

Abstract
Objective:
To describe the consumption of ultra-processed foods according to demographic and socioeconomic characteristics in three birth cohorts.
Design:
Cross-sectional analysis.
Setting:
Data from the 2004, 1993 and 1982 Pelotas Birth Cohorts were used at 11, 22 and 30 years, respectively, collected between 2012 and 2015. Outcome was the relative contribution of ultra-processed foods from the total daily energy intake. Maternal-independent variables were self-reported skin colour, schooling, age and family income (obtained in the perinatal study), and variables of the cohort member, sex, skin colour, schooling and current family income (the last two obtained at the 11-, 22- and 30-year follow-ups of the respective cohorts). We calculated crude and adjusted means of the outcome for the whole cohorts and according to the independent variables.
Participants:
11-, 22- and 30-year-old individuals.
Results:
Daily energetic contribution from ultra-processed foods was higher in the younger cohort (33·7, 29·8 and 25·1 % at 11, 22 and 30 years, respectively). Maternal schooling and family income at birth showed an inverse dose–response relationship at 11 and 22 years, but a positive dose–response at 30 years. Female sex, lower schooling and family income at 22 years and higher schooling at 30 years were associated to a higher contribution from ultra-processed foods in the daily energy intake.
Conclusions:
Information from food and nutrition policies needs a higher dissemination, mostly among women and population groups of lower income and schooling, including its promotion in media and health services, aiming for a decreased consumption of ultra-processed foods.
Keywords: Ultra-processed foods, Cohort studies, Adolescents, Adults
The last decades were marked by a rising prevalence in obesity in high-, low- and middle-income countries(1). Changes in food patterns were observed in the same period and represent one of the main factors related to obesity rising. Basic traditional foods, such as bean, milk, fruit and vegetables, that present low energy density and high nutrient density were replaced by ready-to-eat or ready-to-heat products, which, in general, present high processing level as well as high contents of sugar, salt and fat(2–4).
NOVA classification allocates food products into four groups according to the industrial processing degree: unprocessed or minimally processed foods, processed culinary ingredients, processed foods and ultra-processed foods(5,6). This last group includes ready-to-eat or ready-to-heat products, which are highly convenient as they require little or no cooking. Usually, the consumption of these foods tends to replace that of unprocessed or minimally processed foods, leading to a nutritionally unbalanced diet(5). Moreover, substances for industrial use only, such as dyes and flavours, added for the purpose of increasing durability make these foods highly palatable, helping to increase their consumption(5,6). Although the use of additives is legally authorised, the effects on health of its cumulative lifetime consumption and of the interaction among additives are still unknown(7).
The annual trend in the sales of ultra-processed foods has been increasing, reflecting the rise in the consumption of such foods(8,9). In Brazil, a national study among adolescents and adults showed that about 30 % of the total daily energy intake in 2008–2009 came from ultra-processed foods(10). In studies carried out in high-income countries, daily energies from ultra-processed foods ranged from 48·0 to 58·5 % from 2004 to 2014(11–13).
In cross-sectional studies, the consumption of these products seems to be higher in younger populations(10–12). However, studies about the factors related to ultra-processed food consumption in these age groups are scarce. Thus, we aimed to describe ultra-processed food consumption according to demographic and socioeconomic characteristics using data from the 2004, 1993 and 1982 Pelotas Birth Cohorts at 11, 22 and 30 years, respectively, collected between 2012 and 2015.
Methods
The 2004, 1993 and 1982 Pelotas Birth Cohorts have been following up all live-births throughout life from those years. For the three cohorts, the eligible newborns were children of mothers living in the urban area of Pelotas according to the territorial boundaries on 1 January 1982, as part of the city was emancipated in May 1982. Enrolment strategies were the same in the three cohorts, with the inclusion of births that occurred in all maternity hospitals in the city. In 2004, 1993 and 1982, a total of 4231, 5249 and 5914 mothers, respectively, accepted to participate and were interviewed shortly after delivery (refusal rate of <1 % in all three cohorts), and their children were subsequently followed up over the years. Methodological details of the three cohorts are described in other publications(14–16).
In relation to the original sample, the follow-up rates were 86·6 % in the 2004 cohort (11 years), 76·3 % in the 1993 cohort (22 years) and 68·1 % in the 1982 cohort (30 years). Both during hospital interviews (perinatal study) and follow-ups, trained interviewers applied standardised and pre-coded questionnaires, similar among the cohorts. The instruments contained questions on health-related issues. The data of follow-ups used in this article were collected in a clinic specifically set up for the cohorts(14–16).
Participants’ food consumption was evaluated through the application of semiquantitative FFQs, which investigate eating habits of the 12 months prior to the interview. Consumption frequency of each food item was measured from the following alternatives: never or <1x per month, 1–3x per month, 1x per week, 2–4x per week, 5–6x per week, 1x per day, 2–4x per day and ≥5x per day. The three cohorts’ FFQ contained eighty-eight items(17), and the average portion was based on domestic measures according to the Table for Assessment of Food Intake in Household Measures(18). The average portion was presented to the participant verbally and with the help of images, and the participant answered if its consumption was usually smaller, equal to or larger than the average portion. A few number of foods in the FFQ used in the 1982 cohort were different from those of the other two cohorts. The methods used for building the FFQ are described in another publication(17). Food items investigated in the FFQ are arranged in online supplementary material (Supplementary Table).
For statistical analyses, we converted consumption frequencies reported in each FFQ food item to annual consumption. Answer options represented a consumption of, respectively, 0, 12, 52, 104, 260, 365·25, 730·5 and 1826·25 times a year. To obtain daily consumption, we divided annual consumption by 365·25. Then, we calculated the quantity in grams for each food item, using the daily frequency of consumption and the average portion. To take into account portion sizes, we divided the gram values by two if the reported portion was less than the average, or we multiplied by 1·5 if it was larger than the average portion. Macronutrient content (carbohydrate, protein and fat) was defined for each food, based on the consumed value in grams and the Brazilian Food Composition Table (TACO)(19) or USDA Nutrient Database for Standard Reference(20), when not available in TACO. Energetic value in kJ for each item was obtained multiplying carbohydrates and proteins by 16·7 kJ and lipids by 37·7 kJ (corresponding to 4 and 9 kcal, respectively). Finally, the total daily energetic intake was calculated grouping kilocalories from carbohydrates, proteins and lipids from all food items. The FFQ items were distributed in the four groups proposed by the NOVA classification(5) (see online supplementary material, Supplementary Table) and then the proportion of energies from each food group was calculated, relative to the total energy intake.
Covariables included maternal characteristics evaluated in perinatal study: age (≤24, 25–34, ≥35 years), schooling (0–4, 5–8, 9–11, ≥12 completed years of study), self-reported skin colour (white or black for the 1982 Cohort, and white, brown/yellow/indigenous or black for other cohorts) and total monthly family income (quintiles). Variables of cohort members were sex (male or female) in the perinatal study, and skin colour (white, brown/yellow/indigenous or black), schooling (first–third, fourth–fifth or sixth–seventh scholar years for the 2004 Cohort; and 0–4, 5–8, 9–11 or ≥12 completed years of study for other cohorts) and current total monthly family income (quintiles) at 11-, 22- and 30-year follow-ups. Also, as potential confounders in the follow-ups, we included diet to lose weight in the last 12 months (yes or no) and energy intake/energy expenditure ratio(21).
Energy intake was total daily intake, and energy expenditure was calculated from the equations recommended by the Institute of Medicine (IOM)(22), taking into consideration participants’ sex, nutritional status and level of physical activity. Nutritional status was classified by BMI. At 11-year follow-up, cut-off points for low or normal weight and for overweight were, respectively, <+1 and ≥+1 z-score(23); and at 22- and 30-year follow-ups, respectively, <25 and ≥25 kg/m2(24). In all the three cohorts, the level of physical activity was determined using accelerometers (GENEActiv; ActivInsights; and Actigraph® GT3X) by the participants for about 6 d with a 24-h protocol, and the raw data were analysed with R-package GGIR(25). We used moderate to vigorous-intensity physical activity data (cut-off points of 100 mg, an acceleration threshold corresponding to walking; and 10 min bout)(25). Quartile cut-offs were set to classify participants as very low active, low active, active and very active, according to the levels defined by the IOM(22).
Data were collected and entered directly in Pendragon and REDCap (Research Electronic Data Capture)(26). The statistical package Stata (version 12.1) was used to run the analyses. We calculated the mean percentages of energy contribution from the food groups in each cohort, adjusted for perinatal and current characteristics, for the total sample and after stratification by sex. Thereafter, crude and adjusted average energy contribution from ultra-processed foods was described according to perinatal and current socioeconomic variables, presenting mean values and 95 % confidence intervals (CIs). Energy intake/energy expenditure ratio was included into the adjustment model that described the proportions of energy contribution from each processing group to reduce misclassification bias from under- or overreporting inherent in the use of FFQ(21), as well as information about diet to lose weight in the last 12 months. We ran adjusted analyses by linear regression accounting for demographic and socioeconomic variables. We constructed a hierarchical conceptual model(27) using backward selection procedure by levels and maintaining the variables that presented P-values <0·05 in the level in the adjusted model. First and second levels included perinatal variables (maternal skin colour and age, and maternal schooling and family income, respectively). The third level included participants’ sex and skin colour; and the fourth level, participants’ schooling and current family income (at follow-ups). Energy intake/energy expenditure ratio and diet to lose weight in the last 12 months were not included in the model since they are at a lower hierarchical level and, therefore, are not considered confounders for the association between socioeconomic variables and the outcome. We tested the associations using aggregated and non-aggregated data. In aggregated data, we included time (cohort) and individual as two levels to allow for variables that were not measured. However, we did not find differences between the two ways, then we analysed each cohort separately. Variables presenting P-values <0·05 were considered significantly associated to the outcome, and tests of linear trend were carried out for ordinal variables.
The Ethics Committee of the Faculty of Medicine of the Federal University of Pelotas approved the follow-ups of the 2004, 1993 and 1982 Cohorts (889 753; 1 250 366; and 16/12, respectively). Participants of the 1993 and 1982 Cohorts signed a consent term. In the 2004 Cohort, the mother or legal guardian signed the consent term; and the adolescent, the assent term.
Results
At 11, 22 and 30 years, respectively, 3514, 3648 and 3646 participants had information related to FFQ and were included in the current analysis. In the three cohorts, at the time of delivery, most of the mothers were ≤24 years, had 5–8 years of schooling and self-declared white skin colour (Table 1). Some differences were observed among those who provided food information at 11, 22 and 30 years and those lost in follow-up. At 11 and 30 years, losses were higher among the extreme categories of maternal schooling (0–4 and ≥12 years of study) and family income (first and fifth quintiles). At age 11, there were more losses among children of younger mothers (≤24 years); and at 22 and 30 years, among male participants (Table 1).
Table 1.
Sample description, number and proportion of followed-up* and lost† individuals at 11 years (2004 Cohort), 22 years (1993 Cohort) and 30 years (1982 Cohort), according to perinatal characteristics
| Variables | Original (n 4231) | Followed up at 11 years (n 3514) | Lost at 11 years (n 619) | Original (n 5249) | Followed up at 22 years (n 3648) | Lost at 22 years (n 1408) | Original (n 5914) | Followed up at 30 years (n 3646) | Lost at 30 years (n 1943) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| Maternal perinatal characteristics | ||||||||||||||||||
| Skin colour | ||||||||||||||||||
| White | 3088 | 73·0 | 2561 | 72·8 | 467 | 75·6 | 4058 | 77·3 | 2777 | 76·2 | 1149 | 81·6 | 4851 | 82·1 | 2992 | 82·1 | 1625 | 83·7 |
| Black | 846 | 20·0 | 712 | 20·3 | 105 | 17·0 | 955 | 18·2 | 698 | 19·1 | 211 | 15·0 | 1060 | 17·9 | 653 | 17·9 | 316 | 16·3 |
| Brown/yellow/indigenous | 295 | 7·0 | 241 | 6·9 | 46 | 7·4 | 234 | 4·5 | 171 | 4·7 | 48 | 3·4 | – | – | ||||
| Schooling (completed years) | ||||||||||||||||||
| 0–4 | 654 | 15·6 | 519 | 14·9 | 111 | 18·2 | 1468 | 28·0 | 975 | 26·8 | 414 | 29·5 | 1960 | 33·2 | 1172 | 32·2 | 644 | 33·2 |
| 5–8 | 1731 | 41·4 | 1447 | 41·6 | 243 | 39·7 | 2424 | 46·2 | 1721 | 47·2 | 620 | 44·1 | 2454 | 41·5 | 1569 | 43·1 | 748 | 38·6 |
| 9–11 | 1381 | 33·0 | 1183 | 34·0 | 173 | 28·3 | 923 | 17·6 | 659 | 18·1 | 245 | 17·4 | 654 | 11·1 | 400 | 11·0 | 226 | 11·6 |
| ≥12 | 420 | 10·0 | 332 | 9·5 | 84 | 13·8 | 427 | 8·2 | 288 | 7·9 | 127 | 9·0 | 839 | 14·2 | 500 | 13·7 | 323 | 16·6 |
| Monthly family income (quintiles) | ||||||||||||||||||
| 1° (lowest) | 872 | 20·6 | 684 | 19·5 | 159 | 25·7 | 1031 | 20·1 | 690 | 19·3 | 280 | 20·4 | 1183 | 20·0 | 652 | 17·9 | 419 | 21·6 |
| 2° | 854 | 20·1 | 708 | 20·1 | 122 | 19·7 | 1195 | 23·2 | 823 | 23·0 | 317 | 23·1 | 1178 | 19·9 | 742 | 20·4 | 359 | 18·5 |
| 3° | 816 | 19·3 | 703 | 20·0 | 95 | 15·4 | 889 | 17·3 | 627 | 17·5 | 233 | 17·0 | 1180 | 20·0 | 782 | 21·4 | 342 | 17·6 |
| 4° | 857 | 20·3 | 745 | 21·2 | 96 | 15·5 | 1001 | 19·5 | 734 | 20·5 | 244 | 17·8 | 1185 | 20·0 | 772 | 21·2 | 368 | 18·9 |
| 5° (highest) | 830 | 19·7 | 674 | 19·2 | 146 | 23·6 | 1021 | 19·9 | 705 | 19·7 | 298 | 21·7 | 1188 | 20·1 | 698 | 19·1 | 455 | 23·4 |
| Age (years) | ||||||||||||||||||
| ≤24 | 1947 | 46·1 | 1576 | 44·9 | 320 | 51·8 | 2362 | 45·0 | 1633 | 44·7 | 640 | 45·5 | 2755 | 46·6 | 1666 | 45·7 | 914 | 47·0 |
| 25–34 | 1717 | 40·6 | 1448 | 41·2 | 236 | 38·2 | 2309 | 44·0 | 1615 | 44·3 | 618 | 43·9 | 2572 | 43·5 | 1606 | 44·1 | 846 | 43·5 |
| ≥35 | 563 | 13·3 | 488 | 13·9 | 62 | 10·0 | 577 | 11·0 | 400 | 11·0 | 149 | 10·6 | 586 | 9·9 | 373 | 10·2 | 183 | 9·5 |
| Participant perinatal characteristics | ||||||||||||||||||
| Sex | ||||||||||||||||||
| Male | 2195 | 51·9 | 1816 | 51·7 | 323 | 52·3 | 2603 | 49·6 | 1707 | 46·8 | 790 | 56·1 | 3037 | 51·4 | 1754 | 48·1 | 1089 | 56·1 |
| Female | 2034 | 48·1 | 1698 | 48·3 | 295 | 47·7 | 2645 | 50·4 | 1941 | 53·2 | 618 | 43·9 | 2876 | 48·6 | 1892 | 51·9 | 854 | 43·9 |
Variables marked in bold represent significant statistical differences between followed-up and lost participants at 11, 22 and 30 years (P < 0·05).
Participants with information regarding the FFQ.
Total deaths from birth to 11 (98 deaths), 22 (193 deaths) and 30 (325 deaths) years were discounted from the total n of lost participants.
Table 2 shows that, considering the 11-year participants, about 72 % of them were attending the fourth or fifth scholar years. Among the 22-year participants, 41 % reported 9–11 years of schooling; and for the 30-year participants, 44 % reported ≥12 years of schooling. In all the three cohorts, most of participants self-reported white skin colour (Table 2).
Table 2.
Sample description according to current characteristics (participants with information regarding the FFQ) at 11-year (2004 Cohort), 22-year (1993 Cohort) and 30-year (1982 Cohort) follow-ups
| Variables | 2004 Cohort | 1993 Cohort | 1982 Cohort | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| n 3514 | n 3648 | n 3646 | ||||
| Participants’ current characteristics | ||||||
| Skin colour | ||||||
| White | 2359 | 67·5 | 2176 | 63·0 | 2768 | 76·0 |
| Black | 441 | 12·6 | 526 | 15·3 | 573 | 15·7 |
| Brown/yellow/indigenous | 696 | 19·9 | 750 | 21·7 | 303 | 8·3 |
| Schooling (year/scholar grade) | ||||||
| ≤3° | 231 | 6·7 | – | – | ||
| 4–5° | 2489 | 71·7 | – | – | ||
| 6–7° | 748 | 21·6 | – | – | ||
| Schooling (completed years) | ||||||
| 0–4 | – | 108 | 3·0 | 223 | 6·2 | |
| 5–8 | – | 988 | 27·1 | 720 | 19·9 | |
| 9–11 | – | 1496 | 41·0 | 1087 | 30·0 | |
| ≥12 | – | 1051 | 28·9 | 1590 | 43·9 | |
| Mean | sd | Mean | sd | Mean | sd | |
| Monthly family income (in Brazilian Reais) | 3177·5 | 4698·7 | 3215·2 | 3517·5 | 3388·0 | 4296·9 |
The average energy contribution from ultra-processed foods, adjusted for perinatal and current characteristics, was higher in the younger cohort (at age 11) (33·8 %; 95 % CI 33·6, 34·0) than in the 1993 Cohort (29·6 %; 95 % CI 29·4, 29·8) and in the older cohort (at age 30) (25·1 %; 95 % CI 24·7, 25·4). On the other hand, the proportion of energies from unprocessed or minimally processed foods was lower in the younger cohort: 52·2 % (95 % CI 51·9, 52·4), 56·0 % (95 % CI 55·7, 56·2) and 58·8 (95 % CI 58·6, 59·1) at 11, 22 and 30 years, respectively (Fig. 1).
Fig. 1.
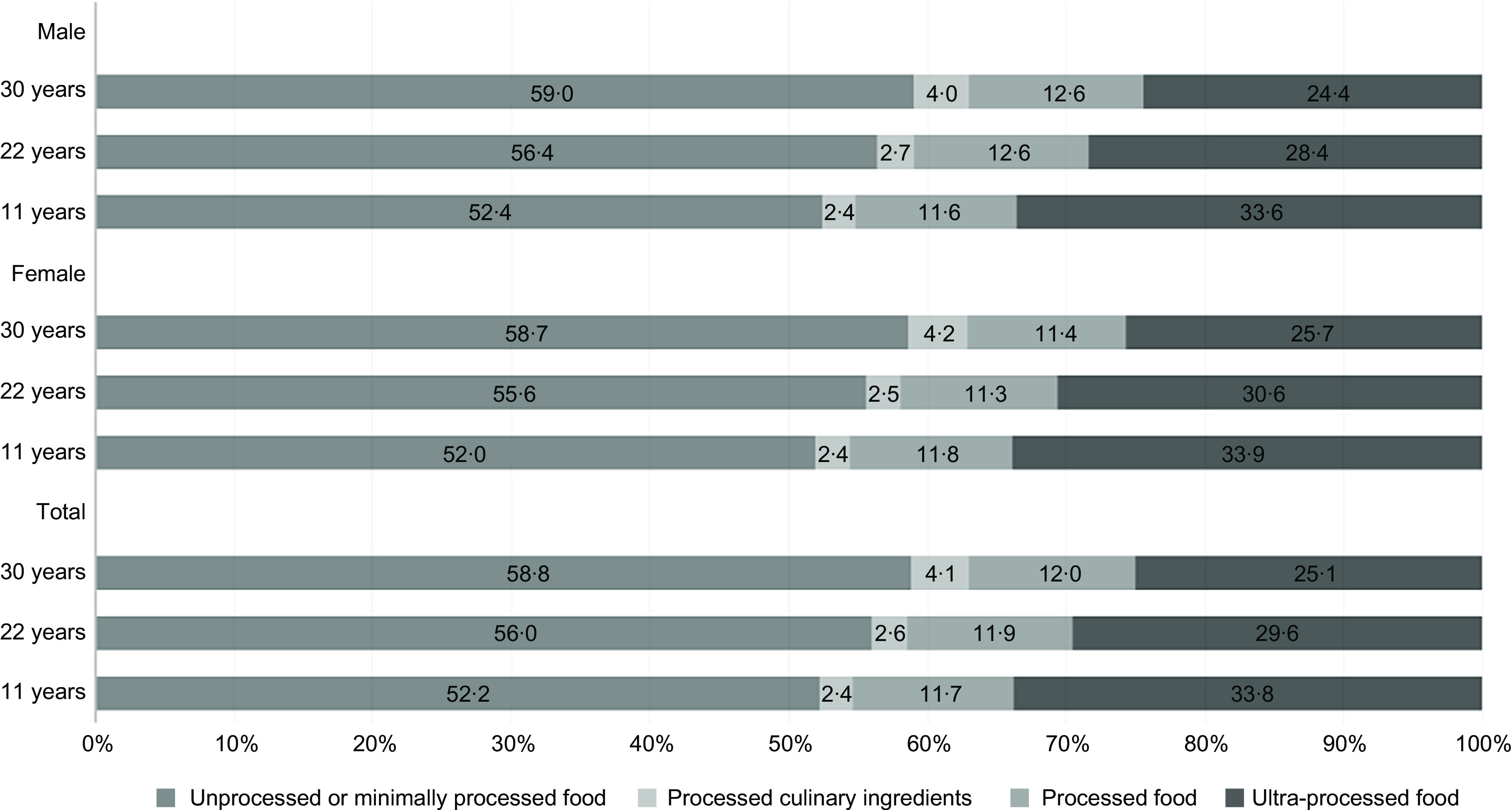
Mean energy contribution (%) from each food processing group at 11, 22 and 30 years, respectively, in the 2004, 1993 and 1982 Pelotas Birth Cohorts, adjusted for perinatal (monthly family income and maternal age, schooling and skin color) and current characteristics (sex, skin colour, schooling, monthly family income, diet for weight loss and energy intake/energy expenditure ratio)
Table 3 shows the average proportions of energy contribution from ultra-processed foods, according to perinatal and current variables. In the 2004 and 1993 Cohorts, those whose mothers self-declared as black had higher mean daily energy contribution from ultra-processed foods, compared to those whose mothers declared themselves as white, as well as those self-declared as brown, yellow or indigenous in the 1993 Cohort. In the two younger cohorts, the average daily contribution from ultra-processed foods was higher among children of younger mothers who had lower schooling and belonged to poorer families. For the 1982 Cohort, the opposite was observed, with the highest averages of energy contribution coming from ultra-processed foods observed among those whose mothers had higher schooling and belonged to wealthiest families. Higher contributions from ultra-processed foods were observed in the 1993 Cohort among those who self-declared as black, brown, yellow or indigenous, compared to those who declared themselves as white; and in the 1993 and 1982 Cohorts, among the women. The lower level of education in the 2004 and 1993 Cohorts and higher education in the 1982 Cohort were associated to higher averages of energy contribution from ultra-processed foods. In the 2004 and 1993 Cohorts, the poorest – and in the 1982 Cohort, the richest – presented higher average energy contributions from ultra-processed foods (Table 3).
Table 3.
Crude mean energy contribution from ultra-processed foods (%) at 11, 22 and 30 years, respectively, in the 2004, 1993 and 1982 Pelotas Birth Cohorts, according to perinatal and current demographic and socioeconomic characteristics
| Variables | Mean energy contribution from ultra-processed foods (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2004 Cohort | 1993 Cohort | 1982 Cohort | |||||||
| Mean | 95 % CI | P | Mean | 95 % CI | P | Mean | 95 % CI | P | |
| Maternal characteristics | |||||||||
| Skin colour | 0·021 | <0·001 | 0·966 | ||||||
| White | 33·3 | 32·8, 33·7 | 29·1 | 28·6, 29·6 | 25·1 | 24·7, 25·5 | |||
| Black | 34·7 | 33·8, 35·5 | 31·6 | 30·6, 32·5 | 25·1 | 24·2, 26·0 | |||
| Brown/yellow/indigenous | 33·6 | 32·0, 35·1 | 32·0 | 30·1, 33·8 | – | ||||
| Age (years) | 0·030 | 0·030 * | 0·284 | ||||||
| ≤24 | 34·1 | 33·6, 34·7 | 30·2 | 29·6, 30·9 | 24·9 | 24·3, 25·4 | |||
| 25–34 | 33·0 | 32·4, 33·6 | 29·3 | 28·6, 29·9 | 25·2 | 24·6, 25·7 | |||
| ≥35 | 33·4 | 32·3, 34·5 | 29·2 | 28·0, 30·4 | 25·8 | 24·6, 27·0 | |||
| Schooling (completed years) | <0·001 * | <0·001 * | <0·001 * | ||||||
| 0–4 | 34·4 | 33·3, 35·5 | 30·6 | 29·8, 31·4 | 23·6 | 23·0, 24·2 | |||
| 5–8 | 34·3 | 33·7, 35·0 | 30·1 | 29·5, 30·7 | 25·3 | 24·8, 25·8 | |||
| 9–11 | 32·8 | 32·1, 33·4 | 28·9 | 27·9, 29·8 | 26·5 | 25·4, 27·6 | |||
| ≥12 | 32·4 | 31·2, 33·6 | 26·0 | 24·8, 27·2 | 26·9 | 25·9, 27·8 | |||
| Monthly family income (quintiles) | 0·004 * | <0·001 * | <0·001 * | ||||||
| 1° (lowest) | 34·3 | 33·4, 35·2 | 30·5 | 29·6, 31·5 | 22·9 | 22·0, 23·7 | |||
| 2° | 33·5 | 32·6, 34·4 | 30·4 | 29·5, 31·3 | 24·4 | 23·6, 25·2 | |||
| 3° | 34·0 | 33·1, 34·9 | 30·3 | 29·3, 31·3 | 25·3 | 24·5, 26·0 | |||
| 4° | 33·9 | 33·0, 34·7 | 29·9 | 29·0, 30·7 | 25·9 | 25·2, 26·7 | |||
| 5° (highest) | 32·0 | 31·2, 32·9 | 27·5 | 26·6, 28·4 | 26·8 | 26·0, 27·6 | |||
| Participants’ characteristics | |||||||||
| Sex | 0·581 | <0·001 | <0·001 | ||||||
| Male | 33·5 | 32·9, 34·0 | 28·5 | 27·9, 29·1 | 24·4 | 23·9, 24·8 | |||
| Female | 33·7 | 33·1, 34·3 | 30·8 | 30·2, 31·3 | 25·8 | 25·3, 26·3 | |||
| Skin colour | 0·058 | <0·001 | 0·354 | ||||||
| White | 33·3 | 32·8, 33·8 | 29·0 | 28·5, 29·5 | 25·1 | 24·7, 25·5 | |||
| Black | 34·7 | 33·6, 35·8 | 31·6 | 30·5, 32·8 | 25·5 | 24·5, 26·4 | |||
| Brown/yellow/indigenous | 33·9 | 33·0, 34·8 | 30·6 | 29·7, 31·5 | 24·4 | 23·1, 25·6 | |||
| Schooling (year/scholar grade) | 0·015 * | – | – | ||||||
| ≤3° | 35·5 | 33·9, 37·1 | – | – | |||||
| 4–5° | 33·6 | 33·1, 34·0 | – | – | |||||
| 6–7° | 33·0 | 32·2, 33·9 | – | – | |||||
| Schooling (completed years) | – | <0·001 * | <0·001 * | ||||||
| 0–4 | – | 33·1 | 30·6, 35·7 | 22·0 | 20·5, 23·5 | ||||
| 5–8 | – | 31·5 | 30·7, 32·3 | 23·7 | 22·9, 24·5 | ||||
| 9–11 | – | 29·9 | 29·3, 30·6 | 25·8 | 25·2, 26·5 | ||||
| ≥12 | – | 27·3 | 26·6, 28·0 | 25·7 | 25·2, 26·2 | ||||
| Monthly family income (quintiles) | 0·016 * | <0·001 * | 0·003 * | ||||||
| 1° (lowest) | 34·3 | 33·4, 35·3 | 30·1 | 29·1, 31·1 | 24·1 | 23·2, 25·0 | |||
| 2° | 33·6 | 32·7, 34·5 | 30·9 | 29·9, 31·9 | 25·2 | 24·4, 26·0 | |||
| 3° | 33·8 | 32·9, 34·6 | 29·9 | 29·0, 30·9 | 24·6 | 23·8, 25·4 | |||
| 4° | 33·4 | 32·6, 34·1 | 29·9 | 29·0, 30·8 | 25·9 | 25·1, 26·7 | |||
| 5° (highest) | 32·7 | 31·8, 33·6 | 27·3 | 26·5, 28·2 | 25·6 | 24·9, 26·4 | |||
| Total (crude) | 33·6 | 33·2, 34·0 | 29·7 | 29·3, 30·1 | 25·1 | 24·7, 25·4 | |||
Mean differences evaluated by linear regression. Values in bold represent statistically significant associations.
P-value for linear trend.
In the adjusted analysis, in the 2004 and 1993 Cohorts, those whose mothers self-reported as black presented a higher energy contribution from ultra-processed foods, as well as those self-declared as brown, yellow or indigenous in the 1993 Cohort, compared to white skin colour. The same was observed in the 1982 Cohort participants who self-declared as black (Table 4). The effect of maternal perinatal schooling on energy contribution from ultra-processed foods to daily energy intake was maintained: in the 2004 and 1993 Cohorts, higher average values were observed among those of less educated mothers; and in the 1982 Cohort, among those of more educated mothers. The same direction was observed for family income in the 1982 Cohort, with participants from richer families showing higher average energy contributions from ultra-processed foods. Also, compared to their counterparts, higher average energy contributions from ultra-processed foods were observed among women in the 1993 (30·7; 95 % CI 30·2, 31·3) and 1982 (25·8; 95 % CI 25·3, 26·3) Cohorts; among individuals with lower education in the 1993 Cohort; and in those with 9–11 completed years of study in the 1982 Cohort (Table 4).
Table 4.
Adjusted analysis of mean energy contribution from ultra-processed foods (%) at 11, 22 and 30 years, respectively, in the 2004, 1993 and 1982 Pelotas Birth Cohorts, according to perinatal and current demographic and socioeconomic variables
| Variables | Mean energy contribution from ultra-processed foods (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2004 Cohort | 1993 Cohort | 1982 Cohort | |||||||
| Mean | 95 % CI | P | Mean | 95 % CI | P | Mean | 95 % CI | P | |
| Maternal characteristics | |||||||||
| First level | |||||||||
| Skin colour | 0·023 | <0·001 | 0·978 | ||||||
| White | 33·3 | 32·8, 33·7 | 29·1 | 28·6, 29·6 | 25·1 | 24·7, 25·5 | |||
| Black | 34·6 | 33·8, 35·5 | 31·6 | 30·6, 32·5 | 25·1 | 24·3, 25·9 | |||
| Brown/yellow/indigenous | 33·6 | 32·1, 35·1 | 32·0 | 30·1, 33·8 | – | ||||
| Age (years) | 0·034 | 0·087 | 0·264 | ||||||
| ≤24 | 34·1 | 33·5, 34·7 | 30·2 | 29·6, 30·8 | 24·8 | 24·3, 25·4 | |||
| 25–34 | 33·0 | 32·4, 33·6 | 29·3 | 28·7, 29·9 | 25·2 | 24·6, 25·7 | |||
| ≥35 | 33·4 | 32·3, 34·5 | 29·2 | 28·0, 30·4 | 25·8 | 24·7, 26·1 | |||
| Second level | |||||||||
| Schooling (completed years) | 0·003 * | <0·001 * | 0·031 * | ||||||
| 0–4 | 34·3 | 33·3, 35·4 | 30·5 | 29·7, 31·2 | 24·2 | 23·5, 24·9 | |||
| 5–8 | 34·2 | 33·6, 34·8 | 30·1 | 29·5, 30·7 | 25·3 | 24·7, 25·9 | |||
| 9–11 | 32·8 | 32·2, 33·5 | 29·0 | 28·1, 30·0 | 25·9 | 24·8, 27·0 | |||
| ≥12 | 32·8 | 31·5, 34·1 | 26·4 | 24·9, 27·8 | 25·9 | 24·7, 27·2 | |||
| Monthly family income (quintiles) | 0·217 | 0·194 | <0·001 * | ||||||
| 1° (lowest) | 33·8 | 32·9, 34·8 | 29·9 | 29·0, 30·9 | 23·4 | 22·5, 24·3 | |||
| 2° | 33·1 | 32·2, 34·0 | 30·1 | 29·2, 30·9 | 24·8 | 24·0, 25·7 | |||
| 3° | 33·9 | 33·1, 34·8 | 30·1 | 29·1, 31·1 | 25·3 | 24·5, 26·0 | |||
| 4° | 34·2 | 33·4, 35·1 | 29·9 | 29·0, 30·8 | 25·7 | 24·9, 26·5 | |||
| 5° (highest) | 32·9 | 31·9, 33·9 | 28·5 | 27·5, 29·6 | 26·2 | 25·1, 27·2 | |||
| Participants’ characteristics | |||||||||
| Third level | |||||||||
| Sex | 0·467 | <0·001 | <0·001 | ||||||
| Male | 33·5 | 33·0, 34·1 | 28·5 | 27·9, 29·1 | 24·4 | 23·9, 24·9 | |||
| Female | 33·8 | 33·2, 34·4 | 30·7 | 30·2, 31·3 | 25·8 | 25·3, 26·3 | |||
| Skin colour | 0·806 | 0·594 | 0·011 | ||||||
| White | 33·7 | 33·1, 34·2 | 29·5 | 28·9, 30·1 | 24·8 | 24·4, 25·2 | |||
| Black | 34·0 | 32·6, 35·4 | 30·3 | 28·9, 31·8 | 26·4 | 25·5, 27·3 | |||
| Brown/yellow/indigenous | 33·5 | 32·5, 34·4 | 30·1 | 29·1, 31·0 | 25·0 | 23·8, 26·3 | |||
| Fourth level | |||||||||
| Schooling (year/scholar grade) | 0·200 | – | – | ||||||
| ≤3° | 35·0 | 33·4, 36·6 | – | – | |||||
| 4–5° | 33·6 | 33·1, 34·0 | – | – | |||||
| 6–7° | 33·4 | 32·5, 34·3 | – | – | |||||
| Schooling (completed years) | – | <0·001 * | <0·001 | ||||||
| 0–4 | – | 33·4 | 31·0, 35·8 | 23·1 | 21·7, 24·5 | ||||
| 5–8 | – | 31·6 | 30·7, 32·4 | 24·6 | 23·7, 25·4 | ||||
| 9–11 | – | 29·8 | 29·2, 30·5 | 26·2 | 25·5, 26·8 | ||||
| ≥12 | – | 27·4 | 26·6, 28·2 | 24·9 | 24·4, 25·5 | ||||
| Monthly family income (quintiles) | 0·932 | 0·123 | 0·265 | ||||||
| 1° (lowest) | 33·9 | 33·0, 34·8 | 29·1 | 28·2, 30·1 | 24·9 | 24·0, 25·7 | |||
| 2° | 33·3 | 32·4, 34·2 | 30·4 | 29·5, 31·3 | 25·5 | 24·7, 26·3 | |||
| 3° | 33·6 | 32·8, 34·5 | 29·8 | 28·9, 30·8 | 24·6 | 23·8, 25·4 | |||
| 4° | 33·7 | 32·8, 34·6 | 30·1 | 28·2, 31·1 | 25·7 | 24·9, 26·5 | |||
| 5° (highest) | 33·6 | 32·6, 34·6 | 28·9 | 27·9, 29·9 | 24·8 | 23·9, 25·7 | |||
Analyses by multiple linear regression. Values in bold represent statistically significant associations.
P-value for linear trend.
Discussion
In summary, the current study showed that energy contribution from ultra-processed foods was higher among participants from the 2004 Cohort (at age 11), while the contribution of fresh or processed foods was higher in the 1982 Cohort (at age 30). Black maternal skin colour in the 2004 and 1993 Cohorts was associated to a higher energy contribution from ultra-processed foods, as well as among the 1982 Cohort members. Maternal schooling was associated to ultra-processed food consumption in the three cohorts (higher consumption among participants from less-schooled mothers in the 2004 and 1993 Cohorts, with an inverse dose–response; and higher consumption among participants from more-schooled mothers in the 1982 Cohort, with a direct dose–response). Perinatal family income was associated to the highest energy contribution from ultra-processed foods only in the 1982 Cohort. Also, female sex in the 1993 and 1982 Cohorts, lower participant schooling in the 1993 Cohort, and higher participant schooling in the 1982 Cohort were associated to a higher energy contribution from ultra-processed foods.
Energy intake from ultra-processed foods in the three cohorts ranged from 25 to 33 %. Three studies with a nationwide representative sample – one carried out in Brazil in 2008–2009, two others with data from the Mexican (in 2012) and Chilean (in 2010) population – found similar values(10,28,29). Lower consumption of ultra-processed foods according to increasing age has been observed among Mexicans, Chileans and Canadians(12,28,29). Children and adolescents may represent populations that are more vulnerable to advertisements on ultra-processed products, which may influence their eating behaviours, perceptions and preferences(30,31).
In the 2004 and 1993 Cohorts, those whose mothers self-declared black skin colour, as well as the participants of the 1982 Cohort, presented a higher energy contribution from ultra-processed foods. It is possible that these results are due to less access to information in health services of individuals with non-white skin colour due to racial discrimination or lower schooling(32,33).
Also in the 2004 and 1993 Cohorts, the relation of the energy contribution from ultra-processed foods with maternal schooling – and with participant schooling in the 1993 Cohort – were inverse; and in the 1982 Cohort, the relation with maternal and participant schooling was direct. It was expected that, in all the three cohorts, higher schooling would promote greater access to information and, consequently, healthier lifestyles. Most studies that evaluated the influence of schooling on ultra-processed food consumption found a direct relationship(10,12,28,34). Family income at birth was associated to energy contribution from ultra-processed foods only in the 1982 Cohort, with higher contributions observed among the richest. Other studies carried out in middle-income countries showed higher energy intake from these foods according to increasing income, possibly due to the greater purchasing power of the richest strata(10,28,29,34). Higher consumption of ultra-processed foods observed in the 1982 Cohort among participants of higher schooling and higher income may be due to eating habits acquired in childhood or adolescence. It is possible that the intensification of globalisation and industrialisation during the 1980s, which has promoted increased sophistication in food processing, marketing and distribution techniques, has also promoted greater access to foods of a higher processing level by those with higher purchasing power – in this case, mothers with higher income and schooling on the birth occasion of the 1982 Cohort members(2,4). Together, during the same period, limited concern to healthy diets and body weight by health services or the media may have promoted the development of preferences based on ultra-processed foods(35).
Regarding sex, a higher contribution from ultra-processed foods was observed among women in the 1993 and 1982 Cohorts, but not in the 2004 Cohort. Louzada etal., who evaluated Brazilians ≥10 years of age, found a higher consumption of ultra-processed foods among females, compared to males. Mais etal. found null results when evaluating children from 2 to 9 years of age(10,36). The results of the current study are not in line with our expectation, considering that women represent the portion of a population using health services the most and, consequently, having greater access to food-related information(37–39). No differences were observed between boys and girls in the 2004 Cohort, possibly due to the existence of other determinants strongly related to consumption, such as dietary habits of the family.
It is important to highlight some limitations of this study. The method used to evaluate food consumption (FFQ) tends to overestimate energy intake, because it includes a large quantity of food items, thus generating a greater sum of energies compared, for example, to food recalls(40). The FFQ used in the Pelotas Birth Cohorts was developed specifically to evaluate the studied population, which reflects the contexts of foods and preparations commonly reported by this population(17). However, the processing degree was not evaluated, which made it impossible to obtain additional information about food preparation. For this reason, the food items from the FFQ were classified in a more conservative way, with culinary preparations such as lasagne, for example, considered as minimally processed foods; and breads (whole or white) classified as processed foods (see online supplementary material, Supplementary Table). The few foods that differ between the FFQ used in the three cohorts have a very low percentage of contribution in relation to total energy consumption (<0·75 % on average; see online supplementary material, Supplementary Table). In addition, the use of percentage of contribution of each processing group aimed to minimise overestimation by representing a measure relative to total energy consumption. The classification of foods according to their processing degree (NOVA) is recent, but its concepts are well established in the literature and recognised by international agencies (Pan-American Health Organization and the UN Organization for Food and Agriculture – FAO) as an important instrument to evaluate the nutritional quality of diets(8,41).
Regarding the losses of follow-up, some differences were observed between those followed and those lost for the three cohorts. In the 11- and 30-year follow-ups, higher losses were observed between the extreme categories of maternal schooling and family income; therefore, some possible bias in the overall estimate regarding energy contribution from ultra-processed foods may have occurred. In the 22- and 30-year follow-ups, a higher proportion of women was evaluated compared to men. Considering this differential loss, the overall proportion of outcome in the 1993 and 1982 Cohorts could be lower than that observed. Also, in the 2004 Cohort, a higher proportion of losses was observed among children of younger mothers (≤24 years); however, maternal age was not associated with outcome in any of the cohorts, considering that CIs are overlapping, and therefore, this differential loss may not interfere in the overall proportion of outcome at 11 years.
Among the study strengths, the calculation of energy contribution of each processing group was adjusted for the variables ‘diet for weight loss’ and ‘energy expenditure/consumption ratio’. Individuals who diet for weight loss tend to present information bias, with underestimated consumption(42,43). Energy consumption/expenditure ratio was included in the adjustment variables as an alternative to the exclusion of outlier values from the FFQ report, aiming to avoid sample losses. Furthermore, the use of data from the three birth cohorts – representative of individuals of the same age groups in medium-sized municipalities who applied the same eligibility criteria in their samples and same fieldwork logistics – represents another strength of this study. Additionally, considering follow-up studies of this size, high response rates were obtained in the three cohorts.
In this study, the contribution of ultra-processed foods to total daily energy consumption was higher among younger cohorts. Maternal schooling was associated to the consumption of these foods in the three cohorts, indicating an inverse dose–response relationship in the 2004 and 1993 Cohorts, and a direct relationship in the 1982 Cohort. These findings indicate that information from nutrition public policies requires greater dissemination among population groups with lower schooling and income, mainly girls and women. Other measures aimed at promoting healthy eating, such as regulation of food advertising focused on children and adolescents and promotion of the Dietary Guidelines for the Brazilian Population(6) by the media, are extremely necessary. Along with that, changes in food taxation, with decreasing costs of unprocessed and minimally processed products and increasing costs of ultra-processed products, represent important strategies to promote the reduction of consumption of these foods in our country.
Acknowledgements
Acknowledgements: This study was conducted in a post-graduate programme supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) – Finance Code 001; and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico – Brazil (CNPq). Financial support: This work was supported by the Wellcome Trust (grant number 086974/Z/08/Z) at the 30-year follow-up for the 1982 Cohort, and by DECIT (Departamento de Ciência e Tecnologia) and the Conselho Nacional de Desenvolvimento Científico e Tecnológico- Brazil CNPq (grant number 400943/2013–1) at the 22- and 11-year follow-ups for the 1993 and 2004 Cohorts, respectively. Conflict of interest: None. Authorship: C.S.C., M.C.F.A. and I.S.S. made substantial contribution to the conception and design, data acquisition, analysis and interpretation; drafted the article and revised it critically for important intellectual content; and approved the final version of manuscript to be published. J.S.V., F.R., I.O.B., A.M., B.L.H., H.G. and F.C.W. made substantial contribution to the analysis and interpretation; revised the article critically for important intellectual content; and approved the final version of manuscript to be published. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the Ethics Committee of the Faculty of Medicine of the Federal University of Pelotas (889 753, 1 250 366 and 16/12, respectively, for the 2004, 1993 and 1982 Cohorts). Written informed consent was obtained from all subjects/patients. Participants of the 1993 and 1982 Cohorts signed a consent term. In the 2004 Cohort, the mother or legal guardian signed the consent term; and the adolescent, the assent term.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980019004245.
click here to view supplementary material
References
- 1. Ng M, Fleming T, Robinson M et al. (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384, 766–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Popkin BM (2006) Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases. Am J Clin Nutr 84, 289–298. [DOI] [PubMed] [Google Scholar]
- 3. Martins APB, Levy RB, Claro RM et al. (2013) Participação crescente de produtos ultraprocessados na dieta brasileira (1987–2009) (Increased contribution of ultra-processed food products in the Brazilian diet (1987-2009)). Rev Saúde Pública 47, 656–665. [DOI] [PubMed] [Google Scholar]
- 4. Popkin BM (2006) Technology, transport, globalization and the nutrition transition food policy. Food Policy 31, 554–569. [Google Scholar]
- 5. Monteiro CA, Cannon G, Moubarac J-C et al. (2018) The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr 21, 5–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Brasil. Ministério da Saúde (2014) Guia alimentar para a população brasileira (Dietary Guidelines for the Brazilian Population), 2ª‾ Edição. Brasília: Ministério da Saúde, 156 p. [Google Scholar]
- 7. Fiolet T, Srour B, Sellem L et al. (2018) Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ 360, k322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. PAHO (2015) Ultra-Processed Food and Drink Products in Latin America: Trends, Impact on Obesity, Policy Implications. Washington, DC: Pan American Health Organization, 60 p. [Google Scholar]
- 9. Stuckler D, McKee M, Ebrahim S et al. (2012) Manufacturing epidemics: the role of global producers in increased consumption of unhealthy commodities including processed foods, alcohol, and tobacco. PLoS Med 9, e1001235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Louzada MLdC, Baraldi LG, Steele EM et al. (2015) Consumption of ultra-processed foods and obesity in Brazilian adolescents and adults. Preventive Med 81, 9–15. [DOI] [PubMed] [Google Scholar]
- 11. Baraldi LG, Steele EM, Canella DS et al. (2018) Consumption of ultra-processed foods and associated sociodemographic factors in the USA between 2007 and 2012: evidence from a nationally representative cross-sectional study. BMJ Open 8, e020574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Moubarac J-C, Batal M, Louzada M et al. (2017) Consumption of ultra-processed foods predicts diet quality in Canada. Appetite 108, 512–520. [DOI] [PubMed] [Google Scholar]
- 13. Rauber F, da Costa Louzada ML, Steele EM et al. (2018) Ultra-processed food consumption and chronic non-communicable diseases-related dietary nutrient profile in the UK (2008–2014). Nutrients 10, 587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Santos IS, Barros AJ, Matijasevich A et al. (2014) Cohort profile update: 2004 Pelotas (Brazil) Birth Cohort Study. Body composition, mental health and genetic assessment at the 6 years follow-up. Int J Epidemiol 43, 1437–1437f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Gonçalves H, Wehrmeister FC, Assunção MC et al. (2018) Cohort profile update: the 1993 Pelotas (Brazil) birth cohort follow-up at 22 years. Int J Epidemiol 47, 1389e–1390e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Horta BL, Gigante DP, Goncalves H et al. (2015) Cohort profile update: the 1982 Pelotas (Brazil) birth cohort study. Int J Epidemiol 44, 441e–441e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Schneider BC, dos Santos Motta JV, Muniz LC et al. (2018) Desenho de um questionário de frequência alimentar digital autoaplicado para avaliar o consumo alimentar de adolescentes e adultos jovens: coortes de nascimentos de Pelotas, Rio Grande do Sul (Design of a digital and self-reported food frequency questionnaire to estimate food consumption in adolescents and young adults: birth cohorts at Pelotas, Rio Grande do Sul, Brazil). Rev Bras Epidemiol 19, 419–432. [DOI] [PubMed] [Google Scholar]
- 18. Pinheiro ABV, Lacerda EMdA, Benzecry EH et al. (2005) Tabela para avaliação de consumo alimentar em medidas caseiras (Table for Assessment of Food Intake in Household Measures), 5th ed. Rio de Janeiro: Atheneu. [Google Scholar]
- 19. Universidade Estadual de Campinas, Núcleo de Estudos e Pesquisas em Alimentação – NEPA (2006) Tabela brasileira de composição de alimentos – TACO (Brazilian Food Composition Table – TACO), 2nd ed. Campinas (SP): UNICAMP. [Google Scholar]
- 20. USDA (2011) National Nutrient Database for Standard Reference [Internet]. Beltsville: Human Nutrition Research Center, Nutrient Data Laboratory. www.ndb.nal.usda.gov (accessed May 2018).
- 21. Leech RM, Worsley A, Timperio A et al. (2018) The role of energy intake and energy misreporting in the associations between eating patterns and adiposity. Euro J Clin Nutr 72, 142. [DOI] [PubMed] [Google Scholar]
- 22. Institute of Medicine (2005) Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Institute of Medicine of the National Academies, 2002 and 2005. Washington, DC: The National Academies Press. www.nap.edu (accessed May 2018). [Google Scholar]
- 23. Onis Md, Onyango AW, Borghi E et al. (2007) Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ 85, 660–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. World Health Organization (WHO) (1995) Physical Status: The Use and Interpretation of Anthropometry. Geneva: WHO. Report of a WHO Expert Committee. WHO Technical Report Series. 854. [PubMed] [Google Scholar]
- 25. da Silva IC, van Hees VT, Ramires VV et al. (2014) Physical activity levels in three Brazilian birth cohorts as assessed with raw triaxial wrist accelerometry. Int J Epidemiol 43, 1959–1968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Harris PA, Taylor R, Thielke R et al. (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42, 377–381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Victora CG, Huttly SR, Fuchs SC et al. (1997) The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. Int J Epidemiol 26, 224–227. [DOI] [PubMed] [Google Scholar]
- 28. Marrón-Ponce JA, Sánchez-Pimienta TG, da Costa Louzada ML et al. (2018) Energy contribution of NOVA food groups and sociodemographic determinants of ultra-processed food consumption in the Mexican population. Public Health Nutr 21, 87–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Cediel G, Reyes M, da Costa Louzada ML et al. (2018) Ultra-processed foods and added sugars in the Chilean diet (2010). Public Health Nutr 21, 125–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Henriques P, Dias PC & Burlandy L (2014) A regulamentação da propaganda de alimentos no Brasil: convergências e conflitos de interesses (Regulation of food advertising in Brazil: convergence and conflicts of interest). Cad Saúde Pública 30, 1219–1228. [DOI] [PubMed] [Google Scholar]
- 31. Kelly B, Halford JC, Boyland EJ et al. (2010) Television food advertising to children: a global perspective. Am J Public Health 100, 1730–1736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Chor D & Lima CRdA (2005) Aspectos epidemiológicos das desigualdades raciais em saúde no Brasil (Epidemiologic aspects of racial inequalities in health in Brazil). Cad Saúde Pública 21, 1586–1594. [DOI] [PubMed] [Google Scholar]
- 33. Phelan JC & Link BG (2015) Is racism a fundamental cause of inequalities in health? Annu Rev Sociol 41, 311–330. [Google Scholar]
- 34. Simões BDS, Cardoso LdO, Benseñor IJM et al. (2018) Consumption of ultra-processed foods and socioeconomic position: a cross-sectional analysis of the Brazilian Longitudinal Study of Adult Health. Cad Saúde Pública 34, e00019717. [DOI] [PubMed] [Google Scholar]
- 35. Barros AJ, Victora CG, Santos IS et al. (2008) Infant malnutrition and obesity in three population-based birth cohort studies in Southern Brazil: trends and differences. Cad Saúde Pública 24, Suppl. 3, s417–s426. [DOI] [PubMed] [Google Scholar]
- 36. Mais LA, Warkentin S, Vega JB et al. (2018) Sociodemographic, anthropometric and behavioural risk factors for ultra-processed food consumption in a sample of 2–9-year-olds in Brazil. Public Health Nutr 21, 77–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Levorato CD, Mello LMd, Silva ASd et al. (2014) Fatores associados à procura por serviços de saúde numa perspectiva relacional de gênero (Factors associated with the demand for health services from a gender-relational perspective). Ciên Saúde Colet 19, 1263–1274. [DOI] [PubMed] [Google Scholar]
- 38. Assumpção Dd, Domene SMÁ, Fisberg RM et al. (2017) Diferenças entre homens e mulheres na qualidade da dieta: estudo de base populacional em Campinas, São Paulo (Differences between men and women in the quality of their diet: a study conducted on a population in Campinas, São Paulo, Brazil). Ciên Saúde Colet 22, 347–358. [Google Scholar]
- 39. Guibu IA, Moraes JCd, Guerra AA et al. (2017) Características principais dos usuários dos serviços de atenção primária à saúde no Brasil (Main characteristics of patients of primary health care services in Brazil). Rev Saúde Pública 51, Suppl. 2, 17s. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Willett WC (1994) Future directions in the development of food-frequency questionnaires. Am J Clin Nutr 59, Suppl. 1, 171S–174S. [DOI] [PubMed] [Google Scholar]
- 41. FAO (2015) Guidelines on the Collection of Information on Food Processing Through Food Consumption Surveys. Rome: Food and Agriculture Organization. [Google Scholar]
- 42. Briefel R, Sempos C, McDowell M et al. (1997) Dietary methods research in the third National Health and Nutrition Examination survey: underreporting of energy intake. Am J Clin Nutr 65, Suppl. 4, 1203S–1209S. [DOI] [PubMed] [Google Scholar]
- 43. Institute of Medicine (2002) Dietary Risk Assessment in the WIC Program. Committee on Dietary Risk Assessment in the WIC Program, p. 167. Washington, DC: The National Academies Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980019004245.
click here to view supplementary material