworthy that in accordance with NLEOMF and national data jobrelated illnesses are a clear and present danger among police officers in the United States. The present study suggests that overall the trend of police deaths for job-related illnesses has significantly increased in frequency and rate over the past 22 years. It also suggests that the frequency and rate of cancer deaths appear to play an important part in this increase. This does not take away from the finding that circulatory deaths, primarily heart attacks, are also prominent. It is also noteworthy that while auto accidents and felony murder rates appear to have significantly decreased during the study time period, overall deaths related to work-related illnesses have significantly increased. This is an indication of the danger element of health being a serious law enforcement issue. As Richardson et al. (2019) pointed out, health is just one more dimension of the danger that police must face. Poor physical health should not be a reason to die from work exposures, and in a sense, this danger is not confined to officers alone but may affect performance, duty and those whom they serve.
Acknowledgments
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for disease Control and Prevention. The authors would like to thank the National Law Enforcement Memorial Fund for supplying the data for this study.
Contributor Information
John M. Violanti, Department of Epidemiology and Environmental Health, State University of New York at Buffalo, Buffalo, New York, USA,
Desta Fekedulegn, Bioanalytics, Health Effects Laboratory Division, National Institute for Occupational Safety and Health, Morgantown, West Virginia, USA.
Mingming Shi, Bioanalytics, Health Effects Laboratory Division, National Institute for Occupational Safety and Health, Morgantown, West Virginia, USA.
Michael E. Andrew, Bioanalytics, Health Effects Laboratory Division, National Institute for Occupational Safety and Health, Morgantown, West Virginia, USA
References
- American Psychiatric Association (2013), Diagnostic and Statistical Manual of Mental Disorders, 5th ed., American Psychiatric Publishing, Washington, DC. [Google Scholar]
- Anderson GS, Litzenberger R and Plecas D (2002), “Physical evidence of police officer stress”, Policing, Vol. 25 No. 2, pp. 399–420. [Google Scholar]
- Austin-Ketch TL, Violanti JM, Fekedulegn D, Andrew ME, Burchfiel CM and Hartley TA (2012), “Addictions and the criminal justice system, what happens on the other side? Posttraumatic stress symptoms and cortisol measures in a police cohort”, Journal of Addictions Nursing, Vol. 23 No. 1, pp. 22–29, doi: 10.3109/10884602.2011.645255. [DOI] [PubMed] [Google Scholar]
- Barnard RJ, Gardner GW, Diaco NV, MacAlpin RN and Kattus AA (1973), “Cardiovascular responses to sudden strenuous exercise–heart rate, blood pressure, and ECG”, Journal of Applied Physiology, Vol. 34 No. 6, pp. 33–837. [DOI] [PubMed] [Google Scholar]
- Baughman P, Fekedulegn D, Charles LE, Gu JK, Ma C, Violanti JM, Wirth M, Mnatsakanova A, Hartley TA, Andrew ME and Burchfiel CM (2014), “Shift work and health consequences in policing”, in Violanti JM. (Ed.), Dying for the Job: Police Work Exposure and Health, Charles C. Thomas, Springfield, IL, pp. 73–92. [Google Scholar]
- Bond J, Hartley TA, Sarkisian K, Andrew ME, Charles LE, Andrew ME and Violanti JM (2013), “Association of traumatic police event exposure with sleep quality and quantity in the BCOPS study cohort”, International Journal of Emergency Mental Health, Vol. 15 No. 4, pp. 255–266. [PMC free article] [PubMed] [Google Scholar]
- Buckley T, Soo Hoo Soon Y, Fethney J, Shaw E, Hanson PS and Tofler GH (2015), “Triggering of acute coronary occlusion by episodes of anger”, European Heart Journal, Vol. 4 No. 6, pp. 493–498. [DOI] [PubMed] [Google Scholar]
- Bureau of Labor Statistics (BLS) (2018), available at: https://www.bls.gov/oes/tables.htm (accessed 17 June 2019).
- Department of Transportation (DOT) (2018), available at: https://www.fmcsa.dot.gov/regulations/hazardous-materials/how-comply-federal-hazardous-materials-regulations (accessed 17 June 2019).
- Elliott JL and Lal S (2016), “Blood pressure, sleep quality and fatigue in shift working police officers: effects of a twelve hour roster system on cardiovascular and sleep health”, International Journal of Environmental Research and Public Health, Vol. 13 No. 2, doi: 10.3390/ijerph13020182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feuer E and Rosenman K (1986), “Mortality in police and firefighters in New Jersey”, American Journal of Industrial Medicine, Vol. 9 No. 3, pp. 517–529. [DOI] [PubMed] [Google Scholar]
- Gaines LK, Falkenberg S and Gambino JA (1993), “Police physical agility testing: an historical and legal analysis”, American Journal of Police, Vol. 12 No. 12, pp. 47–66. [Google Scholar]
- Garbarino S and Magnavita N (2015), “Work stress and metabolic syndrome in police officers. A prospective study”, PloS One, Vol. 10 No. 12, article. e0144318, doi: 10.1371/journal.pone.0144318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbs JC (2019), “Rhetoric vs. reality of decreasing danger for police over time”, Criminology and Public Policy, Vol. 18, pp. 7–10, doi: 10.1111/1745-9133.12423. [DOI] [Google Scholar]
- Gu JK, Charles LE, Bang KM, Ma CC, Andrew ME, Violanti JM and Burchfiel CM (2014), “Prevalence of obesity by occupation among U.S. Workers: the national health Interview survey 2004–2011”, Journal of Occupational Medicine, Vol. 56 No. 5, pp. 516–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartley TA, Burchfiel CM, Fekedulegn D, Andrew ME, Knox SS and Violanti JM (2012), “Association between police officer stress and the metabolic syndrome in the BCOPS Study Cohort”, International Journal of Emergency Mental Health, Vol. 13 No. 4, pp. 243–256. [PMC free article] [PubMed] [Google Scholar]
- Hyland S (2018), “Full-time employees in law enforcement agencies, 1997–2016”, NCJ 251762 Bureau of Justice Statistics, U.S. Dept. of Justice, Washington, DC. [Google Scholar]
- Kirschman E, Kamena M and Fay J (2014), Working with Police Families, Guilford Press, New York, NY, pp. 169–175. [Google Scholar]
- Kuehl KS, Elliot DL, MacKinnon DP, O’Rourke HP, DeFrancesco C, Miocevic M and Valente M (2016), “The SHIELD (safety & health improvement: enhancing law enforcement departments) study: mixed methods longitudinal findings”, Journal of Occupational and Environmental Medicine, Vol. 58 No. 5, pp. 492–498, doi: 10.1097/JOM.0000000000000716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipovetzky N, Hod H, Roth A, Kishon Y, Sclarovsky S and Green MS (2007), “Emotional events and anger at the workplace as triggers for a first event of the acute coronary syndrome: a case-crossover study”, The Israel Medical Association Journal, Vol. 9 No. 4, pp. 310–315. [PubMed] [Google Scholar]
- Lyons K, Radburn C, Orr R and Poped R (2017), “A profile of injuries sustained by law enforcement officers: a critical review”, International Journal of Environmental Research and Public Health, Vol. 14 No. 142, pp. 1–21, doi: 10.3390/ijerph14020142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCanlies EC, Mnatsakanova A, Andrew ME, Burchfiel CM and Violanti JM (2014), “Positive psychological factors are associated with lower PTSD symptoms among police officers: post Hurricane Katrina”, Stress and Health, Vol. 30 No. 5, pp. 405–415, doi: 10.1002/smi.2615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Goldberg RJ and Muller JE (1993a), “Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of myocardial infarction onset study investigators”, New England Journal of Medicine, Vol. 329 No. 23, pp. 1677–1683. [DOI] [PubMed] [Google Scholar]
- Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Goldberg RJ and Muller JE (1993b), “Heavy physical exertion can trigger the onset of acute myocardial infarction, particularly in people who are habitually sedentary”, New England Journal of Medicine, Vol. 329 No. 23, pp. 1677–1683. [DOI] [PubMed] [Google Scholar]
- National Law Enforcement Officers Memorial Fund (NLEOMF) (2018), available at: www.nleomf.com/.
- O’Malley EJ and Nice M (2016), “Staying on the yellow brick road - winning wellness in law enforcement”, available at: https://www.fbinaa.org/FBINAA/Staying_on_the_YBR.aspx. [Google Scholar]
- Police Executive Research Forum (2018), Building and Sustaining an Officer Wellness Program: Lessons from the San Diego Police Department, Office of Community Oriented Policing Services, Washington, DC. [Google Scholar]
- President’s Task Force on 21st Century Policing (2015), Final Report of the President’ s Task Force on 21st Century Policing, Office of Community Oriented Policing Services, Washington, DC. [Google Scholar]
- Pyörälä M, Miettinen H, Halonen P, Laakso M and Pyörälä K (2000), “Insulin resistance syndrome predicts the risk of coronary heart disease and stroke in healthy middle-aged men: the 22-year follow-up results of the Helsinki Policemen Study”, Arteriosclerosis, Thrombosis, and Vascular Biology, Vol. 20 No. 2, pp. 538–544. [DOI] [PubMed] [Google Scholar]
- Ramey S, Downing N and Franke W (2009), “Milwaukee police department retirees: cardiovascular disease risk and morbidity among aging law enforcement officers”, AAOHN, Vol. 57 No. 11, pp. 448–453. [DOI] [PubMed] [Google Scholar]
- Richardson NJ, Barrick K and Strom KJ (2019), “Is policing safer today? The case for a more comprehensive definition of dangerousness”, Criminology and Public Policy, Vol. 18, pp. 37–45. [Google Scholar]
- Shane JM (2010), “Organizational stressors and police performance”, Journal of Criminal Justice, Vol. 38 No. 4, pp. 807–818, doi: 10.1016/j.jcrimjus.2010.05.008. [DOI] [Google Scholar]
- Smyth A, O’Donnell M, Lamelas P, Teo K, Rangaragan S, Yusuf S (2016), “Physical activity and anger or emotional upset as triggers of acute myocardial infarction”, Circulation, Vol. 134, pp. 1059–1067, doi: 10.1161/CIRCULATIONAHA.116.023142. [DOI] [PubMed] [Google Scholar]
- Spence DL, Melissa F, Gilbert CM, Sarah E and Nazmia EAC (2019), Law Enforcement Mental Health and Wellness Act: Report to Congress, U.S. Department of Justice, Washington, DC. [Google Scholar]
- Thompson PD, Franklin BA, Balady GJ, Blair SN, Corrado D, Estes NA III, Fulton JE, Gordon NF, Haskell WL, Link MS, Maron BJ, Mittleman MA, Pelliccia A, Wenger NK, Willich SN and Costa F (2007), “Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American heart association council on nutrition, physical activity, and metabolism and the council on clinical cardiology”, Circulation, Vol. 115 No. 17, pp. 2358–2368. [DOI] [PubMed] [Google Scholar]
- Tiesman HM, Swedler DI, Konda S and Pollack KM (2013), “Fatal occupational injuries among U.S. law enforcement officers: a comparison of national surveillance systems”, American Journal of Industrial Medicine, Vol. 56 No. 6, pp. 693–700. [DOI] [PubMed] [Google Scholar]
- Tiesman HM, Gwilliam M, Konda S, Rojek J and Marsch S (2018), “Nonfatal injuries to law enforcement officers: a rise in assaults”, American Journal of Industrial Medicine, Vol. 54 No. 4, pp. 503–509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varvarigou V, Farioli A, Korre M, Sato S, Dahabreh IJ and Kales SN (2014), “Law enforcement duties and sudden cardiac death among police officers in United States: case distribution study”, British Medical Journal (Clinical Research ed.), No. 349, g6534, doi: 10.1136/bmj.g6534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vena JE, Charles LE, Gu JK, Burchfiel CM, Andrew ME, Fekedulegn D and Violanti JM (2014), “Mortality of a police cohort: 1950–2005”, Journal of Law Enforcement Leadership and Ethics, Vol. 1 No. 1, pp. 7–30. [PMC free article] [PubMed] [Google Scholar]
- Violanti JM, Burchfiel CM, Fekedulegn D, Andrew ME, Dorn J, Hartley TA, Charles LE and Miller DB (2009), “Cortisol patterns and brachial artery reactivity in a high stress environment”, Psychiatry Research, Vol. 169 No. 2, pp. 75–81. [DOI] [PubMed] [Google Scholar]
- Violanti JM, Ma CC, Fekeduelgn D, Andrew ME, Gu JK, Hartley TA, Charles LE and Burchfiel CM (2016), “Association between body fat percentage and fitness among police officers: a statewide study”, Safety and Health at Work, Vol. 8 No. 1, pp. 36–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Violanti JM, Charles LE, McCanlies E, Hartley TA, Baughman P, Andrew ME, Fekedulegn D, Ma CC, Mnatsakanova A and Burchfiel CM (2018), “Police stressors and health: a state-ofthe-art review”, Policing: An International Journal of Police Strategies & Management, Vol. 40 No. 4, pp. 642–656, doi: 10.1108/PIJPSM-06-2016-0097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Violanti JM (2014), Dying for the Job: Police Work Exposure and Health, Charles C. Thomas, Springfield, IL, pp. 41–51. [Google Scholar]
- Webster JH (2014), “Perceived stress among police officers: an integrative model of stress and coping”, Policing: An International Journal of Police Strategies & Management, Vol. 37 No. 4, pp. 839–857, doi: 10.1108/PIJPSM-06-2014-0064. [DOI] [Google Scholar]
- White MD, Dario LM and Shjarback JA (2019), “Assessing dangerousness in policing an analysis of officer deaths in the United States, 1970–2016”, Criminology and Public Policy, Vol. 18, pp. 11–35, doi: 10.1111/1745-9133.12408. [DOI] [Google Scholar]
- Wright NM, Renault J, Willi S, Veldhuis JD, Pandey JP, Gordon L, Key LL and Bell NH (1995), “Greater secretion of growth hormone in black than in white men: possible factor in greater bone mineral density—a clinical research center study”, Journal of Clinical Endocrinology & Metabolism, Vol. 80 No. 8, pp. 2291–2297. [DOI] [PubMed] [Google Scholar]
- Zimmerman FH (2012), “Cardiovascular disease and risk factors in law enforcement personnel: a comprehensive review”, Cardiology in Review, Vol. 20 No. 4, pp. 159–166. [DOI] [PubMed] [Google Scholar]
Further reading
- Albert CM, Mittleman MA, Chae CU, Lee IM, Hennekens CH and Manson JE (2000), “Triggering of sudden death from cardiac causes by vigorous exertion”, New England Journal of Medicine, Vol. 343 No. 19, pp. 1355–1361. [DOI] [PubMed] [Google Scholar]
- Brandl SG (1996), “In the line of duty: a descriptive analysis of police assaults and accidents”, Journal of Criminal Justice, Vol. 24 No. 3, pp. 255–264. [Google Scholar]
- Breznitz S and Goldberger L (1993), “Stress research at a crossroads”, in Goldberger L. and Breznitz S. (Eds), The Handbook of Stress: Theoretical and Clinical Aspects, 2nd ed., The Free Press, New York, pp. 3–6. [Google Scholar]
- Dahabreh IJ and Paulus JK (2011), “Association of episodic physical and sexual activity with triggering of acute cardiac events: systematic review and meta-analysis”, Journal of the American Medical Association, Vol. 305 No. 12, pp. 1225–1233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dubrow R, Burnett CA, Gute DM and Brockert JE (1988), “Ischemic heart disease and acute myocardial infarction mortality among police officers”, Journal of Occupational Medicine, Vol. 30 No. 8, pp. 650–654. [DOI] [PubMed] [Google Scholar]
- Federal Bureau of Investigation (2019), “Law enforcement officers killed and assaulted (LEOKA)”, available at: https://ucr.fbi.gov.
- Federal Motor Carrier Safety Administration, Hazardous Materials Division 2018, “US Department of Transportation (DOT) considers approximately 2000 hazardous materials”. available at: https://www.fmcsa.dot.gov/regulations/hazardous-materials/how-comply-federal-hazardous-materials-regulations.
- Finkelstein MM (1998), “Cancer incidence among Ontario police officers”, American Journal of Industrial Medicine, Vol. 34 No. 2, pp. 157–162. [DOI] [PubMed] [Google Scholar]
- Mittleman MA, Maclure M, Sherwood JB, Mulry RP, Tofler GH, Jacobs SC, Friedman R, Benson H and Muller JE (1995), “Triggering of acute myocardial infarction onset by episodes of anger. Determinants of myocardial infarction onset study investigators”, Circulation, Vol. 92 No. 7, pp. 1720–1725. [DOI] [PubMed] [Google Scholar]
- National Institute of Occupational Safety and Health (2018) “Health Hazard Evaluation (HHE) program investigates hazardous conditions such as chemical exposure”, available at: https://www.cdc.gov/niosh/hhe/about.html.
- Sardinas A, Miller JW and Hansen H (1986), “Ischemic heart disease mortality of firemen and policemen”, American Journal of Public Health, Vol. 76 No. 9, pp. 1140–1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Labor Bureau of Labor Statistics (2012), “The editor’s desk, “how risky is police work”?”, available at: www.bls.gov/opub/ted/1999/jun/wk5/art05.htm.